Department of Obstetrics and Gynecology PPH: We don’t need NO stinkin’ blood! June 11, 2015.
15
Department of Obstetrics and Gynecology PPH: We don’t need NO stinkin’ blood! June 11, 2015
-
Upload
merry-watts -
Category
Documents
-
view
221 -
download
3
Transcript of Department of Obstetrics and Gynecology PPH: We don’t need NO stinkin’ blood! June 11, 2015.
Department of Obstetrics and Gynecology
PPH: We don’t need NO stinkin’ blood!June 11, 2015
Background
Postpartum hemorrhage is a leading cause of maternal mortality.
Several morbidity events at St. Joseph Medical Center led to our focus on this problem.
Vaginal Delivery % Hgb Change
Feb 2012n=88
0%
5%
10%
15%
20%
25%
30%
35%
40%
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51 53 55 57 59 61 63 65 67 69 71 73 75 77 79 81 83 85 87
pt
rate
of
ch
an
ge
Goal <15%
Average Hgb Change = 13.1%
25/88=28% of vaginal deliveries have higher than 15% change in Hgb. These are our target
Avg % Hgb Change vs %Hgb Change >15%Vaginal Deliveries
13.0% 12.6% 13.1%
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
1 2 3June 2010
March 2011
February 2012
Avg % Hgb Change
% Hgb Change >15%
39%
25%
28%
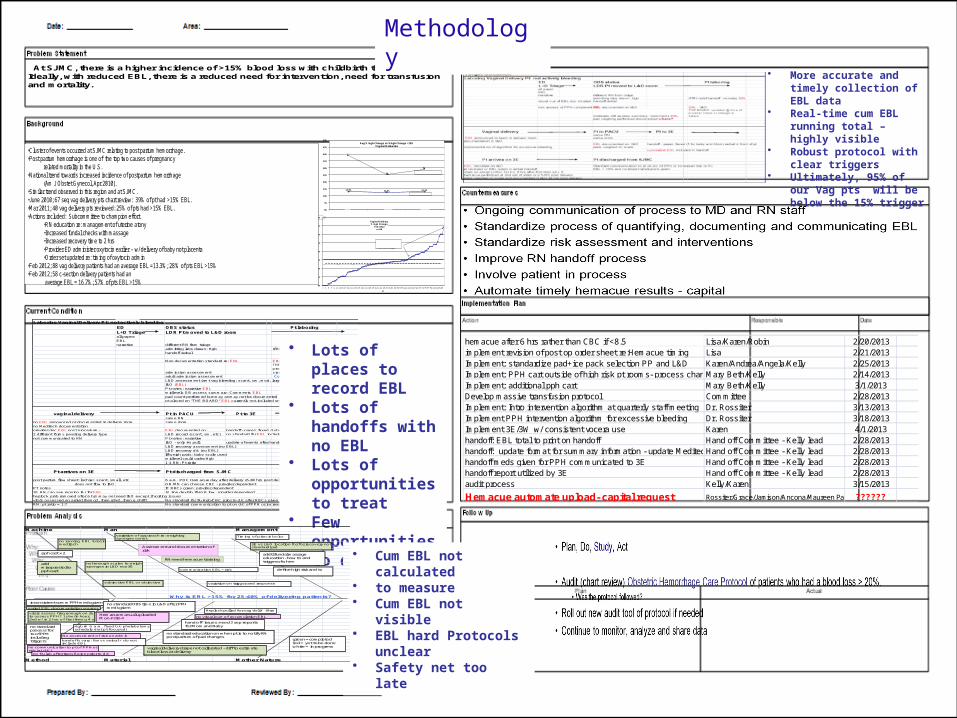
At SJMC, there is a higher incidence of >15% blood loss with childbirth than desirable. Ideally, with reduced EBL, there is a reduced need for intervention, need for transfusion and mortality.
