Describe relationship between neuromodulation, rehabilitation…
32
Brain NeuroModulation for Stroke W. Jerry Mysiw, MD Chair, Department of Physical Medicine and Rehabilitation Wexner Medical Center at The Ohio State University Describe relationship between neuromodulation, rehabilitation… Recognize new modalities and research in expanding the field of neuromodulation and neurorehabilitation
description
Brain NeuroModulation for Stroke W. Jerry Mysiw, MD Chair, Department of Physical Medicine and Rehabilitation Wexner Medical Center at The Ohio State University. Describe relationship between neuromodulation, rehabilitation… - PowerPoint PPT Presentation
Transcript of Describe relationship between neuromodulation, rehabilitation…

Brain NeuroModulation for StrokeW. Jerry Mysiw, MDChair, Department of Physical Medicine and RehabilitationWexner Medical Center at The Ohio State University
Describe relationship between neuromodulation, rehabilitation…Recognize new modalities and research in expanding the field of neuromodulation and neurorehabilitation

Disclosures
Faculty appointment The Ohio State University
Grant support-unrelated topics NIH DOE/NIDRR
Industry Grant support- none Consulting- none Ownership-none

NeuroRehabilitation in Transition
Health care reform Post acute care strategies
Decrease cost Decrease readmission
Post acute activity based therapy discontinued before plasticity reaches plateau
Emerging Solutions Extend the continuum of post
acute rehabilitation into the home Gaming strategies to
provide activity based therapy in the home
Neuroimaging assessment of neuroplasticity Activity based therapy
dose response studies Interval assessment of a
therapy’s impact on plasticity
Neuromodulation drives plasticity

Stroke Related Disability Stroke is a leading cause of adult disability in the US. Data from GCNKSS/NINDS studies show that about
795,000 people suffer a new or recurrent stroke each year. About 610,000 of these are first attacks
About 6,400,000 stroke survivors are alive today In 2010, stroke cost the US $73.7 billion in health care
services, medications, and lost productivity. Death risk and disability can be lowered.
Early complications deprive patients of 2 years of optimum health.
Greater numbers of complications are associated with greater loss of healthy life-years.
CDC; AHA

5
Stroke is the leading cause of Adult Disability

Stroke Rehabilitation Outcomes
80% -Independent Mobility 70% -Independent Personal Care 40% -Independent Outside the Home 30%- Return to Work
30% of strokes occur in people under 65 49% RTW rate for people 21-65 year old
• Overall mortality is declining
• Long-term survival post-stroke is improving

Post Stroke Impairments: Predictors of Disability
Hemiplegia (75-88%)
Emotional lability (mood swings, depression)
Cognitive impairments
Loss of awareness (neglect syndromes)
Dysphagia
Aphasia
Apraxia

Neuroplasticity
Plasticity (adaptive) is experience dependent. maximum impact when coupled with optimal experience
(therapy)
Motor recovery after stroke illustrate the principle that many forms of neuroplasticity can be ongoing in parallel. Spontaneous intra-hemispheric changes in
representational maps Inter-hemispheric balance shift - uninjured hemisphere
assumes extranormal activity in relation to movement Changes in the connections between network nodes Molecular adaptive changes

Brain 2011: 134; 1591–1609
Brain 2011: 134; 1591–1609

Harnessing Neuroplasticity for Clinical ApplicationsBrain 2011: 134; 1591–1609
CNS perturbation Stroke TBI Aging
Neuroplasticity Positive/negative Neurogenesis… Alternate pathway
Intervention Activity based therapy Pharmacology Neuromodulation
Outcome Life years
Impairment resolution
Functional gain
Quality of life
Imaging

Non-invasive brain stimulation
Objective: change brain function promote neuroplasticity
Interventions Transcranial Magnetic Stimulation Transcranial Direct Current Stimulation (tDCS)
General assumption is that the application of noninvasive brain stimulation with parameters that enhance motor cortical excitability could secondarily facilitate motor performance and motor learning

