
Design of biodegradable esophageal stents Mathias Peirlinck · 2013-09-19 · Design of...
106
Design of biodegradable esophageal stents Mathias Peirlinck Promotoren: prof. dr. ir. Benedict Verhegghe, prof. dr. Peter Dubruel Begeleiders: ir. Nic Debusschere, dr. Matthieu De Beule Masterproef ingediend tot het behalen van de academische graad van Master of Science in Biomedical Engineering Vakgroep Civiele Techniek Voorzitter: prof. dr. ir. Peter Troch Vakgroep Organische Chemie Voorzitter: prof. dr. José Martins Faculteit Ingenieurswetenschappen en Architectuur Academiejaar 2012-2013
Transcript of Design of biodegradable esophageal stents Mathias Peirlinck · 2013-09-19 · Design of...

Design of biodegradable esophageal stents
Mathias Peirlinck
Promotoren: prof. dr. ir. Benedict Verhegghe, prof. dr. Peter Dubruel
Begeleiders: ir. Nic Debusschere, dr. Matthieu De Beule
Masterproef ingediend tot het behalen van de academische graad van
Master of Science in Biomedical Engineering
Vakgroep Civiele Techniek
Voorzitter: prof. dr. ir. Peter Troch
Vakgroep Organische Chemie
Voorzitter: prof. dr. José Martins
Faculteit Ingenieurswetenschappen en Architectuur
Academiejaar 2012-2013


Design of biodegradable esophageal stents
Mathias Peirlinck
Promotoren: prof. dr. ir. Benedict Verhegghe, prof. dr. Peter Dubruel
Begeleiders: ir. Nic Debusschere, dr. Matthieu De Beule
Masterproef ingediend tot het behalen van de academische graad van
Master of Science in Biomedical Engineering
Vakgroep Civiele Techniek
Voorzitter: prof. dr. ir. Peter Troch
Vakgroep Organische Chemie
Voorzitter: prof. dr. José Martins
Faculteit Ingenieurswetenschappen en Architectuur
Academiejaar 2012-201

Preface
This master dissertation forms the final chapter of my education in becoming a Biomedical Engineer. It has been a
challenging 5 years with ups and downs, but I’m proud of what I have accomplished. The Master of Science in
Biomedical Engineering intrigued me with fields like biomechanics, implants, regenerative medicine, biomedical
devices, sensors and circuits. I chose this subject because the research area Nic Debusschere is currently working in
seemed very interesting to me and I wanted to contribute.
In this thesis, esophageal stenting is explored and the niche which bioresorbable stents can occupy within this field is
postulated. As complaints or disappointments have risen on the insufficient radial force of contemporary
biodegradable esophageal stents, there is still a lot of improvement to be made. For that reason, the stent’s chemical
degradation is studied and a numerical framework of a (bioresorbable) polymeric braided wire stent is developed.
This model can boost the development of an improved (bioresorbable) stent design, that can be trusted by both
patient and doctor. The word ‘bioresorbable’ is put between brackets because the numerical framework will be
extendable to all kinds of polymeric braided wire stents.
This master dissertation wasn’t an individual merit, so first of all, to Nic and Matthieu De Beule: a big ‘thank you’ for
all your guidance during this research. Your help and support guided me towards this final result. I like to thank
Sandra Van Vlierberghe and Veerle Boterberg for their help in conducting a number of chemical analyses on both the
non-degraded and degraded stent. I also want to thank Sander De Bock for helping me with my models in Abaqus
(Dassault Systèmes, Providence USA). The geometrical modeling done in this thesis is founded on pyFormex and the
BuMPer cluster allowed me to run extensive jobs in Abaqus. Without these tools, I wouldn’t have succeeded in
developing a correct numerical framework, so I’m very grateful to prof Benedict Verhegghe for their development. I
also like to thank prof. Dubruel and prof. Segers for their support and guidance. I am also thankful to Alexander
Stamme from Ethicon for providing me the PDS sutures for comparison with the Ella BD stent. I also like to express
my gratitude to professor Giani Dorta at the CHUV (university hospital) in Lausanne, where I went on Erasmus
exchange, for taking some time out of his busy schedule to discuss the application of biodegradable stents in the
esophagus with me. He pointed out why he was not convinced by the Ella BD stent, which motivated me to
contribute to the development of a better design that could really put bioresorbable stents on the map of esophageal
stenting.
Last but not least and on a very personal note, ‘thank you Dad’. You made me who I am by your constant believe,
trust and pride in me and my sister. Your years of fighting to live and to be able to stand next to me on my
graduation day made you my personal hero. And although it won’t be possible to share that moment of my
graduation physically anymore, I know you’re watching over me, with pride in your eyes.
This thesis can be seen as a concrete application and extension of the research done by Matthieu De Beule and Nic
Debusschere. Hopefully, the developed numerical model can really form a contribution in the development of better
biodegradable esophageal stents. As in my opinion the model can be generalized to all kinds of biodegradable
polymeric braided wire stents, I sincerely hope it can also serve beyond esophageal stenting.
Mathias Peirlinck
Gent, June 3 - 2013

ii
The author and promoter give the permission to make this master dissertation available for consultation
and to copy parts of this master dissertation for personal use. In the case of any other use, the limitations of
the copyright have to be respected, in particular with regard to the obligation to state expressly the source
when quoting results from this master dissertation
Gent, June 2013
The promotors The supervisors The author
Prof. dr. ir. Benedict Verhegghe Dr. ir. Matthieu De Beule Mathias Peirlinck
Prof. dr. Peter Dubruel ir. Nic Debusschere

Design of biodegradable
esophageal stents By
Mathias PEIRLINCK
Masterproef ingediend tot het behalen van de academische graad van
MASTER OF SCIENCE IN BIOMEDICAL ENGINEERING
Academiejaar 2012-2013
Promotoren: prof. dr. ir. Benedict VERHEGGHE, prof. dr. Peter DUBRUEL
Begeleiders: ir. Nic DEBUSSCHERE, dr. Matthieu DE BEULE
Vakgroep Civiele Techniek
Voorzitter: prof. dr. ir. Peter TROCH
Vakgroep Organische Chemie
Voorzitter: prof. dr. José MARTINS
Faculteit Ingenieurswetenschappen en Architectuur
Universiteit Gent
Summary
In this dissertation, a numerical framework to simulate the mechanical behavior of biodegradable
(esophageal) polymeric braided wire stents is developed. The needed implementation of the steric
interaction and friction between the wires is included in this model. Degradation studies on a
polydioxanone stent and wires have been conducted to gain insight in the degradation mechanism of
biodegradable aliphatic polyesters and its influence on the stent’s mechanics. Improvements to the current
stent design are proposed and tested in a total esophageal stent deployment FEM simulation.
Keywords
Biodegradable esophageal stent – polymeric braided wire stent - finite element simulations – polydioxanone
– degradation studies

Design of Biodegradable Esophageal Stents
Mathias Peirlinck
Supervisors: ir. Nic Debusschere, dr. Matthieu De Beule
Promotors: prof. dr. ir. Benedict Verhegghe, prof. dr. Peter Dubruel
Abstract—In this article, a numerical framework to simulate
the mechanical behavior of biodegradable (esophageal)
polymeric braided wire stents is developed. This framework
includes the necessary implementation of the steric
interaction and friction between the wires. Degradation
studies on a polydioxanone stent and wires have been
conducted to gain insight into the degradation mechanism of
biodegradable aliphatic polyesters and its influence on the
stent’s mechanics. Improvements to the current stent design
are proposed and tested in a total esophageal stent
deployment FEM simulation.
Keywords—Biodegradable esophageal stent, polymeric
braided wire stent, finite element simulations, degradation
studies, polydioxanone
I. Introduction
A wide variety of gastro-intestinal pathologies originate from
problems with the esophagus. Any malfunctioning of this organ
can easily lead to considerable discomfort and problems. Until
recently, esophageal stenting was only used as a palliative
treatment to solve intraluminal obstruction or extrinsic
esophageal compression caused by malignant tumor(s),
esophageal strictures and/or perforations, trachea-esophageal
fistula and gastro-esophageal anastomotic leaks. Partially and
fully covered esophageal stents were developed to avoid tumor
ingrowth and to allow esophageal stenting to be used as a
possible temporary treatment for the above-mentioned
pathologies. Migration problems and severe complication rates
(perforations, bleeding, chest pain, nausea, fistula, mal-
positioning, migration, …) and morbidity during stent removal
however did not open up the list of indications for esophageal
stenting. Up till today partially or fully covered self-expanding
metallic or plastic stents (SEMS & SEPS) are not recommended
or FDA approved for benign esophageal conditions. The quality
of evidence for their use in those circumstances is very low
and significant improvements in the design have to be made.
The Polyflex stent is the only exception as it is licensed in the
US for use in benign conditions, but the guidelines still do not
recommend it.
Biodegradable esophageal stents (BDES) can occupy the
niche of temporary esophageal stenting as they can support the
lumen for a certain period and gradually degrade afterwards.
Migration is avoided as the tissue is allowed to grow into the
stent and dangerous stent removal procedures are no longer
needed.
The first bioresorbable esophageal stent has recently been
introduced in Europe, the Ella BD stent, but complaints about
insufficient radial force and premature degradation
demonstrate the need for a better design. As analytical models
appear unable of capturing the mechanical behavior of
bioresorbable polymeric braided wire stents [1], a numerical
model has to be developed. Since finite element modeling is an
important tool in the design of novel stents, such a model will
be developed in this article.
The Ella BD stent consists of polydioxanone-monofilaments
(PDS), the currently applied material for biodegradable sutures.
This polyester generally disintegrates by hydrolytic bulk
degradation.
Figure 1. Radial force during degradation Ella BD stent
II. Degradation studies
To study the evolution of the mechanical properties and the
degradation mechanism, an Ella BD stent and some wires from
such a stent were placed in a phosphate buffered solution
(PBS) at 37°C for 10 weeks. Approximately every week a
compression test and a tensile test were conducted on
respectively the full stent and stent wire samples.
0
10
20
30
40
50
60
70
80
90
8 12 16 20 24
Rad
ial
load
(N
)
Diameter (mm)
Degradation day 0 Degradation day 7
Degradation day 14 Degradation day 23
Degradation day 35 Degradation day 37
Degradation day 48 Degradation day 56

A. Radial force during degradation
A radial stent compression unit was used to measure the
evolution of the radial force of the stent during its degradation.
The results are shown in Figure 1.
B. Stiffness during degradation
Every week, tensile tests were conducted on three
degrading wire samples, initially separated from the Ella BD
stent. The evolution of the Young’s Modulus during
degradation is plotted in Figure 2.
Figure 2. Stiffness during degradation Ella BD stent
C. Degradation mechanism
The hydrolytic degradation process of polydioxanone
monofilaments occurs in two steps. The ester bonds in the
amorphous aliphatic polymer regions are attacked first and the
cleaved chains can rearrange in a more ordered packing which
maintains or increases the polymer’s stiffness initially. In the
second phase, the polymeric chains are attacked randomly and
after a while the shortening chains can diffuse out of the
polymer [2][3]. Strength and stiffness decrease until total
degradation is reached.
As long as the biocompatible, mechanical, geometrical and
absorption rate requirements are met, other and stronger
aliphatic polyesters can be used for a BDES. The visualization
during fluoroscopy might be improved through the inclusion of
radiopaque powders or nanoparticles.
The gained insights in the degradation mechanism can be
used to adapt the existing constitutive degradation models [4]
to match the degradation mechanism of aliphatic polyesters
within the esophageal environment and can subsequently be
implemented in the developed numerical framework.
III. Mechanical modeling
To develop a finite element model, the results of the
degradation studies are used, as it is impossible to determine
friction between the wires experimentally. The friction
coefficient in the model will thus have to be fitted to the result.
The geometrical model must perfectly match the geometry
of the Ella BD stent, as does the simulated stent compression
unit. The (parametric) geometrical model of the Ella-BD wire
stent is developed in pyFormex, an in-house script-based
geometrical and finite element preprocessor. Preprocessing
scripts in Python transform this geometrical model in a finite
element model input file for the finite element solver Abaqus
(Dassault Systèmes, Providence USA). To simulate the steric
interaction and friction between the wires, two methods were
studied: by using connector elements and by implementing
internal self-contact surfaces between the wires reciprocally.
HINGE connector elements were chosen for the first modeling
strategy, although combined REVOLUTE and SLIDE-PLANE
connectors were also an option. The stent compression test
performed during the degradation studies is simulated in detail
for both models and the measured radial forces were
compared to the results of the simulations. The models with
steric interaction and friction between the wires imposed by
HINGE connectors appeared to be too stiff. The models with
friction implemented by internal self-contact however were
capable of capturing the mechanical behavior of biodegradable
(esophageal) polymeric braided wire stents. This is depicted in
Figure 3. A friction coefficient of 0.1 appeared to be the most
appropriate as the experimental results are overestimated at
small diameters due to internal friction effects in the stent
compression unit.
Figure 3. Simulations stent compression test day 35 - Internal self-contact models
0
100
200
300
400
500
600
700
800
900
0 7 14 23 35 37 48 56
Yo
un
g's
Mo
du
lus
(N/m
m²)
Degradation day
0
10
20
30
40
50
8 12 16 20 24
Rad
ial
load
(N
)
Diameter (mm)
experimental FC 0.1
FC 0.3 FC 0.5

The correct numerical framework with steric interaction
and friction between the wires incorporated in it, allows us to
study of the exact mechanical behavior of these stents via finite
element analyzes. The stent design can be easily optimized now
and could, in the future, be personally adapted to the patient’s
specifically needed radial pressure, case by case.
IV. Stent expansion simulation
To study the stent’s deployment and its capability of opening
up the lumen in a real esophageal environment, a full expansion
simulation within a modeled stenosed esophagus was
developed. The esophagus is modeled as a two-layered
(mucosa and muscle) hyperelastic tube with material
parameters deduced from experimental stress-relaxation
curves. The preloading and deployment is simulated as it
occurs in reality (Figure 4).
Figure 4. Stent deployment within the esophagus
The full expansion simulation allows for an easy calculation
of specific displacements or forces in the system. The pressure
exerted on the esophageal wall (Figure 5), for example, is an
important design factor as it has to fall between patient-specific
limits to avoid migration and insufficient opening on the one
hand and pain, pressure necrosis and perforation on the other
hand.
Figure 5. Pressure exerted by the stent on the esophageal wall (spectrum: 0 - 5 kPa)
The stent degradation is imposed in the full expansion
simulation by varying the elastic modulus and thus the stent’s
stiffness through time. This is done equivalent to the stiffness
variation measured in the degradation studies. This gives an
idea about the deterioration of the stent’s capability to open
up the lumen through time. In the case of the Ella BD stent, the
opening capability decreases through time (Figure 6).
Figure 6. Evolution stenosis diameter with stent degradation
V. Conclusion and future prospects
A correct numerical framework for (biodegradable)
polymeric braided wire stents has been developed and
successfully applied in a full esophageal stent expansion
simulation. The stent’s stiffness and exerted esophageal wall
pressure have been studied, together with its capability to
open up the esophageal lumen throughout degradation. The
performed simulations allow for better design and testing of
novel biodegradable esophageal stents. For even more realistic
simulations, some material models have to be adapted to
include long-term effects and the constitutive degradation
models can be implemented after being adapted and fitted to
the degradation of bioresorbable aliphatic polyesters.
References
[1] J.-P. Nuutinen, C. Clerc, and P. Törmälä, “Theoretical and experimental evaluation of the radial force of self-expanding braided bioabsorbable stents,” J. Biomater. Sci. Polym. Ed., vol. 14, no. 7, pp. 677–687, 2003.
[2] M. A. Sabino, S. González, L. Márquez, and J. L. Feijoo, “Study of the
hydrolytic degradation of polydioxanone PPDX,” Polym. Degrad. Stab., vol. 69, no. 2, pp. 209–216, Jul. 2000.
[3] G. Li, Y. Li, P. Lan, J. Li, Z. Zhao, X. He, J. Zhang, and H. Hu, “Biodegradable weft-knitted intestinal stents: Fabrication and physical changes investigation in vitro degradation,” J. Biomed. Mater. Res. A, Apr. 2013.
[4] J. S. Soares, J. E. Moore Jr, and K. R. Rajagopal, “Constitutive framework for biodegradable polymers with applications to biodegradable stents,” Asaio J. Am. Soc. Artif. Intern. Organs 1992, vol. 54, no. 3, pp. 295–301, Jun.
2008.
0
2
4
6
8
10
0 20 40 60
Inn
er
rad
ius
sten
osi
s (m
m)
Days

Contents
Chapter 1 Introduction .......................................................................................................................................................... 1
1.1 The esophagus ........................................................................................................................................................ 1
1.2 Esophageal stents ................................................................................................................................................... 3
1.2.1 Clinical application ........................................................................................................................................ 3
1.2.2 Different types of esophageal stents ........................................................................................................ 7
1.2.3 Stent selection ............................................................................................................................................. 17
1.2.4 Technique of insertion .............................................................................................................................. 17
1.2.5 Complications .............................................................................................................................................. 18
1.2.6 The future ..................................................................................................................................................... 19
1.3 Biodegradable esophageal stents ...................................................................................................................... 19
1.3.1 Biodegradable esophageal stents niche ................................................................................................. 19
1.3.2 Biodegradable materials ............................................................................................................................ 20
1.3.3 Ella-BD stent ................................................................................................................................................ 22
1.3.4 Limitations .................................................................................................................................................... 23
1.4 Challenges .............................................................................................................................................................. 23
1.5 Goal ......................................................................................................................................................................... 25
1.6 Outline ................................................................................................................................................................... 25
Chapter 2 Degradation studies ........................................................................................................................................... 27
2.1 Mechanical degradation ...................................................................................................................................... 27
2.1.1 Radial compression test ............................................................................................................................ 27
2.1.2 Tensile test ................................................................................................................................................... 33
2.1.3 Degradation conditions ............................................................................................................................. 35
2.1.4 Radial force during degradation .............................................................................................................. 36
2.1.5 Stiffness during degradation ..................................................................................................................... 38
2.2 Chemical degradation ......................................................................................................................................... 39
2.2.1 Polydioxanone ............................................................................................................................................. 39
2.2.2 Degradation mechanism ............................................................................................................................ 40
2.2.3 Degradation experiments ......................................................................................................................... 42
2.3 Fit in constitutive model .................................................................................................................................... 47
2.4 Improving the used biodegradable polymer .................................................................................................. 48
Chapter 3 Mechanical modeling ......................................................................................................................................... 50

3.1 Geometric modeling ........................................................................................................................................... 50
3.1.1 Creating the bended wire segment ........................................................................................................ 52
3.1.2 Creating the flares ...................................................................................................................................... 53
3.1.3 Cylindrical stent structure ........................................................................................................................ 54
3.1.4 Preprocessing .............................................................................................................................................. 55
3.2 Finite element model .......................................................................................................................................... 55
3.2.1 Materials and methods .............................................................................................................................. 55
3.2.2 Fine-tuning .................................................................................................................................................... 62
3.2.3 Results ........................................................................................................................................................... 66
3.3 Design optimization............................................................................................................................................. 69
3.3.1 Pitch angle ..................................................................................................................................................... 71
3.3.2 Amount of wires ......................................................................................................................................... 72
Chapter 4 Esophageal stent expansion simulation ......................................................................................................... 73
4.1 Modeling the esophagus ..................................................................................................................................... 73
4.1.1 Geometrical model .................................................................................................................................... 73
4.1.2 Material model............................................................................................................................................. 75
4.2 Total deployment and expansion simulation ................................................................................................. 76
4.2.1 Loading procedure ..................................................................................................................................... 76
4.2.2 Implantation procedure ............................................................................................................................. 77
4.3 Functioning within esophagus ........................................................................................................................... 78
4.4 Stent degradation ................................................................................................................................................. 79
4.5 Future improvements ......................................................................................................................................... 80
Chapter 5 Conclusions and future prospects ................................................................................................................. 82
Bibliography ............................................................................................................................................................................. 84
List of Figures .......................................................................................................................................................................... 88
List of Tables ........................................................................................................................................................................... 90
List of Graphs .......................................................................................................................................................................... 91
List of Scripts ........................................................................................................................................................................... 92

List of Abbreviations & Symbols
Abbreviations
BDES biodegradable esophageal stent(s)
SEMS self-expandable metallic stent(s)
SEPS self-expandable plastic stent(s)
TEF trache-esophageal fistula
GERD gastro-esophageal reflux disease
PCSEMS partially covered self-expanding metallic stent(s)
RBES refractory benign esophageal strictures
LES lower esophageal sphincter
EBTI endoscopic botulinum toxin injection
FDA Food and Drug Administration
PLA poly-lactic acid
PGA poly-glycolic acid
PCL poly-caprolactone
PDS poly(-p-)dioxanone
BDPBWS biodegradable polymeric braided wire stent(s)
SCU stent compressing unit
PBS phosphate buffer solution
FEM finite element model
TGA thermogravimetric analysis
DSC differential scanning calorimetry (analysis)
GPC gel permeation chromatography (analysis)
NMR nuclear magnetic resonance (analysis)
SPR assembled SLIDE-PLANE + REVOLUTE-connector
QLV quasi-linear viscoelastic
CT Computed Tomography
MRI Magnetic Resonance Imaging
Symbols
E axial extension shaft Instron testing machine
D internal diameter MPT SCU
a dimensionless linear coefficient
b off-set coefficient
W virtual work
r radius coupled to the radial force applied on the stent
the general friction coefficient between the SCU segments and in the SCU device
µ friction coefficient stent
Cp specific heat capacity

vii
d degradation parameter of the constitutive degradation model
F deformation gradient of the constitutive degradation model
σ internal stresses constitutive degradation model
E elastic modulus
α parameter correlating degradation parameter to elastic modulus constitutive
degradation model
De external diameter of the stent
fD flared external diameter of the stent
L stent length
fL length of one of the flares
d wire diameter
nx number of wires in one spiral set
β pitch angle
nb number of elements in a strut
ds extra (optional) radial distance between the wires
transverse shear forces
transverse shear strains
slenderness compensation factor
x amount of the user want to impose
inner octahedron radius
outer octahedron radius
( ) moment magnitude of the frictional tangential tractions in the connector in a
direction tangent to the cylindrical surface on which contact occurs
friction-producing normal moment on the same cylindrical surface
magnitude measure of friction-producing connector elements
self-equilibrated internal contact moment of the HINGE connector
µs static friction coefficient
µk kinetic friction coefficient
κ tangential softening coefficient
diam outer diameter esophagus
ltot the total length of the esophagus
lstr the stricture length
thic the esophageal wall thickness
stri the narrowing fraction of the lumen caused by the stenosis
nr the number of partitions in the radial direction
nl the number of partitions in the longitudinal direction (normal open-lumen part)
ns the number of partitions in the longitudinal direction (constricted part)
na the number of partitions in the angular direction
( ) instantaneous elastic response to a step input of strain
( ) reduced relaxation function representing the time-dependent stress response
normalized by the peak stress at the time of the step input of strain
m linear factor with the same dimension as stress (N/mm²)
n non-dimensional parameter representing the rate of stress stiffening.

