
Densitometric Vertebral Fracture Assessment (VFA) - International
37
Vertebral Fracture Initiative Part III Densitometric Vertebral Fracture Assessment (VFA) Authored by: John T. Schousboe 1 , Tamara Vokes 2 , Neil Binkley 3 , Harry K. Genant 4 1. Division of Health Policy and Management, School of Public Health, University of Minnesota, Minneapolis, MN, USA; Park Nicollet Osteoporosis Center, Park Nicollet Health Services Minneapolis, MN, USA 2. Department of Medicine, University of Chicago, Chicago, IL, USA 3. Osteoporosis Clinical Research Program, University of Wisconsin, Madison, WI, USA 4. Department of Radiology, Medicine and Orthopedic Surgery, University of California, San Francisco Reviewed by: Philip Sambrook Kolling Institute of Medical Research (Bone & Joint Research), Sydney Medical School, Royal North Shore Hospital, St Leonards NSW 2065, Australia Nick Pocock Department of Nuclear Medicine, St Vincent's Hospital, Sydney, NSW
Transcript of Densitometric Vertebral Fracture Assessment (VFA) - International
Vertebral Fracture Initiative
Part III
Densitometric Vertebral Fracture Assessment (VFA)
Authored by:
John T. Schousboe1, Tamara Vokes2, Neil Binkley3, Harry K. Genant4
1. Division of Health Policy and Management, School of Public Health, University of Minnesota, Minneapolis, MN, USA; Park Nicollet Osteoporosis Center, Park Nicollet Health Services Minneapolis, MN, USA 2. Department of Medicine, University of Chicago, Chicago, IL, USA
3. Osteoporosis Clinical Research Program, University of Wisconsin, Madison, WI, USA
4. Department of Radiology, Medicine and Orthopedic Surgery, University of California, San Francisco
Reviewed by:
Philip Sambrook Kolling Institute of Medical Research (Bone & Joint Research), Sydney Medical School, Royal North Shore Hospital, St Leonards NSW 2065, Australia Nick Pocock Department of Nuclear Medicine, St Vincent's Hospital, Sydney, NSW

1
Abstract
Vertebral fracture assessment (VFA) can be done seamlessly at the bone densitometry
point of care. Such an approach enhances fracture risk assessment because bone mineral density
(BMD) and prevalent vertebral fracture are independent predictors of incident fractures. Since
two thirds to three quarters of vertebral fractures do not come to clinical attention at the time of
their occurence, spine imaging is required for their detection. Although densitometric lateral
spine images do not have the spatial resolution of lateral spine radiographs, VFA detects
moderate to severe radiographic vertebral fractures with a high level of accuracy. Prevalent
vertebral fractures are particularly likely to be present in women 70 or older and men age 80 or
older, those with significant height loss or history of prior fracture, and those on glucocorticoid
therapy. VFA at the time of bone densitometry is warranted in these individuals if the results of
the test would reasonably influence therapeutic choices to reduce their fracture risk.

2
Introduction
Since the advent of fan-beam dual-energy X-ray absorptiometry (DXA) systems, the
technology has been developed and adapted to obtain near radiographic quality lateral images of
the lumbar and thoracic spine. These images allow evaluation for prevalent and (if a prior image
is available for comparison) incident vertebral fractures, a process called vertebral fracture
assessment (VFA), using qualitative, semi-quantitative, or quantitative morphometric methods.
Bone mineral density (BMD) and vertebral fracture assessment give complementary,
independent information regarding a person’s fracture risk (see below). Densitometric imaging
of the spine allows vertebral fracture assessment to be done efficiently at time of bone
densitometry, improving overall assessment of an individual’s future fracture risk.
This section of the IOF vertebral fracture initiative reviews the advantages and
disadvantages of densitometric lateral spine imaging compared to standard radiography,
indications for VFA, acquisition and interpretation of VFA images, and incorporation of the
results of VFA into overall fracture risk assessment.
Importance of Densitometric VFA
Vertebral fractures are a marker of bone fragility and indicate a higher risk of fractures.
The presence of one or more prevalent vertebral fractures on lateral spine radiographs is a strong
predictor of future incident vertebral fractures and a moderate predictor of non-vertebral
fractures, independent of BMD.(1-4) Similarly, prevalent vertebral fractures on lateral VFA
images are predictive of incident clinical non-vertebral fractures and specifically incident hip
fractures independent of bone density in women age 75 and older.(5) Two-thirds to three
quarters of vertebral fractures, however, are not clinically recognized (6, 7), and hence spine

3
imaging is required for their detection. Among women age 65 and older who do not have
osteoporosis by BMD criteria, 10% to 28% have one or more prevalent vertebral fractures.(8-11)
VFA combined with bone densitometry can alter an individual’s estimated fracture risk
sufficiently to change therapeutic recommendations in over 10% of those referred for bone
densitometry.(12)
Comparison of Densitometric VFA and Lateral Spine Radiography
Densitometric VFA has several advantages over lateral spine radiographs. First, the
images can be obtained easily and quickly at the same time as a bone density scan at less cost
than standard spine radiographs, facilitating estimation of the patient’s fracture risk by
incorporating both bone density and vertebral fracture status. Second, the radiation exposure
required to obtain a VFA image is low, approximately 3-40 microSieverts, whereas the radiation
exposure associated with lateral thoracic and lumbar spine radiographs is upwards of 600
microSieverts. Third, standard lateral spine radiographs are obtained using cone-beam X-rays,
which creates parallax distortion within vertebrae located above or below the central point of the
beam. In contrast, densitometric VFA uses fan-beam methodology to image the spine. Hologic
densitometers use a wide fan-beam of X-rays, which is oriented with the plane of the X-rays
perpendicular to the spine, whereas Lunar-GE densitometers use a narrow fan-beam with the
plane of the X-rays parallel to the spine. In both cases, parallax distortion causing oblique
projections of vertebrae are much less common on VFA images than on lateral spine
radiographs, which makes the detection of lumbar vertebral fractures potentially more
challenging on the radiographs.

