Derivation of an Appropriate Outcome Measure in Lupus · ii Derivation of an Appropriate Outcome...
156
Derivation of an Appropriate Outcome Measure in Lupus by Zahi Touma A thesis submitted in conformity with the requirements for the degree of PhD Institute of Medical Science University of Toronto © Copyright by Zahi Touma 2012
Transcript of Derivation of an Appropriate Outcome Measure in Lupus · ii Derivation of an Appropriate Outcome...

Derivation of an Appropriate Outcome Measure in Lupus
by
Zahi Touma
A thesis submitted in conformity with the requirements for the degree of PhD
Institute of Medical Science University of Toronto
© Copyright by Zahi Touma 2012

ii
Derivation of an Appropriate Outcome Measure in Lupus
Zahi Touma
PhD
Institute of Medical Science
University of Toronto
2012
Abstract
Aim: To develop an outcome measure to identify “responders” for patients who had a clinically
important improvement in lupus disease activity with treatment.
Methods: The outcome measure derived was based on the commonly used disease activity
measure SLEDAI-2K which documents findings over the previous 10 days. Since patients in
drug trials are followed at monthly intervals it was necessary to validate SLEDAI-2K 30 days
against SLEDAI-2K 10 days. Two prospective studies were accomplished for this purpose.
SLEDAI-2K 30 days was used to develop the new responder index, SLEDAI-2K Responder
Index-50 (SRI-50). The SRI-50 data retrieval form was developed to standardize the
documentation of the descriptors. The construct validity of SRI-50 was prospectively evaluated
against an external construct. The reliability of SRI-50 was tested in a multi-centre study. A
retrospective analysis over 10 years was used to further validate SRI-50. SRI-50 ability to
enhance the SLE Responder Index (SRI) in detecting “responders” was evaluated. The
performance of SRI-50 was investigated against SLEDAI-2K and SRI over 12 months.
Results: SLEDAI-2K 30 days was validated to describe disease activity over the previous 30
days. The responder index to SLEDAI-2K, SRI-50 was developed including the SRI-50
Definitions and SRI-50 Data Retrieval Forms. The initial validation of SRI-50 confirmed its

iii
construct validity to identify ≥ 50 % improvement. SRI-50 is reliable and can be used by both
rheumatologists and trainees. The retrospective analysis confirmed that SRI-50 is valid in
identifying ≥ 50 % improvement in an efficient time. SRI-50 enhances the performance of SRI
and identifies more “responders” than SLEDAI-2K and SRI at 6 and 12 months.
Conclusions: SRI-50, is a valid and reliable responder index to identify patients with partial,
≥50% improvement in disease activity in an efficient time. SRI-50 can be used as an independent
outcome measure of improvement in patients with SLE.

iv
Acknowledgments
First and foremost I would like to acknowledge and express my gratitude and appreciation to Dr.
Murray Urowitz and Dr. Dafna Gladman, my thesis supervisors for their guidance and
encouragement. It has been a privilege to work with them and I am very thankful for their time,
new ideas, support and for being role models and mentors. Both their energy and dedication for
their research and patients is an example that I wish to achieve in my career.
Special thanks are also extended to Dr. Earl Silverman and Dr. Edward Keystone for their help
and recommendations as members of the thesis committee.
A very special thanks must be given to the Toronto Lupus Clinic team for their help, kindness
and enthusiasm in contacting the patients and the management of the data. I am especially
grateful for Dominique Ibañez for the statistical analysis of this project. Special thanks to
Shahrzad Taghavi-Zadeh for handling the data entry related to this project. Sincere thanks and
appreciation must be extended to Anne Mackinnon who was involved directly in all aspect of the
research project.
I would also like to thank the examiners that were part of the PhD transfer exam and the PhD
oral defense committee, Dr. Brian Feldman, Dr. Gerald Devins, Dr. David Wofsy, Dr. Elizabeth
Badley and Dr. Harvey Moldofsky, for their time and insightful questions and recommendations.
I would like to thank Lupus Ontario for the Geoff Carr Fellowship and the University of
Toronto Arthritis Centre of Excellence for its fellowship award.
Lastly, I would like to thank my friends and family for all their love and encouragement who
supported me in all my pursuits.

v
Table of Contents
Acknowledgments .......................................................................................................................... iv
List of Figures, Tables and Abbreviations ................................................................................... xiv
Chapter 1 Literature Review ........................................................................................................... 1
1.1 Principles for assessing lupus patients ................................................................................ 2
1.2 Approaches to disease activity measurement in lupus ........................................................ 4
1.2.1 Global indices ......................................................................................................... 4
1.2.1.1 Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) and its
versions ................................................................................................................. 4
1.2.1.1.1 The Mexican version of SLEDAI (MEX-SLEDAI) ........................................ 7
1.2.1.1.2 SELENA-SLEDAI ........................................................................................... 7
1.2.1.1.3 SLEDAI-2000 (SLEDAI-2K) .......................................................................... 8
1.2.1.2 Systemic Lupus Activity Measure (SLAM) ......................................................... 9
1.2.1.3 European Consensus Lupus Activity Measurement (ECLAM) ......................... 10
1.2.1.4 Lupus Activity Index (LAI) ................................................................................ 11
1.2.1.5 SLE Activity Index Score (SIS) ......................................................................... 12
1.2.2 Organ Specific Indices .......................................................................................... 12
1.2.2.1 British Isles Lupus Assessment Group (BILAG) ............................................... 12
1.2.2.2 Renal outcome measures .................................................................................... 14
1.2.2.3 Cutaneous Lupus Erythematosus Disease Area and Severity Index (CLASI) ... 15
1.2.3 Measures of disease activity over time ................................................................. 16
1.2.3.1 Adjusted Mean SLEDAI-2K (AMS) .................................................................. 16
1.2.4 Disease activity in pregnancy ............................................................................... 17
1.3 Clinically meaningful change in disease activity measures .............................................. 17
1.3.1 Improvement ......................................................................................................... 17
1.3.2 Flare ...................................................................................................................... 18
1.3.3 Responder measures .............................................................................................. 19
1.3.3.1 Flares 19

vi
1.3.3.1.1 SELENA-SLEDAI Flare Index (SFI) ............................................................ 19
1.3.3.2 Improvement ....................................................................................................... 20
1.3.3.2.1 Responder Index For Lupus Erythematosus (RIFLE) ................................... 20
1.3.3.2.2 SLE Responder Index (SRI) .......................................................................... 20
1.4 The advantages and disadvantages of the most commonly used indices .......................... 21
Chapter 2 Hypotheses and Aims ................................................................................................... 23
2
2.1 Rationale ........................................................................................................................... 24
2.1.1 Results from clinical trials over the last decade .................................................... 24
2.1.2 Choice of outcome measures in SLE therapeutic trials and their impact on
results .................................................................................................................... 24
2.2 Hypothesis ......................................................................................................................... 25
2.3 Aims .................................................................................................................................. 26
Chapter 3 Validation of SLEDAI-2K 30 Days Against SLEDAI-2K 10 days in Cross-
sectional and Longitudinal Evaluation ..................................................................................... 27
3
3.1 Background ....................................................................................................................... 28
3.2 Methods ............................................................................................................................. 29
3.2.1 Patient Enrollment ................................................................................................ 29
3.2.1.1 Part 1: 29
3.2.1.2 Part 2: 29
3.2.2 Patient Assessment ................................................................................................ 29
3.2.2.1 Part 1 and Part 2: ................................................................................................ 29
3.2.3 Patient Analysis .................................................................................................... 30
3.3 Results ............................................................................................................................... 30
3.3.1 Part 1: .................................................................................................................... 30
3.3.2 Part 2: .................................................................................................................... 33
3.4 Discussion ......................................................................................................................... 37

vii
Chapter 4 Development and Initial Validation of the Systemic Lupus Erythematosus Disease
Activity Index 2000 (SLEDAI-2K) Responder Index 50 (SRI-50) ......................................... 39
4
4.1 Background ....................................................................................................................... 40
4.2 Methods ............................................................................................................................. 41
4.2.1 Derivation of SRI-50 definitions, SRI-50 data retrieval form, and SRI-50
scores ..................................................................................................................... 41
4.2.2 SRI-50 definitions ................................................................................................. 41
4.2.3 Assessment of construct validity .......................................................................... 48
4.2.4 Patient selection .................................................................................................... 48
4.2.5 Patient assessment ................................................................................................. 48
4.2.6 Clinician scoring of disease activity ..................................................................... 49
4.2.7 Method and analysis ............................................................................................. 49
4.2.8 External construct ................................................................................................. 49
4.3 Results ............................................................................................................................... 50
4.3.1 Derivation of SRI-50 definitions, SRI-50 data retrieval form, and SRI-50
score ...................................................................................................................... 50
4.3.2 Practical applicability, administration, scoring ..................................................... 51
4.3.2.1 Administration .................................................................................................... 51
4.3.2.2 Scoring ................................................................................................................ 51
4.3.3 Testing of concurrent construct validity ............................................................... 52
4.3.4 Change in SLEDAI-2K and SRI-50 scores in patients as determined by
external physician ................................................................................................. 54
4.3.5 Change in SLEDAI-2K and SRI-50 scores in patients who improved in
association with the external construct ................................................................. 55
4.4 Discussion ......................................................................................................................... 57
Chapter 5 Reliability of SRI-50 .................................................................................................... 60
5
5.1 Background ....................................................................................................................... 61

viii
5.2 Methods ............................................................................................................................. 62
5.2.1 Patient selection .................................................................................................... 62
5.2.2 Assessment of disease activity. ............................................................................. 62
5.2.2.1 SLEDAI-2K 30 days .......................................................................................... 62
5.2.2.2 SRI-50 63
5.2.2.3 Physician global assessment ............................................................................... 63
5.2.2.4 Likert scale ......................................................................................................... 64
5.2.3 “Standard” SLEDAI-2K and SRI-50 scores ......................................................... 64
5.2.4 Raters, site selection, and procedure at each site .................................................. 64
5.2.5 Statistical analysis ................................................................................................. 65
5.2.6 Sample size calculation ......................................................................................... 66
5.3 Results ............................................................................................................................... 66
5.3.1 Patient demographic data ...................................................................................... 66
5.3.2 Common pitfalls .................................................................................................... 68
5.3.3 Reliability (interrater and intrarater) ..................................................................... 70
5.4 Discussion ......................................................................................................................... 74
Chapter 6 SLEDAI-2K Responder Index (SRI-50) captures 50% improvement in disease
activity over 10 years ............................................................................................................... 77
6
6.1 Background ....................................................................................................................... 78
6.2 Methods ............................................................................................................................. 79
6.2.1 Patients’ selection and assessment ........................................................................ 79
6.2.2 Study design .......................................................................................................... 80
6.2.3 Outcome measures ................................................................................................ 80
6.2.4 Identification of patients with active descriptors .................................................. 82
6.2.5 Identification of patients’ descriptors with ≥ 50% and complete recovery .......... 82
6.2.5.1 Time to partial and complete recovery for active descriptors ............................ 82
6.2.6 Possible situations for progression in disease activity in active descriptors as
determined by SRI-50 and SLEDAI-2K ............................................................... 83

ix
6.2.7 Statistical analysis ................................................................................................. 84
6.3 Results ............................................................................................................................... 85
6.3.1 Demographics ....................................................................................................... 85
6.3.2 Partial and complete recovery in active descriptors over 10 years ....................... 85
6.3.3 Partial and complete recovery in active descriptors with 1 year .......................... 87
6.3.3.1 Time to partial and complete recovery in active descriptors over the course
of 10 years .......................................................................................................... 88
6.4 Discussion ......................................................................................................................... 90
Chapter 7 SRI-50 Enhances the Ability to Identify Responders .................................................. 92
7
7.1 Background ....................................................................................................................... 93
7.2 Methods ............................................................................................................................. 94
7.2.1 Patient enrollment and selection ........................................................................... 94
7.2.2 Outcome measures ................................................................................................ 95
7.2.3 Patient assessment ................................................................................................. 96
7.2.4 Study design .......................................................................................................... 96
7.2.5 Statistical analysis ................................................................................................. 96
7.3 Results ............................................................................................................................... 97
7.3.1 Patient demographics ............................................................................................ 97
7.3.2 Disease activity results .......................................................................................... 99
7.4 Discussion ....................................................................................................................... 102
Chapter 8 Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K)
Responder Index 50 (SRI-50): Sensitivity to Response at 6 and 12 Months ......................... 105
8
8.1 Background ..................................................................................................................... 106
8.2 Methods ........................................................................................................................... 107
8.2.1 Patients’ enrollment and selection ...................................................................... 107
8.2.2 Outcome measures .............................................................................................. 108
8.2.2.1 SLEDAI-2K ...................................................................................................... 108

x
8.2.2.2 SRI-50 (SLEDAI-2K Responder Index-50) ..................................................... 108
8.2.2.3 BILAG .............................................................................................................. 109
8.2.2.4 Physician Global Assessment ........................................................................... 109
8.2.2.5 SLE Responder Index ....................................................................................... 109
8.2.3 Patient assessment ............................................................................................... 110
8.2.3.1 Baseline visit .................................................................................................... 110
8.2.3.2 Follow up visits at 6 and 12 months ................................................................. 110
8.2.4 Treatment ............................................................................................................ 110
8.2.5 Endpoints ............................................................................................................ 110
8.2.5.1 Aim 1: Responders at 6 months and 12 months as compared to baseline visit 110
8.2.5.2 Aim 2: Determine if SRI-50 responders are true responders and not false
responders. ........................................................................................................ 111
8.2.6 Statistical analysis ............................................................................................... 111
8.3 Results ............................................................................................................................. 111
8.3.1 Patient demographics .......................................................................................... 111
8.3.2 Disease activity results ........................................................................................ 113
8.3.2.1 SLEDAI-2K and SRI-50 results ....................................................................... 113
8.3.2.2 Responders at 6 and 12 months as compared to baseline visit ......................... 116
8.3.2.3 Comparison between SRI responders “Gold Standard” and SRI-50
responders at 6 and 12 months ......................................................................... 117
8.4 Discussion ....................................................................................................................... 118
9
Chapter 9. Conclusions and Future Directions .......................................................................... 121
9.1 Achieved aims ................................................................................................................. 122
9.1.1 Validation of SLEDAI-2K 30 days ..................................................................... 122
9.1.2 Derivation and validation of SRI-50: Responder index to SLEDAI-2K ............ 122
9.1.3 Reliability of SRI-50 ........................................................................................... 123
9.1.4 SRI-50 enhances the ability of other indices to identify responders .................. 124
9.1.5 SRI-50 captures 50% improvement in disease activity over 10 years ................ 125

xi
9.2 Relevance ........................................................................................................................ 125
9.3 Future Directions ............................................................................................................ 126
10
References ................................................................................................................................... 127

xii
List of Tables
Table 1-Assessment of lupus by 5 domains .................................................................................... 3
Table 2-SLEDAI-2K (30 DAYS) ................................................................................................... 6
Table 3. Characteristics, advantages and disadvantages of the 3 commonly used disease activity
indices ................................................................................................................................... 22
Table 4. Characteristics of the 149 patients .................................................................................. 31
Table 5. Clinical and laboratory manifestations of 149 patients .................................................. 32
Table 6. Demographics of 41 patients .......................................................................................... 34
Table 7. Clinical and laboratory manifestations of SLEDAI-2K descriptors in 41 patients ........ 35
Table 8. Disease activity in different models ................................................................................ 36
Table 9. Approaches to measure disease activity ......................................................................... 43
Table 10. SLEDAI-2K Responder Index 50 (SRI-50)©
-Definitions. .......................................... 44
Table 11. Data retrieval form of SLEDAI-2K Responder Index-50 (SRI-50) ............................. 46
Table 12. Characteristics of patients ............................................................................................. 53
Table 13. Statistical results in patients whom changed their disease activity............................... 54
Table 14. Change in SLEDAI-2K and SRI-50 scores in patients who improved in association
with the external construct, the Likert scale (LS) score. ....................................................... 56
Table 15. Distribution of clinical and laboratory descriptors of SRI-50 in 40 patient profile
scenarios ................................................................................................................................ 67
Table 16. Raters mis-scorings in rounds 1 and 2 in SLEDAI-2K/SRI-50. ................................... 69
Table 17. Interrater reliability ICC (2,1) and ICC (2,k). ............................................................... 71
Table 18. Intrarater reliability and the corresponding ICC (2,1) and ICC (2,k) for each rater
separately for SLEDAI-2K, SRI-50, and PGA, and the categorical data for SLEDAI-2K and
SRI-50. .................................................................................................................................. 72
Table 19. SLEDAI-2K definitions and definitions of improvement by SRI-50 ........................... 81
Table 20. Frequency, time to partial and complete recovery among active descriptors ............... 86
Table 21. Frequency of partial and complete recovery in active descriptors within 1 year from the
onset of activity ..................................................................................................................... 87

xiii
Table 22. Time to partial and complete recovery among active descriptors in different situations
............................................................................................................................................... 89
Table 23. Characteristic of the patients ......................................................................................... 98
Table 24. Disease activity results ................................................................................................ 100
Table 25. Patients' characteristics ............................................................................................... 112
Table 26. Active SLEDAI-2K descriptors at baseline and follow-up visits at 6 and 12 months 114
Table 27. Disease activity in 103 patients at baseline visits and SLEDAI-2K, SRI-50 and SLE
Responder Index (SRI) responders ..................................................................................... 115
Table 28. Comparison between SRI responders (Gold Standard) and SRI-50 ........................... 118

xiv
List of Figures
Figure 1. Different situations for active descriptors as determined by SRI-50 and SLEDAI-2K on
follow-up visits as compared to initial visit .......................................................................... 84
Figure 2. Disease activity scores at baseline and follow-up ......................................................... 99
Figure 3. Percentage of patients who met SLE Responder Index definition .............................. 101
Figure 4. SLEDAI-2K “responders”, SLE Responder Index “responders” and SLEDAI-2K
Responder Index-50 “responders” at 6 and 12 months ....................................................... 117

xv
List of abbreviations
ACR - American College of Rheumatology
AMS - Adjusted Mean SLEDAI-2K
BILAG - British Isles Lupus Assessment Group
BLIPS - British Lupus Integrated Prospective System
BSA - Body Surface Area
CLASI - Cutaneous Lupus Erythematosus Disease Area and Severity Index
CR - Complete Recovery
ECLAM - European Consensus Lupus Activity Measurement
FDA - US Food and Drug Administration
HRQOL - Health Related Quality Of Life HRQOL
LAI- Lupus Activity Index
LS - Likert Scale
ICC - Intraclass Correlation Coefficient
OMERACT - Outcome Measures in Rheumatoid Arthritis Clinical Trials
MEX-SLEDAI - The Mexican version of SLEDAI
M-LAI - Modified LAI
m-SLAM - modified systemic lupus activity measurement
PGA - Physician Global Assessment
PAD - Persistently Active Disease
PR - Partial Recovery
PRINTO - Pediatric Rheumatology International Trial Organization
RCLASI - Revised CLASI
RIFLE - Responder Index For Lupus Erythematosus
SFI - SELENA Flare Index
SIS - SLE Activity Index Score
SLAM - Systemic Lupus Activity Measure

xvi
SLAM R - Systemic Lupus Activity Measure-Revised
SELENA - The Safety of Estrogens in Lupus Erythematosus-National Assessment Trial
SELENA-SLEDAI - National Assessment trial
SLEPDAI - Systemic Lupus Erythematosus Pregnancy Disease Activity Index
SDI - Systemic Lupus International Collaborating Clinics/American College of Rheumatology
(SLICC/ACR) Damage Index
SLEDAI - Systemic Lupus Erythematosus Disease Activity Index
SLE - Systemic Lupus Erythematosus
SLEDAI-2K - Systemic Lupus Erythematosus Disease Activity Index 2000
SRI - Systemic Lupus Erythematosus Responder Index
SRI-50 - SLEDAI-2K Responder Index-50
TCR - Time to Complete Recovery
TPR - Time to Partial Recovery
VAS - Visual Analog Scale

1
Chapter 1 Literature Review
This chapter will be published with modifications in:
Touma Z, Gladman DD, Urowitz MB. Clinical measures, metrics and indices. In: Wallace D, et
al., editors. Dubois Lupus Erythematosus, 8th Edition (In press).

2
1.1 Principles for assessing lupus patients
Systemic Lupus Erythematosus (SLE) is a protean, multisystem complex disease characterized
by remissions and exacerbations. The lupus disease course varies from flares to persistently
active disease, disease improvements to remissions [1, 2]. Lupus patients may present with
events that are related to lupus disease activity, chronic irreversible damage, and adverse events
from the medications all of which impact their quality of life. Monitoring each of these aspects is
challenging but essential for successful management of patients. The use of validated and
reliable tools is therefore fundamental for the management of lupus patients and to allow for
comparisons among lupus patients from different centers.
The assessment of lupus patients includes the determination of 5 domains: disease activity,
chronic damage resulting from lupus activity or its treatment, adverse events of drugs, health-
related quality of life (HRQOL), and economic impact (Table 1) [3]. To date, there is no
universal agreement regarding the optimal tools to be used to assess each of the 5 domains in
SLE. Whether in research or clinical care settings, investigators and rheumatologists must
identify the appropriate tools suited to the particular research or clinical needs. This chapter
focuses on describing the available measures to assess all domains in lupus patients.

3
Table 1-Assessment of lupus by 5 domains
Domains Tools Where developed Score range Time frame Ref
Disease activity
SLEDAI, its versions
and modifications
SLEDAI Toronto 0-105 Last 10 days [4]
SLEDAI-2K Toronto 0-105 Last 10 days [5]
SLEDAI-2K 30 days Toronto 0-105 Last 30 days [6, 7]
MEX-SLEDAI Mexico 0-32 Last 10 days [8, 9]
The SELENA-SLEDAI† Study investigators† 0-105 Last 10 days [10]
SRI-50 SRI-50 Toronto 0-105 Last 30 days [11]
BILAG and its version BILAG United Kingdom Categories A-E Previous month [12, 13]
BILAG 2004 United Kingdom Categories A-E Previous month [14]
SLAM and its versions SLAM Boston 0-86 Previous month [15]
SLAM-R Boston 0-81 Previous month [16]
SLAQ 0-44 Previous month [17]
ECLAM ECLAM European Union
Concerted
0-17.5
Previous month [18-20]
LAI LAI UCSF, Hopkins 0-3 Last 2 weeks [21]
SIS SIS NIH 0-52 Last week [22]
RIFLE RIFLE [23]
Damage
Physician completed SDI SLICC/ACR 0-49 Present for 6
months
[24]
Patients completed LDIQ
LDIQ Spanish, Portuguese
and French
Present for 6
months
[25, 26]
HRQOL
Generic SF-36 Boston, MA 0-100 Previous month [27]
Specific
LupusQoL
LupusQoL-US
LupusQoL Spanish
(Dutch, French, Greek,
Italian, Hyperion,
Portuguese and Chinese)
Blackburn, UK
Chicago, USA
Spain
0-100
0-100
0-100
Previous month
Previous month
Previous month
[28-30]
SLE Symptom Checklist
(SSC)
(Dutch and English)
Netherland Previous month [31]
SLE specific Quality of
Life instrument (SLEQOL)
(English, Portuguese and
Chinese)
Singapore 0-240 Previous month [32]
L-QoL
(English, Hungarian and
Turkish)
UK Previous month [33]
Adverse events
As reported by patients and or determined by physicians
Economic costs and
impact
Direct/ indirect costs, work productivity
†The SELENA-SLEDAI developed by the Study investigators in the Safety of Estrogen in Lupus Erythematosus-
National Assessment Trial and uses modified version of SLEDAI, includes flare assessment and PGA
SLEDAI-2K Responder Index-50

4
1.2 Approaches to disease activity measurement in lupus
Disease activity can be defined as a reversible clinical or laboratory manifestation, reflecting the
immunologic/inflammatory manifestation of an organ involvement from lupus at a specific point
in time [4]. The ability to quantify and grade disease activity whether in clinical practice or in
research settings, is very important. For this purpose several measures have been developed and
adopted to assess disease activity. Appropriate measures must be shown to be reliable and valid,
as well as sensitive to change. In addition, the practical applicability of the measure will include
the ease of administration, the low costs of data collection and method of scoring and ease of
score interpretation [34]. Two types of disease activity measures have been developed. Global
indices describe the overall burden of inflammatory disease while organ specific indices relate to
disease activity within each organ system, either individually, or incorporated into one summary
score.
1.2.1 Global indices
1.2.1.1 Systemic Lupus Erythematosus Disease Activity Index
(SLEDAI) and its versions
SLEDAI is a global disease activity index that was developed and introduced initially in 1985.
This index was modeled on clinicians’ global judgment. A group of experienced rheumatologists
with expertise in lupus participated in the development of this index. The use of the nominal
group process assured that the resulting index, SLEDAI, represented the consensus of the
developers. From the initial list of 37 descriptors derived from the literature that have been used
to describe disease activity in lupus, 24 “most important” descriptors, were retained for the
development of SLEDAI. The elimination of the 13 descriptors occurred in the first phase of
development (preconference ratings) that was accomplished by 15 clinicians. SLEDAI is thus
based on the presence of 24 descriptors in 9 organ systems. Based on the experts evaluation of
1400 case scenarios, multiple regression models were used to derive the weighted scores for each
descriptor. Most of the definitions of the descriptors were based on the American College of
Rheumatology glossary of rheumatic disease terms, and they were further refined throughout the

5
development process of SLEDAI [4]. The scores of the descriptors were derived from the values
obtained through the regression models and ranged from 1-8 with a total possible score of 105.
The initial validation of SLEDAI was conducted throughout the primary development phase and
descriptors were used to evaluate disease activity on the cohort database from the University of
Toronto Lupus Clinic. The descriptors in SLEDAI were precisely defined in the 10 day period
prior to the assessment within which the manifestation must be recorded [4]. The intrarater and
interrater reliability of SLEDAI was shown during the phase of development on a set of case
scenarios of lupus patients across the investigators [4]. SLEDAI has been successfully used by
rheumatologists from 4 countries in a multicenter study confirming its reliability in real patients
[35]. Furthermore, SLEDAI reproducibility was demonstrated when used in routine clinic visits
and among less experienced observers “rheumatologist trainees” in the assessment of disease
activity in lupus [21, 36]. SLEDAI was shown to correlate with other validated measures of
disease activity [21, 35]. Moreover, SLEDAI has been used in both research and clinical settings
and as a predictive variable and outcome measure in prognostic studies of lupus [21, 37, 38]. It
has also shown sensitivity to change over time and valid in the assessment of childhood lupus
[39-41]. Lupus disease activity as determined by SLEDAI was associated with increased
mortality and reduced survival in studies of lupus patients and was the major determinant of
damage accrual [42, 43]. SLEDAI at a given visit is highly prognostic for mortality in the next 6
months, with increasing relative risks of 1.28 for SLEDAI 1-5, 2.34 for SLEDAI 6-10, 4.74 for
SLEDAI 11-19, and 14.11 for SLEDAI >20 (Table 2) [44].

6
Table 2-SLEDAI-2K (30 DAYS)
(Enter weight in SLEDAI-2K Score column if descriptor is present at the time of the visit or in the preceding 30 days)
Weight SCORE Descriptor Definition
8 ❒ Seizure Recent onset, exclude metabolic, infectious or drug causes.
8 ❒ Psychosis Altered ability to function in normal activity due to severe disturbance in
the perception of reality. Include hallucinations, incoherence, marked
loose associations, impoverished thought content, marked illogical
thinking, bizarre, disorganized, or catatonic behavior. Exclude uremia
and drug causes
8 ❒ Organic brain syndrome Altered mental function with impaired orientation, memory, or other
intellectual function, with rapid onset and fluctuating clinical features,
inability to sustain attention to environment, plus at least 2 of the
following: perceptual disturbance, incoherent speech, insomnia or
daytime drowsiness, or increased or decreased psychomotor activity.
Exclude metabolic, infectious, or drug causes.
8 ❒ Visual disturbance Retinal changes of SLE. Include cytoid bodies, retinal hemorrhages,
serous exudate or hemorrhages in the choroid, or optic neuritis.
Exclude hypertension, infection, or drug causes.
8 ❒ Cranial nerve disorder New onset of sensory or motor neuropathy involving cranial nerves.
8 ❒ Lupus headache Severe, persistent headache; may be migrainous, but must be
nonresponsive to narcotic analgesia.
8 ❒ CVA New onset of cerebrovascular accident(s). Exclude arteriosclerosis.
8 ❒ Vasculitis Ulceration, gangrene, tender finger nodules, periungual infarction,
splinter hemorrhages, or biopsy or angiogram proof of vasculitis.
4 ❒ Arthritis > 2 joints with pain and signs of inflammation (i.e., tenderness, swelling
or effusion).
4 ❒ Myositis Proximal muscle aching/weakness, associated with elevated creatine
phosphokinase/aldolase or electromyogram changes or a biopsy
showing myositis.
4 ❒ Urinary casts Heme-granular or red blood cell casts.
4 ❒ Hematuria >5 red blood cells/high power field. Exclude stone, infection or other
cause.
4 ❒ Proteinuria >0.5 gram/24 hours
4 ❒ Pyuria >5 white blood cells/high power field. Exclude infection.
2 ❒ Rash Inflammatory type rash.
2 ❒ Alopecia Abnormal, patchy or diffuse loss of hair.
2 ❒ Mucosal ulcers Oral or nasal ulcerations.
2 ❒ Pleurisy Pleuritic chest pain with pleural rub or effusion, or pleural thickening.
2 ❒ Pericarditis Pericardial pain with at least 1 of the following: rub, effusion, or
electrocardiogram or echocardiogram confirmation.
2 ❒ Low complement Decrease in CH50, C3, or C4 below the lower limit of normal for testing
laboratory
2 ❒ Increased DNA binding Increased DNA binding by Farr assay above normal range for testing
laboratory.
1 ❒ Fever >38o C. Exclude infectious cause.
1 ❒ Thrombocytopenia <100,000 platelets / x109/L, exclude drug causes.
1 ❒ Leukopenia < 3,000 white blood cells / x109/L, exclude drug causes.
TOTAL
SCORE

7
1.2.1.1.1 The Mexican version of SLEDAI (MEX-SLEDAI)
In 1992 in Mexico a modification of SLEDAI was developed in an attempt to reduce the cost
inherent in a SLEDAI calculation by eliminating the laboratory tests included in SLEDAI [8].
The MEX-SLEDAI excludes immunological descriptors. Moreover, some clinical and laboratory
manifestations were added (fatigue, mononeuritis and myelitis clustered in the descriptor
neurologic disorder, peritonitis grouped with serositis, creatinine increase grouped with renal
disorder, hemolysis and lymphopenia was grouped with leukopenia) and others (lupus headache,
visual disturbance and pyuria) were excluded. The total number of variables in the MEX-
SLEDAI was reduced to 10. In addition investigators modified the definitions for few
descriptors. Different weighted scores were assigned to MEX-SLEDAI as compared to SLEDAI,
with a maximum score of 32 [8]. The MEX-SLEDAI was originally validated in Spanish-
speaking countries [8]. In 2004, for the first time the modifications of (SLEDAI-2000) SLEDAI-
2K were incorporated into the MEX-SLEDAI and applied to non-Hispanic patients [9]. MEX-
SLEDAI-2K was shown to have convergent validity with SLEDAI-2K and Systemic Lupus
Activity Measure-Revised (SLAM-R) and moderate correlation (r=0.54) with physician global
assessment (PGA) [9]. Nevertheless the sensitivity to change of the MEX-SLEDAI needs to be
further studied [8, 9]. MEX-SLEDAI has not been used extensively in clinical trials and its use is
limited to a few centers in Latin America.
1.2.1.1.2 SELENA-SLEDAI
The Safety of Estrogens in Lupus Erythematosus-National Assessment Trial (SELENA)
proposed a new modification of SLEDAI to which a composite flare outcome the SELENA-
SLEDAI Flare Index (SFI) was added [10]. In this version of SLEDAI, several descriptors were
modified. The definition of the descriptor “seizure” was modified in SELENA-SLEDAI to
exclude seizures that are due to past irreversible central nervous system damage and the
descriptor “cerebrovascular accident” was modified to exclude hypertensive causes. However
this was unnecessary as in the original SLEDAI these two descriptors are scored as present only
if the features are attributed to lupus disease activity [4]. The descriptor “visual disturbance” was
modified to include scleritis and episcleritis. This has not been validated as these features do not