Chapter 1
Introduction
This chapter first dives into the anatomy of the esophagus to gain insight into the environment in which the
stent will operate. The esophageal stent as an actual clinical application and its history will be described
afterwards. The different types of esophageal stents will be compared, as will their specific applications.
Once the normal esophageal stenting has been covered, we will focus on biodegradable esophageal stents
and try to analyze which niche in the medical field they will be able to fill. Benefits and disadvantages will be
explored and discussed.
1.1 The esophagus
Figure 1-1. Gastroesophageal junction [1]
The esophagus [1] is one of the many important organs responsible for the human’s digestive system and
links the mouth and the pharynx to the stomach. It is a 18-25cm long muscular tube that passes through the
mediastinum of the thorax and enters the abdomen through the esophageal hiatus (the hole in the
diaphragm where both the esophagus and the vagus nerve pass) [2]. This organ can be subdivided in a
cervical, a thoracic and an abdominal part. The lumen can distend to approximately 2 cm in the anterior-
posterior dimension and up to 3 cm laterally to pass down a swallowed bolus under the control of
peristaltic esophageal muscle contractions. The gastroesophageal sphincter, also called cardiac sphincter,
forms the transition between the esophagus and the stomach. This sphincter is a physical sphincter as it

Introduction 2
forms a valve that has to keep the stomach closed except when a food bolus has to pass or in case of
emesis (vomiting). This sphincter is only slightly visible as a local thickening of the circular smooth muscle.
The gastroesophageal’s junction is supported by the muscular diaphragm which surrounds the sphincter,
thus helping to keep it closed when no food boluses are passing.
The esophageal wall is made up of four basic layers:
The mucosa consists of a stratified squamous epithelium which is in clear contrast with the simple
columnar epithelium of the stomach that is invaginated with gastric pits. The transition between
both mucosa is very abrupt and considered as the esophagogastric junction.
The submucosa is composed of areolar connective tissue and contains mucus-secreting esophageal
glands. Bolus movement through the esophagus compresses these glands which leads to mucus
secretion in order to “grease” the esophageal walls and help the food passage to be pushed
downwards. When no food bolus is passing through the esophagus, both the mucosa and
submucosa fold up in longitudinal folds. These folds get flattened out when food passes.
The muscularis externa comprises an inner circular layer and an outer longitudinal layer formed by
both skeletal and smooth muscle tissue.
The adventitia is the outer layer of the esophagus and consists entirely out of fibrous connective
tissue which is able to blend with surrounding tissue that lies along the esophagus as it passes from
pharynx to stomach.
Figure 1-2. Cross section esophageal lumen [1]

Introduction 3
1.2 Esophageal stents
A wide variety of gastro-intestinal pathologies originate from problems with the esophagus. Any
malfunctioning of this organ can easily lead to considerable discomfort and complications.
1.2.1 Clinical application
As stent designs have undergone significant changes over the past 20 years, the list of indications has
expanded while complication rates have decreased. Some of the indications for which esophageal stents can
be used nowadays are discussed in this section.
1.2.1.1 Esophageal ulcers
An ulcer is defined as a local defect or excavation of the surface of an organ or tissue, produced by
sloughing of necrotic inflammatory tissue. The degradation of the esophageal mucosa is thus defined as an
esophageal ulcer.
Any acidic regurgitation in the esophagus will first cause irritation and eventually digestion of the esophageal
epithelium. These regurgitations can result in edema, small superficial ulcerations or larger flat ulcers,
depending on their frequency of occurrence and duration. The acidity of the gastric content leads
microscopically to necrosis of the epithelium, erosions, hyalinization of the mucosa, small cell infiltration,
hypertrophy of the muscle fibers in the mucosa and connective tissue proliferation, according to the gravity
of the inflammatory process.
In some pathologies, these regurgitation episodes are quite frequent and prolonged, leading to inflammation
of the esophagus (esophagitis). Chronic esophagitis can then cause ulcers and, as an even more threatening
consequence, esophageal cancer. Patients suffering from gastro-esophageal reflux disease (GERD) often
suffer from acid gastric content regurgitation, which is mostly due to a malfunctioning of the lower
esophageal sphincter. Another pathology that can lead to too frequent regurgitation is a hiatal hernia, being
a structural abnormality in which the stomach protrudes above the diaphragm. This hiatal hernia can be
linked to e.g. congenital abnormalities or abnormal relaxation or weakening of the gastroesophageal
sphincter.
Ulcers specifically aren’t treated with esophageal stents although some consequences of ulcers can be, as
will be presented in the following sections. Fully biodegradable (drug-eluting) stents could however include
ulcers as indication for use.
1.2.1.2 Benign strictures
Strictures of the esophagus (Figure 1-3) can originate from a variety of pathologies. Congenital anomalies,
web or ring formation, swallowing of caustics, ulcers produced by foreign bodies and peptic ulcers can all
lead to some kind of esophageal stricture which makes it not so rare in clinical practice.
The swallowing of caustics, as an accidental or a suicidal act, destroys the mucosa of the esophagus and
results in the production of redundant fibrotic tissue, which is the body’s defense mechanism to control the
tissue damage. This fibrotic tissue contracts the esophageal wall, thus leading to a narrowing of the lumen.

Introduction 4
Ulcers, caused by foreign bodies or regurgitation of hydrochloric acid gastric juice, attempt to heal by
proliferation of connective tissue, leaving behind a fibrotic scar. This scar could also constrict the lumen and
thus create an esophageal stricture. [3]
1.2.1.2.1 Refractory benign esophageal strictures
Some people suffer from refractory benign esophageal strictures, a condition that seems to be related to an
extensive fibrosis of the submucosa up to the muscular layer, mostly in case of anastomosis-, caustic-, or
radiation-induced strictures. RBES-patients often do not experience any meaningful improvement after
endoscopic dilation with bougies or balloons. They have a lower quality of life mainly because of dysphagia.
The strictures may lead to severe complications such as malnutrition, weight loss and aspiration. Esophageal
stenting is not considered as a standard treatment for patients suffering with RBES, but with the
development of BDES, it might be in the future (§1.3.1). Some studies indicate that biodegradable stenting
could be considered a relatively effective and safe alternative treatment for patients with RBES (e.g. [4]).
Figure 1-3. Esophageal strictures [1]

Introduction 5
1.2.1.3 Rupture, perforations and fistula
As mentioned before, peptic ulcers might lead to a perforation of the esophagus. Penetration of the wall by
a foreign body or the ingestion of a corrosive liquid are together with the peptic ulcers the most frequent
causes of esophageal rupture. In the cervical esophagus, the introduction of an instrument, as can be the
case during esophagoscopic exams, can also lead to ruptures.
Spontaneous rupture of the esophagus is very rare but does exist. During violent coughing or excessive
vomiting, the sudden increase of intra-esophageal pressure ruptures, in those cases, a presumable pre-
existing weakness of the esophageal wall.
A tracheoesophageal fistula (TEF) is an abnormal connection between the trachea and the esophagus.
Mostly, TEFs are congenital abnormalities, but in some cases they can also be caused by surgical procedures
or by inserted tubes/foreign bodies in the trachea or esophagus.
Both esophageal rupture and perforation are potentially life-threatening events that are associated with high
morbidity and mortality rates. A diagnosis has to be established soon enough and intervention is needed
almost immediately to have any chance of success. Classic surgical treatments consist of surgical repair,
esophagectomy or cervical exclusion. However, in case of delayed diagnosis, the morbidity and mortality of
surgical procedures become increasingly higher with time. Recently, the placement of esophageal stents
have shown some good results and can be considered a promising modality in the treatment of these
conditions. Scientific literature on stenting to treat esophageal ruptures and perforations is limited to case
reports and case series showing mixed results. Some case reports were favorable of ruptures and
perforations as an indication for esophageal stenting [5][6]. Other studies mention complications such as
bleeding, stent-related strictures, tissue ingrowth, fistula formation and stent migration.
TEFs are normally treated by a surgery resecting the fistula making sure to reconnect the esophagus and the
trachea as they should be. As an alternative, treating fistula with removable esophageal stents is possible
although it is still considered to be an off-label indication by the FDA. Again different case reports lead to
mixed results but in general most of them showed pleasing results [7][8].
1.2.1.4 Malignancy
Esophageal cancer is in general a relatively rare form of cancer. Historically, most cases of esophageal
cancer were, histologically seen, squamous-cell carcinomas. This, however, is no longer the case in northern
Europe (e.g. Denmark) as esophageal adenocarcinomas have become the prevailing histological forms of
esophageal cancer. In the EU, the incidence of esophageal cancer in general started to level off compared to
the upward trends that were seen in the 1990s. These changes in trends and leveling off of the incidence are
probably due to changes in smoking habits, alcohol drinking, nutrition, diet and physical activity [9].
Unfortunately for the patient, esophageal cancer is mostly discovered in an advanced stage in which a
curative resection, radio- and/or chemotherapy can no longer lead to recovery from the tumor. Patients
frequently do not recognize any symptoms until at least 50% of the luminal diameter is compromised
because of the distensible nature of the esophagus. In those cases, the only option left is a palliative
treatment. The cancer cannot be cured and will eventually lead to the patient’s death. The tumor will in
most cases lead to dysphagia which causes a lot of problems such as malnutrition, aspiration of saliva,

Introduction 6
aspiration of food, etc. The patient might also suffer from severe thoracic pains caused by the invasion of an
unresectable tumor.
The general goal of treatment for patients in this advanced disease stage is to improve the quality of the
remaining life. This improvement is generally focused on relieving dysphagia and preventing malnutrition.
The aim is to restore the patient’s ability to take in food and fluids orally, as most patients still want to eat
and participate in the social activity that is linked to having a meal together. Esophageal stents can be used in
these cases to solve intraluminal obstruction or extrinsic esophageal compression caused by the primary (or
secondary) tumor(s), esophageal strictures and/or perforations, tracheoesophageal fistula, gastroesophageal
anastomotic leaks and tumor recurrence after surgery or chemoradiotherapy. All these specific indications
can be the result of malignant tumors but might also result from other pathologies.
1.2.1.5 Achalasia
Esophageal achalasia (also called esophageal aperistalsis, achalasia cardiae or cardiospasm) is an esophageal
motility disorder which involves the smooth muscle layer of the lower esophageal sphincter (LES) and the
esophagus itself. Diagnosis of this disorder is often based on difficult swallowing (dysphagia in 90 % of the
patients for both solids and liquids, which forms a difference with dysphagia of typical anatomical disorders),
regurgitation, weight loss and chest pain in some cases (60% of the patients) [10]. Typically, the disorder is
due to incomplete LES relaxation, increased LES tone, lack of esophageal peristalsis without any
concomitant cancer or fibrosis.
As a food bolus enters the esophagus, normally peristaltic waves and LES relaxation guide that bolus
towards the stomach. These waves of relaxation are governed by both excitatory and inhibitory input from
the vagus nerve. For primary achalasia, a failure of distal esophageal inhibitory neurons (degeneration of
ganglion cells in the myenteric plexus of the esophageal body and the LES due to inflammations) causes all
problems. Although no underlying cause has yet been found, possible disease mechanisms have been
postulated [11].
Therapy of achalasia focuses on relaxation or mechanical disruption of the esophagus and/or LES [10][12].
Adverse side effects and a general lack of efficacy have precluded the use of peristalsis-augmenting or LES-
relaxing drugs. The standard treatment of achalasia is thus an endoscopic procedure in which a surgeon
typically makes a lengthwise cut along the esophagus, starting above the LES and extending down onto the
stomach. This surgery is called Heller myotomy and helps 90% of the patients. For patients who cannot
undergo surgery, endoscopic botulinum toxin injection (EBTI) in the LES is often considered, paralyzing the
muscles holding it shut. This treatment only works temporarily however and causes scarring in the
sphincter. In esophageal balloon dilation, the gastroenterologist stretches and slightly tears the muscle fibers
by inflating a balloon inside the LES. As for patients younger than 40 the benefits of this technique might be
shorter-lived, repeated balloon dilatation with larger balloons might be needed for maximum effectiveness.
Temporary esophageal stents however could also stretch and slightly tear these muscle fibers and can thus
also be used for achalasia treatment.

Introduction 7
1.2.1.6 Indications and contraindications of esophageal stenting
Table 1-1 gives a summary of the pathologies for which esophageal stents can be used nowadays and in the
future. The list has opened up due to the development of newer stents, with some specifically designed for
temporary treatments.
Table 1-1. Indications and contraindictions for SEMS and SEPS [13].
Indications
1. Malignant esophageal stricture - inoperable, poor surgical candidate, contraindication to chemoradiation
2. Malignant recurrence - anastomotic or otherwise
3. Extrinsic esophageal compression - primary or secondary mediastinal and lung tumors
4. Tracheoesophageal fistulas - malignant and benign
5. Esophageal perforation - iatrogenic and spontaneous
6. Benign strictures - refractory to balloon dilation and not surgically amenable
7. ± Achalasia patient who is a poor surgical candidate and refractory to other endoscopic treatments-ELLA-BD
stent
8. ± Bleeding esophageal varices refractory to other endoscopic measures as an alternative to or
contraindication to transjugular intrahepatic portosystemic shunt - ELLA-Danis stent
Contra-indications
1. Curable malignant esophageal stricture
2. Terminally ill patients with limited life expectancy
3. ± Stricture within 2 cm of upper esophageal sphincter
4. Risk of airway compression (without addressing this first)
5. ± Recent high-dose chemoradiation (within 3-6 weeks)
6. Unaddressed gastroduodenal and/or small bowel obstruction
7. Sepsis
8. Uncorrected coagulopathy
1.2.2 Different types of esophageal stents
1.2.2.1 History
Rigid polyvinyl plastic or rubber stents were historically the first stents that were used for esophageal
intubation to solve obstruction in the esophagus. They were inserted into the patient’s esophagus by means
of oral pulsion or by the use of an open traction technique (requiring laparotomy and gastrostomy). Typical
complications of these kinds of stents were stent migration, food impaction and perforation. The stents
were also difficult to place and frequently caused severe pain to the patient. Esophageal stenting has
however undergone considerable improvements over the past 20 years.
The importance of rigid polyvinyl plastic stents quickly diminished with the introduction of self-expandable
metal stents (SEMS) in the early 1990s. Stent-related mortality was significantly decreased with the use of
these SEMS, as was esophageal perforation and stent migration. SEMS provided better palliation of
dysphagia, reduced recurrent dysphagia, decreased initial hospital stay and procedure-related morbidity and
mortality [14]. They were more expensive but the extra cost did not weigh up against all the advantages
with respect to the rigid stents. The only complication of the first-generation SEMS was tumor ingrowth
through the open mesh which resulted in a return to dysphagia. Trying to solve this problem lead to the

Introduction 8
development of partially covered SEMS. A thin layer of silicone or plastic covering on the body of the SEMS
impedes tumor ingrowth.
Hypertrophic granulation is the overgrowth effect that can occur when the healing- and immune-factors-
rich wound bed tries to fight infection and contracts the wound shut at the uncovered stent ends over
some time. This tissue could eventually obstruct the esophagus and prevent repositioning or removal of the
stents, rendering them only useful for palliation of malignant dysphagia as stent-adjustment was impossible.
Later on, a new type of esophageal stents was introduced, namely the self-expanding plastic stent (SEPS)
which was fully covered. These SEPS did not have strong contraindications except for palliation of malignant
dysphagia or fistulae as they were designed to be retrieved after a certain period, which wasn’t the case for
the PCSEMS. SEPS (initially) caused higher radial force than the SEMS which could lead to early migration,
discomfort and complaints for some patients. Another possible disadvantage of SEPS is the somewhat stiff
and bulky introducer on which they have to be loaded prior to insertion due to their plastic construction.
They can’t be easily crimped on a small guidewire. Nevertheless, nowadays the newer SEPS designs are still
used for temporary esophageal stenting procedures (see §1.2.2.2.7).
Eventually, the development of fully-covered self-expanding metal stents (SEMS) took place to overcome
this problem with the fully covered SEPS. The majority of recent studies also suggest that despite the
comparable efficacy in the treatment of dysphagia between SEMS and SEPS, significantly less complications
were seen with SEMSs than with SEPSs. Nowadays the covered stent is the mainly used stent type for the
palliation of malignant dysphagia as tumor tissue ingrowth in the stent mesh is prevented. Apart from
malignancy, both fully covered SEPSs and SEMSs are used more and more to treat a variety of benign
esophageal conditions (ex infra). Covering of stents thus also leads to the ability of sealing TEFs with a stent.
Both SEMS and SEPS open up the esophageal lumen due to their inherent material (shape) memory
generating a radial expansile force against the obstructing diseased tissue. Both stainless steel (e.g. Z-stent
(Cook)) as alloys such as Nitinol (e.g. Ultraflex (Boston Scientific)) and Elgiloy (e.g. Wallstent (Boston
Scientific)) can be used for SEMS [15]. Nitinol has become the dominant material however due to its
advantages of shape memory, elasticity, ability to conform better to angulations, higher radial resistive forces
and MRI-compatibility (as nitinol stents are ferromagnetic) [13].
1.2.2.2 Esophageal stents currently on the market
Except for the rigid polyvinyl plastic stents, both self-expandable metal and plastic stents are currently being
used in clinical practice. Various manufacturers around the world have designed different types of
prostheses that differ in stent material (stainless steel, nitinol, plastic, biodegradable polymers), design,
luminal diameter, radial force exerted, flexibility, foreshortening, etc.
A brief summary of the esophageal stents that are currently on the market in the USA, Europe and Asia is
given below [13][16][17][18].
1.2.2.2.1 Alimaxx-ES (Merit Medical Systems, UT)
This prosthesis is a fully polyurethane-coated laser-cut nitinol stent with a silicone lining. ‘Antimigration
struts’ projecting from the length of the stent are introduced to prevent migration. Two different delivery
systems can be used, one using a traditional guidewire to direct the stent’s deployment, the other using a

Introduction 9
pediatric gastroscope on which the stent is mounted and released under “direct visualization”. With a non-
braided design, removal can be defaulted due to coating breaks and prosthesis fragmentation. The smaller
diameters of this stent type were released later for use in very tight strictures and smaller lumen esophagi
(pediatrics).
Figure 1-4. ALIMAXX-ES™ Fully Covered Esophageal Stent
1.2.2.2.2 Evolution (Cook Medical, Bloomington - Ind - USA/ Limerick - Ireland)
Evolution represents a new line of SEMS introduced by Cook Medical. Two different versions are available: a
partially covered and a fully covered version. Interior and exterior surfaces are encased with silicone in
order to prevent tumor ingrowth as this stent was specifically designed to overcome the problem of
recurrent dysphagia. Uncoated flanges on both ends of the stent serve to prevent migration, resulting in a
“dog bone” shape and allowing the stent to embed itself in the esophageal wall. The fully covered version is
equipped with a kind of ‘lasso loop’, a dual purse string, on both the distal and proximal end, which could
aid in stent-repositioning if needed. The Evolution’s gun-like delivery system is also remarkable as it enables
the surgeon to control release and recapturing with a “point of no return” indicator. With each squeeze of
the stent system’s trigger-based introducer, a proportional length of the stent is deployed or recaptured.
Figure 1-5. Evolution® Esophageal Fully Covered Controlled-
Release Stent
Figure 1-6. Evolution® Esophageal Partially Covered Controlled-
Release Stent

Introduction 10
1.2.2.2.3 Ella stents: FerX-Ella, SX-Ella, biodegradable SX-Ella, Ella-Danis (Ella-CS,
Hradec Kralove, Czech Republic)
This stent line has recently been introduced in Europe and is made of stainless steel (FerX), nitionol (SX) or
the polymer poly-p-dioxanone (biodegradable SX/BD). More focus on this biodegradable model will follow
(§1.3.3). Both metal versions are fully coated with polyethylene and are available with or without anti-reflux
flaps.
The SX–ELLA Esophageal HV stent is fully covered to resist tissue ingrowth but has a unique anti-migration
design. This design consists of a flip-flop type ring which is circumferentially attached to the proximal margin
of the stent (Figure 1-7). As mentioned before, this stent is made of a nickel-titanium alloy and braided from
only one wire aiming to make the stent end contacts less traumatic for the tissue. The one-wire braiding
also improves the flexibility of the stent [19].
Figure 1-7. Antimigration ring Ella stents Figure 1-8. SX-Ella Danis stent
The SX-Ella-Danis stent (Figure 1-8) is a novel, fully covered esophageal SEMS which is available in Europe.
This stent has specifically been designed to treat refractory cases of esophageal variceal bleeding [13]. The
stent is made from nitinol and equipped with variable pitches in the braiding (allows normal peristalsis) and
covered atraumatic ends. Retrieval loops are attached to the stent to allow removal, which is recommended
to be done 7 days after insertion. Radio-opaque markers at both ends and in the mid-portion of the stent
facilitate fluoroscopically guided placement.
1.2.2.2.4 (Flamingo) Wallstent (Boston Scientific, Boston, Mass, USA)
The Flamingo Wallstent is an older device that is no longer marketed in Europe. It was an alternative version
of the Wallstent (Boston Scientific) which has also been taken off the market. The stent had a conical or
funnel-shaped design providing greater radial expansion proximally, in order to reduce migration across the
esophagogastric junction. The stent was constructed from a braided stainless steel alloy. Due to higher
costs and increased occurrence of chest pain without differences in outcomes for palliation of dysphagia,
complication rates, or migration rates [20][21], the Flamingo Wallstent has never even been marketed in the
US.

Introduction 11
1.2.2.2.5 Z-stents (Wilson-Cook, Winston-Salem, NC, USA)
Z-stents, also known as the Gianturco-Rösch Z-stents, were the first self-expandable metallic stents and were
available in an uncovered and partially covered version. They were constructed from stainless steel, woven
in an interlocking “Z” configuration. The partially covered (polyethylene membrane) version had a flared
design to prevent migration and provide a certain stability. Following the introduction of the Evolution stent
by the same company (Cook, Inc.), these stents were taken off the market.
1.2.2.2.6 Niti-S (Taewoong Medical, Korea)
This is a double layer configured stent (a single-layer version also exists) specifically designed to resist
migration and tumor ingrowth. The inner layer is made of polyurethane (with the goal of preventing tumor
overgrowth) while an outer uncovered nitinol wire tube allows the mesh to embed in the esophageal wall.
The configuration is similar to the Wallflex (ex supra) as the stent uses widely flaring “dog bone” ends to aid
migration-prevention.
Figure 1-9. Taewoong Niti-S™ Esophageal stent
1.2.2.2.7 Polyflex (Boston Scientific, Boston, Mass, USA)
The Polyflex stent is a fully silicone-membrane-covered polyester netted stent which requires loading onto a
delivery system prior to deployment. This is currently the only removable stent licensed in the US to be
used for benign disease (biodegradable stent development might change this) [15].
Figure 1-10. Polyflex® Esophageal Stent
1.2.2.2.8 Ultraflex (Boston Scientific, Boston, Mass, USA)
The Ultraflex stent is manufactured in both an uncovered and a covered version, both consisting of a
construction mesh knitted from a single strand of nitinol wire. In the covered version, the stent-body is
surrounded by a sheath of polyurethane, covering the midsection. A coiled thread around the stent is used

Introduction 12
to keep it compressed along a supple plastic guide. Pulling this thread, leads to self-expansion of the stent
and thus eventually to its final diameter. It is an extremely flexible SEMS. However, this flexibility comes
with a cost, as it has the lowest expansive force of all available esophageal metal stents. This can lead to the
need for extra balloon dilatation to achieve adequate stent expansion.
Figure 1-11. Ultraflex® Esophageal Stent (1: Large Proximal Flare, 2: Polyurethane Covering, 3: Flexible Knitted-Loop Design)
Comparative studies have been done concerning the last three stents and in general, a significantly higher
complication rate was seen with the Polyflex stents than with the Ultraflex stents (recurrent dysphagia caused
by tissue ingrowth, migration, food obstruction, stent placement technical difficulties). In contrast, Polyflex
stents are better protected against tissue overgrowth with respect to Ultraflex stents and to a lesser degree,
to Niti-S stents (not-significant) [6]. In general, Polyflex was, according to that study, the least preferable of
the three. These comparisons aren’t easy to perform however, as will be further treated in §1.2.2.3.
1.2.2.2.9 Wallflex (Boston Scientific, Boston, Mass, USA)
The Wallflex stent is one of the newer generation SEMS, based on a multiple wire braided construction.
Two versions are available: the fully or partially covered Wallflex stent. In contrast with the other stents
described above, the Wallflex can withstand reconstrainment up to 75% of deployment (and can
consequently be recaptured up to a point where 75% of the stent has been deployed), up to two times
during the initial stent placement procedure. This allows the stent to adjust itself to forces from the
esophageal anatomy such as peristalsis and strictures. At the proximal end, a purse string Teflon coated
polyester suture has also been incorporated to facilitate repositioning or removal. Migration is theoretically
reduced by the anchoring of the stent within the esophageal lumen by using “progressive step flared ends”
(Figure 1-12).
Figure 1-12. Wallflex® Fully Covered Esophageal Stent

Introduction 13
Numerous other esophageal stents are available in specific regions of the world, but the most important
stents for Europe and the US have been mentioned above. A summary of all possible stents can be found in
Table 1-2 and are depicted in Figure 1-13 and Figure 1-14.
Table 1-2. Selected SEMS currently available in the United States, Europe, or Asia
Stent Manufacterer Materials Length
(cm)
Diameter shaft/flare
(mm) Covering
Anti-reflux
valve
FDA
Approval
Braid
ed
Ultraflex Boston Scientific Nitinol 10/12/15 18/23 - 23/28 (NC /) PC No Yes Y
Wallflex Boston Scientific Nitinol 12/12/15 18/23 - 18/25 - 23/28 PC/ FC No Yes Y
Evolution Cook Nitinol 8/10/12.5
/15 18/23 - 20/25 PC/FC No Yes Y
Alimaxx-E Alveolus – Merit
Endotek Nitinol 7/10/12 12/14/16/18/22 FC No Yes N
Polyflex Boston Scientific Polyester 9/12/15 16/20 - 18/23 - 21/28 FC No Yes Y
Niti-S (single or double)
TaeWoong Medical
Nitinol 6/9/12/15 16/24 - 18/26 - 20/28 FC Yes/No Yes Y
Bonastent Standard Sci Tech Nitinol 6/8/10/12
/15 18/23-20/25-22/27 PC/ FC Yes/No Yes Y
SX-Ella HV Ella-CS Nitinol 8.5/11 20/25 FC Yes/No No Y
FerX-Ella Ella-CS Stainless
Steel 9-21 20/36 FC Yes/No No N
Dostent MI Tech Nitinol 6/9/12 18/30 FC Yes/no No Y
Ella-BD Ella-CS Poly-p-
diaxanon
6/8/10
/13.5
18/23 - 20/25 - 23/28
- 25/31 FC No No Y
Ella-Danis Ella-CS Nitinol 13.5 25 FC No No Y
Choo MI Tech Nitinol 6-17 18 PC/FC Yes/No No Y
Song Stentech Nitinon 5-18 16-18 NC/PC/F
C Yes/No No Y
(Esophageal Z) Cook Stainless
Steel 8/10/12
/14 18/25 PC
Yes (Dua variant)
Yes N
(Gianturco Z) Cook Stainless
Steel 8/10/12
/14 18/25 PC Yes No N
PC; shaft
bars No No N
(Flamingo Wallstent)
Boston Scientific Stainless
Steel 12/14 20/30 PC No No Y
FDA=Food and Drug Administration; NC=not covered; PC=partially covered; FC=fully covered; ( )=not marketed anymore; SEMS=self-expanding metal stent
As can be seen in Table 1-2, some stents are also marketed with an optional anti-reflux valve. This is
incorporated in stents that have to be deployed in the lower thoracic or abdominal part of the esophagus,
possibly bridging the esophagogastric junction. If this junction is kept open by the stent or the function of
the lower esophageal sphincter is impeded, the patient might suffer from acid stomach content refluxing
into the esophagus. This acid refluxate leads to a lot of discomfort and complications, as is the case for
people suffering from gastro-esophageal reflux disease (complications include heartburn, chronic cough,
nocturnal choking, chronic hoarseness, sore throat, asthma, dental erosion, hypersalivation, inflammation
and even esophageal cancer). To avoid discomfort and complications, the anti-reflux valves were
incorporated to prevent this gastro-esophageal regurgitation. In most cases, these valves are simple
extensions of the existing lining of the stent. However, direct benefits of these incorporated valves over
using standard stents combined with proton pump inhibitor therapy (which neutralizes the acidity of the
stomach’s content) have never been proven [23][24].