•Cluster of events occurred at SJMC relating to post partum hemorrhage.•Post partum hemorrhage is one of the top two causes of pregnancy
related mortality in the U.S.•National trend towards increased incidence of postpartum hemorrhage
(Am J Obstet Gynecol, Apr 2010).•Similar trend observed in this region and at SJMC.•June 2010; 67 seq vag delivery pts chart review: 39% of pt had >15% EBL.•Mar 2011; 40 vag delivery pts reviewed: 25% of pts had >15% EBL.•Actions included: Subcommittee to champion effort.
•RN education re: management of uterine atony•Increased fundal checks with massage•Increased recovery time to 2 hrs•Provider ED administer oxytocin earlier – w/ delivery of baby not placenta•Order set updated re: timing of oxytocin admin
•Feb 2012; 88 vag delivery patients had an average EBL =13.3%; 28% of pts EBL >15%•Feb 2012; 58 c-section delivery patients had an
average EBL = 16.7%; 57% of pts EBL >15%
Laboring Vaginal Delivery Pt: not actively bleedingED OBS status Pt laboringL+D Triage LDR Pt moved to L&D roomall paper: EBL narrative different RN from triage
admitting labs drawn: Hgb if RN relief handoff may not include EBLhandoff verbal
Non documentation standard re: EBL EBL : pt notes or I&O
admission assessment
THE BOARD: updated @ time of provider check or change in status
adult admission assessment Could the board include running EBL?L&D assessment (amt vag bleeding: scant, sm, mod, large)I&O (EBL)Pt notes: narrative EBLmidlevels OB assess summary: Comments EBLpad count performed but may or may not be documentedpt placed on "THE BOARD" EBL currently not included on BOARD
vaginal delivery Pt in PACU Pt to 3Esame RN
no EBL announced or documented in delivery room same roomno Meditech documentation provider doc EBL post procedure - EBL documented on: handoff - paper, faxed (1=baby, 1=mom)2 different forms pending delivery type L&D record (scant, sm, etc) no standard for EBL includednot communicated to RN Pt notes: narrative
I&O - only #s pull update of events after handoff faxed are verbalL&D recovery assessment (no EBL)L&D recovery d/c (no EBL)If weigh pads: baby scale usedmidlevel could order Hgb1:1 RN: Pt ratio
Pt arrives on 3E Pt discharged from SJMC
post partum flow sheet: lochia= scant, small, etc 6 a.m. POC Hemacue day after delivery (6-30 hrs post delivery)does not flow to I&O OR MD can choose CBC - provider dependent
PT notes IF RBCs given: provider dependent3E RN can see running I&) for EBL IV Iron dextrin if HGB low: provider dependentheplock prob removed after 6 hrs may not need I&O except if voiding issuesvitals assessed on arrival then q2, then q8x2, then q shift? No standard for f/u Hgb/CBC prior to d/c after RBCs givenRN: pt ratio = 1:? No standard communication to pt on d/c of PPH or increased risk or f/u.
• Lots of places to record EBL
• Lots of handoffs with no EBL
• Lots of opportunities to treat
• Few opportunities to diagnosis
• Cum EBL not calculated
• to measure• Cum EBL not visible• EBL hard Protocols
unclear• Safety net too late
• More accurate and timely collection of EBL data
• Real-time cum EBL running total – highly visible
• Robust protocol with clear triggers
• Ultimately, 95% of our Vag pts will be below the 15% trigger
Machine Man Management
Why is EBL >15% for 25-40% of delivering patients?