4
However, the images obtained with standard spine radiography are less noisy and have
higher spatial resolution than VFA images, such that the cortical edges and endplates are better
defined. As a result, more vertebrae are evaluable on conventional radiographs than on VFA
images, especially in the upper thoracic spine. With VFA images 90% to 94% of T8 vertebrae,
60% to 80% of T6 vertebrae, and 30% to 63% of T4 vertebrae are evaluable in three separate
studies.(9, 13, 14) Moreover, the inter-rater reliability for identification of patients with one or
more prevalent vertebral fractures is slightly lower for VFA than for standard radiography, but
still good (kappa scores 0.56 to 0.70 across 4 studies).(11, 14-16) When using the Genant semi-
quantitative method for vertebral fracture assessment on standard lateral spine radiographs as the
gold standard, the sensitivity and specificity of VFA for individuals with one or more moderate
to severe (Genant SQ grade 2 or 3) vertebral fractures is 87% or higher and 85% or higher,
respectively, but is substantially lower (~50%) for Genant grade 1 deformities (Table 1).(17-20)
The inter-rater reliability for vertebral fracture detection is slightly lower on VFA than on
conventional lateral spine radiographs. The accuracy of VFA, like conventional radiography, for
identifying radiographic vertebral fractures appears to be better in the lumbar than in the lower
thoracic spine,(13) may be compromised when there is adjacent degenerative disc disease, and is
poorer in the presence of moderate to severe scoliosis.(20)
Recent VFA technological advancements may further improve performance compared to
standard radiography. In this regard, Buehring and colleagues recently found 92% of all
vertebrae to be evaluable on VFA images using a newest Lunar-GE densitometer (Figure 1),
compared to 76% on VFA images obtained on an older generation densitometer (both
manufactured by GE Healthcare Lunar, Madison, WI).(21) In this study, 43 vertebral fractures

5
were identified by consensus readings on the VFA images obtained with the newer technology,
compared to 21 fractures found on images obtained with the older technology.
The most recently available Hologic VFA technology also yields better VFA images
compared to older Hologic densitometers (Figure 2). The only study assessing the agreement
between VFA images obtained with the newer Hologic technology reported less than 2% of
vertebrae to be unevaluable.(22) Analyzed per vertebra, this study showed very high specificity
of VFA using the newer Hologic technology (99%) and better sensitivity (83%) to detect those
with any grade of fracture (Genant SQ 1, 2, or 3) compared to studies using older Hologic VFA
technology (Table 1).
When VFA should be followed by radiography is controversial and depends on the
individual patient clinical situation.(15, 23) However, additional imaging should be considered if
there are two or more unevaluable vertebrae below T6, poor visualization due to moderate to
severe scoliosis or a need to confirm possible grade 1 vertebrae.(20) For Genant SQ grade 2 or
grade 3 prevalent vertebral fractures, VFA has close to 100% specificity in comparison to
radiographs and at least 93% sensitivity, which is likely to be even higher for the technologies
with the improved resolution mentioned above.
Indications for VFA
The International Society for Clinical Densitometry (ISCD) has published indications for
performing VFA as part of bone densitometry, that were created by a task force for the ISCD
Position Development Conference of 2007 and vetted by a panel of experts.(24) Populations
considered appropriate for VFA are those in whom the pre-test probability of one or more
prevalent vertebral fractures being present exceeds 10%,(25) and for whom documentation of

6
one or more vertebral fractures will alter patient management (Tables 2 and 3). The populations
for whom documentation of a prevalent vertebral fracture is most likely to alter therapy are those
who do not have osteoporosis by bone density criteria and/or in the absence of a prevalent
vertebral fracture would not be judged to have a sufficiently high absolute 10-year fracture risk
to warrant therapy. Among women with a femoral neck T-score of -1.5 to -2.4, VFA is indicated
at the time of bone densitometry for those with one of the following risk factors; age 70 or older,
height loss of more than 4 cm compared to recalled young adult height, more than 2 cm of height
loss between two measurements with the same stadiometer, and self-reported prior vertebral
fracture without prior documentation of that fracture (Table 2). VFA is also indicated for women
with a femoral neck T-score of -1.5 to -2.4 and two of the following; age 60 to 69, historical
height loss of 2 to 4 cm, self-reported prior non-vertebral fracture, or a chronic disease that is
associated with a higher risk of vertebral fracture (such as rheumatoid arthritis, moderate to
severe COPD, or Crohn’s disease).
Older men have a lower age-specific prevalence of vertebral fracture than women of
comparable age (26) and hence the indications for VFA among men are slightly more stringent
compared to those for women (Table 3). Among men with a femoral neck T-score of -1.5 to -
2.4, VFA is indicated for those with one of the following risks factors; age 80 and older, height
loss of more than 6 cm compared to recalled young adult height, more than 3 cm of height loss
between two measurements with the same stadiometer, and self-reported prior vertebral fracture
without prior documentation of that fracture.(24) VFA is also indicated for men with a femoral
neck T-score of -1.5 to -2.4 and two of the following; age 70 to 79, historical height loss of 2 to 4
cm, self-reported prior non-vertebral fracture, or a chronic disease that is associated with a higher
risk of vertebral fracture.(24)

7
Among those for whom pharmacologic fracture risk reducing therapy is indicated,
regardless of the presence or absence of a prevalent vertebral fracture (such as osteoporosis by
bone density criteria or a high absolute 10-year fracture risk), VFA might nonetheless be
appropriate if documentation of a prevalent vertebral fracture would influence the choice of
therapeutic agent or the duration of drug therapy. For example, a reasonable choice for some
individuals with osteoporosis by bone density criteria and prevalent vertebral fracture may be an
initial one to two year treatment period with an anabolic agent followed by an anti-resorptive
agent which may yield superior improvements in BMD (and potentially lower fracture risk to a
greater degree) than anti-resorptive drug therapy alone,(27) Similarly, there remains controversy
over how long anti-resorptive therapy should be continued, particularly in the case of
bisphosphonates. Because of their long-term skeletal retention, some anti-resorptive effect may
persist for years after their discontinuation. This question was explored by the FLEX study that
randomly assigned women treated with alendronate for 5 years to continue that drug for an
additional 5 years or switch to placebo. Among the subset with a prevalent vertebral fracture,
those switched to placebo had a higher risk of subsequent clinical vertebral fracture compared to
those who continued alendronate.(28) At this time, there are no data to specifically guide how
long anti-resorptive therapy should be continued in either those with or without prevalent
vertebral fracture. In the absence of such data, clinicians nonetheless have to make decisions in
individual patients. These decisions should be influenced by that individual’s current fracture
risk. The individual’s risk of fractures after several years of anti-resorptive drug use clearly will
be influenced by whether or not there are any prevalent vertebral fractures. In patients with a
prevalent fracture it may be appropriate to consider a longer treatment period.

