Deficient interleukin-2 responsiveness of T lymphocytes from patients with primary biliary cirrhosis
6
Deficient Interleukin-2 Responsiveness of T Lymphocytes from Patients with Primary Biliary Cirrhosis JOSE LUIS MENENDEZ,~ JOSE ANTONIO GIR6N,2 LUIS MANZAN0,3 AURELIO GARRID0,4 LUIS &3REU,4 AGUSTIN L&BILLOS,~ &BERT0 DURhTEZ4 AND MELCHOR &VAREZ-MON3 'Service of Internal Medicine, Hospital San Agustin, 33400 Auiles, 2Department of Medicine, School of Medicine, Uniuersidad de Cadiz, 11071 Cadiz; 3Hospital Uniuersitario Pn'ncipe de Asturias, Uniuersidad de Alcala de Henares, 28871 Madrid; and 4Seruices of Gastroenterology and Internal Medicine I, Clinica Puerta de Hierro, Uniuersidad Autdnoma, 28035 Madrid, Spain There is increasingevidencethat primarybiliary cir- rhosis is associated with an alteration of the immune @em. Although the cause remains unknown, it has been suggested that the immune system of patients with primary biliary cirrhosis is involved in the patho- genesisof their disease. We have investigated the T-cell function in patients with primary biliary cirrhosis and have found defective phytohemagglutinin-induced T-cell mitogenesis. Likewise, their blastogenic re- sponse to CD3 monoclonal antibody was also de- pressed, although the DNA synthesis induced by stimulation with phorbol esters (12-O-tetradecanoil- phorbol- 13-acetate) plus ionophore (ionomycin) was normal. These alterationscould not be ascribed either to a decreased aynthesis of interleukin-2 or to a de- fective expression of interleukin-2receptor after cel- lular activation. Moreover, this defective proliferative response of T lymphocytes was observed even in the presence of saturating concentrations of exogenous interleukin-2. These results represent evidence of the deficiency in the interleukin-2-dependent pathway found in T lymphocytes from patients with primary biliary Cirrhosis. (HEPMWLOGY 1992; 16931-936.) PBC is a chronic, progressive disease characterized by the inflamaa tory destruction of intrahepatic bile ducts. Although the cause of PBC remains unknown, it has been proposed that a defect in mechanisms of immune system regulation may contribute to the pathogenesis of the disease (1, 2). In line with the concept that the immune system is dynamic and unitary (31, there is increasing evidence of a systemic alteration of immune system function in PBC patients. It has been shown that peripheral blood T lymphocytes from these patients have defective prolif- Received July 5, 1991; accepted May 18, 1992. Supported in part by a grant (no. 92100190202J from the Fondo de Investigaciones de la seguridad Social. Address reprint requests to: M. Alvarez-Mon, M.D., Ph.D., Departamento de Medicina Interna, Facultad de Medicina, Universidad de Al& de Henares, Ald de Hem, 28871 Madrid, Spain. 31/1139489 erative responses to polyclonal mitogens (4-13) such as phytohemagglutinin (PHA). This hypoproliferative re- sponse has been attributed to inhibitory serum factors (4-9) or, according to several authors (10, ll), to an altered distribution of T-lymphocyte subsets. Several distinct steps are involved in the activation of resting T lymphocytes (10, 11). The major pathway of T-cell activation is through the interaction of ap- propriately processed and presented antigens with the T-cell receptor, coupled to its associated CD3 complex (14-16). This interaction results in the expression of interleukin-2 receptor (IL-2r) and secretion of interleukin-2 (IL-2) (17). T-cell mitogenesis is pro- moted by IL-2 after the binding of the cells to their specific receptors. The antigen-T-lymphocyte inter- action can be partially circumvented by the use of polyclonal activators such as plant lectins (181, CD3 monoclonal antibodies (anti-CD3) (19) and protein b a s e C activators (20). For this article we have investigated the mechanisms involved in the defective cellular activation and prolif- eration found in T lymphocytes from PBC patients. In