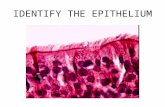
Name the tissue. Ciliated pseudostratified columnar epithelium.
Upload
yeong-yeh-leeCategory
view
222download
0
Dm
YMAa
b
c
d
e
f
a
ARRA
KSHMF
1
eca
vK
1d
Medical Engineering & Physics 34 (2012) 279– 289
Contents lists available at ScienceDirect
Medical Engineering & Physics
jou rna l h omepa g e: www.elsev ier .com/ locate /medengphy
evelopment and validation of a probe allowing accurate and continuousonitoring of location of squamo-columnar junction
eong Yeh Leea,b, John P. Seenana, James G.H. Whitingc, Elaine V. Robertsona,ohammad H. Derakhshana, Angela A. Wirzd, Donald Smithe, Chris Hardyf,
ndrew Kelmana, Patricia Connollyc, Kenneth E.L. McColl a,∗
Institute of Cardiovascular and Medical Sciences, University of Glasgow, Glasgow, United KingdomDepartment of Medicine, Universiti Sains Malaysia, Kota Bahru, Kelantan, MalaysiaBioengineering, University of Strathclyde, Glasgow, United KingdomDyspepsia Research Clinic, Gartnavel General Hospital, Glasgow, United KingdomMedical Devices Unit, Department of Clinical Physics, Southern General Hospital, Glasgow, United KingdomSchool of Engineering, University of Glasgow, United Kingdom
r t i c l e i n f o
rticle history:eceived 3 May 2011eceived in revised form 13 July 2011ccepted 15 July 2011
eywords:quamo-columnar junctionall Effectagnet
luoroscopy
a b s t r a c t
Introduction: Most pathology of the upper gastrointestinal tract now occurs close to the gastro-oesophageal squamo-columnar junction (SCJ). Studying the pathophysiology of this region even usinghigh resolution pH, impedance and manometry is unreliable due to constant movement with respiration,swallowing and transient lower oesophageal sphincter relaxations.Aims and methods: A technique is reported allowing continuous real-time monitoring of the position ofthe SCJ. It involves endoscopically clipping a magnet (2 mm × 1 mm) to the SCJ and monitoring its positionrelative to a probe in the oesophago-gastric lumen. The latter has 26 Hall-Effect sensors mounted at 5 mmspacing on a circuit board within a silicone tube.Results: Bench studies: The recorded position of the magnet along the length of the probe was comparedwith its actual position. Accuracy was related to the distance between magnet and probe, orientation ofthe magnet relative to the probe and whether the magnet was anterior, posterior or lateral to the probe.Including all possible orientations of the magnet at or nearer than 10 mm from the probe, the medianaccuracy along the length of probe was 2.4 mm (IQR 2.1 mm). The proportion of all possible orientationswithin 10 mm of the probe giving an accuracy of ±10 mm was 88.9%. In vivo studies: With simultane-ous fluoroscopy, eight healthy subjects were asked to perform normal breathing, deep breathing, water
swallows and finally advancement and retraction of probe over a 12 cm segment. The position recordedby fluoroscopy and probe at each second interval were compared. The correlation co-efficient for all 224position readings was 0.96 (95% CI: 0.89–0.96). No significant interference was observed when the probewas tested alongside high resolution pH and manometry.Conclusion: Used in conjunction with high resolution pH, impedance and manometry, this technique willallow for the first time detailed studies at the squamo-columnar junction.. Introduction
Gastro-oesophageal reflux disease is probably the common-
st chronic disorder affecting the Western world [1]. It is theonsequence of acidic gastric juice refluxing from the stom-ch into the oesophagus and produces pain (heartburn) and∗ Corresponding author at: Institute of Cardiovascular and Medical Sciences, Uni-ersity of Glasgow, Gardiner Institute, 44 Church Street, Glasgow G11 6NT, Unitedingdom. Tel.: +44 0 141 211 2513; fax: +44 0 141 211 2895.
E-mail address: [email protected] (K.E.L. McColl).
350-4533/$ – see front matter © 2011 IPEM. Published by Elsevier Ltd. All rights reserveoi:10.1016/j.medengphy.2011.07.018
© 2011 IPEM. Published by Elsevier Ltd. All rights reserved.
erosive damage to the oesophageal mucosa. Persistent reflux isalso associated with columnar metaplasia and adenocarcinoma ofthe distal oesophagus [2,3]. In contrast to the columnar mucosaof the stomach, the normal squamous mucosa of the oesophagusis unable to tolerate the acidic and proteolytic nature of gastricjuice.
The transition between the columnar mucosa of the stomachand squamous mucosa of the oesophagus is abrupt and referred to
as the squamo-columnar junction (SCJ) or “Z-line” (Fig. 1). It nor-mally lies within the high pressure zone of the lower oesophagealsphincter (LOS) which is responsible for preventing reflux of gas-tric acid. However, such reflux commonly occurs usually in thed.

280 Y.Y. Lee et al. / Medical Engineering & Physics 34 (2012) 279– 289
Fig. 1. A cartoon depicting the anatomical relationship of various structures withinthe gastro-oesophageal junction. Note the central position of squamo-columnarjunction or “z” line within the gastro-oesophageal junction and this is easily seenendoscopically. The positioning of Hall Effect locator probe and the endoclip withmagnet within the gastro-oesophageal junction are also illustrated. LOS, lowero
ps
asplpnoppa
oStfismapmciiUai
tamtn
2
ss
Fig. 2. A schematic diagram of the locator system is shown here with a photo of theactual overlapping Hall Effect arrays shown above it. There are 13 Hall Effect sensorssoldered on each of the two overlapped printed circuit boards which are then coatedwith silicon tubing (Altecweb Ltd., UK). The probe is connected to a microprocessorbox which outputs through the polygraph machine (Medtronic®) as position (mm)
esophageal sphincter.
resence of functional or structural abnormalities of the high pres-ure zone.
