Davis Ecg Notes
215
-
Upload
yucef-bahian-abang -
Category
Documents
-
view
208 -
download
11
description
A book for ECG review
Transcript of Davis Ecg Notes
-
Contacts Phone/E-Mail
Name
Ph: e-mail:
Name
Ph: e-mail:
Name
Ph: e-mail:
Name
Ph: e-mail:
Name
Ph: e-mail:
Name
Ph: e-mail:
Name
Ph: e-mail:
Name
Ph: e-mail:
Name
Ph: e-mail:
Name
Ph: e-mail:
Name
Ph: e-mail:
Name
Ph: e-mail:
2142_FM_ii-vi.qxd 9/12/09 2:39 PM Page ii
-
ECGECGNotesNotesInterpretation and Management Guide
Shirley A. Jones, MS Ed, MHA, EMT-P
Purchase additional copies of this book at yourhealth science bookstore or directly from F.A. Davisby shopping online at www.fadavis.com or by calling 800-323-3555 (US) or 800-665-1148 (CAN)
A Daviss Notes Book
2nd Edition
2142_FM_ii-vi.qxd 9/12/09 2:39 PM Page iii
-
F. A. Davis Company1915 Arch StreetPhiladelphia, PA 19103www.fadavis.com
Copyright 2010 by F. A. Davis Company
All rights reserved. This book is protected by copyright. No part of it may be reproduced, storedin a retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopying, recording, or otherwise, without written permission from the publisher.
Printed in China by Imago
Last digit indicates print number: 10 9 8 7 6 5 4 3 2 1
Publisher, Nursing: Lisa B. DeitchDirector of Content Development: Darlene D. PedersenProject Editor: Christina C. BurnsCover Design: Carolyn OBrienReviewers: Jill M. Mayo, RN, MSN, ACLS; Jill Scott, RN, MSN, CCRN; Patricia Sweeney, MS,CRNP, FNP, BC; Barbara Tacinelli, RN, MA
As new scientific information becomes available through basic and clinical research, recom-mended treatments and drug therapies undergo changes. The author(s) and publisher have doneeverything possible to make this book accurate, up to date, and in accord with accepted stan-dards at the time of publication. The author(s), editors, and publisher are not responsible forerrors or omissions or for consequences from application of the book, and make no warranty,expressed or implied, in regard to the contents of the book. Any practice described in this bookshould be applied by the reader in accordance with professional standards of care used in regardto the unique circumstances that may apply in each situation. The reader is advised always tocheck product information (package inserts) for changes and new information regarding doseand contraindications before administering any drug. Caution is especially urged when usingnew or infrequently ordered drugs.
Authorization to photocopy items for internal or personal use, or the internal or personal use ofspecific clients, is granted by F. A. Davis Company for users registered with the CopyrightClearance Center (CCC) Transactional Reporting Service, provided that the fee of $.25 per copy ispaid directly to CCC, 222 Rosewood Drive, Danvers, MA 01923. For those organizations that havebeen granted a photocopy license by CCC, a separate system of payment has been arranged. Thefee code for users of the Transactional Reporting Service is: 8036-2142-6/10 0 $.25.
2142_FM_ii-vi.qxd 9/12/09 2:39 PM Page iv
-
BASICS ECGS
TOOLS
12-LEAD MEDS SKILLS CPR ACLS PALS
HIPAA Compliant OSHA Compliant
Waterproof and ReusableWipe-Free Pages
Write directly onto any page of ECG Notes 2ewith a ballpoint pen. Wipe old entries off
with an alcohol pad and reuse
TEST STRIPS
2142_FM_ii-vi.qxd 9/12/09 2:39 PM Page v
-
Look for our other Daviss Notestitles, available now!
RNotes: Nurses Clinical PocketGuide, 2nd edition
ISBN-13: 978-0-8036-1335-5
LPN Notes: Nurses Clinical PocketGuide, 2nd edition
ISBN-13: 978-0-8036-1767-4
DocuNotes: Nurses ClinicalPocket Guide to Effective
Documenting and ReportingISBN-13: 978-0-8036-2092-6
IV Med Notes: IV AdministrationPocket Guide
ISBN-13: 978-0-8036-1466-8
IV Therapy Notes: Nurses Clinical Pocket Guide
ISBN-13: 978-0-8036-1288-4
LabNotes: Guide to Lab &Diagnostic Tests, 2nd editionISBN-13: 978-0-8036-2138-1
MedNotes: Nurses PharmacologyPocket Guide, 2nd Edition
ISBN-13: 978-0-8036-1531-1
MedSurg Notes: Nurses ClinicalPocket Guide, 2nd edition
ISBN-13: 978-0-8036-1868-8
NCLEX-RN Notes: Core Review& Exam Prep
ISBN-13: 978-0-8036-1570-0
NutriNotes: Nutrition & DietTherapy Pocket Guide
ISBN-13: 978-0-8036-1114-6
OB Peds Womens Health Notes:Nurses Clinical Pocket GuideISBN-13: 978-0-8036-1466-6
PsychNotes: Clinical PocketGuide, 2nd edition
ISBN-13: 978-0-8036-1853-4
Critical Care Notes: Clinical Pocket Guide
ISBN-13: 978-0-8036-2084-1
Assess Notes: Assessment andDiagnostic Reasoning
ISBN-13: 978-0-8036-1749-0
Also from Shirley A. Jones
Pocket Anatomy & PhysiologyISBN-13: 978-0-8036-1824-4
ECG Success: Exercises in ECG InterpretationISBN-13: 978-0-8036-1577-9
For a complete list of Daviss Notes and other titles for health care providers, visit www.fadavis.com.
2142_FM_ii-vi.qxd 9/12/09 2:39 PM Page vi
-
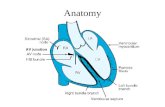
Anatomy of the Heart
The heart, a fist-sized muscular organ located in the mediastinum, is thecentral structure of the cardiovascular system. It is protected by the bonystructures of the sternum anteriorly, the spinal column posteriorly, and therib cage. The heart is roughly conical, with the base of the cone at the topof the heart and the apex (the pointed part) at the bottom. It is rotatedslightly counterclockwise, with the apex tipped anteriorly so that the backsurface of the heart actually lies over the diaphragm.
1
BASICS
Location of the heart
Clinical Tip: The cone-shaped heart has its tip (apex) just above thediaphragm to the left of the midline. This is why we may think of the heartas being on the left sidethe strongest beat can be heard or felt there.
