Department of Microbiology Mymensingh Medical College ...
124
Detection of Different Diarrheagenic Escherichia coli Strains by Multiplex PCR. Dr.Md.Rashedul kabir MBBS Department of Microbiology Mymensingh Medical College Mymensingh. Bangladesh 2011
Transcript of Department of Microbiology Mymensingh Medical College ...

Detection of Different Diarrheagenic Escherichia coli
Strains by Multiplex PCR.
Dr.Md.Rashedul kabir MBBS
Department of Microbiology Mymensingh Medical College
Mymensingh. Bangladesh 2011
id859406 pdfMachine by Broadgun Software - a great PDF writer! - a great PDF creator! - http://www.pdfmachine.com http://www.broadgun.com

This thesis entitled �Detection of Different Diarrheagenic Escherichia coli Strains by
Multiplex PCR� is submitted by Dr. Md. Rashedul Kabir in partial fulfillment of the
requirement for the degree of Master of Philosophy (Medical science) in Microbiology,
University of Dhaka. The study was carried out in the Department of Microbiology,
Mymensingh Medical College, Mymensingh during the period of January 2011 to December
2011.
Acceptance of the thesis had been approved by the following board of examiners.
Chairman
Prof. (Dr.) Md. Akram Hossain
Members
1. Prof. (Dr.) Abdullah Akhter Ahmed
2. Prof. (Dr.) Kalpana Deb
3. Prof (Dr.) Marium Khatun
Date of approval, April 30, 2011
Mymensingh.

TO WHOM IT MAY CONCERN
This is to certify that Dr. Md. Rashedul kabir, a student of thesis part has completed the thesis
entitled, �Detection of Different Diarrheagenic Escherichia coli Strains by Multiplex
PCR� in the Department of Microbiology, Mymensingh Medical College, under my
guidance and supervision and this is up to my satisfaction. His protocol was approved by
protocol approval committee of the Department of Microbiology and ethical review
committee of Mymensingh Medical College.
This unbound thesis work is forwarded for kind consideration and needful.
Professor Dr. Md. Akram Hossain Head of the Department of Microbiology Mymensingh Medical College, Mymensingh, Bangladesh.

Declaration
I hereby declare that the whole work submitted as a thesis entitled �Detection of Different
Diarrheagenic Escherichia coli Strains by Multiplex PCR� in the Department of the
microbiology, Mymensingh Medical College, Dhaka University, for the Degree of Master of
philosophy is the result of my own investigation and was carried out under the supervision of
Professor Dr. Md. Akram Hossain.
I, further declare this thesis or part thereof has not been concurrently submitted for the award
of any Degree or Diploma anywhere.
Dr. Md. Rashedul kabir M Phil, Thesis part Department of Microbiology Mymensingh Medical College Mymensingh.
ACKNOWLEDGEMENT

Thanks to Almighty Allah, the merciful and the beneficial for giving me the opportunity
courage and enough energy to carry out and complete the entire thesis work.
I am grateful and deeply indebted to my guide Professor Dr. Md. Akram Hossain, Head of
the Department of Microbiology, Mymensingh Medical College, Mymensingh. I have the
great privilege and honour to express my indebtedness to him for kindly placing at my
disposal all the facilities available in the department, for his guidance, supervision, inspiring
encouragement, constructive criticism and help in carrying out this thesis work.
I am grateful and express thanks to the honorable members of the Ethical Review Committee
for giving kind approval to my research protocol. I am obliged to Professor Dr. Md. Aminul
Hoque, Principal of Mymensingh Medical College, Mymensingh for his kind permission to
conduct the thesis.
My cordial respect and complements to Dr. Shyamal Kumar Paul, Assistant Professor, of
Microbiology, Mymensingh Medical College, Mymensingh for his help from the beginning
of the course up to completion of my thesis.
I owe my gratitude to respective teacher Dr. Md Chand Mahamud, Assistant Professor of
Microbiology, Mymensingh Medical College, Mymensingh, for his constructive criticism in
correcting this thesis with his wise advice and active cooperation.
I am grateful and express thanks to Professor Nobumichi Kobayashi, Sapporo Medical
University of Japan for providing with me primers for PCR and for his valuable suggestion.
I specially extend my heartfelt gratitude to Dr. Azizul Haque, Associate Professor, of
Pediatrics�, Mymensingh Medical College, Mymensingh for his cordial cooperation and
valuable suggestion.
I like to express gratitude to all other teachers, laboratory technologist and other staffs of
Microbiology department, Mymensingh Medical College, Mymensingh for their constant
help and sincere cooperation during the entire study period.
I express my gratitude to my parents, friends and well wisher who inspire and help me
continuously.
I remained incomplete if I do not express whole hearted thanks and gratitude to my wife
Dr. Tasnuva Mariom for sparing me so much time in this job from all sorts of social and
family responsibilities and sharing my pain and pleasure. Last but not least I express my
heartiest affection for my kid Tahsan who had been deprived of my care and attention during
the thesis work.
Lastly I am indebted to all those persons from whom I have collected samples. May Allah
give them better rewards. Thank again.
Dr. Md. Rashedul Kabir

Dedicated
to
Professor Dr. Md. Akram Hossain
and
My parents

CONTENTS
Page No.
LIST OF TABLES VIII
LIST OF FIGURES IX
LIST OF ABBREVIATIONS X
SUMMARY XI-XII
CHAPTER 1 : INTRODUCTION & OBJECTIVES 1 � 5
INTRODUCTION 1
OBJECTIVES 5
CHAPTER 2 : REVIEW OF LITERATURE 6 � 40
CHAPTER 3 : MATERIALS AND METHODS 41 � 51
CHAPTER 4 : RESULTS 52 � 65
CHAPTER 5 : DISCUSSION 66 � 74
CHAPTER 6 : CONCLUSION & RECOMMENDATIONS 75
LIST OF REFERENCES 76 � 104
PHOTOGRAPHS 105 � 115
APPENDICES i� xiii
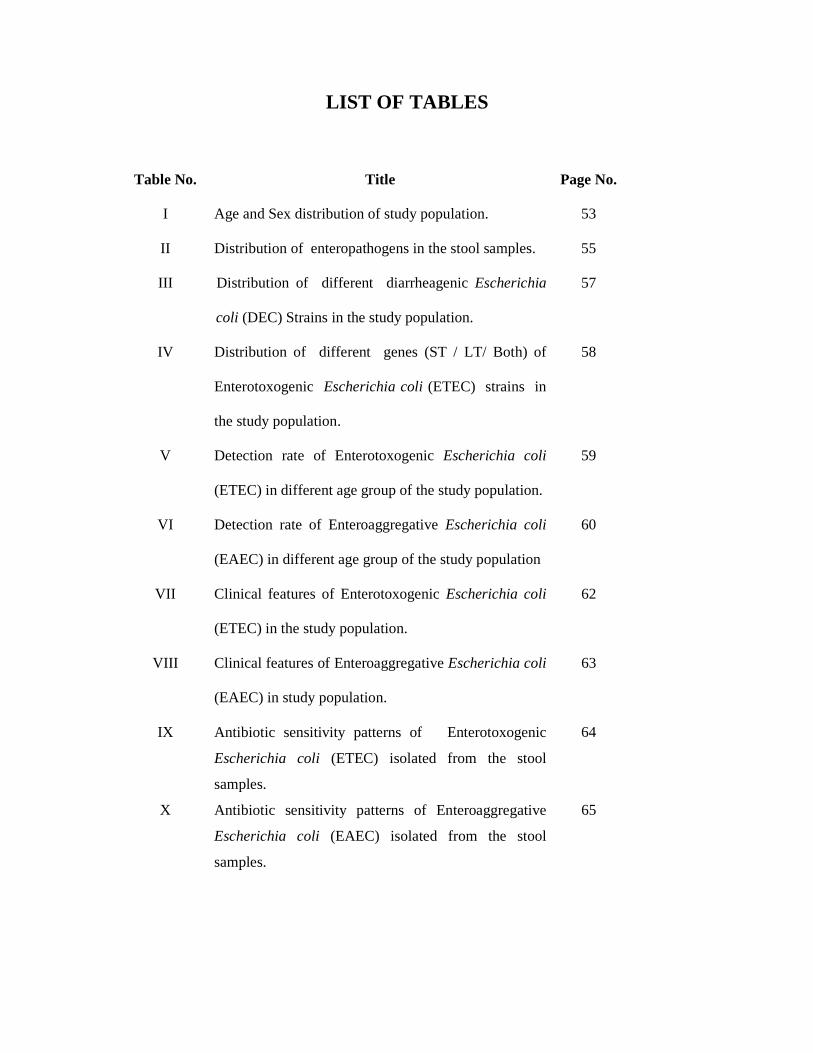
LIST OF TABLES
Table No. Title Page No.
I Age and Sex distribution of study population. 53
II Distribution of enteropathogens in the stool samples. 55
III Distribution of different diarrheagenic Escherichia
coli (DEC) Strains in the study population.
57
IV Distribution of different genes (ST / LT/ Both) of
Enterotoxogenic Escherichia coli (ETEC) strains in
the study population.
58
V Detection rate of Enterotoxogenic Escherichia coli
(ETEC) in different age group of the study population.
59
VI Detection rate of Enteroaggregative Escherichia coli
(EAEC) in different age group of the study population
60
VII Clinical features of Enterotoxogenic Escherichia coli
(ETEC) in the study population.
62
VIII Clinical features of Enteroaggregative Escherichia coli
(EAEC) in study population.
63
IX Antibiotic sensitivity patterns of Enterotoxogenic
Escherichia coli (ETEC) isolated from the stool
samples.
64
X Antibiotic sensitivity patterns of Enteroaggregative
Escherichia coli (EAEC) isolated from the stool
samples.
65

LIST OF FIGURES
Figure No.
Title
Page No.
1.1 Age distribution of study population 54
1.2 Sex distribution of study population 54

LIST OF ABBREVIATIONS
A/A Aggregative adherence
A/E Attaching and effacing
AID Acute Infectious Diarrhea
ATCC American Type Culture collection.
CDC Centre for Disease Control and Prevention
CFU Colony forming unit
CLSI Clinical and Laboratory Standards Institute
DNA Deoxyribonucleic acid
dNTP Deoxynucleoside triphosphate
EIA Enzyme immune assay
ELISA Enzyme Linked Immunosorbent Assay
Ial Invasion-associated locus
LEE Locus of enterocytes effacement
LPS Lipopolysaccharide
LT Heatlabile toxin
PAGE Polyacrylamide Gel electrophoresis
PCR Polymerase Chain Reaction
RNA Ribonucleic acid
SMAC Sorbitol Mac Con key
ST Heat-stable toxin
Taq Thermus aquaticus
TBE Trise bouric acid EDTA buffer
WHO World Health Organization

SUMMARY
Background: Diarrhaegenic Escherichia coli is one of the most important etiologic agent of
acute diarrhea and represent a major public health problem in developing countries like
Bangladesh. Due to lack of facilities diarrhaegenic Escherichia coli can not be detected in the
routine diagnostic microbiology laboratory. Recently various multiplex PCR methods have
been developed to detect diarrheagenic Escherichia coli. Thereby, the present study was
conducted in the Department of Microbiology, Mymensingh Medical College to detect
different diarrheagenic Escherichia coli strains by multiplex PCR.
Methods: This cross sectional study was done during the period from January 2011 to
December 2011 and included all patients with acute diarrhea irrespective of age and sex
admitted in Mymensingh Medical College Hospital and S.K hospital, Mymensingh. A total of
300 stool samples were examined by standard laboratory methods for identification of
enteropathogens. Different diarrheagenic Escherichia coli strains were detected by Multiplex
PCR following standard methods. Rotavirus was detected by Polyacrylamide Gel
electrophoresis (PAGE).
Results: Of the 300 stool samples examined, Enteropathpgens were detected in 160 (53.5%)
cases. Rotavirus was detected in 82 (27.5%) cases, followed by diarrheagenic Escherichia
coli (DEC) in 54 (18%), Shigella spp. in 8 (2.4%), Salmonella spp. in 5 (1.6%), E. Histolytica
in 4 (1.5%) and G. Lamblia in 3 (1.0%) cases. Among the diarrheagenic Escherichia coli
(DEC), Enterotoxogenic Esch.coli (ETEC) was detected in 39 (13%) cases and
Enteroaggregative Esch .coli (EAEC) in 15 (5%) cases. No Enterohemorrhagic Esch .coli
(EHEC), Enteropathogenic Esch .coli (EPEC) and Enteroinvasive Esch .coli (EIEC) could be

detected. Both (ST and LT) genes of ETEC were detected in 26 (67%) cases, ST gene in 9
(23%) cases and LT gene in 4 (10%) cases.
Conclusion: Analyzing the findings of this present study, diarrheagenic Escherichia coli was
found to be one of the most important cause of acute diarrhea. Detection rate of diarrheagenic
Escherichia coli by multiplex PCR method was quite satisfactory. Thereby, Multiplex PCR
could be adapted to detect different diarrheagenic Escherichia coli in setup like Medical
colleges or tertiary medical facilities.
Introduction
Acute infectious diarrhea (AID) is a major cause of morbidity and mortality worldwide, and
it remains a major public health challenge especially in developing countries where it is a
leading cause of death. Every year nearly 1.4 billion episodes of AID occur in children less
than 5 years of age in developing countries (Kosek et al. 2003; Parashar et al. 2003), of which
123.6 million episodes required outpatient medical care and 9 million episodes required
hospitalization. It has been estimated that the mean number of episodes of diarrhea per year
in children under 5 years of age from a developing region is 3.2, with the highest incidence
(4.8 episodes), occurring during the first year of life, decreasing progressively to 1.4 episodes
per year at 4 years of age. Furthermore, the highest age-mortality rate (8.5 children per
1000/year) occurred in children under 1 year of life (Kosek et al. 2003). In addition diarrheal
illness account for an estimated 12600 deaths each day in children under 5 years of age in
Asia, Africa and Latin America (Nguyen et al. 2005).
Kosek and associates (2003) calculated studies from 1990 to 2000 and concluded that
diarrhea accounts for 21% of all deaths at under five years of age causing 2.5 million death
per year in developing countries. Improvements in sanitation, nutrition, education and early
access to oral rehydration therapy among other measures have lowered the lethality of severe
AID from 4.6 million in 1982 to an estimated 1.5�2.5 million in 2010 (Black et al. 2010;
O'Ryan et al. 2010). However, it remains the second most common cause of death in children
under 5 years of age worldwide according to the Global Burden Disease Report of the WHO
(Kosek et al. 2003).
A diversity of recognized microorganisms such as bacteria, viruses and parasites can be
associated with severe AID in children (Al-Gallas et al. 2007; O'Ryan et al. 2005). However,
etiological information that includes all the known agents of severe AID in children is scarce.
Numerous studies performed in different countries have reported diarrheagenic Escherichia

coli (DEC) pathotypes as being the most frequent and important among bacterial pathogens
associated with AID in developing countries. However, the frequencies of these pathogens
vary with geographic region and depend on the socioeconomic/sanitary conditions achieved
(Black et al. 2010; O'Ryan et al. 2010). Altogether, they represent 30-40% of the cases
(Albert et al. 1999), and about 15-30% have required hospital care (Nataro & Karper 1998;
O'Ryan et al. 2005).
In Bangladesh, the AID remains one of the most important health problems surpassed only by
the respiratory diseases. One third of the total child death burden is due to diarrhea. Every
year, a rural child suffers on average from 4.6 episodes of diarrhea, from which about
230,000 children die (Piechulek et al. 2003). Diarrheagenic Escherichia coli has been
reported to be responsible for 34% of diarrheal episodes in Bangladesh (ICDDR, B 2002).
Escherichia coli is the predominant nonpathogenic facultative anaerobic member of the
human intestinal micro flora. Some Escherichia coli strains, however have developed the
ability to cause disease of the gastrointestinal, urinary and central nervous systems in the
human host. Escherichia coli has been implicated as an agent of diarrheal disease since the
1920s (Nguyen et al. 2005).
There are now at least six types of diarrheagenic strains of Escherichia coli on the basis of
distinct epidemiology and clinical feature, special virulence determinants and association
with certain serotypes: Enterotoxogenic Escherichia coli (ETEC), Enteropathogenic
Escherichia coli (EPEC), Enteroheamorragic Escherichia coli (EHEC), Enteroaggregative
Escherichia coli (EAEC), Enteroinvasive Escherichia coli (EIEC) and Diffusely adhering
Escherichia coli (DAEC). Of these EPEC, ETEC, EIEC, EHEC and EAEC are clearly
associated with different types of enteritis, while the another pathotype is candidate as
potential pathogens but their association with diarrhea has not been clearly assessed and

further studies are required to confirm their etiological role in diarrheal diseases (Rappelli et
al. 2005).
Due to lack of facilities diarrhaegenic Escherichia coli can not be detected in the routine
diagnostic microbiology laboratory in developing countries, which is important in
understanding the disease spectrum, tracing the sources of infection and the burden of the
disease. Such identification would also assist the clinician to dispense appropriate
management (Nessa et al. 2007).
Identification of diarrheagenic Escherichia coli can not be done only by culture and
biochemical tests, since they are indistinguishable from the non pathogenic Escherichia coli
commonly found in human feces. Moreover, specific serotyping is not always correlated with
pathogenicity. The discrimination of different diarrheagenic Escherichia coli strains requires
DNA target based screening by molecular techniques (Rappelli et al. 2005).
PCR, one of the molecular based detection methods, commonly used for rapid and reliable
diagnosis, which has a high sensitivity and specificity. To detect different diarrheagenic
Escherichia coli strains, it is necessary to run several individual PCRs with different primer
pairs. In order to simplify diagnosis, various multiplex PCR methods have been developed
for the simultaneous detection of several specific genes of different diarrheagenic
Escherichia coli strains. This method showed high sensitivity and high specificity for
identification of human diarrheagenic Escherichia coli (Toma et al. 2003).
The objective of the present study is to evaluate the multiplex PCR as a diagnostic tool for
different diarrheagenic Escherichia coli.
OBJECTIVES
General objective:
To evaluate the molecular technique for detecting different diarrheagenic Escherichia coli
strains by Multiplex PCR.
Specific objectives:
1. To isolate and identify Escherichia coli by culture and different biochemical tests.
2. To detect different diarrheagenic Escherichia coli strains by amplifying specific genes by
Multiplex PCR.
3. To determine the prevalence of different diarrheagenic Escherichia coli Strains and other
enteropathogens in the study population.
4. To find out antimicrobial sensitivity patterns of isolated strains.