A variety of investigational tools have been developed tollow monitoring of the structure and function of the gastroe-ophageal junction (GOJ) [4–6]. Most involve the insertion ofrobes so that they lie straddling the GOJ and recording the
uminal pH, the movement of fluids within the lumen and theressure of the LOS, oesophagus and stomach. Such probes areow available in high resolution form which allows simultane-us recording to be performed at 10 mm intervals for extendederiod of time [7–9]. These tools can record the frequency androximal extent of the reflux from the stomach into the oesoph-gus.
One deficiency in studies of the physiology and pathophysiol-gy of the GOJ is our lack of ability to monitor the location of theCJ and thus to know when gastric contents have refluxed ontohe oesophageal mucosa. The GOJ is highly dynamic and the SCJrequently moves up and down its cranial/caudal axis due to breath-ng, swallowing and transient relaxations of the lower oesophagealphincter (TLOSR) [10]. This movement can result in the SCJ inter-ittently moving as much as 9 cm proximally [10]. In order to
void artefactual detection of acid reflux by such movement, theH recordings are normally made 6–7 cm above the SCJ. However,ost damage from acid reflux occurs close to the SCJ and within a
entimetre or two of it [9] yet the luminal environment of this areas impossible to study with the currently available technology evenn its high resolution form. The Bravo capsule (Medtronic Inc., MN,SA) can provide information about pH close to the SCJ but only at
single position and placing it within the LOS may interfere withts physiology.
We have developed a novel probe to allow continuous moni-oring of the location of the SCJ which can be used alongside pHnd impedance and manometry equipment thereby allow moreeaningful interpretation of the data they provide. In particular,
he probe will allow us to study accurately the luminal environmentear to the SCJ.
. The Hall Effect locator probe
The method employed is based upon the ability of Hall Effectensors to detect the presence of a magnetic field. By clipping amall magnet to the SCJ, the position of the latter is monitored
and signal strength (mV).
by a series of Hall Effect sensors mounted along the length of aprobe positioned in the lumen of the upper gastrointestinal (GI)tract (Fig. 1).
First discovered by Edwin Hall, in 1879, Hall Effect consists ofvoltage generation as a result of difference in electrical potentialbetween the sides of a conductive material, for example silicon(Si) or gallium arsenide (GaAs) through which a current is flowingwhile in a magnetic field perpendicular to the current [11]. LinearHall Effect sensors produce a ratiometric analog voltage output thatresponds proportionately to magnetic field strength which in turndepends on “effective air gap” or distance between the sensor andthe magnet pole. In general these devices require a regulated volt-age of 5 V supply and the quiescent voltage output is 2.5 V whenthere is no significant magnetic field presence [12]. The Hall Effectsensor which we employed has a sensitivity of 10 mV/G, a recom-mended supply voltage in the range of 2.5–3.5 V (our device uses3.0 V) and offset voltage which is half of supply voltage (our devicehas offset voltage of 1.5 V). The maximum magnetic field strengththat the sensor can detect occurred when the sensor is subjected toapproximately 250 G (when samarium cobalt magnet with Br = 10.2to 10.5 kG was used).
Thirteen Hall Effect sensors each with a dimension of2 mm × 3 mm × 0.75 mm were soldered onto two flexible printed
circuit boards (width 3 mm) at 10 mm spacing (Fig. 2). One cir-cuit board was placed on top of the other so that there was alinear separation of 5 mm between sensors. They were then coatedusing medical grade high tensile strength silicone tubing with a
Y.Y. Lee et al. / Medical Engineering
Fig. 3. Photo illustrating a single use endoclip (model HX-201UR-135, Olympus, UK)with a small samarium cobalt magnet attached by heat shrinkable polyvinylidenefluoride (PLK175; PMG Plastronic Ltd., UK) (shown with black arrow).
bUctczEtcac
arPcnooatpotciPt
mmtleiitmeTuU
strength with increasing distance. The decay in signal strength wasgreater with decreasing degrees in rotation A compared to rotationB with absence of data for 0◦ in both. A lesser degree of decay in
ore of 3.2 mm and 0.8 mm wall (AlteSilTM, Altecweb.com Ltd.,K). Made of specially blended elastomer providing non-toxic andonsistent tubing life, the silicone tubing prevents bodily con-act with the probe’s electrical component [13]. The device wasompliant to electrical safety guidelines and International Organi-ation for Standardization (ISO) certified (BS: EN 60601-1:2006).lectrical safety measures include the probe interface unit’s elec-ronics being powered from a medical grade power adapter; alass II device with a leakage current <10 �A and enhanced with
DC–DC converter between the mains adapter and the electronicircuitry.
The circuit boards were connected to a microprocessor unitnd its digital output connected to a Medtronic Polygraphecorder (Synectics Medical Ltd., UK) and displayed using theolygramNETTM software (version 4.1.1322.28.7; Synectics Medi-al Ltd., UK). There are two outputs recorded from the locator probeamely position (in mm) along the length of the probe with a rangef 0–120 mm and signal strength (in millivolts or mV) with a rangef 0–1200 mV. The probe needs to be calibrated for its minimumnd its maximum working range with the Polygraph machine prioro use. Calibration involves first zeroing the probe at the minimumosition value of 0 mm and minimum strength value of 0 mV with-ut any presence of magnet and then calibrating the probe withhe magnet pole placed directly on top of the last sensor which willalibrate the maximum position value of 120 mm and the max-mum strength of 1200 mV. Raw data can be extracted from theolygramNETTM software at a frequency of 8 Hz and exported inhe ASCII format.