8
The future fracture risk associated with a prevalent vertebral fracture is higher in those
who have sustained their fracture more recently. It may therefore be reasonable to obtain a
baseline VFA at the time that osteoporosis is diagnosed, such that follow-up VFA’s can
determine whether or not incident vertebral fractures have occurred since the baseline study.
Incident fractures remain common even in those on pharmacological treatment; in randomized
controlled trials of oral bisphosphonates, incident vertebral fractures occurred in 5 to 18% of
those on anti-resorptive drug therapy over a three year period.(29-32). It would therefore be
useful to obtain a baseline VFA when drug therapy is initiated even in patients that have a very
high risk of fracture even without knowing their prevalent fracture status. Hence follow-up VFA
a few to several years later would determine incident fractures and influence further treatment
options.
Finally, those who are on chronic systemic glucocorticoid therapy have a much higher
incidence of vertebral fractures at all ages (33-36) and hence even younger individuals who have
been on long-term glucocorticoid therapy have a high prevalence of vertebral fractures. VFA at
the time of bone densitometry, for those requiring ongoing systemic glucocorticoid therapy, is
appropriate if documentation of prevalent and/or incident vertebral fracture will influence choice
or duration of therapeutic fracture prevention therapy.
Obtaining VFA Images
Patient positioning
Obtaining lateral spine images for vertebral fracture assessment can be done quickly and
easily at the time of bone densitometry. Patient positioning is particularly easy when using a
densitometer with a rotating C-arm.(37) In this instance, the patient is kept in the same position

9
used to obtain AP lumbar spine bone density; supine with a bolster under the distal lower
extremities such that the hips are flexed at 90 degrees, and arms held above the head.
Without a rotating C-arm, lateral spine images for VFA are obtained in the lateral
decubitus position. With this approach, proper positioning by the technologist produces VFA
image quality comparable to supine lateral VFA images.(37) The patient needs to be lying on the
side without trunk rotation such that the coronal plane of the body is perpendicular to the plane
of the densitometer table. If the body is rotated forward or backward from this position, the
vertebral body outlines can be obscured. An indication that this has occurred is prominent
appearance of the rib angles of one side of the rib cage posterior to the spinal column (Figure 3).
Additionally, in the lateral decubitus position, most individuals will have a smaller body
circumference at the level of the mid-abdomen compared to the level of the hips, such that they
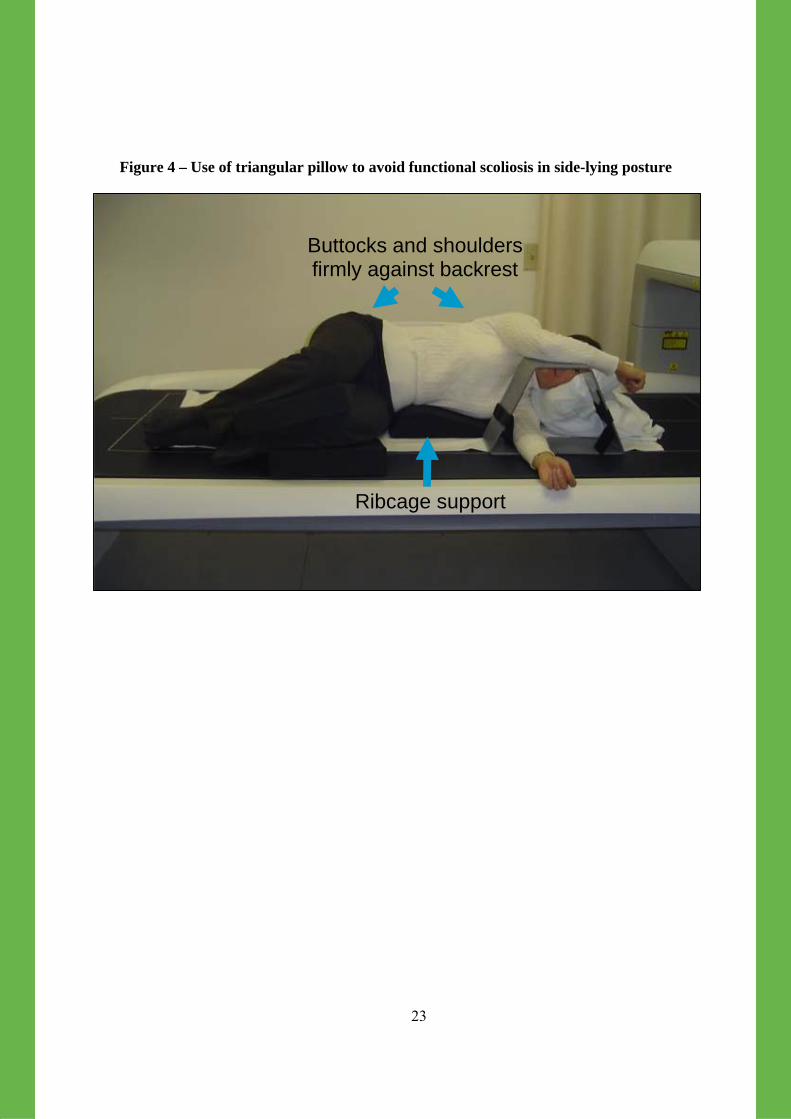
will naturally have a functional scoliosis convex downward when lying on their side. For these
individuals, a triangular pillow needs to be place under their side at the level of the mid-abdomen
such that the spine is parallel to the table without a curve (Figure 4).
Even with the best positioning possible, as noted previously, upper thoracic vertebrae are
more likely to be unevaluable than lower thoracic and lumbar vertebrae. Vallarta-Ast and
colleagues have shown that in some patients obtaining a second VFA image with the patient
lying on their opposite side (reverse lateral decubitus position) will often yield images on which
additional vertebrae are evaluable (Figure 5).(38)
Dual-energy versus single-energy images
VFA images obtained with X-rays of only one level of energy (single-energy) yield
images that include prominent soft tissue features. In contrast, dual-energy X-rays can use a
second level of X-ray beam energy to account for the X-ray absorption by soft tissues, producing

10
images that are noisier but with higher contrast for bone and greatly diminished soft tissue
shadows. Advantages of single-energy imaging are that the images can be obtained faster, and
the endplates and cortices are slightly sharper than on dual-energy images. However, single-
energy images are disadvantaged in that the shadows created by soft tissues can obscure
visualization of the vertebrae, especially in areas where the contrast between adjacent soft tissues
is considerable, such as the diaphragm (Figure 6). Hologic densitometers are optimized to
provide high quality single-energy X-ray images, whereas Lunar densitometers are optimized to
provide high quality dual-energy X-ray images.
AP Image
AP VFA images can aid both labeling of vertebrae and assessing the severity of scoliosis,
which influences how well VFA images can be interpreted. Nonetheless, AP imaging of the
thoraco-lumbar spine is generally not necessary to successfully interpret VFA images with high
quality, and hence is not routinely done.
Interpreting VFA Images
VFA interpretation starts with an evaluation of image quality. The superior portion of the
sacrum should be visualized at the bottom of the image, and none of the rib angles of the rib cage
should be prominent posterior to the spinal column (Figure 3). The next step is to label the
vertebrae correctly, starting with identification of the fourth lumbar vertebra. Ninety-one percent
of individuals have five lumbar vertebrae, and labeling the vertebral immediately superior to the
sacrum as L5 will lead to appropriate vertebral labeling. Seven to eight percent of individuals
have only four lumbar vertebrae, and 2% have six lumbar vertebrae.(39) Correctly identifying
and labeling vertebrae in such individuals is a challenge. There is no easy method of doing so