Major limitationsOnly regions on cortical surface can be stimulatedLocalisation uncertaintyStimulation level uncertainty
Major advantages Reversible lesions without plasticity changeCan establish causal link between brain activation and behaviourCan measure cortical plasticityCan modulate cortical plasticityTherapeutic benefits

Transcranial magnetic stimulation (TMS)
Very safe, when following current safety guidelines (Rossi et al., 2009),
Noninvasive Normal brain activity is disrupted by this induced current
TMS provides a way to produce a transient and reversible period of brain disruption or “virtual lesion.”
TMS can assess whether a given brain area is necessary for a given function rather than simply correlated with it.
Can probe the functional connectivity of different cortical areas in the human cortex using paired-pulse TMS
Repetitive TMS effects persist past the initial period of stimulation. rTMS can increase or decrease the excitability

Low Frequency vs. High Frequency TMS
TMS activates a mixed population of inhibitory and
excitatory cortical interneurons
Low Frequency Stimulation--inhibitory, more focal effect
High Frequency Stimulation--facilitating, multiple, spread out, global “dendritic, axonal effect”.
When higher frequency rTMS is applied, a longer lasting effect can be induced which is thought to result from a long term potentiation (LTP),
or depression (LTD) at the neuronal level.
14

What Could TMS Treat?
I. Affect/Self Regulation Behaviors: Depression (FDA approval, Oct 2008) Anxiety-Panic, OCD, PTSD Addiction- pathologic gambling, food, substance abuse Schizoaffective disorder.
II. Pain Neuropathic pains Phantom pain, Fibromyalgia, Migraine headaches, Tinnitus
III. NeuroRehabilitation Stroke – Hemiplegia, aphasia, neglect Brain Injury- mood

TMS Stimulation
On-line stimulation occurs during task performance• Virtual lesions• Functional connectivity
Off-line stimulation occurs without a task • Plasticity• Interventional
• Depression• Pain

A multi-center study on low-frequency rTMScombined with intensive occupational therapy forupper limb hemiparesis in post-stroke patientsKakuda et al. Journal of NeuroEngineering and Rehabilitation 2012, 9:4
Methods: The study subjects were 204 post-stroke patients with upper limb hemiparesis (mean age 58.5 ± 13.4 years, mean time after stroke 5.0 ± 4.5 years, ± SD) During 15-day hospitalization, each patient received 22 treatment sessions of 20-min low-frequency rTMS and 120-min intensive OT daily. Low-frequency rTMS of 1 Hz was applied to the contralesional hemisphere over the primary motor area.
Results: All patients completed the protocol without any adverse effects. The FMA score increased and WMFT log performance time decreased significantly FMA score: median at admission, 47 points; median at discharge, 51 points; p < 0.001. change in WMFT logperformance time: median at admission, 3.23; median at discharge, 2.51; p < 0.001). These changes were persistently seen up to 4 weeks after discharge in 79 patients.

TMS and Chronic AphasiaNaeser et al. rTMS over RH homologue of Broca’s area
Daily for 10 days, 20 min each time
Tested picture naming speed & accuracy Immediately after 10th session
All patients reliably faster & more accurate than their pre-treatment baseline measures
2 months later & 8 months later Effects decreased over time, but continued through
8 mos for 3 of 4 patients

TMS in Chronic Aphasia

Transcranial Direct Current Stimulation
Noninvasive application of weak direct current through a set of two (or more) electrodes
Applied current enters the brain via the positively charged anode, and flows to the negatively charged cathode.
Neuronal excitability of the targeted brain area can be modified in a polarity-specific manner anodal stimulation increases the excitability cathodal stimulation decreases excitability

Transcranial direct current stimulation
Motor learning is associated with functional and structural changes in a widely distributed cortical network including the primary motor, premotor and supplementary motor cortex, cerebellum Basal ganglia