We employed a small high grade samarium cobalt (SmCo) discagnet (dimension of 2 mm diameter and 1 mm thickness) (e-agnets UK Ltd., UK) in our study. This magnet was chosen due
o its high magnetic strength and resistance to corrosion by bio-ogical fluids including gastric hydrochloric acid [14]. SmCo rarearth magnet is commonly used in orthodontic application andts biological effects were studied in animals and humans wheret was shown to have no direct toxic effects [15,16]. Furthermorehe magnet was securely attached using medical grade heat shrink
aterial (PLK175; PMG Plastronic Ltd., UK) onto the single usendoclip (HX-201UR-135; Olympus Keymed Ltd., UK) (Fig. 3) [17].he endoclip with magnet would then be deployed onto the SCJsing a clip fixing device via a standard 27F endoscope (Pentax Ltd.,
K).& Physics 34 (2012) 279– 289 281
3. Benchtop studies
3.1. Method
The system was assessed by measuring the signal strength withthe magnet at different distances from the probe as well as in differ-ent positions and magnetic field orientation relative to the probe.The ability to accurately measure the location of the magnet alongthe length of the probe was also assessed with the magnet at differ-ent distances, positions and orientations relative to the probe. Thefollowing parameters were measured during benchtop studies:
Position error: The position error is the difference between theactual position and that displayed by probe of the magnet along thelength of the probe.
Signal strength: The displayed signal strength represents thehighest output from any one of the individual Hall Effect sensor.Signal strength lower than approximately 10 mV can be attributedto electromagnetic noise and with such low signal strength thedisplayed position may not be valid. When signal strength isunrecordable as a result of magnet absence the locator recordingwill default to a sensor or location with the highest baseline volt-age or signal strength value. The highest signal output is 1200 mVas the sensors are saturated at this level.
3.2. Results: signal strength
With the magnet maintained at a constant length along theprobe and with its north–south pole always pointing directlytoward the probe, the signal strength was monitored as it wasrotated around the probe at a distance of 5 mm and 10 mm fromthe probe. This rotation is termed rotation A and shown in Fig. 4(rotation A). Maximal signal strength was obtained when the mag-net was anterior to the probe, a reduced signal strength posteriorlyand least strength when positioned lateral to the probe.
With the magnet maintained at a constant length along theprobe and kept directly anterior to the probe, the magnet wasrotated so that its north–south pole is kept in a plane perpen-dicular to the length of the probe. This rotation is referred to asrotation B and shown in Fig. 4 (rotation B). This manoeuvre wasperformed with the magnet at 5 mm and 10 mm distance fromthe probe. Signal strength was greatest when the magnetic fieldpointed directly toward or away from the probe and least whenwas midway between those two orientations.
With the magnet maintained at a constant length along theprobe and kept directly anterior to the probe, the magnet wasrotated to a plane parallel to the length of the probe. This is referredto as rotation C and is shown in Fig. 4 (rotation C). The manoeuvrewas again performed at 5 mm and 10 mm distance from the probe.This rotation produced only very small variation in magnet strengthwith strength being least when north–south pole axis was parallelto the length of the probe.
The magnet was initially placed anterior to the probe and withits north–south axis perpendicular to an imaginary line from thecentre of the Hall sensor to the centre of the magnet. The magnetwas then rotated around the probe while maintaining the samemagnetic field orientation relative to the probe (Fig. 4, rotation D).This rotation produced the least signal strength across all degreesof orientation and the strength being least when the magnet wasat either side of the probe.
When the signal strength was analysed with respect to distancefrom 5 mm to 15 mm in various degrees of orientations for rota-tions A, B and C (Fig. 5), there was an exponential decay of signal
signal strength for all different degrees of orientations was seen in

282 Y.Y. Lee et al. / Medical Engineering & Physics 34 (2012) 279– 289
F otatiot ion ong
rlpis
<o(
3
lbTbpo
idtsrs
v≤02s
t00−
ig. 4. Relationship between signal strength (mV) against various orientations in rhe page. The manoeuvres performed in rotations A, B, C and D are described in sectraph axis are indicative of magnet placement posterior to the probe.
otation C. The strength variation across all orientations was theeast with rotation D. With posterior placement of magnet to therobe, all rotations A, B, C and D showed a greater degree of decay
n strength compared to anterior placement with a lesser degreeeen in rotation C.
The benchtop studies indicated that a poor signal strength of10 mV occurred only during 17.8% of all orientations and positionsf the magnet within 10 mm distance of the Hall Effect sensor probeTable 2).
.3. Results: position accuracy
With the probe stationary, the magnet was moved along theength of the probe at 1 mm increments and the distance recordedy the probe compared with the actual position along the probe.his was performed at 0 mm, 5 mm, 10 mm and 15 mm distanceetween the magnet and probe and with the magnet in differentositions and orientations with respect to the probe as describedn the above section on signal strength (Table 1).
The magnet was first of all moved along the length of the proben the varying angles of rotation described as rotation A above. Atistance ≤10 mm an accuracy of 0–3.4 mm was found for all rota-ions studied except for 0◦ at 10 mm distance when studied signaltrength was inadequate. At 15 mm an accuracy of 1.2–6 mm wasecorded for all rotations except 0◦, +20◦ and −20◦ when againignal strength was inadequate.
The magnet was then moved along the length of the probe in thearying angles of rotation described as rotation B above. At distance10 mm an accuracy of 0.8–3 mm was found for all rotations except◦ when signal strength was inadequate. At 15 mm the error was.1–5.8 mm for all rotations except 0◦, +20◦ and −20◦ when signaltrength was inadequate.
The magnet was moved along the probe at different rota-
ions described as rotation C. At distance ≤10 mm the error was.6–7.7 mm. At 15 mm distance the error was 1.2–12.5 mm for–160◦ and −90◦. For 180◦, −160◦, −140◦, −120◦, −60◦, −40◦, −20◦,0◦ the signal strength was inadequate.ns A, B, C and D. In rotations A, B and D the length of the probe is perpendicular to benchtop studies. For rotations A, B and D, orientations from −20◦ to −100◦ on the
Finally, the magnet was moved along the probe at different rota-tions described as rotation D. At distance ≤10 mm the error was0.8–7.1 mm. At 15 mm distance the error was 7.9 mm for +90◦ withthe rest of rotations having inadequate signal strength.