11
that is always accurate, and there is the possibility that vertebrae considered to be T4 to L4 may
actually be T3 to L3 or T5 to L5. As long as vertebrae are consistently labeled the same way on
repeat VFA’s, this is of little consequence given that fracture ascertainment within each
evaluable vertebra is accurate.
The next step is to determine what vertebrae are evaluable. This is important as the
Genant semi-quantitative method depends on recognizing differences in vertebral shape
compared to what is expected as normal in order to determine whether or not an individual
vertebra is deformed.(40) Hence, for a vertebra to be fully evaluable the anterior and posterior
cortices and the endplates need to be fully visible. If parts of one of the endplates or cortices
cannot be seen, it may nonetheless be possible to identify a vertebra as deformed if, based on that
portion of the vertebra that is visible, it is clear that its shape deviates from what is normal for
that vertebral level. However, one cannot state that a vertebra has no deformity or abnormality
without the full outlines of the vertebra being visible. Generally, the default score is 0 for
reasonably but not completely visible vertebrae.
For each evaluable vertebra, the next step is to determine whether or not the vertebra is
deformed. According to the Genant semi-quantitative criteria, this is done primarily by
comparing the shape of each vertebra to its neighbours; this method is described in much more
detail in Part II. Briefly, normal vertebrae will be roughly in the shape of a rectangle, with the
inferior and superior endplates being parallel to each other. Wedge deformities are recognized by
a reduction in the anterior and to a lesser extent middle height of the vertebra, such that the
superior and inferior endplates are no longer parallel, but rather would converge if extended
along their planes anterior to the vertebra. With biconcave deformities, the anterior and posterior
heights of the vertebrae are maintained, but the middle heights are reduced. Typically, one or

12
both endplates are bowed in (convex) toward the middle of the vertebral body. With crush
deformities, all three vertebral heights are reduced such that the superior and inferior endplates
may remain parallel to each other, but the overall height of the vertebra is reduced compared to
its immediate neighbours. The distinction between these types of deformities is often confounded
by the variable combination of deformities, but fortunately this classification is less important
than the severity score for fracture risk prediction. For questionable cases where it is not obvious
that the apparent height reduction(s) are sufficient to consider the vertebra deformed, it may be
helpful to measure vertebral heights using VFA imaging software: six points are placed on the
borders of the vertebra (as described in part II) and the software reports the vertebral heights,
their ratios and the degree (percent) of deformation. For borderline wedge deformities, the
interpretation of a true fracture is supported by associated endplate deformities or cortical breaks
consistent with fracture.(40,16)
Non-Fracture Deformities
For vertebrae that do appear to be deformed, it is important to assess whether or not non-
osteoporotic pathology could account for the deformity. Several conditions can change vertebral
shape in ways that can mimic vertebral fracture. Disc degeneration can produce osteoarthritic
remodeling that results in some loss of vertebra height and elongation of the vertebra in the
sagittal plane, creating a wedged appearance (anterior height shorter relative to the posterior
height (Figure 7).(41) Sometimes in these instances, the anterior aspect of the endplates are
convex away from the center of the vertebra. Schuermann’s disease is also often characterized
by wedged vertebrae, especially in the mid-thoracic spine (Figure 8). These anomalies can often

13
be recognized by the undulating, wavy nature of the endplates. Congenital fusion of two adjacent
vertebrae can also create a wedged structure, with the posterior height of the fused vertebrae
significantly greater than the anterior height (Figure 9). Schmorl’s nodes are sharply marginated
invaginations of only a portion of the superior or inferior endplate with the bulk of the endplates
intact (Figure 10). Similarly, Cupid’s bow can be recognized as bowing of the posterior aspect
of the inferior endplate toward the middle of the vertebra, more commonly in the lower lumbar
spine.(42) In contrast, biconcave vertebral fractures typically involve the superior endplate to a
greater degree, with the greatest degree of endplate bowing typically in the mid-sagittal plane.
Malignancy within a vertebra may result in destruction of a portion of the cortex, expansion of
the cortex, or areas of radiodensity or lucency in the middle of the vertebra atypical for
osteoporotic fracture (Figure 11).(43, 44)
Indications for follow-up imaging
Follow-up spine radiographs can be very helpful if there are vertebrae that are
unevaluable on VFA between T7 and L3. Similarly, because VFA does not detect Genant grade
1 deformities accurately, follow-up radiography would be appropriate if confirmation of grade 1
vertebral deformities, consistent with fracture, would alter patient management. Follow-up
lateral spine radiography may be advisable for any patient with a vertebral deformity and a
history of malignancy with potential to metastasize to the spine, or with any abnormalities on
VFA that cannot be comfortably ascribed to benign causes.
Incorporating VFA into fracture risk assessment
Both the number and severity of prevalent vertebral fractures substantially influence the
risk of subsequent vertebral and non-vertebral fractures independent of BMD.(1, 4) Moreover,

14
current available pharmacologic fracture prevention therapies have fracture reduction efficacy in
those with prevalent vertebral fracture with T-scores below -1.0,(45, 46) and hence VFA largely
identifies those for whom fracture prevention therapy is indicated virtually regardless of other
risk factors.
The World Health Organization FRAX® model estimating absolute fracture risk gives an
assessment of major osteoporotic (hip, clinical vertebral, humerus, and wrist) fracture and
specifically of hip fracture. The FRAX® algorithm is based on clinical risk factors, one of which
is prior fracture.(47, 48) It may be reasonable to count the presence of one or more prevalent
vertebral fracture as “prior fracture” in the algorithm when estimating absolute fracture risk in
those who have had one or more vertebral fractures documented on VFA. This may
underestimate the risk of subsequent vertebral fractures especially in those with high grade
and/or more than one vertebral fracture,(49) but the extent to which future versions of FRAX®
should be altered to predict skeletal site specific fracture risk is quite controversial.(50)
Nonetheless, VFA may aid calculation of absolute fracture risk by detecting that subset with
prior vertebral fracture(s) that have not come to clinical attention.
Characteristics of good VFA reports
VFA reports at a minimum should state the vertebra(e) within the range of T4 to L4 that
are evaluable for deformity, those that are deformed, and whether or not the deformity is
consistent with a vertebral fracture or is more likely due to non-osteoporotic causes. The
presence of osteoarthritic or degenerative changes should be noted if present in the lumbar spine,
because its presence often results in overestimation of spine bone density to some degree.