Introduction 14
Figure 1-13. Selection of the currently available stents, from left to right Ultraflex, Polyflex, (partially covered) Wallflex, (partially
covered) Evolution, SX-Ella, Niti-S, and Alimaxx-E stents [25].
Figure 1-14. Self-expandable stents: (A) SX Ella, (B) Endoflex, (C) Alimaxx, (D) Polyflex, (E) Ultraflex, (F) Niti-S, (G) Evolution, (H)
Choostent, (I) Dostent, and (J) Hanarostent [26].
1.2.2.3 Comparing studies
The radial force which the stent has to exert has been the source of debate among different stent designers
since the start of its development. An insufficient radial force results in stent migration while an excessively
high radial force results in pain and complications (e.g. pressure necrosis, fistulae formation, stent fracture,
…). Initial stent designs imposed too high radial pressures on the esophageal wall. As the SEMS woven from
shape memory alloys led to softer stents, these problems were averted. The open mesh design made sure
that the stent could enclose itself within the esophagus with a steady radial pressure slowly opening the

Introduction 15
lumen over a timespan of a few days. A tumor could however grow through these stents which led to the
use of silicon or plastic wrapping around the stent. Insufficient embedding of the stent in the esophageal
tissue however led to stent migration, which was partially encountered by the introduction of covered
stents with flared ends/”dogbone” shapes. The flared ends prevented stent migration as esophageal tissue
grew into the mesh of these ends, fixing them in the esophagus. These partially covered stents still weren’t
perfect as hypertrophic granulation tissue could cause recurrent dysphagia. Also, a number of PCSEMS was
still sensitive to migration. Nonetheless, they have been and are still successfully used and have become the
standard of care in the treatment of malignant fistulae and malignant esophago-brancheal leaks.
As these PCSEMS are designed to get rapidly incorporated into the wall, they cannot easily be removed and
thus have a strong contra-indication for anything except these malignant applications. With the development
of fully covered stents, a broad spectrum of new applications of esophageal stents in benign diseases
appeared, such as extrinsic esophageal compression due to primary or secondary tumors, refractory or
recurrent esophageal strictures, trachea-esophageal fistula and esophageal perforation or leak. Stent
migration however is and remains a problem.
The first fully covered stents were made from plastics, which led to high radial forces, pain and
complications. These SEPSs are also more challenging to place.
Fully covered SEMS were the most recent step in the development of esophageal stents, combining
advantages of fully covered SEPSs and partially covered SEMS. As plastic stents cause less tissue damage, the
next evolution in esophageal stent development might be a hybrid stent, combining plastic ends with a
nitinol midsection [13].
In current practice a wide variety of stent designs are commercially available. On what base will we then
decide which stent is most suited for a certain clinical application, compared to others? Studies have been
done to compare one stent design against another but the amount and significance of these studies is
relatively low. The comparison of stent designs is complicated due to randomization difficulties, the large
amount of possible variables (tumor size, tumor location, patient health, …) or even discrimination between
different possible outcomes, apart from survival (especially in the malignant cases). Improved survival rates,
improvement in dysphagia resolution, better quality of life, … are difficult measurements to asses. Some
results of different studies are discussed below and Table 1-3 presents the results of a number of published
test series.
When comparing different studies [27] on migration of different stent types used for malignant dysphagia, it
is noticeable that migration scores are better for the SX-Ella stent (only 20% of the patients) than for the
Alimaxx-E stent (33%) and the Niti-S stent (40 %).
Comparative studies between Wallstent and Ultraflex [28][29][13] have indicated that the Wallstent patient
group generally showed complications due to tumor ingrowth and food impaction, while the Ultraflex
patient group showed incomplete deployment problems (occurred quite often with Ultraflex (P = 0.01)). If a
reintervention was needed, it was also more complex in the case of the Ultraflex stent. In general however,
the Wallstent was associated with higher stent-related mortality (16% vs 0%), higher early complication rate
(32% vs 8%), and severe persistent chest pain (23% vs 0%). That is why the Wallstent is no longer marketed.

Introduction 16
Table 1-3. Recurrent dysphagia and major complications after stent placement of partially or fully covered stents for the palliation
of malignant dysphagia [19].
No. patients (valid %)
Recurrent dysphagia Major complications (hemorrhage, fistula, fever, severe pain, perforation,
aspiration pneumonia)
Author/year Intervention Covering No. Tumoral/ nontumoral
overgrowth Migration
Total reported
Hemorrhage
Randomized trials
Verschuur et al,
2008 [22]
Ultraflex stent Partial 42 13 (31) 7 (17) 9 (21) 5 (12)
Niti-S stent Complete∗ 42 10 (24) 5 (12) 5 (12) 2 (5)
Polyflex stent Complete 41 4 (10) 12 (29) 8 (20) 5 (12)
Conio et al, 2007 [30]
Ultraflex stent Partial 54 14 (26) 2 (4) 3 (6) 0
Polyflex stent Complete 46 14 (30) 6 (13) 4 (9) 2 (4)
Homs et al, 2004 [31]
Ultraflex stent Partial 108 16 (15) 18 (17) 27 (25) 14 (13)
Brachytherapy – 101 – – – –
Sabharwal et al, 2003[20]
Ultraflex stent Partial 31 1 (3) 2 (6) 3 (10) 1 (3)
Flamingo
wallstent
Partial 22 1 (5) 1 (5) 3 (14) 1 (5)
Comparative studies
Verschuur et al,
2007 [32] †
Ultraflex stent Partial 153 20 (13) 27 (18) 38 (25) 23 (15)
Flamingo Wallstent
Partial 96 16 (17) 8 (8) 18 (19) 8 (8)
Gianturco Z
stent
Complete 89 16 (18) 5 (6) 20 (22) 13 (15)
Homs et al, 2004 [33]
Ultraflex stent Partial 75 7 (9)‡ 17 (23)‡ NR NR
Flamingo wallstent
Partial 71 12 (17)‡ 5 (7)‡ NR NR
Gianturco Z stent
Complete 70 11 (16)‡ 4 (6)‡ NR NR
Prospective studies
Uitdehaag et al,
2009 [27]
Alimaxx-E stent Complete 45 7 (16) 16 (36) 9 (20) 2 (4)
Conigliaro et al, 2007 [34]
Polyflex stent Complete 60 8 (14) 12 (20) NR (10) 4 (7)
Szegedi et al, 2006
[35]
Polyflex stent Complete 69 9 (13) 3 (5) 0 0
Verschuur et al, 2006 [36]
Niti-S stent Complete∗ 42 2 (5) 3 (7) 5 (12) 2 (5)
Dormann et al, 2003 [37]
Polyflex stent Complete 33 4 (12) 2 (6) 0 NR
Uitdehaag et al,
2010 [19]
SX-Ella Stent Complete 44 2 (6) 6 (17) 14 (26) 7 (19)
Retrospective studies
Ross et al, 2007 [38]
Wallstent II Partial 97 5 (5) 5 (5) 17 (18) 14 (14)
NR, Not reported.
∗,Inner fully covered with outer uncovered wire tube.
†, Small- and large-diameter stents are counted as 1 group.
‡, Number of events rather than number of patients.

Introduction 17
The clinical performance of the Ultraflex (Boston Scientific, SEMS) and Polyflex (only marketed SEPS) stents
have been extensively compared and the results of these studies (e.g. [21] and [29]) indicate that the
Polyflex is more susceptible to migration. However, these studies also show how hard it is to perform a
specific comparison between results. It is for example known that plastic stents cause less tissue damage
than the nitinol stents but these studies do not reveal a significant difference in major complications.
1.2.3 Stent selection
The selected stent diameter should be approximately 1-2 mm larger than the desired diameter of the
esophagus [3]. The selected stent should also be at least 4-5 cm longer than the length of the to be treated
area [13]. Braided stents shorten, whereas non-braided stents maintain their initial length.
As previously mentioned, comparison between different stent designs is not straightforward, which
complicates a correct stent selection. There is no specific stent design that performs best for all the
different possible pathologies together. In practice, the gastro-enterologist mostly makes decisions based on
the needed diameter and length, whereas the clinician often just decides to use those stents he is used to
work with or that are left in stock [23].
1.2.4 Technique of insertion
Insertion techniques have evolved considerably since the first rigid esophageal stents, which were inserted
into the patient by means of oral pulsion or an open traction technique (requiring laparotomy and
gastrostomy). The development of flexible fiber optic endoscopy in particular boosted the evolution of the
insertion techniques.
In general, current esophageal stents are inserted via the following procedure: first of all, the clinician has to
measure and mark the to be treated zone to know which dimensions are needed and to select a suited
stent. This marking can be done by fluoroscopy and endoscopy. The stents are subsequently deployed from
a stiff or flexible guidewire (dependent on the stent design) using fluoroscopic and sometimes endoscopic
control. For the non-metal Polyflex stents (SEPS), barium is impregnated into the proximal, distal and
midpoints of the stent to facilitate fluoroscopic placement. Some stent designs are deployed by pulling a
constraining sheath (e.g. Wallflex) or coiled thread (e.g. older Ultraflex) from around the folded stent. This
is mostly done starting deployment and fixation from the distal end, but according to clinicians [23], it can
sometimes be more advantageous to have a stent with a proximal to distal release, e.g. for upper esophageal
diseases where the accuracy of the placement of the proximal margin of the stent is more important than
the distal margin. Other designs use a single long constraining suture that needs to be unwound for stent
deployment. For some stent designs a complete delivery system (which is variably rigid) could be developed
for stent deployment (see Figure 1-15). Cook Medical even developed a delivery system with controlled
release and recapturability for their Evolution stent, which is depicted in Figure 1-16. The delivery system of
the only marketed SEPS, the Polyflex stent, is rather bulky, measuring 12-14 mm prior to placement. This
often leads to a necessary dilation of the stricture before stent placement. Sutures or ‘lasso-loop’-purse
strings are incorporated in some stent designs to facilitate stent repositioning or retrieval. A grasping
forceps or a standard polypectomy snare can grasp this suture then. The option to reconstrain during
placement (e.g. Wallflex: up to 75%) makes it easier for the clinician to reposition a semi-deployed stent,
but not every stent design is capable of this.

Introduction 18
Figure 1-15. Delivery system Ella Stents Figure 1-16. Cook Medical’s Evolution® esophageal stent
delivery system
1.2.5 Complications
Complications of esophageal stenting are linked to a myriad of factors such as the type of pathology, the
location that needs to be treated, the presence or absence of a fistula or tumor, the possible concomitant
chemotherapy, the diameter of the stent or the design of the stent [13][39][40][41][42][43]. Due to this,
the ideal stent which can be used for all indications has not yet been designed. If we subdivide the
complications according to their time of occurrence, we distinguish immediate, early and late complications.
Immediate complications involve technical failure, aspiration, stent dislodgement, perforation, airway
impediment and procedure-related mortality. Due to the development of fiber optic endoscopy and newer
esophageal stents, the incidence of these complications has thoroughly decreased, with frequencies mostly
under 1% and have thus become very rare. In the first weeks after stent placement, some patients complain
about chest pain (12-14%) which is more common with larger and more flared stents. Patients can also
suffer from nausea (5-10%) or internal bleeding (3-8%). The group of late complications contains the most
common problem for esophageal stents : stent migration. Uncovered stents (only migrate 0-6% of the time)
have the benefit of easier mucosal ingrowth but also allow tumor and tissue ingrowth (for UC stents: 17-
36% and PC stents: 0-5%) which can cause new dysphagia. Partially covered stents are better protected
against tissue overgrowth but migrated in 25-32% of the cases. Fistulization or perforation occurred in 2.8%
of the cases, bleeding in 3-8% and acid regurgitation in 3.7% of the cases.

Introduction 19
Dealing with peristalsis is also one of the most challenging problems in stent design and to date patients still
need to be educated on following a soft diet combined with abundant fluid consumption.
1.2.6 The future
A lot of improvements to the stent design can still be made. The general goal in the design of new
esophageal stents is to manufacture a stent that is able to remain at its fixed location. Stent migration should
be avoided and major complications (§ 1.2.5) might be significantly reduced using well-engineered stent
designs. Easy deployment, limited tumor or tissue ingrowth and overgrowth, minimal discomfort,
removability if needed, allowing normal peristalsis and so on: the ideal stent has not been developed yet!
However, possible solutions to overcome the challenges in esophageal stent design have been proposed
[13]:
For stents that need to be left in place for a long period, the double stent design (cf. the Niti-S
stent) could form a good solution to withstand migration.
A stent that has to be removed within a certain time after deployment should avoid tissue ingrowth
which might be solved via a combination of fully covered esophageal stents with full-thickness
sutures at the proximal end. Biodegradable stents can also be developed for temporary esophageal
stenting (§ 1.3.1).
Plastic stents cause less tissue damage but display excessive radial forces. Here, a hybrid stent could
represent an option by combining the advantages of both SEPS and SEMS. Hypertrophic granulation
at the flared ends of SEMS can be prevented by designing stents with plastic ends and a nitinol body.
Drug-eluting stents or radiation-emitting esophageal stents are still considered science-fiction as
little research has been done on this topic. They could however bring a solution to tumor ingrowth
or overgrowth and pain management by the incorporation of analgesics.
1.3 Biodegradable esophageal stents
Although biodegradable stents have long been proposed and discussed, only one stent design has made it
to the market in Europe and Asia, being the Ella-BD stent (Ella-CS). Biodegradable stents occupy a separate
niche in esophageal stent treatment.
1.3.1 Biodegradable esophageal stents niche
In general, the major advantages of biodegradable stents are that serious long-term complications are
avoided and removal is not required, which avoids further surgeries and potential morbidity. For these
reasons, biodegradable stents could open up the list of esophageal stenting indications without increasing
migration risks and removal procedure complications. As for BDES tissue ingrowth is allowed because the
stent does not need to be removed surgically afterwards, migration problems are also avoided. These stents
have gained interest during the last few years as they might provide for a prolonged dilatory effect before
being absorbed and progressively degraded. The gradual degradation of these stents can be used to
administer drugs to the tissue in a constant and well-controlled manner. Due to the fact that the
degradation and thus the loss of mechanical strength of the stent is a gradual process, a smooth transition of

Introduction 20
forces on the esophageal wall is ensured. The stent doesn’t form an obstacle in later endoscopic procedures
either as it totally degrades.
As mentioned in §1.2.1.2, benign esophageal strictures can originate from several disorders. E.g. caustic
ingestion, esophageal surgery and radiotherapy can lead to a constriction of the esophageal lumen.
Concomitant dysphagia caused by these strictures severely diminishes the quality of life for the patient and
leads to malnutrition, weight loss, aspiration, etc. The standard treatment for these patients is to use
bougies or balloons to endoscopically dilate the lesion. However, for 10% of these patients [4], endoscopic
dilation will not sufficiently relieve the dysphagia and related complications. Those patients suffer from
refractory benign esophageal strictures (RBES, section 1.2.1.2.1). Removable SEMS have been proposed for
these patients but the tissue ingrowth and the hyperplastic tissue reaction lead to an excessively high rate of
major complications upon stent removal, e.g. perforation or obstruction. Using SEPS for these patients also
showed severe complications. Biodegradable stents could represent a more favorable solution and can thus
be used as an alternative treatment to repeated balloon dilatation of benign esophageal strictures (including
peptic, anastomotic and caustic) and achalasia that are refractory to standard therapy.
In case of esophageal ruptures, perforations or fistula, BDES can be considered a promising treatment
modality. Surgery showed high morbidity and mortality rates and the complications of stenting treatments
for these conditions (bleeding, stent-related strictures, tissue ingrowth, fistula formation and migration) can
be significantly constrained by using self-degrading stents because they avoid any removal procedure. A
BDES can get totally substituted by tissue, hereby bridging the period our body needs to heal itself.
For patients suffering from achalasia, temporary esophageal stenting can also be considered an alternative
for standard treatments, for which BDES could be used.
1.3.2 Biodegradable materials
Biodegradable materials are able to chemically degrade or decompose within a specific time period. Once
implanted, the material is supposed to maintain its mechanical properties as long as needed. Afterwards, it is
absorbed and excreted by the body. Both the mechanical properties and the time of degradation of the
material must match the needs of the application.
The idea of biodegradable stents has existed since the dawn of stenting procedures, but only recently these
stents became a real option due to the development of specific biodegradable materials. A division into two
groups can be made: magnesium alloys and synthetic polymers. The magnesium alloys based biodegradable
materials mainly contain magnesium, zinc, lithium, aluminium and calcium. These alloys show a high
biocompatibility, do not cause artifacts during CT- or MR-Imaging and can be used for cardiovascular stents
and for orthopedic applications (screws, pins, rods, …). For esophageal stenting however they are not the
preferred material as they corrode very fast. These stents degrade typically in one to two months, which is
considered too short for the esophageal stenting indications mentioned in the previous section. The most
important class of biodegradable polymers that can be used for biodegradable polymer stenting are the
biodegradable polyesters. Poly-lactic acid (PLA), poly-glycolic acid (PGA), poly-ε-caprolactone (PCL), poly(-
p-)dioxanone (PDS) and poly-lactide-co-glycolide degrade slower than magnesium alloys. These polymers do
not present themselves as a foreign body because no adverse immunological responses occur. The
prerequisites for biocompatibility (e.g. non-toxigenic, non-cancerogenic, non-mutagenic, non-allergenic, free

Introduction 21
from contaminants, bioresorbable, free from contaminants) are fulfilled [44]. They can easily be processed,
chemically and physically surface-treated and can form a matrix in which cells or biomolecules get
immobilized (options for drug elution). These advantages have attracted considerable attention for use in
biomedical applications. A lot of research has already been devoted to these materials and the list of their
biomedical applications has become immense, ranging from medical devices to tissue engineering, gene
delivery, drug delivery & controlled release, bioseperation and diagnostics [45]. During the 1960s, the
development of biodegradable sutures made from PLA, PGA and/or PCL started the spread of synthetic
biodegradable polymers in medical devices. In the field of stenting, biodegradable synthetic polymers are
mostly used for drug eluting stents, which are nowadays a default treatment for patients with coronary
artery disease. The polymers are applied as a degrading stent-coating with the drugs immobilized in it. The
degradation speed, which can be predicted [46] or pre-tested experimentally, controls the drug release
over time. Apart from stent coatings, these polyesters can also be used to produce fully biodegradable
stents. Dependent on the degradation mechanism and the biocompatibility, biopolymers are classified in
four different classes: biodegradable, bioresorbable, bioerodible and bioabsorbable polymers. Although often
used together in literature, these different terminologies have slightly different meanings, see Table 1-4.
Table 1-4. Clarification of terminology and their definitions with respect to the breakdown of synthetic polymers [47].
Terminology Definition
Biodegradable
For polymeric systems that undergo macromolecular breakdown with dispersion in vivo, but
without proof of its elimination. (Excludes biodegradation by environmental, fungi or bacterial
means). The polymeric systems are degenerated by attacks by biological elements. The formed
waste products can be removed from the degradation spot but not necessarily out of the body.
Bioresorbable For polymeric systems which degrade in the bulk of the material while in vivo and are further
resorbed by the natural metabolism for total elimination.
Bioabsorbable For polymeric systems that dissolve in the presence of body fluids without chain cleavage and
changes in molecular mass.
Bioerodible For polymeric systems which experience degradation on their material surface. Degradation
products are also removed by biological mechanisms.
Once a stent made of one of these polymers is placed in the body, the human physiological medium
(extracellular H2O) provides appropriate conditions for hydrolytic degradation processes [48]. These
processes break down the polymers resulting into low molecular weight species, which can easily be
metabolized or absorbed by the body and eliminated without toxicity. More information is given in §2.2.2.
Figure 1-17. The Ella-BD stent

Introduction 22
1.3.3 Ella-BD stent
The Ella-BD stent is the only biodegradable esophageal stent that is currently marketed in Europe and Asia
(see Figure 1-17) [13]. The manufacturer (Ella-CS) promises [49] a maintained stent integrity and radial
force up to 6 to 8 weeks after stent deployment. 11 to 12 weeks post stent insertion, the stent should be
completely disintegrated. However, the degradation process might be accelerated due to acid reflux (low
pH).
The Ella-BD biodegradable esophageal stent is made of one long single braided wire made of poly-p-
dioxanone, a colorless, crystalline, biodegradable synthetic polymer. This polymer belongs to the class of
biodegradable polyesters of which examples were already given in the previous section. Radio-opaque gold
markers at each end of the stent and at the mid-point are integrated in the stent design, which allows,
according to the manufacturer, an excellent visualization and precise stent positioning (using fluoroscopy).
Migration rates are reduced by the dual flared design. The stent is deliverable with stent diameters of 18, 20,
23 and 25mm (flare diameters 23, 25, 28 and 31mm respectively). Available stent lengths are 6, 8, 10 and
13.5 cm. The stent has to be manually preloaded onto the delivery system prior to advancement over a
0.035mm guidewire. This preloading is explained in detail in the Instructions for Use, as it is no
straightforward task. A specific compression tool facilitates this procedure however (see Figure 1-18). A
specific pull delivery system is designed to make the stent insertion easy for the clinician. The delivery
system can be safely removed once the stent is deployed (see Figure 1-15).
Figure 1-18. Components delivery system Ella-BD Stent

Introduction 23
A clinical trial on the Ella BD stent conducted by Cook Medical in Belgium, the Netherlands, Spain, Italy and
the United Kingdom, has been started in January 2012 and is estimated to end in August 2014.
1.3.4 Limitations
The general complaint heard about the now-marketed Ella-BD stent is that the radial force which the stent
can exert is insufficient [23]. Also the fact that the stent needs to be preloaded prior to use is not ideal, as
is the fluoroscopic visibility during stent deployment. The radio-opacity needs to be improved to really
attain the excellent visualization and precise stent positioning promised by the manufacturer.
1.4 Challenges
The design of a good biodegradable esophageal stent accounts for a combination of both chemical as
mechanical aspects. To ensure that the designed biodegradable esophageal stent is able to adequately dilate
the constricted esophagus, both the mechanical and the chemical behavior of these stents have to be
studied.
In §1.3.2, biodegradable polymers were chosen as the preferred material for biodegradable esophageal
stents. Wires made of polymer-monofilaments get interlaced in specific cris-cross patterns to form a
tubular, three-dimensional textile structure. Braided wire stents can be considered as a subclass of all self-
expendable endoprostheses and can be used in several body passages (e.g. the cardiovascular,
gastrointestinal and respiratory system). Biodegradable polymers are only a part of the wide range of
materials from which braided wire stents can be produced (e.g. phynox, nitinol, …)
Most of the stents described in §1.2.2 are examples of these braided stents and have passed a lot of
promising studies (e.g. [21],[27],[19],[34],[36], …). Despite the promising clinical outcomes, most of these
studies also mention the need for further research as many drawbacks are still observed (§1.2.5). Being able
to predict the mechanical behavior of these stents based on design, geometry and material properties
however would be very beneficial in the design process. Major costs would be saved as the development
cycle and the amount of in-vitro testing is significantly reduced. Jedwab and Clerk [50] proposed a
mathematical model of a self-expanding metallic wire stent, based on Wahl’s spring theory [51]. Based on
the theory of slender rods, Wang and Ravi-Chander [52] developed a mathematically rigorous model
describing the in §1.2.2.2.4 described Wallstent’s response to internal and external loading conditions. Canic
et al. performed an analytical study on the mechanical properties of the bare-metal Wallstent and AneuRX
stent grafts [53]. All the results obtained in these models were validated with experimental data and show
excellent results.
Although the analytical models are capable of predicting the mechanical properties of a specific geometry,
design and material combination, it is difficult to correlate these properties to the actual behavior of such
stents in patient-specific anatomical geometries. Numerical models should form an essential tool in the
design process of these braided stents. Strangely, little literature is dedicated to the numerical simulation of
the mechanical behavior of braided wire stents. The same can be said on the amount of engineering studies
on their behavior.