2142_Tab01_001-031.qxd 9/12/09 2:13 PM Page 1
-
BASICS
2
Layers of the Heart
The heart is composed of several different layers of tissue. Surrounding theheart itself is a protective sac called the pericardium. This double-walled sachas an inner, serous (visceral) layer and an outer, fibrous (parietal) layer.Between these layers is the pericardial cavity, which contains a smallamount of lubricating fluid to prevent friction during heart contraction. Thelayers of the heart wall itself include the epicardium, or outermost layer; themyocardium, the thick middle layer of cardiac muscle; and the endocardium,the smooth layer of connective tissue that lines the inside of the heart.
EndocardiumParietalpericardiumMyocardium(heart muscle)
Epicardium(visceral pericardium)
Fibrous pericardium(pericardial sac)
Pericardial cavityLayers of the heart
Clinical Tip: The pericardial cavity contains a small amount of lubricat-ing fluid to prevent friction during heart contraction.
2142_Tab01_001-031.qxd 9/12/09 2:13 PM Page 2
-
Heart Valves
Properties of Heart Valves Fibrous connective tissue prevents enlargement of valve openings
and anchors valve flaps. Valve closure prevents backflow of blood during and after contraction.
3
BASICS
Pulmonary semilunarvalve
Aortic semilunarvalve Tricuspid
valve
Fibrousskeleton
Mitral valve
Posterior
Coronary artery
Superior view with atria removed
2142_Tab01_001-031.qxd 9/12/09 2:13 PM Page 3
-
BASICS
4
Heart C
ham
bers an
d G
reat Vessels
The heart is a hollow m
uscle with an internal skeleton of connective tissue that creates four separate cham
bers.The superior cham
bers of the heart are the right and left atria. Their primary function is to collect blood as it
enters the heart and to help fill the lower cham
bers. The more thickly m
uscled lower cham
bers of the heart arethe ventricles. These are the prim
ary pumping cham
bers, the left having a thicker myocardial layer than the right.
Brachiocephalic
artery
Superior ven
a ca
va
Left comm
on carotid arteryLeft subcla
vian arteryAortic arch
Right
pulmonary artery
Right
p u lmo n a ry v e in s
Right atrium
Inferior ve
na
cava
Tricuspidvalve
Pu lmo n a ry
s em
ilu n a r v a lv e
Left pulmonary artery
Left atriumL e ft p u lm
o n a ry v e in sM
itra l v a lv eL e ft v e
n tric leAortic sem
ilunarvalveInterve
ntricularseptum
Apex
Chordaetendineae
Right
ventricle
Papi l lary
mu
scl esH
eartAn
terior sectio
n (arro
ws sh
ow
directio
n o
f blo
od
flow
)
2142_Tab01_001-031.qxd 9/12/09 2:13 PM Page 4
-
Co
ron
ary Arteries an
d V
eins
Th
e coro
nary arteries an
d vein
s pro
vide b
loo
d to
the h
eart mu
scle and
the electrical co
nd
uctio
n sys-
tem. T
he left an
d rig
ht co
ron
ary arteries are the first to
bran
ch o
ff the ao
rta, just ab
ove th
e leafletso
f the ao
rtic valve.
5
BASICS
AortaLeft coronary artery
Anteriordescending bra
nch Coronary sin
us
Posterior
arte ry a n d
v e in
Small
cardiac vein
Right coronary artery
AB
Circumfle
x branch
Great cardiac
vein
Right coronary vein
(A) A
nterio
r view(B
) Po
sterior view
2142_Tab01_001-031.qxd 9/12/09 2:13 PM Page 5
-
Anatomy of the Cardiovascular System
The cardiovascular system is a closed system consisting of the heart andall the blood vessels. Arteries and veins are connected by smaller struc-tures that transport substances needed for cellular metabolism to bodysystems and remove the waste products of metabolism from those sametissues. Arteries carry blood away from the heart and, with the exceptionof the pulmonary arteries, transport oxygenated blood. Veins move bloodtoward the heart. With the exception of the pulmonary veins, they carryblood that is low in oxygen and high in carbon dioxide.
BASICS
6
Tunicaexterna
External elasticlamina Tunica
media
Internal elasticlamina Endothelium (lining)
Artery ArterioleEndothelial
cellsSmoothmuscle
Precapillarysphincter
Capillary
Blood flowVenule
Vein
Valve
Tunicaintima
Tunicaexterna
Tunicamedia
Blood vesselsCross-section
2142_Tab01_001-031.qxd 9/12/09 2:13 PM Page 6
-
Cardiovascular SystemMajor Arteries
7
BASICS
OccipitalInternal carotid
VertebralBrachiocephalic
Aortic arch
MaxillaryFacialExternal carotid
Common carotidSubclavian
AxillaryPulmonary
CeliacLeft gastricHepaticSplenic
Superiormesenteric
Abdominal aortaRight common
iliacInternal iliacExternal iliac
Femoral
Popliteal
Anterior tibial
Posterior tibial
IntercostalBrachialRenal
GonadalInferior mesentericRadialUlnarDeep palmar arch
Superficialpalmar arch
Deep femoral
2142_Tab01_001-031.qxd 9/12/09 2:13 PM Page 7
-
BASICS
8
Cardiovascular SystemMajor Veins
Superior sagittal sinusInferior sagittal sinusStraight sinusTransverse sinusVertebral
External jugularInternal jugular
SubclavianBrachiocephalic
PulmonaryHepaticHepatic portalLeft gastric
RenalSplenicInferiormesentericInternal iliac
Femoral
External iliac
Great saphenous
Popliteal
Small saphenous
Anterior tibial
Anterior facial
Superior vena cava
AxillaryCephalic
HemiazygosIntercostal
Inferior vena cavaBrachial
BasilicGonadal
Superiormesenteric
Dorsal arch
Volar digital
Dorsal arch
Common iliac
2142_Tab01_001-031.qxd 9/12/09 2:13 PM Page 8
-
Properties of Cardiac Cells
Property AbilityAutomaticity Generates electrical impulse independently, without
involving the nervous system.Excitability Responds to electrical stimulation.Conductivity Passes or propagates electrical impulses from cell to cell.Contractility Shortens in response to electrical stimulation.
Mechanics of Heart Function
Process ActionCardiac Sequence of events in 1 heartbeat. Blood is pumpedcycle through the entire cardiovascular system.Systole Contraction phaseusually refers to ventricular contraction.Diastole Relaxation phasethe atria and ventricles are filling. Lasts
longer than systole.Stroke Amount of blood ejected from either ventricle in a single volume contraction. Starling's Law of the Heart states that the degree (SV) of cardiac muscle stretch can increase the force of ejected
blood. More blood filling the ventricles increases SV. Cardiac Amount of blood pumped through the cardiovascular output (CO) system per min. CO = SV x Heart rate (HR)
Physiology of the Heart
Normal blood flow through the heart begins at the right atrium, which receivessystemic venous blood from the superior and inferior venae cavae. Bloodpasses from the right atrium, across the tricuspid valve, to the right ventricle.It is then pumped across the pulmonary valve into the pulmonary arteries.