REVIEW OF LITERATURE
Acute Infectious Diarrhea (AID) � A worldwide problem
Acute diarrhea is a clinical condition defined as an increased frequency of defecation (three
or more times per day or at least 200 g of stool per day ) lasting less than 14 days, may be
accompanied by nausea, vomiting, abdominal cramping, clinically significant systemic
symptoms, or malnutrition (Thieman et al. 2004; WHO, 2005). Acute infectious diarrhea
(AID) is a major cause of morbidity and mortality worldwide, and it remains a major public
health challenge especially in developing countries where it is a leading cause of death. Every
year nearly 1.4 billion episodes of AID occur in children less than 5 years of age in
developing countries, of which 123.6 million episodes require outpatient medical care and 9
million episodes require hospitalization (Kosek et al. 2003; Parashar et al. 2003). It has been
estimated that the mean number of episodes of diarrhea per year in children under 5 years of
age from a developing region is 3.2, with the highest incidence (4.8 episodes), occurring
during the first year of life, decreasing progressively to 1.4 episodes per year at 4 years of
age. Furthermore, the highest age-mortality rate (8.5 children per 1000/year) occurred in
children under 1 year of life (Kosek et al. 2003). In addition diarrheal illness account for an
estimated 12600 deaths each day in children under 5 years of age in Asia, Africa and Latin
America (Nguyen et al. 2005).
Kosek and associates (2003) calculated studies from 1990 to 2000 and concluded that
diarrhea accounts for 21% of all deaths at under five years of age causing 2.5 million deaths
per year in developing countries. Improvements in sanitation, nutrition, education and early
access to oral rehydration therapy among other measures have lowered the lethality of severe
AID from 4.6 million in 1982 to an estimated 1.5�2.5 million in 2010 (Black et al. 2010).
However, it remains the second most common cause of death in children under 5 years of age

worldwide according to the Global Burden Disease Report of the WHO (Kosek et al. 2003).
A diversity of recognized microorganisms such as bacteria, viruses and parasites can be
associated with severe AID in children (Al-Gallas et al. 2007; O'Ryan et al. 2005). Numerous
studies performed in different countries have reported diarrheagenic Escherichia coli (DEC)
as being the most frequent and important among bacterial pathogens associated with AID in
developing countries. However, the frequencies of these DEC vary with geographic region
and depend on the socioeconomic/sanitary conditions achieved (Black et al. 2010).
Altogether, they represent 30-40% of the cases (Albert et al. 1999), and about 15-30% have
required hospital care (Nataro & Karper 1998; O'Ryan et al. 2005).
In Bangladesh, the AID remains one of the most important health problems surpassed only by
the respiratory diseases. One third of the total child death burden is due to diarrhea. Every
year, a rural child suffers on average from 4.6 episodes of diarrhea, from which about
230,000 children die (Piechulek et al. 2003). Diarrheagenic Escherichia coli has been
reported to be responsible for 34% of diarrheal episodes in Bangladesh (ICDDR, B 2002).
ESCHERICHIA COLI
Escherichia coli (E. coli) is a Gram-negative, rod-shaped bacterium that is commonly found
in the lower intestine of warm-blooded animals. Most E. coli strains are harmless, but some
serotypes can cause serious food poisoning in humans (CDC 2011). The harmless strains are
part of the normal flora of the gut, and can benefit their hosts by producing vitamin K2, and
by preventing the establishment of pathogenic bacteria within the intestine (Reid et al. 2001).
E. coli and related bacteria constitute about 1% of gut flora (Eckburg et al. 2005), and fecal-
oral transmission is the major route through which pathogenic strains of the bacterium cause
disease. Cells are able to survive outside the body for a limited amount of time, which makes
them ideal indicator organisms to test environmental samples for fecal contamination (Feng
et al. 2002). The bacterium can also be grown easily and inexpensively in a laboratory
setting, and has been intensively investigated for over 60 years. E. coli is the most widely
studied prokaryotic model organism, and an important species in the fields of biotechnology
and microbiology, where it has served as the host organism for the majority of work with
recombinant DNA (Nataro & Karper 1998).
History The scientific history of Escherichia coli (E. coli) started with its first description in 1885 by
Theodor von Escherichia (Escherichia 1988; Gross & Rowe 1985), a pediatrician and
scientist, who in a series of pioneering studies of the intestinal flora of infants discovered a
normal microbial inhabitant of healthy individuals that he named Bacterium coli commune.
Its actual name became used and officially accepted in 1958, in his honor (Kuhnert et al.
2000).
Taxonomy
Domain: Bacteria, Kingdom: Bacteria, Phylum: Proteobacteria, Class: Gamma
Proteobacteria, Order: Enterobacteriales, Family: Enterobacteriaceae, Genus: Escherichia,
Species: Escherichia coli (Wikipedia 2008).
Structure of E.coli
The E. coli cell is about 1 ìm in diameter. It has a protective outer membrane and an inner
plasma membrane that encloses the cytoplasm and the nucleoid. Between the inner and outer
membranes is a thin but strong layer of peptidoglycans (sugar polymers cross-linked by
amino acids), which gives the cell its shape and rigidity. The plasma membrane and the
layers outside it constitute the cell envelope. Differences in the cell envelope account for the

different affinities for the dye Gentian violet, which is the basis for Gram's stain; gram-
positive bacteria retain the dye, and gram-negative bacteria do not (Nataro & Karper 1998;
Chakraborty, P 2003; Wikipedia 2011).
From the outer membrane of E. coli cells and some other eubacteria protrude short, hair- like
structures called pili, by which cells adhere to the surfaces of other cells. Strains of E. coli
have long peritrichous flagella, which can propel the bacterium through its aqueous
surroundings. Bacterial flagella are thin, rigid, helical rods, 10 to 20 nm thick. They are
attached to a protein structure that spins in the plane of the cell surface, rotating the flagellum
(Chakraborty, P 2003; Wikipedia 2011).
The cytoplasm of E. coli contains about 15,000 ribosomes, thousands of copies of each of
several thousand different enzymes, numerous metabolites and cofactors, and a variety of
inorganic ions. Under some conditions, granules of polysaccharides or droplets of lipid
accumulate. The nucleoid contains a single, circular molecule of DNA. Although the DNA
molecule of an E. coli cell is almost 1,000 times longer than the cell itself, it is packaged with
proteins and tightly folded into the nucleoid, which is less than 1 ìm in its longest dimension.
As in all bacteria, no membrane surrounds the genetic material. In addition to the DNA in the
nucleoid, the cytoplasm of most bacteria contains many smaller, circular segments of DNA
called plasmids. These nonessential segments of DNA are especially amenable to
experimental manipulation and are extremely useful to the molecular geneticist. In nature,
some plasmids confer resistance to toxins and antibiotics in the environment (Wikipedia
2011; Nataro & Karper 1998).
Biology and biochemistry
The species Escherichia coli comprises Gram-negative, rod-shaped, non-spore forming,
motile bacteria which are about 1 ìm in diameter, with a cell volume of 0.6-0.7 ìm3
(Darnton et al. 2007; Kubitschek 1990). They are facultative anaerobes, oxidase-negative,
glucose, lactose and sucrose fermenting, with an optimum growth pH of 6.0-7.0 and
temperature of 37°C. However, some laboratory strains can multiply at temperatures up to
49°C (Fotadar et al. 2005).
E. coli and related bacteria possess the ability to transfer DNA via bacterial conjugation,
transduction or transformation, which allows genetic material to spread horizontally through
an existing population. This process led to the spread of the gene encoding shiga toxin from
Shigella to E. coli O157:H7, carried by a bacteriophage (Brüssow et al. 2004).
Serotypes
In 1944, Kauffman proposed a scheme for the serologic classification of E. coli which is still
used in modified form today. According to the modified Kauffman scheme, E. coli are
serotyped on the basis of their O (somatic), H (flagellar), and K (capsular) surface antigen
profiles. Although more than 175 O antigens and 53 H antigens are currently recognized, the
number of serotype combinations responsible for diarrheal disease is small (Nataro & Karper
1998).
Genomes
The first complete DNA sequence of an E. coli genome was published in 1997. It was found
to be a circular DNA molecule 4.6 million base pairs in length, containing 4288 annotated
protein-coding genes, seven ribosomal RNA (rRNA) operons, and 86 transfer RNA (tRNA)
genes. Despite having been the subject of intensive genetic analysis for approximately 40
years, a large number of these genes were previously unknown. The coding density was

found to be very high, with a mean distance between genes of only 118 base pairs. The
genome was observed to contain a significant number of transposable genetic elements,
repeat elements, cryptic prophages, and bacteriophage remnants (Blattner et al. 1997).
Today, over 60 complete genomic sequences of Escherichia species are available.
Comparison of these sequences shows a remarkable amount of diversity; only about 20% of
each genome represents sequences that are present in every one of the isolates, while
approximately 80% of each genome can vary among isolates. The total number of different
genes among all of the sequenced E. coli strains (the pan-genome) exceeds 16,000. This very
large variety of component genes has been interpreted to mean that two-thirds of the E. coli
pan-genome originated in other species and arrived through the process of horizontal gene
transfer (Zhaxybayeva et al. 2011).
Virulence Factors
Several highly adapted strains have acquired virulence factors that allow them to cause
disease. In addition to structural properties that allow survival in the gastrointestinal tract
(Foster 2004), virulence factors include:
i. Adhesin / colonization factors (specific adherence factors that allow colonization of
atypical sites for E coli):
A) Fimbriae (pili) or fibrillae aid cell surface binding.
B) Outer membrane surface structures can trigger signal transduction pathways or
cytoskeletal rearrangements that can lead to illness.
C) Proteins that bind to cell surface receptors can trigger cytokine cascades (eg,

lipopolysaccharide, flagellin)
ii. Toxins (secreted toxins and other effectors proteins):
Heat-labile enterotoxin (LT) activates adenylate cyclase which eventually leads to chloride
secretion and diarrhea. LT-producing strains induce watery diarrhea among adults in Asia,
travelers to Central America, and children in several regions (Guerrant 1980; Guerrant 2005).
Heat-stable enterotoxin a (STa) activates guanylate cyclase that provokes ion secretion,
which leads to diarrhea. Heat-stable enterotoxin b (STb) activates intracellular calcium that
stimulates ion secretion, which leads to diarrhea (Guerrant 1980; Guerrant 2005).
Cytotoxins (Shiga-like toxin SLT-1, SLT-2) cause hemorrhagic colitis or hemolytic uremic
syndrome (HUS). SLT-1 is virtually identical to Shiga toxin, which is produced by Shigella
dysenteriae type 1 and SLT-2 also is very similar to the Shiga toxin molecule. SLT 1 or 2 are
encoded on a lambda-like bacteriophage; the ability to produce SLT was a key step in the
evolution of EHEC from EPEC (Reid 2000; Strockbine 1986).
iii. Type 2 secretion systems (T2SSs) :
T2SSs are comprised of about 12 proteins that form a piston-like structure for exporting
proteins and toxins across the outer membrane. These systems are encoded on pathogenicity
islands (segments of chromosomal DNA that are flanked by insertion or repeat elements)
or on plasmids (Clarke 2003 ; Lathem 2002).
iv. Type 3 secretion systems (T3SSs):
T3SSs contain genes encoding proteins that form a "molecular syringe" for injection of
bacterial proteins or toxins. As with T2SSs, these systems can be encoded on pathogenicity

islands or on plasmids (Donneberg 2005).
v. Plasmids:
Plasmids are genetic elements that can be transmitted between bacteria. They are not
virulence factors, but they can encode genes for a variety of factors that contribute to
pathogenesis, including antibiotic resistance, fimbriae, toxins, secretion systems, and invasion
factors. Transmission of plasmids plays a large role in the growing problem of antibiotic
resistance (Prats 2003).
Diarrheagenic Escherichia coli
The pathogenic E. coli species comprise a very versatile group with numerous virulence
determinants (virulence factors) including adhesins, invasins, toxins and secretion systems
that allow them to act as causative agents in both human and veterinary medicine (Kaper et
al. 2004; Nataro & Karper 1998). In human, these pathogens are responsible for three main
types of clinical infections: (i) enteric or diarrheal diseases, (ii) urinary tract infections, and
(iii) meningitis/septicemia. Based on their distinct virulence properties and clinical symptoms
of the host, pathogenic E. coli strains are divided into numerous categories or pathotypes:
Diarrheagenic Escherichia coli (DEC); Uropathogenic Escherichia coli (UPEC); Neonatal
meningitis/sepsis associated Escherichia coli (NMEC) (Dawson et al. 1999; Kaper et al.
2004).
Diarrheagenic Escherichia coli (DEC) belong to one of the most frequent, interesting and
widespread versatile pathogenic groups of bacteria that cause severe disease in human
(Campos et al. 2004; Nataro & Karper 1998). DEC has been divided into six well-
characterized subgroups or classes [enterotoxigenic E. coli (ETEC), enteropathogenic E. coli

(EPEC), verocytotoxin producing E. coli (VTEC) or enterohemorrhagic E. coli (EHEC),
enteroaggregative E. coli (EAEC), enteroinvasive E. coli (EIEC), diffusely adherent E. coli
(DAEC)] based on clinical manifestations, phenotypic traits, specific virulence properties,
and pathogenesis (Kaper et al. 2004; Nataro & Karper 1998).
Enterotoxigenic E. coli (ETEC)
ETEC is one of the most studied pathotypes of DEC. Most studies have demonstrated the
association of ETEC with diarrhea among infants less than five years of age (Aguero et al.
1985; Shaheen et al. 2004). Most of the illness, both in terms of number of cases and severity
of symptoms, occur in infants after weaning. Moreover, epidemiological studies have
implicated contaminated food and water as the most common vehicles of ETEC infection.
Thus, sampling of both food and water sources from endemic areas have demonstrated the
spread of ETEC bacteria in the community (Black et al. 1982). A high infectious dose
(ranging 106 to 1010 CFU) of ETEC has been demonstrated in human (Levine et al.1979;
Nataro & Karper 1998), and a large number of serogroups of ETEC have been associated
with diarrhea (Stenutz et al. 2006).
ETEC strains cause cholera-like watery diarrhea through the elaboration and action of LT
(heat-labile) and/or ST (heat-stable) enterotoxins. The ability of ETEC strains to produce
diarrheal illness by either or both of theses enterotoxins is what defines an ETEC (Nataro &
Karper 1998).
However, to cause diarrhea, by LT and/or ST, the ETEC must adhere and colonize the
intestinal mucosa. This is achieved by attaching with one or more colonization factor antigens
(CFAs), which are antigenically diverse and usually are encoded by plasmids (Nataro &
Karper 1998; Smith et al.1983). LTs of ETEC are oligomeric toxins that are functionally and
structurally related to the cholera toxin (CT) expressed by Vibrio cholerae, serogroups O1

and O139 (Sixma et al. 1993).
There are two types of LTs, LT-I and LT-II that are commonly found in human and animal
isolates. However, the term LT refers to LT-I, which is associated with disease in both human
and animals, while LT-II is expressed only in animals, but it is rarely associated to disease
(Nataro & Karper, 1998; Smith et al. 1983). LT-I is constituted by ~80% amino acid identity
with CT that consists of a single A subunit and five identical B subunits. The A subunit is
responsible for the enzymatic activity, and the B subunits are responsible for the toxin
binding to the cell surface ganglioside. After endocytosis the A subunit stimulates a series of
intracellular processes leading to increased level of cyclic adenosine monophosphate
(cAMP), resulting in an increased phosphorylation of chloride channels, and hence a reduced
absorption of NaCl. This increased extracellular ions content results in osmotic diarrhea.
Besides, there is an increased secretion of ions in the villi crypts (Nataro & Karper 1998).
STs are small peptides including two unrelated classes, STa and STb, which differ in
structure and mechanism of action. Genes for both classes � estA and estB � have been found
either on plasmids or on transposons. Only toxin of the STa class has been associated with
human and animal diseases. It has been established that the STa receptor is located on the
apical surface of enterocytes and that binding to the receptors leads to increased intracellular
cyclic guanidine monophosphate (cGMP) levels, which affects the electrolytic balance in a
similar manner as LT (Kaper et al. 2004; Nataro & Karper 1998). In contrast, STb is
primarily associated with diarrhea in piglets; however, some human ETEC isolates
expressing STb have been reported (Nataro & Karper 1998; Schulz et al. 1990). STb can
elevate cytosolic Ca+2 concentrations, stimulating both the release of prostaglandin E2 and
serotonin, which lead to increased ion secretion (Kaper et al. 2004; Nataro & Karper 1998).
The clinical features of ETEC diarrhea are constant with the pathogenic mechanisms of its

enterotoxins, and characterized by watery diarrhea without blood, mucus or pus, fever and
vomiting (DuPont 2009). The illness is typically abrupt, but can vary from mild, brief, and
self-limiting to a severe disease similar to in Vibrio cholerae infection (Levine et al. 1977).
Several studies have showed that the percentage of ETEC infection varies from 10 to 30%
and the clinical presentation, as with the other DEC varies among different geographical
areas (Mangia et al. 1993).
Enteropathogenic E. coli (EPEC)
EPEC was the first pathotype of DEC described, and associated to the infant diarrheal
diseases worldwide (Nataro & Karper 1998). The characteristic intestinal histopathology �
attaching and effacing (A/E) lesions - of EPEC are associated to striking cytoskeletal changes
in the epithelial cell. This ability to induce-attaching and effacing lesions is encoded by genes
for the adherence factor intimin (eae), a type II secretion system (TTSS) that includes the esc
genes and the translocated intimin receptor (Tir) (Nataro & Karper 1998) .These genes are
located on a 35-Kb (kilobase) pathogenicity island (PAI), called the locus of enterocyte
effacement (LEE), which is present in all EPEC and EHEC (McDaniel et al. 1995).
The A/E mechanism induce microvilli destruction, intimate adherence of bacteria to the
intestinal epithelium, pedestal formation, and aggregation of polarized actin and other
elements of the cytoskeleton at the site of bacterial attachment (McDaniel et al. 1995; Nataro
& Karper 1998). In addition, an EPEC virulence factor outside the LEE has also been
described (Trabulsi et al. 2002), which is located on a plasmid encoding a type pilus
called bundle forming pilus (bfp). Besides, on another plasmid there is a plasmid encoded
regulator gene (per) which regulates several chromosomal and plasmid genes necessary for
the pathogenesis of A/E lesions (Levine et al. 1985)).Beside the virulence factors described
above, there are other potential virulence factors such as EAST1 (enteroaggregative E. coli

heat-stable enterotoxin1), originally indentified in Enteroaggregative E. coli strains, but its
significance in pathogenesis is uncertain (Nataro &Karper 1998).
Based on these properties, two variants of EPEC � typical and atypical EPEC � have been
reported (Hien et al. 2007) and their prevalence seems to be different between developing and
developed countries. The typical EPEC is a cause of diarrhea in developing countries, while
atypical EPEC seems to be associated with diarrhea in developed countries (Afset et al.
2003).
The most special feature of the epidemiology of disease due to EPEC infection is the
remarkable age distribution. EPEC infection is primarily a disease of infants younger than 2
years of age. EPEC infection, as with other DEC pathotypes, takes place via the faecal-oral
route with contaminated food and water. The infectious dose among infants is not known, but
is presumed to be much lower than 108 CFU/microorganism (Nataro & Karper 1998).
The clinical features of EPEC infection are characterized by watery diarrhea, vomiting and
low-grade of fever. As compared to the developed countries, EPEC infection plays a more
important role in developing countries, where it has been found as one of the foremost causes
of diarrhea (Cravioto et al. 1988). EPEC may also cause diarrhea under other circumstances,
such as nosocomial outbreaks.
Enteroaggregative E. coli (EAEC)
EAEC was first described in 1985, recognized by its distinctive adherence to HEp-2 cells in
an aggregative, �stacked brick-like� pattern (Nataro et al. 1998; Pereira et al. 2008). This
adherence pattern, distinguishable from the adherence patterns manifested by EPEC and
DAEC, was first significantly associated with diarrhea among Chilean children in 1987
(Nataro et al. 1987). EAEC is defined as an E. coli pathotype that does not secrete heatlabile
or heat-stable enterotoxins but adheres to HEp-2 cells and other epithelial cells in an

aggregative adherence (A/A) pattern, the genes for which are encoded on plasmids (Nataro et
al. 1998).
Many epidemiological studies have used the A/A pattern and the plasmid-encoded probe
�CVD432� or simply the A/A probe to identify EAEC (Baudry et al. 1990). Moreover, a
transcription activator known as �AggR�, the gene which regulates the A/A genes has been
described as the major EAEC virulence regulator (Nataro 2005). Recently, some
epidemiological studies have suggested that CVD432-positive strains, which are predicted to
carry the AggR regulators, are the true EAEC pathogens termed �typical EAEC� (Harrington
et al. 2006). However, A/A probe negative isolates share virulence factors with A/A probe
positive isolates, a finding which indicates that additional factors are involved in the A/A
phenotype in these EAEC strains (Bouzari et al. 2001) .
The pathogenesis of EAEC is complex as the strains are relatively heterogeneous. However
three major features of the EAEC infections have been suggested as basic strategy of EAEC:
(i) abundant adherence to the intestinal mucosa (colonization), (ii) elaboration and secretion
of enterotoxins and cytotoxins, and (iii) induction of mucosal inflammation (Harrington et al.
2006; Nataro et al. 1998). Furthermore, several studies have reported the presence of fecal
lactoferrin and proinflammatory cytokines, notably interleukin (IL)-8 (Greenberg et al. 2002),
as well as the presence of a putative virulence factors, such as yersinia-bactin lectin (Basu et
al. 2004), in patients infected with EAEC.
Since its discovery, an increasing number of studies have associated EAEC with diarrhea in a
variety of settings. These include endemic diarrhea of infants in both industrialized and
developing countries (Elias et al. 1999), persistent diarrhea among acquired
immunodeficiency syndrome patients and traveler�s diarrhea (Jenkins et al. 2006). The
implication of EAEC in diarrheal outbreaks confirmed the fact that at least some strains
exhibiting the A/A phenotype were true human pathogens, yet not in all studies were EAEC

associated with diarrheal illness (Nataro et al. 1995). Pathogenesis studies of EAEC
experienced a step-forward in 1994, when the first EAEC volunteer study was published
(Nataro et al. 1995). In this report, it was showed that only one of four A/A probe positive
EAEC strains elicited human diarrhea, confirming that not all EAEC strains were equally
pathogenic.
Although not all EAEC strains have been associated to diarrheal disease, the most commonly
reported symptoms associated with EAEC infection are watery diarrhea with or without
blood and mucus, abdominal pain, nausea, vomiting, and low-grade fever (Adachi et al.
2002). Besides, EAEC can cause both an acute and a chronic (>14 days) diarrheal illness in
different parts of the world. A growing number of studies from both developing and
developed countries have supported the association of EAEC with persistent diarrhea in
young children and adults (Araujo et al. 2007). It has also been reported that EAEC may
be a leading cause of outbreaks of acute diarrheal disease affecting newborns and children
(Cohen et al. 2005). EAEC have been reported as the second most common bacterial
pathogen isolated in US adult travelers to developing countries and deployed US military
personnel (Adachi et al. 2002).
In another study on adult US travelers to Mexico that evaluated the serologic response to the
EAEC anti-aggregative protein dispersin, 48% of the travelers developed increases in
antibody levels over time; the majority of patients, though, remained asymptomatic (Huang et
al. 2008). These findings may possibly suggest that EAEC infection shows a variety of
clinical presentations and support the idea of a great heterogeneity of EAEC as a virulent
pathogen (Nataro et al. 1995).
Enterohemorrhagic E. coli (EHEC)
EHEC is an etiological agent of diarrhea with life-threatening complications. EHEC belongs

to a group of E. coli called VTEC (�verotoxigenic E. coli� or �Verocytotoxin-producing E.
coli�) or STEC (�Shiga toxin-producing E. coli), formerly SLTEC (�Shiga-like
toxinproducing E. coli�). EHEC colonize the intestinal mucosa inducing a characteristic
attaching and effacing (A/E) lesion, which is also present in EPEC and EAEC. The classic
intestinal histopathology characteristic of EHEC infection includes hemorrhage and edema in
the lamina propria, which results in bloody diarrhea, hemorrhagic colitis, necrosis and
intestinal perforation. The major virulence factor, and a defining characteristic of EHEC, is
the Shiga toxin (Stx), a potent cytotoxin that leads to cell death and will aggravate the
symptoms in patients infected (Nataro & Karper 1998).
Most studies have reported EHEC strains as important pathogens causing diarrhea, with
association to Hemorrhagic Colitis (HC) and Hemorrhagic Uremic Syndrome (HUS), which
are due to the interaction of Shiga toxin (Stx) with endothelial cells (Brown et al.1989). The
term �enterohemorrhagic E. coli� (EHEC) was originally created to denote strains that cause
HC and HUS, express Stx, cause A/E lesions on epithelial cells, and possess a plasmid
(Levine 1987). Thus, EHEC denotes a subset of STEC and includes a clinical connotation
that is not implied with STEC. Whereas not all STEC strains are believed to be pathogens, all
EHEC strains by the above definition are considered pathogens (Levine 1987).
The Stx family contains two major, immunologically non-cross-reactive, groups called Stx1
and Stx2. A single EHEC strain may express Stx1 only, Stx2 only, or both toxins or even
multiple forms of Stx2. Stx1 from EHEC is identical to Shiga toxin from Shigella dysenteriae
type I (Kaper et al. 2004).
EHEC is an emerging pathogen that has stimulated worldwide interest in several large food-
borne outbreaks. A wide variety of sources have been implicated in the EHEC transmission,
including beef, unpasteurized milk, fruit juice, and contaminated drinking water (Kaper et al.