Including all the possible orientations of the magnet at or nearerthan 10 mm from the probe, the median accuracy of distancealong the length of probe was 2.43 mm (inter-quartile range (IQR)2.11 mm). The proportion of all possible orientations within 10 mmof the probe giving an accuracy of ±10 mm was 88.9% (Table 2).
3.4. Effects of temperature on the locator probe system
In order to appreciate the error induced as a result of change intemperature on the Hall Effect sensors, drift over time at constanttemperature must first be investigated. To test time drift, the probewas placed in the incubator (Stuart Scientific SI 60, UK) for 1 h at afixed temperature (at 18 ◦C and 33 ◦C) with the magnet and probestationary. The experiment was then repeated with the incubatorinitially at 18 ◦C and then increasing the temperature to 40 ◦C. Thesetemperature and time drift experiments were performed after cal-ibrated at 37 ◦C versus calibrating at room temperature.
There was no change noticeable in signal strength or positionover time for up to a period of one hour at 17 ◦C or 33 ◦C. Therewas significant change in signal strength (36.0%) but not posi-tion recording when the temperature was increased from 20 ◦C to40 ◦C and the change appears to be dependant on the initial signalstrength, where initially high signal strengths decrease and initiallylow signal strengths increase. The probe calibrated at 37 ◦C showedno drift when heated to body temperature. However, the probe cali-brated at room temperature showed a significant decrease in signalstrength (49.2%) when heated to body temperature.
3.5. Electromagnetic interference between locator probe and pH
probe and manometerExperimental tests were run to check for interference betweenthe locator probe and a 4.2 mm diameter solid state high resolution

Y.Y. Lee
et al.
/ M
edical Engineering
& Physics
34 (2012) 279– 289283
Table 1Effects of rotation and proximity on locator probe position error and standard deviation.
Rotation (◦) Rotation A Rotation B Rotation C Rotation D
5 mm 10 mm 15 mm 5 mm 10 mm 15 mm 5 mm 10 mm 15 mm 5 mm 10 mm 15 mm
Error SD Error SD Error SD Error SD Error SD Error SD Error SD Error SD Error SD Error SD Error SD Error SD
0 2.89 3.27 – – – – 1.41 1.65 – – – – 2.31 2.26 7.15 1.22 7.93 1.59 0.94 1.08 – – – –20 2.43 2.71 1.47 1.85 – – 0.61 0.83 1.11 1.42 – – 4.44 1.58 7.58 1 2.58 0.85 1.30 1.37 – – – –40 1.39 1.34 1.30 0.86 1.18 1.45 1.01 0.82 1.45 1.08 5.45 5.77 4.88 1.27 6.56 0.84 6.33 7.72 1.03 1.12 – – – –60 3.40 1.32 1.52 0.76 2.25 1.35 0.9 0.96 1.04 0.62 3.64 2.42 4.15 0.98 5.67 0.66 6.79 1.21 0.84 0.97 – – – –90 2.26 0.75 2.88 0.62 2.70 2.12 2.26 0.75 2.88 0.62 2.70 2.12 2.26 0.75 2.88 0.62 2.70 2.12 2.31 2.26 7.15 1.22 7.93 1.59
120 – – – – – – – – – – – – 2.43 1.04 2.03 1.03 12.45 3.89 – – – – – –140 – – – – – – – – – – – – 2.42 1.27 1.30 1.02 10.88 2.71 – – – – – –160 – – – – – – – – – – – – 2.89 1.43 1.17 1.29 10.14 5.92 – – – – – –180 – – – – – – – – – – – – 2.22 2.70 7.65 1.02 15.86 6.05 – – – – – –
−180 – – – – – – – – – – – – 3.42 3.78 5.29 5.32 – –−160 – – – – – – – – – – – – 1.75 1.38 2.48 0.92 – – – – – – – –−140 – – – – – – – – – – – – 0.95 1.13 0.73 0.8 – – – – – – – –−120 – – – – – – – – – – – – 2.44 1.19 0.53 0.64 – – – – – – – –−90 3.14 1.41 2.04 1.51 3.06 3.72 3.14 1.41 2.04 1.51 3.06 3.72 3.14 1.41 2.04 1.51 3.06 3.72 3.70 2.12 5.28 1.20 – –−60 2.62 1.11 2.53 0.79 3.61 4.54 2.11 1.29 3.09 1.74 3.64 2.42 4.23 0.80 4.62 1.12 – – 3.00 4.01 – – – –−40 2.67 1.35 2.55 0.81 5.30 5.98 1.32 1.04 2.67 1.26 5.45 5.77 3.61 0.93 4.44 0.91 – – 2.90 3.58 – – – –−20 1.75 1.19 1.38 0.84 – – 1.68 0.78 2.21 1.07 – – 3.70 1.77 7.68 0.97 – – – – – – – –−0 2.89 3.27 – – – – 1.41 1.65 – – – – 3.70 2.12 5.28 1.20 – – 0.94 1.08 – – – –
Error denotes the mean of difference for 210 experiments between actual position and the probe recorded position in mm, SD; standard deviation denotes the spread of error in mm, “–”denotes the absence of data due to inabilityof the system to detect any position in that particular rotation as a result of poor magnetic field strength or in the case of rotations A, B and D, the movement from 0 to 90◦ is symmetrical to 90–180◦ , and so is not included. Degreesbetween −180 and −0 are indicative of posterior placement of magnet relative to the probe for rotation C but for rotations A, B and D the degrees 0 and −0 are the same.