8
reflect the same changes included under visual in the original SLEDAI and may not deserve a
score of 8. In the descriptor “cranial nerve disorder” the following was added “include vertigo
due to lupus” to the definition. Nevertheless, vertigo is one of the manifestation of the
vestibulocochlear cranial nerve involvement and this was intended to be reflected in the original
SLEDAI as it is one of the manifestations of the cranial nerve disturbance. The definitions of
pleurisy and pericarditis were modified by adding to the phrase “classic and severe” to ensure the
attribution of the descriptors to lupus disease activity. More importantly, SLEDAI and SLEDAI-
2K mandate the presence of subjective (pleuritic or pericardial pain) and objective (rub, effusion,
electrocardiogram or echocardiogram confirmation, or pleural thickening) findings for pleurisy
and pericarditis to be scored as present [4, 5]. In the SELENA-SLEDAI, researchers accepted
the presence of either the objective or subjective findings to score the descriptor as present [10].
In SELENA-SLEDAI arthritis is scored if more than 2 joints are active while SLEDAI-2K
defined arthritis as 2 or more actively inflamed joints as in the definition of lupus arthritis in the
ACR Glossary of terms [5, 10]. The SELENA-SLEDAI also modified the descriptor
“proteinuria” to include new onset or recent increase of proteinuria>0.5 g/24 hours to reflect
persistent active disease, as was suggested in SLEDAI-2K [5]. As in the original SLEDAI the
score ranges from 0-105 [4, 5, 10]. Despite the modifications in some of the descriptors,
SELENA-SLEDAI looks partially similar to SLEDAI-2K. It is important to highlight that there
has been no validation of all of the modifications introduced in SELENA-SLEDAI. Thus the
SELENA-SLEDAI version lacks the stringent validation steps which are an essential step before
a measure can be used in clinical trials or research settings. It is likely that the SLEDAI-2K
should serve as the SLEDAI component of the SELENA instrument, which also includes a flare
measure.
1.2.1.1.3 SLEDAI-2000 (SLEDAI-2K)
SLEDAI-2K, a modified version of SLEDAI, was introduced in 2002 and validated against
SLEDAI [5]. In the glossary of the original SLEDAI, certain descriptors were scored as active
only if they were new, thus persistently active disease was not scored. This would lead to an
apparent improvement which in fact did not occur. Among SLEDAI descriptors, skin rash,
alopecia, and mucosal ulcers had been scored only if they were new or recurrent, and in the case

9
of proteinuria if there was new onset or a recent increase of more than 0.5g/24 hours. SLEDAI-
2K was modified to allow the documentation of ongoing disease activity in the descriptors: skin
rash, alopecia, mucosal ulcers and proteinuria [4]. Thus SLEDAI-2K includes the presence of
any inflammatory rash, alopecia, or mucosal ulcers and new, recurrent, or persistent proteinuria
>0.5 g/24 hours. As in the original SLEDAI, all the descriptors in SLEDAI-2K must be
attributed to lupus activity [5]. In the validation phase of SLEDAI-2K against SLEDAI, the
entire cohort of the University of Toronto Lupus Clinic was used. Of 18636 visits, 78% of the
scores were concordant in SLEDAI-2K and SLEDAI. In the remaining 22% of the visits the
differences were due to proteinuria, rash, alopecia, and mucosal ulcers. SLEDAI-2K at
presentation was equivalent to SLEDAI at presentation as a predictor of mortality. Moreover,
SLEDAI-2K described disease activity at different activity levels in a comparable manner to the
original SLEDAI. SLEDAI-2K was equivalent to SLEDAI in describing changes in disease
activity from one visit to the next [5].
1.2.1.2 Systemic Lupus Activity Measure (SLAM)
The SLAM was introduced in Boston and was first published in 1989 to measure global disease
activity. The SLAM index uses disease manifestations derived from the American Rheumatology
Association Council on SLE and includes 32 (24 clinical, 7 laboratory and “other”) items in 11
systems with a total possible score of 86. The SLAM assesses global disease severity in the last
month [15, 16]. Most clinical and laboratory items are categorized as present or absent, and are
then scored from 0 to 3 based on the severity without considering the significance of the organ
involved [15, 16]. For instance, mild fatigue or oral ulcers will be scored similar to lupus
headache or seizure. Few items can score only 1 or 2, in particular fatigue, oral ulcers, headache,
alopecia, Raynaud’s, lymphadenopathy and hepato or splenomegaly. The SLAM-Revised
(SLAM-R) includes 23 clinical manifestations and the same 7 laboratory variables and has a
possible range of 0 – 81 with a score of 7 being considered clinically important [16]. In SLAM-R
the definitions of several items were modified in particular pleurisy, pericarditis, and
pneumonitis were dropped because of difficulty in scoring. The definitions and weighting of
fatigue, stroke syndrome, seizure and headache were modified [16]. SLAM-R does not include
immunological tests as in SLEDAI-2K. The SLAM index and its updated version SLAM-R are

10
reliable and valid in measuring disease activity when compared with other disease activity
measures and cross-culturally [15, 16]. Moreover, it was shown that the SLAM and SLAM-R
capture patients' assessments better than the other indices, and this could be explained by the
presence of subjective items in this index that reflect patients’ perception of the disease [15, 16].
The SLAM-R is a valid index for the assessment of disease activity of childhood lupus [40, 41].
A potential drawback in SLAM-R is that it includes subjective items, such as fatigue, shortness
of breath, chest pain, abdominal pain, myalgia, arthralgia which are then scored for their
severity. Although these items reflect the patients’ perception of the disease, similar to other
indices these items should only be scored if the assessor considers they are attributed to lupus
disease activity. Nevertheless, the assessment of these items has been associated with ambiguity
in research settings and clinical trials and it is not unusual to score 7 on SLAM-R for the
subjective complaints that can be misinterpreted as lupus activity. While SLAM and SLAM-R
have been used in clinical trials and research setting in the assessment of adult and childhood
lupus and are sensitive to change, the above listed drawbacks should be considered [35, 40, 41,
45].
1.2.1.3 European Consensus Lupus Activity Measurement
(ECLAM)
The ECALM was first published in 1992 by the Consensus Study Group of the European
Workshop for Rheumatology Research. The ECLAM index was developed based on the analysis
of 704 lupus patients from 29 centers in 14 countries [18-20]. The 15 items of ECLAM were
derived through univariate analysis to reflect the best clinical and laboratory features of SLE and
weighted according to their respective coefficient as determined from the multivariate regression
analyses. In the initial development and validation steps of ECLAM, the physician global
assessment was considered the criterion construct “gold standard” for lupus disease activity.
ECLAM evaluates disease activity over the previous month and the maximum possible score is
10. The ECLAM was shown to be reliable, valid, and sensitive to change when compared against
other indices including SLEDAI and British Isles Lupus Assessment Group (BILAG) [45]. The
ECLAM can be used to evaluate disease activity in patients retrospectively from the data

11
provided in clinical charts as shown in a study conducted on 64 patients [46]. The ECLAM has
been validated for the assessment of disease activity in childhood-onset disease lupus [40]. More
recently, the Pediatric Rheumatology International Trial Organization (PRINTO)/American
College of Rheumatology (ACR) Provisional Criteria for the Evaluation of Response to Therapy
for children with childhood SLE attempted to prospectively validate the provisional criteria for
the evaluation of response in children with SLE. PRINTO could not firmly choose the specific
disease activity tool for the assessment of global disease activity in lupus. The evaluated indices,
in particular SLEDAI-2K, ECLAM, SLAM-R and the BILAG, all of which performed equally in
evaluating disease activity and the differences in sensitivity and specificity between them were
very small. Although the BILAG index may have a slightly higher sensitivity than other indices,
PRINTO emphasized the complexity of the BILAG scoring system which could result in
considerable measurement error in particular when scored by less experienced and trained raters
[41]. More important, ECLAM has not been extensively used in clinical trials.
1.2.1.4 Lupus Activity Index (LAI)
The LAI was proposed in 1989 to assess the global disease activity over the previous 2 weeks
[21]. The LAI includes 5 sections, 8 organ systems and 3 laboratory measures. The physician
global assessment as well as a score for the treatment with corticosteroids and
immunosuppressive drugs are part of this index. The severity of the disease is based on the
physician judgment. The overall score reflects the mean of the physician global assessment,
physician judgment of the severity of clinical manifestations, the degree of laboratory
abnormalities, and treatment. The score of the LAI index ranges from 0 to 3 [21]. The LAI index
validity was demonstrated in a study on 150 patients where the correlation of M-LAI (LAI
modified so as not to contain PGA) was 0.64. The interrater and intrarater reliability of the LAI
was shown in a study conducted on 6 patients in routine practice [21]. The LAI performed well
in assessing disease activity when compared to other disease activity measures and is sensitive to
change; nonetheless its use has been limited as compared to other disease activity measures [45].

12
1.2.1.5 SLE Activity Index Score (SIS)
The SIS is a global disease activity index, developed by clinicians at NIH. The SIS includes 17
clinical items, based on clinical manifestations and subjective features reflecting the perception
of the patients on the disease in particular, fatigue, arthralgia and myalgia, as well as laboratory
items. The SIS is a weighted index and the score ranges from 0-52 and assesses disease activity
over the last week. The SIS categorizes disease activity into inactive, mildly active, moderately
active, active, and very active. The SIS is a valid index that has been adopted in some clinical
trials and research settings [18, 47]. The validity of the SIS index has been demonstrated against
other disease activity indices, in particular SLEDAI, SLAM, and BILAG. In this study all 4
indices were closely correlated with each other (r=0.86 between SIS and SLAM); nevertheless,
the SIS has not been used as extensively as SLEDAI and BILAG [18, 48].
1.2.2 Organ Specific Indices
1.2.2.1 British Isles Lupus Assessment Group (BILAG)
The BILAG index was proposed by a group of investigators from different centers in the United
Kingdom and its first version was published in 1988 [13]. This index was developed using a
nominal consensus approach and is based on the principle of the physician intention to treat.
BILAG includes 86 items including clinical signs, symptoms and laboratory variables in 8
systems: The items recorded must have been attributed to active lupus and present during the 4
weeks prior to the assessment [13] Based on the presence of certain features in each system, a
system is categorized into one of 4 levels: A for action; B for beware; C for content; and D for
discount [12]. The BILAG index was shown to have good between-rater reliability, and valid
when compared with the 'gold standard' criterion (starting or increasing disease-modifying
therapy) [12]. Further validation of the BILAG index showed that disease activity in different
systems in SLE does not follow a common pattern. This study recommended the use of the
individual BILAG components rather than the total BILAG score as a primary endpoint in
clinical and epidemiological studies [13]. The BILAG index sensitivity to change over time was
shown in a study on 23 patients that were followed prospectively every 2 weeks for up to 40

13
weeks, with a standardized response means of 0.57 [45]. The BILAG index was adapted and
validated in the assessment of SLE in children [40]. The BILAG index was found to be reliable
and valid in several studies conducted by the BILAG group and other investigators and
correlated with other disease activity measures in particular SLEDAI and SLAM [12, 13, 15, 39,
45, 49, 50]. The BILAG index has been successfully used in clinical trials and research settings
and particularly effective for demonstrating new organ flares [14, 35, 40, 50-53].
The Classic BILAG index has undergone a series of revisions to the current BILAG-2004 [12,
14, 15] The members of the BILAG proposed the BILAG-2004 index which included further
changes in some division of organs and systems, refinement in the definitions of some items in
particular the neurological system, removal of items attributed to damage rather than reflecting
lupus disease activity in particular avascular necrosis and tendon contracture, and modification in
the glossary and the scoring [14]. As in the Classic BILAG index, the BILAG-2004 index is
based on the physician’s intention to treat [14]. BILAG-2004 contains 97 items whereas the
classic BILAG had only 86. The system vasculitis was removed and its items were included in
other systems, and gastrointestinal and ophthalmic systems were added [14]. In the Classic
BILAG index all items that are improving can only contribute to a C score, which doesn’t reflect
the appropriate level of disease activity for more severe manifestations [14]. In BILAG-2004
index features that contribute to an A score when recorded as being the same, worse or new will
contribute to B score when improving [14].
A complete history and physical examination is required to determine disease activity by BILAG
2004. The BILAG 2004 generates a score for each of the 9 systems assessed. The scoring of
lupus disease activity in each system is graded as A-E based on the assessment of the clinical
features and/or laboratory findings for the appropriate system and representing disease activity.
Similar to the Classic BILAG index, the BILAG-2004 index is a transitional index that is able to
capture changing severity of clinical manifestations. The items in each system are rated using a
scale from 0-4 (0=not present, 1=improving, 2=same, 3=worse and 4=new), and some items are
scored as present or absent, reflecting disease activity over the past 4 weeks as compared to the
previous 4 weeks. Both the Classic BILAG index and its versions including the BILAG-2004
index are ordinal scale indices and an additive numerical scoring scheme for the BILAG-2004
index is available (A grade=12 points, B =8, C=1, D=0, and E=0) [54]. This is mainly adopted in
studies where the BILAG-2004 index needs to be compared to other numerical indices or to

14
facilitate the statistical analysis if required; nevertheless, the BILAG-2004 index was not
designed to be used this way [14, 55]. The British Lupus Integrated Prospective System (BLIPS)
includes a computerized data retrieval form and a program that calculates the BILAG scores with
the option to derive SLEDAI, SLAM-R, the Systemic Lupus International Collaborating
Clinics/American College of Rheumatology (SLICC/ACR) Damage Index (SDI), and SF-36
[56]. BLIPS has also undergone further refinement to reflect the BILAG-2004 index and several
amendments have been made to the other activity indices [14, 56].
The BILAG-2004 index was able to discriminate between patients and showed a good reliability
and high levels of physician agreement in almost all systems [14]. The reliability of the BILAG-
2004 index was evaluated in a larger study involving 11 centers across the UK with the
participation of 14 raters and 97 patients. This study showed that the BILAG-2004 is a reliable
index to assess SLE activity and recommended the training of raters to ensure its optimal
performance [57]. More recently the construct validity of the BILAG-2004 index was confirmed
by its association with ESR, C3 level, C4 level, anti-ds DNA, and more importantly SLEDAI-2K
[58]. The criterion validity of BILAG-2004, where the criterion was defined as change in
therapy, was confirmed by association between the BILAG-2004 index and the increase in
therapy [58]. In this study higher SLEDAI-2K scores were significantly associated with overall
BILAG-2004 scores reflecting higher disease activity. Although BILAG has been extensively
used in clinical trials, its routine use in long term studies has some drawbacks in particular the
practical applicability and the complicated glossary of the clinical features, and the scoring
analysis that requires a specialized computer program.
1.2.2.2 Renal outcome measures
Several renal composite outcome measures have been proposed and adopted in the assessment of
the lupus nephritis clinical trials and research studies. The measures included the quantitative
change in urinary sediments (hematuria, pyuria and cellular casts), proteinuria (24-hour urine
protein level, 24-hour urine protein: creatinine ratio and or spot urine protein/creatinine ratio)
and renal function (e.g. 24-hour creatinine clearance, estimated creatinine clearance, estimated
Cockcroft-Gault formula, and estimated glomerular filtration rate). Patients’ response using the

15
composite outcomes can be defined as either improvement (complete, partial response or no
response), reduction in renal flares or increase time to flare [59, 60]. Renal histology can be
considered to assess renal response in lupus nephritis trials whenever feasible [60].
Organ specific measures concentrate on the findings in one system and this might be critical in a
multisystem disease such as lupus, particularly when efficacy for a treatment for a particular
system such as kidney or skin is sought. If such agents are to be tested in clinical trials, it is
advisable to use the organ specific measures in association with a global disease activity measure
to evaluate lupus activity in all systems. In an effort to standardize the assessment of lupus
nephritis and optimal detection of response to treatment in clinical trials, the members of the
SLICC group in collaboration with nephrologists developed a measure of renal activity in SLE
[61]. The measure was then used to develop an SLE renal response index [61]. The renal activity
score was computed as follows: proteinuria 0.5-1 gm/day (3 points), proteinuria >1-3 gm/day (5
points), proteinuria >3 gm/day (11 points), urine red blood cell count >10/high-power field (3
points), and urine white blood cell count >10/high-power field (1 point). There was a reasonable
agreement among physician ratings in a pilot study. Nevertheless, the developers of the index
suggested further refinement, testing, and validation [61].
1.2.2.3 Cutaneous Lupus Erythematosus Disease Area and
Severity Index (CLASI)
The CLASI index was developed to facilitate the quantification of disease activity and damage of
cutaneous lupus erythematosus and was first published in 2005 [62]. The index has separate
scores for damage and activity of skin manifestations [62]. Activity is scored as a summary
score of erythema, scale/hypertrophy of the skin, mucous membrane lesions, and non-scaring
recent alopecia. Damage is scored in terms of dyspigmentation or scarring which also includes
scarring alopecia. Patients’ subjective symptoms, in particular pruritis, pain, or fatigue are
recorded separately on visual 0-10 analog scales. The total possible scores for activity and
damage are 70 and 56, respectively [62]. The CLASI has good content validity, interrater and
intrarater reliability when used by dermatologists. A recent study conducted on 14 patients with
cutaneous lupus assessed by academic rheumatologists and dermatologists showed superior

16
results with dermatologists in the use of the CLASI. Moreover, this study recommended that
rheumatologists may benefit from incorporating input from dermatologists for the use of CLASI
[63]. The revised CLASI (RCLASI) was proposed to accurately describe all types of cutaneous
lupus [64]. The RCLASI is an expanded version of the CLASI, where the accuracy of the
existing variables was increased (in particular, scaling/hypertrophy and dyspigmentation) and
new variables were added such as edema/infiltration and subcutaneous nodule/plaque [64]. The
RCLASI validity and reliability was proven amongst dermatologists only [64]. Notwithstanding,
the reliability and validity of CLASI and its versions further validation and assessment among
rheumatologists is required before it can be adopted in lupus clinical trials.
1.2.3 Measures of disease activity over time
1.2.3.1 Adjusted Mean SLEDAI-2K (AMS)
SLEDAI-2K assesses disease activity at a single point in time [5]. To summarize disease activity
over time the AMS was developed. The AMS calculates the area under the curve of SLEDAI-2K
divided by the length of the time interval [65]. The AMS has been used as a predictor of major
outcomes in lupus, including mortality, damage and coronary artery disease [65-67]. In
longitudinal studies, an increase of 1 AMS unit increased the risk for mortality by 16%, for
damage 6% and CAD by 12% [67]. A recent study evaluated whether the frequency of visits
would affect the accuracy of estimating the AMS. This study showed that when groups of
patients are analyzed, the frequency of visits within 1 year (quarterly, semi-annually or annually)
does not have a significant effect on the AMS. However in individual patients only visits up to 3
months apart provided an accurate estimation of disease activity over time and visits beyond 3
months compromised this measure [68]. AMS has an important role in measuring disease
activity over time in addition to its prognostic value especially in patients with prolonged follow-
up in longitudinal studies.

17
1.2.4 Disease activity in pregnancy
The assessment of lupus during pregnancy is affected by the physiological changes that influence
the clinical manifestation and laboratory tests of lupus. Since 1999 several lupus activity scales
have been adapted for pregnancy in particular systemic lupus erythematosus pregnancy disease
activity index (SLEPDAI), modified lupus activity measurement (m-SLAM) and lupus activity
index in pregnancy (LAI-P) [69]. Nevertheless demonstrating reliability and validity of these
modifications is fundamental before their use in clinical trials and research studies [69].
1.3 Clinically meaningful change in disease activity measures
1.3.1 Improvement
Improvement has been accepted as a very important and relevant outcome measure in clinical
trials. At present improvement is defined based on disease activity measures, in particular
SLEDAI-2K and BILAG as follows: improvement is a reduction in SLEDAI-2K ≥ 4 or reduction
in the BILAG scores [38]. A major clinical response by BILAG is a BILAG C score or better at
6 months with no new BILAG A or BILAG B scores and maintenance of response with no new
BILAG A or B scores between 6 and 12 months [60]. While the BILAG-2004 was significantly
associated with decrease in therapy with major improvement from Grade A/B to C/D, it was not
definitively responsive to improvement in disease activity from very active to moderately active
(Grade A to B). In fact a reduction from grade A to B is not always reflected by a reduction in
therapy. This led the authors to recommend that clinical trials using the BILAG-2004 index
should use the efficacy criteria of improvement to low level activity (Grade C/D) as the main
outcome, instead of improvement from Grade A to B [70].
Although SLEDAI-2K has been used to define improvement in disease activity it is important to
highlight that SLEDAI-2K captures improvement in the descriptors that resolve completely. This
led to the development of a novel index based on SLEDAI-2K, SRI-50, that measures partial
clinically important, ≥ 50%, improvement in disease activity [11].

18
1.3.2 Flare
Flare is considered as one of the most commonly used outcome measures of disease activity.
Flare is defined as an increase in SLEDAI-2K ≥ 4 points, an increase in SELENA-SLEDAI score
of ≥ 3 points, or 1 new category A or 2 new B grades on BILAG index [38, 50, 71]. In terms of
specific flare indices, the SELENA researchers proposed initially the SFI and more recently the
revised SFI version in an effort to differentiate mild and moderate flare [71, 72]. The revised SFI
suggested specific clinical manifestations for each organ-system and categorized flares (mild,
moderate and severe) based on the treatment decision [71]. A recent study evaluated mild,
moderate and severe flares individually and showed that the intraclass correlation coefficients is
0.54, 0.21 and 0.18 for BILAG-2004 flare, SELENA flare and PGA flare, respectively [71]. The
results of this study highlight the difficulty in the distinction between mild and moderate flares
and the results among the examiners were much less consistent despite using the new SFI
version [71]. Similarly the separation between mild and moderate flare remains problematic even
with the use of the BILAG-2004 index [70]. More importantly, it was found that the BILAG-
2004 index appears to perform better at detecting increase in disease activity as compared with
improvement in disease activity. This led the authors to recommend BILAG-2004 index to be
used in longitudinal studies that aim to determine in particular worsening in disease activity.
Moreover, the renal scoring in BILAG-2004 is powered to detect new onset of lupus nephritis or
significant improvement (Grade C/D) and it is advisable to use more specific criteria to define
response in longitudinal studies on lupus nephritis and ultimately clinical trials [70].
Besides flare, SLEDAI-2K scores are used to define persistently active disease (PAD) with a
SLEDAI-2K score changes of < 4 between visits and remission as a SLEDAI of 0. A recent
study from the Lupus Clinic in Toronto showed that among 417 patients, one-third of the patients
had ≥ 1 flare, whereas nearly half experienced PAD in a given year. Nearly 60% of the patients
had episodes of flare or PAD per year. At least 25% of patients had PAD without achieving the
definition of flare where SLEDAI-2K scores at the start of the outcome interval and prior
cutaneous or musculoskeletal disease activity predicted PAD. Although flare has been
considered the most commonly used outcome measure to describe worsening in disease activity,
PAD also is a common disease state in lupus patients with active disease and should be used in
clinical and research settings.

19
1.3.3 Responder measures
Improvement and flare are considered clinically meaningful changes in disease activity, as
compared to baseline, that can be determined with the use of appropriate tools. Of the validated
tools, SLEDAI-2K and its versions and BILAG along with other measures have been most
adopted in clinical trials to define these concepts [5, 10, 12]. Time to flare, the numbers of flares
and the severity of flare in particular mild/moderate and severe flare have been used as outcome
measures in clinical trials.
1.3.3.1 Flares
1.3.3.1.1 SELENA-SLEDAI Flare Index (SFI)
SFI was proposed by the SELENA trials investigators to define SLE flares which are an
important outcome measure in clinical trials [72]. The original SFI proposed mild/moderate and
severe flares and this separation was applied in a number of RCTs [1, 73]. SFI is a composite
outcome of SELENA-SLEDAI, mild/moderate and severe flares, and the physician’s global
assessment (PGA) (PGA; 0=none, 1=mild, 2=moderate, 3=severe) of disease activity [73]. In a
study conducted on patient scenarios the reliability of the SFI for severe flares was substantial
(k=0.65) and fair (K=0.16) for mild/moderate flares [72]. The developers of SFI showed that the
training of the examiners on SFI improves its performance in particular for mild/moderate
(k=0.54) [72]. Furthermore, a different group evaluated the reliability and the validity of
SELENA-SLEDAI, PGA, and SFI retrospectively on patients’ charts. This group found that
PGA and SELENA-SLEDAI components of SFI are more reliable and valid than the SFI. Both
intrarater and interrater reliability of PGA, SELENA-SLEDAI performed better than SFI [74].
Moreover, PGA, SELENA-SLEDAI demonstrated adequate agreement against each other;
however, SFI demonstrated poor agreement with PGA-defined flare and SELENA-SLEDAI-
defined flare. PGA-defined flare or SELENA-SLEDAI-defined flare also demonstrated poor
agreement. This study raises a question regarding the validity of SFI; nevertheless, the authors
explained that the inadequate performance of SFI could have been related to the method of
retrospective chart abstraction and the study design [74]. With the advances in treatment in

20
lupus the SELENA researchers realized that it is important to distinguish between mild and
moderate disease activity in clinical trials and proposed the revised version of SFI [71]. The
revised SFI suggested specific clinical manifestations for each organ-system and categorized
flares (mild, moderate and severe) based on the treatment decision. In this new version of SFI, 2
of the major components of the original SFI; PGA and SELENA-SLEDAI, were excluded [71].
1.3.3.2 Improvement
1.3.3.2.1 Responder Index For Lupus Erythematosus (RIFLE)
The RIFLE was developed to measure partial and complete responses to therapy in particular in
clinical trials [23]. The RIFLE is a reliable and valid index, able to detect considerable variation
in disease activity and sensitive to change in important disease activity over time [23]. The
RIFLE characterized patients based on their SLE manifestations into: worsening, present/no
change, partial response, resolution and not present [23]. The RIFLE has been used in clinical
trials and research studies [61, 75]. A recent study evaluated the minimal clinically important
differences of validated measures of lupus disease activity in childhood-onset SLE. This study
showed that the RIFLE appears to be less useful for the assessment of childhood-onset SLE than
for adult onset SLE as compared to SLEDAI-2K, SLAM-R, ECLAM and BILAG [76].
1.3.3.2.2 SLE Responder Index (SRI)
Evidence-based exploratory analysis of the B lymphocyte stimulating factor antagonist,
belimumab in a phase II SLE trial led to the development of a novel responder index, the SLE
Responder Index (SRI to define a clinically meaningful change in disease activity) [52]. SRI is a
composite outcome that incorporates the modification of SLEDAI, SELENA-SLEDAI, the
BILAG index, and the Physician’s Global Assessment (PGA) [4, 10, 12, 49]. As proposed by
the authors of SRI, the “SELENA-SLEDAI” score was used to determine global improvement.
The BILAG domain scores were utilized to ensure that no significant worsening in heretofore
unaffected organ systems has occurred. The PGA ensured that improvement in disease activity is

21
not achieved at the expense of the patient’s overall condition [52] . SRI was initially assessed in
a subset of 321 serologically active lupus patients in a phase II belimumab placebo-controlled
clinical trial. In serologically active patients, the addition of belimumab to concomitant standard
of care therapy resulted in a statistically significant response in 46% of patients at week 52
compared with 29% of the placebo patients [52]. More recently, a randomised, placebo-
controlled, phase 3 trial used this novel 3 part outcome response measure and demonstrated a
statistically significant difference in responders in patients on belimumab as compared to placebo
[77]. In the epratuzumab trial, researchers proposed a modification of the SRI whereby the
BILAG index is to be used to define primary improvement, while SLEDAI and PGA are used to
indicate that no deterioration in disease activity has occurred [78].
1.4 The advantages and disadvantages of the most commonly
used indices
With the remarkable advances in biology and the growing number of new therapeutic agents
with potentially lower toxicity it is important to be able to measure a clinically important
improvement in disease activity in response to treatment. The 6 most commonly used disease
activity indices have been grouped into global or organ-based indices as described in the first
chapter. Of these indices, the most commonly used in research settings and clinical trials are
SLEDAI-2K and BILAG and to a lesser extent SLAM-R. The advantages and disadvantages of
these 3 indices in represented in table 3.

22
Table 3. Characteristics, advantages and disadvantages of the 3 commonly used disease activity indices
Strengths and Characteristics Weaknesses
SLEDAI-
2K
-Involve 9 organ systems [79].
-A complete history and examination is needed. For
most patients it takes 10-20 minutes.
-Refers to disease activity during previous 10 days.
-The method of scoring is simple and additive [5].
The score is derived during patient evaluation.
-SLEDAI is able to detect differences between visits
[5, 21, 36].
-Excellent sensitivity and responsiveness to change
have been shown in comparative studies with BILAG
and SLAM.
-There is no cost to use SLEDAI and it is been adopted
by most CRT and clinical trials.
-SLEDAI can be successfully used by both expert
clinicians and trainees [36].
-SLEDAI-2K can detect only 100%
improvement of the features thus it cannot
reflect partial improvement in a disease
manifestation [5].
-Worsening of already existing features is not
detected by SLEDAI-2K.
BILAG -BILAG involves 9 organ systems and generates a
score for each system [13, 14].
-A complete history and examination is needed. For
most patients it takes <10 minutes.
-BILAG is based on physician “intention to treat”.
Refers to disease activity during previous month.
-A computer program facilitates scoring from
numerical to alphabetical scores.
-Excellent sensitivity and responsiveness to change
have been shown in comparative studies with BILAG
and SLAM.
-Although BILAG can capture partial change it
does not provide enough information about each
system (e.g. joint count).
-BILAG may not distinguish between the
patients with one active clinical feature (discoid
rash) from another patient with a combination of
clinical features in the same system; e.g. oral
ulcers, rash and alopecia.
-BILAG is expensive and requires computer
facilitation for scoring from numerical to
alphabetical scores.
-BILAG is time consuming and not user friendly
to clinicians that are not familiar with the
instrument.
SLAM-R -Involves 11 organs and 8 laboratory manifestations.
-A complete history and examination is needed. For
most patients it takes <10 minutes.
-The method of scoring of SLAM-R is simple and
additive.
-It has no associated cost to use.
-It correlates with several aspects of the patient
perception of health as evaluated with SF-36 [16].
-Refers to disease activity during previous month.
-It gives equal weighting to mild and serious
organ disease activity irrespective of the
significance of the involved organ.
-Many items are subjective and not necessarily
related to lupus disease activity (arthralgias,
myalgias, abdominal pain & fatigue) which
might falsely increase the total score.
-SLAM-R groups all cutaneous variables in the
same group and does not allow differentiating
between them.
This chapter will be published with modifications in:
Touma Z, Gladman DD, Urowitz MB. Clinical measures, metrics and indices. In: Wallace D, et
al., editors. Dubois Lupus Erythematosus, 8th Edition (In press).