15
Potential clinically-significant extra-spinal pathology, evident on the VFA images, should
be noted. A common extra-spinal pathology that may be noted is abdominal aortic calcification
(AAC). AAC detected on lateral spine radiographs is an independent predictor of incident
cardiovascular disease, specifically myocardial infarction and stroke, independent of other
clinical cardiovascular disease risk factors.(51-53) Similarly, two recent studies, one with single-
energy VFA images (54) and the other with dual-energy VFA images,(55) have shown that AAC
on densitometric VFA images is a significant predictor of incident myocardial infarction or
stroke, and as significant or more so than the presence of peripheral vascular disease.(53) This
may represent an indication for more aggressive management of modifiable cardiovascular
disease risk factors such as LDL cholesterol.(56) VFA should not be used to regularly screen for
AAC, at this time is the sole indication for VFA is the detection of vertebral fractures.

16
Conclusion
Densitometric lateral spine imaging to detect vertebral fractures (VFA) substantially
improves the utility of bone densitometry to improve fracture risk assessment. VFA detects
moderate and severe radiographic vertebral fractures with a high level of accuracy, and this
accuracy may improve further with technologic advances. VFA is indicated in a substantial
proportion of older women and men having bone densitometry. Non-osteoporotic deformities
need to be distinguished from those due to osteoporotic bone fragility. The presence of one or
more vertebral deformities due to bone fragility constitutes, with unusual exceptions, an
indication for pharmacologic fracture prevention therapy. Follow-up plain radiograph imaging is
advisable if substantial numbers of vertebrae are unevaluable, if the presence of deformity is
uncertain, if abnormalities cannot be ascribed to benign causes, or if deformities are noted in a
person with a history of malignancy with potential to metastasize to the spine.

17
Table 1 – Accuracy of VFA for Detection of Prevalent Vertebral Fractures Compared to
Standard Radiography Citation / Year / Vert Fx Definition
Population (number) & Setting
Proportion Vertebrae Evaluable
VFA Sensitivity / Specificity
Agreement (Kappa) VFA -Rad
Binkley, 2005 (17) Genant SQ
80, mean age 72.8 years; Academic bone densitometry center, U.S.
81% per vertebra 70.0%/96.2%
per vertebra 0.545
Chapurlat, 2006 (13) Genant SQ
85, mean age 71 years; Academic bone densitometry center, France
Reported by vertebral level; <80% & T7 and above
per vertebra T11-L4: Sens. 44%-83%, Spec. 80%-99%
T12-L4: 0.69-0.87 T10, T11: 0.36-0.37 T9 above: 0.34-0.85
Damiano, 2006 (15) Genant SQ
136, mean age 69.1 years; Academic rheumatology dept, France
89% without difficulty, 11% w/ difficulty, 1% unreadable
Per vertebra 82.8% / 98.3% Per person 94%/ 83%
Not reported
Ferrar, 2003 (57) Qualitative Visual X-ray; Qual visual VFA and Quant morphometric VFA
70, mean age 70; academic bone metabolism center, U.K.
88% (Qual. reading) 85% (Quant. morphometry)
Qual. VFA vs Qual. X-ray 85%-92% / 95-98% Quant. VFA vs Qual. X-ray 82% / 94%
Qual. VFA vs Qual. X-ray: 0.85 – 0.87 Quant. VFA vs Qual X-ray 0.77
Ferrar, 2008 (18) ABQ
Low risk=459 mean age 68 yrs), High risk=298 mean age 68 yrs
Not reported Per person Low risk 71.2%/97.4% High risk 84.3% /96.8%
Low risk: 0.62 High risk: 0.81
Fuerst, 2009 (14) Genant SQ
203, mean age 67.5 years; three bone densitometry centers U.S.
42% (T4) 91% (T8)
Per vertebra 70-73% / 99%
Per vertebra 0.64-0.78 per person 0.55-0.73
Hospers, 2009 (22) Genant SQ & Qualitative Visual of radiographs
250, mean age 62years; Bone densitometry center in Netherlands
98.7% VFA 94.3% visual radiography 88.2% SQ radiography
Per vertebra 83.6% / 99.8%
0.82
Rea, 2000 (19) Genant SQ
161, mean age 64 years; metabolic bone disease unit, U.K.
94.9% VFA 99.9% X-ray
Per vertebra 68%/94% Per person 77%/89%
Per vertebra 0.79 Per person 0.68
Schousboe, 2006 (20)
203, mean age 74.2 years. Community bone densitometry unit
70.7% of persons had all vertebrae on VFA evaluable
Per vertebra 47% - 57%/ 98.5% Per person 52%-63%/ 85%-89%
Not reported
Vokes, 2003 (23) ?Genant SQ
66, mean age not reported
89% of persons had all vertebrae between T6 and L4 evaluable
Per person (grade 2-3 only) 95%/92%
Per person 0.73
Abbreviations: Qual. Qualitative; Quant. Quantitative; Sens. Sensitivity; Spec. Specificity
18
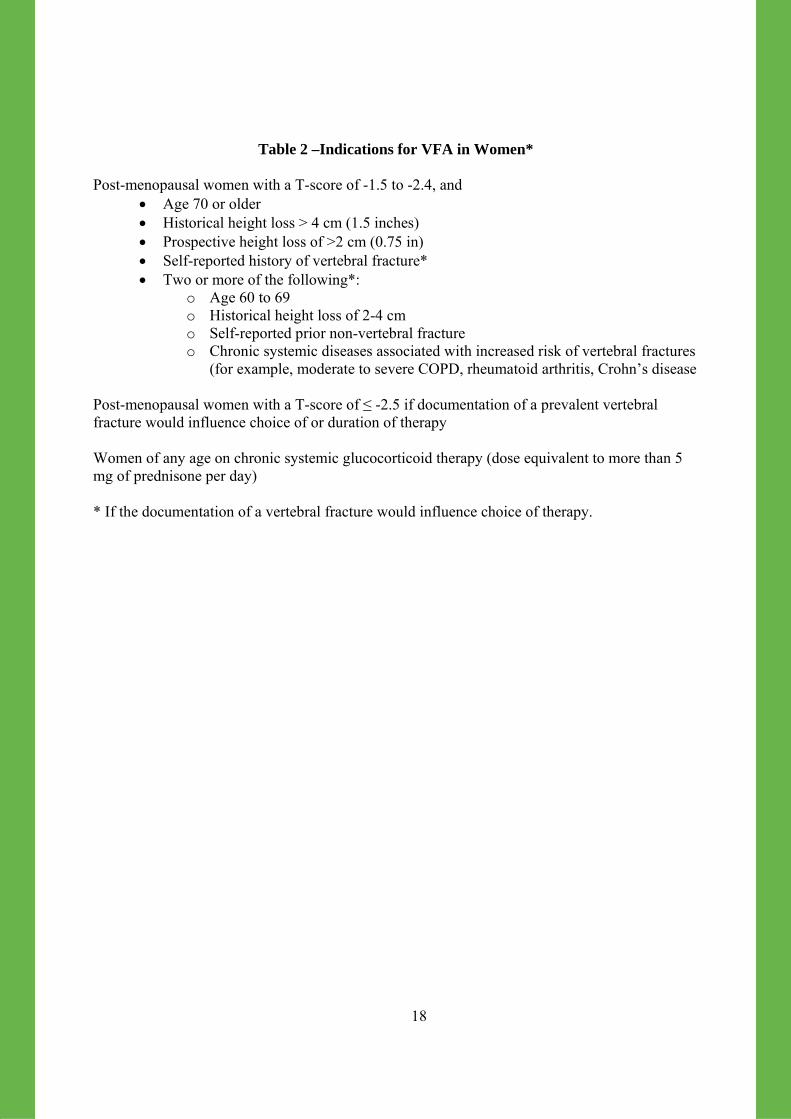
Table 2 –Indications for VFA in Women* Post-menopausal women with a T-score of -1.5 to -2.4, and
• Age 70 or older • Historical height loss > 4 cm (1.5 inches) • Prospective height loss of >2 cm (0.75 in) • Self-reported history of vertebral fracture* • Two or more of the following*:
o Age 60 to 69 o Historical height loss of 2-4 cm o Self-reported prior non-vertebral fracture o Chronic systemic diseases associated with increased risk of vertebral fractures
(for example, moderate to severe COPD, rheumatoid arthritis, Crohn’s disease Post-menopausal women with a T-score of ≤ -2.5 if documentation of a prevalent vertebral fracture would influence choice of or duration of therapy Women of any age on chronic systemic glucocorticoid therapy (dose equivalent to more than 5 mg of prednisone per day) * If the documentation of a vertebral fracture would influence choice of therapy.