284 Y.Y. Lee et al. / Medical Engineering & Physics 34 (2012) 279– 289
Fig. 5. Relationship between signal strength (mV) against distances at 5, 10 and 15 mm in rotations A, B, C and D. In rotations A, B and D the length of the probe is perpendicularto the page. For each rotations A, B, C and D, figures for magnet placement anterior to the probe are shown on the left and figures for magnet placement posterior to theprobe are shown on the right. For rotations A and B, results for 0◦ are not present due to unrecordable signal strength. For rotation D, only result for 90◦ is available sinceother orientations do not have adequate signal strength after 5 mm distance.

Y.Y. Lee et al. / Medical Engineering
Table 2Analyses on orientations with poor signal strength <10 mV and orientations witherror <10 mm for experiments of ≤10 mm between the magnet and the probe.
Orientations Total studiedorientations
Orientations withsignificantly poor signalstrength <10 mV
Orientations witherror <10 mm
Rotation A 18 4 17Rotation B 18 4 17Rotation C 36 0 36Rotation D 18 8 10
mmcass
“tapawlaitoriappftap
msptpwpwmmtimC
4
4
Orn4a
Total 90 16 80
Percentage 100 17.8 88.9
anometry probe (Given Imaging, USA) and between locator andultiple antimony pH sensor probe (Synectics Medical, UK). The
ombined probes were placed in a water bath heated to 37 ◦C and magnet was placed at a fixed position on the locator probe at lowignal strength since any effects in locator’s output would have beenignificant as signal strength is indicative of magnet’s presence.
Tests were conducted with manometer and pH probe in a turnon” and turn “off” mode. In addition, tests were conducted withhe manometer being exposed to a known hydrostatic pressurend pH probe being exposed to abrupt change in pH (from pH 7 toH 1 and vice versa) by addition of appropriate molars of alkali orcid. Finally, tests were conducted on the manometer to determinehether the metallic components within the sensor interfere with
ocator’s output (Fig. 6). In experiment A, both 4.2 mm diameternd 2.7 mm diameter manometer (slim-line model, Given Imag-ng, USA) were initially tested when placed anterior relative tohe locator probe. A magnet was used to move to-and-fro alongne sensor containing the manometer’s metallic part and this wasepeated for the non-metallic portion without any sensor. In exper-ment B, experiment A was repeated but with the 4.2 mm diameternd 2.7 mm diameter manometers placed posterior to the locatorrobe. Lastly for experiment C, the 4.2 mm diameter manometerrobe was compared with the 2.7 mm diameter manometer probeor their difference in accuracy. Both probes were placed anterior tohe locator probe during each experiment. A magnet then movedlong the probes over a distance of 50 mm. Recordings from theolygraph machine were then analysed for all of the above tests.
The position output of the locator did not change whether theanometer or the pH probe in a turn “on” or turn “off” mode
uggesting that there was no electrical interference between therobes. Similarly, the position output remained the same whetherhe manometer was exposed to a pressure over time or the pHrobe was exposed to an abrupt change in pH. However, thereas a loss of accuracy when the 4.2 mm diameter manometer waslaced anterior to the locator probe especially when the magnetas placed overlying the metallic part of the manometer (experi-ent A, Fig. 6). The opposite effect on accuracy occurred when theanometer was placed posteriorly (experiment B, Fig. 6). Finally
he smaller 2.7 mm diameter manometer, having less metal ints sensors produced a better accuracy than the 4.2 mm diameter
anometer probe when their tracings were compared (experiment, Fig. 6).
. In vivo validation study
.1. Methods
Ten volunteers participated in the in vivo validation studies.f these, eight subjects successfully completed the study. The
emaining two subjects were excluded due to absence of mag-et during fluoroscopy. The median age of the eight subjects were1.5 years (range 26–58 years old) where five subjects were malesnd three subjects were females. Two males reported symptoms of
& Physics 34 (2012) 279– 289 285
gastro-oesophageal reflux and one of them had evidence of refluxoesophagitis on endoscopy. Two females had evidence of hiatushernia during upper endoscopy but did not report any symptomsof reflux.
Subjects attended fasted following overnight fast and had themagnet attached endoscopically to the SCJ. The locator probe wascalibrated at room temperature before being passed down throughthe nostril. However in three subjects the locator probe was cali-brated in warm water bath at body temperature of 37◦C. This wasperformed in three subjects after we noticed the effect of body tem-perature had on signal strength when the probe was calibrated inroom temperature.
The probe was passed per nasally until signals were seen on thecomputer display confirming detection of the magnet. Screeningfluoroscopy was then performed at this stage to adjust the locatorprobe until desirable depth and position for subsequent screenings.The setting for fluoroscopy machine was adjusted for correct dosingand was fixed for continuous screening at 5 frames per seconds (PVPulsera, Philips, UK).
The volunteers then rested for 10–15 min. Subsequently, theywere asked to perform a series of manoeuvres which were recordedsimultaneously with fluoroscopy screenings which lasted between15 and 20 s per series of manoeuvre. The manoeuvres performedincluded normal respiration, deep inhalation and full expiration,water swallowing and lastly advancing the probe as far possiblefollowed by its full withdrawal. Each manoeuvre was performedat least twice. Total fluoroscopy screening lasted approximately60–80 s for each volunteer. Markers were placed at the start and theend of each event on both the PolygramNET and the fluoroscopy.The markers were checked to ensure time synchronization betweenthe two equipments. All images taken were then transferred andstored using Picture Archiving and Communications System (PACS).The images can be analysed using measuring tools built in the PACSsoftware. Recordings from the locator probe were then extractedfrom the PolygramNETTM software as described above and subse-quently exported into Microsoft Excel 2007 and SPSS version 18.0(SPSS Inc., IL, Chicago) for analysis. Each volunteer had a chest X-rayperformed 6–8 weeks after the study to ensure that the clip and ormagnet had dislodged.
The research was approved by West Glasgow Research EthicsCommittee and all subjects gave informed consent.