Outside the heart, the left and right pulmonary arteries distribute blood tothe lungs for gas exchange in the pulmonary capillaries. Oxygenated bloodreturns to the left atrium through the left and right pulmonary veins. Afterpassing across the mitral valve, blood enters the left ventricle, where it ispumped across the aortic valve, through the aorta, into the coronary arteriesand the peripheral circulation.
9
BASICS
2142_Tab01_001-031.qxd 9/12/09 2:13 PM Page 9
-
BASICS
10
Systolic and Diastolic Phases in the Heart
Left atrium
Pulmonaryartery
Aorta
Diastole
Atrial systolic phase Ventricular systolic phase
PulmonaryveinSuperior
vena cava
Right atrium
Pulmonaryvalve
Tricuspidvalve
Right ventricle
Inferiorvena cava
Aortic valveMitral valveLeft ventricle
Septum
Papillarymuscle
2142_Tab01_001-031.qxd 9/12/09 2:13 PM Page 10
-
11
BASICS
Electrical Conduction System of the Heart
Electrophysiology
Structure Function and LocationSinoatrial (SA or sinus) Dominant pacemaker of the heart, located in node upper portion of right atrium. Intrinsic rate
60100 bpm.Internodal pathways Direct electrical impulses between the SA and
AV nodes and spread them across the atrialmuscle.
Atrioventricular (AV) Part of the AV junctional tissue, which includes node some surrounding tissue plus the connected bun-
dle of His. The AV node slows conduction, creatinga slight delay before electrical impulses are carriedto the ventricles. The intrinsic rate is 4060 bpm.
Bundle of His At the top of the interventricular septum, this bun-dle of fibers extends directly from the AV nodeand transmits impulses to the bundle branches.
Left bundle branch Conducts electrical impulses to the left ventricle. Right bundle branch Conducts electrical impulses to the right ventricle. Purkinje system The bundle branches terminate with this network of
fibers, which spread electrical impulses rapidlythroughout the ventricular walls. The intrinsic rate is 2040 bpm.
Bundle of His
Left bundlebranch
Purkinjefibers
Right bundlebranch
AV Node
SA NodeInternodalpathways
Conduction system of the heart
Continued
2142_Tab01_001-031.qxd 9/12/09 2:13 PM Page 11
-
Electrophysiology
Action EffectDepolarization The electrical charge of a cell is altered by a shift of
electrolytes on either side of the cell membrane. Thischange stimulates muscle fiber to contract.
Repolarization Chemical pumps re-establish an internal negativecharge as the cells return to their resting state.
Electrical Conduction System of the Heartcontd
BASICS
12
The Depolarization Process
A
B
C
D
(A) A single cell has depolarized. (B) A wave propagates from cell to cell. (C)Wave propagation stops when all cells are depolarized. (D) Repolarizationrestores each cell's normal polarity.
2142_Tab01_001-031.qxd 9/12/09 2:13 PM Page 12
-
Progression of Depolarization Through the Heart
13
BASICS
+ +++
+ ++++
++
++
++
++
+
+ +
+
+
++
++
SANode
Atrialdepolarization
Apicaldepolarization
Left ventriculardepolarization
Septaldepolarization
AVNode
2142_Tab01_001-031.qxd 9/12/09 2:13 PM Page 13
-
Clinical Tip: Mechanical and electrical functions of the heart are influ-enced by proper electrolyte balance. Important components of this balanceare sodium, calcium, potassium, and magnesium.
BASICS
14
Correlation of Depolarization and Repolarization With the ECG
R
P T
QS
Ventriculardepolarization
Ventricularrepolarization
Atrialdepolarization
2142_Tab01_001-031.qxd 9/12/09 2:13 PM Page 14
-
The Electrocardiogram (ECG)
The body acts as a giant conductor of electrical current. Electrical activity thatoriginates in the heart can be detected on the body's surface through anelectrocardiogram (ECG). Electrodes are applied to the skin to measure volt-age changes in the cells between the electrodes. These voltage changes areamplified and visually displayed on an oscilloscope and graph paper.
An ECG is a series of waves and deflections recording the heart'selectrical activity from a certain "view."
Many views, each called a lead, monitor voltage changes betweenelectrodes placed in different positions on the body.
Leads I, II, and III are bipolar leads and consist of two electrodes ofopposite polarity (positive and negative). The third (ground) electrodeminimizes electrical activity from other sources.
Leads aVR, aVL, and aVF are unipolar leads and consist of a singlepositive electrode and a reference point (with zero electrical potential)that lies in the center of the heart's electrical field.
Leads V1V6 are unipolar leads and consist of a single positive electrodewith a negative reference point found at the electrical center of the heart.
An ECG tracing looks different in each lead because the recordedangle of electrical activity changes with each lead. Different anglesallow a more accurate perspective than a single one would.
The ECG machine can be adjusted to make any skin electrode positiveor negative. The polarity depends on which lead the machine isrecording.
A cable attached to the patient is divided into several different-coloredwires: three, four, or five for monitoring purposes, or ten for a 12-lead ECG.
Incorrect placement of electrodes may turn a normal ECG tracing intoan abnormal one.
Clinical Tip: It is important to keep in mind that the ECG shows onlyelectrical activity; it tells us nothing about how well the heart is workingmechanically.
Clinical Tip: Patients should be treated according to their symptoms,not merely their ECG.
Clinical Tip: To obtain a 12-lead ECG, four wires are attached to eachlimb and six wires are attached at different locations on the chest. Thetotal of ten wires provides 12 views (12 leads).
15
BASICS
2142_Tab01_001-031.qxd 9/12/09 2:13 PM Page 15
-
BASICS
16
Limb Leads
Electrodes are placed on the right arm (RA), left arm (LA), right leg (RL),and left leg (LL). With only four electrodes, six leads are viewed. Theseleads include the standard leadsI, II, and IIIand the augmentedleadsaVR, aVL, and aVF.