Method Material Mother Nature
no running EBL total in meditech
not enough scales to weigh sponges in L&D nor 3E
variation of approach re: weighing sponges or not
variation on trigger and response
Timing of pitocin bolus
3E vs L&D location for for recovery not standardized
No assessment of risk on admit
Hgb @ 6 a.m. f ixed b/c phelebotomy schedule (not pt focused)
subjective EBL vs objective
communication EBL +risk
varied EBL documentation sources
no visual cue of accumulation EBL
handoffs vary: fax vs verbal + do not include EBL
Heplock pulled for vag del @ 6hrsvitals assess freq enough on 3E to assess PPH? 1st w/in hour, 2nd w/ in 2 hrs of f irst then q 4 x
no communication to pt of PPH or risk (at d/c)
no f /u lab af ter transfusion prior to d/c
Hemacue manual uploadedMon-Fri 8-4
RN need hemacue training
inconsistent comm PPH meds given no standard OBS time in L&D after PPH meds given
hand off issues: need 2 sep reportsfor Mom and Baby
no standard education on when pt is to notify RN post partum of pad changes
vaginaldelivery drape not calibrated - diff to estimate blood loss at delivery
no standard process for tx of PPH including triggers
pph cart x 2
Assessment and documentation of risk
addtl fundal massage education - how to and trigger of when
define high risk and tx
green = completedred = yet to be donewhite = in progress
add misoprostol to pph cart
hemacue after 6 hrs rather than CBC if <8.5 Lisa/Karen/Robin 2/20/2013implement revision of post op order sheet re:Hemacue timing Lisa 2/21/2013Implement: standardize pad+ice pack selection PP and L&D Karen/Andrea/Angela/Kelly 2/25/2013Implement: PPH cart outside of high risk pt rooms- process changeMary Beth/Kelly 2/14/2013Implement: additional pph cart Mary Beth/Kelly 3/1/2013Develop massive transfusion protocol Committee 2/28/2013Implement: Intro intervention algorithm at quarterly staff meeting Dr. Rossiter 3/13/2013Implement PPH intervention algorithm for excessive bleeding Dr. Rossiter 3/18/2013Implement 3E/3W w/ consistent vocera use Karen 4/1/2013handoff: EBL total to print on handoff Hand off Committee - Kelly lead 2/28/2013handoff: update format for summary information - update MeditechHand off Committee - Kelly lead 2/28/2013handoff meds given for PPH communicated to 3E Hand off Committee - Kelly lead 2/28/2013handoff report utilized by 3E Hand off Committee - Kelly lead 2/28/2013audit process Kelly/Karen 3/15/2013