Introduction 24
At the University of Ghent, a theoretical and numerical framework has been developed to study the
mechanical behavior of braided wire stents under complex (though realistic) loading conditions [54][55]. De
Beule et. al focused their work on the mechanical behavior of the Urolume stent, a nitinol-based urethral
stent used to relieve urinary obstructions. An analytical model based on the mechanical springs theory of
Wahl [51] as was suggested by Jedwab and Clerk [50], was proposed and compared to both experiments as
the results of the study in the developed numerical framework. As both the analytical and the numerical
model were in very close agreement to the experimental results, validation of the models was assured. Both
models were then applied in a virtual optimization procedure [55], automatically adjusting the reference
Urolume geometry reducing the foreshortening while maintaining the required radial stiffness.
Jedwab and Clark’s analytical model is thus proven to be valid for metallic braided wire stents (e.g. Wallstent,
Polyflex, Evolution, SX-Ella HV, etc.) but it appears to be inapplicable to biodegradable polymeric braided wire
stents. Their model is namely based on the following assumptions: the stent fibers behave indepently of each
other (no friction nor steric obstruction), the fibers are not free to rotate, no plastic deformation of the
fibers occurs and the stent’s diameter is sufficiently larger than the fiber diameter. Steric interaction
between the small fibers of metallic braided wire stents is very minimal, but for polymeric fibers this effect is
not negligible, as shown by Nuutinen and Clerk [56].
As analytical models developed for braided wire stents are proven to be incapable of capturing the
mechanics of biodegradable polymeric braided stents, a numerical model needs to be developed. A
numerical framework for biodegradable polymeric stents can provide useful information about their
mechanical behavior, which can improve the clinical outcomes by optimizing the design (as was done by De
Beule et al. for the Urolume stent). The challenge in developing a numerical framework is to incorporate the
steric interaction and friction between the stent wires. This numerical model should overcome the limits of
analytical modeling and in-vitro testing in the design procedure of biodegradable polymeric braided wire
stents (BDPBWS). Eventually, the goal of the numerical model is to be able to simulate stent unfolding and
the degradation process within patient-specific anatomical geometries.
In this study, the choice is made to create a finite element model of the biodegradable polymeric wire stent
as this is currently an accepted aspect of the design process for new biomedical stent devices. To date,
regulatory agencies, such as the Food and Drug Administration office, even require detailed stress analyzes
before approval [57]. Finite element modeling is the recommended way to investigate the stent behavior
during crimping onto the guidewire and deployment into the esophagus given the high amount of
uncertainties in the specifics of these processes. It is considered the most valuable method for design
sensitivity studies and optimization procedures of the mechanical behavior of stents.

Introduction 25
1.5 Goal
The goal of this thesis is to conquer the contemporary limits of designing biodegradable polymeric braided
wire stents. The insights obtained in this study about the degradation and material properties of the single
biodegradable esophageal stent that is already marketed, will be exploited to make concrete propositions
for an improved stent design, both on the chemical as the mechanical level. As no applicable analytical nor
numerical model exists up till now, such a numerical framework will be developed and tested in a basic
model of the human esophagus. This will boost the insights in the chemical and mechanical behavior and will
hopefully be of great use in further design and optimization procedures.
In this dissertation, focus will lie on application in the constricted esophagus but the numerical framework
will be extendable to (biodegradable) polymeric braided wire stents in general.
1.6 Outline
First of all, the degradation mechanism will be studied in Chapter 2. Since only one biodegradable
esophageal stent is marketed up till now (in Europe, not approved by FDA (yet)), we will use this Ella BD
stent as a basis throughout this dissertation. To get an idea of the degradation rate and its influence on the
mechanical properties, stent degradation studies were performed. The radial force and stiffness of the stent
wires are followed throughout a degradation testing process. On the chemical level, a comparison between
the performed study on Ella BD stent wires and a study on polydioxanone biodegradable sutures has been
performed. The degradation mechanism is used to interpret the obtained results in the performed
mechanical tests. A side-note is made on the consequences the acquired insights of the degradation
mechanism might have on constitutive models for polymers undergoing deformation induced-degradation.
Some possible improvements to the contemporary design are proposed at the end of this chapter.
As was mentioned before, a numerical framework for (biodegradable) polymeric braided wire stents would
mean a big support in the design process of new BDPBWS. Numerical models for braided wire stents have
been developed before, but the steric interaction and friction between wires of polymeric braided wire
stents was never incorporated into these models. A numerical model with the steric interaction and friction
between wires incorporated in it is developed in Chapter 3. First, a (parametric) geometrical model of the
Ella-BD wire stent is constructed in pyFormex, an at bioMMeda (Ghent University) developed script-based
geometrical and finite element preprocessor. Specific preprocessing Python scripts transform the
geometrical model automatically into a finite element model. These preprocessing scripts define the material
properties, the elements, the boundary conditions and load cases of the model. As some parameters, such
as the actual friction coefficient between the stent wires, are (almost) impossible to measure in an
experimental setting, these parameters are fitted onto the results of the experiments that were conducted
in the previous chapter. The created finite element model is then analyzed and solved using the commercial
finite element solver ABAQUS. Three methods to simulate the steric interaction and friction between the
wires are proposed and two of them are studied. The results of each method is compared to the
experimental results and the best fit is used for the final numerical model.
In Chapter 4, the obtained numerical model of a (biodegradable) polymeric braided wire stent is used in a
study on its mechanical behavior in the human esophagus. A geometrical model is again developed in

Introduction 26
pyFormex and by preprocessing scripts turned into a basic, but within this setting sufficiently correct, finite
element model of an esophagus with a stenosis in it. Then, the stent will be crimped and deployed in exactly
the same way as it is done in gastroenterological practice. This full esophageal stent deployment FEM allows
us to get an idea about the ability of the stent to open up a stenosis, about which forces are exerted on the
esophageal wall, about the transversal resistance against migration of the stent etc. By imposing the varying
elastic modulus obtained in the degradation studies in Chapter 2, the evolution of this ability, forces,
pressures and resistance can be studied throughout the degradation process, as will be shown.
Chapter 5 concludes this dissertation and gives a sneak peek on what the future might have to offer.

Chapter 2
Degradation studies
As the biodegradable esophageal stent has to bear the intraluminal pressure created by the stenosis and has
to cope with the peristaltic contractions to move food boli down towards the stomach, the stent needs to
exert sufficient radial force to keep the lumen opened and keep its position within the esophagus. This
renders it important to investigate the radial force and circumferential strength of BDES during the
degradation process.
2.1 Mechanical degradation
One of the key design parameters for self-expanding stents is that they provide enough radial force to open
up and/or maintain the conduit’s lumen opened. The radial compression test is one of the frequently
performed tests to assess the stent’s mechanical performance and gives us information regarding the forces
and stresses the stent is able to exert on the lumen wall. Another important property that is needed to
develop a numerical framework is the stiffness of the polymeric braided wires, which is determined via
tensile testing.
2.1.1 Radial compression test
There are numerous testing methods possible to perform a compression test on stents (see Figure 2-1).
One can place the stent between two blocks with both a semi-cylindrical groove incorporated in it and
record the forces exerted by the stent when the two blocks get pushed together [58]. Stents can also be
tested by compressing them between two parallel plates, between an L-shaped (90°) corner and a second
parallel block [59] or between a V-shaped (90°) lower plate and flat upper plate [60]. One can also wrap a
collar around the stent to measure radial compression [61][56].
In this study, a radial compression measurement system from MPT Europe was used (Figure 2-2) as this
method provides much more realistic results to the in vivo situation than the before described conventional
flat plate or V-block methods do. This radial compression method is also recommended by the FDA to test
radial stiffness and strength.
Both ends of this radial compression measurement system were fixed into an Instron tensile testing machine
(Instron 5944 Single Column Tabletop System for Low-Force Universal Testing, capacity 2kN). A load cell
with a capacity of 50N was used and the crosshead speed was set to 25 mm/min (Figure 2-3).

Degradation studies 28
Figure 2-1. Conventional experimental methods to determine stent radial strength: (A) blocks with semi-cylindrical groove, (B)
parallel plates, (C) plates at a 90± angle, (D) collar and (E) V-shaped and flat plate [56].
Figure 2-2. MPT Europe's stent compression unit Figure 2-3. Compression test setup (Instron + MPT SCU)

Degradation studies 29
Figure 2-4. MPT SCU detail
The MPT stent compressing unit (SCU) is controlled by an axial shaft. By pulling out the shaft, a unique
crimping head consisting of 8 segments closes down radially without leaving any open gaps (Figure 2-4). To
correlate the measured forces to radial compression, the tensile force output from the Instron testing
machine has to be processed. First of all, the combination of the SCU with the Instron testing machine has
to be calibrated. The axial extension of the Instron machine can be linked to the radial diameter of the SCU
by measuring the axial extension while the SCU is contacting with rigid cylinders of different diameter. An
easy linear relationship between the axial extension and the SCU diameter can be derived:
2-1
in which E is the axial extension, D is the diameter, a is a dimensionless linear coefficient and b an off-set
coefficient with the same dimension as the extension (mm). In most cases the dimensionless linear
coefficient a varied around a value of 1.6, while coefficient b depends on where the zero extension point
was set. Applying the calculated coefficients and the formula to the instantaneous extension values delivers
the instantaneous diameter values of the SCU. This formula can be implemented in the Bluehill® 3 Software
for Instron’s mechanical testing instruments to directly link the extension to the SCU diameter.
The axial force which has to be applied on the shaft to close the SCU to a certain diameter and open it up
again, is not equal to the radial force which is applied on the clamped stent. This becomes clear when you
apply the theory of virtual work [62]. This theory states that the work of a force acting on a particle as it
moves along a displacement will be different for different displacements. The system in this setting is
considered to be in static equilibrium. The principle of virtual work then states that the virtual work of all
applied forces is zero. Thus,
2-2
in which W is the virtual work and r the radius coupled to the radial force applied on the stent. This leads to
2-3

Degradation studies 30
(
)
which results in
2-4
On average, this leads to a radial force which is the measured axial force ( being ). The
accurate a values are used in the actual force calculations.
The stent compression test is programmed in the Bluehill® 3 Software package. The maximal diameter of
the MPT SCU is about 25mm so to be safe and to avoid damage to the testing machines, the starting
diameter is set to 24mm. With an axial crosshead speed of 25 mm/min, the stent is compressed to a
diameter of 10mm after which the SCU will open again till the initial diameter of 24mm is reached. Due to
the fact that the MPT SCU in the bioMMeda lab (Ghent University) is only about 60mm deep, the test will
be performed in two stages, one half of the stent first, the other half afterwards (Figure 2-5).
Figure 2-5. Stent compression test, conducted in the bioMMeda lab
Before starting the stent compression tests, we have to account for the internal friction inside the MPT
SCU. This is done by going through the radial compression loop 24mm-10mm-24mm without the stent
loaded inside the SCU. This is done two times before stent side A is tested (empty1 and empty2) and then
one time in between the radial compression test of side A and B (empty3), see Graph 2-1.

Degradation studies 31
Graph 2-1. Internal friction MPT Europe's stent compression unit
Stent compression tests were performed on a non-degraded Ella BD-stent with dimensions
⁄⁄ (lot n° S12000470-000002 – fabricated June 2012). The results of the measured
radial forces of each stent-half can be seen in Graph 2-2.
Graph 2-2. Stent compression test non-degraded Ella BD 25⁄20⁄25 x100mm stent (without correction SCU friction)
To correct for the before-mentioned internal friction of the SCU, the average loads of the empty
compression tests in Graph 2-1 are subtracted from the average loads of the stent compression tests in
Graph 2-2. The result of this subtraction is depicted in Graph 2-3.
-10
-5
0
5
10
15
20
25
8 10 12 14 16 18 20 22 24 26
Rad
ial
load
(N
)
Diameter (mm)
Empty 1
Empty 2
Empty 3
-20
-10
0
10
20
30
40
50
60
70
80
90
8 10 12 14 16 18 20 22 24 26
Rad
ial
load
(N
)
Diameter (mm)
A-side
B-side

Degradation studies 32
Graph 2-3. Stent compression test non-degraded Ella BD 25⁄20⁄25 x100mm stent (correction SCU friction)
Yet another correction has to be made though. As the stent is compressed radially, it exerts forces on the
SCU, which causes extra friction within the device. So there is another friction correction to be made:
2-5
In which is the friction coefficient between the SCU segments and in the SCU device in general. This
friction coefficient has to be estimated and is set equal to 0.2. During compression, the radial stent force
is thus overestimated (+) while it is underestimated (-) during expansion. This results in:
2-6
Applying this last friction correction results in Graph 2-4. This graph still does not depict the actual radial
force only, because the before-made estimation that the friction coefficient in the device remains constant is
not correct. It can be reasoned that the internal SCU friction will augment when the 8 segments are more
in contact for smaller diameters, which can also be seen with the increasing internal friction in Graph 2-1.
Although this effect is known, it is hard to account for in yet another correction. This effect is kept in mind
however. For Graph 2-4, this means that the exponential rise of the radial force with ever decreasing
diameter is an overestimation of the radial force.
As can clearly be seen in Graph 2-4, the friction between the braided polymeric wires causes a distinctive
hysteresis effect on the radial force of the stent. During loading, 24mm→10mm, more radial force is needed
to shrink the stent down to a lower diameter than the radial force exerted by the stent during unloading,
10mm→24mm. Chapter 3 focuses on incorporating this frictional effect into the constructed numerical
models. As was mentioned before, it is almost impossible to measure friction between the wires in
experimental settings. For that reason the results of this experimentally conducted compression test are
0
10
20
30
40
50
60
8 10 12 14 16 18 20 22 24 26
Rad
ial
load
(N
)
Diameter (mm)

Degradation studies 33
very important as the results of the developed finite elements models will be fitted to them to accomplish
correct friction modeling.
Graph 2-4. Stent compression test for the non-degraded Ella BD 25⁄20⁄25 x100mm stent (double friction correction)
2.1.2 Tensile test
The radial force of the Ella BD stent has already been studied experimentally. The strength of the separated
wire is another unknown parameter. As these kinds of stents are designed to be used only in elastic regime,
tensile tests are conducted to determine the elastic modulus of these wires. Polydioxanone probably is not
correctly described by a linear elastic material model. A viscoelastic model will be better, but long-term
effects are invisible in very short tensile tests. For polymers, which behave mechanically totally different than
metals, the test conditions are very important. Their measured behavior depends on the temperature, the
load rate and the chemical environment.
Figure 2-6. Isolating a wire from the Ella BD ⁄⁄ stent
0
5
10
15
20
25
30
35
40
45
50
8 10 12 14 16 18 20 22 24 26
Rad
ial
load
(N
)
Diameter (mm)

Degradation studies 34
The wire was collected from an Ella BD stent with dimensions ⁄⁄ (Figure 2-6) which
was produced in the same batch as the stent used in the compression test (lot n° S12000470-000001 –
fabricated June 2012).
To test the wire, the same Instron tensile testing machine as the one used in the compression test was
employed (Instron 5944 Single Column Tabletop System for Low-Force Universal Testing, capacity 2kN). A
load cell with a capacity of 50N was used and the crosshead speed was set to 25 mm/min. The wire was
pinned to the load cell with the use of pneumatic grips. This was not the ideal grip, as Instron also has
specific textile, cord and yarn grips [63]. These grips were unavailable in the bioMMeda lab however. Due to
the same reason, the tests were also conducted without an extensometer. This can lead to some erroneous
results.
Figure 2-7. Tensile testing wire from the Ella BD ⁄⁄ stent
The tensile test procedure is programmed in the Bluehill® 3 Software and the raw data is outputted in an
axial load vs extension format. These loads and extensions are transformed into engineering stress and
strain, with the use of the diameter of the wires (to calculate the cross-sectional area) and the initial wire
sample length that is clamped into the Instron testing machine ( ⁄ ) respectively. To avoid pre-test
breaking of the wires, there was no prestress applied. The stress build-up before linear elastic stretching is
neglected in the data. The results of the tensile test on 3 wires isolated from the non-degraded Ella BD
⁄⁄ stent are depicted in Graph 2-5.
The before-mentioned and -expected errors can be observed in Graph 2-5. If we take sample 2 as an
example, the small plateau-steps in the stress-strain curve are caused by discontinuous slipping of the wire
through the used pneumatic grips. The associated little drop in axial force and extension induce the
discontinuous results in the stress-strain curve. In sample 1, the wire sample is even continuously slipping.
Close attention during the experiment was given to the wire sample and the grips to make sure that no
conclusions were made on tensile tests of slipping wires.

Degradation studies 35
Graph 2-5. Tensile test results separated wire samples from the non-degraded Ella BD ⁄⁄ stent
From the stress-strain curve, one can easily determine the elastic modulus of the wires, the results are
summarized in Table 2-1. Sample 1 results are not considered for determining the Young’s modulus due to
the before-mentioned continuous slipping.
Table 2-1. Young's Modulus results tensile test wire samples from the non-degraded Ella BD ⁄⁄ stent
Young's Modulus E
(N/mm²)
Sample 2 420,19
Sample 3 492,87
Sample 4 509,13
Average 474,0633333
2.1.3 Degradation conditions
To study the degradation process though time, the Ella BD 25⁄20⁄25 x100mm stent and wires from the Ella
BD 31⁄25⁄31 x100mm stent are placed in a pH phosphate buffer solution (PBS) (10mM, based on
hydrogenated sodium phosphate, Na2HPO4 2H2O, and di-hydrogenated potassium phosphate, KH2PO4),
with an initial pH of 7.2. This PBS is used as the hydrolysis medium in which the polydioxanone degrades.
Both the wires and the stent are placed in a thermostatic bath (Julabo, model SW22, Figure 2-8) at a
temperature corresponding to the human body temperature (37°C). Every week, the stent and 3 wire
samples are taken out of the incubator and tested following the same test protocols as described in §2.1.1
and §2.1.2. These tests are performed as long as the stent and the wires have not become too fragile for
testing.
-5
0
5
10
15
20
25
30
35
40
45
50
0.00 0.05 0.10 0.15 0.20
Str
ess
(N
/mm
²)
Strain (-)
Sample 1
Sample 2
Sample 3
Sample 4

Degradation studies 36
Figure 2-8. Experiment preparations
2.1.4 Radial force during degradation
Approximately every week, a similar compression test as the one in §2.1.1 has been conducted. The results
are depicted in two separate figures, for clarity and because two separate degradation stages are observed.
Graph 2-6 depicts the radial force results during the first degradation phase and Graph 2-7 during the
second phase.
Graph 2-6. Radial force degradation Ella BD 25⁄20⁄25 x100mm stent (first phase)
During the first degradation phase, week-by-week the stent gets stiffer and ever-stronger radial forces are
measured during the compression test (Table 2-2). From day 35 on, the second degradation phase is
started, with ever-decreasing radial forces of the stent (Table 2-2). During the compression test on day 63
(week 9), the already damaged (due to compression test in week 8) stent broke into two pieces. The stent
had become too fragile for further testing (see Figure 2-9).
-10
0
10
20
30
40
50
60
70
80
90
100
8 10 12 14 16 18 20 22 24
Rad
ial
load
(N
)
Diameter (mm)
Degradation day 0
Degradation day 7
Degradation day 14
Degradation day 23
Degradation day 35

Degradation studies 37
Graph 2-7. Radial force degradation Ella BD 25⁄20⁄25 x100mm stent (second phase)
Figure 2-9. Stent damage during radial force degradation experiment (top: week 8, bottom: week 9)
-10
0
10
20
30
40
50
60
70
80
8 10 12 14 16 18 20 22 24
Lo
ad
(N
)
Diameter (mm)
Degradation day 37
Degradation day 48
Degradation day 56
Degradation day 63

Degradation studies 38
Table 2-2. Maximal measures loads compression tests during degradation
Max Load (N)
Degradation day 0 46.04278
Degradation day 7 72.65958
Degradation day 14 85.44323
Degradation day 23 75.37885
Degradation day 35 79.49633
Degradation day 37 70.7796
Degradation day 48 63.6469
Degradation day 56 21.73307
Degradation day 63 13.58009
2.1.5 Stiffness during degradation
Every week, tensile tests on 3 wire samples originally isolated from the Ella BD ⁄⁄ stent
were conducted. The same protocol as in §2.1.2 was followed and results are depicted in Graph 2-8.
Graph 2-8. Stiffness during degradation wires Ella BD 31⁄(25⁄31) x100mm stent
Again, two degradation phases are observed. Initially the wires get stiffer during the first 5 weeks, after
which the stiffness decreases rapidly.
As mentioned in §1.3.3, the manufacturer promises 6 to 8 weeks maintained integrity and radial force. The
performed in vitro experiments cannot counter this statement but it has to be noted that during the
performed experiments the stent was not subjected to pH fluctuations or constant varying peristaltic
pressure, which also has an influence on the degradation speed (§2.3). Enzymatic degradation can also take
place in reality but is not accounted for in this in vitro setting. It will appear however in §2.2 that
degradation is governed by hydrolytic cleaving. In the field of clinical practice, insufficient integrity time has
been reported [23].
As was mentioned before, no extensometer was available in the bioMMeda lab. During the first and the
second tensile test, slipping of the wires through the clamps was observed and the value of the measured
Young’s Modulus is probably incorrect. From week 2 on, rougher clamps were used to avoid this slipping.
0
100
200
300
400
500
600
700
800
900
0 7 14 23 35 37 48 56
Yo
un
g's
Mo
du
lus
(N/m
m²)
Degradation day

Degradation studies 39
Based on literature [48][64] and correct values from degradation day 14 on, the correct Young’s Modulus
for degradation day 0 and 7 is estimated to be respectively and . The corrected
stiffness evolution is depicted in Graph 2-9.
Graph 2-9. Corrected stiffness during degradation wires Ella BD 31⁄(25⁄31) x100mm stent
2.2 Chemical degradation
To understand the results obtained in the previous section, the chemical aspects of the degradation of
polydioxanone have to be understood. As the non-enzymatic degradation of polyesters in an aqueous
environment is governed by the hydrolysis of the ester compounds, Sabino et al. [48] conducted research
on the degradation of polydioxanone PDS. In that assay, degradation studies were conducted on
polydioxanone sutures fabricated by Ethicon (PPDX II-0, Ref. Gl 9686). Acid-catalyzed hydrolytic
degradation was found to be the main degradation mechanism for PDS in the in vitro environment (pH=7.4
PBS). Li et al. [64] performed a study investigating the physical and mechanical changes of PDS and weft-
knitted PDS intestinal stents during degradation in a simulated intestinal environment (pH=6.8). Both studies
are interesting to gain insight in the chemical behavior of PDS. Apart from the hydrolytic degradation in
vitro, it has to be kept in mind that in vivo, enzymatic degradation also takes place.
In this section, the material polydioxanone will first be described followed by the chemical degradation
mechanism. Correlation of our studies with these other performed studies will be the subject of §2.2.3.
2.2.1 Polydioxanone
As was mentioned in §1.3.3, poly(-p-)dioxanone is used for the Ella BD stent. This polyester is one of the
possible bioresorbable aliphatic polymers that are often used in medical applications nowadays. PDS has
received the approval of the Food and Drug Administration (FDA) to be used as a suture material and is
currently considered as the standard biodegradable suture material. For sutures, this material is stated to
have a better flexibility and slower general degradation than PGA and PLLA [48]. Appropriate absorption
rate, suitable biocompatibility and minimal inflammatory response is mentioned too [64]. These proclaimed
0
100
200
300
400
500
600
700
800
900
0 7 14 23 35 37 48 56
Yo
un
g's
Mo
du
lus
(N/m
m²)
Degradation day

Degradation studies 40
advantages were probably the reason for Ella-CS, the company that developed the Ella BD stent, to use PDS
for their biodegradable esophageal stents.
Polydioxanone is a colorless, semicrystalline, biodegradable synthetic polymer. This polymer is colored
blue/violet to increase the endoscopic visibility of the stent during deployment in the gastro-intestinal
lumen. PDS, a polymer of repeating p-dioxanone monomer units, is typically synthesized by a ring-opening
polymerization. By heating in the presence of an organometallic catalyst (e.g. zirconium acetylacetone or
zinc L-lactate), ring opening of the cyclic monomers occurs and the polymerization takes place as indicated
in Figure 2-10.
Figure 2-10. The conventional synthesis of poly(-p-)dioxanone
Conventionally, three different fabrication methods can be used to fabricate woven polymeric stents, i.e.
braiding, weft knitting and warp knitting. Ella-CS chose for the braiding technique. The PDS wires
manufacturing method used at Ella-CS is a trade secret of course, but probably consists of an extrusion
immediately followed by a drawing process to create a self-reinforced structure. In this drawing process, the
isotropic polymer is then transformed into a highly anisotropic self-reinforced structure with a high degree
of molecular orientation in the fiber’s long axis direction [56].
2.2.2 Degradation mechanism
The most aliphatic polyesters, such as polydioxanone, can undergo two types of degradation, hydrolytic and
enzymatic. Hydrolytic degradation will mainly take place in the bulk of the material because the diffusion of
water in the bulk of these polyesters is much faster than the hydrolytic degradation reaction [46]. Enzymatic
degradation favors surface erosion [47]. In general, hydrolytic degradation will prevail for aliphatic
polyesters in the esophagus. Due to the fact that the stent and the stent wires in §2.1.3 were degraded in a
PBS buffer (without enzymes), this is also the only degradation process that was studied in this dissertation.
Following the results of the study performed by Sabino et al., the degradation process of polydioxanone
monofilaments occurs in two steps. During the first phase, random chain scission of the ester groups in the
material bulk via hydrolysis takes place. The hydrolysis mechanism proposed in literature [65] is depicted in
Figure 2-11. The amorphous regions are affected first due to the typical looser packing in these zones. The
ester bonds in these regions are more exposed as the water molecules can infiltrate easier there. Ester
bonds are cleaved from the polymeric backbone which shortens the chain lengths. As these cleaved chains
can rearrange within the polymer structure, this can lead to a more ordered packing that maintains or
increases the level of crystallinity.