Standard Limb Lead Electrode Placement
LARA
or
RL LL
RA LA
LLRL
2142_Tab01_001-031.qxd 9/12/09 2:13 PM Page 16
-
Elements of Standard Limb Leads
Lead Positive Electrode Negative Electrode View of HeartI LA RA LateralII LL RA InferiorIII LL LA Inferior
Standard Limb Leads
Leads I, II, and III make up the standard leads. If electrodes are placed on theright arm, left arm, and left leg, three leads are formed. If an imaginary lineis drawn between each of these electrodes, an axis is formed between eachpair of leads. The axes of these three leads form an equilateral triangle withthe heart in the center (Einthoven's triangle).
17
BASICS
I
IIIII
LL
RA LA
Clinical Tip: Lead II is commonly called a monitoring lead. It providesinformation on heart rate, regularity, conduction time, and ectopic beats.The presence or location of an acute myocardial infarction (MI) should befurther diagnosed with a 12-lead ECG.
2142_Tab01_001-031.qxd 9/12/09 2:13 PM Page 17
-
Elements of Augmented Limb Leads
Lead Positive Electrode View of Heart aVR RA NoneaVL LA LateralaVF LL Inferior
BASICS
18
Augmented Limb Leads
Leads aVR, aVL, and aVF make up the augmented leads. Each letter ofan augmented lead refers to a specific term: a = augmented; V = voltage;R = right arm; L = left arm; F = foot (the left foot).
LL
RA LA
aVR aVL
aVF
2142_Tab01_001-031.qxd 9/12/09 2:13 PM Page 18
-
Elements of Chest Leads
Lead Positive Electrode Placement View of Heart
V1 4th Intercostal space to right of sternum Septum
V2 4th Intercostal space to left of sternum Septum
V3 Directly between V2 and V4 Anterior
V4 5th Intercostal space at left midclavicular line Anterior
V5 Level with V4 at left anterior axillary line Lateral
V6 Level with V5 at left midaxillary line Lateral
Chest Leads
Standard Chest Lead Electrode Placement
The chest leads are identified as V1, V2, V3, V4, V5, and V6. Each electrodeplaced in a "V" position is positive.
19
BASICS
Midclavicularline
V1 V2V3 V4
V5
V6
Anterioraxillary line
Midaxillaryline
2142_Tab01_001-031.qxd 9/12/09 2:13 PM Page 19
-
Electrode Placement Using a 5-Wire Cable
BASICS
20
Electrode Placement Using a 3-Wire Cable
RA LA
LL
RA LA
LLRL
V1
Clinical Tip: Five-wire telemetry units are commonly used to monitorleads I, II, II, aVR, aVL, aVF, and V1 in critical care settings.
2142_Tab01_001-031.qxd 9/12/09 2:13 PM Page 20
-
Modified Chest Leads
Modified chest leads (MCL) are useful in detecting bundle branchblocks and premature beats.
Lead MCL1 simulates chest lead V1 and views the ventricular septum. Lead MCL6 simulates chest lead V6 and views the lateral wall of the
left ventricle.
21
BASICS
G
Lead MCL1 electrode placement
G
Lead MCL6 electrode placement
Clinical Tip: Write on the rhythm strip which simulated lead was used.
2142_Tab01_001-031.qxd 9/12/09 2:13 PM Page 21
-
The Right-sided 12-Lead ECG
Chest Leads PositionV1R 4th Intercostal space to left of sternumV2R 4th Intercostal space to right of sternumV3R Directly between V2R and V4RV4R 5th Intercostal space at right midclavicular lineV5R Level with V4R at right anterior axillary lineV6R Level with V5R at right midaxillary line
The Right-sided 12-Lead ECG
The limb leads are placed as usual but the chest leads are a mirrorimage of the standard 12-lead chest placement.
The ECG machine cannot recognize that the leads have beenreversed. It will still print "V1V6" next to the tracing. Be sure to crossthis out and write the new lead positions on the ECG paper.
BASICS
22
Midclavicularline
Anterioraxillary line
Midaxillaryline
V6R
V4R
V5RV1RV2R
V3R
Clinical Tip: Patients with an acute inferior MI should have right-sidedECGs to assess for possible right ventricular infarction.
2142_Tab01_001-031.qxd 9/12/09 2:13 PM Page 22
-
The 15-Lead ECG
Chest Leads Electrode Placement View of Heart
V4R 5th Intercostal space in right anterior Right ventriclemidclavicular line
V8 Posterior 5th intercostal space in left Posterior wall of midscapular line left ventricle
V9 Directly between V8 and spinal column Posterior wall ofat posterior 5th intercostal space left ventricle
The 15-Lead ECG
Areas of the heart that are not well visualized by the six chest leads includethe wall of the right ventricle and the posterior wall of the left ventricle. A15-lead ECG, which includes the standard 12 leads plus leads V4R, V8, andV9, increases the chance of detecting an MI in these areas.
23
BASICS
V9
Spinalcolumn
Leftshoulder
V8
V6
V6 V8 V9V4R
Clinical Tip: Use a 15-lead ECG when the 12-lead is normal but the his-tory is still suggestive of an acute infarction.
2142_Tab01_001-031.qxd 9/12/09 2:13 PM Page 23
-
Recording of the ECG
BASICS
24
1 mm 0.1 mv
0.04 sec
Constant speed of 25 mm/sec
0.20 sec
5 mm0.5 mv
Smallbox
Largebox
Components of an ECG Tracing
R
Q S
QT Interval
P UT
PR Interval
STSegment
QRSInterval
Isoelectricline
2142_Tab01_001-031.qxd 9/12/09 2:13 PM Page 24
-
Electrical Components
Deflection DescriptionP Wave
PR Interval
QRS Complex
ST Segment
T Wave
QT Interval
U Wave
25
BASICS
Electrical Activity
Term DefinitionWave A deflection, either positive or negative, away from the
baseline (isoelectric line) of the ECG tracing Complex Several wavesSegment A straight line between waves or complexesInterval A segment and a wave
Clinical Tip: Between waves and cycles, the ECG records a baseline(isoelectric line), which indicates the absence of net electrical activity.
First wave seenSmall rounded, upright (positive) wave indicating atrial
depolarization (and contraction) Distance between beginning of P wave and beginning
of QRS complexMeasures time during which a depolarization wave
travels from the atria to the ventricles Three deflections following P waveIndicates ventricular depolarization (and contraction)Q Wave: First negative deflectionR Wave: First positive deflectionS Wave: First negative deflection after R waveDistance between S wave and beginning of T waveMeasures time between ventricular depolarization and
beginning of repolarizationRounded upright (positive) wave following QRSRepresents ventricular repolarization Distance between beginning of QRS to end of T waveRepresents total ventricular activitySmall rounded, upright wave following T wave Most easily seen with a slow HRRepresents repolarization of Purkinje fibers
2142_Tab01_001-031.qxd 9/12/09 2:13 PM Page 25
-
BASICS
26
Methods for Calculating Heart Rate
Heart rate is the number of times the heart beats per minute (bpm). On anECG tracing, bpm is usually calculated as the number of QRS complexes.Included are extra beats, such as premature ventricular contractions (PVC),premature atrial contractions (PAC), and premature junctional contractions(PJC). The rate is measured from the R-R interval, the distance between oneR wave and the next. If the atrial rate (the number of P waves) and the ven-tricular rate (the number of QRS complexes) vary, the analysis may showthem as different rates, one atrial and one ventricular. The method chosen tocalculate HR varies according to rate and regularity on the ECG tracing.