purified T cells from PBC patients and healthy controls, we have analyzed the proliferative response to polyclonal mitogenic signals, the subsequent expression of IL-2r and of other cellular activation antigens and IL-2 production. MATERIALS AND METHODS Popuhtion. Twenty patients with PBC and twenty age- and sex-matched healthy controls were studied (Table 1). Each consented to the experimental protocol. The diagnosis of PBC was established by the presence of a histopathologically compatiblelesion and at least three of the followingcriteria: (a) elevation of serum Ighf levels; (b) increase in Serum alkaline phosphatase activity to more than twice the upper limit of the normal range; (c) presence of antimitochondrial antibodies at titers equal to or greater than 1 : 40; and (d) patency of the biliary tract demonstrated by endoscopic retrograde cholan- giopancreatography, echography or both (21, 22). As deter- mined by the histological study of the biopsy specimens, stage I was found in 20% of cases, stage I1 was found in 30%, stage 93 1
-
Upload
jose-luis-menendez -
Category
Documents
-
view
216 -
download
4
Transcript of Deficient interleukin-2 responsiveness of T lymphocytes from patients with primary biliary cirrhosis

Deficient Interleukin-2 Responsiveness of T Lymphocytes from Patients with Primary Biliary Cirrhosis
JOSE LUIS MENENDEZ,~ JOSE ANTONIO GIR6N,2 LUIS MANZAN0,3 AURELIO GARRID0,4 LUIS &3REU,4 AGUSTIN L&BILLOS,~ &BERT0 D U R h T E Z 4 AND MELCHOR &VAREZ-MON3
'Service of Internal Medicine, Hospital San Agustin, 33400 Auiles, 2Department of Medicine, School of Medicine, Uniuersidad de Cadiz, 11071 Cadiz; 3Hospital Uniuersitario Pn'ncipe de Asturias, Uniuersidad de Alcala de Henares,
28871 Madrid; and 4Seruices of Gastroenterology and Internal Medicine I , Clinica Puerta de Hierro, Uniuersidad Autdnoma, 28035 Madrid, Spain
There is increasing evidence that primary biliary cir- rhosis is associated with an alteration of the immune @em. Although the cause remains unknown, it has been suggested that the immune system of patients with primary biliary cirrhosis is involved in the patho- genesis of their disease. We have investigated the T-cell function in patients with primary biliary cirrhosis and have found defective phytohemagglutinin-induced T-cell mitogenesis. Likewise, their blastogenic re- sponse to CD3 monoclonal antibody was also de- pressed, although the DNA synthesis induced by stimulation with phorbol esters (12-O-tetradecanoil- phorbol- 13-acetate) plus ionophore (ionomycin) was normal. These alterations could not be ascribed either to a decreased aynthesis of interleukin-2 or to a de- fective expression of interleukin-2 receptor after cel- lular activation. Moreover, this defective proliferative response of T lymphocytes was observed even in the presence of saturating concentrations of exogenous interleukin-2. These results represent evidence of the deficiency in the interleukin-2-dependent pathway found in T lymphocytes from patients with primary biliary Cirrhosis. (HEPMWLOGY 1992; 16931-936.)
PBC is a chronic, progressive disease characterized by the inflamaa tory destruction of intrahepatic bile ducts. Although the cause of PBC remains unknown, it has been proposed that a defect in mechanisms of immune system regulation may contribute to the pathogenesis of the disease (1, 2).
In line with the concept that the immune system is dynamic and unitary (31, there is increasing evidence of a systemic alteration of immune system function in PBC patients. It has been shown that peripheral blood T lymphocytes from these patients have defective prolif-
Received July 5, 1991; accepted May 18, 1992. Supported in part by a grant (no. 92100190202J from the Fondo de
Investigaciones de la seguridad Social. Address reprint requests to: M. Alvarez-Mon, M.D., Ph.D., Departamento de
Medicina Interna, Facultad de Medicina, Universidad de Al& de Henares, A l d de H e m , 28871 Madrid, Spain.