23
Chapter 2 Hypotheses and Aims

24
2.1 Rationale
2.1.1 Results from clinical trials over the last decade
Cyclophosphamide [80] and steroids have been widely considered the standard of care for lupus
nephritis in many centers throughout the world [81-83]. In fact cyclophosphamide has not been
approved as therapy for lupus nephritis by any of the drug regulatory agencies [84]. Further,
meta-analyses indicate that immunosuppressive drugs, (azathiopirine or cyclophosphamide), and
steroids together are more effective than steroids alone in treating active lupus nephritis [85].
Since then a number of new agents have been introduced and are in various phases of drug
development. Subsequently, SLE patients were allocated to different clinical trials, studying and
comparing the immunosuppressive medications and the new biological agents;
cyclophosphamide, mycophenolate mofetil, anti-CD20 chimeric monoclonal antibodies
(Rituximab), anti-CD22 (epratuzumab), anti-B lymphocyte (BLyS) (Belimumab), anti-CD40L
monoclonal antibodies, LJP 394 treatment (Abetimus sodium), CTLA-4 Ig (Orencia) and
dehydroepiandrosterone (DHEA) [82, 84-86]. It is very important to note that despite the
development of new therapeutic agents none have so far been approved by the FDA and none
have achieved their primary outcome except for the most recent Belimumab study [52]. Using a
combination of responses the 52 and 76 week Belimumab trials achieved their primary endpoints
[52, 87]. Although the results of the previous studies were disappointing, it would be premature
to conclude that these therapeutic strategies cannot be effective in SLE. Indeed, the lack of a
robust responder index for global disease activity in SLE patients is a serious limitation when
designing clinical trials.
2.1.2 Choice of outcome measures in SLE therapeutic trials and their
impact on results
The assessment of disease activity in lupus patients is fundamental and central in disease
management. Due to the diversity of clinical features and the relapsing-remitting course of
disease in SLE patients, it has been difficult to devise a single instrument to evaluate change in
disease status. This led the investigators to adopt composite outcome measures in clinical trials

25
such as SLE Responder Index and others. Although the current validated disease activity indices
have been used to measure improvement in clinical trials, none of them was designed as an
adequate responder index for evaluation of therapies for SLE.
SLEDAI-2K is one of the most commonly used disease activity measures in longitudinal
observational studies and clinical trials. The practical applicability of SLEDAI-2K in clinical
settings, ease of administration and simplicity in scoring are fundamental properties. .
Nevertheless, SLEDAI and its version, SLEDAI-2K, share the same disadvantages by missing a
signal toward improvement as the instrument records only complete resolution of a disease
manifestation. In the current adopted outcomes for the assessment of disease activity in
rheumatoid arthritis and psoriatic arthritis, an improvement is based on the decrease in the
severity of the manifestations and this is reflected by the decrease in the joint count and not
necessarily a complete resolution of arthritis. This approach should also be applied to lupus
patients so that physicians would able to measure a clinically meaningful improvement in each of
the manifestations in a standardized way.
I am aware that several standardized reliable and validated indices assessing the disease activity
in SLE patients have already been developed. Despite the availability of these numerous indices,
the valid ones do not adequately describe improvement in response to new therapies. Therefore
in this thesis I propose to describe the derivation of an appropriate outcome measure, specifically
a responder index to SLEDAI-2K.
2.2 Hypothesis
I hypothesized that an instrument to identify partial, ≥50%, clinically important improvement in
disease activity could be developed based on the SLEDAI-2K and that the newly developed
responder index, SLEDAI-2K Responder Index-50 (SRI-50) will better identify patients with
clinically important improvement in lupus disease activity.
Additionally, I hypothesized that SRI-50 will be a responder sensitive to partial improvement in
disease activity over a 6 and 12 month period, the usual time frame in clinical trials.

26
2.3 Aims
1) To validate Systemic Lupus Erythematosus Disease Activity Index-2000 (SLEDAI-2K) 30
days against SLEDAI-2K 10 days in patients with a spectrum of disease activity levels over
a 12 month period (Chapter 3).
2) To describe the development of the new responder index, SLEDAI-2K Responder Index-50
(SRI-50) (Chapter 4).
3) To evaluate the concurrent construct validity of SRI-50 (Chapter 4).
4) To test the intrarater and interrater reliability of SRI-50 among rheumatologists and
rheumatology fellows in training (Chapter 5).
5) To determine the frequency and time to partial and complete recovery in the descriptors of
SRI-50 over 10 years: Retrospective validation of 3 Organ Systems of SRI-50 (Chapter 6).
6) To test whether SRI-50 will enhance the ability of Systemic Lupus Erythematosus
Responder Index (SRI) to identify responders (Chapter 7).
7) To determine the sensitivity to response at 6 and 12 month period of SRI-50 (Chapter 8).

27
Chapter 3 Validation of SLEDAI-2K 30 Days Against SLEDAI-2K
10 days in Cross-sectional and Longitudinal Evaluation
These 2 papers have been published:
1- Touma Z, Gladman DD, Urowitz MB. SLEDAI-2K for a 30 day window. Lupus
2010;19:49-51. [6]
2- Touma Z, Urowitz MB, Ibañez D, Gladman DD. SLEDAI-2K 10 days versus SLEDAI-
2K 30 days in a longitudinal evaluation. Lupus 2011;20:67-70. [7]

28
3.1 Background
In 1985 the Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) was first
developed to standardize and measure disease activity in SLE patients in the previous 10 days.
This index was modeled on clinicians’ global judgment. It was developed with a panel of
experienced rheumatologists with expertise in SLE, using well established group techniques and
index development methods [4].
SLEDAI has been validated as a clinical index for SLE patients and has been used as a global
measure of disease activity in SLE since its introduction in 1985 [4]. The index has been used
successfully by both expert clinicians and trainees, and has been shown to be valuable in both
research and clinical settings [21, 35-37]. SLEDAI has also been shown to be sensitive to change
in disease activity over time [39].
In 2002 a revised version of SLEDAI, SLEDAI-2000 (SLEDAI-2K), was proposed in which the
persistent active disease in the items alopecia, mucous membrane ulcers, rash, and proteinuria
would be scored [5]. SLEDAI-2K was validated against the original SLEDAI and shown to be a
predictor of mortality and to describe disease activity at various activity levels in a comparable
manner to the original SLEDAI. SLEDAI-2K was equivalent to SLEDAI in describing changes
in disease activity from one visit to the next. SLEDAI-2K has been used for the assessment of
global disease activity in SLE [5]. The 10-day period was still retained [5].
Other major disease activity indices for SLE measure disease activity in the preceding 30 days
[16, 18, 79]. Since the usual time frame of observations within a clinical trial is 30 days, it was
relevant to determine whether a 30-day window would be similar to the 10-day window
originally identified for the SLEDAI.
The aims of this study were to compare: 1) SLEDAI-2K scores when both a 10 day and a 30 day
window were used in a cross-sectional design conducted over 9 weeks on all consecutive lupus
patients seen at the clinic and 2) SLEDAI-2K scores when both a 10 day and a 30 day window
were used in a longitudinal design evaluating a group of patients monthly over 1 year.

29
3.2 Methods
3.2.1 Patient Enrollment
3.2.1.1 Part 1:
Consecutive patients seen in the University of Toronto Lupus Clinic over 9 weeks were included.
All patients had ≥ 4 American College of Rheumatology (ACR) criteria or 3 ACR criteria plus a
typical histological lesion of SLE on renal or skin biopsy [88].
3.2.1.2 Part 2:
Forty one patients seen in The University of Toronto Lupus Clinic were followed at monthly
intervals for 12 months. All patients had ≥ 4 American College of Rheumatology (ACR) criteria
[88]. We enrolled patients who experienced lupus flare over the previous year (flare was defined
as an increase of ≥4 in SLEDAI-2K from the previous visit) and on <20mg/day of prednisone at
the 1st visit in this study.
3.2.2 Patient Assessment
3.2.2.1 Part 1 and Part 2:
A complete history, physical examination and laboratory tests were performed for all patients to
allow the determination of SLEDAI-2K. The SLEDAI-2K score was completed twice, once for a
10-day window and the second for a 30-day window using the same definitions for the
descriptors [5]. Patient in the longitudinal study underwent a complete history, physical
examination and laboratory tests on each visit, monthly, over 12 months.

30
3.2.3 Patient Analysis
We determined the number of total SLEDAI-2K score discrepancies between 10 and 30 days
window in all patient-visits (Part 1 and Part 2).
In the group of patients followed over 1 year (Part 2), we also assessed changes in disease
activity in all patient-visits including flare (≥4 in SLEDAI-2K from the previous visit),
improvement (reduction in SLEDAI-2K >3), remission (SLEDAI-2 of 0), persistently active
disease (SLEDAI-2K ≥4, excluding serology alone, on ≥2 consecutive visits) and unchanged
disease activity (group of patients who did not meet any of the above models for disease activity)
[2].
3.3 Results
3.3.1 Part 1:
Patients’ demographics:
One hundred and forty nine lupus patients seen over 9 weeks were enrolled. The majority of the
149 patients were female (89%) with a mean age of 33 ± 14 years. Sixty-two percent of the
patients were Caucasian, 19% Black, 10% Asian, and the remainder was other ethnicities. The
age at the time of the study visit was 45 ± 15 years and disease duration at study visit in the study
was 14 ± 10 years. The Systemic Lupus International Collaborating Clinics/ACR Damage Index
(SDI) at the study visit was 1.57 ± 2.00. The characteristics of these patients are reflected in table
4.

31
Table 4. Characteristics of the 149 patients
Sex Female 89 %
Age at diagnosis (year) 33 ±14
Race
Caucasian 62%
Black 19%
Asian 10%
Other 9%
Age at the time of the study (year) 45.0 ± 15.2
Disease Duration at 1st visit in the study (year) 14.0 ± 10.1
SDI at 1st visit in the study 1.57 ± 2.00
SDI, Systemic Lupus International Collaborating Clinics/ACR Damage Index
SLEDAI-2K 10 and 30 days results: Of the 149 lupus patients assessed 40 had a SLEDAI-2K of
0. One hundred and nine patients had varying levels of disease activity (3 had SLEDAI-2K of 1;
34 had 2; 24 had 4; 6 had 5; 13 had 6; 9 had 8, 8 had 10, 2 had 12, 1 had 13, 1 had 14, 1 had 16,
5 had 20, 1 had 23 and 1 had 31). The spread of manifestations was demonstrated in 17 of the 24
descriptors and in 7 of the 9 organ systems covered by SLEDAI-2K. The clinical and laboratory
findings of SLEDAI-2K are reflected in table 5.

32
Table 5. Clinical and laboratory manifestations of 149 patients
Clinical
descriptors
Patients
number (%)
Laboratory
descriptors
Patients
number (%)
Seizure 2 (1.3%) Casts 15 (10.1%)
Psychosis 1 (0.7%) Hematuria 10 (10.1%)
Headache 2 (1.3%) Proteinuria 15 (10.1%)
Vasculitis 3 (2.0%) Pyuria 8 (5.4%)
Arthritis 13 (8.7%) Low complement 59 (39.6%)
Rash 14 (9.4%) Increased DNA 68 (45.6%)
Alopecia 15 (10.1%) Thrombocytopenia 3 (2.0%)
Mucosal Ulcers 7 (4.7%) Leukopenia 9 (6.0%)
Pericarditis 1 (0.7%)
In all but 1 patient there was agreement between the SLEDAI-2K 10 and 30 days. This patient
experienced inflammatory skin rash from day -21 to -30 prior to his visit and the use of local
steroid resulted in total resolution of the findings.

33
3.3.2 Part 2:
Patients’ demographics:
Forty one lupus patients seen monthly over 12 months were enrolled. Among the 41 patients 37
were female and 4 were male. Four hundred and nineteen patient-visits in 41 patients were
recorded for SLEDAI-2K for a 10-day and a 30-day window. Among the 41 patients 90% were
female, 56% Caucasian, 17% Black, 7% Asians, and 20% other races. The mean age at SLE
diagnosis was 30.5±10.3 years, age at 1st study visit was 45.4±13.2 years and disease duration at
1st study visit was 14.8±10.3 years. The Systemic Lupus International Collaborating
Clinics/ACR Damage Index at 1st visit in study was 1.57±2.00 (Table 6). The treatment of the
patient at 1st visit is described in table 1 [24].

34
Table 6. Demographics of 41 patients
Sex Female 90 %
Age at diagnosis (year) 30.5±10.3
Age at the time of the study (year) 45.3±13.2
Disease Duration at 1st visit in the study (year) 14.8 ± 10.3
Race Caucasian 56%
Black 17%
Asian 7%
Other 20%
SDI * at 1st visit in the study 1.57 ± 2.00
AMS during study period 2.29 ± 1.83
¥ Prednisone number (% of patients)
mean dose (mg)
26 (63.4%)
dose 8.7 ± 5.8
¥ Anti-malarial number (% of patients)
Chloroquine number
mean dose (mg)
Hydroxychloroquine number
mean dose (mg)
36 (87.8%)
9
218 ± 70
29
324 ± 70
¥ Immunosuppressants number (%)
AZA number of patients (dose mg)
MTX number of patients (dose mg)
MMF number of patients (dose mg)
22 (53.7%)
9 (113 ± 25)
5 (18.8 ± 3.9)
5 (2290 ± 560)
*SDI, The Systemic Lupus International Collaborating Clinics/ACR Damage Index; ¥ Treatment of the
patients at 1st study visit

35
Of the 419 patient-visits 151 patient-visits had a SLEDAI-2K of 0. Two hundred sixty eight
patient-visits had varying levels of disease activity ranging from 1-15 (3 patient-visits had
SLEDAI-2K of 1; 133 had 2, 2 had 3, 68 had 4, 9 had 5, 35 had 6, 11 had 8, 4 had 10, 2 had 12
and 1 had 15).
The spectrum of manifestations demonstrated occurred in 14 of the 24 descriptors and in 7 of the
9 organ systems assessed by SLEDAI-2K. The clinical and laboratory descriptors of SLEDAI-
2K seen are shown in table 7. The Adjusted Mean SLEDAI-2K (AMS) during the study period
was 2.29±1.83.
Table 7. Clinical and laboratory manifestations of SLEDAI-2K descriptors in 41 patients
Clinical descriptors Patient-visits
number (%)
Laboratory
descriptors
Patients-visits
number (%)
Seizure 2 (0.5%) Hematuria 7 (1.7%)
Headache 2 (0.5%) Proteinuria 12 (2.9%)
Vasculitis 2 (0.5%) Pyuria 8 (1.9%)
Arthritis 20 (4.8%) Low complement 122 (29.2%)
Rash 37 (8.9%) Increased DNA 179 (42.8%)
Alopecia 10 (2.4%) Thrombocytopenia 3 (0.7%)
Mucosal Ulcers 11 (2.6%) Leukopenia 14 (3.4%)

36
Fourteen patient-visits had flare, 15 patient-visits showed improvement, 156 went into remission,
8 patient-visits had persistently active disease and 231 patient-visits had unchanged disease
activity (Table 8).
Table 8. Disease activity in different models
Models Definition Number patients-
visits
Patients-visits flare ≥4 in SLEDAI-2K from the previous
visit
14
Patients-visits improvement Reduction in SLEDAI-2K > 3 15
Remission SLEDAI-2K of 0 151
Persistently active disease SLEDAI-2K ≥4, excluding serology
alone, on ≥2 consecutive visits
8
Unchanged Patients who did not meet any of the
above models
231
In all but one patient-visit there was an agreement between the SLEDAI-2K 10 and 30 days. The
discordant patient experienced skin rash as a minor lupus flare, however in the last 10 days prior
to the visit his rash completely faded.

37
3.4 Discussion
The assessment of disease activity in lupus patients is complex. This is related to its variable
disease course, manifestations in more than one organ system, and co-morbidities which could
be related to the sequelae of lupus or as side effects from medications used in the treatment of
lupus. A number of disease activity indices have been developed to score disease activity in SLE
[4, 5, 12, 16, 18, 22, 45, 46]. These include global indices such as the SLEDAI and its
modification, the Safety of Estrogens in Lupus Erythematosus-National Assessment Trial version
of SLEDAI (SELENA-SLEDAI) [13], Systemic Lupus Activity Measure (SLAM) and the
modified version (SLAM-R) [10], European Consensus Lupus Activity Measurement (ECLAM)
[9,12], Lupus Activity Index (LAI) [4], SLE Activity Index Score (SIS) [14], and organ-based
indices such as the British Isle Lupus Assessment Group (BILAG) index [4, 5, 10, 12, 14, 16, 18,
22, 45, 46] These indices have been validated against each other and were shown to be reliable
and sensitive to change in disease activity over time [18, 45]. BILAG and SLAM-R are based on
the presence of items at the time of the visit or in the preceding 30 days [12, 14, 16]. SLEDAI-
2K and SELENA-SLEDAI document descriptors present at the time of the visit or the preceding
10 days [5, 73]. However, both SLEDAI-2K and SELENA-SLEDAI have been used in clinical
studies and clinical trials documenting features over the past 30 days to make them comparable
with other disease activity indices.
This study confirmed that SLEDAI-2K scores 10 days were concordant with SLEDAI-2K 30
days scores in the cross sectional design on 149 patients and in the longitudinal assessment of 41
patients that were followed monthly over 1 year. SLEDAI-2K 10-days scores were concordant
with SLEDAI-2K 30-days scores, both in patients in remission and in patients with a spectrum of
disease activity.
The results of this study confirmed that it is unusual to have a manifestation of active lupus
present at -11 to -30 days prior to a visit and have complete resolution in the 10 days prior to the
visit. Our study shows that this is true over a period of 1 year, over a wide spectrum of SLEDAI-
2K values from inactive to active and in patients with persistently active disease, flare,
improvement and remission.

38
In conclusion, SLEDAI-2K 30 days was validated against SLEDAI-2K 10 and may now be used
to describe disease activity over the previous 30 days. We recommend the use of SLEDAI-2K 30
days in clinical studies and clinical trials to describe disease activity over the previous 30 days.
These 2 papers have been published:
3- Touma Z, Gladman DD, Urowitz MB. SLEDAI-2K for a 30 day window. Lupus
2010;19:49-51. [6]
4- Touma Z, Urowitz MB, Ibañez D, Gladman DD. SLEDAI-2K 10 days versus SLEDAI-
2K 30 days in a longitudinal evaluation. Lupus 2011;20:67-70. [7]

39
Chapter 4 Development and Initial Validation of the Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K) Responder Index 50 (SRI-50)
I-This paper has been published:
Touma Z, Gladman DD, Ibañez D, Urowitz MB. Development and Initial Validation of
SLEDAI-2K (Systemic Lupus Erythematosus Disease Activity Index 2000) Responder Index-50
(SRI-50). J Rheumatol 2011;38:275-84. [11]
II-Patents and Intellectual Property Rights related to SRI-50:
1. SRI-50 Manual
Touma Z, Gladman DD, Mackinnon A, Urowitz MB. SLEDAI-2K Responder Index-50
(SRI-50) Manual. July 2010 (Available online; www.sri-50.com).
2. SRI-50 Website
Touma Z, Gladman DD, Mackinnon A, Urowitz MB. SLEDAI-2K Responder Index-50
(SRI-50) Website July 2010 www.sri-50.com

40
4.1 Background
Systemic lupus erythematosus (SLE) is a complex disease characterized by various clinical
manifestations that can be related to acute disease activity or to chronic damage, which makes
the disease difficult to monitor. In 1998, Outcome Measures in Rheumatoid Arthritis Clinical
Trials (OMERACT) 4 recommended that 5 domains be assessed in all SLE clinical trials and
longitudinal observational cohort studies: disease activity, damage resulting from lupus activity
or its therapy, health related quality of life, adverse events, and economic costs including health
utilities [89, 90].
Disease activity is defined as a reversible manifestation of the underlying inflammatory process
and is a reflection of the type and severity of organ involvement at each point in time [4]. The
assessment of disease activity depends on the use of standardized, reliable, and validated indices.
For this purpose several indices for scoring disease activity in SLE are currently used [4-7, 10,
12-14, 16, 22, 46, 89, 90]. Of those that have been validated, 2 indices, Systemic Lupus
Erythematosus Disease Activity Index (SLEDAI) and British Isles Lupus Assessment Group
Index (BILAG), have been used most in clinical trials and have undergone changes to assure
optimal performance in clinical and research settings [4, 14].
SLEDAI is a global index that was developed and validated and introduced in 1985 as a clinical
index for disease activity. This index was modeled on clinicians’ global judgment. It was
developed with a panel of experienced rheumatologists with expertise in SLE, using well
established group techniques and index development methods. SLEDAI is based on the presence
of 24 features in 9 organ systems and measures disease activity in SLE patients in the previous
10 days [5]. SLEDAI has been used successfully by both expert clinicians and trainees, and has
been adopted in both research and clinical settings [39, 90]. SLEDAI is sensitive to change in
disease activity over time [39]. In 2002 a revised version of SLEDAI, SLEDAI-2000 (SLEDAI-
2K), was introduced, in which the persistent ongoing active disease in the items rash, alopecia,
mucosal ulcers, and proteinuria would be scored, as opposed to only new occurrences as in the
original SLEDAI [5]. SLEDAI-2K was validated against the original SLEDAI and was shown to
describe disease activity at various activity levels in a manner comparable to the original
SLEDAI [5]. However, both SLEDAI and SLEDAI-2K document findings in the past 10 days
prior to the visit [5]. Since patients in drug trials are followed at 30-day window intervals the

41
SLEDAI-2K was validated for a 30-day window both in a cross-sectional study and
longitudinally over 1 year [6, 7].
SLEDAI-2K records features of disease activity in lupus as present or absent [4, 5]. Thus its
utility in clinical trials is limited as it cannot reflect partial improvement in a disease
manifestation. This led us to develop the SLEDAI-2K Responder Index-50 (SRI-50), which
could document a minimum 50% improvement in disease manifestations among lupus patients.
Our aims were: (1) to describe the development of SRI-50, an index derived from SLEDAI-2K
to measure at least 50% improvement in disease activity; (2) to describe the development of the
SRI-50 data retrieval form that would standardize the method of scoring of the descriptors; and
(3) to test the construct validity of SRI-50 as a responder index measuring global disease activity
improvement.
4.2 Methods
4.2.1 Derivation of SRI-50 definitions, SRI-50 data retrieval form, and
SRI-50 scores
We used SLEDAI-2K to develop the new responder index, SRI-50 [11]. A minimum of 50%
improvement was felt by clinicians to reflect a significant improvement.
4.2.2 SRI-50 definitions
We searched the literature and generated definitions to identify 50% improvement in each of the
24 descriptors of SLEDAI-2K. The agreed-upon descriptor definitions of SRI-50 and the SRI-50
data retrieval form were evaluated first by 3 rheumatologists (Zahi Touma, Dafna D. Gladman,
and Murray B. Urowitz) on several occasions. These definitions were then discussed with and
refined by other lupologists and rheumatologists at a series of inter-divisional meetings to
establish areas for improvement, mostly concerning the wording of the index. Where
appropriate, changes were made in accord with the suggestions.

42
Rules for ascertainment were provided for each of the descriptors, whether they were physical
findings, laboratory findings, patient self-evaluation, physician evaluation of variables such as
cognitive dysfunction, laboratory results, or diagnostic tools (Table 9). Each descriptor refers to
the preceding 30 days as in the SLEDAI-2K 30 days and descriptors are measured in a generally
accepted way (Table 10) [6, 7].

43
Table 9. Approaches to measure disease activity
Physical findings Patient self-evaluation Laboratory results Diagnostic tools
Psychosis
Organic brain syndrome
Visual
cranial nerve disorder
CVA
Vasculitis
Arthritis
Myositis
Rash
Alopecia
Seizure
Cranial nerve disorders
Lupus headache
Alopecia
Mucosal ulcers
Pleurisy
Pericarditis
Fever
Myositis
Urinary casts
Hematuria
Proteinuria
Pyuria
Low complements
Increased anti-DNA antibodies
Thrombocytopenia
Leukopenia
Cranial nerve
disorders
CVA
Pleurisy
Pericarditis
CVA cerebrovascular accident; DNA double stranded antibodies.

44
Table 10. SLEDAI-2K Responder Index 50 (SRI-50)© -Definitions.
Descriptors are present at the time of the visit or in the preceding 30 days and attributed to lupus
(Copyright University Health Network)
To determine body surface area use Rule of Nines for skin scoring: Head 9%, chest 9%, abdomen 9%, back 18%, legs 36%,
arms/hands 18% and mucous membrane 1%; physician’s palm for 1%.
* Overlap of symptoms will count for only one descriptor either Psychosis or Organic Brain Syndrome.
# Lupus headache improvement will count regardless of whether patient is using narcotic analgesia or not though it has to be part
of the baseline lupus headache.
§ CVA and Cranial Nerve improvement will count if it occurs within 1 month from the event on the basis of decrease in lupus
disease activity as this more likely on the basis of decrease disease activity.
† Vasculitis, Rash and Alopecia; if the total BSA ≤1%, a ≥50% improvement is defined by ≥50% decrease in the activity of the
most active lesion by decreasing by 2 grades or ≥50% decrease in the number of lesions or decrease in the size of the biggest
lesion with no worsening in either.
Numerical scale: 1is mild and 10 is most severe
DESCRIPTOR SLEDAI-2K DEFINTION DEFINITION OF SRI-50 IMPROVEMENT
Seizure Recent onset. Exclude metabolic, infectious or drug causes. ≥50% reduction in frequency of baseline seizure days/month.
Psychosis* Altered ability to function in normal activity due to severe disturbance in the perception of reality. Include
hallucinations, incoherence, marked loose associations,
impoverished thought content, marked illogical thinking, bizarre, disorganized, or catatonic behavior. Exclude
uremia and drug causes.
≥50% improvement of the psychotic manifestations judged by physician.
Organic brain
syndrome*
Altered mental function with impaired orientation,
memory, or other intellectual function, with rapid onset and
fluctuating clinical features. Include clouding of consciousness with reduced capacity to focus, and inability
to sustain attention to environment, plus at least 2 of the
following: perceptual disturbance, incoherent speech, insomnia or daytime drowsiness, or increased or decreased
psychomotor activity. Exclude metabolic, infectious or
drug causes.
≥50% improvement of the organic brain manifestations judged by
physician.
Visual
disturbance
Retinal changes of SLE. Include cytoid bodies, retinal
hemorrhages, serous exudate or hemorrhages in the choroid, or optic neuritis. Exclude hypertension, infection,
or drug causes.
≥50% improvement of the retinal exam assessed by physician.
Cranial Nerve
disorder§
New onset of sensory or motor neuropathy involving
cranial nerves.
≥50% recovery of motor or sensory function in affected nerve
within 1 month from the event on the basis of decrease in lupus disease activity or ≥50% decrease of the severity of pain within 1
month from the event on the basis of decrease in lupus disease
activity as determined by patient on numerical scale of 1-10 if applicable with no worsening in either.
Lupus headache# Severe, persistent headache; may be migrainous, but must
be nonresponsive to narcotic analgesia.
≥50% decrease of the severity of pain as determined by patient on
numerical scale of 1-10.
CVA§ New onset of cerebrovascular accident(s). Exclude
arteriosclerosis.
≥50% recovery of motor or sensory function related to CVA
within 1 month from the event on the basis of decrease in lupus disease activity as determined by physician without worsening in
either.
Vasculitis† Ulceration, gangrene, tender finger nodules, periungual infarction, splinter hemorrhages, or biopsy or angiogram
proof of vasculitis.
≥50% improvement of the vasculitis lesions present with no new lesion or worsening in either.
A ≥50% improvement for ulceration or gangrene is defined as
≥50% decrease in the body surface area; for periungual infarction, splinter hemorrhages or tender finger nodules a ≥50%
improvement is defined as ≥50% decrease in the total number of
involved digits with periungual infarction, splinter hemorrhages and tender finger nodules.
Multiple lesions in a single digit, count only one.

45
SLEDAI-2K Responder Index 50 (SRI-50)© – Definitions
© The SLEDAI-2K-50 Responder Index (SRI-50) is a licensed work of the University Health Network.
(Copyright University Health Network)
The SRI-50 data retrieval form was developed to standardize the recording of SLEDAI-2K
descriptors in an efficient way to allow calculation of SRI-50 scores (Table 11).
DESCRIPTOR SLEDAI-2K DEFINITION DEFINITION OF SRI-50 IMPROVEMENT
Arthritis ≥ 2 joints with pain and signs of inflammation (i.e. tenderness, swelling or effusion).
≥50% reduction in the number of joints with pain and signs of inflammation (i.e. tenderness, swelling or effusion).
Myositis Proximal muscle aching/weakness, associated with elevated creatinine phosphokinase/aldolase or electromyogram
changes or a biopsy showing myositis.
≥50% increase in muscles power judged by physician or increase by or 1 grade upon a scale of zero to five
or
≥50% decrease in the level of creatinine phosphokinase/aldolase level comparing to previous visit with no worsening in either.
Urinary casts Heme-granular or red blood cell casts.
Decrease by ≥50% in the total number of casts (heme-granular and
red blood cell casts).
Hematuria >5 red blood cells/high power field. Exclude stone, infection, or other cause.
Decrease by ≥50% in the number of red blood cell /high power field at this visit.
Proteinuria New onset, recurrent, or persistent proteinuria of more than
> 0.5 gram/24 hours.
Decrease by ≥50% in the range of proteinuria.
Pyuria >5 white blood cells/ high power field. Exclude infection. Decrease by ≥50% in the number of white blood cells/ high power
field.
Rash† New onset, recurrent or persistent inflammatory lupus rash.
Activity of skin lesions should be based on the evaluation of the most active lesion.
Decrease by ≥50% of involved body surface area and/or activity of
most active lesion with no worsening in either.
Activity of the lesion should be determined by the color of the
lesions:
0 –absent 1 – pink, faint erythema
2 – red
3 – dark red/purple/violaceous/crusted/hemorrhagic
A ≥50% decrease in the activity of the lesion is defined by
decreasing by 2 grades. Dyspigmentation, scarring and atrophy are not active lesions.
Alopecia† New onset, recurrent, or persistent abnormal, patchy or
diffuse loss of hair.
Size of patchy alopecic lesion should be determined based on involved total scalp surface. Total scalp surface is 4.5%.
Diffuse alopecia is determined by patient on numerical scale of 1-10.
Activity of alopecia should be based on the evaluation of the most active lesion.
Decrease by ≥50% of total scalp involved area for patchy alopecic
lesion or ≥50% reduction in the diffuse alopecia as determined by patient on numerical scale of 1-10, and/or activity of the most active
alopecic lesions with no worsening in either. Activity of the alopecic lesion should be determined by the color of
the most active lesion:
0 –absent 1 – pink, faint erythema
2 – red
3 – dark red/purple/violaceous/crusted/hemorrhagic A ≥50% decrease in the activity of the lesion is defined by
decreasing by 2 grades.
Mucosal Ulcers New onset, recurrent, or persistent oral or nasal ulcerations. Decrease by ≥50% in the number of ulcers at this visit.
Pleurisy Pleuritic chest pain with pleural rub or effusion, or pleural
thickening.
≥50% reduction in the pain severity as determined by patient on
numerical scale of 1-10 and/or ≥50% reduction in the amount of fluid (on imaging) with no worsening in either.
Pericarditis Pericardial pain with at least one of the following: Rub,
effusion, electrocardiogram or echocardiogram confirmation.
≥50% reduction in the pain severity as determined by patient on
numerical scale of 1-10 and/or ≥50% reduction in the amount of fluid (on imaging) with no worsening in either.
Low Complement Decrease in CH50, C3, or C4 below the lower limit of
normal for testing laboratory.
≥50% increase in the level of any complement or normalization of
one of them without a drop in either.
Increased anti-DNA
antibodies levels
Increase in the level of anti-DNA antibodies above normal
range for testing laboratory.
≥50% reduction in the level of anti-DNA antibodies.
Fever >38º C. Exclude infectious causes. ≥50% reduction in the degree of fever above normal.
Thrombocytopenia <100,000 platelets/ x 109/L. Exclude drug causes. ≥50% increase in the level of platelets but <100,000 platelets/mm3.
Leukopenia <3,000 white blood cells/x 109/L. Exclude drug causes. ≥50% increase in the level of white blood cells but <3,000/mm3.