4.2. Data and statistical analysis
Data analyses were divided according to the four manoeuvresor “events” as described above. The fluoroscopy clip position data(which is regarded as the “standard”) extracted from PACS werecorrelated and compared with the locator position data. The changein amplitude during each event was determined from both setsof data. Change in amplitude denotes a change from the baseline(selected from an average of 2 s of data prior to the actual event) tothe peak of studied event. Wilcoxon matched pair ranks sum testwas used to test if there is a difference between the locator and thefluoroscopy amplitude change during the studied event where nullhypothesis is the median of differences between the two variablesequals zero. Null hypothesis is retained if the P value >0.05. Lin-ear regression analysis and Pearson correlation co-efficient wereused to correlate the events’ position data-points at 1 s intervalfrom both the locator probe and the fluoroscopy. A correlation co-efficient >0.80 and adjusted residual squared (R2) >80% suggesta good correlation between the two parameters. Signal strength
of locator position recording was expressed as median of averagesignal strength for each event, maximum value, minimum valueand the percentage of signal strength above 10 mV during eachevent.
286 Y.Y. Lee et al. / Medical Engineering & Physics 34 (2012) 279– 289
Fig. 6. Experiments on magnetic interference between the metallic sensors of solid-state manometer (Given imaging, USA) and the locator probe as recorded by the Polygraphmachine. In experiment A, the 4.2 mm diameter and 2.7 mm diameter manometers are placed anterior to the locator probe. A magnet is moving to-and-fro along one metallicsensor of the manometer probes as indicated by the black arrow and the test is repeated with the non-metallic portion of the manometer probes as indicated by the whitearrow for comparison. In experiment B, the 4.2 mm diameter and 2.7 mm diameter manometers are placed posterior to the locator probe. Similar to experiment A, the magnetis moving to-and-fro along the metallic and non-metallic portion of the manometer probes. As noted in these experiments, there was a loss of accuracy when the 4.2 mmdiameter manometer was placed anterior to the locator probe especially when the magnet was moving along the metallic portion of the manometer probe. This loss inaccuracy was less with the 2.7 mm diameter manometer. In experiment C, the recordings for 4.2 mm diameter manometer was compared to the smaller 2.7 mm diametermanometer. Both the manometer probe was placed anterior to the locator probe. A magnet then moves along the probes during each experiment over a distance of 50 mm.A compc e in sc
2
4
nsRt2awatl
rfipi(1
ANm
5
pdswqt
m
s shown in this experiment, the 2.7 mm diameter manometer has a better accuracyontent in the smaller sensors for the 2.7 mm diameter manometer. Note differenc
All statistical analyses were carried out using Microsoft Excel007 and SPSS version 18.0 (SPSS Inc., IL, Chicago).
.3. Results
There were a total of 31 analysable events of which six fromormal respiration, ten from deep respiration, seven from waterwallows and six from insertion and withdrawal of locator probe.epresentative traces of the locator probe and fluoroscopic posi-ions of each of these events are shown in Fig. 7. Overall a total of25 data-points at 1 s interval for both locator and fluoroscopy werecquired from these events. The overall correlation co-efficientas 0.96 (P < 0.001; 95% confidence interval (CI) 0.89–0.96) and
djusted R2 was 0.91. The median amplitude of fluoroscopic posi-ions for each of the events was similar to median amplitude ofocator probe positions (Table 3).
When the signal strength was analysed for the entire locatorecording for all volunteers from the beginning when the proberst detected the magnet upon insertion to the end when therobe last detected the magnet upon withdrawal (median record-
ng time of 1045.44 s) there was a median proportion of 96.82%range 87.05–99.29) of data points where signal strength was above0 mV (Table 4).
So far all volunteers turned up for chest X-ray after 6–8 weeks.ll but one volunteer were documented cleared from the magnet.one of the volunteers reported any side effects from having theagnet in the gut.
. Discussion
The current studies indicate that it is possible to monitor theosition of the SCJ by means of clipping a magnet to it and which isetected by a linear probe consisting of a series of Hall Effect sen-ors. This technique allows the location of the SCJ for the first timeithout fluoroscopy and the associated radiation exposure. Conse-
uently, the technique can be applied over much longer periods ofime than has been previously possible.
The system was initially assessed by benchtop studies. Threeain factors influenced the signal strength and the ability to
ared to the 4.2 mm diameter manometer and this is presumably due a less metallicales for all three figures.
accurately localise the position of the magnet along the length ofthe probe, namely distance between the magnet and Hall Effect sen-sor probe, the orientation of the magnetic field relative to the HallEffect sensors and whether the magnet was positioned anterior,posterior or lateral to the Hall Effect sensors. The human oesoph-agus normally has a small diameter which is unlikely to be morethan a few millimetres except when it dilates temporarily duringswallowing of food boluses. We found that when the magnet waswithin 10 mm distance of the probe that the system could detect itsposition along the length of the probe with an accuracy of within±10 mm over 88.9% of the full range of possible orientations andpositions relative to the probe. Including all the possible orienta-tions of the magnet at or nearer than 10 mm from the probe, themedian accuracy of position detection along the length of probewas 2.43 mm (IQR 2.11 mm).
The system constantly displays the signal strength as well asposition so that positions obtained during periods of low signalstrength are interpreted with caution. When the signal strengtharising from detection of the magnet becomes very low, the systemwill display the highest output from the Hall Effect sensor with thehighest background output. The location reported by the systemonly changes to another location when the signal strength fromanother Hall Effect sensor becomes higher than the one currentlyrecording. Similarly positions obtained during signal strength sat-uration should be interpreted with caution. Saturation only occurswhen the magnet is less than 2 mm from the probe. However, withtubing and coating of the probe with secretion, signal saturationdoes not pose a problem. This was supported from data of in vivostudy where signal strength saturation never occurs.