31/1139489
erative responses to polyclonal mitogens (4-13) such as phytohemagglutinin (PHA). This hypoproliferative re- sponse has been attributed to inhibitory serum factors (4-9) or, according to several authors (10, ll), to an altered distribution of T-lymphocyte subsets.
Several distinct steps are involved in the activation of resting T lymphocytes (10, 11). The major pathway of T-cell activation is through the interaction of ap- propriately processed and presented antigens with the T-cell receptor, coupled to its associated CD3 complex (14-16). This interaction results in the expression of interleukin-2 receptor (IL-2r) and secretion of interleukin-2 (IL-2) (17). T-cell mitogenesis is pro- moted by IL-2 after the binding of the cells to their specific receptors. The antigen-T-lymphocyte inter- action can be partially circumvented by the use of polyclonal activators such as plant lectins (181, CD3 monoclonal antibodies (anti-CD3) (19) and protein b a s e C activators (20).
For this article we have investigated the mechanisms involved in the defective cellular activation and prolif- eration found in T lymphocytes from PBC patients. In purified T cells from PBC patients and healthy controls, we have analyzed the proliferative response to polyclonal mitogenic signals, the subsequent expression of IL-2r and of other cellular activation antigens and IL-2 production.
MATERIALS AND METHODS Popuhtion. Twenty patients with PBC and twenty age- and
sex-matched healthy controls were studied (Table 1). Each consented to the experimental protocol. The diagnosis of PBC was established by the presence of a histopathologically compatible lesion and at least three of the following criteria: (a) elevation of serum Ighf levels; (b) increase in Serum alkaline phosphatase activity to more than twice the upper limit of the normal range; (c) presence of antimitochondrial antibodies at titers equal to or greater than 1 : 40; and (d) patency of the biliary tract demonstrated by endoscopic retrograde cholan- giopancreatography, echography or both (21, 22). As deter- mined by the histological study of the biopsy specimens, stage I was found in 20% of cases, stage I1 was found in 30%, stage
93 1

932 MENENDEZ ET AL. HEPATOLOGY
A) PBMC
7 * PIC
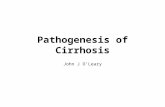
6 ) T cells FIG. 1. Kinetics of the blastogenic response of (A) PBMC and (B) T
lymphocytes from 10 PBC patients and 10 healthy controls to stimulation with PHA for 3, 5 and 7 days. Results are expressed as mean counts per minute t S.D. Statistical differences between the two groups (p < 0.05) were found at 3, 5 and 7 days of culture.
I11 was found in 30% and stage IV was found in 20%. Exclusion criteria for this study were prior treatment with immunosup- pressors; a clinical, epidemiological, serological or pathological sign of liver disease other than PBC; and intercurrent diseases or drugs that could modify the results of the immunological studies performed.
Reagents. Several monoclonal antibodies (MoAb) were used in the studies of phenotypic characterization and activation: OKTll (CD2), OKT3 (CD3), OKT4 (CD4) and OKTB (CD8) (Ortho-mune; Ortho Pharmaceutical Corp., Raritan, NJ); anti-B1 (CD20), anti-Mo2 (CD14) and anti-TAC (CD25) (Coulter Clone; Coulter Immunology, Hialeah, FL); anti-4F2 (donated by A. S. Fauci, National Institutes of Health, Bethesda, MD); and anti-HLA-DR and Leu-llb (CD16) (Becton Dickinson, Mountain View, CAI. Recombinant interleukin-2 (rIL-2) was the gift of Hoffmann-LaRoche (Montclair, NJ).