46
Table 11. Data retrieval form of SLEDAI-2K Responder Index-50 (SRI-50)
Descriptors are present at the time of the visit or in the preceding 30 days and must be
attributable to lupus. BASELINE VISIT
Visit Date: / /
Score
(Circle) FOLLOW-UP VISIT
Visit Date: / / Score (Circle)
Improvement
< 50% ≥ 50% 100%
Seizure
Partial (focal, local) seizures simple partial seizures (consciousness not impaired)
complex partial (with impairment of consciousness)
partial seizures (simple or complex) evolving to secondarily generalized seizures
Generalized seizures
nonconvulsive (absence) convulsive
Days per month
8
Seizure
Partial (focal, local) seizures simple partial seizures (consciousness not impaired)
complex partial (with impairment of consciousness)
partial seizures (simple or complex) evolving to secondarily generalized seizures
Generalized seizures
nonconvulsive (absence) convulsive
Days per month
8
4
0
Psychosis
Altered ability to function in normal activity due to: hallucinations incoherence
marked loose associations
impoverished thought content marked illogical thinking
bizarre, disorganized or catatonic behavior
8
Psychosis
Altered ability to function in normal activity due to: hallucinations incoherence
marked loose associations
impoverished thought content marked illogical thinking
bizarre, disorganized or catatonic behavior
Percentage of improvement of the acute event %
8
4
0
Organic brain syndrome
Altered mental function (with rapid onset and fluctuating
clinical features) with impaired: orientation
memory
other intellectual function clouding of consciousness with reduced capacity to
focus and inability to sustain attention to environment
perceptual disturbance incoherent speech
insomnia or daytime drowsiness
increased or decreased psychomotor activity
8
Organic brain syndrome
Altered mental function (with rapid onset and fluctuating
clinical features) with impaired: orientation
memory
other intellectual function clinical features clouding of consciousness with reduced capacity to
focus and inability to sustain attention to environment
perceptual disturbance incoherent speech
insomnia or daytime drowsiness
increased or decreased psychomotor activity Percentage of improvement of the acute event %
8
4
0
Visual disturbance cytoid bodies retinal hemorrhage serous exudates in the choroid
hemorrhage in the choroid optic neuritis
8
Visual disturbance
cytoid bodies retinal hemorrhage serous exudates in the choroid
hemorrhage in the choroid optic neuritis
Percentage of improvement of the retinal exam %
8
4
0
Cranial nerve disorder
Nerves involved
motor power
sensory deficit
pain as determined by patient on numerical scale of
1-10
8
Cranial nerve disorder
Nerves involved
motor power
Percentage of improvement of the acute event %
sensory deficit
Percentage of improvement of the acute event %
pain as determined by patient on numerical scale of
1-10
8
4
0
Lupus headache
pain as determined by patient on numerical scale of 1-10
8
Lupus headache
pain as determined by patient on numerical scale of
1-10 8 4 0
CVA
Clinical diagnosis: Date of CVA (yyyy/mm/dd)
face upper extremities lower extremities
motor power sensory deficit location:
8
CVA
Clinical diagnosis: Date of CVA (yyyy/mm/dd)
face upper extremities lower extremities
motor power sensory deficit location:
Percentage of improvement of the acute event %
8
4
0
Vasculitis
ulceration of gangrene of
Body Surface Area %
Number of lesions: Size of biggest lesion:
periungual infarction # of involved digits
splinter hemorrhages # of involved digits tender finger nodules # of involved digits
8
Vasculitis
ulceration of gangrene of
Body Surface Area %
Number of lesions:
Size of biggest lesion: periungual infarction # of involved digits
splinter hemorrhages # of involved digits tender finger nodules # of involved digits
8
4
0
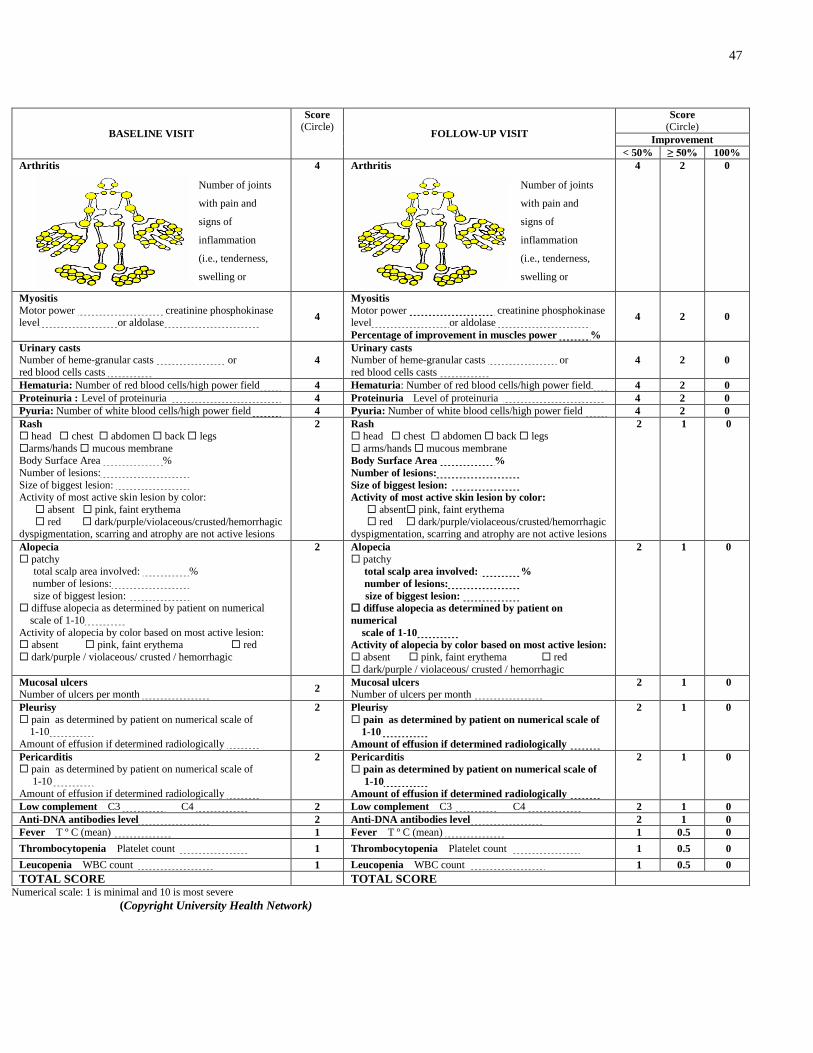
47
BASELINE VISIT
Score
(Circle)
FOLLOW-UP VISIT
Score
(Circle)
Improvement
< 50% ≥ 50% 100%
Arthritis
4 Arthritis
4 2 0
Myositis
Motor power creatinine phosphokinase level or aldolase
4
Myositis
Motor power creatinine phosphokinase level or aldolase
Percentage of improvement in muscles power %
4 2 0
Urinary casts
Number of heme-granular casts or
red blood cells casts
4
Urinary casts
Number of heme-granular casts or
red blood cells casts
4 2 0
Hematuria: Number of red blood cells/high power field 4 Hematuria: Number of red blood cells/high power field- 4 2 0
Proteinuria : Level of proteinuria 4 Proteinuria Level of proteinuria 4 2 0
Pyuria: Number of white blood cells/high power field 4 Pyuria: Number of white blood cells/high power field 4 2 0
Rash
head chest abdomen back legs
arms/hands mucous membrane Body Surface Area %
Number of lesions:
Size of biggest lesion: Activity of most active skin lesion by color:
absent pink, faint erythema
red dark/purple/violaceous/crusted/hemorrhagic dyspigmentation, scarring and atrophy are not active lesions
2 Rash
head chest abdomen back legs
arms/hands mucous membrane
Body Surface Area %
Number of lesions:
Size of biggest lesion: Activity of most active skin lesion by color:
absent pink, faint erythema
red dark/purple/violaceous/crusted/hemorrhagic dyspigmentation, scarring and atrophy are not active lesions
2 1 0
Alopecia
patchy total scalp area involved: %
number of lesions:
size of biggest lesion: diffuse alopecia as determined by patient on numerical
scale of 1-10
Activity of alopecia by color based on most active lesion: absent pink, faint erythema red
dark/purple / violaceous/ crusted / hemorrhagic
2 Alopecia
patchy
total scalp area involved: %
number of lesions:
size of biggest lesion:
diffuse alopecia as determined by patient on
numerical
scale of 1-10
Activity of alopecia by color based on most active lesion:
absent pink, faint erythema red
dark/purple / violaceous/ crusted / hemorrhagic
2 1 0
Mucosal ulcers
Number of ulcers per month 2
Mucosal ulcers
Number of ulcers per month
2 1 0
Pleurisy
pain as determined by patient on numerical scale of 1-10
Amount of effusion if determined radiologically
2 Pleurisy
pain as determined by patient on numerical scale of
1-10
Amount of effusion if determined radiologically
2 1 0
Pericarditis
pain as determined by patient on numerical scale of
1-10
Amount of effusion if determined radiologically
2 Pericarditis
pain as determined by patient on numerical scale of
1-10
Amount of effusion if determined radiologically
2 1 0
Low complement C3 C4 2 Low complement C3 C4 2 1 0
Anti-DNA antibodies level 2 Anti-DNA antibodies level 2 1 0
Fever T º C (mean) 1 Fever T º C (mean) 1 0.5 0
Thrombocytopenia Platelet count 1 Thrombocytopenia Platelet count 1 0.5 0
Leucopenia WBC count 1 Leucopenia WBC count 1 0.5 0
TOTAL SCORE TOTAL SCORE
Numerical scale: 1 is minimal and 10 is most severe
(Copyright University Health Network)
Number of joints
with pain and
signs of
inflammation
(i.e., tenderness,
swelling or
effusion)
#
Number of joints
with pain and
signs of
inflammation
(i.e., tenderness,
swelling or
effusion)
#

48
SRI-50 score is evaluated at the follow up visit and corresponds to the sum of each of the 24
descriptors’ scores found on the SRI-50 data retrieval form. For patients with multiple follow up
visits, we recommend determining the score of the SRI-50 using the baseline visit scores. For
patients who become worse after a period of improvement in a specific manifestation, or if a new
manifestation develops in a follow up visit, a subgroup analysis can be conducted to include that
visit in the determination of SRI-50.
4.2.3 Assessment of construct validity
Construct validity of the SRI-50 definitions and the SRI-50 data retrieval form was assessed.
4.2.4 Patient selection
We conducted a cross-sectional study on all patients who attended the Lupus Clinic from
September 2009 to December 2009. Of the 298 patients enrolled, 141 had a follow up visit and
were studied further.
4.2.5 Patient assessment
Patients were assessed initially (at an anchor visit) and then reassessed, after treatment was
initiated or adjusted, in 1 to 3 months. SLEDAI-2K 0 (anchor visit) was determined on the
baseline visit and the SRI-50 data retrieval form was completed. SLEDAI-2K 1 (follow up visit)
and SRI-50 scores were determined on a follow up visit at 1 to 3 months. During the first visit a
physician global assessment was determined on visual analog scale (VAS) line of 100 mm, with
anchors of 0 “no disease activity” and 10 for “very active disease.” During the follow up visit a
physician response assessment was determined on a 7-point Likert scale (LS); 7 = much
improved, 6 = moderately improved, 5 = slightly improved, 4 = unchanged, 3 = slightly worse, 2
= moderately worse, and 1 = much worse. We defined a 50% improvement as LS score ≥ 6.

49
4.2.6 Clinician scoring of disease activity
A clinician who did not know the patients and who was not aware of the SLEDAI-2K scores
evaluated each patient’s record and assigned a clinical activity score for each assessment
according to the following scale: improved, same, and worse, using standardized predefined
definitions. “Improved,” defined as one of the following: (1) stopping treatment in the presence
of improvement of an already active system or in response to complete remission of an active
system; (2) a decrease in medication dosage for the above reason; (3) indication of improvement
in SLE disease activity in the physician’s notes; (4) use of the term improvement in the
physician’s notes. “Worse,” defined as one of the following: (1) introduction of new treatment in
the presence of worsening of an already active system, or in response to activation of a new
system; (2) increase in medication dosage for the above reasons; (3) indication of concern
regarding SLE disease activity in the physician’s notes — arrangement for an earlier
appointment/investigation to assess SLE disease activity; (4) the use of the term flare/worsening
in the physician’s notes; (5) new diagnosis of SLE (new presentation, not just the accumulation
of American College of Rheumatology criteria [91]) [92]. “Same”, defined as no change in
disease activity in patients who did not qualify for the definitions of improved or worse.
4.2.7 Method and analysis
Descriptive statistics were used to describe the characteristics of the patients. We determined the
mean change of SRI-50 scores (Δ SRI-50 = SLEDAI-2K 0 – SRI-50) and the mean change of
SLEDAI-2K scores (Δ SLEDAI-2K = SLEDAI-2K 0 – SLEDAI-2K 1) among patients who
improved, got worse, and remained unchanged as determined by the external physician.
4.2.8 External construct
The external construct was the LS. We further divided into 4 groups the group of patients who
improved as determined by the external physician; that is, LS 4 (unchanged), LS 5 (mildly
improved), LS 6 (moderately improved; ≥ 50%), and LS 7 (much improved; ≥ 50%). We

50
determined the mean change of SRI-50 (Δ SRI-50) scores and mean change of SLEDAI-2K (Δ
SLEDAI-2K) in each of the 4 groups. Spearman correlation coefficient was determined between
Δ SRI-50 and Δ SLEDAI-2K, with LS 4, LS 5, LS 6, and LS 7. The paired t test was used to
compare the mean Δ SRI-50 and the mean Δ SLEDAI-2K scores in patients with LS ≥ 6 to those
with LS 4–5. We hypothesized that patients who had ≥ 50% improvement (LS ≥ 6–7) would be
identified better by SRI-50 than by SLEDAI-2K, and the change in their SRI-50 scores would
meet the definition of improvement by SLEDAI-2K (decrease > 3).
Written consent was obtained from all patients and the study was approved by the Institutional
Review Board at the University of Toronto, Toronto Western Hospital.
4.3 Results
4.3.1 Derivation of SRI-50 definitions, SRI-50 data retrieval form, and
SRI-50 score
The SRI-50 definitions were developed as a 2-page document including 24 definitions for the
descriptors of SLEDAI-2K to define ≥ 50% improvement (Table 10).
The SRI-50 data retrieval form is a 2-page document to standardize the recording of descriptors
to allow the calculation of SRI-50 (Table 11). The assigned scores for the descriptors of SRI-50
were derived by dividing the score of the corresponding SLEDAI-2K descriptor by 2.
For the individual descriptors, separate approaches are utilized by both physician and patient to
evaluate improvement between visits. The physician analyzes the results of physical findings and
laboratory and diagnostic results (radiological, electrocardiogram, and others), all based on hard,
well defined outcomes, to complete the SRI-50 data retrieval form (Table 9). For the descriptors,
which are more subjective and require patient self-evaluation (namely cranial nerve disorder,
headache, the pain of pleurisy and pericarditis, and diffuse alopecia), the SRI-50 data retrieval
form records the patient self-evaluation based on a numerical scale ranging from 1 to 10 (1 is
mild and 10 is most severe). For descriptors requiring a health professional’s evaluation, e.g., ≥
50% improvement in cognitive dysfunction, the percentage improvement discerned by the

51
professional is recorded on the data retrieval form. The physician collects and records the
patients’ information on the SRI-50 data retrieval form (Table 11).
For the descriptors related to neurolupus, and more specifically psychosis and organic brain
syndrome, we left it to the rheumatologist to determine if there is ≥ 50% improvement or not.
Presumably the rheumatologist will confer/consult with other healthcare providers with expertise
in this area, e.g., neuropsychologists or psychiatrists, to help judge percentage improvement. In
trials looking specifically at these outcomes such expertise could be included in the design. As an
example, in a trial of therapy for the treatment of acute cognitive dysfunction, evaluation by a
neurocognitive expert would be included.
4.3.2 Practical applicability, administration, scoring
4.3.2.1 Administration
The SRI-50 data retrieval form is completed by the physician during the visit based on the
history and clinical and laboratory findings. A complete history and physical examination are
required in addition to the laboratory results related to the index. Similarly to SLEDAI-2K, for
most patients it takes a couple of minutes to complete the form.
4.3.2.2 Scoring
The method of scoring is simple, cumulative, and intuitive as in the original SLEDAI-2K. In
general, if required, one session of training is enough to become familiar with the definitions of
SRI-50.
When a descriptor is recorded as present at the initial visit, one of 3 situations can follow: (1) the
descriptor achieves complete remission at follow up, in which case the score would be “0”; (2)
the descriptor does not achieve a minimum of 50% improvement at follow up, in which case the
score would be identical to its corresponding SLEDAI-2K value; or (3) the descriptor improves
by ≥ 50% (according to the SRI-50 definition) but has not achieved complete remission, in which

52
case the score is evaluated as one-half the score that would be assigned for SLEDAI-2K. If a
descriptor was not present at the initial visit, the value for SRI-50 at the follow up visit will be
the same as that for SLEDAI-2K. This process is repeated for each of the 24 descriptors. Finally,
the SRI-50 score at follow up is evaluated as the sum of the 24 individual descriptor scores.
SRI-50 score is evaluated at the follow up visit and corresponds to the sum of each of the 24
descriptor scores found on the SRI-50 data retrieval form.
As recommended by the US Food and Drug Administration (FDA) in clinical trials, landmark
analyses are important for comparing current patient scores versus scores recorded at their
baseline visit. These landmark comparisons can be made at a series of intervals, e.g., at 2, 4, and
6 months (vs anchor visit), even though the primary outcome may be 6 months. Any
deterioration in SRI-50 at 2 or 4 months would indicate a worsening in the original disease
manifestation or the development of a new disease manifestation. Such occurrences could be
secondary outcomes. In clinical practice, the physician is interested in how the patient is today
compared to the last visit and here the comparison to the last visit may be appropriate.
4.3.3 Testing of concurrent construct validity
Between September 2009 and December 2009, of the 298 patients enrolled, 141 patients had
followup visits and were studied further. The majority of the 141 patients were female (89.4%).
The patients’ ethnic distribution was Caucasian 57.4%, Black 16.3%, Asian 9.9%, and other
16.3%. The mean age at diagnosis of SLE was 29.1 ± 11.4 years and age at first visit in this
study was 44.5 ± 12.8 years. Patient characteristics are presented in (Table 12).

53
Table 12. Characteristics of patients
Sex (F/M) 89.4%/10.6%
Race Caucasian
Black
Asian
Other
57.4%
16.3%
10%
16.3%
Age at diagnosis 29.1 ± 11.4 years
Age at 1st visit in study 44.5 ± 12.8 years
Disease duration at 1st visit in study 15.3 ± 11.2 years
Time between baseline and follow-up visits 3.2 ± 1.4 months
SLEDAI-2K at 1st visit in study 4.79±4.67

54
4.3.4 Change in SLEDAI-2K and SRI-50 scores in patients as
determined by external physician
The external physician rated patients as follows: 14 patients were worse, 65 the same, and 62
improved. SRI-50 scores did not decrease significantly below their presenting SLEDAI-2K score
in patients who remained stable or worsened. In patients who improved as determined by the
external physician, the SRI-50 score decreased by a mean of 2.40 ± 3.11, while SLEDAI-2K
scores decreased by 1.65 ± 2.91 (Table 13). This decrease in the score of SRI-50 reflects partial
improvement in the descriptors that was not determined by SLEDAI-2K on follow up visit.
Table 13. Statistical results in patients whom changed their disease activity
Worse
(n=14)
Same
(n=65)
Improved
(n=62)
SLEDAI-2K 0 4.43±3.32 3.15±4.16 6.58±4.84
SLEDAI-2K 1 7.29±4.55 2.97±4.03 4.94±4.47
SRI-50 7.21±4.61 2.76±3.86 4.18±4.06
∆ SLEDAI-2K 2.86±3.76 -0.18±2.64 -1.65±2.91
∆ SRI-50 2.79±3.79 -0.39±2.74 -2.40±3.11
∆ SLEDAI-2K= (SLEDAI-2K 0) – (SLEDAI-2K 1)
∆ SRI-50= (SLEDAI-2K 0) – (SRI-50)

55
4.3.5 Change in SLEDAI-2K and SRI-50 scores in patients who
improved in association with the external construct
The correlation between the external construct, LS, was moderate with the SLEDAI-2K (r1 =
0.39; p = 0.02) and with the SRI-50 (r2 = 0.48; p < 0.0001). It is not surprising that SLEDAI-2K
detected improvement when there was complete resolution of a feature, which could happen with
LS improvement ≥ 6. Moreover, SLEDAI-2K scores decreased with LS 4–5 (0.69 ± 2.40) and to
a greater extent with LS ≥ 6 (2.89 ± 3.09) (p = 0.03). However, SRI-50 scores decreased to a
greater extent with both LS 4–5 (1.06 ± 2.48) and with LS ≥ 6 (4.15 ± 3.01) (p < 0.0001).
Importantly, the decrease in SRI-50 scores compared to the decrease in SLEDAI-2K scores on
followup visit in patients with LS ≥ 6 was statistically and clinically more significant, meeting
the definition of improvement by SLEDAI-2K, with a reduction > 3 (Table 14).

56
Table 14. Change in SLEDAI-2K and SRI-50 scores in patients who improved in
association with the external construct, the Likert scale (LS) score.
∆ SLEDAI-2K ∆ SRI-50
LS 4(n=15) -0.33±1.99 -0.47±2.07
LS 5(n=20) -0.95±2.68 -1.50±2.72
LS 6(n=20) -2.40±2.60 -3.80±2.95
LS 7(n=7) -4.29±4.07 -5.14±3.18
Correlation (p) 0.42 (0.0009) 0.52 (0.0001)
Improvement (n=62)
LS 4-5 -0.69±2.40 -1.06±2.48
LS ≥ 6 -2.89±3.09 -4.15±3.01
t-test 0.003 <0.0001
LS; Likert scale

57
4.4 Discussion
In the development of SLEDAI and its updated version, SLEDAI-2K, investigators were focused
on describing disease activity and documenting descriptors as present or absent [4, 5]. In clinical
trials and observational studies it is very important to identify improvement related to treatment
between visits. The improvement need not be total resolution to suggest that a therapeutic agent
is useful. Recognition that SLEDAI-2K and other disease activity measures adopted in clinical
trials have limited ability to identify partial improvement led us to consider developing
alternative measures for monitoring disease activity of lupus patients [38]. The development of a
new measurement based on a simple known index is an important advance.
We describe development and initial validation of a novel clinical index measuring improvement
of SLE disease activity between visits, the SRI-50. SLEDAI-2K is a reliable and valid index that
has been adopted in clinical trials and observational studies [4].
Our goal was to modify
SLEDAI-2K to allow it to record partial improvement in disease activity, which would be useful
to detect response to treatment in both clinical trials and observational studies. A minimum 50%
improvement was felt by clinicians to reflect a clinically important improvement. The SRI-50
comprises the same 24 descriptors and covers the 9 organ systems found in the original
SLEDAI-2K. SRI-50 reflects disease activity over the previous 30 days. The SRI-50 data
retrieval form, which standardizes the documentation of the descriptors, performed extremely
well in all descriptors; this is especially relevant for multicenter studies that form the backbone
of any therapeutic evaluation for SLE.
As a first effort toward validating SRI-50, we assessed its content validity, face validity, practical
applicability including administration and scoring, and concurrent construct validity. Content and
face validity are qualitative assessments of a measure that rely on understanding how the items
or individual questions in a measure were derived. Since the SRI-50 is derived from the
SLEDAI-2K, face and content validity related to selection of the 24 descriptors to study disease
activity were assumed to be present [4, 5, 38]. Moreover, content validity and face validity of the
SRI-50 definitions and the SRI-50 data retrieval form were confirmed according to the
methodology adopted in the development of the SRI-50. The agreed-on descriptor definitions of
the SRI-50 definitions and the SRI-50 data retrieval form were thoroughly revised as described
in Materials and Methods.

58
The traditional way to validate a new measure is to determine its correlation with some other
measure of the trait, ideally, a “gold standard,” concurrent criterion validity. In the absence of a
gold standard measure, correlation is conducted on the most commonly adopted measure in the
field. In our initial validation we studied the concurrent construct validity of SRI-50 and the
physician response assessment, as determined by LS, both obtained at the same time [93]. A
moderate correlation (0.30–0.70) and preferably strong correlation (> 0.70) is desirable in this
step [94]. We evaluated the performance of SRI-50 on 141 patients seen in our lupus clinic and
determined its correlation with physician response assessment determined by LS. We showed
that the SLEDAI-2K and SRI-50 scores on followup visit correlated with LS score ≥ 6.
Importantly, the decreases in SRI-50 scores were clinically significant, meeting the accepted
definition of improvement of a decrease in SLEDAI-2K of > 3, but this was not achieved with
the SLEDAI-2K followup visit. Indeed, this reflected the ability of the SRI-50 to determine
partial improvement between visits in patients who improved, while the SLEDAI-2K did not
discern this improvement. This confirmed the SRI-50 concurrent construct validity.
In the early stage of the development of SLEDAI in 1985, the authors retained the 24 “most
important” descriptors along with their corresponding weighted scores to constitute what we
know today as SLEDAI. In the SRI-50, descriptors are scored as present, absent, or improved by
≥ 50%. Similar to SLEDAI-2K, the weighted scores of the descriptors in SRI-50 are not affected
by their severity but are weighted by their status. A 50% improvement in certain severe features
might not have a great influence on the score when compared to a 50% improvement in certain
milder features. However, in a moderate to large size study, the effect of such instances is likely
to be relatively small.
A number of new agents have been introduced and are in various phases of drug development in
lupus; nevertheless, none have to date been approved by the FDA, and few achieved their
primary outcomes in clinical trials. Although the results of these studies were disappointing, it
would be premature to conclude that these therapeutic strategies cannot be effective in SLE.
Several aspects of clinical design could have affected the outcomes of these trials, namely,
inclusion criteria and difficulty ensuring the enrollment only of patients with active disease, the
choice of primary outcomes, and use of concomitant drugs. More importantly, the lack of a
robust responder index for global disease activity in SLE patients is a serious limitation when
designing clinical trials. The use of the SRI-50 has the potential to overcome these problems.

59
In the initial validation of the SRI-50, we have used the data available at baseline and at one
follow up visit. We have currently analyzed our data on a larger sample size and multiple follow
up visits for each patient (Chapters 7-8). Nevertheless, we recommend determining the score of
the SRI-50 by using the baseline visit scores, whereas in a subgroup analysis, the visit that
includes the worsening can be used.
Additional validation for the SRI-50 will be necessary. The minimal clinically important
difference of the SRI-50 and responsiveness in clinical trials have yet to be determined. Studies
are currently under way to evaluate these aspects. This validation of the SRI-50 enables it to be
used as an outcome measure in clinical trials.
I-This paper has been published:
Touma Z, Gladman DD, Ibañez D, Urowitz MB. Development and Initial Validation of
SLEDAI-2K (Systemic Lupus Erythematosus Disease Activity Index 2000) Responder Index-50
(SRI-50). J Rheumatol 2011;38:275-84. [11]
II-Patents and Intellectual Property Rights related to SRI-50:
3. SRI-50 Manual
Touma Z, Gladman DD, Mackinnon A, Urowitz MB. SLEDAI-2K Responder Index-50
(SRI-50) Manual. July 2010 (Available online; www.sri-50.com).
4. SRI-50 Website
Touma Z, Gladman DD, Mackinnon A, Urowitz MB. SLEDAI-2K Responder Index-50
(SRI-50) Website July 2010 www.sri-50.com

60
Chapter 5 Reliability of SRI-50
This paper has been published in:
Touma Z, Urowitz MB, Fortin PR, Landolt-Marticorena C, Toloza SM, Riddell C, Chandran V,
Eder L, Ghanem A, Ziouzina O, Taghavi-Zadeh S, Ibañez D, Gladman DD. SLEDAI-2K
Responder Index (SRI)-50: A Reliable Index for Measuring Improvement in Disease Activity. J
Rheumatol 2011:38:868-73. [95]

61
5.1 Background
Systemic lupus erythematosus (SLE) is a complex disease with highly variable patterns of organ
involvement and prognosis [38]. During the course of their disease, patients with lupus
experience events that are related to acute disease activity or to chronic damage, which makes
the disease difficult to monitor [38]. Lupus disease activity is an important domain that must be
assessed in clinical trials and outcome studies. Other domains, namely damage resulting from
lupus activity or its therapy, health-related quality of life, adverse events, and economic costs
including health utilities, are utilized to adequately describe the effects of the disease [38, 90]. It
is essential that measures used to monitor such outcomes have evidence of validity and reliability
[96]. The Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K) Responder
Index (SRI-50) is a valid index able to demonstrate incomplete but clinically significant ≥ 50%
improvement in disease activity in lupus patients [11].
The SRI-50 comprises the same 24 descriptors, covering 9 organ systems, and reflects disease
activity over the previous 30 days as does SLEDAI-2K [4, 5, 7, 11]. The SRI-50 data retrieval
form standardizes the documentation of the descriptors and performed extremely well in all
descriptors, which is especially relevant for multicenter studies that form the backbone of any
therapeutic evaluation for SLE [11]. The practical applicability of the SRI-50, including ease of
administration, low costs of data collection, method of scoring and ease of score interpretation,
and construct validity, has been demonstrated [11].
Clinicians seeking a tool to measure disease activity should look for evidence of reliability, e.g.,
stability of a tool when no change has occurred in disease activity, test-retest or intrarater
reliability, and within-rater reliability or interrater reliability [93, 96, 97].
Our study assessed the interrater and intrarater reliability of the SRI-50 in patient profile
scenarios derived from real adult lupus patients with the participation of rheumatologists from
different centers in different countries.

62
5.2 Methods
5.2.1 Patient selection
This study was performed on patient profile scenarios derived from a longitudinal cohort of
lupus patients receiving follow up care at a single center. All patients in the cohort are followed
longitudinally and met the American College of Rheumatology (ACR) classification criteria for
SLE [91, 98]. Patients attend the lupus clinic at 2–6 month intervals regardless of the state of
activity of their lupus. Patients are assessed using a standard protocol that includes complete
history, physical examination, and laboratory evaluation. Collection and storage of data at the
lupus clinic are conducted in accord with the Declaration of Helsinki and is approved by the
Research Ethics Board of the University Health Network, Toronto, Canada. Signed informed
consent is obtained from patients at the time of enrollment into the cohort at the lupus clinic.
The sampling strategy adopted in this study to evaluate the reliability of SRI-50 assured that each
of the 24 descriptors of SLEDAI-2K was represented in at least 1 patient profile [5]. After
selecting the patients that would be included in the study, 40 patient profiles were created based
on the information available for the selected visit. Each patient profile was composed of an initial
visit and a follow up visit. The patient profile was based on the patient’s subjective complaints
and the objective findings of the clinical, laboratory, and radiological assessments. This was
based on the data available from the lupus clinic database, from the medical chart, and from the
electronic medical record. On follow up visits, there were patients who either had improvement
in all active systems as compared to baseline visit, or had improvement in one system and/or
worsening in another. This gave the raters the possibility to determine if there had been
improvement in the descriptors.
5.2.2 Assessment of disease activity
5.2.2.1 SLEDAI-2K 30 days
Disease activity was measured by the SLEDAI-2K, a valid measure of disease activity in SLE, at
the first visit [5, 7]. SLEDAI-2K was modeled on clinicians’ global judgment to standardize and

63
measure disease activity. SLEDAI-2K is based on the presence of 24 descriptors in 9 organ
systems over the patient’s past 10 days. SLEDAI-2K 30 days was validated against SLEDAI-2K
10 days to describe disease activity over the previous 30 days [6, 7]. The total score of SLEDAI-
2K falls between 0 and 105, with higher scores representing increased disease activity [5].
5.2.2.2 SRI-50
The SRI-50 is a responder index based on the SLEDAI-2K 30 days that describes partial
improvement ≥ 50% in disease activity between visits in lupus patients [11]. SRI-50 score is
evaluated at the follow up visit and corresponds to the sum of each of the 24 descriptor scores on
the SRI-50 data retrieval form. The method of scoring is simple, cumulative, and intuitive and
similar to the SLEDAI-2K. One of 3 situations can result when a descriptor is present at the
initial visit: (1) the descriptor has achieved complete remission at follow up, in which case the
score would be “0”; (2) the descriptor has not achieved a minimum of 50% improvement at
follow up, in which case the score would be identical to its corresponding SLEDAI-2K value; or
(3) the descriptor has improved by ≥ 50% (according to the SRI-50 definition) but has not
achieved complete remission, in which case the score is evaluated as one-half the score that
would be assigned for SLEDAI-2K. If a descriptor was not present at the initial visit, the value
for the SRI-50 at the follow up visit will be the same as that for SLEDAI-2K. This process is
repeated for each of the 24 descriptors. Finally, the SRI-50 score at follow up is evaluated as the
sum of the scores of the 24 individual descriptors [11]..
5.2.2.3 Physician global assessment
Physician global assessment (PGA) was determined initially at baseline assessment on a 100-mm
visual analog scale (VAS; 0 = no disease activity, 100 = very active disease). Physicians
documented the PGA based on the baseline assessment of the patient.