19
Table 3 – Indications for VFA in Men* Post-menopausal women with a T-score of -1.5 to -2.4, and
• Age 80 or older • Historical height loss > 6 cm (2.4 inches) • Prospective height loss of >3 cm (1.2 inches) • Self-reported history of vertebral fracture* • Two or more of the following*:
o Age 70 to 79 o Historical height loss of 3-6 cm o Self-reported prior non-vertebral fracture o Chronic systemic diseases associated with increased risk of vertebral fractures
(for example, moderate to severe COPD, rheumatoid arthritis, Crohn’s disease o Androgen deprivation therapy or following orchiectomy
Men with a T-score of ≤ -2.5 if documentation of a prevalent vertebral fracture would influence choice of or duration of therapy Men of any age on chronic systemic glucocorticoid therapy (dose equivalent to more than 5 mg of prednisone per day) * If the documentation of a vertebral fracture would influence choice of therapy.

20
Figure 1 – Improved VFA imaging with GE Lunar iDXA (right) vs Prodigy (left)
Prodigy
iDXA

21
Figure 2 - Improved VFA imaging with Hologic Discovery (panel A) vs. Hologic
Delphi/QDR (panel B)
Acquisition Time 10 seconds Acquisition Time 15 seconds
Panel A Panel B

22
Figure 3 – Lateral decubitus VFA with poor positioning (left) and good positioning (right)*
*Poor thoracic alignment from shoulder rotation can be recognized by the prominent rib angles posterior to the spine
Poor thoracic alignment
Better alignment
Scapular shadow
23
Figure 4 – Use of triangular pillow to avoid functional scoliosis in side-lying posture
Ribcage support
Buttocks and shoulders firmly against backrest

24
Figure 5 – Improvement in number of evaluable vertebrae on reverse decubitus image

25
Figure 6 – Dual-energy on Prodigy (panel A) and single-energy on Hologic QDR (panel B)
VFA images
Panel A Panel B

26
Figure 7 – Non-osteoporotic deformity in thoracic spine caused by degenerative spondylosis

27
Figure 8 – Non-osteoporotic deformity on VFA due to Schuermann’s disease

28
Figure 9 – Non-osteoporotic deformity due to lack of vertebral segmentation (congenital vertebral fusion)

29
Figure 10 – Non-osteoporotic deformity due to Schmorl’s nodes, note also the calcified disc, a relatively uncommon occurrence.

30
Figure 11 – Metastatic prostate carcinoma at T12 and grade 3 vertebral fracture at T7 on
VFA (left panel) and lateral spine radiograph (right panel)

31
References
1. Black DM, Arden NK, Palermo L, Pearson J, Cummings SR (1999) Prevalent vertebral deformities predict hip fractures and new vertebral deformities but not wrist fractures. Study of Osteoporotic Fractures Research Group. J Bone Miner Res 14:821-828. 2. van der Klift M, de Laet CE, McCloskey EV, Johnell O, Kanis JA, Hofman A, Pols HA (2004) Risk factors for incident vertebral fractures in men and women: the Rotterdam Study. J Bone Miner Res 19:1172-1180. 3. Ross PD, Davis JW, Epstein RS, Wasnich RD (1991) Pre-existing fractures and bone mass predict vertebral fracture incidence in women. Ann Intern Med 114:919-923. 4. Siris ES, Genant HK, Laster AJ, Chen P, Misurski DA, Krege JH (2007) Enhanced prediction of fracture risk combining vertebral fracture status and BMD. Osteoporos Int 18:761-770. 5. McCloskey EV, Vasireddy S, Threlkeld J, Eastaugh J, Parry A, Bonnet N, Beneton M, Kanis JA, Charlesworth D (2008) Vertebral fracture assessment (VFA) with a densitometer predicts future fractures in elderly women unselected for osteoporosis. J Bone Miner Res 23:1561-1568. 6. Cooper C, O'Neill T, Silman A (1993) The epidemiology of vertebral fractures. European Vertebral Osteoporosis Study Group. Bone 14 Suppl 1:S89-97. 7. Fink HA, Milavetz DL, Palermo L, Nevitt MC, Cauley JA, Genant HK, Black DM, Ensrud KE (2005) What proportion of incident radiographic vertebral deformities is clinically diagnosed and vice versa? J Bone Miner Res 20:1216-1222. 8. Greenspan SL, von Stetten E, Emond SK, Jones L, Parker RA (2001) Instant vertebral assessment: a noninvasive dual X-ray absorptiometry technique to avoid misclassification and clinical mismanagement of osteoporosis. J Clin Densitom 4:373-380. 9. Schousboe JT, DeBold CR, Bowles C, Glickstein S, Rubino RK (2002) Prevalence of vertebral compression fracture deformity by X-ray absorptiometry of lateral thoracic and lumbar spines in a population referred for bone densitometry. J Clin Densitom 5:239-246. 10. Melton LJ, 3rd, Lane AW, Cooper C, Eastell R, O'Fallon WM, Riggs BL (1993) Prevalence and incidence of vertebral deformities. Osteoporos Int 3:113-119. 11. Schousboe JT, Ensrud KE, Nyman JA, Kane RL, Melton LJ, 3rd (2006) Cost-effectiveness of vertebral fracture assessment to detect prevalent vertebral deformity and select postmenopausal women with a femoral neck T-score>-2.5 for alendronate therapy: a modeling study. J Clin Densitom 9:133-143.