cell Sepamtion. Peripheral blood mononuclear cells (PBMC) were obtained by Ficoll-Hypaque gradient (Nyegaard
TABLE 1. Characteristics of the 20 PBC patients studied Characteristics Data
Age (yr)" 56 (34-77) Duration of disease (mo)" 62 (56-80) Clinicid manifestationsb
No symptoms 5 (20%) Jaundice 6 (30%) Hepatomegaly 8 (40%) Portal hypertension 6 (30%) ASCiteS 2 (10%)
Bilirubin (mg/dl) 4.3 * 5.6 Alkaline phosphatase (U/dl) 433 t 245 ALT (U/dl) 100 2 46 AST (U/dl) 114 t 62 GGT (U/dl) 191 t 145
93 t 3.8 I& (mddl) 1,162 + 479 IgA (mddl) 259 t 98 IgM (mddl) 531 k 262
Antimitochondrial antibodies > 1 : 40' Antinuclear antibodies > 1 : 4@ 8 (40%)
Laboratory data'
Prothrombin activity (%)
20 (100%)
"Data expressed as mean (range). bData expressed as number of patients (percentage of whole). 'Data expressed as mean t S.D.
TABLE 2. Phenotypic study of the PBMC and purified T cells from PBC patients and controls
Phenotype PBC Control
PBMC T lymphocytes (CD3') 65.2 t 8.0" 66.8 t 6.6 B lymphocytes (CD20+) 13.1 2 3.7 13.9 t 6.7 Monocytes (CD14+) 21.9 t 7.2 20.8 * 8.4 Natural killer cells (CD16+) 17.1 k 4.4 13.7 t 6.6
CD2+ 95.6 f 2.7 96.0 2 3.2 CD3 + 87.4 2 4.2 88.2 t 6.3 CD4 + 56.3 2 8.2 54.7 % 6.6 CD8 + 29.5 t 6.5 30.5 ? 5.7
Purified T lymphocytes
PBMC and purified T lymphocytes were studied by flow cytometry
a second-step fluoresceinated reagent, as indicated in "Materials and Methods." Table depicts the percentage of cells staining above the second-step reagent background.
with OKT3,OKT4, OKT8, OKT11, B1, Mo2 v d Leu-llb MoAb and
"Data expressed as the mean t S.D.
Co., Oslo, Norway). T cells were purified by double rosetting as previously described (23); the purity was greater than 95% in every case. After three cycles of washing in RPMI 1640 medium (Flow Laboratories, Irvine, CAI, cells were counted and resuspended in RPMI 1640 supplemented with 10% heat-inactivated FCS (Gibco, Grand Island, NY), with 2-mercaptoethanol (5 x loL5 mom), with L-glutamine (2 mmom) and with 1% penicillin-gentamicin. They were then checked for viability by trypan blue exclusion. In other experiments supplementation with autologous or pooled AB serum (10% and 20% vol/vol) was performed.
h l i f e m t i o n Studiee. T lymphocytes (50,000 cells/ml) were cultured on 96 flat-bottom culture plates. Soluble PHA 10

Vol. 16, No. 4, 1992 T-LYMPHOCYTE RESPONSE TO IL-2 IN PBC 933
cpm (Thouaandn) 140 r
1201
100 i- T
Banal PHA anti-CDB TPA*lon
cpm (Thousands) , ,
140 i
1 2 0 ,
m PBC = PBC 80
Control @@ Control 60
40
20
0
FIG. 2. Tritiated thymidine uptake by T cells from PBC patients and healthy controls in response to PHA, anti-CD3 or TPA plus ionomycin. Results are expressed as mean counts per minute t S.D. Statistically significant differences were found between the T-cell mitogenic responses of PBC and healthy controls in the presence of PHA (p < 0.05) and anti-CD3 (p < 0.05). However, there were no statisti- cally significant differences (p > 0.05) between PBC and control groups when the mitogenic association TPA plus ionomycin was used.
pg/ml (Difco Laboratories, Detroit, MI); OKT3 5 pdml coupled to bead; or 12-0-tetradecanoil-phorbol-13-acetate (TPA) 10 n g / d (Sigma, St. Louis, MO) plus ionomycin 5 p,g/ml (Sigma) was added at the beginning of proliferation studies. Each reagent was tested in doselresponse titrations before use. Cultures were incubated at 37" C in a humidified atmosphere containing 5% CO, for 3 ,5 and 7 days. Eighteen hr before the end of incubation, 1 KCi of tritiated thymidine (ICN Radio- chemicals, Irvine, CA) was added. The cells were harvested and results expressed as mean counts per minute of triplicate cultures * S.D.