2004). EHEC belongs to different serotypes or serogroups, which are useful for diagnostic
and epidemiological studies. The most notorious serogroups associated with EHEC is
O157:H7, which has caused several large outbreaks of the disease, mainly in North America,
Europe, and Japan (Ezawa et al. 2004).
Enteroinvasive E. coli (EIEC)
Like most enteropathogens, these bacteria may also be important pathogens in developing
countries where sanitation and hygiene levels have deteriorated. EIEC strains are
biochemically, genetically, and pathogenically closely related to Shigella spp., but produce
less severe diarrheal disease, compared to the dysentery caused by Shigella dysenteriae type
1 (Nataro & Karper 1998). The precise pathogenetic scheme of EIEC has yet to be
elucidated. However, pathogenesis studies of EIEC suggest that its pathogenic features are
virtually those of Shigella spp. (Sansonetti 1992). EIEC invades the colonic epithelial cell,
thereby inducing an inflammation and mucosal ulceration, leading to the release of blood and
mucus in the stool (Hart et al. 1993), similar to bacillary dysentery.
Although EIEC is the prototype of invasive bacteria, that are unable to penetrate enterocytes
via their luminal aspect. Instead, it passes through the M cells, which are antigen-sampling
cells that are a major constituent of the specialized epithelium overlying the lymphoid
follicles in the small and large intestine (Sansonetti 1992). The ability of EIEC to
penetrate, survive, and multiply within the colonic enterocytes is part of rearrangements of
the cell cytoskeleton, leading to disturbance and engulfment of the bacterium within a
vacuole, a process which is encoded by a cluster of genes carried on a large plasmid .
Afterwards, bacteria move through the cytoplasm and extent into adjacent epithelial cells
without being exposed to the external surroundings. Infection results in a shigellosis-like
syndrome in which patients exhibit abdominal pain, nausea, vomiting, fatigue, mucus, and

bloody stools, but many cases show signs of watery diarrhea that is indistinguishable from
that due to infection by other E. coli pathotypes (Nataro & Karper 1998).
Diffusely adherent E. coli (DAEC)
DAEC is a category of DEC that produces the diffuse adherence on Hep-2 cells (Nataro et
al. 1998) similar to those EAEC strains. However, little is know about the pathogenesis of
DAEC, but cells with a surface with fimbriae that mediate diffuse adherence have been
cloned and characterized (Kaper et al. 2004). Few epidemiological and clinical studies have
been carried out to adequately describe the epidemiology and clinical aspect of diarrhea
caused by DAEC. It was suggested that DAEC may cause disease in immunologically naïve
or malnourished infants. Furthermore, DAEC has been associated to diarrhea in infants older
than 1 year of age (Scaletsky et al. 2002).
Reservoirs
Reservoirs of most diarrheagenic E coli strains are humans, animals and contaminated food
or water (Cole 2006).
Transmission
Transmission of most diarrheagenic E coli strains occurs from consumption of food or water
contaminated with human or animal feces (Kaper 2004; Kassenborg 2004). For some
pathotypes, fewer than1000 colony forming units can cause disease; therefore, person-to-
person transmission from infected symptomatic people or asymptomatic carriers can be an
important mechanism for secondary spread (Belongia 1993; Russo 2006).
EHEC: Major modes of transmission include consumption of contaminated foods (especially
undercooked ground beef), exposure to contaminate recreational or drinking water, or contact
with farm and petting zoo animals (Kassenborg 2004). Person-to-person transmission most
often occurs in schools, long-term care institutions, families, and day-care centers (Belongia
1993; Bopp 2003).
EPEC: The major mode of transmission is person-to-person contact. Although outbreaks
among infants in industrialized countries have largely disappeared, atypical EPEC have
caused large outbreaks of diarrheal disease among children and adults in industrialized
countries (Nguyen 2006). Nosocomial outbreaks have been reported and have been
associated with person-to-person transmission as well as transmission via fomites and
contaminated formula or weaning foods (Nataro 1998).
ETEC: Transmission is primarily via consumption of fecally contaminated food or water
(Qadri 2005).
EIEC: Several foodborne outbreaks have been identified (Gordillo 1992). Person-to-person
spread also can occur.
EAEC: Several nosocomial outbreaks have been identified but the mechanisms of
transmission were not clear. Foodborne transmission has been suggested (Nataro 1998).
DAEC: Modes of transmission have not been clarified. Risk factors for infection include:
i. Consumption of contaminated food, especially undercooked ground beef
(Kassenborg 2004).
ii. Drinking or swimming in contaminated water
Laboratory Diagnosis
Diarrheagenic E. coli is diagnosed by serotyping from stool samples, enzyme immunoassay,

or by other molecular methods (Lopez-Saucedo 2003).
Diagnostic Tests
These pathotypes are identified by detection of their respective virulence-associated factors
(toxins, adherence, or invasiveness). Techniques for testing include bioassays (eg, cell
culture), immunologic assays (eg, immunoblotting or EIA), and DNA assays (eg, PCR,
colony blots).
Methods for identification of ETEC, EPEC, EIEC, DAEC, EHEC and EAEC generally are
available only in reference laboratories or research settings.
Diagnosis of diarrheagenic E coli is difficult for most clinical laboratories, because of the
difficulty in differentiating illness-causing organisms from the usual E. coli strains present in
stool (Voetsch 2004).
Detection of ETEC
Detection of ETEC has long relied on detection of the enterotoxins LT and/or ST. ST was
initially detected in a rabbit ligated ileal loop assay (Evans et al. 1973), but the expense and
lack of standardization caused this test to be replaced by the suckling-mouse assay (Gianella
1976), which became the standard test for the presence of STa for many years. The suckling-
mouse assay entails the measurement of intestinal fluid in infant mice after percutaneous
injection of culture supernatants.
Several immunoassays have been developed for detection of ST, including a
radioimmunoassay and an enzyme-linked immunosorbent assay (ELISA). Both of these tests
correlate well with results of the suckling-mouse assay and require substantially less expertise
(Cryan 1990).
The traditional bioassay for detection of LT involves the use of cell culture, either the Y1

adrenal cell assay or the Chinese hamster ovary (CHO) cell assay. In the Y1 assay, ETEC
culture supernatants are added to Y1 cells and the cells are examined for rounding. In the
CHO cell assay, LT will cause elongation of the CHO cells (Donta et al. 1974).
Immunologic assays are easier to implement in clinical laboratories and include the
traditional Biken test as well as newer immunologic methods such as ELISA, latex
agglutination and two commercially available tests, the reversed passive latex agglutination
test and the staphylococcal coagglutination test. Both of the commercially available tests are
reliable and easy to perform (Honda et al. 1981).
ETEC strains were among the first pathogenic microorganisms for which molecular
diagnostic techniques were developed. As early as 1982, DNA probes were found to be
useful in the detection of LT- and ST-encoding genes in stool and environmental samples.
Since that time, several advances in ETEC detection have been made, but genetic techniques
continue to attract the most attention and use. It should be stressed that there is no perfect test
for ETEC: detection of colonization factors is impractical because of their great number and
heterogeneity; detection of LT and ST defines an ETEC isolate, yet many such isolates will
express colonization factors specific for animals and thus lack human pathogenicity (Moseley
et al. 1981).
Several PCR assays for ETEC are quite sensitive and specific when used directly on clinical
samples or on isolated bacterial colonies. A useful adaptation of PCR is the �multiplex� PCR
assay, in which several PCR primers are combined with the aim of detecting one of several
different diarrheagenic E. coli pathotypes in a single reaction. After multiplex PCR, various
reaction products can usually be differentiated by product size, but a second detection step
(e.g., non-isotopic probe hybridization) is generally performed to identify the respective PCR
products definitively (Lang et a . 1995).

Detection of EPEC
There are two approaches to the detection of EPEC in the laboratory: phenotypic and
genotypic. The phenotypic approach requires the use of cell cultures and fluorescence
microscopy, and the genotypic method requires the use of DNA hybridization or PCR.
Phenotypic tests:
The A/E (attaching and effacing) phenotype can be identified by using cultured HEp-2 or
HeLa cells and the mushroom toxin phalloidin conjugated to rhodamine (available from
Sigma, Molecular Probes,) as described by Knutton and associates (2002).
The A/E phenotype can also be identified by electron microscopic examination of intestinal
biopsy specimens or of cultured epithelial cells incubated with EPEC.
There are a number of phenotypic tests to determine the other crucial characteristic of EPEC,
the lack of Stx expression. An excellent phenotypic marker for the presence of the EAF
(EPEC adhesive factor) plasmid is localized adherence on HEp-2 or HeLa cells. An ELISA
for the detection of EAF-positive EPEC, based on an antiserum raised against an EAF
plasmid containing strain and absorbed against a plasmid-cured strain (Albert et al. 1991).
There are no readily available immunoassays to detect the A/E pattern.
Genotypic tests:
DNA probes and PCR primers have been developed and evaluated for the three major
characteristics of EPEC: A/E, EAF plasmid, and lack of Shiga toxin.
Typical EPEC strains would possess the eae gene for A/E and the EAF probe or bfp
sequences, indicating the presence of the EAF plasmid. Atypical EPEC strains would possess
the eae gene only without the EAF plasmid.
(a) eae gene: Possession of eae sequences correlates with possession of the 35-kb LEE

pathogenicity island encoding A/E (McDaniel et al.1995). No exceptions to this
generalization have been reported, and so there is no need to test for other sequences in the
LEE such as espB and sep unless specific strain differences are sought for molecular
epidemiology purposes (Ebel et al. 1996).
A variety of eae primers for detecting this gene by PCR have been tested. As reported by
Gannon and associates (1997), primer pairs for the conserved 59 region amplified fragments
from all eae-positive strains whereas primers from the 39 end were specific for certain
serotype.
(b) EAF plasmid: The 1-kb EAF fragment probe originally described by Nataro and
associates (1998) is from a region of the EAF plasmid with an unknown function. This probe
may be used with non radioactive labeling techniques. A sensitive and specific
oligonucleotide probe consisting of 21 bases of the EAF fragment was developed by Jerse
and associates (1991). Franke and associates (1989) developed a PCR primer pair to amplify
a 397-bp region of the EAF probe.
The cloning of the bfpA gene allowed the development of DNA probes for specific plasmid-
encoded virulence factors. Giro´n and associates (1997) reported an 850-bp bfpA fragment
probe that was slightly more sensitive than the EAF probe; among EPEC strains exhibiting
localized adherence to HEp-2 cells, the bfpA and EAF probes hybridized with 99 and 96% of
the strains, respectively.
Detection of EHEC
There are three major categories of methods used to diagnose EHEC infections.
These are (i) isolation of E. coli O157 strains from stool samples, (ii) detection of Stx-
producing organisms or fecal Stx, and (iii) detection of elevated antibody levels to O157 LPS
or other EHEC antigens in serum.
Detailed protocols for many of these methods have been reviewed by Smith and Scotland

(Smith and Scotland 1993).
There are no common biochemical characteristics that are associated with the great majority
of EHEC serotypes. However, there are some biochemical characteristics of E. coli O157:H7
that have been exploited in the isolation and identification of this serotype. An important
characteristic is that O157:H7 strains do not ferment D-sorbitol rapidly, in contrast to about
75 to 94% of other E. coli strains. E. coli O157 strains also do not ferment rhamnose on agar
plates, whereas 60% of non-sorbitol-fermenting E. coli belonging to other serogroups ferment
rhamnose (Smith and Scotland 1993).
Culture techniques:
The agar medium most commonly used for the isolation of E. coli O157:H7 is SMAC agar
which is available from multiple commercial sources. This medium contains 1% sorbitol in
place of lactose in the standard MacConkey medium. Sorbitol-nonfermenting colonies,
indicative of E. coli O157:H7, are colorless on this medium. Multiple sorbitol-nonfermenting
colonies (at least 3 and up to 10) should be selected for testing as potential E. coli O157.
SMAC agar is not generally useful for Stx-producing E. coli strains of serotypes other than
O157:H7 because there is no known genetic linkage between Stx production and sorbitol
fermentation (Smith and Scotland 1993).
Immunoassays:
Most of the immunological assays currently available for EHEC detect either O and H
antigens or Stx. The available immunoassays for the O and H antigens are limited largely to
detecting EHEC expressing O157 LPS and the H7 flagellar antigen, whereas toxin
immunoassays are suitable for detecting both O157 and non-O157 serogroups of EHEC.
(i) O and H antigens: Colonies can be screened for the O157 LPS directly from SMAC agar
or after subculture, whereas screening for the H antigen may require passage through motility
medium before testing. Antisera to the O157 LPS and the H7 antigen have been incorporated

into a variety of diagnostic kits involving ELISA, latex reagents, colloidal gold-labeled
antibody, and other formats are available from numerous commercial sources. More
specialized reagents in which antibodies to O157 LPS are already conjugated to fluorescein,
peroxidase, or phosphatase are also available (Sowers et al. 1996).
Commercially available ELISA kits to detect E. coli O157 antigen directly in stool samples
offer testing times of less than 1 hour. These kits are accurate and easy to use in clinical
laboratory settings. Compared to a method involving colony sweeps and immunofluorescence
microscopy, this ELISA had a sensitivity of 91.2% and a specificity of 99.5%. Positive
results from this ELISA should be considered presumptive and should be confirmed by
culture, Stx tests, or PCR (Park et al . 1996).
(ii) Shiga toxins: Numerous immunological assays using various formats have been
developed for the detection of Stx and Stx-producing E. coli. These tests generally take less
than 1 h to complete and have the most potential to be adopted by clinical laboratories for
detection of non- O157:H7 EHEC (Nataro & Karper 1998).
An ELISA system to detect Stx1 and Stx2, which uses antibodies against Stx1 and Stx2 to
capture the antigen, has recently been developed by LMD Laboratories. Another test using a
Gb3 receptor capture system is the VeroTest (Nataro & Karper 1998).
DNA probes and PCR:
Most DNA probes and PCR techniques for EHEC are directed toward the detection of genes
encoding Stx. Frequent loss of stx genes upon subculture can also occur. For these reasons,
probes and PCR techniques for additional EHEC virulence factors can often provide crucial
information.
(i) Detection of stx genes: DNA fragment probes have been used in research studies for
nearly 10 years to detect EHEC. The use of fragment probes requires two different probes,

one for stx1 and one for stx2. With synthetic oligonucleotide probes, at least two probes are
usually used for stx1 and stx2 and additional probes specific for stx2c and stx2e are required
to detect strains containing these genes (Thomas et al. 1993).
The PCR technique has been extensively used to detect stx genes either in stx-only techniques
or in multiplex PCR techniques incorporating primers for eae, ehx, uidA, or fliC (Schmidt et
al. 1995).
(ii) Detection of eae genes: The same eae probes used to identify EPEC can also be used to
identify EHEC if they are derived from the highly conserved 59 end of the gene. The 1-kb
fragment probe described by Jerse and associates (1987) has been shown to be highly
sensitive and specific in many studies. Primers for eae have been combined with primers for
stx1 and stx2 in multiplex PCRs.
(iii) Detection of the pO157 plasmid/hemolysin gene: The pO157 plasmid is present in
nearly all O157:H7 strains and many other EHEC strains. A 3.4-kb fragment probe
empirically derived from this plasmid (called CVD419) was reported by Levine and
associates (1985). This probe has been extensively used to identify and characterize EHEC
strains despite the unknown function of the sequences contained on this fragment. This
fragment was subsequently shown to contain the ehxA (hlyA) genes encoding the EHEC
hemolysin. Oligonucleotide probes and PCR techniques to detect genes encoding the
hemolysin on the pO157 plasmid have also been developed (Thomas et al. 1993).
(iv) Detection of other genes: PCR techniques to detect the gene (fliC) encoding the H7
antigen have been developed. The fliC primer pair has also been combined with primers for
stx and eae in a multiplex PCR to allow the specific identification of E. coli O157:H7,
O157:NM, and other EHEC strains (Gannon et al. 1997).

Serodiagnosis:
Detection of a serum immune response is not usually used for the diagnosis of infections due
to other diarrheagenic E. coli strains, but serodiagnostic techniques can provide valuable
diagnostic information for EHEC infections, particularly since many cases of HUS are not
recognized until after fecal shedding of the organism has ceased. Unfortunately, there is no
single antigen that is ideal for use in serodiagnostic assays. Stx represents an obvious choice
for an important antigen produced in vivo (Nataro & Karper 1998).
Detection of EAEC
There are two major categories of methods used to diagnose EAEC infections.
1) Cell culture:
EAEC infection is diagnosed definitively by the isolation of E. coli from the stools and the
demonstration of the AA pattern in the HEp-2 assay (Fang et al. 1995).The HEp-2 assay
remains the gold standard for detection of EAEC. The presence of bacterial clusters in a
stacked-brick configuration should be used to identify EAEC strains.
The technique as first described by Cravioto and associates (1990) (i.e., a single 3-h
incubation of bacteria with cells, without a change in medium during the course of the assay)
is best able to discriminate the three patterns (AA, DA, and LA). It should also be stressed
that AAF adhesins are maximally expressed in static Luria broth cultures at 37°C.
ii) Molecular methods :
DNA probe: Baudry and associates (1990) selected a 1.0-kb plasmid-derived Sau3a fragment
that hybridized with a fragment of similar size from the 65-MDa plasmid of other strain. In
an evaluation of this fragment as a diagnostic probe, 56 of 63 (89%) EAEC strains (by HEp-2
assay) were positive with the EAEC probe by colony blot hybridization.
A PCR with oligonucleotide primers derived from the probe sequence has also been

developed. The sensitivity and specificity of the EAEC PCR are similar to those of the AA
probe (Schmidt et al. 1995).
Other tests for EAEC:
Several methods other than the HEp-2 and DNA probe assays have been described. Albert
and associates (1991) have reported that EAEC probe-positive organisms display an unusual
pellicle formation in Mueller-Hinton broth. Similarly, when EAEC strains are grown in
polystyrene culture tubes or dishes at 37°C overnight without shaking, a bacterial film is
produced on the polystyrene surface and is easily visualized with Giemsa stain (Nataro et al.
1985).
Detection of EIEC EIEC strains can be difficult to distinguish from Shigella spp. and from other E. coli strains,
including nonpathogenic strains. In general, identification of EIEC entails demonstrating that
the organism possesses the biochemical profile of E. coli, yet with the genotypic or
phenotypic characteristics of Shigella spp.
The classical phenotypic assay for EIEC identification is the Sereny (guinea pig
keratoconjunctivitis) test, which correlates with the ability of the strain to invade epithelial
cells and spread from cell to cell .The ability to form plaques in a HeLa cell monolayer also
correlates with these virulence characteristics (Menard et al. 1994).
Two polynucleotide probe for the detection of EIEC have been described. Probe ial is a 2.5-
kb fragment isolated from an EIEC strain. This probe is virtually 100% sensitive and specific
for EIEC strains that have retained their virulence. A 21-base oligonucleotide derived from
ial is identical in sensitivity and specificity to the polynucleotide probe (Small et al. 1986).
A PCR assay with primers derived from ial was able to detect as few as 10 CFU of S. flexneri
in stool without enrichment of the sample; this compares with 1,000 CFU detectable by DNA
probe. The ial PCR is also effective in a multiplex PCR system to identify EIEC strains

simultaneously with other E. coli categories (Frankel et al. 1989).
Pal and associates (1997) have developed an ELISA to detect the ipaC gene, which is
contained on the plasmid of EIEC. An advantage of this assay over other methods is that it
does not require costly or highly sophisticated equipment.
Detection of DAEC
DAEC strains are defined by the presence of the DA pattern in the HEp-2 adherence assay
(Schmidt et al. 1995). A 700-bp (base pair) polynucleotide fragment derived from the daaC
gene has been used as a DAEC DNA probe; daaC encodes a molecular fragment necessary
for expression of the F1845 fimbriae. Approximately 75% of DAEC strains from around the
world are positive with this F1845 gene probe. However, due to the genetic relatedness of
F1845 to other members of the family of adhesins, false-positive reactions with the DA probe
may occur (Nataro et al. 1996).
No PCR assay has yet been described to identify DAEC.
Antimicrobial Susceptibility
Antimicrobial resistance in E coli has been reported worldwide (Kuntaman 2005; Oteo 2005),
but pathogen occurrence and susceptibility profiles vary region to region (von Baum 2005).
In developing countries resistance levels are usually high for broad-spectrum penicillins and
trimethoprim and low for third-generation cephalosporins and nitrofurantoin (von Baum
2005).The emerging resistance to fluoroquinolones (Kuntaman 2005) and the production of
extended-spectrum beta-lactamases by multidrug resistant E coli strains (Oteo 2005) has
prompted much concern in the developing world, and has implications for developed nations
(Paton 2006). In a study of 3,174 healthy children in Bolivia and Peru, examination of fecal
carriage of drug-resistant E coli was high. Resistance rates were as follows: for ampicilin,