Degradation studies 41
Figure 2-11. Scheme for the hydrolysis process of an aliphatic polyester like PDS in an aqueous medium such as PBS. [48]
In the second instance, the remaining molecular chains are attacked randomly over their length generating
smaller and smaller molecular chains. As more molecules break down, small molecular pieces can diffuse out
of the stent which causes a decrease of the overall stent weight (documented in [48],[66] and [64]). As the
remainder of the initial large polymers from the first phase of degradation is hydrolytically cleaved into ever
smaller particles, this leads to a decrease in stiffness and strength of the total polymer. The entire
degradation mechanism is depicted in Figure 2-12.
The degradation rate is thus controlled by the molecular weight, the crystallinity and for aliphatic polyesters
in general by the type of functional groups which are present along the polymer backbone. An example can
be seen with PCL, which degrades slower than PDS due to the more hydrophobic backbone of PCL (less
ester groups).
Figure 2-12. Degradation mechanism [64]
Now that we have acquired insight in the degradation mechanism, we can explain the results obtained in the
mechanical degradation section (§2.1). Both the stiffness and radial force exerted by the stent initially
increased, and decreased after day 35. The increase is linked to the before-mentioned chain cleaving in

Degradation studies 42
amorphous polymer regions and rearrangement of the cleaved chains in a more crystalline and thus stiffer
and stronger total polymer. During the second phase of degradation, the random attacks shorten the chains
more and more leading to a decrease in physical integrity and consequently a reduction of its mechanical
integrity. Similar trends were seen in [48] and [64].
2.2.3 Degradation experiments
As mentioned before, Sabino et al. [48] studied the hydrolytic degradation of polydioxanone sutures
fabricated by Ethicon (PPDX II-0, Ref. Gl 9686). Aiming to correlate the results of that study with the
mechanical degradation results performed throughout this thesis, Ethicon was contacted to obtain exactly
the same PPDX II-0 sutures. As Sabino’s study was conducted in 2000, Ethicon does no longer produce the
sutures with this specific reference, but they could however provide the analogous PDS*II sutures with
reference Z303. According to Ethicon, exactly the same starting polymer is still used.
Making correlations between results obtained in one setting, with results from a study obtained in another
setting however, is almost impossible. Too many parameters have an influence on the obtained mechanical
test data. The mechanical testing protocol for instance, can significantly influence the results. The crosshead
speed for example was different. And although the sutures were also kept in a pH buffer to study the
degradation, other environmental factors can also have influence on the results.
Another fact that makes correlating nearly impossible is that we are not sure if it is indeed the exact same
product that Ethicon offered us. First of all, even if we got exactly the same product, we still do not have
the sutures coming from the same batch as those in 2000, which already influences the results. The
molecular weight and crystallinity can be compared but the processing procedure of the polymer into
monofilament wires can have totally changed throughout the years as well. During processing, which
consists of an extrusion immediately followed by a drawing process (§2.2.1), polymer degradation can
already take place to some extent because of the heating step. It is very well possible that Ethicon improved
the procedure to minimalize this degradation.
To get insight and be able to make correlations between different results, access to the detailed procedures
and applied protocol is needed. This information is a protected trade secret, so another option is to set up
a polymer analysis in which the production, processing and degradation is studied. Polydioxanone can then,
for example, be produced in different molecular weights to study the effect of this change on the mechanical
and degradation behavior. The possible degradation or other changes (reorganization, recrystallization) that
occur during a certain processing technique can also be studied by running TGA- (degradation,
thermostability, …), DSC- (Tg, recrystallization, postcuring, …) and GPC-tests (molecular weight, …) just
prior to the processing step and directly afterwards. Only such a study allows the characterization of
parameters influencing the polymer’s mechanical behavior such as molecular weight, fiber packing,
crystallinity, … Such a study falls out of the scope of this dissertation but is certainly very interesting. It can
be of use in improving the mechanical behavior of polydioxanone stents such as the Ella BD or to assess the
limits of this polymer w.r.t. other aliphatic polyesters.
Although correlation with the study of Sabino et al. [48] or of Li et al. [64] is impossible, it still remains
interesting to run DSC-analyzes on the PDS*II suture from Ethicon and both non- and 10 weeks-degraded
wire samples of the Ella BD stent. To run a DSC analysis, a TGA analysis has to be run first to determine

Degradation studies 43
the degradation temperature. Initially, the goal was also to run GPC (Gel Permeation Chromatography) and
NMR (Nuclear Magnetic Resonance) analyzes to determine the molecular weight distribution and the
structure of the different samples. Solving the samples in deuterated chloroform, the typically used NMR
solvent for polydioxanone, didn’t succeed however. The solvent mentioned in the polymer handbook for
this polydioxanone, dichloromethane, was not able to dissolve the samples either. Possibly, the used
polymer for the PDS*II suture and Ella BD stent wires has a crosslinked structure, rather than a linear one.
All the analysis results were obtained with help from the Polymer Chemistry and Biomaterials Group of
Ghent University.
2.2.3.1 Thermogravimetric analysis
A thermal gravimetric analysis (TGA) was run on the PDS*II suture from Ethicon and both non- and 10
weeks-degraded wire samples of the Ella BD stent. This analysis is used to determine the maximum
temperature before the sample starts to degrade, which is needed as the maximum temperature input of
the DSC analyzes. These TGA analyzes were run on a Q50-model of TA Instruments according to a
protocol where the temperature was first equilibrated at 30.0°C and the sample was subsequently heated at
a rate of 10.0°C per minute up to 800°C. The results of the three analyzes are listed in Table 2-3 and an
example of the results of such an analysis is shown in Graph 2-10.
Table 2-3. Results TGA analyzes
Non-degraded Degraded PDS*II - Z303
Mass (mg) 13.6410 9.5750 4.2140
1% weight loss temperature (°C) 188.00 137.00 169.00
Onset temperature (°C) 286.20 245.55 269.20
Total weight loss temperature (°C) 304.19 281.30 291.56
Residue (mg) at 600°C 0.02131 0.02553 0.01966
Similar graphs were obtained for the three different samples, which informs us that the wires from the Ella
BD stent and the PDS*II-Z303 sutures exist of solely one organic component, polydioxanone, as no steps or
plateaus in the TGA are seen. All lost weight at 600°C is classified as organic content (the polymer), while
the remaining residue above this temperature is classified as inorganic content (e.g. mineral dyes, fillers). All
TGA temperatures are quite similar for the three samples, considering that the lower 1% weight loss and
onset temperature of the degraded sample can be due to some water molecules that were still left in the
sample as the samples were only patted dry before testing.

Degradation studies 44
Graph 2-10. Results TGA degraded wire sample Ella BD stent
2.2.3.2 Differential Scanning Calorimetry
A DSC analysis is a thermo-analytical technique that provides qualitative and quantitative information about
physical and chemical changes that involve endothermic or exothermic processes or changes in heat
capacity using minimal amounts of sample material. In DSC, the measuring principle is to compare the
amount of heat required to increase or decrease the temperature of a sample and a reference when it is
heated or cooled at the same rate as a function of temperature. In other words, while heating or cooling
the sample and the reference, no difference in heat flow will be measured as long as no thermal transition is
taking place. In case such a transition in the sample occurs, heat will be absorbed (endo) or released (exo)
by the sample and this event causes a change in the differential heat flow which is then recorded as a peak.
As the Cp value before and after the glass-transition is different, this transition is seen as a jump in the
baseline. Information on melting, (re-)crystallization, degree of crystallinity, glass transition temperature,
post-curing and so on can be deducted from these analyzes.
It can be noted that although the TGA proposes one component in the samples, polydioxanone normally,
that color additives are added to the starting polymer. These additives are probably added in such a small
amount that they are not visible in the TGA. The blue/violet color is added, as was mentioned before, to
increase visibility for the surgeon or the gastro-enterologist. These additives can be of organic or inorganic
nature. Organic low molecular-weight additives have an influence on the glass temperature as they can act
like plasticizers within the polymer structure.
DSC analyzes were run and the results are depicted in Graph 2-11, Graph 2-12, Graph 2-13 and Table 2-4.
During these analyzes, the samples were heated two times because only during the second heating, samples
can be compared as they then have the same thermal history. The first heating is thus used to delete each
sample’s different thermal history. This is done by heating the sample up to 130°C (10°C/min) after

Degradation studies 45
temperature equilibration at 40°C. Isothermal conditions at 130°C are kept for 3 minutes, marking the end
of the first heating procedure. The sample is then cooled down to -50°C at -10°C per minute and then kept
isothermal for 5 minutes. The sample is then heated again to 130°C (10°C/min) for the 2nd heating. Graph
2-11, Graph 2-12 and Graph 2-13 depict the results measured during the second heating cycle.
Table 2-4. Results DSC analyzes
Non-degraded Degraded PDS*II - Z303
Mass (mg) 6.5000 7.4000 1.3000
Glass transition temperature (Tg) (°C) -10.97 -17.33 -10.49
Melting energy (J/g) 66.98 87.30 51.33
Melting onset1 temperature (°C) 97.57 96.16 97.33
Melting peak temperature (°C) 107.63 104.29 104.40
Graph 2-11. DSC analysis non-degraded wire sample Ella BD stent
After a first heating, it can be noticed that during the controlled cooling (10°C/min), the nondegraded wire
sample crystallizes in two different crystal structures (two endothermal peaks during cooling, Graph 2-11).
During a secondary heating, a recrystallization occurs just prior to melt, in which less perfect crystals
probably are transformed in more perfect crystals, so eventually only one melt peak is noticed.
1 The melting onset temperature is difficult to indicate cause (re)crystallization occurs just prior to the melt. This
renders an accurate integration of the melt peak impossible.

Degradation studies 46
Graph 2-12. DSC analysis degraded wire sample Ella BD stent
For the degraded wire (Graph 2-12), only one crystallization peak is measured during the controlled
heating. Also now, during the second heating, just prior to melting, an exothermal process is measured. This
can be a re- or postcrystallization. Two melting peaks are measured, in which less perfect crystals (possibly
formed just before melting) will melt first. Although a lower crystallinity is expected with the lower
molecular weight due to degradation, a higher crystallinity is recorded.
It is clear when comparing Graph 2-11 and Graph 2-12 that the degradation has altered the crystal
structure of the wires. With the original, non-degraded Ella BD wire, two recrystallization peaks were
recorded, while the degraded wire shows only one recrystallization peak. In the non-degraded wire, two
crystal structures are probably present with less and more perfect crystals. The degradation mechanism
causes the crystal structures to change and only one homogeneous crystal structure eventually remains.
Similar conclusions have been made by Sabino et al. [48].
The DSC analysis of the Ethicon PDS*II-Z303 sutures shows almost no recrystallization during controlled
cooling (Graph 2-13). In contrast to the wires from the Ella BD stent, cold crystallization occurs during the
second heating. Just prior to melting, similarly as is the case for the Ella BD stent wires, recrystallization
occurs and finally one melting peak is recorded. These PDS*II-Z303 generally shows a lower crystallinity
compared to the Ella BD stent wires. Similar energy, melting and recrystallization temperatures are
recorded though.

Degradation studies 47
Graph 2-13. DSC analysis non-degraded PDS*II-Z303 suture
2.2.3.3 Post analysis
In §2.2.1, the presumption was uttered that Ella-CS used a similar polydioxanone polymer as the PDS
typically used in biodegradable sutures. With the performed analyzes, this presumption can still be valid, but
the crystal structure is clearly different however. Although GPC or NMR analyzes could confirm or
contradict this presumption, solvent problems made these analyzes impossible during this thesis.
As was mentioned before, making other correlations between the mechanical behavior of the Ella BD stent
and the mechanical behavior of the PDS sutures in the study of Sabino et al. is impossible. A proper
chemical analysis procedure is a logic next step to determine the ideal polymer, polymerization technique,
molecular weight, …
2.3 Fit in constitutive model
A theoretical framework for the degradation of these biodegradable polymers has been developed by
Soares et al. [67] in 2008 and was applied in a numerical model of a real stent geometry by Debusschere,
Nic in 2011 [46]. In this constitutive model, a scalar field
( ) 2-7
is introduced, reflecting the local state of degradation (x represents the location in the polymer, t the time
and d varies between 0, non-degraded state, and 1, totally degraded state). As several studies (Miller &
Williams 1984, Chu 1985, Zhong 1993, da Silva Soares 2008) showed that mechanical deformation induces
faster degradation, the degradation rate is defined by

Degradation studies 48
( ) 2-8
with F representing the deformation gradient and σ the internal stresses. Then, this framework assumes the
degradation speed to decrease directly proportional to the decreasing degradation.
( ) ( ) 2-9
The stress state is in its turn also dependent on the degradation and deformation state.
( ) 2-10
When assuming degradation of a linear isotropic material, this can be imposed into the model by letting the
Young’s modulus depend on the degradation state by a parameter β.
( ) ( ) 2-11
The assumed inverse first-order kinetics of the degradation parameter d cannot be used considering the
degradation mechanism that was seen in the previous section. To develop a correct constitutive model for
the degradation of polydioxanone wires, the relation between time t, the scalar degradation parameter d
and the elastic modulus have to be fitted by other equations than those assumed by Soares et al. As too
little data has been collected to perform such an equation fitting in this study, it is considered beyond the
scope of this thesis. Creating a sufficiently correct numerical framework with degradation mechanics
incorporated in it, is future work to be done.
2.4 Improving the used biodegradable polymer
A full chemical analysis of the polymerization, processing technique, packing, … could help in the
development of a better BDES. For example, one of the complaints (§1.3.4) of the Ella BD stent is that in
some case they degraded too fast. Recently, it has been shown that synthesizing poly(dioxanone-b-
caprolactone) co-polymers (PDOCLs) can allow the manufacturer to control the degradation time by
adjusting the DO/CL ratio of the co-polymers (increasing CL composition leads to slower degradation rate)
[68].
Table 2-5. Possible biodegradable stent materials and their mechanical properties
Young’s
Modulus (GPa)
Tensile Strength
(GPa)
Degradation Time
(months)
Poly(L-lactide) 3.1-3.7 60-70 24+
Poly(D-lactide) 3.1-3.7 45-55 12-16
Polyglycolide 6.5-7.0 90-110 6-12
50/50 poly(DL-lactide/glycolide) 3.4-3.8 40-50 1-2
82/18 poly(L-lactide/glycolide) 3.3-3.5 60-70 12-18
70/30 poly(L-lactide/ε-caprolactone) 0.2-0.4 18-22 12-24
Magnesium alloy 40-45 220-330 1-3

Degradation studies 49
Next to PDS, many other aliphatic polyesters can be considered as possible materials for biodegradable
(esophageal) stenting. As long as the biocompatible, mechanical, geometrical and absorption rate
requirements can be met by these polymers, they can be used to develop biodegradable esophageal stents.
Some of these polyesters are currently used or have been used in clinical trials [69]. A list of some different
polyesters and their mechanical characteristics is given in Table 2-5.
Other combinations than those mentioned in Table 2-5 are possible and the production process can be
manipulated to attain polymers with favorable molecular weight and crystallinity, thus fine-tuning the
stiffness, the strength and the degradation time of the stent. In that way, the complaints of insufficient radial
forces or premature degradation can be tackled.
Another proposition can be made to improve the visibility of the stent during deployment. According to
some clinicians, the gold markers at the stent’s ends are insufficient for a good visualization of the stent
during deployment. Prof. G. Dorta [23] proposed to incorporate more of these markers on the stent, but
there are other options. The first proposition that can be made is to add a radiopaque additive into the
polymer itself. A typical example of such an additive is BaSO4 powder (particle size ranging between 1 and
10 µm, 20 wt%). As long as the polymer processing techniques allow mixing of this BaSO4 powder in the
polymer melt without destabilizing the polymer’s structure, this can easily be done. Such a large amount of
micro-sized particles can deteriorate the strength of the polymer or can migrate to the surface during
processing however, so caution is necessary. As this BaSO4 can leach out of the polymer during
degradation, biocompatibility has to be checked. From a physical and biological standpoint, tricalcium
phosphate for example is another radiopaque inorganic filler showing better biocompatibility [70]. To avoid
leaching, the radiopaque agent can also be covalently coupled to the polymer backbone. A second option is
to incorporate other radiopaque contrast agents that can render higher contrast with smaller size particles,
e.g. incorporation of gold nanoparticles. Of course, the effect of any modification or additives has to be
extensively studied first.

Chapter 3
Mechanical modeling
In Chapter 2, the mechanical behavior of the Ella BD stent was studied and the degradation mechanism of
aliphatic polyesters in an esophageal environment was explored. The gathered data can now be used to
develop a correct numerical model of these stents. The unknown friction between the wires will be fitted
onto the results of the conducted compression tests of the previous chapter.
First, a geometric model of the studied stent is developed in pyFormex. With the help of a developed
preprocessing script, this geometric model is then transformed into a finite element model ready to be
imported into Abaqus. The performed compression test in the bioMMeda lab will be simulated to the
smallest detail to ensure correct fitting of the unknown friction (coefficient). This results in a correct
numerical model of the (biodegradable) polymeric braided wire stent with the steric interaction and friction
incorporated in it.
Figure 3-1. Flowchart of the development of the numerical framework for BDPBWS.
3.1 Geometric modeling
As was stated before, few literature has been dedicated to the simulation of the mechanical behavior of self-
expandable braided wire stents. This can be partially linked to the fact that building a correct geometrical
model of these stents is no easy task.
Before a geometrical model can be made, the correct element type to be used for the finite element model
has to be chosen as this is of uttermost importance during the development of a geometric model. Hall and
Kasper [57] compared various methodologies to analyze typical biomedical stent devices within a finite
element setting. Comparing the use of the following elements,
C3D8: 8-node linear hexahedral solid element.
C3D8R: 8-node linear hexahedral solid element with reduced integration and hourglass stabilization.
C3D8I: 8-node linear hexahedral incompatible mode solid element.
S4: 4-node linear quadrilateral shell element with 5 integration points through the thickness.
pyFormex preprocessing
• Geometry (De, fD, L, fL, d, nx, β, ds)
•Material (E,ν)
•Friction (µ, κ)
•Boundary conditions
Abaqus processing
• Calculations
• Output generation
Postprocessing & fitting
• Output processing
• Fitting to degradation studies results
Numerical framework

Mechanical modeling 51
S4R: 4-node linear quadrilateral shell element with reduced integration and 5 integration points
through the thickness.
B31: 2-node Timoshenko beam element with 5×5 cross section integration points.
the B31 elements appear to be the best choice to have a computationally efficient model with regard to
problem size, time and memory requirements, without losing accuracy in predicting stress and strain. The
most efficient methodology for the numerical analysis of stent deployment is stated to be the use of beam
elements in conjunction with contact surfaces (Hall and Kasper [57]). The results will be similar to those of
a solid continuum element model, with a great gain in computational efficiency. Remember that the scientific
value of a numerical analysis is, and should be, a tool in the development of improved biodegradable
polymeric braided stents in a timely and accurate manner.
Just as was done by De Beule et al. [54], the geometrical modeling in this study is done with the use of
pyFormex, a script-based geometrical and finite element preprocessor [71]. This python based preprocessor,
currently developed at Ghent University by prof. Benedict Verhegghe et al., implements Formex algebra to
generate a whole structure with a limited number of commands. One can start from a single line
(considering the choice of B31 elements was made) and manipulate it into braided wire stents with
translate-, replicate-, scale-, rotate-, coordmodification-, … commands. Virtually, this means that there is
no limitation to what pyFormex can model. Another advantage of this program is that it works
parametrically, which means that one can simply change a few parameters to get a totally different stent
design. This can be of great use when performing optimization procedures (e.g. [55] and §3.3).
To be able to build up a mechanical model of BDPBWS, we have to make the correct link between a model
of the Ella-BD stent and the results of the mechanical tests on this stent. So it is important to build up a
correct geometrical replica of this Ella-BD stent. A condensed script to build a geometrical model of beam
elements of the Urolume stent (WireStent.py) was already available but some extra commands were needed
to create a correct geometrical Ella-BD model. A full step by step explanation of the WireStent.py-script can
be found in [54]. This document gives a short summary of the WireStent.py-script and explains the extra
added command lines to the for this thesis developed BDPBWireStent.py-script in detail.
First of all, the constructor of the FlaredClosedDoubleHelixStent class in the BDPBWireStent.py -script needs
ten arguments:
external diameter of the stent De (mm)
flared external diameter of the stent fD (mm)
stent length L (mm)
length of one of the flares fL (mm)
wire diameter d (mm)
number of wires in one spiral set nx (-)
the pitch angle β ( )
extra (optional) radial distance between the wires ds (mm)
number of elements in a strut nb (-)
false or true value for the connectors parameter
A nearly planar (bumped along the z-axis) base module is used as the smallest element to build up the
braided stent. This base module is used to create a unit cell of the nearly planar braided sheet and the

Mechanical modeling 52
folded wire segments (see §3.1.1). The elementary base module is skewed (shear command) and reflected
(reflect command) to form a unit cell of two crossing wires. This unit cell then is extended with a translated
and mirrored copy. Subsequently, this new extended base module is replicated along both directions of the
base plane to form a planar braided wire sheet. After incorporating the flares (see §3.1.2), the grid is rolled
into a cylindrical stent structure.
To create a perfect geometrical copy of the Ella-BD stent, the following parameters need to be set:
Table 3-1. Geometrical modeling parameters Ella-BD stent
external diameter of the stent De 20 mm
flared external diameter of the stent fD 25 mm
stent length L 100 mm
length of one of the flares fL 20 mm
wire diameter d 0.650 mm
number of wires in one spiral set nx 18
the pitch angle β 30°
extra (optional) radial distance between the wires ds 0.0
number of elements in a strut nb 2
3.1.1 Creating the bended wire segment
As was stated before (§1.3.3), the Ella-BD stent is constructed from one single long polymeric wire. To
achieve this, the wires have to be folded when reaching the end of the stent grid, which can clearly be seen
in Figure 1-17. To achieve correct simulations of the mechanical behavior of the stent, this feature cannot
be ignored.
(a) (b) (c)
Figure 3-2. Creating a bended wire strut (XZ-view)
The before-mentioned base module consists of a bumped and scaled strut (Figure 3-2a). We start with the
creation of the bended strut BS by mirroring the bumped and scaled base module around the YZ-plane and
then translating the whole unit step in the negative X-direction (Figure 3-2b). Now we have one upward
braiding bend. A fitting downward bend is created by rotating the original full upward bend 180° around and
then reflecting it against the XY-plane. Before transforming this up- and down-bend into a bend in the XY-
plane, we need to translate them a certain distance in the Y-direction. This distance will serve as the radius
of the XY-plane bend and thus has to match with the distance between the wire-ends which it has to

Mechanical modeling 53
connect (which is equal to two unit steps). A NE and SE strut arrive at their ends in a 45° angle, so the
length of the XY-bend in the X-direction has to be equalized according to the following equation
( ) ( ) √ 3-1
The up- and down- XZ-bend thus has to be translated in the Y-direction over a distance of √ unit steps.
Then the sum of both Y-translated XZ-bends (see Figure 3-2c) can be transformed into cylindrical
coordinates:
The Y-coordinates serve as the radius of the bend
The X-coordinates scaled by ¼ as the theta-coordinates on a quarter of a circle
The Z-coordinates scaled by ½ as the Z-coordinates
of the bended wire segment.
Figure 3-3. Bended wire segment (left: XY view, middle: XZ view, right: iso view)
Script 3-1 summarizes how this bended wire segment is programmed in pyFormex.
1 # a single bumped strut, oriented along the x-axis
2 bump_z=lambda x: 1.-(x/nb)**2
3 base = Formex('l:1').replic(nb,1.0).bump1(2,[0.,0.,dz],bump_z,0)
4 # scale back to size 1.
5 base = base.scale([1./nb,1./nb,1.])
6 # create bended strut (stent ends)
7 BS = base.mirror(0).translate(0,-1.).setProp(4)
8 BS += BS.rotate(180.,2).reflect(2)
9 BS = BS.translate(1,-sqrt(2.)).cylindrical([1,0,2],[1.,90./4,0.5]).rotate(90.,2).translate(0,2.)
Script 3-1. Implementation of the bended wire segment
3.1.2 Creating the flares
Skipping a few steps (see step-by-step script development in [54]), a full planar braided wire sheet, with
closed ends in this setting, is built up. To avoid migration, the longitudinal ends of these polymeric braided
wire stents are flared. Thanks to the flare()-functionality in the Formex class, implementing these flares into
the geometrical model is an easy task (Figure 3-4 and Script 3-2). This flare(xf, f, dir=[0, 2], end=0, exp=1.0)-
function creates a flare at the end of a Coords block flare by setting 5 parameters: xf is the distance over

Mechanical modeling 54
which the flare has to extend in the setted direction dir[0], f the maximal amplitude in the setted direction
dir[1], end denoting on which side of the Coords block the stent has to be implemented (at the start (end=0)
or end (end=1) and exp the index of the power function describing the curvature of the flare. The set
parameters can be found in Script 3-2.
1 # Implementation of the flares
2 fH = (fD-D)/2
3 F = F.flare(fL,fH,[1,2],0,2)
4 F = F.flare(fL,fH,[1,2],1,2)
Script 3-2. Implentation of the flares
Figure 3-4. Creating the flared nearly planar pattern
3.1.3 Cylindrical stent structure
The final cylindrical stent structure is created by translating the flared nearly planar pattern over the stent
radius in the Z-direction, followed by a cylindrical coordinate transformation with the Z-coordinates as
distance r, the X-coordinates as angle θ and the Y-coordinates as height z and a rescaling to the correct
circumference and length.
The resulting stent geometry is depicted in Figure 3-5.
(a)