64
5.2.2.4 Likert scale
During the follow up visit a physician response assessment was determined on a 7-point Likert
scale (LS), where 7 = much improved, 6 = moderately improved, 5 = slightly improved, 4 =
unchanged, 3 = slightly worse, 2 = moderately worse, and 1 = much worse. We defined a 50%
improvement as LS ≥ 6. Raters were instructed to circle the appropriate number on the LS to
indicate how active the patient’s lupus disease activity was on follow up visit. The use of
numerical scales in the assessment of global disease activity of lupus and rheumatoid arthritis has
been adopted in several studies [99, 100].
5.2.3 “Standard” SLEDAI-2K and SRI-50 scores
“Standard” SLEDAI-2K and SRI-50 scores were established by the creator of the scenarios (ZT),
who described each of the clinical and laboratory variables, and who did not participate in the
study as an assessor. The evaluation of raters’ scores of SLEDAI-2K and SRI-50 was compared
to the “Standard” SLEDAI-2K and SRI-50 results.
5.2.4 Raters, site selection, and procedure at each site
Ten rheumatologists who represented university and community hospitals from 3 centers in
different countries, Canada, United Kingdom, and Argentina, participated in this study. All had
worked at or had trained at the University of Toronto Lupus Clinic and were comfortable with
the use of the original SLEDAI-2K. Four rheumatologists were from university hospitals and 2
from community hospitals and 4 were postdoctoral rheumatology fellows. The level of training
among rheumatologists in the use of the SRI-50 in the reliability study differed. This approach
allowed us to evaluate the performance of the SRI-50 among trainees and rheumatologists.
Patient profiles were sent to each rater in 2 separate packages, each containing 20 cases. The
same 40 equivalent patient profiles were sent again in 2 packages to the same 10 rheumatologists
after 2 weeks from the first occasion to complete the SRI-50 data retrieval form, along with LS.
This approach was adopted to reduce the possibility of true clinician recall [93]. These patient

65
profiles were returned to the coordinating center after completion, for evaluation and comparison
to the “Standard” scores, by one external assessor (ZT).
5.2.5 Statistical analysis
Descriptive statistics were used to describe the characteristics of the patients. We evaluated the
number of mis-scorings in each round, and in both rounds for all raters for the SLEDAI-2K 30
days and the SRI-50.
We determined the interrater intraclass correlation coefficient (ICC) for SLEDAI-2K, SRI-50,
and PGA. The intrarater ICC were evaluated for each rater separately for SLEDAI-2K, SRI-50,
and PGA. Specifically, in all the above analyses we determined both ICC (2, 1) and ICC (2, k).
The first number “2” designates the model and is used when all subjects are rated by the same
raters, who are assumed to be a random subset of all possible raters [101]. The second number
signifies the form, using either a single measurement “1” ICC (2, 1) or the mean of several
measurements “k” ICC (2,k) as the unit of analysis in the model. The mean scores have the effect
of increasing reliability estimates, as means are considered better estimates of true scores,
theoretically reducing error variance [101-103]. As suggested by Streiner and Norman [93] we
considered ICC ≥ 0.85 to reflect good reliability. We determined the average intrarater ICC for
SLEDAI-2K, SRI-50, and PGA [93, 104].
We transformed the data available on 80 patient profiles for SLEDAI-2K and SRI-50 as
categorical data, “yes” for right score and “no” for wrong score, compared to the “Standard”
solutions. We evaluated the number and percentage of right answers for both SLEDAI-2K and
SRI-50 scores as compared to the “Standard” SLEDAI-2K and SRI-50 solutions, respectively.
We applied paired t tests and compared the mean SLEDAI-2K and SRI-50 scores from both
rounds. P values ≤ 0.05 were considered significant.
We determined the interrater kappa for LS scores. According to Landis and Koch [105],
agreement indexes were interpreted as follows: 0.81–1.00 = almost perfect, 0.61–0.75 =
substantial agreement, 0.41–0.60 = moderate agreement, 0.21–0.40 = fair agreement, 0–0.20 =
slight agreement, and ≤ 0 = poor agreement.

66
5.2.6 Sample size calculation
Sample size determined in this study was based on 3 estimates: reliability estimate, number of
raters, and the confidence interval [93]. The sample size sufficient for an ICC of 0.80, a standard
error of 0.05, and 10 raters is 31 patient profiles. Oversampling of 9 scenarios was done to allow
for incomplete forms. Generally, samples of 40–50 are sufficient, and “going above 50 subjects
in many situations is probably statistical overkill” (Streiner and Norman [93]). Indeed, the
methodology adopted in our study to evaluate the intrarater reliability allowed us to double this
number to 80 profiles. An ICC ≥ 0.75 is suggestive of good reliability and those below 0.75 poor
to moderate reliability. For many clinical measurements, reliability should exceed 0.90 to ensure
reasonable validity [106].
5.3 Results
5.3.1 Patient demographic data
The patient profiles included 35 females and 5 males; 55% were Caucasian, 22% Black, 5%
Asian, and 18% others. Age at diagnosis was 30.4 ± 12.7 years, age at the study date was 38.0 ±
13.5 years, and disease duration at study date was 7.6 ± 8.1 years. The mean SLEDAI-2K score
at baseline visit was 11.90 ± 7.09 and the mean SRI-50 on follow up visit was 5.98 ± 3.40. The
Systemic Lupus International Collaborating Clinics/ACR Damage Index (SDI) was 1.05 ± 1.45
[24]. As described above the sampling strategy we adopted assured that each of the 24
descriptors of SLEDAI-2K was represented in at least 1 patient profile (Table 15).

67
Table 15. Distribution of clinical and laboratory descriptors of SRI-50 in 40 patient profile
scenarios
Seizure 1 (2.5%) Proteinuria 6 (15%)
Psychosis 3 (7.5%) Pyuria 5 (12.5%)
Organic brain 3 (7.5%) Rash 16 (40%)
Visual 3 (7.5%) Alopecia 8 (20%)
Cranial nerve 2 (5.0%) Mucosal ulcers 3 (7.5%)
Lupus headache 2 (5.0%) Pleurisy 3 (7.5%)
CVA 2 (5.0%) Pericarditis 1 (2.5%)
Vasculitis 7 (17.5%) Low complement 13 (32.5%)
Arthritis 11 (27.5%) DNA 18 (45%)
Myositis 1 (2.5%) Fever 1 (2.5%)
Casts 5 (12.5%) Thrombocytopenia 1 (2.5%)
Hematuria 4 (10%) Leucopenia 2 (5.0%)

68
5.3.2 Common pitfalls
For SLEDAI-2K scoring, a total of 3 mis-scorings were found in the clinical descriptors
compared to 27 in the laboratory descriptors in both rounds. For SRI-50 scoring, 12 mis-scorings
were found in the clinical descriptors compared to 48 in the laboratory descriptors in both
rounds. The mis-scorings were the result of the rater’s failure to identify the appropriate relevant
data available in the patient profile scenario or the wrong application (misunderstanding and
unawareness) of the SLEDAI-2K or SRI-50 definitions. The most common pitfalls by raters in
SLEDAI-2K scoring in both rounds were related to the 2 descriptors “casts” and “leukopenia.”
In scoring the SRI-50, the most common mis-scorings were related to complement, casts, pyuria,
and leukopenia, and to a lesser extent to rash and fever. Almost all mis-scorings that were related
to casts originated from one rater, who did not translate the number of casts from the case
scenarios to the data retrieval form of the SRI-50. This resulted in wrong scoring in both
SLEDAI-2K and SRI-50. The mis-scorings related to the complements were present only in the
followup visit. This was related to mathematical miscalculation when determining whether there
is a 50% improvement by the raters. Thus virtually all the mis-scorings were rater failures rather
than instrument failures (Table 16)

69
Table 16. Raters mis-scorings in rounds 1 and 2 in SLEDAI-2K/SRI-50.
Descriptors R1
(n=400)
R2
(n=400)
Total/descriptor
(n=800)
SLEDAI-2K CD 0 3 3
LD 11 16 27
Total/round 11 19 30
SRI-50 CD 3 9 12
LD 20 28 48
Total/round 23 37 60
CD clinical descriptors; LD laboratory descriptors, R1 round 1; R2 round 2; n number of
patients’ scenarios

70
5.3.3 Reliability (interrater and intrarater)
Table 17 lists the interrater reliability and the corresponding ICC (2, 1) and ICC (2, k) values for
each round separately and for all 80 patient profiles for SLEDAI-2K, SRI-50, and PGA. The ICC
(2, k) performed on 80 patient profiles for interrater ranged from 1.00 for SLEDAI-2K and SRI-
50 to 0.96 for PGA. The average intrarater ICC for SLEDAI-2K, SRI-50, and PGA were 0.99,
0.98, and 0.90, respectively [104].

71
Table 17. Interrater reliability ICC (2, 1) and ICC (2, k).
ICC (2, 1) ICC (2, k)
R1+R2 (n=800)
SLEDAI-2K 0.94 1.00
SRI-50 0.99 1.00
PGA 0.69 0.96
R1 (n=400)
SLEDAI-2K 0.99 1.00
SRI-50 0.97 1.00
PGA 0.63 0.94
R2 (n=400)
SLEDAI-2K 0.99 1.00
SRI-50 0.98 1.00
PGA 0.60 0.94
SLEDAI-2K, Systemic Lupus Erythematosus-2000; SRI-50, SLEDAI-2K Responder Index-50;
PGA, Physician Global Assessment; LS, Likert Scale; n, number of patient profile; R1 round 1;
R2 round 2

72
Table 18 lists the intrarater reliability and the corresponding ICC (2, 1) and ICC (2, k) for each
rater separately for SLEDAI-2K, SRI-50 and PGA. The ICC (2, k) for SLEDAI-2K and SRI-50
ranged from 0.97 to 1.00 among raters [93]. The PGA ICC (2, k) ranged from 0.86 to 1.00.
Table 18. Intrarater reliability and the corresponding ICC (2, 1) and ICC (2, k) for each
rater separately for SLEDAI-2K, SRI-50, and PGA, and the categorical data for SLEDAI-
2K and SRI-50.
Continuous data
Categorical data†
Raters SLEDAI-2K SRI-50 PGA SLEDAI-2K= Standard
SLEDAI-2K
SRI-50=
Standard SRI-50
N=number of profiles (%)
1 ICC(2,1)
ICC(2,k)
0.98
0.99
0.97
0.99
0.75
0.86 78 (97.5%) 73 (91.3%)
2 ICC(2,1)
ICC(2,k)
1.00
1.00
1.00
1.00
0.85
0.92 76 (95.0%) 73 (91.3%)
3 ICC(2,1)
ICC(2,k)
0.99
1.00
0.97
0.98
0.86
0.93 68 (85.0%) 66 (82.5%)
4 ICC(2,1)
ICC(2,k)
0.99
0.99
0.96
0.98
0.91
0.95 77 (96.3%) 73 (91.3%)
5 ICC(2,1)
ICC(2,k)
1.00
1.00
1.00
1.00
0.84
0.91 79 (98.8%) 77 (96.3%)
6 ICC(2,1)
ICC(2,k)
1.00
1.00
0.99
0.99
0.88
0.94 77 (96.3%) 74 (92.5%)
7 ICC(2,1)
ICC(2,k)
1.00
1.00
1.00
1.00
0.90
0.95 78 (97.5%) 73 (91.3%)
8 ICC(2,1)
ICC(2,k)
1.00
1.00
0.94
0.97
0.67
0.81 78 (97.5%) 76 (95.0%)
9 ICC(2,1)
ICC(2,k)
1.00
1.00
1.00
1.00
0.99
0.99 78 (97.5%) 77 (96.3%)
10 ICC(2,1)
ICC(2,k)
1.00
1.00
1.00
1.00
0.99
1.00 80 (100%) 66 (82.5%)
Total N of
equal scores
374 (93.5%)
346 (86.5%)
† N=number of profiles representing the number and percentage of right answers for both
SLEDAI-2K and SRI-50 scores as compared to the “Standard” SLEDAI-2K and SRI-50
solutions respectively

73
Categorical data for the SLEDAI-2K and SRI-50 are presented in (Table 18). Of 400 patient
profiles that were completed by 10 raters, 374 (93.5%) and 346 (86.5%) were concordant with
the “Standard” results of SLEDAI-2K and SRI-50, respectively. The mean SLEDAI-2K scores
were 11.83 ± 7.02, 11.83 ± 7.04, and 11.90 ± 7.09 in round 1 and round 2 and as per the
“Standard,” respectively. There was no statistically significant difference between round 1
compared to round 2 (p = 0.82). However, round 1 versus “Standard” (0.07 ± 0.71; p = 0.05) and
round 2 versus “Standard” (0.08 ± 0.67; p = 0.020) showed results that were either statistically
significant or borderline significant, but the actual differences from the “Standard” were not
clinically significant.
The mean SRI-50 scores were 5.93 ± 3.34, 5.89 ± 3.33, and 5.98 ± 3.40 in round 1 and round 2
and per the “Standard,” respectively. There was no statistically significant difference between
round 1 versus round 2 (p = 0.28) or round 1 versus the “Standard” (p = 0.12). There was a
statistically significant difference between round 2 compared to “Standard” of 0.08 ± 0.46 (p =
0.02), but this was not clinically significant. Substantial agreement was determined for interrater
LS scores, with a kappa statistic of 0.57 (95% CI 0.49–0.66) [93, 105].

74
5.4 Discussion
Prior to use in clinical research or clinical practice, a health status measurement tool should be
valid, reliable, and responsive for its intended use in its intended population [92]. We previously
demonstrated that the SRI-50 is valid and is able to measure ≥ 50% improvement in disease
activity of patients with lupus between visits4. In this study we have demonstrated that SRI-50 is
reliable.
In our study, we evaluated both inter- and intraobserver reliability. To determine intrarater
reliability, the rheumatologists reevaluated the same patient scenarios on 2 occasions, 14 days
apart [93]. We developed patient scenarios to assure that all the descriptors were present,
including some relatively rare manifestations of lupus. We used the valid standardized SRI-50
data retrieval form to help minimize other sources of variability [11].
The use of patient profile scenarios as compared to live case scenarios has been reported. Case
scenarios were previously adopted in the initial development and validation of the SLEDAI, the
SDI, and the ACR response criteria for SLE clinical trials [5, 24, 107]. A recent study showed
that the use of paper case scenarios to determine the interrater reliability of triage scales in the
emergency department is an efficient method that approximates that of live cases. Further, the
authors concluded that if the results are found to be within an acceptable performance range,
further testing of interrater reliability using live cases may be unnecessary [108]. In our study,
the results of the ICC for SRI-50 exceeded 0.90, ensuring reasonable reliability [106].
For test-retest and interrater reliability, indexes of agreement are required as opposed to tests of
association. The ICC deals with continuous data and is sensitive to systematic biases between
observers or administration times and, more importantly, it is sensitive to both association and
agreement [92, 93, 106, 109]. The kappa statistic deals better with categorical data. In this study,
we adopted the ICC in determining the reliability of SRI-50, SLEDAI-2K, and PGA and the
kappa statistic in determining the reliability of the LS results. We observed high ICC for
interrater and intrarater, confirming the reliability of SRI-50 along with SLEDAI-2K. These
findings are in agreement with studies that also have demonstrated that the original SLEDAI and
its updated version, SLEDAI-2K, are reliable indices [21, 35, 36, 110]. Further, when we
converted the results of SLEDAI-2K and SRI-50 into categorical data, we found no clinically

75
significant difference compared with the “Standard.” Our study thus provides evidence that
rheumatologists from different centers and different countries are able to assess disease activity
by SRI-50 along with SLEDAI-2K 30 days in a particular patient in a similar way. This
information is useful for collaborative studies of patients with SLE that include the assessment of
disease activity.
Model 2 of the ICC (2,1) was adopted in our study. This model partitions the total variance into
effects due to differences between subjects, differences between raters, and error variance [106].
In this model, patients are evaluated by the same raters, and these raters are considered
representative of a large population of similar raters. More important, we chose this model for
our study because we were interested in establishing the SRI-50 intrarater and interrater
reliability and documenting that SRI-50 has a broad application [106]. Our results confirmed that
the SRI-50 can be used with confidence and equally by all rheumatologists despite heterogeneity
in the level of training [106].
Guidelines for acceptable ICC values vary. Streiner and Norman suggest that a tool with good
reliability when studying groups of people should have an ICC exceeding 0.85, and Tammemagi,
et al lower the cutoff value to > 0.75 to be acceptable [111, 112]. McHorney and Tarlov, among
others, required to have a coefficient > 0.90 when interpreting individual data rather than group
data [113]. In our study, the test-retest and intrarater coefficients exceeded 0.9. The raters’ recall
bias for test-retest reliability was eliminated with the methodology adopted in our study, where
patients were reevaluated after at least 14 days [93]. The reliability for PGA exceeded 0.9 and LS
scores showed substantial agreement for interrater LS scores with kappa statistics.
Several factors can improve the reliability of a measurement and, to improve the reliability of
SRI-50, we intended to ensure the presence of the following factors: (1) using more clearly
written descriptors with universally understood words; and this was confirmed to be present in
both SRI-50 definitions and SRI-50 data retrieval forms [11]; (2) selecting clear detailed
definitions to cover all the aspects within each descriptor; and (3) using categorical and
numerical rating scales in each of the descriptors, whenever applicable, instead of dichotomous
response choices. As examples, numerical scales are used to determine if there is an
improvement in headache, pleurisy, cranial nerve disorder, alopecia, pericarditis; and categorical
scales to determine the improvement in myositis, alopecia, and rash [96] .

76
Overall, the performance of the SRI-50 was excellent, despite the mis-scorings that occurred
during this study. Virtually all the mis-scorings were rater failures rather than instrument
failures. Indeed, the mis-scorings that resulted from the scoring of the laboratory descriptors and
the calculation of the 50% improvement could be avoided by more accurate readings of the
cases. It is very important that all rheumatologists familiarize themselves with the definitions of
SLEDAI-2K initially and then learn the SRI-50 to ensure better performance. In research centers
and clinical trials, the laboratory data that include lupus serology (complements and anti-
dsDNA), white blood cell counts and platelets, and urinalysis variables are entered and analyzed
systematically in the database after being reviewed by rheumatologists. The review by
rheumatologists is not just for the purpose of patient safety; it is also to assess whether
abnormalities are due to SLE and in some cases (such as drug toxicities) might override scoring
of some of these on the SLEDAI. Using the SRI-50 data retrieval form would help to minimize
mistakes when transferring the data from laboratory reports.
The training of all rheumatologists to accomplish this task is crucial. An SRI-50 manual has been
developed for this purpose, along with an electronic version of the SRI-50. The dedicated
website for SRI-50 is under construction at this time. This will include training and examination
modules, after which certification will be granted for successful completion of the examination
module.
Our study shows that the SRI-50 is reliable in detecting ≥ 50% improvement in disease activity
between visits in patients with lupus [11]. Thus SRI-50 can be adopted as a responder index in
clinical and research settings and in clinical trials.
This paper has been published in:
Touma Z, Urowitz MB, Fortin PR, Landolt-Marticorena C, Toloza SM, Riddell C, Chandran V,
Eder L, Ghanem A, Ziouzina O, Taghavi-Zadeh S, Ibañez D, Gladman DD. SLEDAI-2K
Responder Index (SRI)-50: A Reliable Index for Measuring Improvement in Disease Activity. J
Rheumatol 2011:38:868-73. [95]

77
Chapter 6 SLEDAI-2K Responder Index (SRI-50) captures 50% improvement in disease activity over 10 years
This study has been submitted to:
Touma Z, Gladman DD, Ibanez D, Urowitz MB. SLEDAI-2K Responder Index (SRI-50)
captures 50% improvement in disease activity over 10 years. Lupus 2011 December 22
(submitted).

78
6.1 Background
The Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K) Responder
Index 50 (SRI-50) was developed and validated as a responder index derived from SLEDAI-2K
for the measurement of improvement of disease activity in SLE [4, 5, 7, 11]. SRI-50 captures
partial improvement in each of the active descriptors at subsequent visits and generates a lower
weighted score to the improved descriptors as compared to SLEDAI-2K. SRI-50 is a reliable
index and has been successfully evaluated and used by expert clinicians and trainees [95]. This
responder index has shown ability in research settings to identify patients with clinically
meaningful improvement and currently is been evaluated in ongoing clinical trials of new drugs
in lupus [11, 51]
The SRI-50 includes the same 24 descriptors of SLEDAI-2K with new definitions to each of the
SRI-50 descriptors which can measures ≥ 50% improvement. The sum of all 24 descriptors
generates a total score for SRI-50 describing disease activity overall as in SLEDAI-2K [11]. In
SRI-50 the clinical and laboratory data is collected in a standardized manner using the validated
SRI-50 data retrieval form [11]. In the initial phase of SRI-50 validation, SRI-50 was found to be
superior to SLEDAI-2K in identifying “responders” at 3 months [11]. A more recent study
confirmed that SRI-50 identified more responders as compared to SLEDAI-2K in patients
evaluated at 6 and 12 months [114].
One of the acceptable modalities in the validation of new measures is to use available data from
an existing database. This approach allows the validating of new measures over a short period of
time. Nevertheless, a retrospective validation of SRI-50 required that the data was collected in a
standardized way as mandated by SRI-50 definitions and the SRI-50 data retrieval form. At the
Lupus Clinic, data has been collected prospectively since 1970. The data was available on the 3
laboratory organ systems out of the total 9 organ systems of SLEDAI-2K and SRI-50 which
allowed us to conduct this study.

79
In this study we aimed: 1) to determine, in a 10 year period, the frequency of complete (by
SLEDAI-2K) and partial ( 50% by SRI-50) recovery in the active descriptors of 3 systems at
subsequent follow-up visits, 2) to determine the time to complete (by SLEDAI-2K) and partial
recovery ( 50% by SRI-50) in the active descriptors at subsequent follow-up visits and 3) to
determine the percent of patients who achieved complete (by SLEDAI-2K) and partial ( 50%
by SRI-50) recovery within 1 year of onset of active descriptors.
6.2 Methods
6.2.1 Patients’ selection and assessment
This is a retrospective analysis conducted on patients enrolled in the prospective longitudinal
Lupus Cohort at the Toronto Western Hospital, Toronto, Ontario, Canada. Patients with SLE
(four or more ACR criteria or three ACR criteria plus a typical histological lesion of SLE on
renal or skin biopsy) have been followed prospectively at the University of Toronto Lupus Clinic
[98, 115] Collection and storage of data at the lupus clinic were conducted in accordance with
the Declaration of Helsinki and approved by the Research Ethics Board of the University Health
Network. Signed informed consent was obtained from all patients at the lupus clinic. Patients
attended the lupus clinic at 2 to 6 month intervals regardless of the state of activity of their lupus.
The standard protocol of patients’ assessment included: complete history, physical examination
and laboratory evaluation. Disease activity was measured at each visit by the SLEDAI-2K, a
valid measure of disease activity in SLE [5, 7]. Based on the available data we were able to
calculate SRI-50 scores on follow-up visits in 3 organ systems in particular, renal,
immunological and hematologic.

80
6.2.2 Study design
This retrospective analysis was conducted on the prospectively collected data available on all
consecutive patients who attended the Lupus Clinic between January 2000 and October 2010 and
who had a minimum of 6 regular visits (every 4-6 months).
6.2.3 Outcome measures
Standardized data was available on the 3 laboratory organ systems out of the total 9 organ
systems of SLEDAI-2K and SRI-50 as follows: 1) Renal system descriptors: casts, hematuria,
proteinuria and pyuria 2) Immunological system descriptors: low complement and increased
anti-DNA antibodies and 3) Hematologic system descriptors: thrombocytopenia and leucopenia
(Table 19).

81
Table 19. SLEDAI-2K definitions and definitions of improvement by SRI-50
Descriptors Definitions of SLEDAI-
2K
Weighted
score
Definitions of SRI-50
improvement
Weighted
score
Urinary casts Heme-granular or red
blood cell casts.
4 Decrease by ≥50% in the total
number of casts (heme-granular
red blood cell casts).
2
Hematuria >5 red blood cells/high
power field. Exclude
stone, infection, or other
cause.
4 Decrease by ≥50% in the number
of red blood cell /high power
field.
2
Proteinuria New onset, recurrent, or
persistent proteinuria of
more than > 0.5 gram/24
hours.
4 Decrease by ≥50% in the range of
proteinuria.
2
Pyuria >5 white blood cells/ high
power field. Exclude
infection.
4 Decrease by ≥50% in the number
of white blood cells/ high power
field.
2
Low Complement Decrease in CH50, C3, or
C4 below the lower limit
of normal for testing
laboratory.
2 ≥50% increase in the level of any
complement or normalization of
one of them without a drop in
either.
1
Increased anti-DNA
antibodies levels
Increase in the level of
anti-DNA antibodies
above normal range for
testing laboratory.
2 ≥50% reduction in the level of
anti-DNA antibodies.
1
Thrombocytopenia
<100,000 platelets/ x
109/L. Exclude drug
causes.
1 ≥50% increase in the level of
platelets but <100,000
platelets/mm3.
0.5
Leukopenia <3,000 white blood
cells/x 109/L. Exclude
drug causes.
1 ≥50% increase in the level of
white blood cells but
<3,000/mm3.
0.5

82
6.2.4 Identification of patients with active descriptors
Patients with onset of active descriptors were identified during the study period based on
SLEDAI-2K definitions (Table 19). Each patient could contribute to each descriptor only once
during the study period.
6.2.5 Identification of patients’ descriptors with ≥ 50% and complete
recovery
Active descriptors were deemed to have partial (≥ 50%) or complete recovery at subsequent
follow-up visits if the recovery met the definitions of SRI-50 or SLEDAI-2K respectively (Table
19).
6.2.5.1 Time to partial and complete recovery for active descriptors
Time to complete recovery reflected the time when SLEDAI-2K descriptor goes from onset of
activity to complete recovery at subsequent follow-up visit (descriptor = 0) as defined by
SLEDAI-2K. Time to partial recovery reflected the time when SLEDAI-2K descriptor goes from
onset of activity to partial recovery at subsequent follow-up visit as defined by SRI-50
definitions.

83
6.2.6 Possible situations for progression in disease activity in active
descriptors as determined by SRI-50 and SLEDAI-2K
For each of the 8 descriptors, the following possible situations have been identified:
Situation 1: Descriptor goes from active to complete recovery (descriptor = 0).
Situation 2a: Descriptor goes from active to an identified partial (≥50%) recovery by SRI-50
and, at a later date, to a complete recovery by SLEDAI-2K.
Situation 2b: Descriptor goes from active to an identified partial (≥50%) recovery by SRI-50
and has not yet completely recovered by SLEDAI-2K as of the last clinic visit.
Situation 3: Descriptor goes from active and has not achieved at least partial (≥50%) recovery
by SRI-50 as of the last clinic visit (Figure 1).

84
Figure 1. Different situations for active descriptors as determined by SRI-50 and SLEDAI-
2K on follow-up visits as compared to initial visit
Complete recovery (by SLEDAI-2K)
Partial recovery (≥50% by SRI-50)
6.2.7 Statistical analysis
Descriptive statistics were used to describe the characteristics of the patients and the results of
the analysis (proportions and percentages). We identified the number and percentage of active
descriptors and determined their partial (≥ 50% by SRI-50) along with complete recovery (by
SLEDAI-2K) at subsequent follow-up visits within the first year and over 10 years. We
evaluated time to partial and complete recovery (mean time in months) for all active descriptors
at subsequent follow-up visits. The same analysis was also applied for each of the situations
listed above (situation 1, 2a, 2b, and 3) to calculate the percentage of partial and total recovery
along with the time to partial and complete recovery among the active descriptors. The statistical

85
software SAS (version 9.2; SAS Institute, Cary, NC) was used for all statistical analyses, and the
significance level was set at 5%.
6.3 Results
6.3.1 Demographics
795 patients and 13796 visits were identified over the study period. The patients included 700
(88%) females and 95 (12%) males. Sixty four percent of the patients were Caucasian, 14%
Black and 11% Asian and 11% others. The mean (±std) length of follow–up for patients in the
study period was 6.1 ± 3.1 years.
6.3.2 Partial and complete recovery in active descriptors over 10 years
Of the 795 patients, 748 patients (94%) had an active organ system (defined as activity of at least
one descriptor within a specific system) at some point during the study period as follows: 516
patients had active renal system, 667 patients had active immunological system and 207 patients
had active hematologic system. Four hundred and ninety two patients (66%) of the 748 patients
showed partial (50%) recovery by SRI-50 in at least one of the active descriptors among the 3
studied systems. The identified partial recovery by SRI-50 in the active descriptors was not
discerned by SLEDAI-2K. In the renal system, SRI-50 identified an overall recovery in 174
(34%) of the 516 patients, in the immunological system 420 (63%) of the 667 patients, and in the
hematological system 52 (25%) of the 207 patients (Table 20).

86
Table 20. Frequency, time to partial and complete recovery among active descriptors
Active
descriptors*
n
PR †
N
TPR †
situation 2
CR †
n
TCR †
situations 1 and 2a
Casts 324 32 4.97 ± 4.10 314 6.69 ± 6.06
Hematuria 199 57 6.79 ± 5.43 174 10.44 ± 11.77
Proteinuria 288 109 9.65 ± 7.79 244 13.69 ± 15.05
Pyuria 308 60 6.94 ± 5.44 274 8.92 ± 9.77
Low complements 572 293 12.58 ± 12.50 434 17.64 ± 18.57
DNA 542 288 15.29 ± 16.11 321 20.69 ± 23.38
Thrombocytopenia 68 10 16.94 ± 24.93 57 10.33 ± 17.49
Leukopenia 166 42 8.91 ± 10.33 149 9.02 ± 10.21
n number
*At onset of active descriptors during the study period
† Identified at subsequent follow-up visits during the study period
CR Complete Recovery (by SLEDAI-2K)
PR Partial Recovery (≥50% by SRI-50)
TCR Time to Complete Recovery (by SLEDAI-2K)
TPR Time to Partial Recovery (≥50% by SRI-50)
Time is represented in months in the table 20

87
6.3.3 Partial and complete recovery in active descriptors with 1 year
The percentage of active descriptors that achieved a partial and complete recovery at subsequent
follow-up visits within 1 year of onset of activity was always greater than the percentage of
descriptors with complete recovery (Table 21).
Table 21. Frequency of partial and complete recovery in active descriptors within 1 year
from the onset of activity
Active
descriptors*
n
CR † CR or PR †
Casts 324 273 (84.3%) 284 (87.7%)
Hematuria 199 134 (67.3%) 160 (80.4%)
Proteinuria 288 137 (47.6%) 193 (67.0%)
Pyuria 308 223 (72.4%) 248 (80.5%)
Low complements 572 230 (40.2%) 365 (63.8%)
DNA 542 169 (31.2%) 306 (56.5%)
Thrombocytopenia 68 48 (70.6%) 54 (79.4%)
Leukopenia 166 122 (73.5%) 134 (80.7%)
*at the initial visit in the study
† Improvement at subsequent follow-up visit with the 1st year from onset of active descriptor
CR Complete Recovery (by SLEDAI-2K)
PR Partial Recovery (≥50% by SRI-50)

88
6.3.3.1 Time to partial and complete recovery in active descriptors over
the course of 10 years
As expected the time to partial recovery by SRI-50 was shorter than the time to complete
recovery by SLEDAI-2K for all descriptors in 3 systems. Since partial recovery will occur prior
to complete recovery by construct, all p values are highly significant (data not shown). Similarly
the time to partial recovery was always shorter than the time to complete recovery in all possible
situations of progression in disease activity (Table 22).