95%; trimethoprim-sulfamethoxazole, 94%; tetracycline, 93%; streptomycin, 82%; and
chloramphenical, 70%. Lower resistance rates were observed for nalidixic acid (35%),
kanamycin (28%), gentamicin (21%), and ciprofloxacin (18%) (Bartoloni 2006).
Treatment
Treatment is usually supportive. Patients who are dehydrated should receive oral
administration of solutions with electrolytes .Children who have inflammatory or bloody
diarrhea should not be given antimotility agents. Patients who have no laboratory evidence of
hemolysis, thrombocytopenia, or nephropathy 3 days after diarrhea resolves have a low risk
of HUS. Those who have hemorrhagic colitis should have careful follow-up (complete blood
cell count with smear, blood urea nitrogen concentration and creatinine levels) to detect
changes that suggest HUS (CDC 2004).
Antibiotic Therapy
Persons with travelers' diarrhea who develop three or more loose stools in an 8-hour period
(especially if associated with nausea, vomiting, abdominal cramps, fever, or blood in stools)
may benefit from antimicrobial therapy. Antibiotics usually are given for 3-5 days. Currently,
fluoroquinolones are the drugs of choice. Commonly prescribed regimens are 500 mg of
ciprofloxacin twice a day or 400 mg of norfloxacin twice a day for 3-5 days. Trimethoprim-
sulfamethoxazole and doxycycline are no longer recommended because of the high level of
resistance to these agents.. Patients suspected of having systemic infection should receive
parenteral antimicrobial therapy (CDC 2005).
Vaccines

No vaccines have been approved, but some vaccine candidates have advanced to clinical
trials and other experimental treatments are being developed.
Infection Control Recommendations
Patients with E coli infections should be managed with Standard Precautions. According to
CDC and the Hospital Infection Control Practices Advisory Committee (HICPAC), Contact
Precautions should be added when caring for diapered or incontinent children younger than
age 6 for the duration of illness (CDC/HICPAC 1996). Place the patient in a private room
or if a private room is not available, place in a room with a patient who has an active
infection with the same pathogen. At least 3 feet of spatial separation should be maintained
between the infected patient and other patients and visitors.
Gloves should be worn when entering the room and removed before leaving the room; hands
should be washed with an antimicrobial agent or waterless hand washing agent immediately
after removing gloves, and clean hands should not touch potentially contaminated items or
environmental surfaces. Gowns should be worn when entering the room if clothing will have
substantial contact with the patient, environmental surfaces, or items in the room; the gown
should be removed before leaving the patient's environment.
Patient transport should be limited to essential purposes only; if the patient is transported out
of the room, precautions should be maintained.
MATERIALS AND METHODS
Type of study:

Descriptive type cross sectional study.
Place of study:
Department of Microbiology, Mymensingh Medical College, Mymensingh.
Period of study:
The study was carried out from January 2011 to December 2011.
Subjects/ cases:
All patients with acute diarrhea irrespective of age and sex admitted in Mymensingh Medical
College Hospital and S.K hospital, Mymensingh were included in this study. Informed
consents were taken from each patient before his/her entry into the study. Information about
children and their consent were taken from their parents/guardians.
Case selection: Children, adult (male and female), with following criteria �
Inclusion criteria:
1) At least 3 times passage of loose stool or watery stool within 24 hours.
2) At least one time passage of bloody stool within 24 hours.
Exclusion criteria:
1) Chronic diarrhea (diarrhea more than 14 days).
Sample or specimen:
Stools were collected as specimen.
Method of collection:
Stool samples (10 mL of liquid or 10 gm of loose stool) were collected in a clean, leak-
proof, wide-mouth container (Cheesbrough 2010).
Sampling technique:
Non- probability purposive type of sampling.
Sample size:

Sample size was calculated by the following formula:
2
2
d
pqZn
n= Desired sample size
p= Prevalence of the disease/problem in community.
q= (1-p)
d= Degree of accuracy (it is, 0.05),
z= Confidence interval (usually we take 95%Ci, in which z =1.96)
According to the prevalence of diarrheagenic Escherichia coli in Bangladesh (34%)
minimum sample size is 344. But in our study sample size is 300 due to limitation of
resources and time.
Data collection instrument:
All relevant history, clinical findings and laboratory records of every case were
systematically recorded in a pre designed data sheet (appendix-I) for subsequent analysis by
computer programme SPSS version 16.0.
Laboratory procedure:
Culture of stool specimen (Isolation of bacteria):
All samples were inoculated into Mac Conkey�s agar (MCA), Salmonella-shegila agar and
Tri-citrate bile sugar media within 10 hours of collection and were incubated at 370C for 24
hours aerobically (Cheesbrough 2010).
Identification of bacteria:

The isolates were identified on the basis of colony morphology, Gram staining, motility and
following biochemical tests.
Grams staining: A drop of distilled water was taken on the centre of a clear glass slide and a
colony was emulsified by a sterilized inoculating loop to make a thin smear. A very thin
smear was made by spreading specimen uniformly. This smear was fixed by passing it over
the flame for two or three times. Smear was covered with crystal violet stain for 30 -60
seconds. Then stain was washed with distilled water and cover with Lugol�s iodine for 30-60-
seconds. Again stain was washed with distilled water and decolourize with acetone alcohol
and wash with distilled water .The back of the slide was wiped and place it in a draining rack,
for the smear to air dry .Test specimen was examined and compared with positive and
negative control under microscope (Cheesbrough 2011).
Motility test: Semisolid agar was used for this purpose. The organism was inoculated by
stabbing a straight wire carrying the inoculam once vertically in to the centre of the agar butt.
After over night inoculation motility was shown by a spreading turbidity from the stab line
or turbidity throughout the medium (Cheesbrough 2010).
Triple sugar iron agar (TSI): This medium was used for initial identification of gram
negative bacilli, particularly member of the Enterobacteriaecae. Three primary characteristics
of a bacterium detect by this medium include ability to produce gas, the production of
hydrogen sulfide gas and the ability to ferment carbohydrate (lactose, sucrose, glucose).To
inoculate a slope and butt medium, a few colonies from a pure culture were picked onto a
straight wire and inoculated to the medium by streaking the surface of the slant slope in a
zigzag pattern and stabbing the butt of the tube all the way to the bottom . This tube was
inoculated at 350C for overnight to observe the colour change of the slant and butt for
differentiation of Enterobacteriaecae ( Cheesbrough 2010).

Indole test: Indole production was tested for some bacteria, which has the ability to degrade
tryptophan to indole. Indole production was detected by Kavac�s reagent (4-dimethyl amino
benzaldehyde, isoamyl alcohol, hydrochloric acid). The test organism was cultured in
peptone broth which contains tryptophan. This broth was inoculated at 350C for overnight
and Kavac�s reagent was added. Development of red colour surface in the broth within 10
minutes indicates positive test (Cheesbrough 2010).
Citrate utilization test: Simon�s citrate agar medium was used for differentiating the
intestinal bacteria and other organism on the basis of citrate utilization .A very light inoculam
was picked with a straight wire and the organism was inoculated to the surface of Semmon�s
citrate agar slant. This tube was inoculated at 350C for overnight to observe the change of
color from light green to blue of the slant (Cheesbrough 2010).
Oxidase test: This test was used for differentiating the intestinal bacteria and other
organism on the basis of oxidase production. A piece of filter paper was placed in a clean
petridish and 2 or 3 drops of freshly prepared oxidase reagent (tetramethyl-p-phenylene
diamine dihydrochloride 10gm/l) was added. With a sterile glass rod 1 or 2 colonies of the
test organisms was taken and rubbed on the filter paper. Development of blue purple colour
within 10 seconds indicates positive test (Cheesbrough 2010).
(The interpretation of the biochemical tests is shown in tabulated form in appendix IV.)
Isolates of Escherichia coli were identified on the basis of pink colour , rounded colonies of
1 � 4 mm diameter in MacConkey�s agar. On Gram stained smear from colonies, those
appeared as Gram negative bacilli. Biochemically isolates were motile, Indole positive,
Citrate negative and Oxidase negative. On TSI, both butt and slunt were found as acidic
(yellow) with production of gas.
Maintenance and preservation of culture strains:
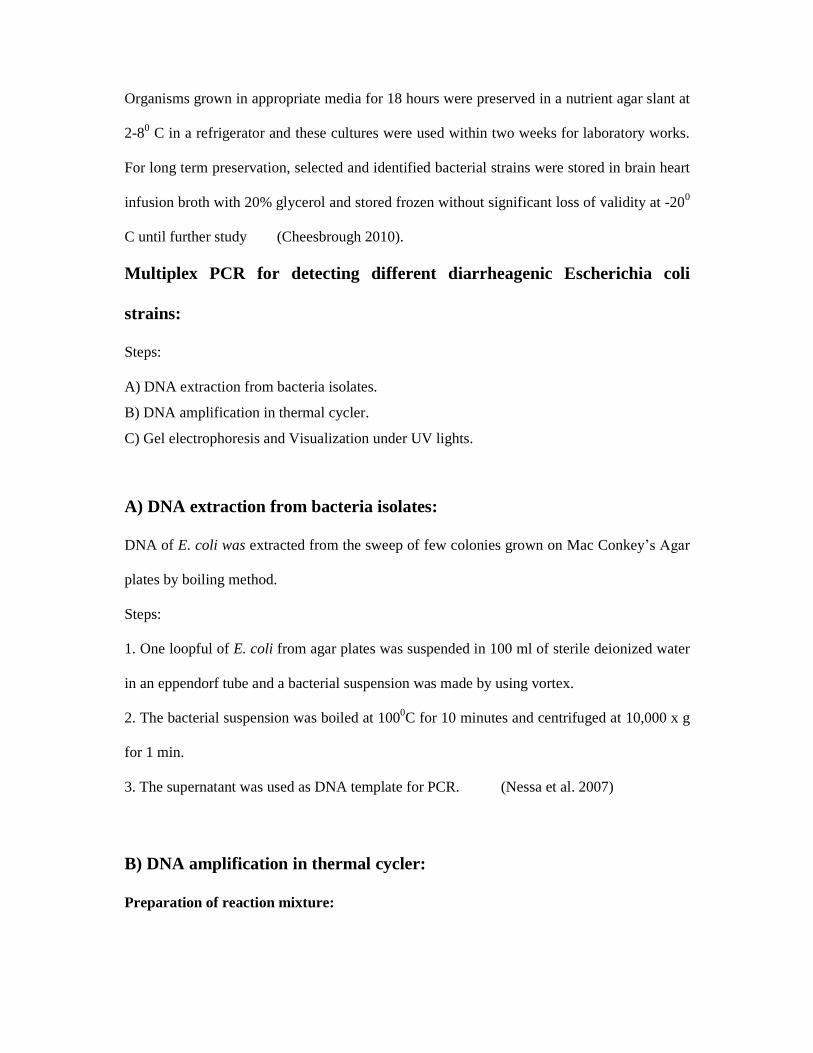
Organisms grown in appropriate media for 18 hours were preserved in a nutrient agar slant at
2-80 C in a refrigerator and these cultures were used within two weeks for laboratory works.
For long term preservation, selected and identified bacterial strains were stored in brain heart
infusion broth with 20% glycerol and stored frozen without significant loss of validity at -200
C until further study (Cheesbrough 2010).
Multiplex PCR for detecting different diarrheagenic Escherichia coli
strains:
Steps:
A) DNA extraction from bacteria isolates.
B) DNA amplification in thermal cycler.
C) Gel electrophoresis and Visualization under UV lights.
A) DNA extraction from bacteria isolates:
DNA of E. coli was extracted from the sweep of few colonies grown on Mac Conkey�s Agar
plates by boiling method.
Steps:
1. One loopful of E. coli from agar plates was suspended in 100 ml of sterile deionized water
in an eppendorf tube and a bacterial suspension was made by using vortex.
2. The bacterial suspension was boiled at 1000C for 10 minutes and centrifuged at 10,000 x g
for 1 min.
3. The supernatant was used as DNA template for PCR. (Nessa et al. 2007)
B) DNA amplification in thermal cycler:
Preparation of reaction mixture:

A total volume of 50 µl master mixture was prepared according to the following composition
(Toma et al. 2003).
Composition of master mixture for each reaction:
10x buffer 5 µl
dNTP (0.2mM each) 4 µl
Primer mixture (30 p mol concentration of each) 3 µl
Taq polymerase ( 2.5 U) 0.5µl
Nuclease free water 36.5µl
DNA template (sample) 1 µl
50 µl
Multiplex PCR was designed for the detection of target genes: eae for enteropathogenic E.
coli (EPEC), eae and stx for enterohemorrhagic E. coli (EHEC), ipaH for enteroinvasive E.
coli (EIEC), CVD432, aspU and aggR for enteroaggregative E. coli (EAEC) and elt and est
for enterotoxigenic E. coli (ETEC).
PCR primers used for detecting different Diarrheagenic Escherichia coli
strains:
Designation - Sequence (5 to 3) - Target gene - Amplicon size (bp) SK1 CCC GAA TTC GGC ACA AGC ATA AGC eae 881 SK2 CCC GGA TCC GTC TCG CCA GTA TTC G VTcom-u GAG CGA AAT AAT TTA TAT GTG stx 518 VTcom-d TGA TGA TGG CAA TTC AGT AT AL65 TTA ATA GCA CCC GGT ACA AGC AGG est 147 AL125 CCT GAC TCT TCA AAA GAG AAA ATT AC LTL TCT CTA TGT GCA TAC GGA GC elt 322 LTR CCA TAC TGA TTG CCG CAA T

ipaIII GTT CCT TGA CCG CCT TTC CGA TAC CGT C ipaH 619 ipaIV GCC GGT CAG CCA CCC TCT GAG AGT AC aggRks1 GTA TAC ACA AAA GAA GGA AGC aggR 254 aggRkas2 ACA GAA TCG TCA GCA TCA GC Eaggfp AGA CTC TGG CGA AAG ACT GTA TC CVD432 194 Eaggbp ATG GCT GTC TGT AAT AGA TGA GAA C spU-3 GCC TTT GCG GGT GGT AGC GG aspU 282 aspU-2 AAC CCA TTC GGT TAG AGC AC Amplification: The prepared PCR tubes with master mixture were placed in the eppendrof thermal cycler
(Eppendrof, Germany). Amplification was carried out according to the following thermal and
cycling condition:
95ºC (Initialization) 5 minutes,
95ºC (Denaturation) 1 minute
56ºC (Annealing) 1 minute 30 cycles
72ºC (Extension) 1 minute
72ºC (Final extension) 10 minutes ( Toma et al. 2003)
C) Gel electrophoresis and Visualization under UV lights:
Agarose gel electrophoresis:
The PCR products were analyzed after electrophoresis in 1.0% agarose gel to detect specific
amplified product by comparing with standard molecular weight marker (Toma et al. 2003).
Preparation of agarose gel:
One percent agarose gel was prepared by melting 2.0 gm agarose in 200 ml of diluted TBE
Buffer(Appendix iv) using a microwave woven. The melted agarose was allowed to cool to
about 50ºC and 20 µl ethidium bromide was mixed and shacked and was poured into gel tray
and combs were placed. After solidification of the gel, the comb was removed. During

electrophoresis, the gel was placed in a Horizontal electrophoresis apparatus containing TBE
buffer and ethidium bromide (Toma et al. 2003).
Loading and electrophoresis of the sample:
Five µl of amplified PCR product was mixed with 2.0 µl of loading buffer. The mixture was
slowly loaded into the well using disposable micropipette tips. Hundred bp molecular weight
marker was loaded in one well to determine the size of the amplified PCR products.
Electrophoresis was carried out at 100 volts for 35 minutes (Toma et al., 2003).
Visualization of the gel:
The amplified products of the study samples were visualized by trans-illuminator. And the
gel was photographed by a digital camera and transferred data to computer for further
documentation (Toma et al. 2003).
Antimicrobial susceptibility testing by disc diffusion method:
All the isolates were put into antibiotic susceptibility test by Kirby-Bauer disc diffusion
technique (Bauer et al., 1966) as per recommendation of CLSI, 2007. Panel of antibiotics
were used. All tests were performed on Muller-Hinton agar (appendix-II). The surface was
lightly and uniformly inoculated by cotton swab. Prior to inoculation, the swab stick was
dipped into bacterial suspension having visually equivalent turbidity to 0.5 McFarland
standards (Appendix-II).The swab stick was then took out and squeezed on the wall of the
test tube to discard extra suspension. Inoculated plates were incubated at 37 0C for 24 hours.
On the next day, plates were read by taking measurement of zone of inhibition. Results were
recorded and graded as Resistant (R) and Sensitive (S) according to the reference zone of
inhibition of particular antibiotic (CLSI, 2007). Known control strain ATCC, No. 25922 and
ATCC No. 25923 were used for quality control.
Antimicrobial agents used

A total of 10 antimicrobial agents were used for determining antibiogram of isolated
organisms according to Gram negative panel recommended by CLSI, 2007. Antibiotics:
Amoxycillin, Cephalexin, Ciprofloxacin, Gentamicin, Amikacin, Nalidixic acid, Ceftriazone,
Cotrimoxazole, Nitrifurantioin and Tetracyclin.
Detection of other enteropathogens :
Other enteropathgens were detected by standard laboratory methods and rotavirus were
detected by PACE (Appendix VI).
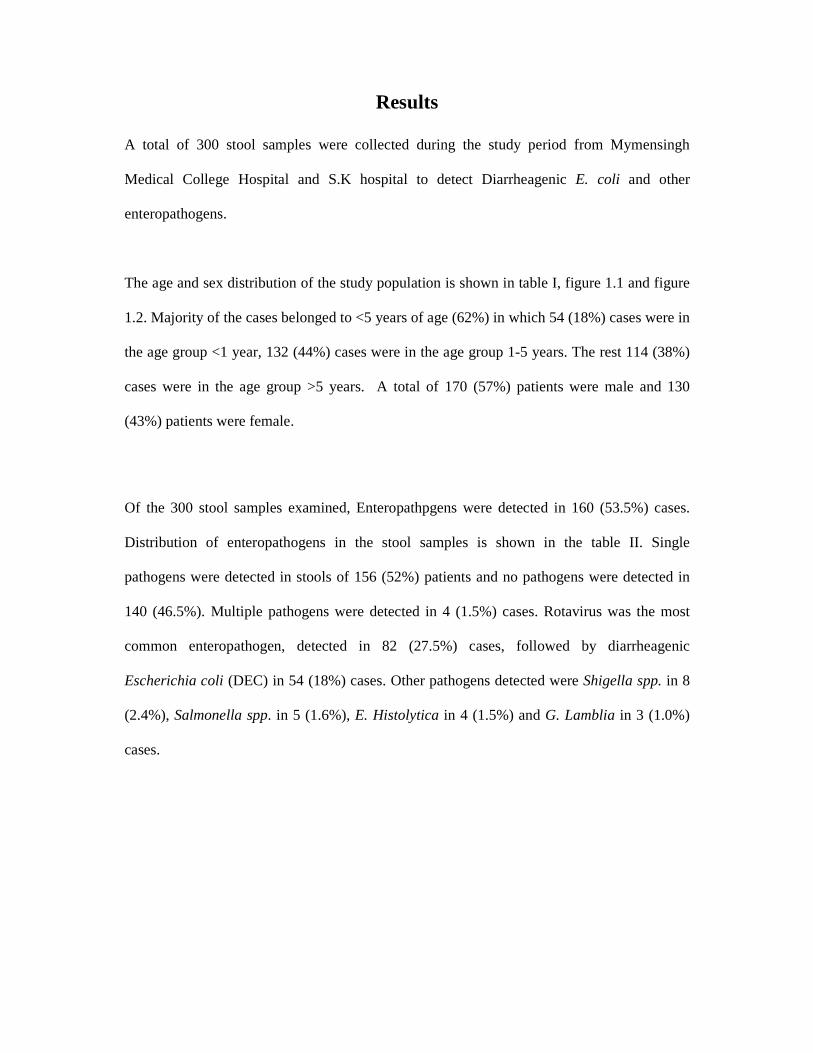
Results
A total of 300 stool samples were collected during the study period from Mymensingh
Medical College Hospital and S.K hospital to detect Diarrheagenic E. coli and other
enteropathogens.
The age and sex distribution of the study population is shown in table I, figure 1.1 and figure
1.2. Majority of the cases belonged to <5 years of age (62%) in which 54 (18%) cases were in
the age group <1 year, 132 (44%) cases were in the age group 1-5 years. The rest 114 (38%)
cases were in the age group >5 years. A total of 170 (57%) patients were male and 130
(43%) patients were female.
Of the 300 stool samples examined, Enteropathpgens were detected in 160 (53.5%) cases.
Distribution of enteropathogens in the stool samples is shown in the table II. Single
pathogens were detected in stools of 156 (52%) patients and no pathogens were detected in
140 (46.5%). Multiple pathogens were detected in 4 (1.5%) cases. Rotavirus was the most
common enteropathogen, detected in 82 (27.5%) cases, followed by diarrheagenic
Escherichia coli (DEC) in 54 (18%) cases. Other pathogens detected were Shigella spp. in 8
(2.4%), Salmonella spp. in 5 (1.6%), E. Histolytica in 4 (1.5%) and G. Lamblia in 3 (1.0%)
cases.