Hemacue automate upload- capital request Rossiter/Grace/Jamison/Ancona/Maureen Paul ??????
Methodology
Walk the process
What we had to fix
1. Many places to record EBL
2. Handoffs without EBL included
3. Many opportunities to treat
4. Few opportunities to diagnose
Highlights of implementation
Interventions Standardized:
Timing of postpartum oxytocin Timing of postpartum hemoglobin
Assembled PPH carts Developed intervention algorithm Developed massive transfusion protocol
Highlights of implementation
Quantification of blood loss Purchased scales for every room in L&D and
postpartum floor
Purchased graduated drapes for vaginal deliveries
Educated MDs and CNMs to announce EBL at both c/s and vaginal deliveries
Educated nurses to teach patients re: need to weigh all peri-pads for the 1st 24 hours
Highlights of implementation
Communication Added blood loss entry to I’s +O’s in EMR
Added EBL to communication tool for nursing handoff from L&D to postpartum
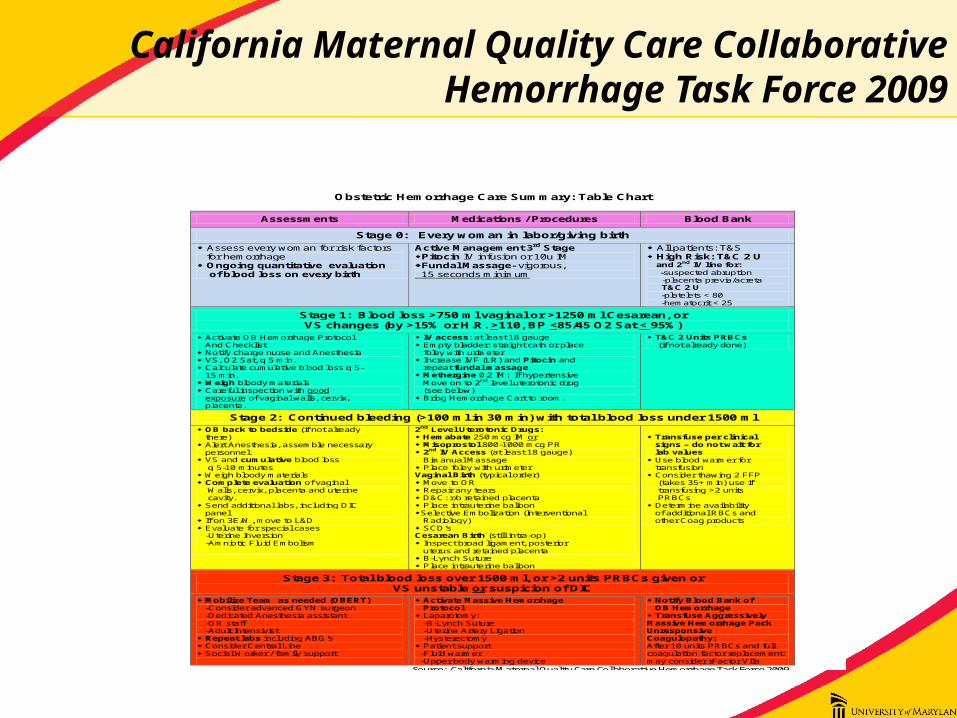
California Maternal Quality Care Collaborative Hemorrhage Task Force 2009
Obstetric Hemorrhage Care Summary: Table Chart
Assessments Medications / Procedures Blood Bank
Stage 0: Every woman in labor/giving birth
Assess every woman for risk factors for hemorrhage Ongoing quantitative evaluation of blood loss on every birth
Active Management 3rd Stage Pitocin IV infusion or 10u IM Fundal Massage- vigorous, 15 seconds minimum
All patients: T&S High Risk: T&C 2 U and 2nd IV line for:
-suspected abruption -placenta previa/acreta T&C 2 U
-platelets < 80 -hematocrit < 25
Stage 1: Blood loss >750 ml vaginal or >1250 ml Cesarean, or VS changes (by >15% or H.R. >110, BP <85/45 O2 Sat < 95%)
Activate OB Hemorrhage Protocol And Checklist Notify charge nurse and Anesthesia VS, O2 Sat, q 5 min. Calculate cumulative blood loss q 5- 15 min. Weigh bloody materials Careful inspection with good exposure of vaginal walls, cervix, placenta.