Lpnphokine Pmdmtwn. Lymphokine-enriched superna- tants were obtained by culturing T cells at 37" C at a density of 5 x lo6 /ml in complete medium in the presence or absence of PHA (10 pglml). Supernatants were harvested at 24 and 72 hr of incubation, sterilized by filtration through a 0.22-p,m filter (Millipore Company, Bedford, MA) and stored at - 20" C until use. IL-2 activity was determined in the supernatants by evaluating the dose-dependent proliferation induced in the cytotoxic murine line CTL-L2 by the lymphokine present in the cultures (24).
Immunojluoreecence Analysis. Immunofluorescence stain- ing of cell surface antigens was performed by use of a standard method as previously described (25). Cellular preparations were incubated in the presence of the respective MoAb for 30 min. After two washings, the cells were resuspended in a medium containing fluorescein isothiocyanate-labeled F(ab'), goat anti-mouse I@. Control samples were incubated with the fluorescein isothiocyanate-coupled reagent alone. After a 30-min incubation period, all samples were washed three times and surface immunofluorescence was quantified with an EPICS C flow cytometer (Coulter) equipped with a 2-W argon laser tuned to the 488-nm line. The results of positively stained cells were expressed as the percent of the total PBMC or T-cell population.
Statistical Analysis. The data from the groups were compared by use of the Mann-Whitney U test. A p value of less than 0.05 was considered to indicate a significant difference between groups.
1001- T T
FCS AB Autologous
FIG. 3. Proliferative response of T lymphocytes from PBC patients and controls to stimulation with PHA for 5 days, in the presence of FCS, pooled human Al3 serum or autologous serum at a concentration of 10% or 20% (vol/vol) in the culture medium. Results are expressed as mean counts per minute ~t S.D. No statistical differences (p > 0.05) were detected in the proliferative response of T cells from either group of subjects, regardless of the serum used.
cpm (Thousands) 35 -
30 1 T, 25 1
PBC
Control
20 '
15
10
5
n Banal 24 hour8 72 hours
FIG. 4. IL-2 production by PHA-activated T cells from PBC patients and controls. Results are expressed as mean 2 S.D. No statistical difference was detected between the two groups (p > 0.05).
RESULTS The results of our study are as follows. First, the T-cell
blastogenic response to mitogens that interact with membrane receptors, but not with intracellular mole- cules (protein kinase C and Ca + + ), is diminished in PBC patients. We analyzed the blastogenic response of PBMC from PBC patients and controls to stimulation with PHA. PBMC from PBC patients showed a reduced mitogenesis after PHA stimulation throughout the entire kinetic study (p < 0.05) (Fig. 1A). Next, the kinetics of the proliferative response of purified T lymphocytes to this mitogen were analyzed. A defective blastogenic response of T cells from PBC patients was evident throughout the entire kinetic study (p < 0.05) (Fig. 1B).

934 MENENDEZ ET AL. HEPATOLOGY
FIG. 5. Expression of (A) IL-2r (TAC), (B) glycoprotein 4F2 and (C) major histocompatibility complex-class I1 molecules (DR) on the cytoplasmic membrane of T cells of patients with PBC and healthy controls, under basal conditions and after activation with PHA for 24, 72 or 106 hr. A more marked expression of these antigens (p < 0.05) was detected under basal conditions on the membrane of T cells from PBC patients with respect to that of the controls. Similar results were detected in the two groups (p > 0.05) throughout the entire kinetic study when PHA-stimulated T-cell cultures were analyzed.