Table I. Age and sex distribution of the study population.
Age group (years)
Number of patients (%)
Male Female
<1 54 (18.00) 29 24
1-5 132 (44.00) 56 47
>5-15 76 (25.40) 43 38
>15-45 33 (11.00) 31 21
>45 05 (01.60) 11 0
Total 300 (100) 170 (57%) 130 (43%)

Figure 1.1. Age distribution of the study population.
Figure 1.2 . Sex distribution of the study population.

Table II. Distribution of enteropathogens in the stool samples.
Enteropathogen no. of patients Percentage
Rotavirus 82 27.5
Diarrheagenic Escherichia coli 54 18.0
Salmonella spp. 05 1.6
Shigella spp. 08 2.4
E.Histolytica 04 1.5
G.lamblia 03 1.0
Mixed pathogens 04 1.5
No pathogen identified 140 46.5
Total 300 100
Table III. shows distribution of DEC Strains in the study population. Enterotoxogenic E. coli
(ETEC) was detected in 39 (13%) cases and Enteroaggregative E. coli (EAEC) in 15 (5%)
cases. No Enterohemorrhagic E. coli (EHEC), Enteropathogenic E. coli (EPEC) and
Enteroinvasive E. coli (EIEC) could be detected.
Table IV. shows distribution different genes of ETEC Strains in the study population. Both
(ST and LT) genes of ETEC were detected in 26 (66.68%) strains, ST gene in 9 (23.07%)
strains and LT gene in 4 (10.25%) strains.

Table V. shows detection rate of Enterotoxogenic Escherichia coli (ETEC) in different age
group of the study population. Highest detection of ETEC 19 (6.34%) were in the age group
1-5 years, followed by age group >5 years 16 (5.33%) and 4 (1.33%) in the age group <1
year.
Table VI. shows detection rate of Enteroaggregative Escherichia coli (EAEC) in different
age group of the study population. Highest detection of EAEC 8 (2.70%) were in
the age group 1-5 years, followed by age group <1 year 5 (1.64%) and 2 (0.66%) in
the age group >5 years.
Table III: Distribution of different diarrheagenic Escherichia coli (DEC)
Strains in the study population (n=300).
Diarrheagenic Escherichia coli Number of cases (%).
ETEC 39 (13)
EAEC 15 (5)
EPEC 0 (0)
EIEC 0 (0)
EHEC 0 (0)
Total 54 (18)

Table IV: Distribution of different genes (ST / LT/ Both) of
Enterotoxogenic Escherichia coli (ETEC) strains in the study population.
Diarrheagenic
Escherichia
coli
Number of
strains
ST
gene (%)
LT
gene (%)
Both
(ST<)
genes (%)
ETEC 39 9(23.07) 4(10.25) 26(66.68)

Table V. Detection rate of Enterotoxogenic Escherichia coli (ETEC) in
different age group of the study population (n=300).
Age group
(years) Number of ETEC positive cases (%).
<1 04 (1.33)
1-5 19 (6.34)
>5-15 10 (3.33)
>15-45 06 (2.00)
>45 00 (00)
Table VI. Detection rate of Enteroaggregative Escherichia coli (EAEC) in
different age group of the study population (n=300).
Age group
(years) Number of EAEC positive cases(%).
<1 05 (1.64)
1-5 08 (2.70)
>5-15 02 (0.66)
>15-45 00 (00)
>45 00 (00)


Clinical features of Enterotoxogenic Escherichia coli (ETEC) in the study population are
shown in table VII. Watery diarrhea and vomiting were the chief complaint and were present
in 87% and 46% cases respectively. No cases were found with bloody stool. Fever occurred
in 64% of the infected patients. Clinical assessment for dehydration revealed some and severe
dehydration in 38% and 62% of the cases respectively.
Clinical features of Enteroaggregative Escherichia coli (EAEC) in the study population are
shown in table VII. Watery diarrhea and vomiting were the chief complaint and were present
in 80% and 60% cases respectively. No cases were found with bloody stool. Fever occurred
in 74% of the infected patients. Clinical assessment for dehydration revealed some and severe
dehydration in 20% and 80% of the cases respectively.
Table IX. shows antimicrobial susceptibility patterns of Enterotoxogenic E. Coli (ETEC)
isolated from the stool samples. ETEC isolated from the stool samples were 100% sensitive
to Ceftriaxone, Nitrofurantioin and Amikacin, 94% to Nalidixic acid, 89% to Gentamycin,
83% to Ciprofloxacin, 79% to Cephalexin, 46% to Tetracycline, 39% to Amoxycillin and
31% to Cotrimoxazole.
Table IX. shows antimicrobial susceptibility patterns of Enteroaggregative E. Coli (EAEC)
isolated from the stool samples. EAEC isolated from the stool samples were 100% sensitive
to Ceftriaxone, Nitrofurantioin, Amikacin and Nalidixic acid, 90% to Gentamycin and
Ciprofloxacin, 85% to Cephalexin, 41% to Amoxicillin, 49% to Tetracycline and 31% to
Cotrimoxazole.
Table VII: Clinical features of Enterotoxogenic Escherichia coli (ETEC) in
the study population.
Clinical features ETEC infected Cases (%).
Watery stool 34(87.17)
Loose stool 05(12.83)
Bloody stool 00(00)
Vomiting 18(46.15)
Fever 25(64.10)
No dehydration 00(00)
Some dehydration 15(38.46)
Severe dehydration 24(61.54)
Table VIII: Clinical features of Enteroaggregative Escherichia coli (EAEC)
in the study population.
Clinical features EAEC infected Cases (%).
Watery stool 12(80)
Loose stool 03(20)
Bloody stool 00(00)
Vomiting 09(60)
Fever 11(74)
No dehydration 00(00)
Some dehydration 03(20)
Severe dehydration 12(80)

Table IX: Antibiotic sensitivity patterns of Enterotoxogenic E. coli
(ETEC) isolated from the stool samples (n=39).
Antibiotic Number of ETEC strains sensitivity to
different antibiotics (%).
Ceftriaxone 39(100)
Amikacin 39(100)
Nitrofurantioin 39(100)
Nalidixic acid 36(94)
Gentamycin 34(89)
Ciprofloxacin 32(83)
Cephalexin 30(79)
Tetracycline 18(46)
Amoxycillin 15(39)
Cotrimoxazole 12(31)

Table X: Antibiotic sensitivity patterns of Enteroaggregative E. coli
(EAEC) isolated from the stool samples (n=15).
Antibiotic Number of EAEC strains sensitivity to
different antibiotics (%).
Ceftriaxone 15(100)
Amikacin 15(100)
Nalidixic acid 15(100)
Nitrofurantioin 15(100)
Ciprofloxacin 13(90)
Gentamycin 13(90)
Cephalexin 12(85)
Tetracyclin 7(49)
Amoxycillin 6(41)
Cotrimoxazole 5(31)

Discussion
Acute diarrhea is one of the most common illness and cause of death in young children in
Bangladesh. The present study to detect diarrheagenic Escherichia coli (DEC) is meaningful
in that it provides information about the prevalence of different diarrheagenic E. coli in the
study population.
In the present study, majority of the cases belonged to <5 years of age (62%) in which 54
(18%) cases were in the age group <1 year, 132 (44%) cases were in the age group 1-5 years.
The rest 114 (38%) cases were in the age group >5 years (Table I). Many studies have
reported that diarrhea is more common in children under 5 years of age in both developed and
developing countries (Antikainen et al. 2009). Albert and associates (1995) reported that 53%
of diarrheal patients were below 5 years of age in Bangladesh, which supports the present
study findings. Stoll and associates (1982) reported that most of the diarrheal patients were
children in Bangladesh: 20% were under 1 year of age, 42% between 1 and 5 years, 12%
between 5 and 15, and 26% were 15 and over, which also correlates with the present study
findings. In a recent study from Vietnam by Nguyen and associates (2005), it was found that
diarrhea was more frequent in children less than 5 years of age, which correlates with the
present study findings. Similar findings were reported in other study in Germany (Presterl et
al. 2003).
Out of 300 cases, 170 (57%) were male and 130 (43%) were female. The male and female
ratio was 1.32:1. These findings were similar with the study done by Albert and associates
(1999) where they found the male and female ratio was 1.42:1. Similar findings of male
dominance over female cases were reported in other study in Bangladesh (Strockbine et al
1992). The increase number of male patients over female irrespective of age in the present
study might be due to more exposure of male in the external environment and taking out-door

foods which has more chance to be contaminated by diarrheal pathogens (Nataro & Karper
1998).
Of the 300 stool samples examined, Enteropathpgens were detected in 160 (53.5%) cases.
Overall, Rotavirus was detected in 82 (27.5%) cases, followed by diarrheagenic Escherichia
coli (DEC) in 54 (18%), Shigella spp. in 8 (2.4%), Salmonella spp. in 5 (1.6%), Entamoeba
Histolytica in 4 (1.5%) and Giardia. Lamblia in 3 (1.0%) cases (Table II). The prevalence of
enteropathogens in the study population was lower compared to previous study carried out in
Bangladesh (ICDDR,B 2002) where they found association of enteropathogens with 81%
diarrheal diseases. In biological research some sorts of variation is not unexpected because it
depends upon some factors like age, seasonality, epidemicity, methods of samples collection
and tools used (Antikainen et al. 2009). Among bacterial pathogens, Campylobacter spp.,
Yersina spp. and Plesiomonas spp. and some recognized viral agents of diarrhea (enteric
adenovirus, Calici virus and astrovirus) were not sought in the present study due to resource
constraints.
In the present study, rotavirus (27.5%, 82/300) was the most predominant cause of acute
diarrhea in the study population. This finding for rotavirus infection was slightly lower than
similar study reported by ICDDR, B (ICDDR, B 2002) and slightly higher than other studies
done in Bangladesh (Paul et al. 2008; Baqui et al. 1992). The lower prevalence than ICDDR,
B might be due to use of different detection method (PAGE) in the present study.
Among the bacterial pathogens, diarrheagenic Escherichia coli (18%, 54/300) was the most
prevalent in the study population. The prevalence of DEC was lower compared to previous
studies carried out in Bangladesh. In 2002, it was reported that DEC was responsible for 34%
of diarrheal diseases in Bangladesh (ICDDR, B 2002). In 1999, Albert and associates (1999)
found that DEC was associated with 30% of diarrheal diseases in Bangladesh. All the above
study findings were higher than the present study findings. Various factors might be

responsible for such a difference. The samples collected were neither directly inoculated in
culture media nor transported by transport media, history of taking antibiotics before sample
collection and seasonality might be important factors to reduce the identification of DEC in
the study population (Stoll et al. 1982).
In Iraq, Sehand and associates (2010) and in Vietnum, Nguyen and associates (2005) found
DEC was responsible for 20% and 22.5% of diarrheal diseases respectively, which correlates
well with the present study findings.
Shigella spp. was found to be the second most bacteria in the present study and the detected
rate was 2.4% (8/300). In previous studies carried out in Bangladesh, Shigella spp. detection
rate varied from 2.6% to 12% in diarrheal patients (Albert et al. 1999; Stoll et al. 1982). The
isolation rate of Shigella spp. was highly variable from country to country which ranges from
1.6% in Ghana to 27% in Jardan (Youssef et al. 2001).
In the present study, the prevalence of Salmonella spp. was found to be 1.6% (5/300) which
was all most similar with the study findings reported by ICDDR, B in 2002 (ICDDR,B 2002).
Albert and associates (1995) found that Salmonella spp. was associated with 1.1% of
diarrheal disease in Bangladesh, which supports the present study results.
Among diarrheagenic parasites E . Histalytica and G. lamblia were found in 1.4% (4/300)
and 1.0% (3/300) cases in the present study respectively. Similar results were reported by
Albert and associates (1999) in Bangladesh. Recently it is reported that the prevalence of
diarrheagenic parasites is decreasing in Bangladesh (ICDDR, B 2003), it may be due to
improvement in sanitation, personal hygiene and safe water supply.
In the present study, among the diarrheagenic Escherichia coli (18%, 54/300),
Enterotoxogenic E. coli (ETEC) was detected in 39 (13%, 39/300) patients and
Enteroaggregative E. coli (EAEC) in 15 (5%, 15/300) patients (table III). No
Enterohemorrhagic E .coli (EHEC), Enteropathogenic E. coli (EPEC) and Enteroinvasive E.
coli (EIEC) could be detected. ETEC was found to be the most prevalent DEC in the study

population. ETEC has been attributed as a common diarrheal pathogen in children in many
developing countries of Asia, Africa and South America (Nguyen et al. 2005). In Bangladesh,
ETEC was reported as a cause of diarrhea with a prevalence of 14.0%, which correlates well
with the present study findings (Qadri et al. 2005). In 2002, it was reported that ETEC was
responsible for 12.7% of diarrheal diseases in Bangladesh, which was almost similar with the
present study findings (ICDDR,B 2002). Albert and associates (1999) showed that ETEC was
associated with 15.8% of diarrheal disease in Bangladesh, which supports the present study
results. Giron and associates (1995) and Stoll and associates (1982) found ETEC was
responsible for 19% and 20% of diarrheal diseases in Bangladesh respectively, which was
slightly higher than the present study findings.
Similar studies with acute diarrhea were performed in different parts of world. In Japan,
different types of diarrheagenic E. coli were the most frequently identified enteropathogens
(Toma et al. 2003). In Iran, Arif and associates (2010) and in Finland, Antikainen and
associates (2009) found ETEC was associated with 10% and 11% of diarrheal diseases
respectively, which correlates well with the present study findings. However in Thailand,
Hein and associates (2008) and in Vietnam, Nguyen and associates (2005) found ETEC was
associated with 5.8% and 4% of diarrheal diseases respectively, which was lower than the
present study findings. This might be due to important regional differences in the prevalence
of different categories of diarrheagenic E. coli (Albert et al. 1995).
EAEC (5%, 15/300) was the second most prevalent DEC in the present study population.
EAEC has been found as a common diarrheal pathogen in children in many developing
countries (Nguyen et al. 2005). In 2002, it was reported that EAEC was responsible for 6.1%
of diarrheal diseases in Bangladesh (ICDDR, B 2002). Albert and associates (1999) found
EAEC was associated with 6.9 % of diarrheal diseases in Bangladesh. In 1992, Faruque and

associates also found EAEC was responsible for 5.9% diarrheal diseases in Bangladesh. All
the above study findings correlate well with the present study findings.
EAEC has been implicated as the etiological agent of diarrhea not only in developing
countries but also as a cause of gastroenteritis outbreaks in some industrialized countries. It
was reported as the cause of a massive outbreak of gastrointestinal illness in school children
in Japan, as the cause of acute diarrhea in children in Brazil, and in other developed countries
(Smith et al.1997; Fang et al. 1995; Schmidt et al. 1995). In Iran, Arif and associates (2010)
foumd that EAEC was associated with 6.7% diarrheal diseases, which correlates with the
present study findings. However Rappelli and associates(2005) reported that EAEC was
responsible for 9.1% diarrheal diseases in Finland, which was higher than the present study
findings. In Vietnam, Nguyen and associates (2005) showed that EAEC was associated with
11% diarrheal diseases which was also higher than the present study findings. This might be
due to important regional differences in the prevalence of different categories of
diarrheagenic E. coli (Alert et al. 1995).
EPEC could not be detected in the present study population. The most important feature of
the diarrheal diseases due to EPEC infection is the remarkable age distribution. EPEC
infection is primarily a disease of infants younger than 1 year of age (Nataro & Karper 1998).
In the present study, only 18% cases were found in the age group below 1 year. Unicomb and
associates (1996) and Nessa and associates (2007) could not detect EPEC from any age group
in Bangladesh. However Baqui and associates (1992) and, Albert and associates (1995) found
EPEC in 8% and 12% cases respectively in Bangladesh.
In the present study, EIEC and EHEC could not be detected in the study population. In many
previous studies carried out in Bangladesh, EIEC and EHEC could not be detected in
diarrheal patients (Strockbine et al 1992; Albert et al. 1995: ICDDR, B 2002; Baqui et al.

1992)). The absence of these strains is not surprising since these pathotypes are not
frequently detected in developing countries of Africa and Asia (Rappelli et al. 2005).
In the present study, ST gene of ETEC was found in majority of cases compared to LT gene.
Out of 39 Enterotoxogenic Escherichia coli, both (ST and LT) genes of ETEC were detected
in 26 (67%) cases, ST gene in 9 (23%) cases and LT gene in 4 (10%) cases (Table IV).
Significant association with diarrhea was seen with ETEC producing both ST and LT and
ETEC producing only ST; ETEC producing only LT was not significantly associated with
diarrhea. This trend agrees with the findings in other studies in Bangladesh (Albert et al.
1995; Qudri et al. 2005). Similar findings were reported in other study in Finland (Antikainen
et al. 2009).
In the present study, highest detection of ETEC 19 (6.34%) were in the age group 1-5 years,
followed by age group >5 years 16 (5.33%) and 4 (1.33%) in the age group <1 year (Table
V). Majority of ETEC (8%) belonged to <5 years of age. It was reported that most of the
diarrheal patients infected with ETEC were <5 years of age in Bangladesh (ICDDR,B 2002).
Qudri and associates (2000) also reported that the most of the diarrheal patients infected with
ETEC were children <5 years of age in Bangladesh. All the above study findings were similar
with the present study findings.
Many studies have reported ETEC as a major agent of traveller�s diarrhoea in adults, and the
leading cause of child diarrhoea in both developed and developing countries (Antikainen et
al. 2009; Parashar et al. 2003). Those findings are correlated with the present study findings
as the high prevalence of ETEC was detected in child and adults in the present study
population.
In the present study, highest detection of EAEC 8 (2.70%) were in the age group 1-5 years,
followed by age group <1 year 5 (1.64%) and 2 (0.66% ) in the age group >5 years (Table 5).
Majority of EAEC (4.5%) belonged to < 5 years of age. Baqui and associates (1992) reported

that the most of the diarrheal patients infected with EAEC were children <5 years of age in
Bangladesh which agrees with the present study findings. Nessa and associates (2007) also
found association of EAEC mostly with diarrheal patients of <5 years of age in Bangladesh.
In a recent study from Japan by Nguyen and associates (2006), it was shown that EAEC was
more frequently associated with diarrhoea in children less than 5 years of age, which
correlates with the present study findings.
In the present study, Watery diarrhea and vomiting were the chief complaint and were present
in 87% and 46% respectively in patients infected with ETEC. No cases were found with
bloody stool. Clinical assessment for dehydration revealed some and severe dehydration in
38% and 62% of the cases respectively. Similar findings were reported in other studies in
Bangladesh (Stoll et al. 1982; Qudri et al. 2005). Jafari and associates (2008) also found
similar findings in Tehran.
In the present study Watery diarrhea and vomiting were the chief complaint and were present
in 80% and 60% respectively in patients infected with EAEC. No cases were found with
bloody stool. Clinical assessment for dehydration revealed some and severe dehydration in
20% and 80% of the cases respectively. Similar findings were reported in other study in
Bangladesh (Stoll et al., 1982; Albert et al. 1995). Presterl and associates (2003) also found
similar findings in Germany.
In the present study, detected ETEC were 100% sensitive to Ceftriaxone, Nitrofurantioin,
Amikacin, 94% sensitive to Nalidixic acid, 89% sensitive to Gentamycin, 83% sensitive to
Ciprofloxacin, 79% sensitive to Cephalexin, 39% sensitive to Amoxycillin, 46% sensitive to
Tetracyclin and 31% sensitive to Cotrimoxazole. Detected EAEC were 100% sensitive to
Ceftriaxone, Nitrofurantioin, Amikacin, Nalidixic acid, 90% sensitive to Gentamycin and
Ciprofloxacin, 85% sensitive to Cephalexin, 41% sensitive to Amoxycillin, 49% sensitive to
Tetracycline and 31% sensitive to Cotrimoxazole. Both ETEC and EAEC isolates exhibited

decreased susceptibility for Amoxycillin, Tetracycline and Cotrimoxazole. This trend agrees
with the findings in other study in Germany (Presterl et al. 2003). kalantar and associates
(2011) found similar type of results that supports the present study findings.
The prevalence of all the five categories of diarrheagenic E. coli was studied previously in
Bangladesh. However, these studies suffered from several deficiencies which included the
following: (i) not all categories of E. coli were sought in a single study, which resulted in
generation of data in a piecemeal fashion and (ii) some researchers relied on phenotype-based
tissue culture assay for aggregative E. coli, whose interpretation is prone to observer variation
(Strockbine et al. 1992; Albert et al. 1995). The present study overcomes all these
deficiencies and shows that multiplex PCR is a suitable method for DEC detection by
amplifying specific genes, where facilities are available.

Conclusion and Recommendations
Analyzing the findings of the present study, diarrheagenic Escherichia coli was found to be
one of the most important cause of acute diarrhea. Detection rate of diarrheagenic
Escherichia coli by multiplex PCR was quite satisfactory. Thereby, Multiplex PCR could be
adapted to detect different Diarrheagenic Escherichia coli in setup like Medical colleges or
tertiary medical facilities.