Method 1: Count Large Boxes
Regular rhythms can be quickly determined by counting the number oflarge graph boxes between two R waves. That number is divided into 300to calculate bpm. The rates for the first one to six large boxes can be easilymemorized. Remember: 60 sec/min divided by 0.20 sec/large box = 300large boxes/min.
506075100300 150
Counting large boxes for heart rate. The rate is 60 bpm.
2142_Tab01_001-031.qxd 9/12/09 2:13 PM Page 26
-
Methods 1 and 2 for Calculating Heart Rate
Number of Large Number of Small Boxes Rate/Min Boxes Rate/Min
1 300 2 7502 150 3 5003 100 4 3754 75 5 3005 60 6 2506 50 7 2147 43 8 1868 38 9 1679 33 10 150
10 30 11 13611 27 12 12512 25 13 11513 23 14 10714 21 15 10015 20 16 94
Method 2: Count Small Boxes
The most accurate way to measure a regular rhythm is to count the numberof small boxes between two R waves. That number is divided into 1500 tocalculate bpm. Remember: 60 sec/min divided by 0.04 sec/small box =1500small boxes/min. Examples: If there are three small boxes between two R waves: 1500/3 =
500 bpm.If there are five small boxes between two R waves: 1500/5 =300 bpm.
27
BASICS
Clinical Tip: Approximate rate/min is rounded to the next-highestnumber.
2142_Tab01_001-031.qxd 9/12/09 2:13 PM Page 27
-
BASICS
28
Meth
od
3: Six-S
econ
d E
CG
Rh
ythm
Strip
Th
e best m
etho
d fo
r measu
ring
irregu
lar heart rates w
ith varyin
g R
-R in
tervals is to co
un
t the n
um
ber
of R
waves in
a 6-sec strip (in
clud
ing
extra beats su
ch as P
VC
s, PAC
s, and
PJC
s) and
mu
ltiply b
y 10. Th
isg
ives the averag
e nu
mb
er of b
eats per m
inu
te.
Usin
g a 6-sec E
CG
rhyth
m strip
to calcu
late heart rate: 7 x 10 = 70 b
pm
.
Clin
ical Tip
:If a rh
ythm
is extremely irreg
ular, it is b
est to co
un
t the n
um
ber o
f R-R
intervals p
er 60 sec (1 m
in).
2142_Tab01_001-031.qxd 9/12/09 2:13 PM Page 28
-
The bpm is commonly the ventricular rateIf atrial and ventricular rates differ, as in a 3rd-degree
block, measure both ratesNormal: 60100 bpmSlow (bradycardia): 100 bpmMeasure R-R intervals and P-P intervalsRegular: Intervals consistentRegularly irregular: Repeating patternIrregular: No patternIf present: Same in size, shape, position?Does each QRS have a P wave?Normal: Upright (positive) and uniform Inverted: Negative Notched: P' None: Rhythm is junctional or ventricularConstant: Intervals are the sameVariable: Intervals differNormal: 0.120.20 sec and constantNormal: 0.060.10 secWide: >0.10 secNone: Absent Beginning of QRS complex to end of T waveVaries with HRNormal: Less than half the RR interval Occur in AV blocksOccur in sinus arrestCompensatory: Complete pause following a premature
atrial contraction (PAC), premature junctional contraction(PJC), or premature ventricular contraction (PVC)
Noncompensatory: Incomplete pause following a PAC,PJC, or PVC
ECG Interpretation
29
BASICS
Analyzing a Rhythm
Component CharacteristicRate
Regularity
P Waves
PR Interval
QRS Interval
QT Interval
Dropped beatsPause
Continued
2142_Tab01_001-031.qxd 9/12/09 2:13 PM Page 29
-
Classification of Arrhythmias
Heart Rate ClassificationSlow BradyarrhythmiaFast TachyarrhythmiaAbsent Pulseless arrest
Bigeminy: Repeating pattern of normal complex followedby a premature complex
Trigeminy: Repeating pattern of 2 normal complexes followed by a premature complex
Quadrigeminy: Repeating pattern of 3 normal complexesfollowed by a premature complex
Couplet: 2 Consecutive premature complexesTriplet: 3 Consecutive premature complexes
BASICS
30
Notes:
Analyzing a Rhythmcontd
Component CharacteristicQRS Complex grouping
Normal Heart Rate (bpm)
Age Awake Rate Mean Sleeping RateNewborn to 3 months 85205 140 801603 months to 2 years 100190 130 751602 to 10 years 60140 80 6090>10 years 60100 75 5090
2142_Tab01_001-031.qxd 9/12/09 2:13 PM Page 30
-
31
BASICS
Notes:
2142_Tab01_001-031.qxd 9/12/09 2:13 PM Page 31
-
32
Sin
oatrial (S
A) N
od
e Arrh
ythm
ias
U
prig
ht P
waves all lo
ok sim
ilar. No
te: All E
CG
strips in
Tab 2 w
ere record
ed in
Lead II.
P
R in
tervals and
QR
S co
mp
lexes are of n
orm
al du
ration
.
No
rmal S
inu
s Rh
ythm
(NS
R)
Rate:N
orm
al (60100 bp
m)
Rh
ythm
:Reg
ular
P W
aves:No
rmal (u
prig
ht an
d u
nifo
rm)
PR
Interval :N
orm
al (0.120.20 sec)Q
RS
:No
rmal (0.060.10 sec)
Clin
ical Tip:A
no
rmal E
CG
do
es no
t exclud
e heart d
isease.
Clin
ical Tip:This rhythm
is generated by the sinus node and its rate is within norm
al limits (6080 bpm
).
ECGS
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 32
-
Sin
us B
radycard
ia
T
he S
A n
od
e disch
arges m
ore slo
wly th
an in
NS
R.
33
ECGS
Ra t e :S
low
(
-
34
Sin
us Tach
ycardia
T
he S
A n
od
e disch
arges m
ore freq
uen
tly than
in N
SR
.