Mechanical modeling 55
(b)
(c)
Figure 3-5. Full stent geometry (a: iso view, b: right view, c: front view)
3.1.4 Preprocessing
Once the stent geometry has been created in pyFormex, the geometric model has to be transformed into a
finite element model.
A lot of settings have to be defined when developing a finite element model: material properties, element
type, boundary conditions, load cases, etc. To simplify the process of transforming a geometric model to a
finite element inputfile for Abaqus, the developed BDPBWireStent.py-script is equipped with a whole set of
finite element model building tools. Specific classes are defined to set up parts, sections, orientations,
connectorbehaviors, materials, assemblies, equations, instances and eventually full model input files. Another
option would have been to use the already existing pyFormex libraries to write the Abaqus input file.
3.2 Finite element model
3.2.1 Materials and methods
First of all, the stent is imported from pyFormex. This is done with the use of the defined preprocessing
classes in the BDPBWireStent.py-script (§3.1). All nodes are imported and linked with each other by B31-
elements. These beam elements are set to have a circular profile with radius 0.325 mm (the diameter of the
Ella BD stent wires was measured with a Vernier caliper in the bioMMeda lab). As mentioned in the

Mechanical modeling 56
beginning of this chapter, beam elements are the best choice to study the stent’s mechanical behavior in a
computationally efficient way [57]. The geometric pyFormex model also defined specific connector elements
(no length, ds was set 0.0, see Table 3-1) where the wires of the Ella BD stent cross. The 2plex connector
Formices are defined as CONN3D2-elements. To easily impose boundary conditions or assign section
properties, several node sets on the stent are created as well as beam and connector element sets. The
circumferential mantles of the beam elements are used to define the surface of the stent.
The MPT SCU described in §2.1.1 that was used for the mechanical compression test, consisted of 8 flat
segments which compressed the stent radially, see Figure 2-4. To simulate this test set up, a crimper part
with 8 SFM3D4R-elements (4-node quadrilateral surface elements, reduced integration) was created. (Figure
3-7). The outer cylinder of the octahedral crimper’s cross-section is given an average radius of 15mm to
avoid overclosure problems. The length of the crimper is set equal to the depth of the MPT SCU used in
the bioMMeda lab.
Figure 3-6. The STENT part Figure 3-7. The CRIMPER part
3.2.1.1 Material
Although the MPT SCU is made out of steel, no material model is defined for the crimper. Surface elements
do not require the definition of a material model. The crimper material has no influence on the radial
strength of the stent.
The material ‘PDS’ was defined with results attained from the mechanical tensile test in §2.1.2 and from
literature [56]. The Young’s modulus is set to 690 N/mm², the Poisson ratio to 0.45 and the density to 1400
kg/m³. A lot of polymers show time-dependent material behavior, showing characteristics of both elastic
solids as viscous liquids. For fast deformations however, they behave like linear elastic materials. Because
the deformations during the conducted compression test are relatively fast, the visco-elastic effects are
considered negligible and a linear elastic defined polydioxanone suffices in this setting.
Abaqus neglects the effect of shear stresses due to transverse shear forces at individual material points and
elastic behavior of the section is assumed in transverse shear [72], leading to the relations
3-2

Mechanical modeling 57
where are the transverse shear forces, the transverse shear strains, A the cross-sectional surface, G
the shear modulus (calculated based on the elastic modulus and the Poisson ratio) and the ”slenderness
compensation factor”. This factor is used to prevent the shear stiffness from becoming too big in slender
beams. This slenderness compensation factor can be set in the section definition manually or automatically
calculated by Abaqus based on the length, the cross-sectional surface and the moments of inertia of the
beams. The geometrical model in this setting is not build up out of slender beams, as can be seen in Figure
3-8.
Figure 3-8. Rendered beam thickness detail of the STENT part
A simple calculation shows the influence of correcting for this transverse shear stiffness in this model. The
slenderness compensation factor for first-order Timoshenko beams (B31) is defined as
(
)
3-3
in which x is the amount of compensation the user wants to impose. Filling in the correct length, cross-
sectional area and the moment of inertia of e.g. the red marked beam in Figure 3-8 results in
( ( ) (( ) )
( ( ) )
)
( ) 3-4
The amount of compensation is mostly chosen equal to 0.25, so the influence of slenderness compensation
isn’t so big in this model and thus disabled.
3.2.1.2 Kinematic constraints
The imposition of correct boundary conditions to the model is critical in obtaining an approximate solution
which can accurately capture the behavior of a physical system. It is of uttermost importance to not restrict
the space of solutions because this could induce too stiff responses. By providing only the essential
boundary conditions, rigid body motion in the solution can be avoided and a realistic solution can be
obtained. All boundary conditions are applied in one general cylindrical coordinate system.

Mechanical modeling 58
The stent did not rotate or twist in the MPT SCU during the radial compression test (§2.1.1), so the first
boundary condition forces the stent not to rotate or twist by fixing the θ-degree of freedom of some axi-
symmetric nodes. By only fixing these nodes, the stent remains free to fold up how it does in reality.
It was also noticed during the radial compression test that the Ella BD stent slipped out of the crimper a
little bit. The imposition of a fixation in the Z-direction of some stent nodes at the stent end within the
crimper lead to an exaggeration of this phenomenon. A fixation in the Z-direction in the middle of the stent,
near the edge of the crimper, was considered the most adequate boundary condition.
Two methods can be chosen for the numerical compression load implementation, a force driven or a
displacement driven method. The resulting mechanical stent behavior is independent of the chosen method,
as was shown in [54] for the Urolume stent. The performed compression test in the bioMMeda lab was
displacement driven, so in this setting, the choice is given to a displacement driven numerical load
implementation.
The MPT SCU consisted of eight elements that compressed the stent radially. During the whole
compression, the segments shrank radially holding their combined octahedral shape. It is considered correct
to entirely fix the crimper instance in the θ- and Z-direction and force the radial compression on the stent
by imposing a radially inward displacement of the crimper. This radial displacement has to shrink the stent
to a diameter of 10mm. As the crimper in Abaqus is defined by the diameter of the outer circle and we want
to correlate this to the diameter of the inner circle (stent), a simple trigonometric calculation has to be
made:
(
) ( ) 3-5
This means that an inner octahedron radius of corresponds to an outer octahedron radius of
. To simulate the compression test procedure in §2.1.1, the crimper octahedron, which at the start
of the simulation has an outer radius of , has to be changed to an outer radius of . This
corresponds to a radially inward displacement equal to . This radial displacement is applied in
Step-1 with a smooth step amplitude as depicted in Graph 3-1.
Graph 3-1. Amplitude Step-1
0
0.2
0.4
0.6
0.8
1
0 0.2 0.4 0.6 0.8 1
Am
plitu
de
Time (s)

Mechanical modeling 59
3.2.1.3 Steric interaction and friction
To model the contact between the stent and the crimper, the choice for a general contact or a surface-to-
surface contact can be made. The general contact method is an automatic treatment algorithm for all node-
to-facet and edge-to-edge interactions of the nodes, facets and contact edges of the default surface [72].
These edge-to-edge interactions are very effective in enforcing contact that cannot be detected as
penetrations of nodes into faces. The general contact method is chosen to avoid overclosure problems.
In literature, no friction data can be found for contact between steel (material MPT SCU segments) and
polydioxanone. Based on general friction coefficients between polymers and steel however, the friction
coefficient is estimated to be around 0.05 [73]. To avoid excessive frictional stick, some fine-tuning on the
initial simulation results will be needed, see §3.2.2.
Two different approaches are tested to model the steric interaction and friction between the wires in this
finite element model. The first approach uses the previously defined connector elements and imposes
specific connector behavior. The second approach suppresses the connector elements and imposes direct
friction and interaction between the wires.
3.2.1.3.1 Hinge connector
During compression or expansion of the BDPBWS, it can be assumed that the cross-points of the wires
stay connected but rotate within the θ-Z-plane. The angle between the wires is initially equal to double the
pitch angle β but as this pitch angle increases during radial compression (or axial elongation), so does the
angle between the connecting wires. This is illustrated in Figure 3-9.
Figure 3-9. Increase in pitch angle during radial compression or axial elongation [54]
To model this assumed connector behavior, a search in the connection-library of Abaqus [72] leads to the
connection type HINGE, which joins the position of two nodes and provides a revolute constraint between
their rotational degrees of freedom. This connection type combines the connection types JOIN and
REVOLUTE.

Mechanical modeling 60
Figure 3-10. Kinematic constraints HINGE connection type
Figure 3-10 summarizes the kinematic constraints linked with this HINGE connection type. The nodes a and
b, each part of one of the crossing wires, are constrained in the u1, u2, u3, ur2 and ur3 directions. The only
available degree of freedom is ur1. The orientation at a and b is defined by use of a cylindrical coordinate
system ORI.
A formal description of the frictional effect in the HINGE connector is given by
( ) 3-6
in which the potential ( ) represents the moment magnitude of the frictional tangential tractions in the
connector in a direction tangent to the cylindrical surface on which contact occurs, is the friction-
producing normal moment on the same cylindrical surface and µ the friction coefficient.
This friction coefficient is the general unknown in this whole study and will have to be fitted to the
experimental radial force graphs produced in §2.1.1 and §2.1.4. The friction-producing normal moment on
the cylindrical surface on which contact occurs is defined by
| | | ( )
| 3-7
in which , the magnitude measure of friction-producing connector elements is defined as
( ) 3-8
which is the sum of an axial moment contribution and a radial&bending-force moment contribution. An axial
force is present between both crossing wires due to the braided structure of the BDPBWS. These forces
however are almost impossible to measure experimentally. is considered as the effective friction arm
associated with the constraint force in the axial direction, which in this setting has no meaning as the
contact surface between both wires is infinitely small (two circular wires pushed on top of one another). As
the force is an unknown, we just define , so the axial force has an influence on the friction in the
HINGE connector. The second term, , is related to friction and bending between the ‘pin and the
sleeve’ of the HINGE connector, but as the wires of the BDPBWS have no other contacts than an axial one,
these frictional terms have to be neglected. This is done by setting and . , a self-
equilibrated internal contact moment of the HINGE connector can also be set to zero in this setting.
The predefined friction parameters that have to be inputted in the friction definition of the HINGE
connector behavior are thus set, leaving the friction coefficient µ the remaining unknown which will be
fitted to the experimentally conducted compression tests in the bioMMeda lab (§2.1.1 and §2.1.4). Due to
some excessive rotation errors that were encountered, a very small amount of linear uncoupled viscous

Mechanical modeling 61
damping with a damping coefficient of 0.001 is imposed on the connector elements. This method can be
used to solve for errors as long as it does not alter the radial force results. This demand is checked by
comparing the internal energy (ALLIE) with the sum of the total energies dissipated by viscous effects in each
stent element (ELVD), see Graph 3-2. Material damping and bulk viscosity are included in these viscous
effects.
Graph 3-2. Damping energy negligible compared to total internal energy
3.2.1.3.2 Revolute + Slide-Plane connector
In the previous section, it was presumed that both nodes of the connector element only rotate relatively to
one another along the radial axis. Relative shifting of both nodes of the connector element in the θ-Z-plane
might however be a possible degree of freedom too.
In that case the assembled JOIN + REVOLUTE = HINGE-connector has to be changed to an assembled SLIDE-
PLANE + REVOLUTE-connector. No specific connector type for this combination is defined within Abaqus,
but we’ll call it an SPR-connector for referencing. An SPR-connector would allow the wires to rotate
relatively (as was the case with the HINGE-connector) and slide (also with some friction) over each other.
Slippage between the wires would thus also be treated with these connectors.
Again, the only unknown in this case is the friction coefficient µ, which can be fitted to the experimentally
conducted compression test in the bioMMeda lab (§2.1.1 and §2.1.4). The study of the capability of this SPR-
connector to capture the mechanical behavior of the BDPBWS falls out of the study scope of this
dissertation but can be considered an interesting alternative connector to investigate.
3.2.1.3.3 Internal self-contact model
Instead of defining an SPR-connector to allow rotation and sliding between the wires, a finite element
model with no connector elements was chosen. The friction and slippage between the stent wires
themselves is modeled by incorporating friction into imposed internal self-contact between the
circumferential surfaces of the stent’s beam elements.
-50
0
50
100
150
200
250
300
350
400
0 0.2 0.4 0.6 0.8 1
En
erg
y (
mJ)
Time (s)
Internal energy Summed viscously dissipated energy

Mechanical modeling 62
For both models, three simulations are run with friction coefficients 0.1, 0.3 and 0.5.
3.2.1.4 Solution technique
ABAQUS includes the ability to solve problems with an implicit or explicit solution technique [72]. Both
techniques use a time integration scheme to solve discrete dynamical equilibrium equations in terms of
displacements, velocities and accelerations. The implicit integration scheme, which is unconditionally stable
independent on the time step size, assumes constant average acceleration over each time step. The
equations are solved by performing a matrix inversion of the structural stiffness matrix. Accelerations and
velocities are calculated and displacements are determined. In the explicit integration schemes, a linear
change of the displacement in each time step is assumed. The governing equations are calculated (no matrix
inversion needed here) and the resulting accelerations and velocities at the end of the considered time step
are calculated. This allows for the calculation of the unknown displacements at the beginning of the time
step. In contrast to the implicit integration scheme, the explicit scheme is only stable for time step sizes
smaller than a critical size evaluated for the analyzed structure, in undamped conditions equal to ⁄ , with
the largest natural circular frequency. As this stable time step size is often a very small value, the
computational cost of these solutions is magnitudes greater than implicit integration solutions. But since no
matrix inversion is required in the explicit solution scheme, it is significantly more efficient.
As the Abaqus/Explicit solver can treat the contact problem between beam elements effectively and is able
to avoid the divergence problems that are due to the contact instability which occurs frequently in
Abaqus/Standard solver, the explicit integration scheme is chosen to solve the FEMs. It is more suited for
quasi-static problems, especially those involving extremely complex contact conditions.
Initially, during the development of this finite element model, implicit solutions were still possible, but the
limits of this solution technique were reached from the moment the contact between the stent and the
crimper or the friction in the connector elements was imposed. Further FEM development was done with
the explicit integration scheme.
3.2.2 Fine-tuning
3.2.2.1 Friction modeling
Modeling the friction in a correct way is essential to come to a correct numerical model fitting of the
friction between the wires. To model the friction between the stent wires and the crimper, and between
the stent wires mutually, the basic Coulomb friction model in Abaqus/Explicit is used. In this model, two
contacting surfaces can carry shear stresses up to a certain magnitude across their interface before they
start sliding relative to one another. This state is known as ‘sticking’. This critical shear stress, at which
sliding starts, is defined as a fraction of the contact pressure p between the surfaces. This fraction is known
as the coefficient of friction, µ. The Coulomb friction model is depicted in Graph 3-3.

Mechanical modeling 63
Graph 3-3. Slip regions for the basic Coulomb friction model [72]
As is known from Physics, the friction coefficient opposing the initiation of slipping from a sticking condition
is different from the friction coefficient that opposes established slipping. The former is typically described
as the ‘static’ friction coefficient µs, and the latter is referred to as the ‘kinetic’ friction coefficient µk. In most
cases, µs > µk. These friction coefficients can be implemented via the input of slip-rate dependent data,
contact-pressure-dependent data, … or directly via an exponential decay friction model. In this setting
however, such data are not available and the default Coulomb friction model with one general friction
coefficient µ is imposed.
In the first working FEM simulations of the stent compression test performed in the bioMMeda lab, it was
noticed that the ‘stick state’ was too strong. A force peak was seen in the beginning of the compression as
the stent had to start sliding within the CRIMPER. To fine-tune the correct friction between the stent and
the simulated MPT SCU, Abaqus allows the user to define an elastic slip while sticking. The default model
imposes stick till the before-mentioned critical shear stress is reached. Slip can only occur once that critical
shear stress is reached. Tangential softening can however be imposed to allow a certain slip while the shear
stress is building up to its critical value (see Graph 3-4).
Graph 3-4. Elastic slip versus shear traction for sticking and slipping friction [72]
The coefficient κ, which in the default model without tangential softening is set equal to infinity, has to be
defined based on shear stresses and allowed slip. As without this tangential softening, the initial stick friction
in the compression test simulations was too strong, this softening had to be enabled in the imposed friction
model. To get an idea of a value for κ, the simulation was run and the shear stresses were studied. It was
important to study the shear stresses on the moment of initial contact between the stent and the crimper.

Mechanical modeling 64
In Figure 3-11, the maximal contact shear forces at initial contact between stent and crimper are around
. Knowing that these forces initially work on a very small contact surface between crimper and stent,
we can assume this surface to be around . This gives a shear stress of ⁄ . For this shear
stress a slip equal to the diameter of the stent wires can be set: . This leads to for the
tangential softening between the stent and the crimper.
Figure 3-11. Contact shear forces between stent and crimper at the beginning of the stent compression simulation
Between the stent wires reciprocally, the average shear force is approximately (Figure 3-12).
Assuming a contact surface between the wires that is half the size of the cross-sectional area of the wires,
, and again a slip ratio equal to the wire diameter, , leads to for the
tangential softening between the stent wires.
Figure 3-12. Contact shear forces between stent wires reciprocally at the beginning of the stent compression simulation

Mechanical modeling 65
3.2.2.2 Mesh size
The number of elements of a full geometrical stent model can easily be controlled by adjusting the nb
parameter, the number of elements in a strut in the BDPWireStent-script (§3.1). Due to the complex
geometrical model, the length of the stent and the high number of wires in the model, the number of
elements is rather large, see Table 3-2.
Table 3-2. Size geometrical model
nb # beam
elements
# connector
elements
1 7776 1908
2 15552 1908
4 31104 1908
8 62208 1908
(a) (b)
(c) (d)
Figure 3-13. Comparing geometrical model sizes ((a) -model; (b) -model; (c) -model; (d) -model)
The higher the amount of elements, the larger the computational cost. Other geometrical model sizes can
be obtained by remeshing procedures if needed. Due to the extremely high computational cost of the
-models, a mesh sensitivity analysis wasn’t performed but the smallest model with still appropriate

Mechanical modeling 66
geometry was chosen. Figure 3-13 shows the 4 different model sizes listed in Table 3-2. The -models
are too coarse, but the -models are acceptable. Larger models are computationally less interesting.
3.2.2.3 Analysis time – Mass Scaling
The mechanical behavior of the polymeric braided wire stents in this study is static, so the analysis time or
the applied mass scaling has to be chosen in such a way that the kinetic energy of the stent is much smaller
that its potential (strain) energy during deformation analysis. For a quasi-static analysis, Abaqus suggests that
the kinetic energy should not become larger than 5% of the potential (strain) energy. A few preliminary runs
were carried out to ensure this limit is not exceeded, which led to disabled mass scaling and an analysis step
time of 1s. Graph 3-5 depicts the kinetic and potential energies of the model with these settings and would
suggest that the mass scaling can be increased or the analysis time decreased. Doing this however induces
dynamic effects in which the stent starts to oscillate in the z-direction, which has to be avoided during the
simulation.
Graph 3-5. Quasi-static analysis: energy fraction requirement satisfied
3.2.3 Results
The final stent compression test simulations mimic the compression test performed in the bioMMeda lab as
accurately as possible and allow us to determine which finite element model is capable of correctly
simulating the mechanical behavior of biodegradable polymeric braided wire stents with the effect of steric
interaction and friction incorporated in it. As was mentioned before, two different approaches are followed
to simulate this steric interaction and friction between the wires mutually, a model with hinge connectors
and a model without connectors but with imposed internal self-contact between the wires.
-5
0
5
10
15
20
25
30
35
40
0 0.2 0.4 0.6 0.8 1
En
erg
y (
mJ)
Time (s)
Internal energy Kinetic Energy

Mechanical modeling 67
Figure 3-14. Simulation vs experiment
3.2.3.1 Hinge connector model
The created finite element model with imposed hinge connectors was used to simulate the performed stent
compression test at day 35 of the degradation studies. The Young’s Modulus of the wires was set equal to
the measured . The results of these simulations are depicted in Graph 3-6.
Graph 3-6. Simulations stent compression test day 35 - HINGE connector models
The assumption that the cross-points of the wires stay connected and rotate within the θ-Z-plane is clearly
too strict as this makes the simulated stent behave much stiffer than it does in reality. The HINGE
connectors approach did not succeed in incorporating steric interaction and friction in a correct way and
cannot be used to create a correct numerical model to simulate the stent’s mechanical behavior.
-20
0
20
40
60
80
100
120
140
160
8 10 12 14 16 18 20 22 24
Lo
ad
(N
)
Diameter (mm)
experimental FC0.1 FC0.3 FC0.5

Mechanical modeling 68
3.2.3.2 Internal self-contact model
The created finite element model without connector elements but with imposed internal self-contact
between the wires was used to simulate the stent compression test conducted on day 35 of the degradation
studies. The Young’s Modulus of the wires was set equal to the measured . The results of the
simulations are depicted in Graph 3-7.
Graph 3-7. Simulations stent compression test day 35 - Internal self-contact models
Keeping in mind the remark of §2.1.1 on the experimental radial force overestimation for the smaller
diameters, the internal self-contact model seems to be able to capture the mechanical behavior of the stent
quite well. To select the correct friction coefficient between the wires, it is more important to look at the
corresponding behavior at the larger diameters. To validate this chosen model and the choice for a specific
friction coefficient, these internal-friction models are also run for day 0 and day 48 of the degradation
studies. The Young’s moduli are respectively set to and . The results of these
simulations are depicted in Graph 3-8 and Graph 3-9.
The simulation results in the three graphs with friction coefficient 0.1 seem to be in good agreement with
the experimental results, except for the experimentally overestimated small-diameter radial forces. The
friction coefficient heavily influences the hysteretic behavior of the braided polymeric stents. As the friction
coefficient increases, the resistance of the stents against compression increases, as bigger forces need to be
overcome. The hysteresis itself however seems to be reduced due to reduced slippage between the wires
and thus less energy loss.
To conclude, a numerical framework was developed, which is able to capture the mechanical behavior of
(biodegradable) polymeric braided wire stents. A correct geometrical model, with steric interaction and
friction between the wires incorporated by imposing internal self-contact with friction coefficient
and tangential softening , is able to predict the stiffness of a specific polymeric braided stent design.
-10
0
10
20
30
40
50
60
8 10 12 14 16 18 20 22 24
Lo
ad
(N
)
Diameter (mm)
experimental FC 0.1 FC 0.3 FC 0.5

Mechanical modeling 69
Graph 3-8. Simulations stent compression test day 0 - Internal self-contact models
Graph 3-9. Simulations stent compression test day 48 - Internal self-contact models
3.3 Design optimization
Now that the numerical framework is developed, the influence of altering the stent design can be studied
quite easily and the design can be almost automatically optimized. An inherent feature of script-based
modeling is the possibility to easily adapt a design and create variations on it. This is a huge advantage for
conducting parametric analyzes. By altering a simple design parameter, the geometrical model can instantly
be remodeled again. Abaqus then calculates the stresses, strains, … and postprocessing scripts are capable
0
5
10
15
20
25
30
35
40
45
50
8 10 12 14 16 18 20 22 24
Lo
ad
(N
)
Diameter (mm)
experimental FC 0.1 FC 0.3 FC 0.5
-5
0
5
10
15
20
25
30
35
40
45
50
8 10 12 14 16 18 20 22 24
Lo
ad
(N
)
Diameter (mm)
experimental FC 0.1 FC 0.3 FC 0.5

Mechanical modeling 70
to process the output, compare this output to the optimization goal and adapt the geometrical design
parameters for a new optimization iteration. Such a virtual optimization procedure was conducted by De
Beule et al. [55] for metallic braided wire stents and can now easily be extended to (biodegradable)
polymeric braided wire stents (Figure 3-15).
Figure 3-15. Flowchart of De Beule's optimization modeling strategy [54]
Such a complete optimization procedure has not been conducted in this study but as an example, the
influence of the pitch angle and the number of wires upon the stent’s stiffness will be studied in this section.
50mm long stent numerical polymeric braided wire stent models with pitch angles 15°, 30° and 45° and
build up from 12, 15 and 18 wires (Table 3-3) are created and crimped over their total length.
Table 3-3. Design optimization simulations
Simulation code Pitch angle (°) Number of wires
A15 15 12
A30 30 12
A45 45 12
B30 30 14
C30 30 16
The radial forces exerted by the designed stents during simulated compression and expansion tests
(25mm→10mm→25mm) are compared. For these simulated compression and expansion tests, the stent is
shrunk by a radially inward driven cylinder with frictionless contact between the stent and the crimper but
imposed internal self-contact between the wires with friction coefficient and tangential softening
. It will become clear that solely by varying the pitch angle and the number of wires, the
manufacturer already has a lot of control on the radial stiffness of the stent.
pyFormex preprocessing
- Geometry (De,fD,L,fL,d,nx,β,ds) - Material (E,ν) - Friction (µ, κ)
- Boundary conditions
Abaqus processing
- Calculations - Output generation
pyFormex postprocessing
- Output processing
pyFormex iteration
Compare mechanical behavior and factors to be optimized
→ Adapt geometry