LIST OF REFERENCES
Adachi, JA, Jiang, ZD, Mathewson, JJ, Verenkar, MP, Thompson, S, Steffen, R, Ericsson,
CD and DuPont, H 2001, Enteroaggregative Escherichia coli as a major etiologic agent in
travelers, J Clin Microbiol, vol: 32, pp. 1706-1709.
Adachi, JA, Ericsson, CD, Jiang, Z D, Pallegar, SR and DuPont, HL 2002, Natural history of
enteroaggregative and enterotoxigenic Escherichia coli infection among US travelers to
Guadalajara, Mexico, J infect dis, vol. 185, pp. 1681-1683.
Afset, JE, Bergh, K and Bevanger, L 2003, High prevalence of atypical enteropathogenic
Escherichia coli (EPEC) in Norwegian children with diarrhea, J M Microbiol, vol. 52, pp.
1015-1019.
Aguero, ME, Reyes, L, Prado, V, Orskov, I, Orskov, F and Cabello, FC 1985,
Enterotoxigenic Escherichi coli in a Population of Infants with Diarrhea in Chile, J Clin
Microbiol, vol. 22, pp. 576-581.
Ahmed, A, Li, J and Shiloach, Y 2006, Safety and immunogenicity of Escherichia coli O157
O-specific polysaccharide conjugate vaccine in 2-5-year-old children, J Infect Dis, vol. 193,
no. 4, pp . 515-21.
Albert, MJ, Faruque, AS,G, Faruque, SM, Sack, B and Mahalian, D 1999, Case-Control
Study of Enteropathogens Associated with Childhood Diarrhea in Dhaka, Bangladesh ,J C
Microb, vol. 37, no. 11, pp. 3458-3464.
Albert, MJ, Faruque, SM, Ansaruzzaman, M, Bhuiyan, NA, Alam, K and Akbar, MS
1995, Controlled Study of Escherichia coli Diarrheal Infections in Bangladeshi Children, J
C Microb, vol. 33, no. 4, pp. 973�977.
Albert, MJ, Ansaruzzaman, M, Faruque, SM, Neogi , PK,B, Haider, K and Tzipori, S 1991,
An ELISA for the detection of localized adherent classical enteropathogenic Escherichia coli
serogroups, J Infect Dis, vol. 164, pp. 986�989.
Al-Gallas, N, Abbassi, SM, Hassan, AB and Aissa, RB 2007, Genotypic and phenotypic
profiles of enterotoxigenic Escherichia coli associated with acute diarrhea in Tunis, Tunisia,
Curr Microbiol ,vol. 55, pp. 47-55.
Ansaruzzaman, M, Bhuiyan, NA, Begum, YA, Kühn, I, Nair, B, Sack, DA, Svennerholm,
AM and Qadri, F et al. 2007, Characterization of enterotoxigenic Escherichia coli from
diarrhoeal patients in Bangladesh using phenotyping and genetic profiling, J Med Microb,
vol. 56, pp. 217-222.
Antikainen, J, Tarkka, E, Haukka, K, Siitonen, A, Vaara, M and Kirveskari, J 2009, New 16-
plex PCR method for rapid detection of diarrheagenic Escherichia coli directly from stool
samples, J Clin Microbiol Infect Dis, vol. 28, pp. 899�908.
Araujo, JM, Tabarelli, GF, Aranda, KU, Mendes, CM and Scaletsky, I C 2007, Typical
enteroaggregative and atypical enteropathogenic types of Escherichia coli are the most
prevalent diarrhea-associated pathotypes among Brazilian children, J Clin Microb, vol. 45,
pp. 3396-3399.
Armstrong, GD, Mulvey, GL and Marcat, P 2006, Human serum amyloid P component
protects against Escherichia coli O157:H7 Shiga toxin 2 in vivo: therapeutic implications for
hemolytic-uremic syndrome, J Infect Dis, vol. 193, no. 8, pp. 1120-1124.
Baqui, AH, Sack, RB, Black, RE, Haider, K, Hossain, A, Yunus, M, Chowdhury, HR and
Siddique, AK 1992, Enteropathogens Associated with Acute and Persistent Diarrhea in
Bangladeshi Children <5 Years of Age, J Infec Dis, vol. 166, pp. 792-796.
Baron, EJ, Peterson, LR and Fine-gold, SM 1994, Conventional and rapid microbiological
method for identification of bacteria and fungi, Bailey and Scott Diagnostic Microbiology,
11th edition , pp.374-379.
Bartoloni, A, Pallecchi, L and Benedetti, M 2006, Multidrug-resistant commensal
Escherichia coli in children, Peru and Bolivia, Emerg Infect Dis, vol. 12, no. 6, pp. 907-913.

Basu, S, Ghosh, S, Ganguly, NK and Majumdar, S 2004, A biologically active lectin of
enteroaggregative Escherichia coli, Biochimie, vol. 86, pp. 657-666.
Battistuzzi, FU, Feijao, A and Hedges, SB, 2004, A genomic timescale of prokaryote
evolution: insights into the origin of methanogenesis, phototrophy, and the colonization of
land, BMC Evolutionary Biology, vol. 4, pp. 44-56.
Bauer, AW, Kirby, WM, Sherris, JC and Turck, M 1996, Antibiotic susceptibility testing by a
standardized single disk method, Am J Clin Path, vol. 45, pp. 493 � 501.
Baudry, B, Savarino, SJ, Vial, P, Kaper, JB and Levine, M 1990, A sensitive and specific
DNA probe to identify enteroaggregative Escherichia coli, a recently discovered diarrheal
pathogen, J infect dis, vol. 161, pp. 1249-1251.
Belongia, EA, Osterholm, MT and Soler, JT 1993, Transmission of Escherichia coli O157:H7
infection in Minnesota child day-care facilities, JAMA, vol. 269, no. 7, pp. 883-888.
Bhan, MK, Raj, P, Levine, MM, Kaper, JB, Bhandari, N, Srivastava, R, Kumar, R and
Sazawal, S 1989, Enteroaggregative Escherichia coli associated with persistent diarrhea in a
cohort of rural children in India, J Infect Dis, vol. 159, no. 6, pp. 1061-1064.
Black, RE, Brown, KH, Becker, S, Alim, AR and Merson, MH 1982, Contamination of
weaning foods and transmission of enterotoxigenic Escherichia coli diarrhoea in children in
Bangladesh, Trans R Soc Trop Med Hyg, vol. 76, pp. 259-264.
Black, RE, Cousens, S, Johnson, HL, Lawn, JE, Rudan, I, Bassani, DG and Jha, P 2010,
Global, regional, and national causes of child mortality in 2008: a systematic analysis,
Lancet, vol. 375, pp. 1969-1987.
Blattner, FR, Plunkett, G, Bloch, CA, Riley, M, Collado-vides, J and Glasner, JD 1997, The
Complete Genome Sequence of Escherichia coli K-12, Science , vol. 277, no. 53, pp. 1453�
62.

Bopp, CA, Brenner, FW and Fields, PI 2003, Escherichia, Shigella and Salmonella, in
Murray, PR, Baron, EJ and Jorgensen, JH, Manual of clinical microbiology, 8th edition,
Washington, pp. 234-289.
Boschi-Pinto, C, Velebit, L and Shibuya, K 2008, Estimating child mortality due to diarrhoea
in developing countries. Bull World Health Organ, vol. 86, pp. 710-717.
Bouzari, S, Jafari, A, Azizi, A, Oloomi, M and Nataro, JP 2001, Short report: characterization
of enteroaggregative Escherichia coli isolates from Iranian children, Am J Trop Med Hyg,
vol. 65, pp. 13-14.
Branger, C, Zamfir, O and Geoffrey, S 2005, Genetic background of Escherichia coli and
extended-spectrum beta-lactamase type, Emerg Infect Dis , vol. 11, no. 1, pp. 54-61.
Breed, R and Conn, H 1936, The Status of the Generic Term Bacterium Ehrenberg 1828, J
bacteriol, vol. 31, no. 5, pp. 517�518.
Britannica 2011, Diversity of structure of Bacteria, viewed 12 September 2011,
<http://www.britannia.com/fact/s/5/463522/ E.coli, >.
Brown, JE, Echeverria, P, Taylor, DN, Seriwatana, J and Newland, J W 1989,
Determination by DNA hybridization of Shiga-like-toxin-producing Escherichia coli in
children with diarrhea in Thailand, J Clin Microbiol, vol. 27, pp. 291-294.
Brussow, H, Canchaya, C and Hardt, WD 2004, Phages and the evolution of bacterial
pathogens: from genomic rearrangements to lysogenic conversion, Microbiol MolBiol Rev,
vol. 68, no. 3, pp. 560�602.

Campos, LC, Franzolin, MR & Trabulsi, LR 2004, Diarrheagenic Escherichia coli categories
among the traditional enteropathogenic E. coli O serogroups, Memorias Do Instituto Oswaldo
Cruz , vol. 99, pp. 545-552.
Castellani, A and Chalmers, AJ 1919, Manual of Tropical Medicine, 3rd edition, Williams
Wood and Co., New York.
CDC 2011, Escherichia coli O157:H7, viewed 19 June 2011,
<www.cdc.gov/nczved/divisions/dfbmd/diseases/ecoli_o157h7/htm>.
CDC 2006, Advice for consumers on the multistate outbreak of E coli from fresh spinach,
viewed 11 July 2011, < www.cdc.gov/foodborne/ecolispinach/htm>.
CDC 2005, Compendium of measures to prevent disease associated with animals in
public settings, viewed 15 July 2011, <www.cdc.gov/mmwr
/preview/mmwrhtml/rr6004a1.htm>.
CDC 2004, Diagnosis and management of food borne illnesses: a primer for physicians and
other health care professionals, viewed 9 June 2011,
<www.cdc.gov/mmwr/preview/mmwrhtml/rr5304a1.htm>.
CDC 2005, Travelers� diarrhea, viewed 11 September 2011, <wwwnc.cdc.gov
/travel/yellowbook/2008/ch4/diarrhea.htm>.
CDC 2006, Update on multi-state outbreak of E. coli O157:H7 infections from fresh spinach,
viewed 12 July 2011,<www.cdc.gov/foodborne/ecolispinach/htm>.
CDC/HICPAC 1996, Recommendations for isolation precautions in hospitals, Am J Infect
Control, vol. 24, no. 1, pp. 24-52, viewed 19 July 2011,
<www..cdc.gov/wonder/prevguid/p0000419/entire.htm>.
Chakraborty, P 2003, A Text Book of Microbiology, 2nd edition, New Central Book
Agency (P) Ltd., 8/1 Chintamoni Das Lane, Kolkata, pp. 316-324.

Cheesbrough, M 2010, District laboratory practice in tropical countries, Cambridge
Editions, Cambridge University press, The Edinburgh Building, Cambridge,United Kingdom.
Cho, S, Bender, JB and Diez-Gonzalez, F 2006, Prevalence and characterization of
Escherichia coli O157 isolates from Minnesota dairy farms and county fairs, J Food Prot,
vol. 69, no. 2, pp. 252-9.
Clark, SG, Price, L and Ahmed, k 2003, Characterization of waterborne outbreak�associated
Campylobacter jejuni, Ontario, Emerg Infect Dis, vol. 9, no. 10, pp. 1232-4.
Clinical and Laboratory Standards Institute 2007, Performance standards for antimicrobial
susceptibility testing, Seventeenth Informational Supplement, M 100-S17.
Cohen, MB, Nataro, JP, Bernstein, DI, Hawkins, J, Roberts, N and Staat, MA 2005,
Prevalence of diarrheagenic Escherichia coli in acute childhood enteritis: A prospective
controlled study, J Pediatr, vol. 146, pp. 54-61.
Cole, D, Drum, DJ and Stallknecht, DE 2005, Free-living Canada geese and antimicrobial
resistance, Emerg Infect Dis J, vol. 11 , no. 6, pp. 935-8.
Cravioto, A, Reyes, RE, Fernandez, G, Hernandez, R and Lopez, D 1988, Prospective study
of diarrhoeal disease in a cohort of rural Mexican children: incidence and isolated pathogens
during the first two years of life, Epidemiology and infection, vol. 101, pp. 123-134.
Cravioto, A, Reyes, RE, De La Roca, JM, Hernandez, JM, Perez, G and Vazquez, V 1990,
Risk of diarrhea during the first year of life associated with initial and subsequent
colonization by specific enteropathogens, Am J Epidemiol, vol. 131, pp. 886-904.
Cryan, B 1990, Comparison of three assay systems for detection of enterotoxigenic
Escherichia coli heat-stable enterotoxin, J Clin Microbiol, vol. 28 pp. 792�794.
Darnton, NC, Turner, L, Rojevsky, S and Berg, HC 2006, On torque and tumbling in
swimming Escherichia coli, J Bacteriol, vol. 189, no. 5, pp. 1756�1764.

Dawson, KG, Emerson, JC and Burns, JL 1999, Fifteen years of experience with bacterial
meningitis, Infect dis J, vol. 18, pp. 816-822.
Donnenberg, MS 2005, Enterobacteriaceae, in Mandell, GL, Bennett, JE and Dolin R,
Mandell and Bennett's Principles and Practice of Infectious Diseases, 6th edition,
Philadelphia: Elsevier Churchill Livingstone, vol. 2, pp. 2567-86.
Donta, ST, Moon, HW and Whipp, SC 1974, Detection of heat-labile Escherichia coli
enterotoxin with the use of adrenal cells in tissue culture, Science , vol. 183, pp. 334�336.
DuPont, HL 2009, Clinical practice: Bacterial diarrhea, N Engl J Med, vol. 361, pp. 1560-
1569.
DuPont, HL, Formal, SB, Snyder, DG, LaBrec, E H and Kalas, J P 1971, Pathogenesis of
Escherichia coli diarrhea, N Engl J Med ,vol. 285, pp. 1-9.
Ebel, F, Deibel, AU, Kresse, CA, Guzman, A and Chakraborty, T 1996, Temperature- and
medium-dependent secretion of proteins by Shiga toxinproducing Escherichia coli, Infect
Immun, vol. 64, pp. 4472�4479.
Eckburg, PB, Bik, EM, Bernstein, CN and Purdom, E 2005, Diversity of the human
intestinal microbial flora, Science , vol. 308 , pp. 1635�1638.
Elias, WP, Suzart, S, Trabulsi, LR, Nataro, JP and Gomes, TA 1999, Distribution of aggA
and aafA gene sequences among Escherichia coli isolates with genotypic or phenotypic
characteristics, or both, of enteroaggregative E. coli, J Med Microbiol, vol. 48, pp. 597-599.
Escherich, T 1885, Die Darmbakterien des Neugeborenen und Säuglinge, Fortschr Med, vol.
3, pp. 515�522.

Escherich, T 1988, The intestinal bacteria of the neonate and breast-fed infant 1884, Rev
Infect Dis, vol. 10, no. 6, pp. 1220-5.
Evans, DJ and Evans DG, 1996, Escherichia coli in diarrheal disease, in Goldman, AS,
Prabhakar BS, Immunology overview, Chap 25, University of Texas Medical Branchat
Galveston.
Evans, DG, Evans, DJ and Pierce, NF 1973, Differences in the response of rabbit small
intestine to heat-labile and heat-stable enterotoxins of Escherichia coli, Infect Immun, vol. 7,
pp. 873�880.
Evans, DJ, and Evans, DG 1983, Classification of pathogenic Escherichia coli according to
serotype and the production of virulence factors, with special reference to colonization-factor
antigen, Rev Infect Dis , vol. 4, pp. 692-701.
Ezawa, A, Gocho, F, Saitoh, M, Tamura, T, Kawata, K, Takahashi, T and Kikuchi, N 2004,
A three-year study of enterohemorrhagic Escherichia coli O157 on a farm in Japan, J Vet
Med Sci ,vol. 66, pp. 779-784.
Fang, GD, Lima, AM, Martins, CV, Nataro, JP and Guerrant, LR 1995, Etiology and
epidemiology of persistent diarrhea in northeastern Brazil: a hospital-based, prospective,
case-control study, J Pediat. Gastroenterol Nutr, vol. 21, pp. 137�144.
Faruque, SM, Haider, K, Albert, MJ, Ahmad, S and Alam, N 1992, A comparative study of
specific gene probes and bioassays to identify diarrhoeagenic Escherichia co/I in paediatric
patients with diarrhoea in Bangladesh ,J Med Microbiol, vol. 36, pp. 37-40.
Feng, P, Weagant, S and Grant, M 2002, Enumeration of Escherichia coli and the Coliform
Bacteria, Bacteriological Analytical Manual, 8th edition, New York: Springer.
Foster, JW, 2004, Escherichia coli acid resistance: Tales of an amateur acidophile, Nat. Rev.
Microbiol, vol. 2, no. 11, pp. 898-907.

Fotadar, U, Zaveloff, P and Terracio, L 2005, "Growth of Escherichia coli at elevated
temperatures", J. Basic Microbiol. Vol.45, no.5, pp. 403�410.
Frankel, G, Giron, JA, Vlamossoi, J and Schoolnik 1989, Multi-gene amplification:
simultaneous detection of three virulence genes in diarrheal stool, Mol Microbiol, vol. 3, pp.
1729�1734.
Frenzen, PD, Drake, A and Angulo, FJ 2005, Economic cost of illness due to Escherichia
coli O157 infections in the United States, J Food Prot , vol. 68, no. 12, pp. 2623-30.
Galan, JE and Collmer, A 1999, Type III secretion machines: bacterial devices for protein
delivery into host cells, Science, vol. 284, no. 5418, pp. 1322-8.
Gannon, VP, D�Souza, JS, Graham, T, King, RK, Rahn, K and Read, S 1997, Use of the
flagellar H7 gene as a target in multiple PCR assays, J Med Microbiol, vol. 57, pp. 123-34.
George, Garrity, M 2005, The Gammaproteobacteria, Bergey's, Manual of Systematic
Bacteriology, 2nd edition, New York: Springer.
Germani, Y, Minssart, P, Vohito, M, Hocquet, D, Berthelemy, P and Morvan, J 1998,
Etiologies of acute, persistent, and dysenteric diarrheas in adults in Bangui, Central African
Republic, in relation to human immunodeficiency virus serostatus, Am J Trop Med Hyg ,vol.
59, pp. 1008-1014.
Gianella, RA 1976, Suckling mouse model for detection of heat-stable Escherichia coli
enterotoxin: characteristics of the model, Infect Immun , vol. 14, pp .95�99.
Girard, MP, Steele, D and Chaignat, CL 2006, A review of vaccine research and
development: human enteric infections, Vaccine, vol. 24, no. 15, pp. 2732-50.
Giron, JA , Gloria, I, Viboud, V, Oscra, G and Kaper, JP 1995, Prevalence and Association
of the Longus Pilus Structural Gene (lngA) with Colonization Factor Antigens, Enterotoxin

Types, and Serotypes of Enterotoxigenic Escherichia coli , infect and immun, vol. 63, no. 10,
pp. 4195�4198.
Gomes, TA, Toledo, RF, Trabulsi, RL, Wood, PK and Morris, JG 1987, DNA probes for
identification of enteroinvasive Escherichia coli, J Clin Microbiol, vol. 25, pp. 2025�2027.
Gomes, TA, Rassi, V, MacDonald, KL, Ivey, C and Toledo, MR 1991, Enteropathogens
associated with acute diarrheal disease in urban infants in Sao Paulo, Brazil, J infect Dis, vol.
164, pp. 331-337.
Gordillo, ME, Reeve, GR and Pappas, J 1992, Molecular characterization of strains of
enteroinvasive Escherichia coli O143, including isolates from a large outbreak in Houston,
Texas, J Clin Microbiol, vol. 30, no. 4, pp. 889-93.
Greenberg, DE, Jiang, ZD, Steffen, R, Verenker, MP and DuPont, HL 2002, Analysis of
incidence of infection with enterotoxigenic Escherichia coli in a prospective cohort study
of infant diarrhea in Nicaragua, J Clin Microb, vol. 35, pp. 1404-1410.
Gross, RJ and Rowe, B 1985, Escherichia coli diarrhea, J Hyg (Lond), vol. 95, pp. 531-550.
Guerrant, RL and Steiner, TS 2005, Principles and syndromes of enteric infection. in
Mandell, GL, Bennett, JE, Dolin, R, Douglas and Bennett's principles and practice of
infectious diseases, 6th edition, Philadelphia: Elsevier Churchill Livingstone, vol. 1, pp. 1215-
31.
Guerrant, RL, Rouse, JD and Hughes, JM 1980, Turista among members of the Yale Glee
Club in Latin America, Am J Trop Med Hyg , vol. 29, no. 5, pp. 895-900.
Hallander, H 1997, Analysis of incidence of infection with enterotoxigenic Escherichia coli
in a prospective cohort study of infant diarrhea in Nicaragua, J Clin Microbiol, vol. 35, pp.
1404-1410.

Hasan, KZ , Pathela, P, Alam, K, Podder, G, Faruque, SM and Roy, E 2006, Aetiology of
Diarrhoea in a Birth Cohort of Children Aged 0-2 Year(s) in Rural Mirzapur, Bangladesh, J
Healthpopul Nurt, vol. 24, no. 1, pp. 25-35.
Harrington, SM, Dudley, EG and Nataro, JP 2006, Pathogenesis of enteroaggregative
Escherichia coli infection, FEMS Microbiol Lett, vol. 254, pp 12-18.
Hart, CA, Batt, RM and Saunders, JR 1993, Diarrhoea caused by Escherichia coli. J Clin
Microbiol, vol. 75, pp. 404-419.
Hien, BT, Scheutz, F, Cam, PD, Serichantalergs, O, Huong and Dalsgaard, A 2008,
Diarrheagenic Escherichia coli and Shigella strains isolated from children in a hospital case-
control study in Hanoi, Vietnam, J Clin Microb, vol. 46, pp. 996-1004.
Hien, BT, Trang, d, Cam, PD, Molbak, K and Dalsgaard, A 2007, Diarrhoeagenic
Escherichia coli and other causes of childhood diarrhoea: a casecontrol study in children
living in a wastewater-use area in Hanoi, Vietnam, J Clin Microb, vol. 56, pp. 1086-1096.
Honda, T, Taga, S, Takeda, Y and Miwatani, T 1981, Modified Elek test for detection of
heat-labile enterotoxin of enterotoxigenic Escherichia coli, J Clin Microbiol, vol. 13, pp. 1�5.
Huang, DB and Dupont, HL 2004, Enteroaggregative Escherichia coli: an emerging pathogen
in children, Pediatr Infect Dis, vol. 15, pp. 266-271.
Huppertz, HI, Rutkowski, S, Aleksic, S and Karch, H 1997, Acute and chronic diarrhoea and
abdominal colic associated with enteroaggregative Escherichia coli in young children living
in western Europe, Lancet , vol. 349, pp. 1660-1662.
Ingledew, WJ and Poole, RK 1984, The respiratory chains of Escherichia coli, Microbiol
Rev, vol. 48, no. 3, pp. 222�71.