Modulation of motor performance and learning bytranscranial direct current stimulation in healthy subjects
Anodal tDCS applied to M1 in temporal relation to motor practice transiently improves performance within a single session or when given repeatedly in the absence of practice
Anodal tDCS augments prolonged skill acquisition skill gains between sessions (consolidation) anodal tDCS-stimulated subjects skill
remained superior to controls even after 3 months Current Opinion in Neurology 2011, 24:590–596

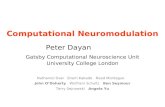
Effects of timing of anodal transcranial direct current stimulation in relation to motor training sessions Current Opinion in Neurology 2011, 24:590–596
Depicted is the relation of anodal tDCS sessions (blue) to training sessions (green) in the time domain, in healthy volunteers. The effect on early and delayed motor performance of each stim/training configuration is shown (, - decrease; =unchanged; + increase; ?, not investigated). A-tDCS, anodal
A tDCS A tDCS A tDCS A tDCS
Training TrainingTraining
Early/late +/? +/+ +/? +/=

Transcranial direct current stimulation and‘motor rehabilitation’ in patients with motordeficits after stroke
Proof of principle studies showed that anodal tDCS can transiently improve cognitive and motor function of the upper and lower extremity post brain injury.
Lindenberg et al. showed that bihemispheric tDCS (anodal stimulation applied to the ipsilesional M1, cathodal stimulation to the contralesional M1) combined with 5 days of occupational therapy/physiotherapy improved motor performance in chronic stroke patients(>5 months after stroke)performance remained superior for at least 1 week

Transcranial Direct Current Stimulation (tDCS)and Chronic Aphasia
(Monti et al., 2008) One session cathodal tDCS to L Broca’s area
improved naming was observed with an increase of 33.6% (SEM 13.8%) immediately post-tDCStreatment, in eight chronic nonfluent aphasia patients

Transcranial direct current stimulation (tDCS) and modulation of motor performance
Simultaneous anodal transcranial direct current
stimulation (tDCS) and training promotes improvement
in motor performance and motor learning in
healthy individuals and chronic stroke patients.
The time-locked application of tDCS and training
appears to be crucial to induce lasting effects.

Theoretical tDCS safety concerns Potential side effects with tDCS
electrode-tissue interface could lead to skin irritation and damage.
Stimulations could lead to excitotoxic firing rates. Tissue damage due to heating.
Rat studies suggest injury only when current density is several orders of magnitude beyond those used in humans (Liebetanz et al. 2009).
Datta (2009) heating in humans is negligible. Nitsche et at. (2003) reports that in more than 500
participants the only side effects are initial scalp tingling or sensation of a light flash.
Some studies suggest that higher current densities can lead to skin irritation.

Transcranial Direct Current Stimulation (tDCS)
Transcranial direct current stimulation Very inexpensive (~$250 for iontophoresis unit). Believed to be safe. Believed to modulate the firing rate of active neurons.
Depending on polarity, tDCS can induce cortical excitability reduction or enhancement can persists for hours.

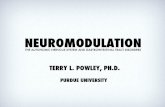
Where to stimulate
Stimulation region not well focused.
Must create electrical circuit: both anode and cathode. If both on scalp, are effects due to
facilitation or inhibition? If one electrode on shoulder/limbs
(Baker, 2010), perhaps spinal influence.
One option is large, diffuse electrode over mastoid (Elmer, 2009).
+
_
+_

Designing TMS/tDCS Studies1. Type of stimulation
• Repetitive vs single or paired
2. Choosing control conditions
3. Targeting stimulation
4. Choosing parameters Stimulation intensity / duration / rate
Inter-stimulation interval
Type of coil
Type of stimulation / stimulator
Accessibility
Number of trials per condition?

TMS stimulation
Single-pulse TMS Paired-pulse TMS Repetitive TMS (rTMS) Low frequency rTMS (1 Hz) High frequency rTMS (>1 Hz) Theta-burst, etc

Creating the future of medicine to improve people's lives through personalized health care