In every case the blastogenic response to PHA of purified T cells from the PBC patients was significantly less than that observed in the control population (p < 0.05) (Fig. 2). This hypoproliferative response cannot be ascribed to an alteration in the distribution of the mononuclear populations or of the T-cell subsets studied (Table 2).
The PHA-induced T-lymphocyte blastogenesis was studied simultaneously in a culture medium supple- mented with either FCS, heterologous AB serum or autologous serum. There was no significant difference in the PHA-induced T-cell mitogenic response in either PBC patients or healthy controls, regardless of the serum used (p > 0.05). The defective T-cell blasto- genesis of PBC was found under all the different experimental conditions (p < 0.05) (Fig. 3).
It was found that T lymphocytes from PBC patients have a decreased anti-CD3-induced mitogenesis when compared with those of the controls (p < 0.05). However, the TPA-plus-ionomycin-induced prolifer- ative responses of T cells from PBC patients and healthy controls were similar (p > 0.05) (Fig. 2).
Second, T lymphocytes from PBC patients normally produce IL-2. There was no statistical difference in the low rate of spontaneous production of IL-2 by T cells between PBC patients and healthy controls (p > 0.05). Likewise, similar levels of IL-2 production were found in PHA-stimulated T cells from the two populations (p > 0.05) (Fig. 4).
Third, T lymphocytes from PBC patients present spontaneously enhanced and normal post activation interleukin-2 receptor expression but show deficient blastogenic response to this lymphokine. The membrane expression of IL-2r was analyzed by quantitative flow cytometric studies after T-cell staining with MoAb specific for IL-2r. As shown in Figure 5, nonstimulated T cells from PBC patients show an enhanced basal expression of IL-2r on their cytoplasmic membrane (p < 0.05). However, after PHA stimulation, the pro- portion of cells stained by this antigen was similar in the T-cell cultures from PBC patients and from healthy controls (p > 0.05). Similar patterns were also found in the T-cell membrane expression of 4F2 glycoprotein and HLA-DR molecules.

Vol. 16, No. 4, 1992 T-LYMPHOCYTE RESPONSE TO IL-2 IN PBC 935
TABLE 3. Effect of supplementation with rIL-2 on the blaetogenic response of T lymphocytes of patients with PBC and controls in the presence or absence of PHA
rIL-2 (U/ml)
Subjects 0 10 100
PBC patients (n = 20) PHA 0 Fg/mI 540 f 402” 3,623 f 2,984 7,238 5 4,202 PHA 10 pg/ml 42,900 f 15,584 40,572 ? 18,417 44,279 f 17,813
PHA 0 pg/d 642 f 350 4,608 f 3,374 8,052 t 5,363 PHA 10 pg/d 85,052 f 16,778 88,639 f 24,826 84,641 ? 21,172
Controls (n = 20)
“Data expressed as mean counts per minute t S.D
Despite the spontaneously enhanced expression of IL-2r on the membranes of T lymphocytes from PBC patients, the patients’ proliferative responses to stimu- lation with saturating amounts of exogenous rIL-2 did not differ from those of healthy controls (p > 0.05). Moreover, the exogenous addition of saturating concen- trations of rIL-2 to the PHA-stimulated T-cell cultures from PBC patients neither normalized nor sigdicantly increased their defective blastogenic response (p > 0.05) (Table 3).
DISCUSSION The results of this study demonstrate that PBC
patients have a defective T-lymphocyte blastogenesis after mitogenic stimulation. This hypoproliferative re- sponse cannot be ascribed to either a suppressive effect of non-T cells, an anomalous distribution of CD4 and CD8 T-cell subsets or the presence of a soluble inhibitory factor in the patients’ sera. Previous investigations have shown the anomalous distribution of these T-cell subsets (10, 11) and the presence of inhibitory soluble factors (4-9). The discrepancies with respect to our data could be related to the selection criteria and to the different clinical characteristics of the patients studied.