Ito, T, Kuwahara, S and Yokota, Y 1983, Automatic and manual latex agglutination tests for
measurement of cholera toxin and heat-labile enterotoxin of Escherichia coli, J Clin
Microbiol, vol. 17, pp. 7�12.
Itoh, Y, Nagano, I, Kunishima, M and Ezaki, T 1997, Laboratory investigation of
enteroaggregative Escherichia coli O untypeable: H10 associated with massive outbreak of
gastrointestinal illness, J Clin Microbiol, vol. 35, pp. 2546-2550.
ICDDR, B 2002, Trends in Aetiologies for Diarrhoeal Diseases, Health and Science Bulletin,
vol. 1, no. 1 , pp. 12-15.
Jafari, F, Shokrzadeh, L, Hamidian, M and Zali, MR 2008, Acute diarrhea due to
enteropathogenic bacteria in patients at hospital in Tehran, Jpn J Infect Dis, vol. 61, pp. 269-
273.
Jenkins, C, Chart, H, Willshaw, GA, Cheasty, T and Smith, HR 2006, Genotyping of
enteroaggregative Escherichia coli and identification of target genes for the detection of both
typical and atypical strains, Diagnostic Microbiology and Infectious Disease, vol. 55, pp. 13-
19.
Jerse, AE, and Kaper, JB 1991, The eae gene of enteropathogenic Escherichia coli encodes a
94-kilodalton membrane protein, the expression of which is influenced by the EAF plasmid,
Infect Immun, vol. 59, pp. 4302�4309.
Jertborn, M, Svennerholm, AM 1991, Enterotoxin-producing bacteria isolated from Swedish
travelers with diarrhea, Scand J Infect Dis, vol. 23, no. 4, pp. 473-479.
Jiang, ZD, Guo, DC, He, R, King, TM, DuPont, HL and Milewicz, DM 2003, Genetic
susceptibility to enteroaggregative Escherichia coli diarrhea: polymorphism in the
interleukin-8 promotor region, J Infect Dis, vol. 188, pp. 506-511.

Kalantar, E, Soheili, F, Salimi, H, Soltan, D and allal, MM 2011, Frequency, antimicrobial
susceptibility and plasmid profiles of Escherichia coli pathotypes obtained from children
with acute diarrhea, Jundishapur J Microbial , vol. 4, pp. 23-8.
Kaper, JB, Nataro, JP and Mobley, HL 2004, Pathogenic Escherichia coli, Nat Rev
Microbiol ,vol. 2, no. 2, pp. 123-40.
Karmali, MA 2004, Infection by Shiga toxin-producing Escherichia coli: an overview, Mol
Biotechnol, vol. 26, pp. 117-122.
Kassenborg, HD, Hedberg, CW and Hoekstra, M 2004, Farm visits and undercooked
hamburgers as major risk factors for sporadic Escherichia coli O157:H7 infection: data from
a case-control study in 5 FoodNet sites, J Clin Infect Dis, vol. 5, pp. 38-45.
Keen, JE, Wittum, TE and Dunn, JR 2006, Shiga-toxigenic Escherichia coli O157 in
agricultural fair livestock, United States, Emerg Infect Dis, vol. 12, no. 5, pp. 780-6.
Knutton, S, Shaw, R, Phillips, AD, Smith, HR, Willshaw, GA, Watson, P and Price, E 2001,
Phenotypic and genetic analysis of diarrhea-associated Escherichia coli isolated from
children in the United Kingdom, J Pediatr Gastroenterol Nutr, vol. 33, pp. 32-40.
Kopecko, DJ 1994, Experimental keratoconjunctivitis (Sereny) assay, pp. 39�46. in Clark,
VL and Bavoil, PM, Bacterial pathogenesis, part A, Academic Press, Inc, San Diego, Calif.
Kosek, M, Bern, C and Guerrant, RL 2003, The global burden of diarrhoeal disease, as
estimated from studies published between 1992 and 2000, Bull World Health Organ, vol. 81,
pp. 197-204.
Kubitschek, HE 1990, Cell volume increase in Escherichia coli after shifts to richer media, J
Bacteriol, vol. 172, no. 1, pp. 94�101.
Kucharzik, T, Hudson, JT, Ziegler, TR, Merlin, D, Madara, JL and Williams, IR 2005, Acute
induction of human IL-8 production by intestinal epithelium triggers neutrophil infiltration
without mucosal injury, Gut , vol. 54, pp. 1565-1572.

Kuhnert, P, Boerlin, P and Frey, J 2000, Target genes for virulence assessment of
Escherichia coli isolates from water, food and the environment, FEMS Microbiol Rev ,vol.
24, pp. 107-117.
Kuntaman, K, Lestari, ES and Severin, J 2005, Fluroroquinolone-resistant Escherichia coli,
Indonesia. Emerg Infect Dis, vol. 11, no. 9, pp. 1363-9.
Lang, AL, Tsai, YL, Mayer, CL and Palmer, CJ 1994, Multiplex PCR for detection of the
heat-labile toxin gene and Shiga-like toxin I and II genes in Escherichia coli isolated from
natural waters, Appl Environ Microbiol, vol. 60, pp. 3145�3149.
Lathem, WW, Grys, TE and Witkowski 2002, StcE, a metalloprotease secreted by
Escherichia coli O157:H7, specifically cleaves C1 esterase, Mol Microbiol, vol. 45, no. 2, pp.
277-88.
Lecointre, G, Rachdi, L, Darlu, P and Denamur, E 1998, Escherichia coli molecular
phylogeny using the incongruence length difference test, Molecular biology and evolution,
vol. 15,no. 12, pp. 1685�1695.
Leila, JF, Shokrzadeh, Hamidian, M and Zail, MR 2008, Acute Diarrhea Due to
Enterpathogenic Bacteria in Patients at Hospitals in Tehran, Jpn J Infect Dis, vol. 61, pp. 269-
273.
Levine, MM & Edelman, R 1984, Enteropathogenic Escherichia coli of classic serotypes
associated with infant diarrhea: epidemiology and pathogenesis, Epidemiol Rev, vol. 6, pp.
31-51.
Levine, MM 1987, Escherichia coli that cause diarrhea: enterotoxigenic, enteropathogenic,
enteroinvasive, enterohemorrhagic, and enteroadherent, J Infect Dis, vol. 155, pp. 377-389.
Levine, MM, Caplan, ES, Waterman, D, Hornick, RB and Snyder, MJ 1977, Diarrhea caused
by Escherichia coli that produce only heat-stable enterotoxin, Infect Immun, vol. 17, pp. 78-
82.
Levine, MM, Nalin, DR, Hoover, DL, Bergquist, EJ, Hornick, RB and Young, CR 1979,
Immunity to enterotoxigenic Escherichia coli, Infect Immun, vol. 23, pp. 729-736.
Levine, MM, Nataro, JP, Karch, H, Baldini, MM, Kaper, JB and Black, RE 1985, The
diarrheal response of humans to some classic serotypes of enteropathogenic Escherichia coli
is dependent on a plasmid encoding an enteroadhesiveness factor, J Infect Dis, vol. 152, pp.
550-559.
Long, KZ, Wood, JW, Cabada, FJ, DuPont, HL & Wilson, RA 1994, Proportional hazards
analysis of diarrhea due to enterotoxigenic Escherichia coli and breast feeding in a cohort of
urban Mexican children, Am J Epidemiol, vol. 139, pp. 193-205.
Lopez-Saucedo, C, Cerna, JF and Villegas-Sepulveda 2003, Single multiplex polymerase
chain reaction to detect diverse loci associated with diarrheagenic Escherichia coli, Emerg
Infect Dis, vol. 9, no. 1, pp. 127-31.
Mangia, AH, Duarte, AN, Duarte, R, Silva, LA, Bravo, VL and Leal, MC 1993, Markers of
inflammation in bacterial diarrhea among travelers, with a focus on enteroaggregative
Escherichia coli pathogenicity, J Infect Dis, vol. 185, pp. 944-949.
Mayatepek, E, Seebass, E, Hingst, A and Kroegeer 1993, Prevalence of enteropathogenic
and enterotoxigenic Escherichia coli in children with and without diarrhoea in Esteli,
Nicaragua, J Diarrhoeal Dis Res, vol. 11, pp. 169-171.

McDaniel, TK, Jarvis, KG, Donnenberg, MS and Kaper, JB 1995, A genetic locus of
enterocyte effacement conserved among diverse enterobacterial pathogens, J Infect Dis , vol.
46, pp. 69-81.
Menard, R and Sansonetti, PJ 1994, Shigella flexneri: isolation of noninvasive mutants of
gram-negative pathogens, Methods Enzymol, vol. 236, pp. 493�509.
Mendes, CM and Scaletsky, IC 2007, Typical enteroaggregative and atypical
enteropathogenic types of Escherichia coli are the most prevalent diarrhea-associated
pathotypes among Brazilian children, J Infect Dis, vol. 45, pp. 3344-3349.
Moseley, SL, Echeverria, P, Tirapat, C and Chaicumpa, W 1982, Identification of
enterotoxigenic Escherichia, J Infect Dis, vol. 18, pp. 44-49.
Müller, D, Greune, L, Heusipp, G, Karch, H, Fruth, A, Tschape, H and Schmidt, MA 2007,
Identification of unconventional intestinal pathogenic Escherichia coli isolates expressing
intermediate virulence factor profiles by using a novel single-step multiplex PCR, Appl
Environ Microbiol, vol. 73, pp. 3380-3390.
Nataro, JP and Karper, JB 1998, Diarrheagenic Escherichia coli, Clin Microbial Rev, vol. 11,
pp. 142-201.
Nataro, JP, Deng, Y, Cookson, S, Guers, LD, Levine, MM and Tacket, CO 1995,
Heterogeneity of enteroaggregative Escherichia coli virulence demonstrated in volunteers, J
Infec. Dis, vol. 171, pp. 464-469.
Nataro, JP, Scaletsky, IC, Kaper, JB, Levine, MM and Trabulsi, LR 1985, Plasmid-mediated
factors conferring diffuse and localized adherence of enteropathogenic Escherichia coli,
Infect Immun, vol. 48, pp. 378�383.
Nataro, JP, Kaper, JB, Robins-Browne, R, Prado, V, Vial, P and Levine, MM 1987, Patterns
of adherence of diarrheagenic Escherichia coli to HEp-2 cells, J Infect dis, vol. 6, pp. 829-
831.

Nataro, JP, Hicks, A and Sears, AR 1996, T84 cells in culture as a model for
enteroaggregative Escherichia coli pathogenesis, Infect Immun, vol. 64, pp. 4761�4768.
Nataro, JP, Steiner, T and Guerrant, RL 1998, Enteroaggregative Escherichia coli, Emerg
Infect Dis, vol. 4, pp. 251-261.
Nataro, JP 2005, Enteroaggregative Escherichia coli pathogenesis, Curr Opin Gastroenterol,
vol. 21, pp. 4-8.
Nessa, k, Dilruba, A, Islam, J, Kabir, L and Hossain, MA 2007 , Usefulness of a Multiplex
PCR for Detection of Diarrheagenic Escherichia coli in a Diagnostic Microbiology
Laboratory Setting, Bangladesh, J Med Microbiol, vol. 01, no. 2, pp. 38-42.
Nguyen, RN, Taylor, LS and Tauschek, M 2006, Atypical enteropathogenic Escherichia coli
infection and prolonged diarrhea in children, Emerg Infect Dis, vol. 12, no. 4, pp. 597-603.
Nguyen, TV, Le Van, P, Le Huy, C, Gia, KN and Weintraub, A 2005, Detection and
Characterization of Diarrheagenic Escherichia coli from Young Children in Hanoi, Vietnam,
J Clin Microbiol, vol. 43, no. 2, pp. 755�760.
Nguyen, TV, Le Van, P, Le Huy, C, Gia, KN and Weintraub, A 2006, Etiology and
epidemiology of diarrhea in children in Hanoi, Vietnam. J Infect dis, vol. 10, pp. 298-308.
Okeke, IN, Lamikanra, A, Dubovsky, F, Kaper, JB and Nataro, JP 2000, Heterogeneous
virulence of enteroaggregative Escherichia coli strains isolated from children in Southwest
Nigeria, J Infect Dis, vol. 181, pp. 252-260.
Orskov, I, Orskov, F, Jann, B and Jann, K 1977, Serology, chemistry, and genetics of O and
K antigens of Escherichia coli, Bacteriol Rev, vol. 41, pp. 667�710.
O'Ryan, M, Lucero, Y, O'Ryan-Soriano, MA and Ashkenazi, S 2010, An update on
management of severe acute infectious gastroenteritis in children, Expert Rev Anti Infect ,
vol. 8, pp. 671-682.

O'Ryan, M, Prado, V and Pickering, LK 2005, A millennium update on pediatric diarrheal
illness in the developing world, Semin Pediatr Infect Dis, vol. 16, pp. 125-136.
Oteo, J, Lazaro, E, and Abajo FJ, 2005, Antimicrobial-resistant invasive E.coli in Spain,
Emerg. Infect. dis, vol. 11, pp. 546-553.
Pal, T, Al-Sweith, NA, Herpay, M and Chugh, TD 1997, Identification of enteroinvasive
Escherichia coli and Shigella strains in pediatric patients by an IpaC-specific enzyme-linked
immunosorbent assay, J Clin Microbiol, vol. 35, pp. 1757�1760.
Paniagua, M, Espinoza, F, Ringman, M, Reizenstein, E, Svennerholm, AM and Hallander, H
1997, Analysis of incidence of infection with enterotoxigenic Escherichia coli in a
prospective cohort study of infant diarrhea in Nicaragua, J Clin Microbiol, vol. 35, pp.
1404�1410.
Parashar, UD, Hummelman, E, Bresee, JS, Miller, MA and Glass, RI 2003, Global illness
and deaths caused by rotavirus disease in children, Emerg Infect Dis , vol. 9, pp. 565-572.
Park, CH, Gates, KM, Vandel, NM and Hixon, DL 1996, Isolation of Shiga-like toxin
producing Escherichia coli (O157 and non-O157) in a community hospital, Diagn Microbiol
Infect Dis, vol. 26, pp. 69�72.
Paton, AW, Morona, R and Paton, JC 2006, Designer probiotics for prevention of enteric
infections, Nat Rev Microbiol, vol. 4, no. 3, pp. 193-200.
Pereira, AC, Britto-Filho, JD, Jose de Carvalho, J, de Luna, MG and Rosa, AC 2008,
Enteroaggregative Escherichia coli (EAEC) strains enter and survive within cultured
intestinal epithelial cells, Microb Pathog, vol. 45, pp. 310-314.
Piechulek, H, Al-Sabbir, A and Mendoza-Aldana, J 2003, Diarrhea and ARI in rural areas of
Bangladesh, J Trop Med, vol. 34, no. 2, pp. 337-342.
Prats, G, Mirelis, B and Miro, E 2003, Cephalosporin-resistant Escherichia coli among
summer camp attendees with salmonellosis, Emerg Infect Dis , vol. 9, pp. 1273-80.

Presterl, E, Zwick, RK, Reichiman, S and Alcheburg, A 2003, Frequency and virulence
properties of diarrheagenic Escherchia coli in children with diarrhea in Gabon, J Trop Med
Hyg, vol. 69, no. 4, pp. 406�410 .
Qadri, F, Ashraful, IK, Syed, A, Faruque, G, Begum, YA, Chowdhury, F and Svennerholm,
AM 2005, Enterotoxigenic Escherichia coli and Vibrio cholerae Diarrhea, Bangladesh, 2004,
Emerg infect dis, vol. 11, no. 7, pp.1104-1006.
Qadri, F, Das, SK, Faruque, G, Fuchs, J, Albert, MJ and Svennerholm, AM 2000,
Prevalence of Toxin Types and Colonization Factors in Enterotoxigenic Escherichia coli
Isolated during a 2-Year Period from Diarrheal Patients in Bangladesh, J Med Microbiol, vol.
38, no. 1, pp. 27�31.
Qadri, F, Svennerholm, AM and Faruque, AS 2005, Enterotoxigenic Escherichia coli in
developing countries: Epidemiology, microbiology, clinical features, treatment, and
prevention, Clin Microbiol, vol. 3, pp. 465-483.
Rappelli, P, Folgosa , E, Solinas , ML, DaCosta , JL and Colombo, MM 2005, Pathogenic
enteric Escherichia coli in children with and without diarrhea in Maputo, Mozambique ,
FEMS Immun and Medical Microbiol, vol. 43, pp. 67�72.
Reid, G, Howard, J and Gan, BS 2001, Can bacterial interference prevent infection, Trends
Microbiol, vol. 9, pp. 424�428.
Reid, SD, Herberin, CJ and Bumbaugh, AC 2000, Parallel evolution of virulence in
pathogenic Escherichia coli, Natur , vol. 406, pp. 64-67.
Rivera, FP, Ochoa, TJ, Medina, AM, Meza, R, Gil, A, Huicho, L and Lanata, CF 2010,
Genotypic and phenotypic characterization of enterotoxigenic Escherichia coli (ETEC)
strains isolated from Peruvian children, J Clin Microbiol, vol. 78, pp. 404�410.

Robins-Browne, RM and Hartland, EL 2002, Escherichia coli as a cause of diarrhea, J Gastro
and Hepato, vol. 17, pp. 467-475.
Russo TA 2006, Diseases caused by gram-negative enteric bacteria, J Clin. Microbiol, vol.
13, pp. 1�5.
Sansonetti, PJ 1992, Molecular and cellular biology of Shigella flexneri invasiveness: from
cell assay systems to shigellosis, Curr Top Microbiol Immunol, vol. 180, pp. 1-19.
Scaletsky, IC, Fabbricotti, SH, Aranda, KR, Morais, MB and Neto, U 2002, Comparison of
DNA hybridization and PCR assays for detection of putative pathogenic enteroadherent
Escherichia coli, J Clin Microbiol, vol. 40, pp. 1254-1258.
Schmidt, H, Knop, C, Franke, S, Aleksic, S, Heeseman, J and Karch, H 1995, Development
of PCR for screening of enteroaggregative Escherichia coli, J Clin. Microbiol, vol. 33, pp.
701�705.
Schmidt, H, Beutin, L, and Karch, H 1995, Molecular analysis of the plasmid-encoded
hemolysin of Escherichia coli O157:H7 strain EDL 933, Infect Immun, vol. 63, pp. 1055�
1061.
Schulz, S, Green, CK, Yuen, PS and Garbers, DL 1990, Guanylyl cyclase is a heatstable
enterotoxin receptor, Cell, vol. 63, pp. 941-948.
Sehand, K, Arif and Salih, FL 2010, Identification of Different Categories of Diarrheagenic
Escherichia coli in Stool Samples by Using Multiplex PCR Technique, Asian J M Scien, vol.
2, pp. 237-243.
Shaheen, HI, Messih, A and Wierzba 2009, Phenotypic and genotypic analysis of
enterotoxigenic Escherichia coli in samples obtained from Egyptian children presenting to
referral hospitals, J Clin Microbiol, vol. 47, pp. 189-197.

Shaheen, HI, Khalil, SB, Rao, MR, Wierzba, TF, Peruski, LF and Putnam 2004, Phenotypic
profiles of enterotoxigenic Escherichia coli associated with early childhood diarrhea in rural
Egypt, J Clin Microbiol, vol.42, pp.588-596.
Sixma, TK, Kalk, KH, van Zanten, BA, Kingma, J, Witholt, B and Hol, W 1993, Refined
structure of Escherichia coli heat-labile enterotoxin, a close relative of cholera toxin, J Mol
Biol, vol. 230, pp. 890-918.
Small, PL and Falkow, S 1986, Development of a DNA probe for the virulence plasmid of
Shigella spp. and enteroinvasive Escherichia coli, pp. 121�124. in . Leive, L, Bonventre, PB,
Silver, SD and Wu, WC, Microbiology�1986, American Society for Microbiology,
Washington,
Smith, HR, Cheasty, T and Rowe, B 1997, Enteroaggregative Escherichia coli and outbreaks
of gastroenteritis in UK, J Clin Microbiol, vol. 35, pp. 814-815.
Smith, HR and Scotland, SM 1993, Isolation and identification methods for Escherichia coli
O157 and other Vero cytotoxin producing strains, J Clin Pathol vol. 46, pp. 10�17.
Smith, HR, Scotland, SM and Rowe, B 1983, Plasmids that code for production of
colonization factor antigen II and enterotoxin production in strains of Escherichia coli, Infect
Immun, vol. 40, pp. 1236-1239.
Sneath, P and Sokal, R 1973, Numerical taxonomy, the principles and practice of numerical
classification, San Francisco, WH Freeman.
Sowers, EG, Wells, JG and Strockbine, NA 1996, Evaluation of commercial latex reagents
for identification of O157 and H7 antigens of Escherichia coli, J Clin Microbiol, vol. 34, pp.
1286�1289.
Spangler, BD 1992, Structure and function of cholera toxin and the related Escherichia coli
heat-labile enterotoxin, Microbiol Rev, vol. 56, pp. 622-647.