89
Table 22. Time to partial and complete recovery among active descriptors in different
situations
Situations Active
descriptors*
N
TPR † TCR † Time to last
clinic visit †
Casts
1 284 6.07 ± 5.23
2a 30 5.08 ± 4.22 12.60 ± 9.48
2b 2 3.22 ± 0.09 6.54 ± 0.74
3 8 3.49 ± 4.37
Hematuria
1 123 7.17 ± 6.26
2a 51 6.39 ± 5.36 18.34 ± 17.13
2b 6 10.20 ± 5.26 22.58 ± 17.07
3 19 5.77 ± 7.92
Proteinuria
1 140 9.14 ± 11.73
2a 84 8.89 ± 6.77 21.28 ± 16.88
2b 25 12.22 ± 10.28 34.24 ± 24.92
3 39 16.48 ± 21.80
Pyuria
1 255 7.49 ± 8.90
2a 49 6.91 ± 5.55 15.48 ± 10.94
2b 11 7.06 ± 5.17 18.00 ± 12.32
3 23 3.20 ± 7.76
Low complements
1 232 9.81 ± 11.03
2a 202 10.22 ± 10.62 26.63 ± 21.24 54.36 ± 34.71
2b 91 17.82 ± 14.66 40.50 ± 37.21
3 47
DNA
1 166 9.97 ± 13.58
2a 155 12.56 ± 13.01 32.17 ± 26.11
2b 133 18.49 ± 18.64 60.48 ± 34.87
3 88 46.32 ± 35.67
Thrombocytopenia
1 51 6.68 ± 9.09
2a 6 19.97 ± 32.31 41.31 ± 36.22
2b 4 12.39 ± 8.83 36.97 ± 32.27
3 7 15.98 ± 23.42
Leukopenia
1 110 5.84 ± 5.29
2a 39 9.05 ± 10.65 17.97 ± 14.64
2b 3 7.19 ± 5.25 20.81 ± 17.19
3 14 2.61 ± 4.85
n number
*At onset of active descriptors during the study period
† Identified at subsequent follow-up visits during the study period
CR Complete Recovery (by SLEDAI-2K)
PR Partial Recovery (≥50% by SRI-50)
TCR Time to Complete Recovery (by SLEDAI-2K)
TPR Time to Partial Recovery (≥50% by SRI-50)
Time is represented in months in the table 22

90
6.4 Discussion
SRI-50 is a novel reliable responder index derived from the SLEDAI-2K that was initially
developed in 2009 [Arthritis Rheum 2010 (abstract);60 Suppl:S899] [11, 95] This was followed
up by further prospective validation for SRI-50 over 3 months and 12 months [11, 51, 114]. In
the derivation of SLEDAI-2K, researchers were focused on describing disease activity in the 24
descriptors of SLEDAI-2K as either present or absent. Subsequently, an improvement in the
SLEDAI-2K descriptors is captured when a manifestation has completely resolved. In the
currently adopted outcomes for the assessment of disease activity in rheumatoid arthritis and
psoriatic arthritis, an improvement is based on the decrease in the severity of the manifestations
and this is reflected by the decrease in the joint count and not necessarily a complete resolution
of arthritis. This should also be applied to lupus patients and lupologists need to be able to
measure a clinically meaningful improvement in each of the manifestations in a standardized
way. SRI-50 was developed and validated based on this principle and thus might improve and
facilitate the identification of responders in research studies and clinical trials [115].
In the current study we proposed a validation of SRI-50 using the available data on 795 patients
and 13796 visits that were collected in the Lupus Clinic over the last 10 years. This validation
was conducted on 3 of the 9 organ systems of SRI-50, in particular, renal, hematological and
immunological systems. The availability of standardized data on all 8 descriptors of the 3 organ
systems has allowed us to calculate SRI-50 scores on follow-up visits. The use of SRI-50 has
allowed the identification of the descriptors with partial improvement during the study period.
This was very useful in particular for the situations where patients initially recovered partially
than completely and in the situations where only a partial recovery occurred as of last clinic
visits. More importantly, by definition, the time to partial recovery (by SRI-50) in the active
descriptors preceded the time to complete recovery (by SLEDAI-2K). This is important
especially in research studies and clinical trials where time plays a major role.
Although only the 3 laboratory systems were studied, 66% of the patients showed partial, ≥50%,
improvement by SRI-50 in at least one of their active descriptors over the study period. The use

91
of SRI-50 and SRI-50 data retrieval form allows the documentation and derivation of scores in a
standardized manner.
In conclusion in a research setting SRI-50 was able to identify clinically important improvements
in active laboratory descriptors in an efficient time on data available over 10 years.
This study has been submitted to:
Touma Z, Gladman DD, Ibanez D, Urowitz MB. SLEDAI-2K Responder Index (SRI-50)
captures 50% improvement in disease activity over 10 years. Lupus 2011 December 22
(submitted).

92
Chapter 7 SRI-50 Enhances the Ability to Identify Responders
This paper has been published in:
Touma Z, Gladman DD, Taghavi-Zadeh S, Ibañez D, Urowitz MB SLEDAI-2K Responder
Index (SRI)-50 enhances the ability to identify responders in clinical trials. J Rheumatol 2011
Sep 1. [Epub ahead of print] [51]

93
7.1 Background
With the advent of potential new therapies for systemic lupus erythematosus (SLE), there is a
great need to refine the SLE Disease Activity Index 2000 (SLEDAI-2K) to be able to measure
partial clinically important improvement, ≥ 50%, in disease activity in clinical trials. For this
purpose the SLEDAI-2K Responder Index-50 (SRI-50) was developed in 2009 [Arthritis Rheum
2010 (abstract);60 Suppl:S899] [11]. In 2010, the initial validation of SRI-50 was reported
[Arthritis Rheum 2010 (abstract);62 Suppl:S785]. As a first effort toward validating SRI-50, we
assessed its content validity, face validity, practical applicability including administration and
scoring, and concurrent construct validity [11]. We studied 141 patients with SLE and showed
that SRI-50 is a valid index that detects clinically significant improvements (≥ 50%) between
visits in patients with SLE [11]. SRI-50 was able to measure improvement in both clinical
disease manifestations and SLE-related laboratory abnormalities [11]. Further, SRI-50 detected
partial improvement between visits in some patients who improved but in whom the SLEDAI-
2K 30-day measure did not discern this improvement [4, 5, 7, 11]. The SRI-50 Data Retrieval
Form, developed and validated to standardize the documentation of the descriptors of SRI-50,
ensures the optimal performance of SRI-50 [11]. More recently we have shown that SRI-50 has
intrarater and interrater reliability and can be used by both rheumatologists and trainees, and
performs equally well with rheumatologists familiar with the instrument and those not familiar
with it [95]. To facilitate the introduction of SRI-50 for general use, an SRI-50 manual has been
developed along with a dedicated Website for SRI-50, www.sri-50.com. The Website includes
both training and examination modules that familiarize rheumatologists with the SRI-50
Definitions and the SRI-50 Data Retrieval Form and assesses their success in mastering the
instrument.
Evidence-based exploratory analysis of the B lymphocyte stimulating factor antagonist
belimumab in a phase II SLE trial led to the development of a novel responder index for SLE,
the SRI, able to define a clinically meaningful change in disease activity [52]. SRI is a composite
outcome that incorporates the modification of SLEDAI that was developed for the Safety of
Estrogens in Lupus Erythematosus: National Assessment trial (SELENA-SLEDAI), the British
Isles Lupus Assessment Group (BILAG) activity index, and the Physician’s Global Assessment
(PGA) [4, 10, 12, 49]. As proposed by the authors of SRI, the SELENA-SLEDAI score was used

94
to determine global improvement. The BILAG domain scores were used to ensure that no
significant worsening in organ systems has occurred (no new “A” score or 2 new “B” scores).
The PGA ensured that improvement in disease activity is not achieved at the expense of the
patient’s overall condition [52]. The SRI was initially assessed in a subset of 321 serologically
active patients in a phase II belimumab placebo-controlled clinical trial. In serologically active
patients, the addition of belimumab to the standard of care therapy resulted in a statistically
significant response in 46% of patients at Week 52 compared with 29% of the placebo patients
[52]. More recently, a phase III study of the effect of belimumab used this novel 3-part outcome
response measure and was able to show a statistically significant difference in response among
patients taking the drug as compared to placebo [53].
The purpose of our study was (1) to evaluate the performance of the SRI when the SLEDAI-2K
is substituted with the SRI-50; and (2) to determine if the SRI-50 will enhance the ability of the
SRI in detecting improvement in disease activity. We hypothesized that the substitution of
SLEDAI-2K with SRI-50 in the SRI increases the ability to identify patients with clinically
significant improvement [11, 52].
7.2 Methods
7.2.1 Patient enrollment and selection
All patients attending the Lupus Clinic from September 2009 to September 2010 were enrolled
in a prospective longitudinal study. All patients met the American College of Rheumatology
classification criteria for SLE [98]. At each visit a complete history was taken including
demographics, and a physical examination and laboratory tests were performed. Patients were
studied who had active SLE at the baseline visit, with SLEDAI-2K 30 days ≥ 4, and had 1 follow
up visit 1–3 months later [7].

95
7.2.2 Outcome measures
SLEDAI-2K is based on the presence of 24 descriptors in 9 organ systems over the patient’s past
30 days. The total score of SLEDAI-2K falls between 0 and 105, with higher scores representing
increased disease activity [5, 7]
The SRI-50 comprises the same 24 descriptors, covering 9 organ systems, and reflects disease
activity over the previous 30 days, as does SLEDAI-2K [5]. The SRI-50 data retrieval form
standardizes the documentation of the descriptors and performed extremely well in all
descriptors, which is especially relevant for multicenter studies that form the backbone of any
therapeutic evaluation for SLE [11]. The SRI-50 score is evaluated at the follow up visit and
corresponds to the sum of each of the 24 descriptors’ scores found on the SRI-50 data retrieval
form. The method of scoring is simple, cumulative, and intuitive, similar to the SLEDAI-2K.
One of 3 situations can occur when a descriptor is present at the initial visit: (1) the descriptor
has reached complete remission at follow up and the score would be “0”; (2) the descriptor has
not reached a minimum of 50% improvement at follow up and the score would be identical to its
corresponding SLEDAI-2K value; or (3) the descriptor has improved by ≥ 50% (according to the
SRI-50 definition) but has not achieved complete remission, in which case the score is evaluated
as half of the score that would be assigned for SLEDAI-2K. If a descriptor was not present at the
initial visit, the value for SRI-50 at the follow up visit will be the same as that for SLEDAI-2K.
This process is repeated for each of the 24 descriptors. Finally the SRI-50 score at follow up is
evaluated as the sum of the 24 individual descriptors’ scores.
The revised BILAG index (BILAG 2004) has been developed from the original index, based on
the principle of a physician’s intention to treat [12, 14]. BILAG 2004 includes 9 systems. Based
on physician’s intention to treat, the scoring of BILAG is categorized as follows: A = severe
disease activity, B = moderate disease activity, C = mild disease activity, D = inactive disease
but previously affected, and E = inactive with no previous involvement [14]. In BILAG 2004,
index items that are improving are scored less severely than those that are new, worse, or the
same. BILAG scores in this study were generated with the British Lupus Integrated Prospective
System [56].

96
During the baseline and follow up visit, a PGA was determined on a visual analog scale (VAS)
line of 100 mm, with anchors of 0 (no disease activity) and 10 (very active disease). Any
increase on PGA from baseline was considered clinically significant worsening. Patients with
worsening on PGA from baseline were defined as nonresponders to the SRI.
7.2.3 Patient assessment
At the baseline visit, SLEDAI-2K 30 days and BILAG scores were determined and the SRI-50
data retrieval form was completed [7, 12, 14].
At the follow up visit at 1–3 months, the SRI-50 data retrieval form was completed, and
SLEDAI-2K and SRI-50 scores were determined [11]. BILAG scores and PGA were determined.
Patients were treated with standard of care as determined by the treating rheumatologist.
7.2.4 Study design
SRI was determined at the follow up visit according to the original definition using SLEDAI-2K
score [52]. SRI was defined as (1) ≥ 4-point reduction in SLEDAI-2K score, (2) no new BILAG
A or no > 1 new BILAG B domain score, and (3) no deterioration from baseline in the PGA.
The SLE Responder Index was further evaluated in the same group of patients, but this time
substituting SLEDAI-2K with SRI-50 [11]. Patients who showed worsening in disease activity
on the follow up visit (an increase in the SLEDAI-2K score) were excluded from the analysis.
7.2.5 Statistical analysis
Descriptive statistics were used for the characteristics of the patients and the results of the
analysis (proportions and percentages). We determined the number of responders who met the
SRI on the follow up visit using SLEDAI-2K and SRI-50. We determined the mean change of

97
SLEDAI-2K scores among all patients [Δ SLEDAI-2K = SLEDAI-2K (baseline to follow up)]
and the mean change of SRI-50 scores [Δ SRI-50 = SLEDAI-2K (baseline) to SRI-50 (follow
up)]. The paired t test was used to compare the mean Δ SLEDAI-2K and the mean Δ SRI-50
scores.
7.3 Results
7.3.1 Patient demographics
One hundred seventeen patients had baseline SLEDAI-2K ≥ 4 and a follow up visit and were
studied further. The patient profiles included 106 (90.6%) women and 11 (9.4%) men. Fifty-five
percent were white, 19% black, 10% Asian, and 16% others. The age at baseline visit was 42.0 ±
14.0 years and disease duration at baseline was 13.0 ± 10.1 years. The time from baseline to
follow up visits was 3.0 ± 1.2 months (Table 23).
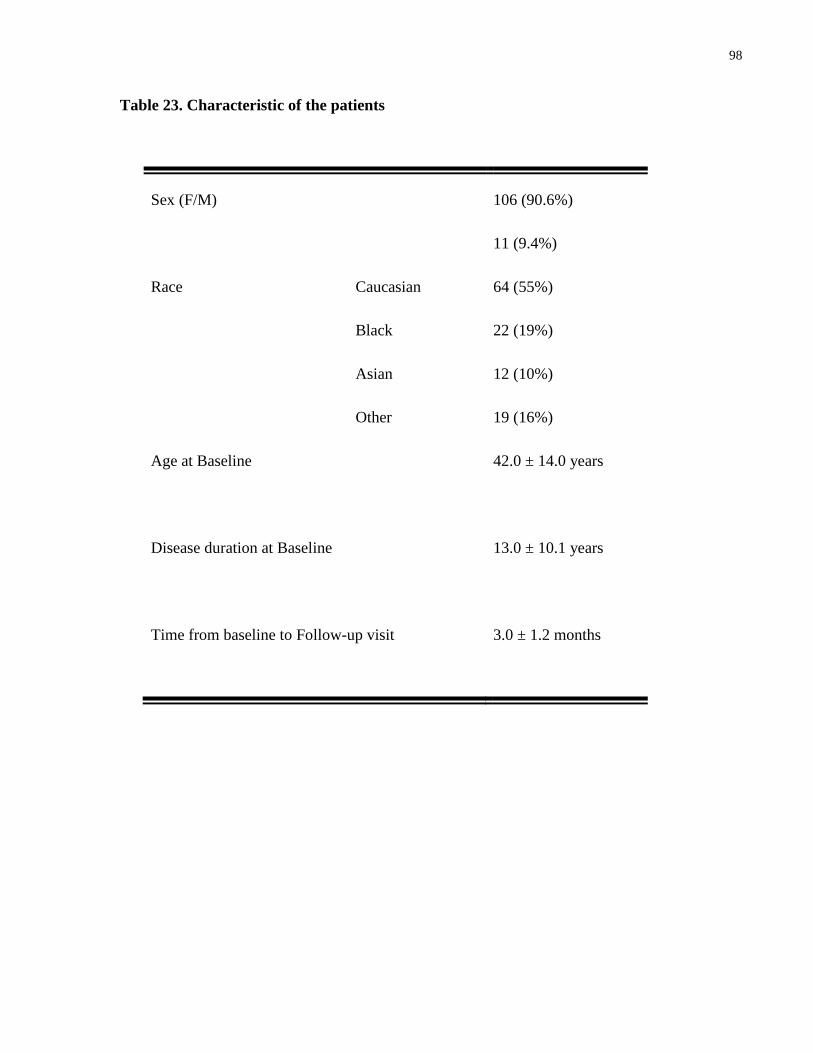
98
Table 23. Characteristic of the patients
Sex (F/M)
106 (90.6%)
11 (9.4%)
Race Caucasian
Black
Asian
Other
64 (55%)
22 (19%)
12 (10%)
19 (16%)
Age at Baseline
42.0 ± 14.0 years
Disease duration at Baseline
13.0 ± 10.1 years
Time from baseline to Follow-up visit
3.0 ± 1.2 months

99
7.3.2 Disease activity results
Mean SLEDAI-2K scores were 8.02 ± 4.53 at baseline visit and 5.82 ± 4.50 at follow up visit,
while mean SRI-50 scores were lower at 5.10 ± 3.95 at follow up (p < 0.0001). The mean change
of SLEDAI-2K scores (Δ SLEDAI-2K) among all patients was −2.20 ± 2.87 and the mean
change of SRI-50 scores (Δ SRI-50) was −2.91 ± 3.03. The mean change Δ SLEDAI-2K and the
mean change Δ SRI-50 scores at follow up visits were statistically significantly different (p <
0.0001; Table 24 and Figure 2.
Figure 2. Disease activity scores at baseline and follow-up
0
1
2
3
4
5
6
7
8
9
BASELINE SLEDAI-2K SLEDAI-2K follow-up SRI-50 follow-up

100
Table 24. Disease activity results
SLEDAI-2K at Baseline
8.02 ± 4.53*
SLEDAI-2K at Follow-up
5.82 ± 4.50*
SRI-50 at Follow-up
5.10 ± 3.95*
∆ SLEDAI-2K
(SLEDAI-2K Baseline -SLEDAI-2K Follow-up )
-2.20 ± 2.87*
∆ SRI-50
(SLEDAI-2K Baseline - SRI-50 Follow-up)
-2.91 ± 3.03*
Number of patients who met SRI
(Using SLEDAI-2K)
(Using SRI-50)
34 (29%) patients
41 (35%) patients
*The p value of SLEDAI-2K (Baseline) vs. SLEDAI-2K (Follow-up) scores was <0.0001
The p value of SLEDAI-2K (Baseline) vs. SRI-50 (Follow-up) scores was <0.0001.
The p value of ∆ SLEDAI-2K (Follow-up) vs. ∆ SRI-50 (Follow-up) scores was <0.0001

101
Thirty-four patients (29%) met the original definition of SRI. Forty-one patients (35%) met the
definition of SLE Responder Index when SLEDAI-2K was substituted with SRI-50 score. The
use of SRI-50 definitions allowed determination of a clinically significant improvement in 7
additional patients (Table 24 and Figure 3).
Figure 3. Percentage of patients who met SLE Responder Index definition
0%
5%
10%
15%
20%
25%
30%
35%
40%
Using SLEDAI-2K Using SRI-50

102
7.4 Discussion
In light of the complexity and heterogeneity of SLE manifestations, it has become clear that a
reliable, valid responder index is required to accurately detect and verify the efficacy of new
therapeutic strategies in clinical trials. We have recently described the development and
validation of SRI-50 [11]. The newly developed SRI-50 is a reliable and valid index to reflect
partial important improvement (≥ 50%) in disease activity between visits in response to
treatment.
We compared the performance of SRI on 117 patients with active disease treated with standard
of care and followed up after 3 months. The advantage of using SRI-50 instead of SLEDAI-2K
as a component of SRI was demonstrated by increasing the percentage of responders from 29%
to 35%. This degree of improvement could not be discerned with the use of SLEDAI-2K as a
component of SRI. In our previous study, we used SRI-50 in 141 patients and showed that the
decrease in SRI-50 scores was clinically significant, meeting the accepted definition of
improvement of a decrease in SLEDAI-2K of ≥ 4. This improvement was not achieved with
SLEDAI-2K scores on followup visits [11]. Indeed, this reflected the ability of SRI-50 to detect
partial and important improvement between visits in patients who improved, while the SLEDAI-
2K did not discern this improvement. In our current study, we showed that on followup visits,
SRI-50 scores in studied patients decreased to a greater extent compared to SLEDAI-2K scores,
and this was statistically significant (p < 0.0001). This difference between SRI-50 and SLEDAI-
2K scores resulted from the ability of SRI-50 to pick up partial improvement in the descriptors
that meet the SRI-50 definitions of improvement. The results of the previous and current studies
encourage the use of SRI-50 as an independent outcome measure of disease activity
improvement in current trials [11].
It is important to note that the original SLE Responder Index used in the belimumab trials
required for response “no more than 0.3 units increase in the PGA using the point scoring on the
SELENA-SLEDAI PGA.” In our study no worsening was allowed in the PGA using the VAS of
100 mm. The SELENA trial proposed a new modification of SLEDAI. In the SELENA-
SLEDAI, several descriptors were modified in particular: visual disturbance, pleurisy and
pericarditis, arthritis, and others. For instance, SLEDAI and its new version SLEDAI-2K
mandate the presence of subjective (pleuritic or pericardial pain) and objective (rub, effusion,
103
electrocardiogram or echocardiogram confirmation, or pleural thickening) findings for pleurisy
and pericarditis to be scored as present. In the SELENA-SLEDAI, researchers accepted the
presence of either the objective or subjective findings to score the descriptor as present. Despite
the modifications in some of the descriptors, SELENA-SLEDAI acts similarly to SLEDAI-2K. It
is important to highlight that there has been no validation of all of the modifications introduced
in SELENA-SLEDAI. Thus the SELENA-SLEDAI version lacks the stringent validation steps
that are essential before a measure can be used in clinical trials or research settings. SLEDAI-2K
was validated against SLEDAI using the entire cohort of the University of Toronto Lupus Clinic.
In our research center we have used the SLEDAI-2K and not the SELENA-SLEDAI. We have
also used SLEDAI-2K to assess the patients in our current study. Thus the first component of the
SRI was determined using SLEDAI-2K. The modification of PGA and SELENA-SLEDAI in the
SRI definition would be unlikely to change the outcome of our study. Nevertheless, it does
require clarification that this protocol is not identical to the original PGA component and
SLEDAI component of the SRI and should be referred to as a modified SRI.
Retrospective application of the SRI to data from a phase II randomized controlled trial of
belimumab in patients with active SLE demonstrated that belimumab treatment resulted in a
statistically larger percentage of responders than treatment with placebo [116]. More recently,
SRI was used as the primary outcome measure in a multicenter phase 3 study at Week 52. The
results showed that belimumab with standard of care resulted in a significantly higher response
rate than did placebo with standard of care at Week 52. Belimumab 10 mg/kg resulted in a
significantly greater response than did placebo in all 3 SRI components, while belimumab 1
mg/kg resulted in a greater response than did placebo in 2 components (SELENA-SLEDAI and
PGA) [53]. It is likely that the percentage of responders in this trial would have been higher and
still be clinically significant had SRI-50 been used rather than SELENA-SLEDAI.
The results of our study showed that SRI-50 detects partial but clinically important improvement
(≥ 50%) in disease activity between visits in response to treatment. The substitution of SRI-50
for SLEDAI-2K in the SRI increases its ability to identify responders. This validation of the SRI-
50 enables it to be used as an outcome measure in clinical trials.

104
This paper has been published in:
Touma Z, Gladman DD, Taghavi-Zadeh S, Ibañez D, Urowitz MB SLEDAI-2K Responder
Index (SRI)-50 enhances the ability to identify responders in clinical trials. J Rheumatol 2011
Sep 1. [Epub ahead of print] [51].

105
Chapter 8 Systemic Lupus Erythematosus Disease
Activity Index 2000 (SLEDAI-2K) Responder Index 50
(SRI-50): Sensitivity to Response at 6 and 12 Months
This study has been accepted and is in press:
Touma Z, Urowitz MB, Taghavi-Zadeh S, Ibañez D, Gladman DD. Systemic Lupus
Erythematosus Disease Activity Index 2000 (SLEDAI-2K) Responder Index (SRI)-50 identifies
more responders than Systemic Lupus Erythematosus Responder Index (SRI) at 6 and 12 months
Rheumatology (Oxford) January 2012 (In press) [114].

106
8
8.1 Background
The assessment of disease activity in systemic lupus erythematosus (SLE) depends on the use of
standardized, reliable and validated indices. A number of measures have been developed to
assess lupus disease activity. The Systemic Lupus Erythematosus Disease Activity Index
(SLEDAI) is a global index that was developed and introduced initially in 1985 as a clinical
index for the assessment of disease activity overall [4]. The newer version of SLEDAI, SLEDAI-
2000 (SLEDAI-2K) allows the documentation of ongoing disease activity in the descriptors: skin
rash, alopecia, mucosal ulcers and proteinuria, and was validated against the original SLEDAI
[5]. SLEDAI and SLEDAI-2K record descriptors of disease activity as present or absent in the
preceding 30 days [6, 7]. Although SLEDAI-2K has been used to define improvement in disease
activity, it is important to highlight that SLEDAI-2K captures improvement in the descriptors
that resolve completely. Thus the utility of SLEDAI-2K in observational studies and more
importantly in clinical trials is limited, as it doesn’t allow one to discern a signal toward
improvement. The recognition of this limitation of SLEDAI-2K led us to develop SLEDAI-2K
Responder Index-50 (SRI-50) for monitoring improvement in disease activity [11]. In the SRI-
50, each the 24 descriptors has a definition which measures ≥ 50% improvement resulting in an
appropriate scores for the corresponding descriptor and a total score describing disease activity
overall as in SLEDAI-2K [11].
Evidence-based exploratory analysis of the B lymphocyte stimulating factor antagonist,
belimumab, in a phase II SLE trial led to the development of the SLE Responder Index (SRI), a
three part index requiring a reduction in SLEDAI of ≥4, no worsening in the BILAG score and
no deterioration in physician global assessment [52]. SRI is used to define a clinically
meaningful improvement in disease activity in response to treatment. SRI has been successfully
used to identify responders in recent trials [53]. The phase III study of belimumab in SLE used
SRI as the primary outcome measure and demonstrated a statistically significant difference in
responders in patients on drug compared to placebo [53]. SRI uses SLEDAI to determine global
improvement, and improvement in SLEDAI descriptors is captured when a manifestation has
completely resolved. Thus SRI and SLEDAI share the same disadvantages by missing a signal

107
toward improvement. In the current adopted outcomes for the assessment of disease activity in
rheumatoid arthritis and psoriatic arthritis, an improvement is based on the decrease in the
severity of the manifestations and this is reflected by the decrease in the joints count and not
necessarily a complete resolution of arthritis. This should also be applied to lupus patients and
lupologists need to be able to measure a clinically meaningful improvement in each of the
manifestations in a standardized way. SRI-50 was developed and validated based on this
principle and thus might improve and facilitate the identification of responders in longitudinal
research studies and clinical trials.
In this study we aimed to: 1) identify responders using SLEDAI-2K, SLEDAI-2K Responder
Index-50 (SRI-50) and SLE Responder Index (SRI) and 2) determine if patients who are defined
as SRI-50 responders are true responders.
8.2 Methods
8.2.1 Patients’ enrollment and selection
Patients met the American College of Rheumatology classification criteria for SLE [98]. All
patients who attended the Lupus Clinic from September 2009 to April 2011 and had active
disease at baseline visit (SLEDAI-2K ≥6) were enrolled in this prospective study. Patients were
assessed initially at the baseline visit and then reassessed, after treatment was initiated or
adjusted, in 1-3 months over 12 months. At each visit a complete history, including
demographics, physical exam and laboratory tests, were performed. Only 6 and 12 month visits
were analyzed in this study.

108
8.2.2 Outcome measures
8.2.2.1 SLEDAI-2K
SLEDAI-2K is based on the presence of 24 descriptors in 9 organ systems over the preceding 30
days. Descriptors of SLEDAI-2K are documented as present or absent. Each of the descriptors
has a weighted score and the total score of SLEDAI-2K is the sum of all 24 descriptors’ scores.
The total SLEDAI-2K score falls between 0 and 105, with higher scores representing higher
disease activity [4-7].
8.2.2.2 SRI-50 (SLEDAI-2K Responder Index-50)
The SRI-50 comprises the same 24 descriptors, covering 9 organ-systems, generates a total score
and reflects disease activity over the previous 30 days as does SLEDAI-2K [11]. Disease activity
in each of the 9 organ system can be derived if required [11]. The SRI-50 data retrieval form is
used in this study to standardize the documentation of the descriptors of SLEDAI-2K and SRI-50
and determine their scores [11]. Each of the SRI-50 descriptors has a definition to identify ≥ 50%
improvement and generates score for the corresponding descriptor. The SRI-50 score is
evaluated at follow up visits and corresponds to the sum of each of the 24 descriptors’ scores
found on the SRI-50 data retrieval form. One of three situations can occur when a descriptor is
present at the initial visit: 1) the descriptor has achieved complete remission at follow up, in
which case the score would be “0”; 2) the descriptor has not achieved a minimum of 50%
improvement at follow up in which case the score would be identical to its corresponding
SLEDAI-2K value; or 3) the descriptor has improved by 50% (according to the SRI-50
definition) but has not achieved complete remission in which case the score is evaluated as ½ of
the score that would be assigned for SLEDAI-2K. If a descriptor was not present at the initial
visit, the value for SRI-50 at the follow up visit will be the same as that for SLEDAI-2K. This
process is repeated for each of the 24 descriptors [11].

109
8.2.2.3 BILAG
The BILAG index is based on the principle of a physician’s intention to treat and consists of 86
items (based on patient’s history, some on examination findings, and others on laboratory
results) and includes eight systems [12, 13]. Each the BILAG’s index items are rated using a
scale from 0-4 (0=not present, 1=improving, 2=same, 3=worse and 4=new), and some items are
scored as present or absent, reflecting disease activity over the past 4 weeks as compared to the
previous assessment. The BILAG categorizes disease activity as follow: A= severe disease
activity, B = moderate disease activity, C = mild disease activity, D = inactive but previously
affected, and E = inactive with no previous involvement [13]. BILAG scores in this study were
generated with BLIPS (British Lupus Integrated Prospective System) [56].
8.2.2.4 Physician Global Assessment
Physician Global Assessment (PGA) was determined on a visual analog scale (VAS) line of 100
mm, with anchors of 0 “no disease activity” and 100 for “very active disease”. Any increase on
PGA from baseline was considered clinically significant worsening. Patient with worsening on
PGA from baseline were defined as non-responder in the SLE Responder Index.
8.2.2.5 SLE Responder Index
SRI is a composite outcome that incorporates a modification of SLEDAI, the Safety of Estrogens
in Lupus Erythematosus: National Assessment trial (SELENA-SLEDAI), the British Isles Lupus
Assessment Group (BILAG) activity index, and the Physician’s Global Assessment (PGA) [4,
10, 12, 49, 52]. SLE Responder Index is defined as: 1) ≥4 point reduction in SELENA-SLEDAI
score, 2) no new BILAG A or no more than 1 new BILAG B domain score and 3) no
deterioration from baseline in the PGA by ≥0.3 points (>10% on the 3-point visual analogue
scale) [52]. In our study we used SLEDAI-2K and not SELENA-SLEDAI and no deterioration in
PGA at all was allowed.