32
12. Olenginski TP, Newman ED, Hummel JL, Hummer M (2006) Development and evaluation of a vertebral fracture assessment program using IVA and its integration with mobile DXA. J Clin Densitom 9:72-77. 13. Chapurlat RD, Duboeuf F, Marion-Audibert HO, Kalpakcioglu B, Mitlak BH, Delmas PD (2006) Effectiveness of instant vertebral assessment to detect prevalent vertebral fracture. Osteoporos Int 17:1189-1195. 14. Fuerst T, Wu C, Genant HK, von Ingersleben G, Chen Y, Johnston C, Econs MJ, Binkley N, Vokes TJ, Crans G, Mitlak BH (2009) Evaluation of vertebral fracture assessment by dual X-ray absorptiometry in a multicenter setting. Osteoporos Int 20:1199-1205. 15. Damiano J, Kolta S, Porcher R, Tournoux C, Dougados M, Roux C (2006) Diagnosis of vertebral fractures by vertebral fracture assessment. J Clin Densitom 9:66-71. 16. Ferrar L, Jiang G, Schousboe JT, DeBold CR, Eastell R (2008) Algorithm-based qualitative and semiquantitative identification of prevalent vertebral fracture: agreement between different readers, imaging modalities, and diagnostic approaches. J Bone Miner Res 23:417-424. 17. Binkley N, Krueger D, Gangnon R, Genant HK, Drezner MK (2005) Lateral vertebral assessment: a valuable technique to detect clinically significant vertebral fractures. Osteoporos Int 16:1513-1518. 18. Ferrar L, Jiang G, Clowes JA, Peel NF, Eastell R (2008) Comparison of densitometric and radiographic vertebral fracture assessment using the algorithm-based qualitative (ABQ) method in postmenopausal women at low and high risk of fracture. J Bone Miner Res 23:103-111. 19. Rea JA, Li J, Blake GM, Steiger P, Genant HK, Fogelman I (2000) Visual assessment of vertebral deformity by X-ray absorptiometry: a highly predictive method to exclude vertebral deformity. Osteoporos Int 11:660-668. 20. Schousboe JT, Debold CR (2006) Reliability and accuracy of vertebral fracture assessment with densitometry compared to radiography in clinical practice. Osteoporos Int 17:281-289. 21. Buehring B, Krueger D, Checovich M, Gemar D, Vallarta-Ast N, Genant HK, Binkley N (2010) Vertebral fracture assessment: impact of instrument and reader. Osteoporos Int 21(3): 487-494. 22. Hospers IC, van der Laan JG, Zeebregts CJ, Nieboer P, Wolffenbuttel BH, Dierckx RA, Kreeftenberg HG, Jager PL, Slart RH (2009) Vertebral fracture assessment in supine position: comparison by using conventional semiquantitative radiography and visual radiography. Radiology 251:822-828. 23. Vokes TJ, Dixon LB, Favus MJ (2003) Clinical utility of dual-energy vertebral assessment (DVA). Osteoporos Int 14:871-878.

33
24. Schousboe JT, Vokes T, Broy SB, Ferrar L, McKiernan F, Roux C, Binkley N (2008) Vertebral Fracture Assessment: the 2007 ISCD Official Positions. J Clin Densitom 11:92-108. 25. Vogt TM, Ross PD, Palermo L, Musliner T, Genant HK, Black D, Thompson DE (2000) Vertebral fracture prevalence among women screened for the Fracture Intervention Trial and a simple clinical tool to screen for undiagnosed vertebral fractures. Fracture Intervention Trial Research Group. Mayo Clin Proc 75:888-896. 26. Kaptoge S, Armbrecht G, Felsenberg D, Lunt M, O'Neill TW, Silman AJ, Reeve J (2004) When should the doctor order a spine X-ray? Identifying vertebral fractures for osteoporosis care: results from the European Prospective Osteoporosis Study (EPOS). J Bone Miner Res 19:1982-1993. 27. Black DM, Greenspan SL, Ensrud KE, Palermo L, McGowan JA, Lang TF, Garnero P, Bouxsein ML, Bilezikian JP, Rosen CJ (2003) The effects of parathyroid hormone and alendronate alone or in combination in postmenopausal osteoporosis. N Engl J Med 349:1207-1215. 28. Black DM, Schwartz AV, Ensrud KE, Cauley JA, Levis S, Quandt SA, Satterfield S, Wallace RB, Bauer DC, Palermo L, Wehren LE, Lombardi A, Santora AC, Cummings SR (2006) Effects of continuing or stopping alendronate after 5 years of treatment: the Fracture Intervention Trial Long-term Extension (FLEX): a randomized trial. Jama 296:2927-2938. 29. Black DM, Cummings SR, Karpf DB, Cauley JA, Thompson DE, Nevitt MC, Bauer DC, Genant HK, Haskell WL, Marcus R, Ott SM, Torner JC, Quandt SA, Reiss TF, Ensrud KE (1996) Randomised trial of effect of alendronate on risk of fracture in women with existing vertebral fractures. Fracture Intervention Trial Research Group. Lancet 348:1535-1541. 30. Reginster J, Minne HW, Sorensen OH, Hooper M, Roux C, Brandi ML, Lund B, Ethgen D, Pack S, Roumagnac I, Eastell R (2000) Randomized trial of the effects of risedronate on vertebral fractures in women with established postmenopausal osteoporosis. Vertebral Efficacy with Risedronate Therapy (VERT) Study Group. Osteoporos Int 11:83-91. 31. Harris ST, Watts NB, Genant HK, McKeever CD, Hangartner T, Keller M, Chesnut CH, 3rd, Brown J, Eriksen EF, Hoseyni MS, Axelrod DW, Miller PD (1999) Effects of risedronate treatment on vertebral and nonvertebral fractures in women with postmenopausal osteoporosis: a randomized controlled trial. Vertebral Efficacy With Risedronate Therapy (VERT) Study Group. JAMA 282:1344-1352. 32. Chesnut IC, Skag A, Christiansen C, Recker R, Stakkestad JA, Hoiseth A, Felsenberg D, Huss H, Gilbride J, Schimmer RC, Delmas PD (2004) Effects of oral ibandronate administered daily or intermittently on fracture risk in postmenopausal osteoporosis. J Bone Miner Res 19:1241-1249.