Spano, LC, Sadovsky, AD, Fagundes-Neto, U and Scaletsky, IC 2008, Age-specific
prevalence of diffusely adherent Escherichia coli in Brazilian children with acute diarrhea, J
Med Microbiol ,vol. 57, pp. 359-363.
Steiner, TS, Lima, AA, Nataro, JP and Guerrant, RL 1998, Enteroaggregative Escherichia
coli produce intestinal inflammation and growth impairment and cause interleukin-8 release
from intestinal epithelial cells, J Clin Microbiol, vol. 37, pp. 286�289.
Stenutz, R, Weintraub, A and Widmalm, G 2006, The structures of Escherichia coli
Opolysaccharide antigens, FEMS Microbiol Rev, vol. 30, pp. 382-403.
Stoll, BJ, Glass, RI, Huq, MI, Khan, MU, Holt, JE and Banu, H 1982, Surveillance of
patients attending a diarrhoeal disease hospital in Bangladesh, B M J, vol. 23 , pp. 1135-
1139.
Stoll, BJ 1997, The global impact of neonatal infection, Clin Perinatol, vol. 24, pp. 1-21.
Strockbine, NA, Faruque, SM, Alam, K, Tzipori, S and Wachsmuth 1992, DNA probe
analysis of diarrhoeagenic Escherichia coli: detection of EAF-positive isolates of traditional
enteropathogenic E. coli serotypes among Bangladeshi paediatric diarrhea patients, Mol Cell
Probes, vol. 6, pp. 93�99.
Thomas, A, Smith, HR and Rowe, B 1993, Use of digoxigenin-labelled oligonucleotide DNA
probes for VT2 and VT2 human variant genes to differentiate Vero cytotoxin-producing
Escherichia coli strains of serogroup O157, J Med Microbiol, vol. 31, pp. 1700�1703.
Thompson, RB and Miller, JM 2007, Specimen collection, transport, and processing:
bacteriology in Murray, PR, Baron, EJ, Jorgensen, JH et al. Manual of Clinical Microbiology,
8th edition, ASM Press, Washington, DC.
Toma, C, Lu, Y, Higa, N, Nakasone, N, Rivas, M and Iwanaga, M 2003. Multiplex PCR
Assay for Identification of Human Diarrheagenic Escherichia coli, J Clin Microbiol, vol. 41,
no. 6, pp. 2669�2671.

Tornieporth NG, John J, Salgado K, Gunzburg ST and Riley LW 1995, Differentiation of
pathogenic Escherichia coli strains in Brazilian children by PCR, J Clin Microbio , vol. 33,
pp. 1371-1374.
Tornieporth, NG, John, J, de Jesus, P and Riley, LW 1995, Differentiation of pathogenic
Escherichia coli strains in Brazilian children by PCR, J Clin Microbiol, vol. 33, pp. 1371�
1374.
Trabulsi, LR, Keller, R and Gomes, TA 2002, Typical and atypical enteropathogenic
Escherichia coli, Emerg Infect Dis , vol. 8, pp. 508-513.
Unicomb, LE, Faruque, SM, Malek, MA, Faruque, AG and Albert, MJ 1996, Demonstration
of a Lack of Synergistic Effect of Rotavirus with Other Diarrheal Pathogens on Severity of
Diarrhea in Children, J Clin Microbiol, vol. 34, no. 5, pp. 1340�1342 .
Von Baum, H and Marre, R 2005, Antimicrobial resistance of Escherichia coli and
therapeutic implications, Int J Med Microbiol, vol. 295, pp. 503-11.
Voetsch, AC, Angulo, FJ, Rabatsky-Her, T, et al. 2004, Laboratory practices for stool-
specimen culture for bacterial pathogens, including Escherichia coli O157:H7, in the Food
Net sites, 1995-2000, Clin Infect Dis , vol. 38, pp. 190-7.
WHO 2003, Guidelines for safe recreational-water environments, in Coastal and Fresh-
Waters, vol 1, World Health Organization, Geneva, Switzerland, viewed 18 July 2011,<
whqlibdoc.who.int/publications/2003/9241545801.pdf>.
WHO 2004, 5 Keys for safer food�in regions hit by disasters, World Health Organization,
Geneva, Switzerland, viewed 19 July 2011,
<www.who.int/foodsafety/publications/general/en/terrorist.pdf>.
WHO 2005, The treatment of diarrhoea: A manual for physicians and other senior health
workers, 4th rev edn. Department of Child and Adolescent Health and Development

(DCAHD), World Health Organization, Geneva, Switzerland, viewed 16 June 2011,
<whqlibdoc.who.int/publications/2005/9241593180.pdf>.
WHO 2006, Food safety. WHO, Geneva, Switzerland, viewed 18 July 2011,
<www.who.int/foodsafety/publications/general/en/terrorist.pdf>.
Wikipedia 2008, Bacterial cell structure, viewed 18 May 2011, <http://bio-
articles.blogspot.com/2008/04/structure-of-prokaryotic-cell-e-coli.html>.
Wikipedia 2011, Escherichia coli Toxonomy, viewed 18 May 2011 ,
<http://en.wikipedia.org/wiki/Escherichia_coli>.
Wong, CA, Jelacic, S and Habeeb, RL 2000, The risk of the hemolytic-uremic syndrome
after antibiotic treatment of Escherichia coli O157:H7 infections, N Engl J Med, vol. 342, pp.
1930-38.
Wood, LV, Ferguson, LE, Hogan, P, Thurman, D, Morgan, DR, DuPont, HL and Ericsson,
CD 1983, Incidence of bacterial enteropathogens in foods from Mexico, App and Envir
Microbiol, vol. 46, pp. 328-332.
Youssef, M, Shurman, A, Bougnoux M, and Strockbine, N 2001, Bacterial, viral, parasitic
enteric pathogens associates with acute diarrhea in hospitalized children Jordan, FEMS
Immunol Med Microbiol, vol. 28, pp. 257-265.
Zhaxybayeva, O and Doolittle, WF 2011, Lateral gene transfer, Current Biology, vol. 21, no.
7, pp. 242�246.
Zychlinsky, A, Prevost, CM and Sansonetti, PJ 1992, Shigella flexneri induces apoptosis in
infected macrophages, Nature, vol. 358, pp. 167-9.


PHOTOGRAPH
Vortex Mechine
Dry water bath.
Photograph of Centrifuge Machine
Photograph of Thermal cycler

Photograph of Horizontal Electrophoresis Chamber
Photograph of Documentation
chamber wit


eae gene � 881 bp
Stx gene-518 bp
est gene-147 bp
elt gene-322 bp
ipaH gene-619 bp
aggR gene-254 bp
CVD432 gene-194 bp
aspU gene -282 bp
PCR of Different diarrheagenic Esch coli
322 bp
147 bp
254 bp 600bp
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
147bp
1500 bp
Photograph of Multiplex PCR showing aggR gene (254 bp) of EAEC in lane 1,
est gene (147 bp) and elt gene (322 bp) of ETEC in lane 4, only est gene (147
bp) of ETEC in lane 14 and ladder marker (100bp) in lane 5 and 12.

Photograph of Mac-Conkey agar medium showing pink colure colonies of E
.coli.

A B C
Photograph of biochemical reaction of E. coli in TSI agar medium.
A- Positive control showing yellow shunt and butt.
B- Test organism showing yellow shunt and but
C- Negative control showing red shunt and butt.
A B C
Photograph of Indole test of E. coli. A- Positive control showing pink colored ring at the top of the broth medium.
B- Test organism showing pink colored ring at the top of the broth medium.
C- Negative control showing no colored ring at the top of the broth medium

A B C Photograph of Citrating utilization test of E . coli. A - Positive control showing no change of colure in the medium.
B- Test organism showing no change of colure in the medium.
C- Negative control showing blue colure in t the medium..

Polyacrylamide gel electrophoresis Chamber

Extracted RNA
Loading In Electrophoresis Chamber
Visualized RNA Segments of Rotavirus Electrophoresis
Staining
Pictorial presentation of major steps of PAGE

APPENDICES Appendix � I
DATA SHEET
Thesis title: �Detection of Different Diarrheagenic Escherichia coli Strains by multiplex PCR�. A. S.L No: Identification number :
B. Particulars of the patients: 1. Name:
2. Age:
3. Sex: Male/Female
4. Address:
Village: P.O: Union: Thaana: Dist:
5. Admitted patients: Ward no: Bed no: Reg.no:
6. Date of admission:
7. Socio-economic condition:
8. Housing condition: city/village/slum area.
9. Latrine: sanitary/non sanitary (kacha/paka/open).
10. Source of drinking water: supply/tube well/pond/River. C) Presenting complains:
a) Duration of diarrhea for : days b) Onset: c) Frequency of motion: e) Nausea/abdominal discomfort/ anorexia/vomiting.
D) On examination:
1. Pulse /min.
2. Anemia:
3. Abdominal tenderness

4. Dehydration
5. Temp:
Past history: History of antibiotic intake: Name of antibiotic: dose & duration: Complication:
LABORATORY FINDINGS:
Specimen: stool.
Microscopic examination:
Pus cells:
E. histolytica: Not found/ Cyst/ Trophozoite
G. lamblia: Not found/ Cyst/ Trophozoite
Culture:
Organism isolated: Culture Finding: On MacConkey agar media: On Salmonella-Shigella agar media:
Gram staining : Gram Positive Cocci/ bacilli.
Gram Negative Cocci / bacilli.
Motility test: Motile/ Nonmotile
Biochemical tests:
i) Triple sugar iron agar:
shunt:
butt:
ii) Indole test : Positive\ Negative

iii) Citrate utilization test: Positive\ Negative
iv)Oxidase test: Positive\ Negative
Antibiotic sensitivity:
Antibiogram of isolates (CLSI, 2007):
S= sensitive, R= Resistant,
PCR result : Signature:
Zone diameter (mm) Antibiotics Disk content
µgm/disc Resistant Sensitive
Result Comments
Amoxycillin 10 ≤ 13 ≥ 17
Tetracycline 30 ≤ 11 ≥ 15
Cotrimoxazole 25 ≤ 10 ≥ 16
Gentamicin 10 ≤ 12 ≥ 15
Ciprofloxacin 5 ≤15 ≥ 21
Nitrofurantoin 300 ≤ 14 ≥ 17
Nalidixic acid 30 ≤13 ≥ 19
Ceftriaxone 30 ≤13 ≥ 21
Amikacin 15 ≤ 13 ≥ 18
Cephalexin 30 ≤12 ≥ 18

Appendix � II
The composition and methods of preparation of different media, chemicals and reagents used
in this study are given below �
Muller Hinton agar medium
Composition:
Ingredients gram/liter Beef dehytrated infusion 300 Casein hydrolysate 17.50 Starch agar 17.00 Agar 17.00
Thirty eight grams of dehydrated Mueller Hinton agar medium was suspended in 1000 ml
cold distilled water and boiled to dissolve the medium completely. The solution was then
sterilized by autoclaving at 1210C and 15 lbs pressure for 15 minutes. The autoclaved media
was stored at 40C
MacConkeys agar medium
Composition: Ingredients gram/liter Peptone 19.0 Lactose 10.0 NaCl 5.0 Na- Deoxycholat 1.0 Neutral Red 0.03 Crystal Violet 0.001 Agar 15.0
Fifty two grams of dehydrated MacConkeys agar medium was suspended in 1000 ml cold
distilled water and boiled to dissolve the medium completely. The solution was then sterilized
by autoclaving at 1210C and 15 lbs pressure for 15 minutes.
Triple sugar iron agar:
Composition:
Ingredients gram/liter Peptic digest of animal tissue 10.00 Casein enzymic hydrolysate 10.00 Yeast extract 3.00

Beef extract 3.00 Lactose 10.00 Sucrose 10.00 Dextrose 1.00 Sodium chloride 5.00
Sixty five grams of dehydrated triple sugar iron agar medium was suspended in 1000 ml cold
distilled water and boiled to dissolve the medium completely. The solution was then sterilized
by autoclaving at 1210C and 15 lbs pressure for 15 minutes.
Simon�s citrate medium
Composition:
Ingredients Dehydrated media 24.2 gram
Distilled water 1000.0 ml
pH- 6.8, Ingredients dissolved, dispense into test tubes autoclaved at 1210C for 15 minutes
and allowed to set as slopes.
MacFarland Standard 0.5
Composition and preparation 1% (V/V) solution of chemically pure 0.36 (N) sulphuric acid
and 1.175% (W/V) solution of chemically pure (0.048M) barium choloride was prepared in
two separate sterile flasks. Than 9.9ml of sulphuric acid and 0.1ml of barium chloride were
added to the clean screw capped test tube and sealed. The barium sulphate suspension
corresponds approximately to Mcfarland standard tube number1 with corresponding cell
density of 3× 108 organism/ ml to made the turbidity standard of cell density to one half of
the Mcfarland standard tube number 1 which correspond to cell density of 1.5 ×108
organism/ml for determination of antibiotic sensitivity by Kirby-Bauer inoculated technique
0.5ml of 1.75% (W/V) barium chloride (Bacl2 2H2) was added to 99.5ml of 1% (V/V)
sulphuric acid (0.36N), mixed well and 5 � 10 ml was distributed in sterile capped test tube
and sealed.
Kovac�s reagent (Collee et al, 1996)

Composition
Ingredients Amyl or isoamyl alcohol 150ml P-Dimethyl-aminobenzaldehyde 10gram Concentrated hydrochloric acid 50ml
Aldehyde was dissolved in alcohol and acid is added slowly.
Method: Medium was inoculated with test organisms and incubated for 48 hours at 370C. 0.5
ml of Kovacs reagent was added and shaken gently. A red colour in the alcohol layer
indicates a positive reaction.
Oxides reagent
To make 10ml
Tetramethyl-p-phenylenedimine(dihydrocholoride) 0.1g
Distilled water 10 ml
Tris-EDTA buffer:
To make 1 litre TE buffer required:
Tris (10mM)������.1.21gm
EDTA (1mM)������0.372gm
Distilled water������1 litre
EDTA will not be soluble until pH reaches 8.0. pH was checked with pH papers and then
stored at 2-8ºC.
6× Disruption solution for PAGE
6% Sodium Dodecyl Sulphate (SDS), 0.6% 2-mercptoethanol and 60 mM Ethylene diamine tetra acitic acid (EDTA).
10% polyacrylamide gel (2ml)

0.75 M tris-HCL buffer (pH 8.8)- 20ml, Acrylamide solution- 13.3 ml, o.1 M EDTA- 0.4 ml, Distilled water- 4.7 ml, 3% amonnium per sulfate- 1.6 ml and TEMED (Tetramethlenediamine)- 70 µl.
Appendix � III
The composition and methods of preparation of different stains, diluents and
chemicals used in this study are given below
Crystal violet Gram stain:
Crystal violet 20g
Ammonium oxalate 9g
Ethanol or methanol, absolute 95ml
Distilled water to 1 liter
Lugol�s iodine solution:
Potassium iodide 20g
Iodine 10g
Distilled water 1 liter
Alcohol fixative solution:
To make 200ml
Ethanol (ethyl alcohol), absolute 180ml
Acetic acid, glacial 10ml
Distilled water 10ml
Immerse the fixative for 20 minutes. Rinse with 95% ethanol and allow the smear to
dry.
Carbol fuchsin:
Basic fuchsin 10g
Ethanol or methanol 100ml
Phenol 50g
Distilled water 1 liter

Appendix � IV
The biochemical results were interpreted as per the following table:
TSI Species Oxidase
Citrate
utilization Indole
slant butt H2S gas
E. coli - - + Y
Acidic
Y
Acidic
- +
Shigella
spp.
- - - R
Alkalne
Y
Acidic
- -
Klebsilla
spp.
- + - Y
Acidic
Y
Acidic
- +
Salmonela
spp.
- + (d) - R
Alkalne
Y
Acidic
+ +(d)
Positive= (+)
Negative= (--)
Yellow=Y
Red=R
D= different strains give different results.
Appendix � V
Equipments for PCR
Centrifuge 5415 R with refrigerator

Vortex Mixer (Digi system VM-2000)
Micropipettee (Company-Eppendrof)
Laminar Flow Cabinet (Company stremline)
Microwave oven for gel preparation
Electric heated dryer (Model Jo2714)
Thermal cycler (Model-Master cycler personal)
Gel apparatus (Major science Minis-300)
Major science Minis UVDI
Appendix � VI
Rotavirus detection by PAGE (Polyacrylamide Gel electrophoresis):
This test is based on the detection of rotavirus double stranded RNA genome which is
separated into 11 segments by electrophoresis through polycrylamide gels.
Steps (Extraction of RNA, electrophoresis and staining):
1. Transfer the 300 µl sample to 1.5 ml tube.
2. Add 60 µl of 6× Disruption solution and vortex.
3. Incubate at 370C for 30 minutes.

5. Centrifuge at 12000 rpm for 1 minute.
6. Transfer supernatant (300 µl) to a new tube.
7. Add 600 µl of ethanol and add 10 µl of 5M NaCl and mix by inverting.
8. Incubate at 800C for 30 minutes.
9. Centrifuge at 12000 rpm for 15 minutes.
10. Discard the supernatant.
11. Dry up to for 15 minutes.
13. Add 10 µl of loading buffer.
14. Subject RNA sample to electrophoresis in a polyacrylamide slab gel (for 4 hours).
15. Stain the Gel with Silver nitrate for 40 minutes.
Silver Staining of the gel
1. Stain the gel with silver nitrate (0.2 gm in 100 ml) for 40 min.. 2. Wash the gel 3 times with distilled water. 3. Stain the gel with NaOH (3 gm in 100ml) and formaldehyde (HCHO) (0.4 ml) for 10 min. 4. Add stop solution (5% acetic acid).

Appendix-VII
For Patients AeMwZµ�g m¤§wZcÎ
GB m¤§wZc�Îi D�Ïk¨ Avcbv�K cÖ�qvRbxq Z_¨ cÖ̀ vb Kiv, �h Z_¨¸�jv Avcbv�K wm×v�� wb�Z mvnvh¨ Ki�e,
Avcbvi m��vb/ �ivMx GB M�elYvq Ask MÖnb Ki�e wK bv ?
D�Ïk¨ I c×wZ
GB M�elYvq m¤úb� n�j Avkv Kiv hv��Q �h evsjv�`�k Wvqvwiqv �iv�M Avµv�� �ivMxi Wvqvwiqvi wbw`ó Kvib �ei
K�i mwVK wPwKrmv Ges cÖwZ�iv�a h_vh_ e¨e �̄v MÖnb Kiv hv�e|
GB M�elvi Rb¨ gqgbwmsn �gwW�Kj K�jR nvmcvZv�ji wkï I �gwWwmb wefv�M Ges Gm.�K nvmcvZv�j AvMZ
�ivMx�K A�� ©f~³ Kiv n�e| Avcwb hw` Avcbvi m��vb/ �ivMx�K GB M�elYvq AskMÖnb Kiv�Z m¤§Z _v�Kb Zvn�j
Avcbvi �ivMxi Amy¯ �Zv I wPwKrmv m¤ú©wKZ wKQy cÖk � Kiv n�e Ges Zv bw_�Z msi¶b Kiv n�e| M�elYvi Rb¨ 10
wgwjwjUvi /MÖvg cvqLvbv �bIqv n�e|
M�elYvi SuzwK
GB M�elbvq AskMÖn�b �Kvb kvixwiK SzuwKi m¤¢vebv �bB|
LiP
M�elbvq AskMÖn�bi Rb¨ Avcbvi m��vb/ �ivMxi wPwKrmvi cÖK�Z LiP e¨ZxZ Avi �Kvb LiP bvB ev Avcbv�K Avw_©K
mn�hvwMZv Kivi �Kvb e¨e¯ �v bvB|
�MvcbxqZv
M�elYv PjvKvjxb I cieZx©�Z cÖk � �_�K cÖvß Z_¨ I j¨ve�iUix �_�K cÖvß Z_¨ K�Vvifv�e �Mvcb ivLv n�e|
M�elYvq AskMÖnb
GB M�elYvq AskMÖnb m¤ú~b© �¯^�Qvg~jK| Avcwb M�elYvq AskMÖn�b A¯x̂K�wZ Rvbv�Z cv�ib A_ev M�elY& PjvKvjxb
�h�Kvb mg�q M�elYv �_�K Avcbvi m��vb/�ivMx�K cÖZ¨vnvi K�i wb�Z cv�ib| GB di�g ¯v̂¶i Ki�j Avcbvi
AvBbMZ �Kvb AwaKvi Le© n�e bv| Avcbvi m��vb/ �ivMxi wPwKrmv h_vh_fv�e Pj�e| hw` Avcbvi �Kvb cÖk � _v�K,
Avcwb wRÁvmv Ki�Z cv�ib, Avgiv DËi cÖ̀ vb Kivi h_vmva¨ �Póv Kie|
m¤§wZ ¯x̂Kv�ivw³
Avwg M�elYvq wb�qvwRZ wPwKrm�Ki mv�_ GB M�elYv wb�q Av�jvPbv m��wó cÖKvk KiwQ| Avwg m¤§wZc�Îi kZ©̧ �jv
c�o�wQ/ Avgvi m¤§y�L cwVZ n�q�Q Ges �¯̂�Qvq Avgvi m��vb/ �ivMx�K M�elYvq AvskMÖnb Ki�Z m¤§wZ Ávcb
KiwQ|
mv¶vrMÖnbKvixi ¯v̂¶i
ZvwiL t
Awffve�Ki ¯v̂¶i/ e �×v½yjxi Pvc
ZvwiLt