Information regarding the location of the SCJ will be highly valu-able in interpreting information obtained from pH and pressuresensors positioned in the gastro-oesophageal lumen. We thereforedetermine whether there was any interference from multiple pHsensors or solid state high resolution manometry probes. We didnot test perfusion manometry as they have no metallic content or
electrical activity. There was no noticeable interference betweenthe Hall Effect sensor probe and solid state pH probes. There wassome interference between the large diameter (4.2 mm) highresolution manometry probe. When the magnet was positioned
ering
wbTtt(mac
pflbicctt8
trpuestnott
teowd
Ffltfi
Y.Y. Lee et al. / Medical Engine
ith one of the 1 cm long metal segments of the manometer probeetween it and the Hall Effect sensors, the accuracy was reduced.his did not occur when the manometer was on the other side ofhe Hall Effect sensors from the magnet and indeed this tendedo enhance the signal strength and accuracy. When the slim-line2.7 mm) high resolution manometer probe was used there was
uch less interference with the accuracy of the locator probend this can be explained by its presumably much reduced metalontent.
We proceeded to assess the validity of the probe in vivo com-aring it with the position recorded by simultaneous gold standarduoroscopy. This was done during various manoeuvres includingreathing, swallowing and advancing and withdrawing the probe
n order to vary the location of the magnet relative to the probe. Theorrelation co-efficient was 0.96 (0.001) and the median amplitudehange for each of the manoeuvres was similar when recorded byhe probe or fluoroscopy. The proportion of total recording timehat the signal strength was more than 10 mV was 96.82% (range7.05–99.29%).
Taking the benchtop and in vivo studies together indicates thathe probe is able to detect the position of the SCJ to an accu-acy superior to 10 mm for the great majority of the recordingeriod. However, the accuracy is likely to be reduced slightly ifsed alongside a large diameter solid state high resolution manom-try system and we would therefore recommend employing thelim-line manometer. It is also much more comfortable to passhe slim-line manometer along with the pH and locator probe perasally than to pass the wide manometer along with these twother probes. It is important to pass the equipment nasally in orderhat the effect of meals can be studied. It is difficult to consume aest meal with three probes per orally.
There were other challenges when using this new techniqueo monitor the location of SCJ. Firstly, not all subjects can toleratendoscopy and there are certain risks related to the procedure. Sec-
ndly, training and experience are needed to deploy the endoclipith magnet onto the SCJ with an endoscope. The ideal position foreployment onto the SCJ was found to be between 2 and 6 o’clockig. 7. Graphs showing four studied manoeuvres from four different volunteers. All grapuoroscopy clip position data (red dots) and a bottom line graph for the signal strengthherefore the location will default to a sensor with a higher baseline voltage (example asgure legend, the reader is referred to the web version of the article.)
& Physics 34 (2012) 279– 289 287
when looking at the circular SCJ face-on. Thirdly, after deploy-ment, ideally studies with the Hall Effect locator probe shouldbe performed within the next 48–72 h since we noticed the cliptend to fall away after 72 h in many of our subjects. Finally, thesize of probe (outer diameter of 4.2 mm) can be passed throughthe nostril for most people but we did have 2 subjects where weattempted to pass the probe through oral route. However oral routewas uncomfortable and the position of probe was difficult to main-tain.
The main disadvantage of this novel technique was the poor ori-entation and distance of magnet in relation to the probe can affectthe signal strength and accuracy of location monitoring. Safety is acritical issue with any in vivo device. The electronics are ISO certi-fied. The magnet needs special consideration. Clipping the magnetto the mucosa is usually straightforward but we would not recom-mend clipping two magnets or clipping a further magnet if one failsto attach. This is to avoid the potential of two magnets being freewithin the lumen of the intestines and the consequent risk of themattaching to each other between two loops of bowel. This couldpotentially cause intestinal torsion or localised ischaemic necro-sis of the bowel wall. It is observed from our volunteers that themagnet with clip attached usually spontaneously detaches within6 weeks. When the clips without a magnet attached are used inroutine clinical practice, it is not customary to check whetherthey have spontaneously detached and passed in the stool. It isuncertain whether this should be done with the clip with magnetattached. The manufacturer advises not to perform MRI procedureson patients who have clips placed within their gastrointestinal tractas this can be harmful without further details. We routinely advisepatients that if they subsequently have an MRI scan that they shouldinform the operator that a clip with magnet attached was fixed totheir gastro-oesophageal junction.
In conclusion, the Hall Effect sensor probe provides for the firsttime a method of constantly monitoring the location of the SCJ and
due to the absence of associated radiation exposure this can bedone over a prolonged period of time. The accuracy of the system isequivalent to that obtained by fluoroscopy and likely to be superiorhs have two scatter-plots for the position data of locator probe (blue dots) and the (black). The low signal strength below 10 mV will result in a loss of position and
shown as with a black arrow). (For interpretation of the references to color in this

288 Y.Y. Lee et al. / Medical Engineering & Physics 34 (2012) 279– 289
Tab
le
3C
omp
aris
on
and
corr
elat
ion
of
dat
a
from
loca
tor
pro
be
and
flu
oros
cop
y
scre
enin
gs.
Even
ts
(N;
n)M
edia
nfl
uor
osco
py
amp
litu
de
chan
ge(m
m)
Med
ian
loca
tor
amp
litu
de
chan
ge(m
m)
Wil
coxo
n
mat
ched
pai
r
sign
ed
ran
kte
st
(P
valu
e)
Cor
rela
tion
co-e
ffici
ent
(95%
CI)
Ad
just
ed
R2
Sign
al
stre
ngt
h(m
axim
um
, min
imu
m)
(mV
)
Sign
al
stre
ngt
hab
ove
10
mV
(%)
Nor
mal
brea
thin
g
(N
=
6,
n
=
24)
5.50
5.17
0.92
0.94
(0.9
3–1.