ECGS
Ra t e :F a s t (>1 0 0 b
pm
)R
hy t h
m:R
egu
la rP
Waves:N
orm
al (up
righ
t and
un
iform
)P
R In
terval:No
rmal (0.120.20 sec)
QR
S:N
orm
al (0.060.10 sec)
Cl in
ical T ip:S
inu
s tachycard
ia may b
e caused
by exercise, an
xiety, fever, hyp
oxem
ia, hyp
ovo
lemia,
or card
iac fai lure.
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 34
-
Sin
us A
rrhyth
mia
T
he S
A n
od
e disch
arges irreg
ularly.
T
he R
-R in
terval is irregu
lar. 35
ECGS
Ra t e :U
sua lly n
orm
a l (6 0 1 0 0 bp
m); fr e q
uen
tly inc r e a s e s w
ith in
s pir a tio
n a n
d d
e c r e a s e s with
e x pir a -
tion
; may b
e 0.12 sec P
Waves:N
orm
al (up
righ
t and
un
iform
)P
R In
terval :No
rmal (0.120.20 sec)
QR
S:N
orm
al (0.060.10 sec)
Clin
ical T ip:
Th
e pacin
g rate o
f the S
A n
od
e varies with
respiratio
n, esp
ecially in ch
ildren
and
eld-
erly peo
ple.
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 35
-
36
Sin
us P
ause (S
inu
s Arrest)
T
he S
A n
od
e fails to d
ischarg
e and
then
resum
es.
Electrical activity resu
mes eith
er wh
en th
e SA
no
de resets itself o
r wh
en a slo
wer laten
t pacem
akerb
egin
s to d
ischarg
e.
Th
e pau
se (arrest) time in
terval is no
t a mu
ltiple o
f the n
orm
al PP
interval.
ECGS
3.96 - sec pause/arrest
Rate:N
orm
al to slo
w; d
etermin
ed b
y du
ration
and
frequ
ency o
f sinu
s pau
se (arrest)R
hyth
m:Irreg
ular w
hen
ever a pau
se (arrest) occu
rsP
Waves:N
orm
al (up
righ
t and
un
iform
) except in
areas of p
ause (arrest)
PR
Interval :N
orm
al (0.120.20 sec)Q
RS
:No
rmal (0.060.10 sec)
Cl in
ical T ip:C
ardiac o
utp
ut m
ay decrease, cau
sing
synco
pe o
r dizzin
ess.
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 36
-
Sin
oatrial (S
A) B
lock
T
he b
lock o
ccurs in
som
e mu
ltiple o
f the P
P in
terval.
After th
e dro
pp
ed b
eat, cycles con
tinu
e on
time.
37
ECGS
Dropped beat
X
Ra t e :N
orm
a l to s lo
w; d
e te r min
e d b
y du
r a tion
a nd
fr e qu
enc y o
f SA
blo
c kR
hyth
m:Irreg
ular w
hen
ever an S
A b
lock o
ccurs
P W
aves:No
rmal (u
prig
ht an
d u
nifo
rm) excep
t in areas o
f dro
pp
ed b
eatsP
R In
terval:No
rmal (0.120.20 sec)
QR
S:N
orm
al (0.060.10 sec)
Cl in
ical T ip:C
ardiac o
utp
ut m
ay decrease, cau
sing
synco
pe o
r dizzin
ess.
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 37
-
38
Atrial A
rrhyth
mias
P
waves d
iffer in ap
pearan
ce from
sinu
s P w
aves.
QR
S co
mp
lexes are of n
orm
al du
ration
if no
ventricu
lar con
du
ction
distu
rban
ces are presen
t.
Wan
derin
g A
trial Pacem
aker (WA
P)
P
acemaker site tran
sfers from
the S
A n
od
e to o
ther laten
t pacem
aker sites in th
e atria and
the A
Vju
nctio
n an
d th
en m
oves b
ack to th
e SA
no
de.
ECGS
Rate:N
orm
al (60100 bp
m)
Rh
ythm
:I rregu
larP
Waves:A
t least three d
ifferent fo
rms, d
etermin
ed b
y the fo
cus in
the atria
PR
Interval :Variab
le; determ
ined
by fo
cus
QR
S:N
orm
al (0.060.10 sec)
Clin
ical Tip:W
AP
may o
ccur in
no
rmal h
earts as a result o
f fluctu
ation
s in vag
al ton
e.
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 38
-
Mu
ltifocal A
trial Tachycard
ia (MA
T)
T
his fo
rm o
f WA
P is asso
ciated w
ith a ven
tricular resp
on
se >100 bp
m.
M
AT
may b
e con
fused
with
atrial fibrillatio
n (A
-fib); h
ow
ever, MA
T h
as a visible P
wave.
39
ECGS
Ra t e :F a s t (>1 0 0 b
pm
)R
hyth
m:Irreg
ular
P W
ave:At least th
ree differen
t form
s, determ
ined
by th
e focu
s in th
e atriaP
R In
terval:Variable; d
etermin
ed b
y focu
sQ
RS
:No
rmal (0.060.10 sec)
Cl in
ical T ip:M
AT
is com
mo
nly seen
in p
atients w
ith ch
ron
ic ob
structive p
ulm
on
ary disease (C
OP
D)
bu
t may also
occu
r in an
acute M
I .
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 39
-
40
Prem
ature A
trial Co
ntractio
n (PA
C)
A
sing
le con
traction
occu
rs earlier than
the n
ext expected
sinu
s con
traction
.
After th
e PAC
, sinu
s rhyth
m u
sually resu
mes.
ECGS
PACPAC
Ra t e :D
epen
ds o
n r a te o
f un
de r ly in
g r h
y thm
Rh
ythm
:Irregu
lar wh
enever a PA
C o
ccurs
P W
aves:Presen
t; in th
e PAC
, may h
ave a differen
t shap
eP
R In
terval:Varies in th
e PAC
; oth
erwise n
orm
al (0.120.20 sec)Q
RS
:No
rmal (0.060.10 sec)
Cl in
ical T ip:In
patien
ts with
heart d
isease, frequ
ent PA
Cs m
ay preced
e paro
xysmal su
praven
tricular
tachycard
ia (PS
VT
), atrial fibri l latio
n (A
-fib), o
r atrial flutter (A
-flutter).
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 40
-
Atrial Tach
ycardia
A
rapid
atrial rate overrid
es the S
A n
od
e and
beco
mes th
e do
min
ant p
acemaker.
S
om
e ST
segm
ent an
d T
wave ab
no
rmalities m
ay be p
resent.