IV access: at least 18 gauge Empty bladder: straight cath or place foley with urimeter Increase IVF (LR) and Pitocin and repeat fundal massage Methergine 0.2 IM: If hypertensive Move on to 2nd level uterotonic drug (see below) Bring Hemorrhage Cart to room.
T&C 2 Units PRBCs (if not already done)
Stage 2: Continued bleeding (>100 ml in 30 min) with total blood loss under 1500 ml OB back to bedside (if not already there) Alert Anesthesia, assemble necessary personnel. VS and cumulative blood loss q 5-10 minutes Weigh bloody materials Complete evaluation of vaginal Walls, cervix, placenta and uterine cavity. Send additional labs, including DIC panel If on 3E/W, move to L&D Evaluate for special cases -Uterine Inversion -Amniotic Fluid Embolism
2nd Level Uterotonic Drugs: Hemabate 250 mcg IM or Misoprostol 800-1000 mcg PR 2nd IV Access (at least 18 gauge) Bimanual Massage Place foley with urimeter Vaginal Birth (typical order) Move to OR Repair any tears D&C: r/o retained placenta Place intrauterine balloon Selective Embolization (Interventional Radiology) SCD’s Cesarean Birth (still intra-op) Inspect broad ligament, posterior uterus and retained placenta B-Lynch Suture Place intrauterine balloon
Transfuse per clinical signs – do not wait for lab values Use blood warmer for transfusion Consider thawing 2 FFP (takes 35+ min) use if transfusing >2 units PRBCs Determine availability of additional RBCs and other Coag products
Stage 3: Total blood loss over 1500 ml, or >2 units PRBCs given or VS unstable or suspicion of DIC
Mobilize Team as needed (OBERT) -Consider advanced GYN surgeon -Dedicated Anesthesia assistant -OR staff -Adult Intensivist Repeat labs including ABG’s Consider Central Line Social Worker / family support
Activate Massive Hemorrhage Protocol Laparotomy: -B-Lynch Suture -Uterine Artery Ligation -Hysterectomy Patient support -Fluid warmer -Upper body warming device
Notify Blood Bank of OB Hemorrhage Transfuse Aggressively Massive Hemorrhage Pack Unresponsive Coagulopathy: After 10 units PRBCs and full coagulation factor replacement: may consider rFactor VIIa