Remarkably, the T-cell hypoproliferative response was observed not only with PHA, but also on direct stimulation with MoAb against the CD3 complex. However, normal T-cell proliferation was found after direct activation of protein kinase C (by TPA) and calcium mobilization (by ionomycin). These findings strongly suggest that T cells from PBC patients have a functional defect in a step proximate to the generation of second messengers (protein kinase C and ionic calcium) of the T-lymphocyte activation.
It is relevant that this functional abnormality is associated with neither a defective production of IL-2 by T cells nor a decreased expression of IL-2r. Moreover, a defective PHA-induced proliferative response was ob- served even in the presence of saturating amounts of exogenous rIL-2. These results suggest that an alter- ation in the metabolic process, subsequent to the activation of the cytoplasmic membrane receptors of T lymphocytes implicated in the regulation of the cell cycle, could be involved in their defective mitogenesis.
In this article, we have also demonstrated that in uiuo T cells from PBC patients express cytoplasmic mem-
brane antigens associated with cell activation. It has been hypothesized that the damage of the liver filter could expose the peripheral blood T cells from patients with several liver diseases to an increased antigenic charge (2). However, data of our group have demon- strated the absence of activation markers on T cells from alcoholic cirrhotic patients (Girbn JA, Manuscript in preparation, 1992). The in uiuo activation of T cells and their simultaneous functional abnormality in the pro- liferative IL-2 pathway have been demonstrated in other autoimmune diseases such as systemic lupus erythema- tosus (26, 27). These functional alterations of T lym- phocytes can be associated with an abnormal regulation of the T-cell effedor mechanisms that could be involved in the pathogenetic sequence leading to the liver lesion described in PBC patients.
Acknowledgments: We thank Ms. C. Lorences and Ms. G. Peraile for their skillful technical assistance and Ms. M. Messman for her expert editorial assistance.
1.
2.
3.
4.
5.
6.
7.
8.
REFERENCES
Kaplan MM. Primary biliary cirrhosis. N Engl J Med 1987;316:
James SP, Hoofnagle JH, Strober W, Jones EA. Primary biliary cirrhosis: a model autoimmune disease. Ann Intern Med 1983;99:
Marms MAR, Toribio ML, de la Hera A, Mdrquez C, Gaspar ML, Martinez-A C. Mutual cell interactions and the selection of immune repertoires: implication in autoimmunity. Immunol
MacSween RNM, Galbrait I, Thomas MA, Watkinson G, Ludlam GB. Phytohemagglutinin (PHA) induced transformation and Tomplasma gondii antibody studies in primary biliary cirrhosis. Evidence of impaired cell-mediated immunity. Clin Exp Immunol
Fox RA, Dudley FJ, Samuels M, Milligan J, Sherlock S. Lym- phocyte transformation in response to phytohemagglutinin in primary biliary cirrhosis: the search for a plasma inhibitory fador.
Newberry WM, Shorey JW, Sanford JP, Combes B. Depression of lymphocyte reactivity to phytohemagglutinin by serum from patients with liver disease. Cell Immunol 1973;6:87-97. Gianni L, Padova F, Zuin M, Podda M. Bile acid-induced inhibition of the lymphoproliferative response to phytohemagglu- tinin and pokeweed mitogen: an in vitro study. Gastroenterology
Logie SA, Quigley EM, MacSween RN, Sandilands GP. Serum mediated inhibition of T-cell activation in primary biliary cir- rhosis. J Immunol 1982;129:81-85.
521-528.
500-512.
Today 1988;9:204-207.
1973;15:35-42.
Gut 1973;14:89-93.
1980;78:231-235.