41
ECGS
Ra t e :1 5 0 2 5 0 b
pm
Rh
ythm
:Reg
ular
P W
aves:No
rmal (u
prig
ht an
d u
nifo
rm) b
ut d
iffer in sh
ape fro
m sin
us P
waves
PR
Interval:M
ay be sh
ort (
-
42
Su
praven
tricular Tach
ycardia (S
VT
)
T
his arrh
ythm
ia has su
ch a fast rate th
at the P
waves m
ay no
t be seen
.
ECGS
P wave
buried in T w
ave
Ra t e :1 5 0 2 5 0 b
pm
Rh
y t hm
:Reg
ula r
P W
aves:Frequ
ently b
uried
in p
recedin
g T
waves an
d d
ifficult to
seeP
R In
terval:Usu
ally no
t po
ssible to
measu
reQ
RS
:No
rmal (0.060.10 sec) b
ut m
ay be w
ide if ab
no
rmally co
nd
ucted
thro
ug
h ven
tricles
Cl in
ical T ip: S
VT
may b
e related to
caffeine in
take, nico
tine, stress, o
r anxiety in
health
y adu
lts.
Cl in
ical T ip:
So
me p
atients m
ay experien
ce ang
ina, h
ypo
tensio
n, l ig
ht-h
eaded
ness, p
alpitatio
ns,
and
inten
se anxiety.
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 42
-
Paro
xysmal S
up
raventricu
lar Tachycard
ia (PS
VT
)
P
SV
T is a rap
id rh
ythm
that starts an
d sto
ps su
dd
enly.
Fo
r accurate in
terpretatio
n, th
e beg
inn
ing
or en
d o
f the P
SV
T m
ust b
e seen.
P
SV
T is so
metim
es called p
aroxysm
al atrial tachycard
ia (PAT
).
43
ECGS
Sudden onset of SVT
Rate:150250 b
pm
Rh
ythm
:Irregu
larP
Waves:Freq
uen
tly bu
ried in
preced
ing
T w
aves and
difficu
lt to see
PR
Interval:U
sually n
ot p
ossib
le to m
easure
QR
S:N
orm
al (0.060.10 sec) bu
t may b
e wid
e if abn
orm
al ly con
du
cted th
rou
gh
ventricles
Cl in
ical T ip:T
he p
atient m
ay feel palp
itation
s, dizzin
ess, l igh
thead
edn
ess, or an
xiety.
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 43
-
44
Atrial Flu
tter (A-flu
tter)
A
V n
od
e con
du
cts imp
ulses to
the ven
tricles at a ratio o
f 2:1, 3:1, 4:1, or g
reater (rarely 1:1).
Th
e deg
ree of A
V b
lock m
ay be co
nsisten
t or variab
le.
ECGS
Flutter wave
s
Ra t e :A
tr ia l: 2 5 0 3 5 0 bp
m; v e n
tr ic ula r : v a r ia b
leR
hyth
m:A
trial: regu
lar; ventricu
lar: variable
P W
aves:Flutter w
aves have a saw
-too
thed
app
earance; so
me m
ay be b
uried
in th
e QR
S an
d n
ot visib
leP
R In
terval:Variable
QR
S:U
sual ly n
orm
al (0.060.10 sec), bu
t may ap
pear w
iden
ed if flu
tter waves are b
uried
in Q
RS
Cl in
ical T ip:A
-flutter m
ay be th
e first ind
ication
of card
iac disease.
Cl in
ical T ip:S
ign
s and
symp
tom
s dep
end
on
ventricu
lar respo
nse rate.
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 44
-
Atrial Fib
rillation
(A-fib
)
R
apid
, erratic electrical disch
arge co
mes fro
m m
ultip
le atrial ectop
ic foci.
N
o o
rgan
ized atrial d
epo
larization
is detectab
le.45
ECGS
Irregular R-R intervals
Ra t e :A
tr ia l: 3 5 0 bp
m; v e n
tr ic ula r : v a r ia b
leR
hyth
m:Irreg
ular
P W
aves:No
true P
waves; ch
aotic atrial activity
PR
Interval:N
on
eQ
RS
:No
rmal (0.060.10 sec)
Cl in
ical T ip:A
-fib is u
sual ly a ch
ron
ic arrhyth
mia asso
ciated w
ith u
nd
erlying
heart d
isease.
Cl in
ical T ip:S
ign
s and
symp
tom
s dep
end
on
ventricu
lar respo
nse rate.
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 45
-
46
Wo
lff-Parkin
son
-Wh
ite (WP
W) S
ynd
rom
e
In
WP
W, an
accessory co
nd
uctio
n p
athw
ay is presen
t betw
een th
e atria and
the ven
tricles.E
lectrical imp
ulses are rap
idly co
nd
ucted
to th
e ventricles.
T
hese rap
id im
pu
lses slur th
e initial p
ortio
n o
f the Q
RS
; the slu
rred effect is called
a delta w
ave.
ECGS
Delta
wa ve
Rate:D
epen
ds o
n rate o
f un
derlyin
g rh
ythm
Rh
ythm
:Reg
ular u
nless asso
ciated w
ith A
-fibP
Waves:N
orm
al (up
righ
t and
un
iform
) un
less A-fib
is presen
tP
R In
terval :Sh
ort (0.10 sec); d
elta wave p
resent
Cl in
ical T ip:W
PW
is associated
with
narro
w-co
mp
lex tachycard
ias, inclu
din
g A
-flutter an
d A
-fib.
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 46
-
Jun
ction
al Arrh
ythm
ias
T
he atria an
d S
A n
od
e do
no
t perfo
rm th
eir no
rmal p
acemakin
g fu
nctio
ns.
A
jun
ction
al escape rh
ythm
beg
ins.
Jun
ction
al Rh
ythm
47
ECGS
Inve
rted P wave
Absent P wave
Rate:4060 b
pm
Rh
ythm
:Reg
ular
P W
aves:Ab
sent, in
verted, b
uried
, or retro
grad
eP
R In
terval :No
ne, sh
ort, o
r retrog
rade
QR
S:N
orm
al (0.060.10 sec)
Clin
ical T ip:
Sin
us n
od
e disease th
at causes in
app
rop
riate slow
ing
of th
e sinu
s no
de m
ay exacer-b
ate this rh
ythm
. You
ng
, health
y adu
lts, especially th
ose w
ith in
creased vag
al ton
e du
ring
sleep, o
ftenh
ave perio
ds o
f jun
ction
al rhyth
m th
at is com
pletely b
enig
n, n
ot req
uirin
g in
terventio
n.