34
33. Kanis JA, Johansson H, Oden A, Johnell O, de Laet C, Melton IL, Tenenhouse A, Reeve J, Silman AJ, Pols HA, Eisman JA, McCloskey EV, Mellstrom D (2004) A meta-analysis of prior corticosteroid use and fracture risk. J Bone Miner Res 19:893-899. 34. van Staa TP, Leufkens HG, Cooper C (2002) The epidemiology of corticosteroid-induced osteoporosis: a meta-analysis. Osteoporos Int 13:777-787. 35. Van Staa TP, Laan RF, Barton IP, Cohen S, Reid DM, Cooper C (2003) Bone density threshold and other predictors of vertebral fracture in patients receiving oral glucocorticoid therapy. Arthritis Rheum 48:3224-3229. 36. Naganathan V, Jones G, Nash P, Nicholson G, Eisman J, Sambrook PN (2000) Vertebral fracture risk with long-term corticosteroid therapy: prevalence and relation to age, bone density, and corticosteroid use. Arch Intern Med 160:2917-2922. 37. Pearson D, Horton B, Green DJ, Hosking DJ, Goodby A, Steel SA (2006) Vertebral morphometry by DXA: a comparison of supine lateral and decubitus lateral densitometers. J Clin Densitom 9:295-301. 38. Vallarta-Ast N, Krueger D, Binkley N (2006) Addition of right lateral decubitus positioning improves vertebral visualization with VFA in selected patients. J Clin Densitom 9:375-379. 39. Peel NF, Johnson A, Barrington NA, Smith TW, Eastell R (1993) Impact of anomalous vertebral segmentation on measurements of bone mineral density. J Bone Miner Res 8:719-723. 40. Genant HK, Wu CY, van Kuijk C, Nevitt MC (1993) Vertebral fracture assessment using a semiquantitative technique. J Bone Miner Res 8:1137-1148. 41. Abdel-Hamid Osman A, Bassiouni H, Koutri R, Nijs J, Geusens P, Dequeker J (1994) Aging of the thoracic spine: distinction between wedging in osteoarthritis and fracture in osteoporosis--a cross-sectional and longitudinal study. Bone 15:437-442. 42. Chan KK, Sartoris DJ, Haghighi P, Sledge P, Barrett-Connor E, Trudell DT, Resnick D (1997) Cupid's bow contour of the vertebral body: evaluation of pathogenesis with bone densitometry and imaging-histopathologic correlation. Radiology 202:253-256. 43. Harrington KD (1993) Vertebral compression fractures: differentiation between benign and malignant causes. Iowa Orthop J 13:85-96. 44. Fornasier VL, Czitrom AA (1978) Collapsed vertebrae: a review of 659 autopsies. Clin Orthop Relat Res 261-265. 45. Kanis JA, Barton IP, Johnell O (2005) Risedronate decreases fracture risk in patients selected solely on the basis of prior vertebral fracture. Osteoporos Int 16:475-482.

35
46. Marcus R, Wang O, Satterwhite J, Mitlak B (2003) The skeletal response to teriparatide is largely independent of age, initial bone mineral density, and prevalent vertebral fractures in postmenopausal women with osteoporosis. J Bone Miner Res 18:18-23. 47. McCloskey EV, Johansson H, Oden A, Kanis JA (2009) From relative risk to absolute fracture risk calculation: the FRAX algorithm. Curr Osteoporos Rep 7:77-83. 48. Kanis JA, Oden A, Johansson H, Borgstrom F, Strom O, McCloskey E (2009) FRAX and its applications to clinical practice. Bone 44:734-743. 49. Donaldson MG, Palermo L, Schousboe JT, Ensrud KE, Hochberg MC, Cummings SR (2009) FRAX and risk of vertebral fractures: the fracture intervention trial. J Bone Miner Res 24:1793-1799. 50. Leslie WD, Hans D (2009) On lumpers and splitters: the FRAX debate continues. J Bone Miner Res 24:1789-1792. 51. Wilson PW, Kauppila LI, O'Donnell CJ, Kiel DP, Hannan M, Polak JM, Cupples LA (2001) Abdominal aortic calcific deposits are an important predictor of vascular morbidity and mortality. Circulation 103:1529-1534. 52. Hollander M, Hak AE, Koudstaal PJ, Bots ML, Grobbee DE, Hofman A, Witteman JC, Breteler MM (2003) Comparison between measures of atherosclerosis and risk of stroke: the Rotterdam Study. Stroke 34:2367-2372. 53. van der Meer IM, Bots ML, Hofman A, del Sol AI, van der Kuip DA, Witteman JC (2004) Predictive value of noninvasive measures of atherosclerosis for incident myocardial infarction: the Rotterdam Study. Circulation 109:1089-1094. 54. Schousboe JT, Taylor BC, Kiel DP, Ensrud KE, Wilson KE, McCloskey EV (2008) Abdominal aortic calcification detected on lateral spine images from a bone densitometer predicts incident myocardial infarction or stroke in older women. J Bone Miner Res 23:409-416. 55. Bolland MJ, Wang TK, van Pelt NC, Horne AM, Mason BH, Ames RW, Grey AB, Ruygrok PN, Gamble GD, Reid IR (2009) Abdominal Aortic Calcification on Vertebral Morphometry Images Predicts Incident Myocardial Infarction. J Bone Miner Res. 56. Grundy SM, Cleeman JI, Merz CN, Brewer HB, Jr., Clark LT, Hunninghake DB, Pasternak RC, Smith SC, Jr., Stone NJ (2004) Implications of recent clinical trials for the National Cholesterol Education Program Adult Treatment Panel III guidelines. Circulation 110:227-239. 57. Ferrar L, Jiang G, Eastell R, Peel NF (2003) Visual identification of vertebral fractures in osteoporosis using morphometric X-ray absorptiometry. J Bone Miner Res 18:933-938.

36
© International Osteoporosis Foundation


