936 MENENDEZ ET AL. HEPATOLOGY
9. Behrens U, Friedrich I, Vernace S, Schaffner F, Paronetto F. Lymphocyte responsiveness per unit of volume of blood in patients with nonalcoholic and alcoholic liver disease. Plasma inhibitory factors and functional defects of responder cells. J Clin Lab Immunol 1982;8:143-152.
10. Routhier G, Epstein 0, Janossy G, Thomas HC, Sherlock S. Effects of cyclosporin A on suppressor and inducer T lymphocytes in primary biliary cirrhosis. Lancet 1980;2:1223-1226.
11. Miller KB, Elta GH, Rudders RA, Kaplan MM. Lymphocyte subsets in primary biliary cirrhosis. Ann Intern Med 1984;lOO:
12. Cancellerini V, Scaroni C, Vernace SJ, Schaffner F, Paronetto F. Subpopulations of T lymphocytes in primary biliary cirrhosis. Clin Immunol Immunopathol 1981;20:255-260.
13. Kershenobich D, Alcocer J , Quiroga A, Rojkind M. Effect of mlchicine on immunoregulatory T-lymphocytes and monocytes in patients with primary biliary cirrhosis. Clin Res 1984;32:490A.
14. Allison JP, Lanier LL. Structure, function and serology of the T-cell antigen receptor complex. Annu Rev Immunol 1987;5:
15. Goverman J , Hunkapiller T, Hood L. A speculative view of the multicomponent nature of T-cell antigen recognition. Cell 1986; 45:475-484.
16. Isakov N, Scholz W, Altman A. Signal transduction and intracel- lular events in T lymphocyte activation. Immunol Today 1986;7:
17. Waldmann TA. The structure, function and expression of IL-2 receptors on normal and malignant lymphocytes. Science 1986;
18. Mills GB, Lee JWW, Cheung RK, Gelfand EW. Characterization of the requirements for human T cell mitogenesis by using subop-
385-387.
503-540.
271-277.
232:727-732.
timal concentrations of phytohemagglutinin. J Immunol 1985;
19. Davis L, Vida R, Lipsky PE. Regulation of human T lymphocyte mitogenesis by antibodies to CD3. J Immunol 1986;137:3758- 3767.
20. Droge W. Protein kinase C in T cell regulation. Immunol Today
21. Moreno D, Solis JA, Colina F, Martinez MP, Cuenca B, Shuller A. Manifestaciones sist6micas de la cirrosis biliar primaria. Med Clin
22. Klatskin G, Kantor FS. Mitochondrial antibody in primary biliary cirrhosis and other diseases. Ann Intern Med 1972;77:533-541.
23. Alvarez-Mon M, Casas J , Laguna R, Toribio ML, Ortiz de Landburi M, Durhtez A. Lymphokine induction of NK-like cytotoxicity in T cells from B-CLL. Blood 1986;67:228-232.
24. Gillis S, Ferm M, Ou W, Smith K. T cell growth factor: param- eters of production and a quantitative microassay for activity. J Immunol 1978;120:2027-2032.
25. AlBs-Martinez J, Alvarez-Mon M, Merino F, Bonilla F, Martinez- A C, Durhtez A, de la Hera A. Decreased TcR-CD3+ T cell numbers in healthy aged humans. Evidence that T cell defects are masked by a reciprocal increase in TcR-CD3-CD2+ natural killer cells. Eur J Immunol 1988;18:1827-1830.
26. Cohen PL, Litvin DA, Winfield JB. Association between endoge- nously activated T cells and immunoglobulin-secreting B cells in patients with active systemic lupus erythematosus. Arthritis Rheum 1982;25:168-173.
27. Gaspar ML, Alvarez-Mon M, GutiBrrez C. B cell activation pathway in human systemic lupus erythematosus (SLE): imbal- anced in vitro production of lymphokines and association with serum analytical findings. J Clin Immunol 1988;8:266-274.
135~3087-3093.
1987;8:46-51.
(Bart) 1986;87:265-270.