Mechanical modeling 71
3.3.1 Pitch angle
To study the effect of altering the pitch angle β, FEM A15, A30 and A45 are compared. Looking at these
stent designs in Figure 3-16, it might seem like design A15 has a lot more wires than A45 for example but
this is not the case. The smaller pitch angle creates a denser structure and more wire length in total is
needed of course. The results of the tested mechanical behavior are depicted in Graph 3-10.
Figure 3-16. Comparison stent designs with pitch angle 15°(left), 30° (middle) and 45° (right) and same number of wires
Graph 3-10. Results comparison stent designs with pitch angles: 15° (A15), 30° (A30) and 45° (A45) – 12 wires each
As can be seen from these results, decreasing the pitch angle increases the stiffness of the stent. The
foreshortening effect of these braided stents however is increased by decreasing the pitch angle.
-5
0
5
10
15
20
25
30
35
8 10 12 14 16 18 20 22 24 26 28
Lo
ad
(N
)
Diameter (mm)
A15 A30 A45

Mechanical modeling 72
3.3.2 Amount of wires
Increasing the amount of longitudinally starting wires, increases the density of the stent structure too. It can
thus be expected that this will increase the radial stiffness, which is also the case (see Graph 3-11).
Figure 3-17. Comparison stent designs with number of wires: 12 (left), 14 (middle) and 16 (right) - constant pitch angle: 30°
Graph 3-11. Results comparison stent designs with number of wires: 12 (A30), 14 (B30) and 16 (C30) - pitch angle: 30°
With a higher number of wires, more wires contact each other too, so the hysteresis effect due to steric
interaction and friction increases too. It can be noted that decreasing the pitch angle had a stronger effect
than increasing the number of wires, but these two design alterations have to be in function of the stent’s
flexibility, the foreshortening, etc. and not only in function of the stent’s radial stiffness.
0
5
10
15
20
25
30
8 10 12 14 16 18 20 22 24 26 28
Rad
ial
load
(N
)
Diameter (mm)
A30 B30 C30

Chapter 4 Esophageal stent expansion simulation
The actual behavior of a stent in a patient-specific anatomical geometry is not easy to assess if just based on
the parameters that can be derived from the (analytical and/or numerical) polymeric braided stent model.
The deployment and expansion of the constricted esophagus by such BDPBWS is therefore simulated in this
chapter with a developed FEM of stent and esophagus. For the stent, the in Chapter 3 developed FEM of an
Ella BD 25⁄20⁄25 x100mm stent is used. The steric interaction and friction is incorporated by imposing
internal self-contact between the wires with the fitted friction coefficient and tangential softening
. The FEM of the constricted esophagus is developed in this chapter.
4.1 Modeling the esophagus
4.1.1 Geometrical model
Next to a parametric geometrical model of the (biodegradable) polymeric braided wire stent, pyFormex can
also be used to build a geometrical model of an esophagus. In this setting, this geometrical model will be
simple though based on realistic geometrical parameters. To simulate the stent’s behavior in a patient-
specific anatomy one can use medical image processing tools (e.g. [74]) to segment 3D medical images (e.g.
MRI, which is suited to image soft tissue) and create highly accurate 3D models of your patient’s anatomy.
As was mentioned before (§1.1), the adult esophagus is a muscular tube of 18 to 26cm long and can be
stretched to diameters of 2 to 3cm when passing a food bolus. Based on anatomical images of Netter
(Figure 1-2 and [1]) the esophageal wall in rest state is about 3-4 mm thick. A stenosis will be incorporated
in the geometrical esophageal model, making it possible to study the stent’s capability of reopening the
constricted esophageal lumen. A stenosis can narrow the esophageal lumen to about 25% of its initial lumen
diameter (Figure 1-3). In practice, when the lumen is constricted too much to be able to pass the guidewire-
loaded-stent through, a balloon dilatation is performed first to dilate the stenosis enough for the loaded
stent to pass. With these considerations made, the geometrically modeled esophagus will have the
dimensions listed in Table 4-1.
Table 4-1. Geometrical parameters modeled esophagus
Outer diameter esophagus 22 mm
Length esophagus 200 mm
Wall thickness esophagus 4 mm
Stricture length 40 mm
Stricture narrowing ratio 0.50

Esophageal stent expansion simulation 74
Ten arguments are defined in the beginning of the class Esophagus in the BDPBWireStent.py-script, being the
outer diameter diam, the total length of the esophagus ltot, the stricture length lstr, the esophageal wall
thickness thic, the narrowing fraction of the lumen caused by the stenosis stri, the number of partitions in
the radial direction nr, the longitudinal direction (normal open-lumen part: nl, constricted part: ns) and the
angular direction na. The esophagus is modeled in Abaqus using 3D solid elements (C3D8R), so for that
reason a simple cube is chosen as the base element. As was the case for the stent, the whole esophagus will
first be modeled as an angular line segment in the X-direction with wall thickness in the Y-direction,
replicated into a nearly planar element grid in the XZ-plane after which it is rolled into a cylindrical
structure by transforming the coordinate system (Script 4-1).
Initially, half a stricture is modeled. The simple cube base element is replicated ns times in the X-direction
and nr times in the Y-direction. Subsequently, the resulting elements are scaled to obtain a line segment
with length 1 in the X-direction and a length equal to the specified wall thickness in the Y-direction. This
scaled line segment is then transformed into a unilateral Y-directed bump according to the function
( ), with s being the calculated stricture ratio. Scaling this bumped line segment to the
length of half a stricture completes the first part of the line segment. One side of the non-constricted part
of the esophagus is modeled by replication and scaling of a simple cubical element again. The full line
segment results from mirroring both stricture and non-stricture halves after correct translations (see Figure
4-1). One line segment counts as one angular segment of the final esophagus, so this segment has to
replicated na times in the Z-direction. This creates the before-mentioned nearly planar grid that was
needed, Figure 4-2. By translating this grid a distance equal to the esophageal radius perpendicularly away
from the XZ-plane and then performing a transformation towards a cylindrical coordinate system, the
geometrical model of the esophagus is finished (Figure 4-3).
Figure 4-1. Angular line segment of modeled esophagus with stenosis
Figure 4-2. Nearly planar grid of modeled esophagus with stenosis
Figure 4-3. Final geometrical model esophagus with stenosis
In Script 4-1, the outer and inner layer of the esophagus are deliberately separated with two property
assignments to be able to make a distinction between the inner mucosal and outer muscular layer later on
for the finite element model (§4.1.2)

Esophageal stent expansion simulation 75
1 class Esophagus(object):
2 # diam = outer diameter
3 # ltot = total length
4 # lstr = stricture length
5 # thic = wall thickness
6 # stri = stricture fraction
7 # nr = radial partition
8 # nl = longitudinal partition
9 # na = angular partition 10
11 def __init__(self,diam,ltot,lstr,thic,stri,p,angle=360.):
12 [nr,nl,na,ns] = p
13 s = 0.5*(diam-2*thic)/thic*stri 14
15 F1a = simple.cuboid().replic2(ns,nr/2).scale([1./ns,thic/nr,1.]).setProp(1)
16 F1b = F1a.translate(1,thic/2).setProp(2)
17 F1 = F1a+F1b
18 F1 = F1.map(lambda x,y,z:[x,y+s*(3*x**2-2*x**3)*y,z]).scale([0.5*lstr,1.,1.])
19 F2a = simple.cuboid().replic2(nl,nr/2).scale([0.5*(ltot-lstr)/(nl),thic/nr,1.]).setProp(1)
20 F2b = F2a.translate(1,thic/2).setProp(2)
21 F2 = F2a+F2b
22 F = (F1+F2.translate(0,-0.5*(ltot-lstr))).translate(0,-0.5*lstr).mirror(0)
23 self.F = F.replic(na,1.,2).translate(1,-0.5*diam).cylindrical([1,2,0],[1.,angle/na,1.]) 24
25 def getFormex(self):
26 return self.F 27
28 def getMesh(self):
29 return correctHexMeshOrientation(self.F.toMesh()) 30
31 def getFusedMesh(self):
32 return mergeMeshes([correctHexMeshOrientation(self.F.toMesh().withProp(1))
33 ,correctHexMeshOrientation(self.F.toMesh().withProp(2))],fuse=True)
Script 4-1. Class Esophagus
4.1.2 Material model
Modeling the esophageal tissue is no straightforward task. Biological tissues can generally be modeled with a
quasi-linear viscoelastic model [75], capable of capturing both the nonlinearity in elasticity (hyperelasticity)
and the temporal behavior (e.g. stress relaxation, creep and hysteresis) of these tissues. The following
equation expresses the stress relaxation behavior of such a QLV model:
( ) ( ) ( ) 4-1
where ( ) is the instantaneous elastic response to a step input of strain and ( ) is the reduced
relaxation function representing the time-dependent stress response normalized by the peak stress at the
time of the step input of strain.

Esophageal stent expansion simulation 76
In this setting, the focus does not lie on the long-term tissue relaxation effects so these long-term effects
can be ignored. This reduces the quasi-linear viscoelastic model to a hyperelastic model described by the
following equation:
( ) ( ) ( ) 4-2
in which m is a linear factor with the same dimension as stress (N/mm²) and n is a non-dimensional
parameter representing the rate of stress stiffening.
The esophagus is of course a highly anisotropic tissue due to variable muscle and collagen fiber orientations
in both the mucosal and the muscle layer. For that reason, the esophagus can be modeled as two separate
layers, each with their own anisotropic material properties. Values for c and d were found in literature
(Table 4-2).
Table 4-2. Material parameters estimated using experimental stress-relaxation curves [75]
Parameters m (MPa) n
Muscle Cir. 0.21 E-3 16.31
Axial 0.65 E-3 20.81
Mucosa Cir. 0.05 E-3 9.01
Axial 0.002 E-3 22.23
In this setting, only the circular material properties are of interest and the esophagus will thus be modeled
in Abaqus as a two-layered homogeneous (circular material properties) hyperelastic material.
It can be noted that the tissue in the stenosis does not totally correspond to this material model. The local
tissue in a stricture is generally stiffer than the normal esophageal tissue and plastic deformation effects
aren’t incorporated. The plastic deformation effect is the most exploited feature in treatment procedures
where the stricture is opened up by repeated balloon or bougie dilatation. As no data on the tissue of
esophageal strictures is available the stricture is modeled as normal hyperelastic esophageal tissue in this
setting. However, the thicker modeled layer will also impose a certain local stiffness of the modeled
esophagus in the stenosis.
4.2 Total deployment and expansion simulation
The FEM simulation consists of two steps, based on the way the Ella BD stent and typically other
(biodegradable polymeric) braided wire stents are inserted into the patient. First, the stent is preloaded
onto an Ultra Stiff guidewire with the use of a delivery system. This allows to position the stent in the
appropriate location before the stent gets gradually released and is allowed to expand freely.
4.2.1 Loading procedure
To load the stent prior to implantation, a very specific procedure has to be followed to correctly shrink the
stent into the sheath of the delivery system. This loading procedure is simplified in Abaqus by implemeting a

Esophageal stent expansion simulation 77
cylindrical surface that makes a frictionless contact with the stent and is able to crimp it to the loading
diameter, which in the case of the Ella BD stent is . This procedure is depicted in Figure 4-4.
Figure 4-4. Loading the stent onto the guidewire
4.2.2 Implantation procedure
The implantation procedure is then simulated by pulling the cylinder back, which is comparable to the
sheath that is pulled back allowing the stent to expand freely while exiting the delivery system. An extra
contact has to be defined in this secondary step between the inner surface of the modeled esophagus and
the circumferential beam surface of the modeled stent. A friction coefficient equal to 0.2 is assumed
between the mucosa and the stent. Figure 4-5 depicts the stent deployment in different steps.
As can be seen in Figure 4-5, the stent has been deployed too fast. This simulation example is kept
deliberately in this report because it shows that caution is needed during stent deployment. If the stent is
released too fast, the last released proximal part of the stent shoots out of the delivering sheath too strong
and the folding pattern of the braided polymer structure is affected. Clinicians have to be aware of this fact,
they are not only responsible for the esophagus but also for the correct and careful implantation without
damaging the stent structure itself.
Although the stenotic tissue wasn’t modeled stiffer than the normal esophageal tissue, an extra stiff effect is
still seen due to the thicker modeled mucosal and muscular layer. In step 3 of Figure 4-5, the stent
temporarily overstretches a bit due to this change in esophageal resistance.

Esophageal stent expansion simulation 78
Figure 4-5. Stent deployment (Y-plane-cut)
4.3 Functioning within esophagus
Now that the stent loading and implantation procedure in the modeled esophagus is totally simulated, a lot
of interesting parameters can easily be studied.
The capability of the stent to open up the lumen for example can readily be consulted. Figure 4-6 shows
how the modeled stent open ups the lumen at different time steps during stent deployment
Figure 4-6. Opening up of the constricted esophageal lumen (Z-plane-cut)

Esophageal stent expansion simulation 79
Another important example is the pressure exerted on the lumen’s wall. This pressure has to be kept
between specific limits. For the esophagus for example, too little radial stiffness and thus too low pressures
on the esophageal wall lead to insufficient opening of the lumen and migration risks while excessive
pressures can lead to chest pain, pressure necrosis, bleeding or even perforation. The developed model
allows us easily to determine which pressures are exerted on the esophageal wall, as depicted in Figure 4-7.
With the geometrical and mechanical parameters set equal to a new, non-degraded Ella BD 25⁄20⁄25
x100mm stent, it can be seen that the maximum pressure exerted on the esophageal wall is focused on the
local stricture zone and reaches pressures up to .
Figure 4-7. Pressure exerted by the stent on the esophageal wall (MPa)
As these stents typically show a big amount of foreshortening, it is not always easy for the clinician to
determine where he has to start deploying the stent. If a patient-specific geometry of the esophagus is
loaded into Abaqus, correct placement can easily be simulated. The best location to start releasing the stent
can be determined before the actual operation.
4.4 Stent degradation
As mentioned in §2.3, a correct constitutive model for the degradation of polydioxanone wires was not
developed due to insufficient experimental data. The stent degradation can however still be studied by
imposing the measured change in elastic modulus throughout time. The obtained elastic moduli of the stent
wires throughout the degradation studies are incorporated in the FEM of the BDPBWS while expanding the
constricted esophagus. As no plastic deformation is incorporated in the esophageal material model, the
evolution of the lumen’s radius depicts the stent’s capability to keep the lumen open. This is depicted in
Graph 4-1 and Figure 4-8. In reality the persistent radial pressure induces a permanent deformation of the
esophageal wall.

Esophageal stent expansion simulation 80
Graph 4-1. Evolution stenosis diameter with stent degradation
Day 0
Day 1
Day 14
Day 56
Figure 4-8. Evolution stenosis diameter with stent degradation
4.5 Future improvements
The developed numerical framework was already partially validated as the model appeared capable of
predicting the stent’s mechanical behavior in different stages of degradation. To fully validate the numerical
model however, other stent designs should be fabricated and their mechanical behavior should be compared
to the numerical predictions.
There is always room for improvement, and this is also the case for the performed simulations in this
dissertation. It would be interesting to implement the degradation behavior of the stent wires in the
simulations. An adaptation of the constitutive degradation model of Soares et al. [67] to the in §2.2.2 studied
degradation mechanism of aliphatic polyesters is needed. Additional experiments have to be conducted to
correlate the time t, the scalar degradation parameter d and the elastic modulus. Relaxation tests have to be
conducted on the wires to measure long-term creep and relaxation in the aliphatic polymer wires.
Implementing a viscoelastic material model would allow for the study of long-term effects. If the long-term
effects of the polymers are implemented, the long-term effects of the esophageal tissue will also have to be
0
1
2
3
4
5
6
7
8
9
0 10 20 30 40 50 60
Inn
er
rad
ius
sten
osi
s (m
m)
Days

Esophageal stent expansion simulation 81
implemented. A quasi-linear viscoelastic material model for the esophagus has been developed already [75]
but the additional stiffness of stenotic esophageal tissue is not incorporated in these models. Further
research and characterization is needed to implement a quasi-linear viscoelastoplastic material model with
locally increased stiffness. For now, linear elastic and hyperelastic material models were imposed on the
polymer wires and the esophageal tissue respectively.

Chapter 5
Conclusions and future prospects
As was seen in the first introductory chapter, a wide variety of esophageal pathologies are considered
treatable by successful temporary esophageal stenting. Partially and fully covered self-expandable metallic
and plastic stents have been developed, but these stents display migration problems, severe complication
rates (perforations, bleeding, chest pain, nausea, fistula, mal-positioning, migration, …) and high morbidity
rates during stent removal. Except for the Polyflex stent, no other SEMS or SEPS have received FDA
approval to be used for benign conditions. Bioresorbable esophageal stents however have the intrinsic
advantage of degrading within the esophagus and thus transcend SEMS or SEPS as no secondary removal
procedure is needed. These biodegradable esophageal stents also suffer less from migration issues as tissue
ingrowth allows for sufficient anchoring of the stent. Bioresorbable esophageal stents form their own niche
in esophageal stenting and are capable of extending the list of indications for esophageal stenting.
The Ella BD stent is the first marketed bioresorbable esophageal stent and clinical trials are ongoing.
However, complaints about insufficient radial force and premature degradation have already been uttered. A
better design is needed and as analytical models appear to be unable to capture the mechanical behavior of
bioresorbable polymeric braided wire stents, a mechanical model for finite element analysis was developed.
The degradation mechanism and its influence upon the mechanical behavior had to be studied first.
Degradation studies were conducted on both the mechanical as the chemical level. It appeared that the
degradation of the typical bioresorbable polymers, i.e. aliphatic polyesters, occurs in two phases. During the
first phase, the amorphous regions are affected and the hydrolytically cleaved chains rearrange so that the
stiffness of the polymers increases. In the second phase, the polyester chains are hydrolytically cleaved in a
random way along their length which causes strength and stiffness to decrease. The assumptions made in
the constitutive degradation model of Soares et al. can be adapted to fit the gained insights in this
degradation mechanism. The Ella BD stent was manufactured from polydioxanone, the standard polymer
currently used for bioresorbable sutures. A chemical study was conducted to check whether Ella-CS used
the same polymer as those used in bioresorbable sutures. It appeared that both the Ella BD stent as the
bioresorbable suture consisted of one single organic compound but the crystal structure was different. The
presumption that the same starting polymer was used for both application couldn’t be confirmed nor
contradicted due to solvent problems. Other aliphatic polyesters might be more suited for a stronger
bioresorbable esophageal stent and were suggested. The incorporation of radiopaque additives was
proposed to overcome poor fluoroscopic visibility of these stents.
With the help of the mechanical degradation studies, a sufficiently correct numerical model of the Ella BD
stent was developed and it can easily be adapted towards any bioresorbable polymeric braided wire stent.
This model incorporates the steric interaction and friction between the wires of the stent. It was

Conclusions and future prospects 83
demonstrated that such a correct numerical model could be of great use in design optimization procedures
or to validate the mechanical behavior of the stent within the patient-specific diseased esophagus. The
deployment and short-term behavior of a polymeric braided wire stent within an esophageal anatomical
environment was modeled and provided knowledge on the capability of the stent to open up the lumen and
on the pressures exerted on the esophageal wall.
To get a good insight into the long-term effects of bioresorbable esophageal stenting, some extra research
has to be conducted. Instead of the linear elastic material model for the aliphatic polymers, hyperelastic or
visco-elastic models have to be considered. The constitutive degradation model of Soares et al. has to be
adapted and fitted to the two-phase degradation mechanism before it can be implemented in the numerical
framework.
New insights were obtained during this thesis that should allow a manufacturer to optimize its prospective
biodegradable esophageal stents: the influence of steric interaction and friction in polymeric braided wire
stent on its mechanical behavior, the degradation mechanism of polydioxanone and its influence on the
stent’s mechanical behavior, pressures exerted on the esophageal wall etc. The developed numerical
framework can also be used for optimization procedures in other settings. Bioresorbable polymeric braided
wire stents can serve in other regions of the gastro-intestinal tract or in coronary angioplasty.

Bibliography
[1] F. H. Netter, “The Netter Collection of Medical Illustrations,” in The Netter Collection of Medical
Illustrations, 9th ed., vol. Part 1: Upper Digestive Tract., USA: Icon Learning Systems, 2000.
[2] B. Kuo and D. Urma, “Esophagus - anatomy and development,” GI Motility online, 2006.
[3] J. H. Kim, J. H. Shin, and H.-Y. Song, “Benign strictures of the esophagus and gastric outlet:
interventional management,” Korean J Radiol, vol. 11, no. 5, pp. 497–506, Oct. 2010.
[4] A. Repici, F. P. Vleggaar, C. Hassan, P. G. van Boeckel, F. Romeo, N. Pagano, A. Malesci, and P. D.
Siersema, “Efficacy and safety of biodegradable stents for refractory benign esophageal strictures: the
BEST (Biodegradable Esophageal Stent) study,” Gastrointest. Endosc., vol. 72, no. 5, pp. 927–934, Nov.
2010.
[5] L. Petruzziello, A. Tringali, M. E. Riccioni, M. Mutignani, S. Margaritora, A. Cesario, and G.
Costamagna, “Successful early treatment of Boerhaave’s syndrome by endoscopic placement of a
temporary self-expandable plastic stent without fluoroscopy,” Gastrointest. Endosc., vol. 58, no. 4, pp.
608–612, Oct. 2003.
[6] M. G. Chung, D. H. Kang, D. K. Park, J. J. Park, H. C. Park, and J. H. Kim, “Successful treatment of
Boerhaave’s syndrome with endoscopic insertion of a self-expandable metallic stent: report of three
cases and a review of the literature,” Endoscopy, vol. 33, no. 10, pp. 894–897, Oct. 2001.
[7] S. H. Blackmon, R. Santora, P. Schwarz, A. Barroso, and B. J. Dunkin, “Utility of removable esophageal
covered self-expanding metal stents for leak and fistula management,” Ann. Thorac. Surg., vol. 89, no. 3,
pp. 931–936; discussion 936–937, Mar. 2010.
[8] R. K. Freeman and A. J. Ascioti, “Esophageal Stent Placement for the Treatment of Perforation,
Fistula, or Anastomotic Leak,” Seminars in Thoracic and Cardiovascular Surgery, vol. 23, no. 2, pp. 154–
158, Jun. 2011.
[9] C. Bosetti, F. Levi, J. Ferlay, W. Garavello, F. Lucchini, P. Bertuccio, E. Negri, and C. La Vecchia,
“Trends in oesophageal cancer incidence and mortality in Europe,” Int. J. Cancer, vol. 122, no. 5, pp.
1118–1129, Mar. 2008.
[10] D. L. Francis and D. A. Katzka, “Achalasia: update on the disease and its treatment,” Gastroenterology,
vol. 139, no. 2, pp. 369–374, Aug. 2010.
[11] W. Park and M. F. Vaezi, “Etiology and pathogenesis of achalasia: the current understanding,” Am. J.
Gastroenterol., vol. 100, no. 6, pp. 1404–1414, Jun. 2005.
[12] A. E. Spiess and P. J. Kahrilas, “Treating achalasia: from whalebone to laparoscope,” JAMA, vol. 280,
no. 7, pp. 638–642, Aug. 1998.
[13] S. Irani and R. Kozarek, “Esophageal stents: past, present, and future,” Techniques in Gastrointestinal
Endoscopy, vol. 12, no. 4, pp. 178–190, Oct. 2010.
[14] K. Knyrim, H. J. Wagner, N. Bethge, M. Keymling, and N. Vakil, “A controlled trial of an expansile
metal stent for palliation of esophageal obstruction due to inoperable cancer,” N. Engl. J. Med., vol.
329, no. 18, pp. 1302–1307, Oct. 1993.
[15] M.-T. McLoughlin and M.-F. Byrne, “Endoscopic stenting: where are we now and where can we go?,”
World J. Gastroenterol., vol. 14, no. 24, pp. 3798–3803, Jun. 2008.
[16] J. C. Martinez, M. M. Puc, and R. M. Quiros, “Esophageal stenting in the setting of malignancy,” ISRN
Gastroenterol, vol. 2011, p. 719575, 2011.
[17] S.-G. Kang, “Gastrointestinal stent update,” Gut Liver, vol. 4 Suppl 1, pp. S19–24, Sep. 2010.