28)
0.88
193.
84
(79.
51, 3
37.3
3)10
0D
eep
brea
thin
g
(N
=
10, n
=
66)
12.2
5
12.0
1
0.17
0.95
(0.9
1–1.
07)
0.90
129.
87
(30.
05, 3
04.2
3)10
0W
ater
swal
low
(N
=
7,
n
=
55)
25.0
0
26.2
3
0.61
0.92
(0.5
8–0.
94)
0.84
166.
83
(12.
01, 4
36.3
8)
100
Inse
rtio
n
and
wit
hd
raw
al
(N
=
6,
n
=
80)
92.8
0
85.5
9
0.92
0.95
(0.8
2–0.
96)
0.90
99.8
4 (0
.80,
297.
03)
89.5
7
N, n
um
ber
of
even
ts;
n,
nu
mbe
r
of
dat
a
poi
nts
per
1
s
inte
rval
;
CI,
con
fid
ence
inte
rval
;
R2, r
esid
ual
squ
ared
;
mm
, mil
lim
etre
s;
mV
, mil
livo
lts;
sign
al
stre
ngt
h, m
edia
n, m
axim
um
and
min
imu
m
ran
ge
of
aver
age
sign
al
stre
ngt
hd
uri
ng
stu
die
d
even
ts
(mV
).
Table 4Analysis of signal strength reliability during total recording time for each volunteer.
Volunteer Time (s) with signalstrength <10 mV
Total recordingtime (s)
% Time with signalstrength >10 mV
1 25.5 353.5 92.792 12.75 1180.87 98.923 19.75 1229.87 98.394 79.25 611.75 87.055 63.62 703.12 90.956 6.50 910 99.297 73.25 1540.5 95.258 21.12 1322.75 98.40
Median 23.31 1045.44 96.82
Total recording time = range of recording time of in vivo study starting from the timewhen the probe first detected the magnet as it was inserted into the volunteer untilthe time when the probe last detected the magnet when it was withdrawn from the
[
[
[
volunteer.
to the performance of currently obtained by available high resolu-tion manometry or high resolution pH whose sensors are mounted10 mm apart.
Funding
None.
Acknowledgements
We would like to thank all volunteers who have participatedin the study. We expressed our appreciation to all staffs fromEndoscopy Unit and Radiology Department of Gartnavel GeneralHospital, Glasgow, United Kingdom for providing their supportsand generous assistance during the study.
Conflict of interest statement
All authors declared no conflict of interest that could influencethe current study.
References
[1] Nebel O, Fornes M, Castell DO. Symptomatic gastro-oesophageal reflux inci-dence and precipitating factors. Dig Dis Sci 1976;21:953–6.
[2] Oberg S, Peters JH, DeMeester TR, Chandrasoma P, Hagen JA, Ireland AP,et al. Inflammation and specialized intestinal metaplasia of cardiac mucosais a manifestation of gastroesophageal reflux disease. Ann Surg 1997;225(4):522–30.
[3] Lagergren J, Bergstrom R, Lindgren A, Nyren O. Symptomatic gastroe-sophageal reflux as a risk factor for esophageal adenocarcinoma. N Eng J Med1990;340(11):825–31.
[4] Gawron AJ, Hirano I. Advances in diagnostic testing for gastroesophageal refluxdisease. World J Gastroenterol 2010;16(30):3750–6.
[5] Ravi K, Francis DL. New technologies to evaluate esophageal function. ExpertRev Med Devices 2007;4(6):829–37.
[6] Sifrim D, Blondeau K. New techniques to evaluate esophageal function. Dig Dis2006;24(3–4):243–51.
[7] Ayazi S, Crookes PF. High resolution esophageal manometry: using technicaladvances for clinical advantages. J Gastrointest Surg 2010;14(Suppl. 1):S24–32.
[8] Kahrilas PJ, Sifrim D. High resolution manometry and impedance-pH/manometry: valuable tools in clinical and investigational esophagology.Gastroenterology 2008;135(3):756–69.
[9] Fletcher J, Wirz A, Henry E, McColl KEL. Studies of acid exposure immediatelyabove the oesophageal squamocolumnar junction: evidence of short segmentreflux. Gut 2004;53:168–73.
10] Pandolfino JE, Zhang QG, Ghosh SK, Han A, Boniquit C, Kahrilas PJ. Tran-sient lower esophageal sphincter relaxations and reflux: mechanistic analysisusing concurrent fluoroscopy and high resolution manometry. Gastroenterol-
ogy 2006;131:1725–33.11] Pepka G. Position and level sensing using Hall-effect sensing technology. SensorRev 2007;27(1):29–34.
12] Ramsden E. Hall-Effect sensors: theory and application, vol. 7. Burlington: New-ness; 2006. pp. 2–73.

ering
[
[
[
[nets in orthodontics and biological implications: a review. Eur J Orthod
Y.Y. Lee et al. / Medical Engine
13] AlteSilTM High strength silicone tubing [Online]. AltecWeb.com Ltd. UK.http://www.altecweb.com/home.asp?cat=category1201 [July 2010].
14] An Introduction to Samarium Cobalt (SmCo) Disc Magnets [Online]. E-magnets UK. http://emagnetsuk.com/magnets/samarium cobalt/smco discmagnets.aspx [July 2009].
15] Noar JH, Evans RD. Rare earth magnets in orthodontics: an overview. Br J Orthod1999;26(1):29–37.
[
& Physics 34 (2012) 279– 289 289
16] Darendeliler MA, Darendeliler A, Mandurino M. Clinical application of mag-
1997;19(4):431–42.17] Heat shrink tubing: PLK175 [Online]. PMG Plastronic Ltd. UK. http://www.
pmgcompany.co.uk/Products/HeatShrinkTubing/tabid/61/ArticleId/19/PLK175-19.aspx [July 2009].