Source: California Maternal Quality Care Collaborative Hemorrhage Task Force 2009
University of Maryland St. Joseph Medical Center
7601 Osler Drive • Towson, MD 21204-7582 Draft 2/1/13
Q1
2011
Q2
2011
Q3
2011
Q4
2011
Q1
2012
Q2
2012
Q3
2012
Q4
2012
Q1
2013
Q2
2013
Q3
2013
Q4
2013
Q1
2014
Q2
2014
Q3
2014
Q4
2014
Q1
2015
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
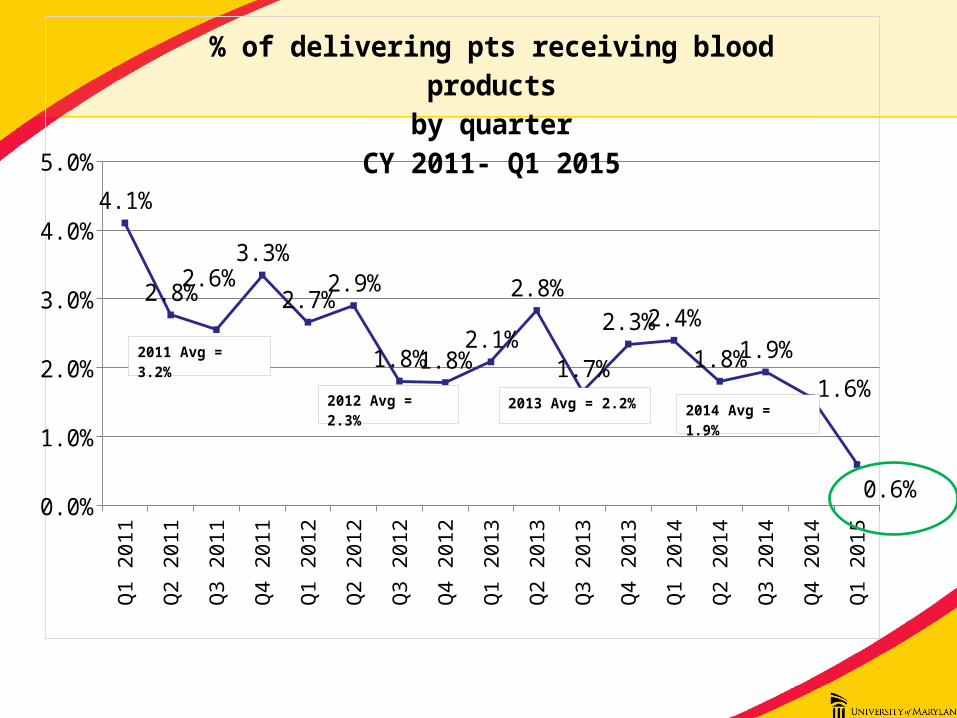
4.1%
2.8%2.6%
3.3%
2.7%2.9%
1.8%1.8%2.1%
2.8%
1.7%
2.3%2.4%
1.8%1.9%
1.6%
0.6%
% of delivering pts receiving blood productsby quarter
CY 2011- Q1 2015
2012 Avg = 2.3%
2011 Avg = 3.2%
2013 Avg = 2.2% 2014 Avg = 1.9%
Q1 13 Q2 13 Q3 13 Q4 13 Q1 14 Q2 14 Q3 14 Q4 14 Q1 150
10
20
30
40
50
60
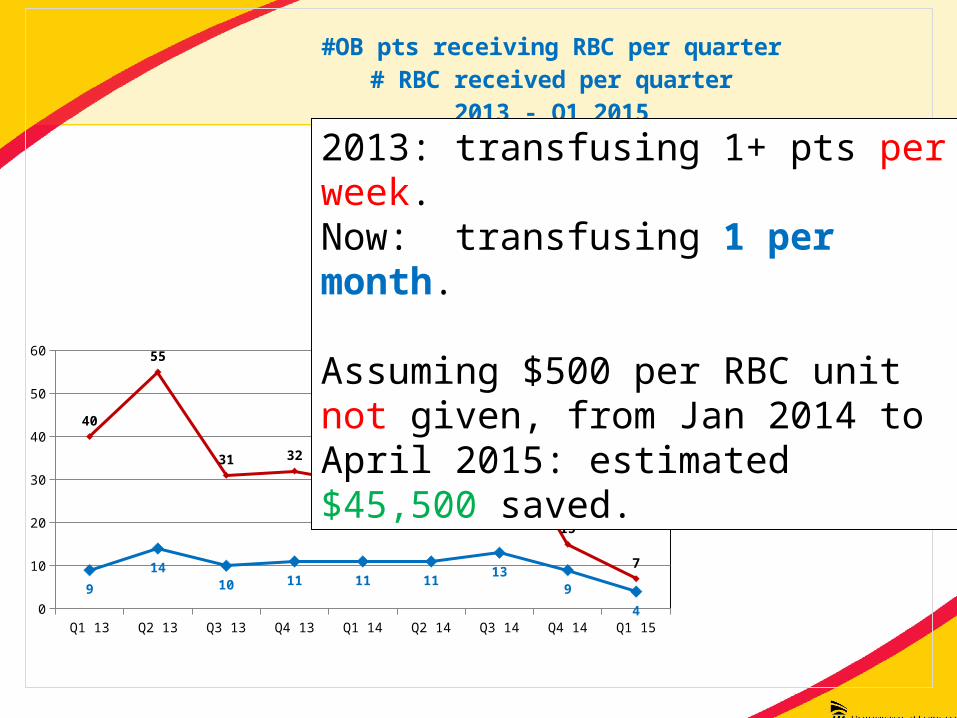
9
1410 11 11 11
139
4
40
55
31 3229 29
42
15
7
#OB pts receiving RBC per quarter# RBC received per quarter
2013 - Q1 2015
# pts transfused
# units given
2013: transfusing 1+ pts per week. Now: transfusing 1 per month.
Assuming $500 per RBC unit not given, from Jan 2014 to April 2015: estimated $45,500 saved.
Current state: sustainment
Education of providers:Transfuse to symptomatic patients Transfuse single unit at a time
Chart review: 100% of delivering patients receiving blood products
Feedback to all providers and staff
Lessons learned
• ClinicalChange in perspective
“We measure everything else, why not blood?”
Change in process results in fewer surprises
Lessons learned
• TeamworkMultidisciplinary approach including the day to day
staff
Involvement in creating the solution engenders enthusiasm and buy in
Standardized approach and walking the process is profoundly valuable
• Kelly Archer, RN L&D
• David Brinker, MD Blood Bank Advisory Chair
• Mary Beth Campbell, RN L&D
• Alice Cootauco, MD MFM• Phi Duong, Blood Bank
• Tracey Duke, MD OB/GYN
• Lisa Everhart, RN Clinical Educator
• Maria Giachini, RN L&D
• Robin Harper, RN Postpartum
• Diane Interrante, RN Quality
• Nikki Koklanaris, MD MFM• Mary Knauer, CNM • Laurie Mathis, RN
Postpartum
• Maureen Paul, Laboratory
• Charlie Rizzuto, MD Anesthesiology
• Nancy Stec, Blood Bank
• Karen Tomcho, RN Postpartum
• Judy Rossiter, MD Chief OB/GYN
The PPH initiative team: it takes a village!