Bibliography 85
[18] D. Schembre, “Advances in esophageal stenting: the evolution of fully covered stents for malignant
and benign disease,” Adv Ther, vol. 27, no. 7, pp. 413–425, Jul. 2010.
[19] M. J. Uitdehaag, P. D. Siersema, M. C. W. Spaander, F. P. Vleggaar, E. M. L. Verschuur, E. W.
Steyerberg, and E. J. Kuipers, “A new fully covered stent with antimigration properties for the
palliation of malignant dysphagia: a prospective cohort study,” Gastrointest. Endosc., vol. 71, no. 3, pp.
600–605, Mar. 2010.
[20] T. Sabharwal, M. S. Hamady, S. Chui, S. Atkinson, R. Mason, and A. Adam, “A randomised prospective
comparison of the Flamingo Wallstent and Ultraflex stent for palliation of dysphagia associated with
lower third oesophageal carcinoma,” Gut, vol. 52, no. 7, pp. 922–926, Jul. 2003.
[21] P. D. Siersema, W. C. Hop, M. van Blankenstein, A. J. van Tilburg, D. J. Bac, M. Y. Homs, and E. J.
Kuipers, “A comparison of 3 types of covered metal stents for the palliation of patients with
dysphagia caused by esophagogastric carcinoma: a prospective, randomized study,” Gastrointest.
Endosc., vol. 54, no. 2, pp. 145–153, Aug. 2001.
[22] E. M. L. Verschuur, A. Repici, E. J. Kuipers, E. W. Steyerberg, and P. D. Siersema, “New design
esophageal stents for the palliation of dysphagia from esophageal or gastric cardia cancer: a
randomized trial,” Am. J. Gastroenterol., vol. 103, no. 2, pp. 304–312, Feb. 2008.
[23] G Dorta, “Interview with a gastro-enterologist at CHUV, Lausanne,” 09-Dec-2012.
[24] T. Sabharwal, M. S. Gulati, N. Fotiadis, R. Dourado, A. Botha, R. Mason, and A. Adam, “Randomised
comparison of the FerX Ella antireflux stent and the ultraflex stent: proton pump inhibitor
combination for prevention of post-stent reflux in patients with esophageal carcinoma involving the
esophago-gastric junction,” J. Gastroenterol. Hepatol., vol. 23, no. 5, pp. 723–728, May 2008.
[25] L. R. H. de Wijkerslooth, F. P. Vleggaar, and P. D. Siersema, “Endoscopic Management of Difficult or
Recurrent Esophageal Strictures,” The American Journal of Gastroenterology, vol. 106, no. 12, pp. 2080–
2091, Dec. 2011.
[26] M. Conio, A. De Ceglie, S. Blanchi, and D. A. Fisher, “Esophageal strictures, tumors, and fistulae:
stents for primary esophageal cancer,” Techniques in Gastrointestinal Endoscopy, vol. 12, no. 4, pp. 191–
202, Oct. 2010.
[27] M. J. Uitdehaag, J. E. van Hooft, E. M. L. Verschuur, A. Repici, E. W. Steyerberg, P. Fockens, E. J.
Kuipers, and P. D. Siersema, “A fully-covered stent (Alimaxx-E) for the palliation of malignant
dysphagia: a prospective follow-up study,” Gastrointest. Endosc., vol. 70, no. 6, pp. 1082–1089, Dec.
2009.
[28] G. Dorta, J. Binek, A. L. Blum, H. Bühler, C. P. Felley, H. R. Koelz, F. Lammer, C. Lang, R. Meier, C.
Meyenberger, B. Meyer-Wyss, P. Michetti, P. Protiva, U. Scheurer, B. Weber, P. Wiesel, and S. Vogel,
“Comparison between esophageal Wallstent and Ultraflex stents in the treatment of malignant
stenoses of the esophagus and cardia,” Endoscopy, vol. 29, no. 3, pp. 149–154, Mar. 1997.
[29] A. Schmassmann, C. Meyenberger, J. Knuchel, J. Binek, F. Lammer, B. Kleiner, S. Hürlimann, W.
Inauen, B. Hammer, U. Scheurer, and F. Halter, “Self-expanding metal stents in malignant esophageal
obstruction: a comparison between two stent types,” Am. J. Gastroenterol., vol. 92, no. 3, pp. 400–406,
Mar. 1997.
[30] M. Conio, A. Repici, G. Battaglia, G. De Pretis, L. Ghezzo, M. Bittinger, H. Messmann, J.-F.
Demarquay, S. Blanchi, M. Togni, R. Conigliaro, and R. Filiberti, “A randomized prospective
comparison of self-expandable plastic stents and partially covered self-expandable metal stents in the
palliation of malignant esophageal dysphagia,” Am. J. Gastroenterol., vol. 102, no. 12, pp. 2667–2677,
Dec. 2007.
[31] M. Y. Homs, E. W. Steyerberg, W. M. Eijkenboom, H. W. Tilanus, L. J. Stalpers, J. F. Bartelsman, J. J.
van Lanschot, H. K. Wijrdeman, C. J. Mulder, J. G. Reinders, H. Boot, B. M. Aleman, E. J. Kuipers, and
P. D. Siersema, “Single-dose brachytherapy versus metal stent placement for the palliation of
dysphagia from oesophageal cancer: multicentre randomised trial,” The Lancet, vol. 364, no. 9444, pp.
1497–1504, 23.

Bibliography 86
[32] E. M. L. Verschuur, E. W. Steyerberg, E. J. Kuipers, and P. D. Siersema, “Effect of stent size on
complications and recurrent dysphagia in patients with esophageal or gastric cardia cancer,”
Gastrointestinal Endoscopy, vol. 65, no. 4, pp. 592–601, Apr. 2007.
[33] M. Y. Homs, E. W. Steyerberg, E. J. Kuipers, A. van der Gaast, J. Haringsma, M. van Blankenstein, and
P. D. Siersema, “Causes and Treatment of Recurrent Dysphagia after Self-Expanding Metal Stent
Placement for Palliation of Esophageal Carcinoma,” Endoscopy, vol. 36, no. 10, pp. 880–886, Oct. 2004.
[34] R. Conigliaro, G. Battaglia, A. Repici, G. De Pretis, L. Ghezzo, M. Bittinger, H. Messmann, J.-F.
Demarquay, M. Togni, S. Blanchi, R. Filiberti, and M. Conio, “Polyflex stents for malignant oesophageal
and oesophagogastric stricture: a prospective, multicentric study,” European Journal of Gastroenterology
& Hepatology, vol. 19, no. 3, pp. 195–203, Mar. 2007.
[35] L. Szegedi, I. G??l, I. K??sa, and G. G. Kiss, “Palliative treatment of esophageal carcinoma with self-
expanding plastic stents: a report on 69 cases,” European Journal of Gastroenterology & Hepatology, pp.
1197–1201, Nov. 2006.
[36] E. M. L. Verschuur, M. Y. V. Homs, E. W. Steyerberg, J. Haringsma, P. J. Wahab, E. J. Kuipers, and P.
D. Siersema, “A new esophageal stent design (Niti-S stent) for the prevention of migration: a
prospective study in 42 patients,” Gastrointestinal Endoscopy, vol. 63, no. 1, pp. 134–140, Jan. 2006.
[37] A. J. Dormann, P. Eisendrath, B. Wigginghaus, H. Huchzermeyer, and J. Devière, “Palliation of
Esophageal Carcinoma with a New Self-Expanding Plastic Stent,” Endoscopy, vol. 35, no. 3, pp. 207–
211, Mar. 2003.
[38] W. A. Ross, F. Alkassab, P. M. Lynch, G. D. Ayers, J. Ajani, J. H. Lee, and M. Bismar, “Evolving role of
self-expanding metal stents in the treatment of malignant dysphagia and fistulas,” Gastrointestinal
Endoscopy, vol. 65, no. 1, pp. 70–76, Jan. 2007.
[39] F. C. Ramirez, B. Dennert, S. T. Zierer, and R. A. Sanowski, “Esophageal self-expandable metallic
stents--indications, practice, techniques, and complications: results of a national survey,” Gastrointest.
Endosc., vol. 45, no. 5, pp. 360–364, May 1997.
[40] M. O. Baerlocher, M. R. Asch, P. Dixon, P. Kortan, A. Myers, and C. Law, “Interdisciplinary Canadian
guidelines on the use of metal stents in the gastrointestinal tract for oncological indications,” Can
Assoc Radiol J, vol. 59, no. 3, pp. 107–122, Jun. 2008.
[41] T. H. Baron, “Minimizing endoscopic complications: endoluminal stents,” Gastrointest. Endosc. Clin. N.
Am., vol. 17, no. 1, pp. 83–104, vii, Jan. 2007.
[42] T. Sabharwal, J. P. Morales, F. G. Irani, and A. Adam, “Quality improvement guidelines for placement
of esophageal stents,” Cardiovasc Intervent Radiol, vol. 28, no. 3, pp. 284–288, Jun. 2005.
[43] R. Morgan and A. Adam, “Use of metallic stents and balloons in the esophagus and gastrointestinal
tract,” J Vasc Interv Radiol, vol. 12, no. 3, pp. 283–297, Mar. 2001.
[44] A.-C. Albertsson, Degradable Aliphatic Polyesters. Springer, 2002.
[45] H. Tian, Z. Tang, X. Zhuang, X. Chen, and X. Jing, “Biodegradable synthetic polymers: Preparation,
functionalization and biomedical application,” Progress in Polymer Science, vol. 37, no. 2, pp. 237–280,
Feb. 2012.
[46] N. Debusschere, “Ontwerp van biodegradeerbare polymeer stents, Master Thesis.” Faculty of
Engineering, Ghent University, Belgium, Jun-2011.
[47] L. A. Bosworth and S. Downes, “Physicochemical characterisation of degrading polycaprolactone
scaffolds,” Polymer Degradation and Stability, vol. 95, no. 12, pp. 2269–2276, Dec. 2010.
[48] M. A. Sabino, S. González, L. Márquez, and J. L. Feijoo, “Study of the hydrolytic degradation of
polydioxanone PPDX,” Polymer Degradation and Stability, vol. 69, no. 2, pp. 209–216, Jul. 2000.
[49] UK Medical Limited., “Product description brochure Ella-BD Esophageal Stent.” Jul-2011.
[50] M. R. Jedwab and C. O. Clerc, “A study of the geometrical and mechanical properties of a self-
expanding metallic stent--theory and experiment,” J Appl Biomater, vol. 4, no. 1, pp. 77–85, 1993.
[51] A.M. Wahl, “Mechanical Springs, 2nd edition,” McGraw-Hill Book Company, 1963, pp. 241–254.
[52] R. Wang and K. Ravi-Chandar, “Mechanical Response of a Metallic Aortic Stent—Part I: Pressure-
Diameter Relationship,” J. Appl. Mech., vol. 71, no. 5, pp. 697–705, Nov. 2004.

Bibliography 87
[53] S. Canic, K. Ravi-Chandar, Z. Krajcer, D. Mirkovic, and S. Lapin, “Mathematical Model Analysis of
Wallstent(R) and AneuRx(R),” Tex Heart Inst J, vol. 32, no. 4, pp. 502–506, 2005.
[54] De Beule, Matthieu, Finite element stent design, PhD Thesis. Faculty of Engineering, Ghent University,
Belgium, 2008.
[55] M. De Beule, S. Van Cauter, P. Mortier, D. Van Loo, R. Van Impe, P. Verdonck, and B. Verhegghe,
“Virtual optimization of self-expandable braided wire stents,” Medical Engineering & Physics, vol. 31, no.
4, pp. 448–453, May 2009.
[56] J.-P. Nuutinen, C. Clerc, and P. Törmälä, “Theoretical and experimental evaluation of the radial force
of self-expanding braided bioabsorbable stents,” J Biomater Sci Polym Ed, vol. 14, no. 7, pp. 677–687,
2003.
[57] G. J. Hall and E. P. Kasper, “Comparison of element technologies for modeling stent expansion,” J
Biomech Eng, vol. 128, no. 5, pp. 751–756, Oct. 2006.
[58] M. Jedwab and C. Clerk, “J. Appl. Biomater., 4th edition,” 1993, p. 77.
[59] Y. Saito, K. Minami, M. Kobayashi, Y. Nakao, H. Omiya, H. Imamura, N. Sakaida, and A. Okamura,
“New tubular bioabsorbable knitted airway stent: biocompatibility and mechanical strength,” J. Thorac.
Cardiovasc. Surg., vol. 123, no. 1, pp. 161–167, Jan. 2002.
[60] R. Rieu, P. Barragan, C. Masson, J. Fuseri, V. Garitey, M. Silvestri, P. Roquebert, and J. Sainsous,
“Radial force of coronary stents: a comparative analysis,” Catheter Cardiovasc Interv, vol. 46, no. 3, pp.
380–391, Mar. 1999.
[61] C. M. Agrawal and H. G. Clark, “Deformation characteristics of a bioabsorbable intravascular stent,”
Invest Radiol, vol. 27, no. 12, pp. 1020–1024, Dec. 1992.
[62] Prof. Dr. ir. Rudy Van Impe, Berekening van Bouwkundige Constructies, vol. 1, 3 vols. Technologiepark
904B, 9052 Zwijnaarde, Belgium: Laboratorium voor Modelonderzoek, Vakgroep Bouwkundige
Constructies TW14, Ghent University, Belgium, 2010.
[63] “http://www.instron.us/wa/product/5900-Series-Single-Column-Testing-Systems.aspx.” .
[64] G. Li, Y. Li, P. Lan, J. Li, Z. Zhao, X. He, J. Zhang, and H. Hu, “Biodegradable weft-knitted intestinal
stents: Fabrication and physical changes investigation in vitro degradation,” J Biomed Mater Res A, Apr.
2013.
[65] O. Böstmann, Journal of Bone and Joint Surgery, p. 148.
[66] R. Kontio, P. Ruuttila, L. Lindroos, R. Suuronen, A. Salo, C. Lindqvist, I. Virtanen, and Y. T. Konttinen,
“Biodegradable polydioxanone and poly(l/d)lactide implants: an experimental study on peri-implant
tissue response,” Int J Oral Maxillofac Surg, vol. 34, no. 7, pp. 766–776, Oct. 2005.
[67] J. S. Soares, J. E. Moore Jr, and K. R. Rajagopal, “Constitutive framework for biodegradable polymers
with applications to biodegradable stents,” ASAIO J., vol. 54, no. 3, pp. 295–301, Jun. 2008.
[68] S. H. Oh, S. C. Park, H. K. Kim, Y. J. Koh, J.-H. Lee, M. C. Lee, and J. H. Lee, “Degradation Behavior of
3D Porous Polydioxanone-b-Polycaprolactone Scaffolds Fabricated Using the Melt-Molding
Particulate-Leaching Method,” Journal of Biomaterials Science, Polymer Edition, vol. 22, no. 1–3, pp. 225–
237, 2011.
[69] R. Waksman, “Biodegradable stents: they do their job and disappear,” J Invasive Cardiol, vol. 18, no. 2,
pp. 70–74, Feb. 2006.
[70] P. Chang, “Polymer implant materials with improved X-ray opacity and biocompatibility,” Biomaterials,
vol. 2, no. 3, pp. 151–155, Jul. 1981.
[71] “http://www.nongnu.org/pyformex/.” .
[72] “Abaqus Documentation - SIMULIA Advantage Support.” .
[73] “Friction,” Wikipedia, the free encyclopedia. 16-May-2013.
[74] “http://biomedical.materialise.com/mimics.” .
[75] W. Yang, T. C. Fung, K. S. Chian, and C. K. Chong, “Viscoelasticity of esophageal tissue and
application of a QLV model,” J Biomech Eng, vol. 128, no. 6, pp. 909–916, Dec. 2006.

List of Figures
Figure 1-1. Gastroesophageal junction [1] ....................................................................................................................................................................... 1
Figure 1-2. Cross section esophageal lumen [1] ............................................................................................................................................................ 2
Figure 1-3. Esophageal strictures [1] ................................................................................................................................................................................. 4
Figure 1-4. ALIMAXX-ES™ Fully Covered Esophageal Stent .................................................................................................................................... 9
Figure 1-5. Evolution® Esophageal Fully Covered Controlled-Release Stent ......................................................................................................... 9
Figure 1-6. Evolution® Esophageal Partially Covered Controlled-Release Stent .................................................................................................. 9
Figure 1-7. Antimigration ring Ella stents ....................................................................................................................................................................... 10
Figure 1-8. SX-Ella Danis stent ......................................................................................................................................................................................... 10
Figure 1-9. Taewoong Niti-S™ Esophageal stent ....................................................................................................................................................... 11
Figure 1-10. Polyflex® Esophageal Stent ....................................................................................................................................................................... 11
Figure 1-11. Ultraflex® Esophageal Stent (1: Large Proximal Flare, 2: Polyurethane Covering, 3: Flexible Knitted-Loop Design) . 12
Figure 1-12. Wallflex® Fully Covered Esophageal Stent .......................................................................................................................................... 12
Figure 1-13. Selection of the currently available stents, from left to right Ultraflex, Polyflex, (partially covered) Wallflex, (partially
covered) Evolution, SX-Ella, Niti-S, and Alimaxx-E stents [25]. ............................................................................................................................. 14
Figure 1-14. Self-expandable stents: (A) SX Ella, (B) Endoflex, (C) Alimaxx, (D) Polyflex, (E) Ultraflex, (F) Niti-S, (G) Evolution,
(H) Choostent, (I) Dostent, and (J) Hanarostent [26]. ............................................................................................................................................. 14
Figure 1-15. Delivery system Ella Stents ........................................................................................................................................................................ 18
Figure 1-16. Cook Medical’s Evolution® esophageal stent delivery system ........................................................................................................ 18
Figure 1-17. The Ella-BD stent .......................................................................................................................................................................................... 21
Figure 1-18. Components delivery system Ella-BD Stent .......................................................................................................................................... 22
Figure 2-1. Conventional experimental methods to determine stent radial strength: (A) blocks with semi-cylindrical groove, (B)
parallel plates, (C) plates at a 90± angle, (D) collar and (E) V-shaped and flat plate [56]. ...................................................................... 28
Figure 2-2. MPT Europe's stent compression unit ...................................................................................................................................................... 28
Figure 2-3. Compression test setup (Instron + MPT SCU) ..................................................................................................................................... 28
Figure 2-4. MPT SCU detail ................................................................................................................................................................................................ 29
Figure 2-5. Stent compression test, conducted in the bioMMeda lab .................................................................................................................. 30
Figure 2-6. Isolating a wire from the Ella BD stent ....................................................................................................... 33
Figure 2-7. Tensile testing wire from the Ella BD stent ............................................................................................... 34
Figure 2-8. Experiment preparations .............................................................................................................................................................................. 36
Figure 2-9. Stent damage during radial force degradation experiment (top: week 8, bottom: week 9) .................................................. 37
Figure 2-10. The conventional synthesis of poly(-p-)dioxanone .............................................................................................................................. 40
Figure 2-11. Scheme for the hydrolysis process of an aliphatic polyester like PDS in an aqueous medium such as PBS. [48] ....... 41
Figure 2-12. Degradation mechanism [64] .................................................................................................................................................................. 41
Figure 3-1. Flowchart of the development of the numerical framework for BDPBWS................................................................................... 50
Figure 3-2. Creating a bended wire strut (XZ-view) .................................................................................................................................................. 52
Figure 3-3. Bended wire segment (left: XY view, middle: XZ view, right: iso view) ......................................................................................... 53
Figure 3-4. Creating the flared nearly planar pattern ............................................................................................................................................... 54
Figure 3-5. Full stent geometry (a: iso view, b: right view, c: front view) ............................................................................................................. 55
Figure 3-6. The STENT part ............................................................................................................................................................................................... 56
Figure 3-7. The CRIMPER part .......................................................................................................................................................................................... 56

List of Figures 89
Figure 3-8. Rendered beam thickness detail of the STENT part ........................................................................................................................... 57
Figure 3-9. Increase in pitch angle during radial compression or axial elongation [54] ................................................................................ 59
Figure 3-10. Kinematic constraints HINGE connection type ................................................................................................................................... 60
Figure 3-11. Contact shear forces between stent and crimper at the beginning of the stent compression simulation ....................... 64
Figure 3-12. Contact shear forces between stent wires reciprocally at the beginning of the stent compression simulation ............. 64
Figure 3-13. Comparing geometrical model sizes ((a) -model; (b) -model; (c) -model; (d) -model) ........................ 65
Figure 3-14. Simulation vs experiment ........................................................................................................................................................................... 67
Figure 3-15. Flowchart of De Beule's optimization modeling strategy [54] ...................................................................................................... 70
Figure 3-16. Comparison stent designs with pitch angle 15°(left), 30° (middle) and 45° (right) and same number of wires ........ 71
Figure 3-17. Comparison stent designs with number of wires: 12 (left), 14 (middle) and 16 (right) - constant pitch angle: 30° .. 72
Figure 4-1. Angular line segment of modeled esophagus with stenosis ............................................................................................................... 74
Figure 4-2. Nearly planar grid of modeled esophagus with stenosis .................................................................................................................... 74
Figure 4-3. Final geometrical model esophagus with stenosis ................................................................................................................................. 74
Figure 4-4. Loading the stent onto the guidewire ........................................................................................................................................................ 77
Figure 4-5. Stent deployment (Y-plane-cut)................................................................................................................................................................... 78
Figure 4-6. Opening up of the constricted esophageal lumen (Z-plane-cut) ..................................................................................................... 78
Figure 4-7. Pressure exerted by the stent on the esophageal wall (MPa) .......................................................................................................... 79
Figure 4-8. Evolution stenosis diameter with stent degradation ............................................................................................................................. 80

List of Tables
Table 1-1. Indications and contraindictions for SEMS and SEPS [13]. .................................................................................................................. 7
Table 1-2. Selected SEMS currently available in the United States, Europe, or Asia ..................................................................................... 13
Table 1-3. Recurrent dysphagia and major complications after stent placement of partially or fully covered stents for the
palliation of malignant dysphagia [19]. .......................................................................................................................................................................... 16
Table 1-4. Clarification of terminology and their definitions with respect to the breakdown of synthetic polymers [47]. ................. 21
Table 2-1. Young's Modulus results tensile test wire samples from the non-degraded Ella BD stent ........... 35
Table 2-2. Maximal measures loads compression tests during degradation ..................................................................................................... 38
Table 2-3. Results TGA analyzes ...................................................................................................................................................................................... 43
Table 2-4. Results DSC analyzes ...................................................................................................................................................................................... 45
Table 2-5. Possible biodegradable stent materials and their mechanical properties ...................................................................................... 48
Table 3-1. Geometrical modeling parameters Ella-BD stent ................................................................................................................................... 52
Table 3-2. Size geometrical model................................................................................................................................................................................... 65
Table 3-3. Design optimization simulations .................................................................................................................................................................. 70
Table 4-1. Geometrical parameters modeled esophagus ......................................................................................................................................... 73
Table 4-2. Material parameters estimated using experimental stress-relaxation curves [75] .................................................................... 76

List of Graphs
Graph 2-1. Internal friction MPT Europe's stent compression unit ....................................................................................................................... 31
Graph 2-2. Stent compression test non-degraded Ella BD 25⁄20⁄25 x100mm stent (without correction SCU friction) ................ 31
Graph 2-3. Stent compression test non-degraded Ella BD 25⁄20⁄25 x100mm stent (correction SCU friction) ................................ 32
Graph 2-4. Stent compression test for the non-degraded Ella BD 25⁄20⁄25 x100mm stent (double friction correction) ............. 33
Graph 2-5. Tensile test results separated wire samples from the non-degraded Ella BD stent ...................... 35
Graph 2-6. Radial force degradation Ella BD 25⁄20⁄25 x100mm stent (first phase) ................................................................................ 36
Graph 2-7. Radial force degradation Ella BD 25⁄20⁄25 x100mm stent (second phase) .......................................................................... 37
Graph 2-8. Stiffness during degradation wires Ella BD 31⁄(25⁄31) x100mm stent .................................................................................... 38
Graph 2-9. Corrected stiffness during degradation wires Ella BD 31⁄(25⁄31) x100mm stent ................................................................ 39
Graph 2-10. Results TGA degraded wire sample Ella BD stent ............................................................................................................................. 44
Graph 2-11. DSC analysis non-degraded wire sample Ella BD stent................................................................................................................... 45
Graph 2-12. DSC analysis degraded wire sample Ella BD stent ........................................................................................................................... 46
Graph 2-13. DSC analysis non-degraded PDS*II-Z303 suture .............................................................................................................................. 47
Graph 3-1. Amplitude Step-1............................................................................................................................................................................................. 58
Graph 3-2. Damping energy negligible compared to total internal energy ........................................................................................................ 61
Graph 3-3. Slip regions for the basic Coulomb friction model [72] ...................................................................................................................... 63
Graph 3-4. Elastic slip versus shear traction for sticking and slipping friction [72] ........................................................................................ 63
Graph 3-5. Quasi-static analysis: energy fraction requirement satisfied .............................................................................................................. 66
Graph 3-6. Simulations stent compression test day 35 - HINGE connector models ...................................................................................... 67
Graph 3-7. Simulations stent compression test day 35 - Internal self-contact models .................................................................................. 68
Graph 3-8. Simulations stent compression test day 0 - Internal self-contact models ..................................................................................... 69
Graph 3-9. Simulations stent compression test day 48 - Internal self-contact models .................................................................................. 69
Graph 3-10. Results comparison stent designs with pitch angles: 15° (A15), 30° (A30) and 45° (A45) – 12 wires each ............. 71
Graph 3-11. Results comparison stent designs with number of wires: 12 (A30), 14 (B30) and 16 (C30) - pitch angle: 30° ........ 72
Graph 4-1. Evolution stenosis diameter with stent degradation ............................................................................................................................ 80

List of Scripts
Script 3-1. Implementation of the bended wire segment ......................................................................................................................................... 53
Script 3-2. Implentation of the flares .............................................................................................................................................................................. 54
Script 4-1. Class Esophagus ............................................................................................................................................................................................... 75



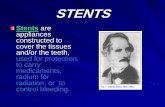



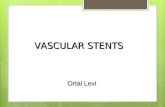




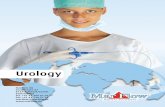



![Bioabsorbable Stents - · PDF fileCompany Picture Polymer/Drug Features Bioabsorbable Vascular Solutions (BVS) [Guidant] All biodegradable polymers (PLLA) with everolimus Igaki-Tamai](https://static.fdocuments.net/doc/165x107/5a70b7c97f8b9ab1538c312d/bioabsorbable-stents-summitmdcomwwwsummitmdcompdfpdf060526lec6pdfpdf.jpg)