110
8.2.3 Patient assessment
8.2.3.1 Baseline visit
Patients were assessed at baseline visit with SLEDAI-2K, British Isles Lupus Assessment Group
(BILAG) and Physician Global Assessment (PGA). SRI-50 data retrieval form was completed at
all visits.
8.2.3.2 Follow up visits at 6 and 12 months
The BILAG index and PGA were determined on follow up visits in 1-3 months over 12 months.
We used the SRI-50 data retrieval form to determine SLEDAI-2K and SRI-50 scores on follow-
up visits. The change in scores of SLEDAI-2K and SRI-50 were defined as follows:
1) Change in SLEDAI-2K= SLEDAI-2K Baseline – SLEDAI-2K Follow-up and
2) Change in SRI-50= SRI-50 Baseline – SRI-50 Follow-up.
8.2.4 Treatment
Patients were treated with standard of care as determined by the treating rheumatologist.
8.2.5 Endpoints
8.2.5.1 Aim 1: Responders at 6 months and 12 months as compared to
baseline visit
We identified "SLEDAI-2K responders", "SRI-50 responders" and "SLE Responder Index
responders" at 6 and 12 months as compared to baseline visit. Responders at 6 and 12 months
were patients who improved over their baseline value. Patients who decreased their SLEDAI-2K
and SRI-50 scores by ≥ 4 on follow-up visits as compared to baseline visit were defined as
"SLEDAI-2K responders" and "SRI-50 responders", respectively [38]. Patients who met the 3
components of SRI were defined as "SRI responders"; otherwise, the patient was considered
non-responder [52].

111
8.2.5.2 Aim 2: Determine if SRI-50 responders are true responders and
not false responders.
Using the SRI as “Gold Standard”, we analyzed the results of this study by constructing a 2x2
table in which we included: true positives (SRI responders and SRI-50 responders), false
positives (SRI non-responders and SRI-50 responders), true negatives (SRI non-responders and
SRI-50 non-responders) and false negative (SRI responders and SRI-50 non responders).
We identified the active descriptors at the baseline visit and analyzed the partial (by SRI-50)
improvement that is not discerned by SLEDAI-2K at 6 and 12 months for each corresponding
descriptor.
8.2.6 Statistical analysis
Descriptive statistics were used to describe the characteristics of the patients and the results of
the analysis (proportions and percentages). We determined the number and percentage of
responders on follow-up visits at 6 and 12 months. The McNemar’s test was used to compare the
number of responders by SLEDAI-2K and by SRI-50 to responders by SRI.
8.3 Results
8.3.1 Patient demographics
One hundred and three patients had baseline SLEDAI-2K ≥6 and were included in this study.
One hundred and two patients had a follow-up visit at 6 and 71 patients at 12 months and were
studied further. The patients included 90 (87%) female and 13 (13%) males. Fifty two percent of
the patients were Caucasian, 23% Black, 7% Asian 2% Native North American, 4% were
Filipino, 1% were mixed and the remaining 11% were only classified as ‘Other’. The mean ± SD
age of patients at baseline visit was 39.5 ± 13.0 years and disease duration at baseline was 11.8 ±
9.7 years. Seventy-nine (77%) of the patients were on prednisone at baseline visit. Similarly, 79

112
(77%) patients were maintained on anti-malarial while 64 (62%) patients were on
immunosuppressants (Table 25).
Table 25. Patients' characteristics
Variables n (%) or mean ± SD
Sex Female
90 (87%)
Age at diagnosis (years) 27.6 ± 11.2
Age at 1st visit in the study (years) 39.5 ± 13.0
Disease Duration at 1st visit in the study (years) 11.8 ± 9.7
Race
Caucasian
Black
Asian
Others
54 (52%)
24 (23%)
7 (7%)
18 (18%)
SDI at 1st visit in the study 1.2 ± 1.6
Prednisone at baseline visit: patients number (%) 79 (77%)
Anti-malarial number: patients number (%) 79 (77%)
Immunosuppressants: patients number (%) 64 (62%)

113
8.3.2 Disease activity results
8.3.2.1 SLEDAI-2K and SRI-50 results
Among the active clinical and laboratory descriptors of SLEDAI-2K present at baseline visit,
some descriptors improved completely at follow-up visits (6 and 12 months) as determined by
SLEDAI-2K, some descriptors improved partially as determined by SRI-50 and some descriptors
did not meet the definitions of improvement by either SLEDAI-2K or SRI-50. SRI-50 identified
partial improvement in the active clinical descriptors (vasculitis, arthritis, rash, alopecia, mucosal
ulcers and pleurisy) and almost all of the laboratory descriptors (Table 26).

114
Table 26. Active SLEDAI-2K descriptors at baseline and follow-up visits at 6 and 12
months
Active descriptors Baseline
visit
n
6 months 12 months
n
Completely
recovered by
SLEDAI-2K
Partially
recovered by
SRI-50
N
Completely
recovered by
SLEDAI-2K
Partially
recovered by
SRI-50
Seizure 1 1 1 1 0
Psychosis 0 0
Organic brain 0 0
Visual disturbance 1 1 1 1 0
Cranial nerve disorder 2 2 2 2 2 1 2
Headache 2 2 2 2 2 1 2
CVA 1 1 1 1 0
Vasculitis 5 5 2 5 5 2 2
Arthritis 36 35 24 29 29 19 23
Myositis 1 1 1 1 0
Urinary casts 23 23 16 17 16 12 13
Hematuria 23 23 10 12 17 5 8
Proteinuria 39 39 8 17 27 6 11
Pyuria 33 33 11 16 21 11 13
Rash 21 21 12 16 14 9 11
Alopecia 18 18 7 9 16 10 11
Mucosal ulcers 12 12 9 10 11 9 10
Pleurisy 2 2 1 2 2 2 2
Pericarditis 2 2 2 2 2 2 2
Low complement 60 59 12 27 45 11 22
Increased anti-DNA 65 64 6 17 47 9 15
Fever 2 2 2 2 2 2 2
Thrombocytopenia 2 2 0 1 2
Leucopenia 9 9 5 5 8 6 7
n number of patients with active corresponding descriptor

115
The mean ± SD SLEDAI-2K scores were 10.5 ± 5.0 at baseline visit and 7.9 ± 4.9 and 7.3 ± 5.1
at 6 months and 12 months respectively. The mean SRI-50 scores were lower than SLEDAI-2K
with values of 6.9 ± 4.6 at 6 months and 6.5 ± 4.9 at 12 months. P values comparing mean
SLEDAI-2K and mean SRI-50 at 6 months and mean SLEDAI-2K and mean SRI-50 at 12
months were both < 0.001 (Table 27)
Table 27. Disease activity in 103 patients at baseline visits and SLEDAI-2K, SRI-50 and
SLE Responder Index (SRI) responders
SLEDAI-2K * SRI-50 * SLEDAI-2K
responders
n (%)
SRI
responders
n (%)
p values
between
SLEDAI-
2K/SRI
responders
SRI-50
responders
n (%)
p values
between
SRI/SRI-
50
responders
Baseline
n=103
10.5±5.0 10.5±5.0
6 months
n=102
7.9±4.9 6.9±4.6 45 (44%) 44 (43%) 0.32 52 (51%) 0.005
12 months
n=71
7.3±5.1 6.5±4.9 36 (51%) 36 (51%) 1 41 (58%) 0.03
p values between mean SLEDAI-2K and mean SRI-50 at 6 months and mean SLEDAI-2K and mean SRI-50 at 12
months were both < 0.001.
* Mean ± SD

116
8.3.2.2 Responders at 6 and 12 months as compared to baseline visit
The number of SLEDAI-2K responders was almost equal to the SRI responders at 6 months with
45 (44%) and 44 (43%) patients, respectively (p=0.32). The number of SLEDAI-2K responders
and SRI responders as compared to baseline visit was equal at 12 months with 36 (51%) patients.
More importantly, the number of SRI-50 responders was statistically greater as compared to
SLEDAI-2K responders and SRI responders at 6 and 12 months with 52 (51%) and 41 (58%),
respectively (p=0.005 at 6 months and p=0.03 at 12 months (Table 27 and Figure 4).

117
Figure 4. SLEDAI-2K “responders”, SLE Responder Index “responders” and SLEDAI-2K
Responder Index-50 “responders” at 6 and 12 months
44% 43%
51%51% 51%
58%
S L E D A I - 2 K r e s p o n d e r s
S L E R e sp o n d e r I n d e x ( S R I ) r e s p o n d e r s
S L E D A I - 2 K R e sp o n d e r I n d e x -5 0 ( S R I - 5 0 ) r e s p o n d e r s
Responders at 6 and 12 months6 months
12 months
P=0.32
P=1
P=0.005
P=0.03
8.3.2.3 Comparison between SRI responders “Gold Standard” and SRI-
50 responders at 6 and 12 months
Among the 102 patients evaluated at 6 months, 8 patients were defined as SRI-50
responders/SRI non-responders (false positive). At 12 months, among the 71 patients analyzed, 5
patients were defined as SRI-50 responders/SRI non-responders. In this group of patients, SRI-
50 responders/SRI non-responders, a clinically important partial improvement in the active
clinical or laboratory descriptors was identified (Table 28).

118
Table 28. Comparison between SRI responders (Gold Standard) and SRI-50
6 months
n (%)
SRI-50
responders
SRI-50 non
responders
12 months
n (%)
SRI-50
responders
SRI-50 non
responders
SRI
responders
True +
44 (43%)
False -
0 SRI
responders
True +
36 (51%)
False -
0
SRI non
responders
False +
8 (8%)
True –
50 (49%) SRI non
responders
False +
5 (7%)
True –
30 (42%)
This partial improvement was documented in the following clinical and laboratory descriptors:
lupus headache, vasculitis, arthritis, proteinuria, complements, DNA antibodies and
thrombocytopenia (data not shown).
8.4 Discussion
The novel SLEDAI-2K Responder Index-50 is a valid and reliable index, developed to reflect
partial important improvement, ≥50%, in disease activity between visits [11]. In our initial study,
we have shown that SRI-50 is superior to SLEDAI-2K in identifying “responders” after
treatment with standard of care treatment for a period of 3 months [11]. More importantly, the
measured partial improvement by SRI-50 was shown to be clinically important as confirmed by
the physician global assessment [11].
This is the first study that prospectively validates SLEDAI-2K Responder Index-50 as a measure
of clinically important improvement in lupus patients over 12 months which is considered the
usual time frame in clinical trials. In this study, we included 103 patients with active disease at
baseline (SLEDAI-2K of 10.5 ± 5.0) and we analyzed their results at 6 and 12 months of follow
up as compared to baseline visit. The percentage of SRI-50 responders was greater than those
identified by SLEDAI-2K, 51% as compared to 44% at 6 months, and 58% as compared to 51%

119
at 12 months. The use of SRI-50 has allowed us to identify patients with a clinically important
partial improvement not discerned with the use of SLEDAI-2K.
This study confirmed that SRI-50 is able to identify more responders compared to SRI. SLE
Responder Index is a composite outcome that incorporates a SLEDAI variant, SELENA-
SLEDAI, to determine global improvement in disease activity [5, 10]. The advantage of using
SLEDAI-2K Responder Index-50 instead of SLEDAI-2K as a component of SLE Responder
Index was demonstrated in a previous study by increasing the percentage of SRI responders from
29% to 35% over a 3 month period [51]. In the current study, we evaluated the performance of
SLEDAI-2K Responder Index-50 and SLE Responder Index in identifying responders. We found
that the percentage of SRI-50 responders was greater than SRI responders; 51% as compared to
43% at 6 months, and 58% as compared to 51% 12 months. More importantly, we showed that
the SRI-50 responders are true responders and not falsely positive responders when using the
SRI as “Gold Standard”. These findings justify considering the use of SRI-50 as an independent
responder index in clinical trials. Recently, SRI-50 has been adopted as the primary outcome
measure in a few clinical trials evaluating the effectiveness of new potential drugs in lupus. It is
likely that the percent of responders in trials that adopted the SLE Responder Index as a primary
outcome would have been higher had SLEDAI-2K Responder Index-50 been used instead of
SLEDAI-2K as a component of SRI to determine improvement in disease activity overall or had
SLEDAI-2K Responder Index-50 been used as an independent responder index rather than SLE
Responder Index to identify responders [52, 53].
In observational studies, the decrease in the dose of prednisone is usually based on the
physician’s judgment driven by the improvement of disease activity. In this study, the percentage
of SRI-50 responders in the group of patients who had their prednisone dose decreased within
the first 3 months was superior to the group of patients whose dose of prednisone was the same
over 12 months (data not shown). This is a very important finding especially because it shows
that SRI-50 is sensitive to the change in prednisone dose in patients who improved.

120
Although the SLE Responder Index utilizes SELENA-SLEDAI, in our research center we used
and we continue to use the SLEDAI-2K and not the SELENA-SLEDAI [10, 52]. We have also
used SLEDAI-2K to assess the patients in the current study. Thus the first component of the SLE
Responder Index was determined using SLEDAI-2K. Moreover, in the SLE Responder Index,
the PGA is used to ensure that improvement in disease activity is not achieved at the expense of
the patient’s overall condition [52]. The SLE Responder Index required for response "no more
than 0.3 units increase in the PGA using the point scoring on the SELENA-SLEDAI PGA". In
our study no worsening was allowed in the PGA using the visual analogue scale of 100 mm. The
modification of PGA and use of SLEDAI-2K instead of SELENA-SLEDAI in the SLE
Responder Index component would be unlikely to change the outcome of our study. More
importantly, in our study we did not encounter scenarios in which SLEDAI-2K and BILAG
improved while PGA worsened (data not presented). Nevertheless, it does require clarification
that the adopted design in our study is not identical to the original PGA and SELENA-SLEDAI
components of the SLE Responder Index and should be referred to as a “modified SLE
Responder Index”.
In conclusion, the results of this study showed that SLEDAI-2K Responder Index-50 enhances
the identification of true responders with clinically important improvement in response to
standard care over 12 month period. SLEDAI-2K Responder Index-50 identified more
responders than SLE Responder Index with 8% and 7% additional responders at 6 and 12
months, respectively that could not be discerned with the use of SLE Responder Index. This
validation of the SRI-50 suggests that it may be used as an outcome measure in clinical trials to
identify responders.
This study has been accepted and is in press:
Touma Z, Urowitz MB, Taghavi-Zadeh S, Ibañez D, Gladman DD. Systemic Lupus
Erythematosus Disease Activity Index 2000 (SLEDAI-2K) Responder Index (SRI)-50 identifies
more responders than Systemic Lupus Erythematosus Responder Index (SRI) at 6 and 12 months
Rheumatology (Oxford) January 2012 (In press) [114].

121
9
Chapter 9. Conclusions and Future Directions

122
9.1 Achieved aims
9.1.1 Validation of SLEDAI-2K 30 days
Before embarking on the development of the new SLEDAI-2K Responder Index-50 (SRI-50) it
was necessary to determine whether the SLEDAI-2K score over the month would be similar to
that scored only in the previous 10 days as recommended in the original instrument. The
validation of SLEDAI-2K 30 days against SLEDAI-2K 10 days was accomplished in 2 studies
one using a cross-sectional design and another a longitudinal design over a 12 month period.
These two studies confirmed that it is unusual for patients to display features of disease activity
at -11-30 days prior to a visit and have those features totally resolve in the 10 days prior to a
visit. Therefore, a preceding 30 day window for SLEDAI-2K should now be used in clinical
studies and clinical trials to describe disease activity in SLE [6, 7].
9.1.2 Derivation and validation of SRI-50: Responder index to SLEDAI-
2K
SLEDAI and its versions record descriptors of disease activity as present or absent [4-8, 73]. In
order to demonstrate improvement a manifestation has to completely resolve. Thus SLEDAI-2K
utility in observational studies and more importantly in clinical trials is limited, as it doesn’t
allow one to discern a signal toward but still incomplete improvement. The recognition of this
limitation of SLEDAI-2K led us to consider modifications to capture partial improvement in
disease activity. A minimum of 50% improvement was felt by clinicians to reflect a clinically
important improvement and this gave rise to the concept of SRI-50 [11]. In 2009 the SLEDAI-
2K 30 days was used to build the SRI-50 [11]. The SRI-50 comprises the same 24 descriptors of
SLEDAI-2K and covers 9 organ systems. After reviewing the literature, the new definitions of
the SRI-50 were generated to identify 50% improvement in each of the 24 descriptors of
SLEDAI-2K. Content and face validity of the SRI-50 definitions were confirmed according to
the methodology adopted in the development of SRI-50. The SRI-50 definitions were developed
as a 2 page-document. As in SLEDAI-2K 30 days, each descriptor in SRI-50 refers to the
preceding 30 days [6, 7]. The assigned scores for the descriptors of SRI-50 were derived by

123
dividing the score of the corresponding SLEDAI-2K by 2. As in SLEDAI-2K the score of the
SRI-50 can range from 0-105 [11]. The method of scoring of the SRI-50 is simple, cumulative
and intuitive as in the original SLEDAI-2K [5, 11].
The SRI-50 data retrieval form was developed to standardize the recording of the descriptors in
an efficient way to allow the calculation of SRI-50 scores [11]. In the initial validation of SRI-
50, the concurrent construct validity of SRI-50 and the physician response assessment was
evaluated in 141 patients. In the group of patients who experienced clinically partial
improvement as determined by the “Gold Standard”, Likert scale, the decrease in SRI-50 scores
were statistically and clinically more significant than the decrease in SLEDAI-2K scores. A
moderate correlation was found between SRI-50 and the physician response assessment. More
importantly the decrease in SRI-50 scores was clinically more important than the decrease in
SLEDAI-2K scores in patients who improved meeting the definition of improvement by
decreasing by ≥ 4 [2, 11]. This study demonstrated that SRI-50 has construct validity and is able
to demonstrate incomplete but clinically important improvement in disease activity between
visits in lupus patients [11].
9.1.3 Reliability of SRI-50
It was very essential to demonstrate that the newly developed responder index, SRI-50, has
evidence of reliability. For this purpose, I have conducted a multicentre study, where patient
profile scenarios were derived from real adult patients followed at the Toronto Lupus Clinic to
evaluate the reliability of SRI-50. Ten rheumatologists, from university and community
hospitals, and postdoctoral rheumatology fellows participated in this task. This study confirmed
that SRI-50 is reliable to assess ≥50% improvement in lupus disease activity with an average
intrarater and interrater ICC of 0.99 and 1.00 respectively [95]. The use of the SRI-50 data
retrieval form was essential to ensure the optimal performance of SRI-50. Additionally, this
study confirmed that SRI-50 can be used by both rheumatologists and trainees and performs
equally well in trained as well as untrained rheumatologists [95].

124
9.1.4 SRI-50 enhances the ability of other indices to identify responders
Evidence-based exploratory analysis of the B lymphocyte stimulating factor antagonist,
belimumab, in a phase II SLE trial led to the development of the new composite outcome; SLE
Responder Index (SRI). SRI is a three part index requiring a reduction in SLEDAI of ≥4, no
worsening in the BILAG score and no deterioration in physician global assessment [52]. SRI is
used to define a clinically meaningful improvement in disease activity in response to treatment.
SRI has been successfully used to identify responders in recent trials [53]. SRI uses SLEDAI to
determine global improvement, and improvement in SLEDAI descriptors is captured when a
manifestation has completely resolved. Thus SRI and SLEDAI share the same disadvantages by
missing a signal toward improvement. This led us to consider further modification of SRI by
substituting SLEDAI-2K with SRI-50.
As a first effort towards further validation of SRI-50, we assessed its capability to enhance the
ability of SRI in identifying patients with clinically important improvement between visits. For
this purpose, I have conducted a study on patients who attended the Lupus Clinic from
September 2009 to September 2010. SRI was determined at follow-up visit according to its
original definition using SLEDAI-2K score and also by substituting SLEDAI-2K with SRI-50.
Twenty nine percent of patients met the original definition of SRI and 35% patients met the
definition of SRI when SLEDAI-2K was substituted with SRI-50. This study confirmed that the
use of SRI-50 identified significant improvement in 7 additional patients. SRI-50 enhances the
ability of SRI to capture patients with clinically important improvement in disease activity. This
improvement could not be discerned with the use of SLEDAI-2K as a component of SRI [11].
More recently, I have evaluated the performance of SRI-50 as compared to SLEDAI-2K and SRI
in identifying “responders” over a 12 month period, which is the time frame adopted in clinical
trials. Among the103 patients studied, the percentage of responders at 6 and 12 months was 44%
and 51% when determined by SLEDAI-2K and 43% and 51% by SRI respectively. The
percentage of "SRI-50 responders" at 6 and 12 months was 51% and 58%, respectively. SRI-50
identified more responders as compared to SLEDAI-2K and SRI at 6 and 12 months.

125
These 2 studies allowed us to conclude that SRI-50 enhances the ability of SRI to capture
patients with clinically important improvement in disease activity [11]. More importantly, SRI-
50 was superior to SLEDAI-2K and SRI in detecting patients with significant improvement,
between visits. These properties of the SRI-50 enable it to be used as an independent outcome
measure of improvement in clinical trials.
9.1.5 SRI-50 captures 50% improvement in disease activity over 10
years
One of the acceptable modalities in the validation of new measures is to use available data from
an existing database. This approach allows the validating of new measures over a short period of
time. This is a retrospective analysis conducted on data available from patients who attended the
Toronto Lupus Clinic over the last 10 years. Patients with SLEDAI-2K renal, immunological and
hematologic active descriptors were identified. The percentage of descriptors with partial and
complete recovery was studied at subsequent follow-up visits within 1 year and over the study
period. Time to partial and complete recovery was analyzed over the study period. Of the 795
patients 94% had one of the active systems at some point during the study period. 516 patients
had renal, 667 had immunological and 207 had hematologic active systems. 66% of patients
showed partial recovery (≥ 50% by SRI-50) in at least one descriptor over the study period. None
of these partial findings identified would have been captured using SLEDAI-2K alone. As
expected the time to partial recovery was shorter than the time to complete recovery in all
possible clinical situations of improvement in disease activity. This retrospective analysis on data
available over 10 years confirms that SRI-50 is a valid responder index derived form SLEDAI-
2K and very helpful in identifying clinically important improvement in active laboratory
descriptors in an efficient time.
9.2 Relevance
I am aware that several standardized reliable and validated indices assessing the disease activity
in SLE patients have already been developed. Despite the availability of these numerous indices,

126
the valid ones do not adequately describe improvement as a response to new therapies. The
newly developed and validated index, SRI-50, can detect partial and clinically important
improvement in disease activity between visits in response to therapy. The importance of this
novel responder index cannot be underestimated as previous measures of disease activity failed
to perform adequately in clinical trials, hampering the development and testing of novel
treatments for SLE. The use of a more sensitive responder index, SRI-50, should have a major
positive impact on the assessment of disease activity improvement in lupus patients and better
help identify newer agents with therapeutic potential.
9.3 Future Directions
We have learned from previous clinical trials in lupus how important it is to provide
rheumatologists with appropriate training for a specific measure. This has led us to develop a
dedicated website to SRI50, www.sri-50.com, including: SRI-50 training manual, computer-
adaptive training modules and a data-bank for examination cases with a spectrum of disease
complexity with the aim of providing proficiency certificates to those who successfully complete
these cases for clinical trials. We also aim to further evaluate the training and examination
modules, and the overall performance of the website. For this purpose, an ongoing study is
currently being carried out.
Future studies related to SRI-50 validation will focus on grouping and analyzing data that will be
collected from different centres. At this time, we have planned to collaborate with centres from
Australia and Europe, where SRI-50 will be applied in their Lupus Clinics.
Currently, SRI-50 has been incorporated into clinical trials of novel SLE therapeutics. I expect
that future trials will incorporate SRI-50 as a primary outcome measure to identify improvement
in disease activity in lupus patients. The analysis of data from ongoing trials which incorporated
SRI-50 as the primary/secondary outcome measure will allow us to further validate SRI-50.
The published studies on SRI-50 have used the information collected from data available for the
last 2 years. Currently, the SRI-50 data retrieval form has been incorporated in the protocol of
the Toronto Lupus Clinic. In the future we will be able to address more research questions on
SRI-5-50.

127
References 1. Petri, M., J. Buyon, and M. Kim, Classification and definition of major flares in SLE
clinical trials. Lupus, 1999. 8(8): p. 685-91.
2. Nikpour, M., M.B. Urowitz, D. Ibanez, and D.D. Gladman, Frequency and determinants
of flare and persistently active disease in systemic lupus erythematosus. Arthritis Rheum,
2009. 61(9): p. 1152-8.
3. Smolen, J.S., V. Strand, M. Cardiel, S. Edworthy, D. Furst, D. Gladman, C. Gordon, D.A.
Isenberg, J.H. Klippel, M. Petri, L. Simon, P. Tugwell, and F. Wolfe, Randomized
clinical trials and longitudinal observational studies in systemic lupus erythematosus:
consensus on a preliminary core set of outcome domains. J Rheumatol, 1999. 26(2): p.
504-7.
4. Bombardier, C., D.D. Gladman, M.B. Urowitz, D. Caron, and C.H. Chang, Derivation of
the SLEDAI. A disease activity index for lupus patients. The Committee on Prognosis
Studies in SLE. Arthritis Rheum, 1992. 35(6): p. 630-40.
5. Gladman, D.D., D. Ibanez, and M.B. Urowitz, Systemic lupus erythematosus disease
activity index 2000. J Rheumatol, 2002. 29(2): p. 288-91.
6. Touma, Z., M.B. Urowitz, and D.D. Gladman, SLEDAI-2K for a 30-day window. Lupus,
2010. 19(1): p. 49-51.
7. Touma, Z., M.B. Urowitz, D. Ibanez, and D.D. Gladman, SLEDAI-2K 10 days versus
SLEDAI-2K 30 days in a longitudinal evaluation. Lupus, 2011. 20(1): p. 67-70.
8. Guzman, J., M.H. Cardiel, A. Arce-Salinas, J. Sanchez-Guerrero, and D. Alarcon-
Segovia, Measurement of disease activity in systemic lupus erythematosus. Prospective
validation of 3 clinical indices. J Rheumatol, 1992. 19(10): p. 1551-8.
9. Uribe, A.G., L.M. Vila, G. McGwin, Jr., M.L. Sanchez, J.D. Reveille, and G.S. Alarcon,
The Systemic Lupus Activity Measure-revised, the Mexican Systemic Lupus
Erythematosus Disease Activity Index (SLEDAI), and a modified SLEDAI-2K are
adequate instruments to measure disease activity in systemic lupus erythematosus. J
Rheumatol, 2004. 31(10): p. 1934-40.
10. Petri, M., M.Y. Kim, K.C. Kalunian, J. Grossman, B.H. Hahn, L.R. Sammaritano, M.
Lockshin, J.T. Merrill, H.M. Belmont, A.D. Askanase, W.J. McCune, M. Hearth-Holmes,
M.A. Dooley, J. Von Feldt, A. Friedman, M. Tan, J. Davis, M. Cronin, B. Diamond, M.
Mackay, L. Sigler, M. Fillius, A. Rupel, F. Licciardi, and J.P. Buyon, Combined oral

128
contraceptives in women with systemic lupus erythematosus. The New England journal of
medicine, 2005. 353(24): p. 2550-8.
11. Touma, Z., D.D. Gladman, D. Ibanez, and M.B. Urowitz, Development and initial
validation of the systemic lupus erythematosus disease activity index 2000 responder
index 50. J Rheumatol, 2011. 38(2): p. 275-84.
12. Hay, E.M., P.A. Bacon, C. Gordon, D.A. Isenberg, P. Maddison, M.L. Snaith, D.P.
Symmons, N. Viner, and A. Zoma, The BILAG index: a reliable and valid instrument for
measuring clinical disease activity in systemic lupus erythematosus. The Quarterly
journal of medicine, 1993. 86(7): p. 447-58.
13. Symmons, D.P., J.S. Coppock, P.A. Bacon, B. Bresnihan, D.A. Isenberg, P. Maddison,
N. McHugh, M.L. Snaith, and A.S. Zoma, Development and assessment of a
computerized index of clinical disease activity in systemic lupus erythematosus. Members
of the British Isles Lupus Assessment Group (BILAG). The Quarterly journal of medicine,
1988. 69(259): p. 927-37.
14. Isenberg, D.A., A. Rahman, E. Allen, V. Farewell, M. Akil, I.N. Bruce, D. D'Cruz, B.
Griffiths, M. Khamashta, P. Maddison, N. McHugh, M. Snaith, L.S. Teh, C.S. Yee, A.
Zoma, and C. Gordon, BILAG 2004. Development and initial validation of an updated
version of the British Isles Lupus Assessment Group's disease activity index for patients
with systemic lupus erythematosus. Rheumatology, 2005. 44(7): p. 902-6.
15. Liang, M.H., S.A. Socher, M.G. Larson, and P.H. Schur, Reliability and validity of six
systems for the clinical assessment of disease activity in systemic lupus erythematosus.
Arthritis Rheum, 1989. 32(9): p. 1107-18.
16. Bae, S.C., H.K. Koh, D.K. Chang, M.H. Kim, J.K. Park, and S.Y. Kim, Reliability and
validity of systemic lupus activity measure-revised (SLAM-R) for measuring clinical
disease activity in systemic lupus erythematosus. Lupus, 2001. 10(6): p. 405-9.
17. Karlson, E.W., L.H. Daltroy, C. Rivest, R. Ramsey-Goldman, E.A. Wright, A.J.
Partridge, M.H. Liang, and P.R. Fortin, Validation of a Systemic Lupus Activity
Questionnaire (SLAQ) for population studies. Lupus, 2003. 12(4): p. 280-6.
18. Bencivelli, W., C. Vitali, D.A. Isenberg, J.S. Smolen, M.L. Snaith, M. Sciuto, and S.
Bombardieri, Disease activity in systemic lupus erythematosus: report of the Consensus
Study Group of the European Workshop for Rheumatology Research. III. Development of
a computerised clinical chart and its application to the comparison of different indices of

129
disease activity. The European Consensus Study Group for Disease Activity in SLE. Clin
Exp Rheumatol, 1992. 10(5): p. 549-54.
19. Vitali, C., W. Bencivelli, D.A. Isenberg, J.S. Smolen, M.L. Snaith, M. Sciuto, A.
d'Ascanio, and S. Bombardieri, Disease activity in systemic lupus erythematosus: report
of the Consensus Study Group of the European Workshop for Rheumatology Research. I.
A descriptive analysis of 704 European lupus patients. European Consensus Study Group
for Disease Activity in SLE. Clin Exp Rheumatol, 1992. 10(5): p. 527-39.
20. Vitali, C., W. Bencivelli, D.A. Isenberg, J.S. Smolen, M.L. Snaith, M. Sciuto, R. Neri,
and S. Bombardieri, Disease activity in systemic lupus erythematosus: report of the
Consensus Study Group of the European Workshop for Rheumatology Research. II.
Identification of the variables indicative of disease activity and their use in the
development of an activity score. The European Consensus Study Group for Disease
Activity in SLE. Clin Exp Rheumatol, 1992. 10(5): p. 541-7.
21. Petri, M., D. Hellmann, and M. Hochberg, Validity and reliability of lupus activity
measures in the routine clinic setting. J Rheumatol, 1992. 19(1): p. 53-9.
22. Smolen, J.S., Clinical and serological features, in Systemic Lupus Erythematosus:
clinical and experimental aspects, J.S. Smolen, Zielinski, C.C., Editor 1987, Spring-
Verlag. p. 170-196.
23. Petri, M., S.G. Barr, J. Buyon, J. Davis, E. Ginzler, K. Kalunian, and J.T. Merill, RIFLE:
Responder Index for Lupus Erythematosus. Arthritis Rheum, 2000. 43:S244.
24. Gladman, D., E. Ginzler, C. Goldsmith, P. Fortin, M. Liang, M. Urowitz, P. Bacon, S.
Bombardieri, J. Hanly, E. Hay, D. Isenberg, J. Jones, K. Kalunian, P. Maddison, O.
Nived, M. Petri, M. Richter, J. Sanchez-Guerrero, M. Snaith, G. Sturfelt, D. Symmons,
and A. Zoma, The development and initial validation of the Systemic Lupus International
Collaborating Clinics/American College of Rheumatology damage index for systemic
lupus erythematosus. Arthritis Rheum, 1996. 39(3): p. 363-9.
25. Costenbader, K.H., M. Khamashta, S. Ruiz-Garcia, M.T. Perez-Rodriguez, M. Petri, J.
Elliott, S. Manzi, E.W. Karlson, T. Turner-Stokes, B. Bermas, J. Coblyn, E. Massarotti,
P. Schur, P. Fraser, I. Navarro, J.G. Hanly, T.S. Shaver, R.S. Katz, E. Chakravarty, P.R.
Fortin, M.L. Sanchez, J. Liu, K. Michaud, G.S. Alarcon, and F. Wolfe, Development and
initial validation of a self-assessed lupus organ damage instrument. Arthritis Care Res
(Hoboken), 2010. 62(4): p. 559-68.

130
26. Pons-Estel, B.A., J. Sanchez-Guerrero, J. Romero-Diaz, A. Iglesias-Gamarra, E. Bonfa,
E.F. Borba, S.K. Shinjo, S. Bernatsky, A. Clarke, M.A. Garcia, J.C. Marcos, A. Duarte,
G.A. Berbotto, H. Scherbarth, C.D. Marques, L. Onetti, V. Saurit, A.W. Souza, E.
Velozo, L.J. Catoggio, O. Neira, P.I. Burgos, L.A. Ramirez, J.F. Molina, I.G. De La
Torre, R. Silvarino, J.A. Manni, S. Duran-Barragan, L.M. Vila, P.R. Fortin, J. Calvo-
Alen, M.J. Santos, M. Portela, M.H. Esteva-Spinetti, M. Weisman, E.M. Acevedo, M.I.
Segami, S.B. Gentiletti, J. Roldan, I. Navarro, E. Gonzalez, J.M. Liu, E.W. Karlson, K.H.
Costenbader, F. Wolfe, and G.S. Alarcon, Validation of the Spanish, Portuguese and
French versions of the Lupus Damage Index questionnaire: data from North and South
America, Spain and Portugal. Lupus, 2009. 18(12): p. 1033-52.
27. McHorney, C.A., J.E. Ware, Jr., J.F. Lu, and C.D. Sherbourne, The MOS 36-item Short-
Form Health Survey (SF-36): III. Tests of data quality, scaling assumptions, and
reliability across diverse patient groups. Med Care, 1994. 32(1): p. 40-66.
28. McElhone, K., J. Abbott, J. Shelmerdine, I.N. Bruce, Y. Ahmad, C. Gordon, K. Peers, D.
Isenberg, A. Ferenkeh-Koroma, B. Griffiths, M. Akil, P. Maddison, and L.S. Teh,
Development and validation of a disease-specific health-related quality of life measure,
the LupusQol, for adults with systemic lupus erythematosus. Arthritis Rheum, 2007.
57(6): p. 972-9.
29. Jolly, M., A.S. Pickard, C. Wilke, R.A. Mikolaitis, L.S. Teh, K. McElhone, L. Fogg, and
J. Block, Lupus-specific health outcome measure for US patients: the LupusQoL-US
version. Ann Rheum Dis, 2010. 69(1): p. 29-33.
30. Gonzalez-Rodriguez, V., M.I. Peralta-Ramirez, N. Navarrete-Navarrete, J.L. Callejas-
Rubio, A.M. Santos Ruiz, and M. Khamashta, [Adaptation and validation of the Spanish
version of a disease-specific quality of life measure in patients with systemic lupus
erythematosus: the Lupus quality of life]. Med Clin (Barc), 2010. 134(1): p. 13-6.
31. Grootscholten, C., G. Ligtenberg, R.H. Derksen, K.M. Schreurs, J.W. de Glas-Vos, E.C.
Hagen, A.W. van den Wall Bake, T.W. Huizinga, F.H. van den Hoogen, M. Bijl, J.C. van
Houwelingen, F.J. Snoek, and J.H. Berden, Health-related quality of life in patients with
systemic lupus erythematosus: development and validation of a lupus specific symptom
checklist. Qual Life Res, 2003. 12(6): p. 635-44.
32. Leong, K.P., K.O. Kong, B.Y. Thong, E.T. Koh, T.Y. Lian, C.L. Teh, Y.K. Cheng, H.H.
Chng, H. Badsha, W.G. Law, T.C. Lau, L.C. Chew, H.J. Ho, L.Y. Pong, L.S. Hoi, N.

131
Sangeetha, S.P. Chan, and H.S. Howe, Development and preliminary validation of a
systemic lupus erythematosus-specific quality-of-life instrument (SLEQOL).
Rheumatology (Oxford), 2005. 44(10): p. 1267-76.
33. Doward, L.C., S.P. McKenna, D. Whalley, A. Tennant, B. Griffiths, P. Emery, and D.J.
Veale, The development of the L-QoL: a quality-of-life instrument specific to systemic
lupus erythematosus. Ann Rheum Dis, 2009. 68(2): p. 196-200.
34. Boers, M., P. Brooks, C.V. Strand, and P. Tugwell, The OMERACT filter for Outcome
Measures in Rheumatology. J Rheumatol, 1998. 25(2): p. 198-9.
35. Gladman, D.D., C.H. Goldsmith, M.B. Urowitz, P. Bacon, C. Bombardier, D. Isenberg,
K. Kalunian, M.H. Liang, P. Maddison, O. Nived, and et al., Crosscultural validation and
reliability of 3 disease activity indices in systemic lupus erythematosus. J Rheumatol,
1992. 19(4): p. 608-11.
36. Hawker, G., S. Gabriel, C. Bombardier, C. Goldsmith, D. Caron, and D. Gladman, A
reliability study of SLEDAI: a disease activity index for systemic lupus erythematosus. J
Rheumatol, 1993. 20(4): p. 657-60.
37. McLaughlin, J.R., C. Bombardier, V.T. Farewell, D.D. Gladman, and M.B. Urowitz,
Kidney biopsy in systemic lupus erythematosus. III. Survival analysis controlling for
clinical and laboratory variables. Arthritis Rheum, 1994. 37(4): p. 559-67.
38. Gladman, D.D., M.B. Urowitz, A. Kagal, and D. Hallett, Accurately describing changes
in disease activity in Systemic Lupus Erythematosus. J Rheumatol, 2000. 27(2): p. 377-9.
39. Gladman, D.D., C.H. Goldsmith, M.B. Urowitz, P. Bacon, C. Bombardier, D. Isenberg,
K. Kalunian, M.H. Liang, P. Maddison, O. Nived, and et al., Sensitivity to change of 3
Systemic Lupus Erythematosus Disease Activity Indices: international validation. J
Rheumatol, 1994. 21(8): p. 1468-71.
40. Brunner, H.I., B.M. Feldman, C. Bombardier, and E.D. Silverman, Sensitivity of the
Systemic Lupus Erythematosus Disease Activity Index, British Isles Lupus Assessment
Group Index, and Systemic Lupus Activity Measure in the evaluation of clinical change in
childhood-onset systemic lupus erythematosus. Arthritis Rheum, 1999. 42(7): p. 1354-60.
41. Brunner, H.I., G.C. Higgins, K. Wiers, S.K. Lapidus, J.C. Olson, K. Onel, M. Punaro, J.
Ying, M.S. Klein-Gitelman, and E.H. Giannini, Prospective validation of the provisional
criteria for the evaluation of response to therapy in childhood-onset systemic lupus
erythematosus. Arthritis Care Res (Hoboken), 2010. 62(3): p. 335-44.

132
42. Zonana-Nacach, A., P. Yanez, F.J. Jimenez-Balderas, and A. Camargo-Coronel, Disease
activity, damage and survival in Mexican patients with acute severe systemic lupus
erythematosus. Lupus, 2007. 16(12): p. 997-1000.
43. Becker-Merok, A. and H.C. Nossent, Damage accumulation in systemic lupus
erythematosus and its relation to disease activity and mortality. J Rheumatol, 2006.
33(8): p. 1570-7.
44. Cook, R.J., D.D. Gladman, D. Pericak, and M.B. Urowitz, Prediction of short term
mortality in systemic lupus erythematosus with time dependent measures of disease
activity. J Rheumatol, 2000. 27(8): p. 1892-5.
45. Ward, M.M., A.S. Marx, and N.N. Barry, Comparison of the validity and sensitivity to
change of 5 activity indices in systemic lupus erythematosus. J Rheumatol, 2000. 27(3):
p. 664-70.
46. Mosca, M., W. Bencivelli, C. Vitali, P. Carrai, R. Neri, and S. Bombardieri, The validity
of the ECLAM index for the retrospective evaluation of disease activity in systemic lupus
erythematosus. Lupus, 2000. 9(6): p. 445-50.
47. Aringer, M., W.B. Graninger, G. Steiner, and J.S. Smolen, Safety and efficacy of tumor
necrosis factor alpha blockade in systemic lupus erythematosus: an open-label study.
Arthritis Rheum, 2004. 50(10): p. 3161-9.
48. Vitali, C., W. Bencivelli, M. Mosca, P. Carrai, M. Sereni, and S. Bombardieri,
Development of a clinical chart to compute different disease activity indices for systemic
lupus erythematosus. J Rheumatol, 1999. 26(2): p. 498-501.
49. Stoll, T., G. Stucki, J. Malik, S. Pyke, and D.A. Isenberg, Further validation of the
BILAG disease activity index in patients with systemic lupus erythematosus. Ann Rheum
Dis, 1996. 55(10): p. 756-60.
50. Gordon, C., N. Sutcliffe, J. Skan, T. Stoll, and D.A. Isenberg, Definition and treatment of
lupus flares measured by the BILAG index. Rheumatology, 2003. 42(11): p. 1372-9.
51. Touma, Z., D.D. Gladman, D. Ibanez, S. Taghavi-Zadeh, and M.B. Urowitz, Systemic
Lupus Erythematosus Disease Activity Index 2000 Responder Index-50 enhances the
ability of SLE Responder Index to identify responders in clinical trials. J Rheumatol,
2011. 38(11): p. 2395-9.
52. Furie, R.A., M.A. Petri, D.J. Wallace, E.M. Ginzler, J.T. Merrill, W. Stohl, W.W.
Chatham, V. Strand, A. Weinstein, M.R. Chevrier, Z.J. Zhong, and W.W. Freimuth,

133
Novel evidence-based systemic lupus erythematosus responder index. Arthritis Rheum,
2009. 61(9): p. 1143-51.
53. Navarra, S.V., R.M. Guzman, A.E. Gallacher, S. Hall, R.A. Levy, R.E. Jimenez, E.K. Li,
M. Thomas, H.Y. Kim, M.G. Leon, C. Tanasescu, E. Nasonov, J.L. Lan, L. Pineda, Z.J.
Zhong, W. Freimuth, and M.A. Petri, Efficacy and safety of belimumab in patients with
active systemic lupus erythematosus: a randomised, placebo-controlled, phase 3 trial.
Lancet, 2011. 377(9767): p. 721-31.
54. Yee, C.S., L. Cresswell, V. Farewell, A. Rahman, L.S. Teh, B. Griffiths, I.N. Bruce, Y.
Ahmad, A. Prabu, M. Akil, N. McHugh, D. D'Cruz, M.A. Khamashta, D.A. Isenberg, and
C. Gordon, Numerical scoring for the BILAG-2004 index. Rheumatology (Oxford), 2010.
49(9): p. 1665-9.
55. Yee, C.S., L. Cresswell, V. Farewell, A. Rahman, L.S. Teh, B. Griffiths, I.N. Bruce, Y.
Ahmad, A. Prabu, M. Akil, N. McHugh, D. D'Cruz, M.A. Khamashta, D.A. Isenberg, and
C. Gordon, Numerical scoring for the BILAG-2004 index. Rheumatology, 2010. 49(9): p.
1665-9.
56. Isenberg, D.A. and C. Gordon, From BILAG to BLIPS--disease activity assessment in
lupus past, present and future. Lupus, 2000. 9(9): p. 651-4.
57. Yee, C.S., V. Farewell, D.A. Isenberg, A. Prabu, K. Sokoll, L.S. Teh, A. Rahman, I.N.
Bruce, B. Griffiths, M. Akil, N. McHugh, D. D'Cruz, M.A. Khamashta, S. Bowman, P.
Maddison, A. Zoma, E. Allen, and C. Gordon, Revised British Isles Lupus Assessment
Group 2004 index: a reliable tool for assessment of systemic lupus erythematosus
activity. Arthritis Rheum, 2006. 54(10): p. 3300-5.
58. Yee, C.S., V. Farewell, D.A. Isenberg, A. Rahman, L.S. Teh, B. Griffiths, I.N. Bruce, Y.
Ahmad, A. Prabu, M. Akil, N. McHugh, D. D'Cruz, M.A. Khamashta, P. Maddison, and
C. Gordon, British Isles Lupus Assessment Group 2004 index is valid for assessment of
disease activity in systemic lupus erythematosus. Arthritis Rheum, 2007. 56(12): p. 4113-
9.
59. Touma, Z., D.D. Gladman, M.B. Urowitz, J. Beyene, E.M. Uleryk, and P.S. Shah,
Mycophenolate mofetil for induction treatment of lupus nephritis: a systematic review
and metaanalysis. J Rheumatol, 2011. 38(1): p. 69-78.
60. Guidance for Industry. Lupus Nephritis Caused By Systemic Lupus Erythematosus —
Developing Medical Products for Treatment.

134
http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guid
ances/UCM216280.pdf. 2010.
61. Petri, M., N. Kasitanon, S.S. Lee, K. Link, L. Magder, S.C. Bae, J.G. Hanly, D.A.
Isenberg, O. Nived, G. Sturfelt, R. van Vollenhoven, D.J. Wallace, G.S. Alarcon, D. Adu,
C. Avila-Casado, S.R. Bernatsky, I.N. Bruce, A.E. Clarke, G. Contreras, D.M. Fine, D.D.
Gladman, C. Gordon, K.C. Kalunian, M.P. Madaio, B.H. Rovin, J. Sanchez-Guerrero, K.
Steinsson, C. Aranow, J.E. Balow, J.P. Buyon, E.M. Ginzler, M.A. Khamashta, M.B.
Urowitz, M.A. Dooley, J.T. Merrill, R. Ramsey-Goldman, J. Font, J. Tumlin, T. Stoll,
and A. Zoma, Systemic lupus international collaborating clinics renal activity/response
exercise: development of a renal activity score and renal response index. Arthritis
Rheum, 2008. 58(6): p. 1784-8.
62. Albrecht, J., L. Taylor, J.A. Berlin, S. Dulay, G. Ang, S. Fakharzadeh, J. Kantor, E. Kim,
G. Militello, K. McGinnis, S. Richardson, J. Treat, C. Vittorio, A. Van Voorhees, and
V.P. Werth, The CLASI (Cutaneous Lupus Erythematosus Disease Area and Severity
Index): an outcome instrument for cutaneous lupus erythematosus. J Invest Dermatol,
2005. 125(5): p. 889-94.
63. Krathen, M., J. Albrecht, and V.P. Werth, The cutaneous lupus disease activity and
severity index as a validated outcome measure for cutaneous lupus erythematosus:
comment on the article by Stamm et al. Arthritis Rheum, 2008. 59(4): p. 601-2.
64. Kuhn, A., A.M. Meuth, D. Bein, S. Amler, S. Beissert, M. Bohm, R. Brehler, J. Ehrchen,
S. Grundmann, M. Haust, V. Ruland, M. Schiller, P. Schulz, S. Stander, C. Sauerland, W.
Kopcke, T.A. Luger, and G. Bonsmann, Revised Cutaneous Lupus Erythematosus
Disease Area and Severity Index (RCLASI): a modified outcome instrument for cutaneous
lupus erythematosus. Br J Dermatol, 2010. 163(1): p. 83-92.
65. Ibanez, D., M.B. Urowitz, and D.D. Gladman, Summarizing disease features over time: I.
Adjusted mean SLEDAI derivation and application to an index of disease activity in
lupus. J Rheumatol, 2003. 30(9): p. 1977-82.
66. Ibanez, D., D.D. Gladman, and M.B. Urowitz, Adjusted mean Systemic Lupus
Erythematosus Disease Activity Index-2K is a predictor of outcome in SLE. J Rheumatol,
2005. 32(5): p. 824-7.
67. Ibanez, D., D. Gladman, and M. Urowitz, Summarizing disease features over time: II.
Variability measures of SLEDAI-2K. J Rheumatol, 2007. 34(2): p. 336-40.

135
68. Ibanez, D., D.D. Gladman, Z. Touma, M. Nikpour, and M.B. Urowitz, Optimal frequency
of visits for patients with systemic lupus erythematosus to measure disease activity over
time. J Rheumatol, 2011. 38(1): p. 60-3.
69. Buyon, J.P., K.C. Kalunian, R. Ramsey-Goldman, M.A. Petri, M.D. Lockshin, G. Ruiz-
Irastorza, and M. Khamashta, Assessing disease activity in SLE patients during
pregnancy. Lupus, 1999. 8(8): p. 677-84.
70. Yee, C.S., V. Farewell, D.A. Isenberg, B. Griffiths, L.S. Teh, I.N. Bruce, Y. Ahmad, A.
Rahman, A. Prabu, M. Akil, N. McHugh, C. Edwards, D. D'Cruz, M.A. Khamashta, P.
Maddison, and C. Gordon, The BILAG-2004 index is sensitive to change for assessment
of SLE disease activity. Rheumatology (Oxford), 2009. 48(6): p. 691-5.
71. Buyon, J., K.C. kalunian, and M.B. Urowitz, Revision of the SELENA fl are index.
Arthritis Rheum 2009;60:S339.
72. Petri, M., J. Buyon, M. Skovron, M. Kim, and . Reliability of SELENA SLEDAI and flare
as clinical trials outcome measures [abstract]. Arthritis &Rheumatism, 1997. 40 (No 9
Suppl):S218.
73. Petri, M., M.Y. Kim, K.C. Kalunian, J. Grossman, B.H. Hahn, L.R. Sammaritano, M.
Lockshin, J.T. Merrill, H.M. Belmont, A.D. Askanase, W.J. McCune, M. Hearth-Holmes,
M.A. Dooley, J. Von Feldt, A. Friedman, M. Tan, J. Davis, M. Cronin, B. Diamond, M.
Mackay, L. Sigler, M. Fillius, A. Rupel, F. Licciardi, and J.P. Buyon, Combined oral
contraceptives in women with systemic lupus erythematosus. N Engl J Med, 2005.
353(24): p. 2550-8.
74. FitzGerald, J.D. and J.M. Grossman, Validity and reliability of retrospective assessment
of disease activity and flare in observational cohorts of lupus patients. Lupus, 1999. 8(8):
p. 638-44.
75. Burt, R.K., A. Traynor, L. Statkute, W.G. Barr, R. Rosa, J. Schroeder, L. Verda, N.
Krosnjar, K. Quigley, K. Yaung, M. Villa Bs, M. Takahashi, B. Jovanovic, and Y.
Oyama, Nonmyeloablative hematopoietic stem cell transplantation for systemic lupus
erythematosus. Jama, 2006. 295(5): p. 527-35.
76. Brunner, H.I., G.C. Higgins, M.S. Klein-Gitelman, S.K. Lapidus, J.C. Olson, K. Onel, M.
Punaro, J. Ying, and E.H. Giannini, Minimal clinically important differences of disease
activity indices in childhood-onset systemic lupus erythematosus. Arthritis Care Res
(Hoboken), 2010. 62(7): p. 950-9.

136
77. Navarra, S.V., R.M. Guzman, A.E. Gallacher, S. Hall, R.A. Levy, R.E. Jimenez, E.K. Li,
M. Thomas, H.Y. Kim, M.G. Leon, C. Tanasescu, E. Nasonov, J.L. Lan, L. Pineda, Z.J.
Zhong, W. Freimuth, and M.A. Petri, Efficacy and safety of belimumab in patients with
active systemic lupus erythematosus: a randomised, placebo-controlled, phase 3 trial.
Lancet, 2011.
78. Wallace, D., Epratuzumab Demonstrates Clinically Meaningful Improvements in Patients
with Moderate to Severe Systemic Lupus Erythematosus (SLE): Results from
EMBLEM™, a Phase IIb Study. Lupus, 2010. 19 (1 suppl) p. 1-185
79. Isenberg, D.A., A. Rahman, E. Allen, V. Farewell, M. Akil, I.N. Bruce, D. D'Cruz, B.
Griffiths, M. Khamashta, P. Maddison, N. McHugh, M. Snaith, L.S. Teh, C.S. Yee, A.
Zoma, and C. Gordon, BILAG 2004. Development and initial validation of an updated
version of the British Isles Lupus Assessment Group's disease activity index for patients
with systemic lupus erythematosus. Rheumatology (Oxford), 2005. 44(7): p. 902-6.
80. McCune, W.J., J. Golbus, W. Zeldes, P. Bohlke, R. Dunne, and D.A. Fox, Clinical and
immunologic effects of monthly administration of intravenous cyclophosphamide in
severe systemic lupus erythematosus. N Engl J Med, 1988. 318(22): p. 1423-31.
81. Steinberg, A.D. and S.C. Steinberg, Long-term preservation of renal function in patients
with lupus nephritis receiving treatment that includes cyclophosphamide versus those
treated with prednisone only. Arthritis Rheum, 1991. 34(8): p. 945-50.
82. Boumpas, D.T., H.A. Austin, 3rd, E.M. Vaughn, J.H. Klippel, A.D. Steinberg, C.H.
Yarboro, and J.E. Balow, Controlled trial of pulse methylprednisolone versus two
regimens of pulse cyclophosphamide in severe lupus nephritis. Lancet, 1992. 340(8822):
p. 741-5.
83. Bansal, V.K. and J.A. Beto, Treatment of lupus nephritis: a meta-analysis of clinical
trials. Am J Kidney Dis, 1997. 29(2): p. 193-9.
84. Urowitz, M.B., D. Ibanez, Y. Ali, and D.D. Gladman, Outcomes in patients with active
lupus nephritis requiring immunosuppressives who never received cyclophosphamide. J
Rheumatol, 2007. 34(7): p. 1491-6.
85. Felson, D.T. and J. Anderson, Evidence for the superiority of immunosuppressive drugs
and prednisone over prednisone alone in lupus nephritis. Results of a pooled analysis.
The New England journal of medicine, 1984. 311(24): p. 1528-33.

137
86. McCune, W.J., J. Golbus, W. Zeldes, P. Bohlke, R. Dunne, and D.A. Fox, Clinical and
immunologic effects of monthly administration of intravenous cyclophosphamide in
severe systemic lupus erythematosus. The New England journal of medicine, 1988.
318(22): p. 1423-31.
87. Stohl, W., F. Hiepe, K.M. Latinis, M. Thomas, M.A. Scheinberg, A. Clarke, C. Aranow,
F.R. Wellborne, C. Abud-Mendoza, D.R. Hough, L. Pineda, T.S. Migone, Z.J. Zhong,
W.W. Freimuth, and W.W. Chatham, Belimumab reduces autoantibodies, normalizes low
complement, and reduces select B-cell populations in patients with systemic lupus
erythematosus. Arthritis and rheumatism, 2012.
88. Tan, E.M., A.S. Cohen, J.F. Fries, A.T. Masi, D.J. McShane, N.F. Rothfield, J.G.
Schaller, N. Talal, and R.J. Winchester, The 1982 revised criteria for the classification of
systemic lupus erythematosus. Arthritis and rheumatism, 1982. 25(11): p. 1271-7.
89. Gladman, D.D., Indicators of disease activity, prognosis, and treatment of systemic lupus
erythematosus. Curr Opin Rheumatol, 1994. 6(5): p. 487-92.
90. Strand, V., D. Gladman, D. Isenberg, M. Petri, J. Smolen, and P. Tugwell, Outcome
measures to be used in clinical trials in systemic lupus erythematosus. J Rheumatol,
1999. 26(2): p. 490-7.
91. Tan, E.M., A.S. Cohen, J.F. Fries, A.T. Masi, D.J. McShane, N.F. Rothfield, J.G.
Schaller, N. Talal, and R.J. Winchester, The 1982 revised criteria for the classification of
systemic lupus erythematosus. Arthritis Rheum, 1982. 25(11): p. 1271-7.
92. Beaton DE, et al. Course notes: measurement skills workshop; University of Toronto
Health Policy, Management and Evaluation; 2010.
93. Streiner DL, Norman GR. Health measurement scales: a practical guide to their
development and use. In: StreinerDL, NormanGR, editors. Validity. New York: Oxford
University Press; 2008:247–76.
94. Streiner, D.L., A checklist for evaluating the usefulness of rating scales. Canadian journal
of psychiatry. Revue canadienne de psychiatrie, 1993. 38(2): p. 140-8.
95. Touma, Z., M.B. Urowitz, P.R. Fortin, C. Landolt, S.M. Toloza, C. Riddell, V. Chandran,
L. Eder, A. Ghanem, O. Ziouzina, S. Taghavi-Zadeh, D. Ibanez, and D.D. Gladman,
Systemic lupus erythematosus disease activity index 2000 responder index-50: a reliable
index for measuring improvement in disease activity. J Rheumatol, 2011. 38(5): p. 868-
73.

138
96. McHorney, C.A., J.E. Ware, Jr., and A.E. Raczek, The MOS 36-Item Short-Form Health
Survey (SF-36): II. Psychometric and clinical tests of validity in measuring physical and
mental health constructs. Medical care, 1993. 31(3): p. 247-63.
97. Deyo, R.A., P. Diehr, and D.L. Patrick, Reproducibility and responsiveness of health
status measures. Statistics and strategies for evaluation. Controlled clinical trials, 1991.
12(4 Suppl): p. 142S-158S.
98. Hochberg, M.C., Updating the American College of Rheumatology revised criteria for
the classification of systemic lupus erythematosus. Arthritis Rheum, 1997. 40(9): p. 1725.
99. Wollaston, S.J., V.T. Farewell, D.A. Isenberg, C. Gordon, J.T. Merrill, M.A. Petri, and
K.C. Kalunian, Defining response in systemic lupus erythematosus: a study by the
Systemic Lupus International Collaborating Clinics group. The Journal of rheumatology,
2004. 31(12): p. 2390-4.
100. Wolfe, F., K. Michaud, T. Pincus, D. Furst, and E. Keystone, The disease activity score is
not suitable as the sole criterion for initiation and evaluation of anti-tumor necrosis
factor therapy in the clinic: discordance between assessment measures and limitations in
questionnaire use for regulatory purposes. Arthritis and rheumatism, 2005. 52(12): p.
3873-9.
101. Shrout, P.E. and J.L. Fleiss, Intraclass correlations: uses in assessing rater reliability.
Psychological bulletin, 1979. 86(2): p. 420-8.
102. Bernatsky, S., J.F. Boivin, L. Joseph, S. Manzi, E. Ginzler, D.D. Gladman, M. Urowitz,
P.R. Fortin, M. Petri, S. Barr, C. Gordon, S.C. Bae, D. Isenberg, A. Zoma, C. Aranow,
M.A. Dooley, O. Nived, G. Sturfelt, K. Steinsson, G. Alarcon, J.L. Senecal, M. Zummer,
J. Hanly, S. Ensworth, J. Pope, S. Edworthy, A. Rahman, J. Sibley, H. El-Gabalawy, T.
McCarthy, Y. St Pierre, A. Clarke, and R. Ramsey-Goldman, Mortality in systemic lupus
erythematosus. Arthritis Rheum, 2006. 54(8): p. 2550-7.
103. Gladman, D.D., N. Hirani, D. Ibanez, and M.B. Urowitz, Clinically active serologically
quiescent systemic lupus erythematosus. J Rheumatol, 2003. 30(9): p. 1960-2.
104. Agarwal, G.G., S. Awasthi, and S.D. Walter, Intra-class correlation estimates for
assessment of vitamin A intake in children. Journal of health, population, and nutrition,
2005. 23(1): p. 66-73.
105. Landis, J.R. and G.G. Koch, The measurement of observer agreement for categorical
data. Biometrics, 1977. 33(1): p. 159-74.

139
106. Portney LG, Watkins MP. Statistical measures of reliability. In: PortneyLG, WatkinsMP,
editors. Foundations of clinical research: Applications to practice. International edition.
Upper Saddle River, NJ: Pearson Higher Education; 2008:557–85.
107. The American College of Rheumatology response criteria for systemic lupus
erythematosus clinical trials: measures of overall disease activity. Arthritis Rheum,
2004. 50(11): p. 3418-26.
108. Worster, A., A. Sardo, K. Eva, C.M. Fernandes, and S. Upadhye, Triage tool inter-rater
reliability: a comparison of live versus paper case scenarios. Journal of emergency
nursing: JEN : official publication of the Emergency Department Nurses Association,
2007. 33(4): p. 319-23.
109. Beaton, D.E., S. Hogg-Johnson, and C. Bombardier, Evaluating changes in health status:
reliability and responsiveness of five generic health status measures in workers with
musculoskeletal disorders. Journal of clinical epidemiology, 1997. 50(1): p. 79-93.
110. Yee, C.S., D.A. Isenberg, A. Prabu, K. Sokoll, L.S. Teh, A. Rahman, I.N. Bruce, B.
Griffiths, M. Akil, N. McHugh, D. D'Cruz, M.A. Khamashta, P. Maddison, A. Zoma, and
C. Gordon, BILAG-2004 index captures systemic lupus erythematosus disease activity
better than SLEDAI-2000. Ann Rheum Dis, 2008. 67(6): p. 873-6.
111. Fleiss JL. The design and analysis of clinical experiments. New York: John Wiley and
Sons; 1986.
112. Tammemagi, M.C., J.W. Frank, M. Leblanc, H. Artsob, and D.L. Streiner,
Methodological issues in assessing reproducibility--a comparative study of various
indices of reproducibility applied to repeat ELISA serologic tests for Lyme disease.
Journal of clinical epidemiology, 1995. 48(9): p. 1123-32.
113. McHorney, C.A. and A.R. Tarlov, Individual-patient monitoring in clinical practice: are
available health status surveys adequate? Quality of life research : an international
journal of quality of life aspects of treatment, care and rehabilitation, 1995. 4(4): p. 293-
307.
114. Touma Z, Urowitz MB, Taghavi-Zadeh S, Ibañez D, Gladman DD. Systemic Lupus
Erythematosus Disease Activity Index 2000 (SLEDAI-2K) Responder Index (SRI)-50:
Sensitivity at 6 and 12 months. Rheumatology (Oxford) January 2012 (In press).

140
115. Urowitz, M.B. and D.D. Gladman, Contributions of observational cohort studies in
systemic lupus erythematosus: the university of toronto lupus clinic experience. Rheum
Dis Clin North Am, 2005. 31(2): p. 211-21, v.
116. Furie, R.A., M.A. Petri, D.J. Wallace, E.M. Ginzler, J.T. Merrill, W. Stohl, W.W.
Chatham, V. Strand, A. Weinstein, M.R. Chevrier, Z.J. Zhong, and W.W. Freimuth,
Novel evidence-based systemic lupus erythematosus responder index. Arthritis and
rheumatism, 2009. 61(9): p. 1143-51.