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 47
-
48
Accelerated
Jun
ction
al Rh
ythm
ECGS
Absent P wave
Ra t e :6 1 1 0 0 b
pm
Rh
y t hm
:Reg
ula r
P W
a v e s :Ab
s e nt, in
v e r te d, b
ur ie d
, or r e tr o
gr a d
eP
R In
terval:No
ne, sh
ort, o
r retrog
rade
QR
S:N
orm
al (0.060.10 sec)
Clin
ical Tip:M
on
itor th
e patien
t, no
t just th
e EC
G, fo
r clinical im
pro
vemen
t.
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 48
-
Jun
ction
al Tachycard
ia
49
ECGS
Retrog
rade P wave
Ra t e :1 0 1 1 8 0 b
pm
Rh
y t hm
:Reg
ula r
P W
a v e s :Ab
s e nt, in
v e r te d, b
ur ie d
, or r e tr o
gr a d
eP
R In
terval:No
ne, sh
ort, o
r retrog
rade
QR
S:N
orm
al (0.060.10 sec)
Clin
ical Tip
:S
ign
s an
d
symp
tom
s o
f d
ecreased
cardiac
ou
tpu
t m
ay b
e seen
in
resp
on
se to
the rap
id rate.
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 49
-
50
Jun
ction
al Escap
e Beat
A
n escap
e com
plex co
mes later th
an th
e next exp
ected sin
us co
mp
lex.
ECGS
Jun
ctional escape beats
Ra t e :D
epen
ds o
n r a te o
f un
de r ly in
g r h
y thm
Rh
y t hm
:Ir r e gu
la r wh
ene v e r a n
e s c a pe b
e a t oc c u
r sP
Waves:N
on
e, inverted
, bu
ried, o
r retrog
rade in
the escap
e beat
PR
Interval:N
on
e, sho
rt, or retro
grad
eQ
RS
:No
rmal (0.060.10 sec)
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 50
-
Prem
ature Ju
nctio
nal C
on
traction
(PJC
)
E
nh
anced
auto
maticity in
the A
V ju
nctio
n p
rod
uces P
JCs.
51
ECGS
PJCPJC
Ra t e :D
epen
ds o
n r a te o
f un
de r ly in
g r h
y thm
Rh
y t hm
:Ir r e gu
la r wh
ene v e r a P
J C o
c c ur s
P W
aves:Ab
sent, in
verted, b
uried
, or retro
grad
e in th
e PJC
PR
Interval:N
on
e, sho
rt, or retro
grad
eQ
RS
:No
rmal (0.060.10 sec)
Cl in
ical T ip:B
efore d
ecidin
g w
heth
er isolated
PJC
s are insig
nifican
t, con
sider th
e cause.
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 51
-
52
Ven
tricular A
rrhyth
mias
In
all ventricu
lar rhyth
ms, th
e QR
S co
mp
lex is >0.10 sec. P W
aves are absen
t or, if visib
le, have n
oco
nsisten
t relation
ship
to th
e QR
S co
mp
lex.
Idio
ventricu
lar Rh
ythm
ECGS
Rate:2040 b
pm
Rh
ythm
:Reg
ular
P W
aves:No
ne
PR
Interval :N
on
eQ
RS
:Wid
e (>0.10 sec), bizarre ap
pearan
ce
Clin
ical T ip:D
imin
ished
cardiac o
utp
ut is exp
ected b
ecause o
f the slo
w h
eart rate. An
idio
ventricu
-lar rh
ythm
may b
e called an
ago
nal rh
ythm
wh
en th
e heart rate d
rop
s belo
w 20 b
pm
. An
ago
nal rh
ythm
is gen
erally termin
al and
is usu
ally the last rh
ythm
befo
re asystole.
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 52
-
Accelerated
Idio
ventricu
lar Rh
ythm
53
ECGS
Ra t e :4 1 1 0 0 b
pm
Rh
y t hm
:Reg
ula r
P W
a v e s :No
ne
PR
Interval:N
on
eQ
RS
:Wid
e (>0.10 sec), bizarre ap
pearan
ce
Clin
ical Tip:
Idio
ventricu
lar rhyth
ms ap
pear w
hen
sup
raventricu
lar pacin
g sites are d
epressed
or
absen
t. Dim
inish
ed card
iac ou
tpu
t is expected
if the h
eart rate is slow
.
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 53
-
54
Prem
ature V
entricu
lar Co
ntractio
n (P
VC
)
P
VC
s result fro
m an
irritable ven
tricular fo
cus.
P
VC
s may b
e un
iform
(same fo
rm) o
r mu
ltiform
(differen
t form
s).
Usu
ally a PV
C is fo
llow
ed b
y a full co
mp
ensato
ry pau
se becau
se the sin
us n
od
e timin
g is n
ot in
ter-ru
pted
. In co
ntrast, a P
VC
may b
e follo
wed
by a n
on
com
pen
satory p
ause if th
e PV
C en
ters the sin
us
no
de an
d resets its tim
ing
, enab
ling
the fo
llow
ing
sinu
s P w
ave to ap
pear earlier th
an exp
ected.
ECGS
PVC
Rate:D
epen
ds o
n rate o
f un
derlyin
g rh
ythm
Rh
ythm
:Irregu
lar wh
enever a P
VC
occu
rsP
Waves:N
on
e associated
with
the P
VC
PR
Interval :N
on
e associated
with
the P
VC
QR
S:W
ide (>0.10 sec), b
izarre app
earance
Clin
ical Tip:
Patien
ts may sen
se PV
Cs as skip
ped
beats. B
ecause th
e ventricles are o
nly p
artiallyfilled
, the P
VC
frequ
ently d
oes n
ot g
enerate a p
ulse.
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 54
-
Prem
ature V
entricu
lar Co
ntractio
n: U
nifo
rm (sam
e form
)
55
ECGS
Prem
ature V
ent r icu
lar Co
nt r act io
n: M
ult if o
rm (d
if f er ent f o
rms )
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 55
-
56
Prem
ature V
entricu
lar Co
ntractio
n: V
entricu
lar Big
emin
y (PV
C every 2
nd
beat)
ECGS
Prem
ature V
ent r icu
lar Co
nt r act io
n: V
ent r icu
lar Tr igem
iny (P
VC
every 3rd
beat )
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 56
-
Prem
ature V
entricu
lar Co
ntractio
n: V
entricu
lar Qu
adrig
emin
y (PV
C every
4th
beat)
57
ECGS
Co u p le ts
Prem
ature V
ent r icu
lar Co
nt r act io
n: C
ou
plet s (p
air ed P
VC
s )
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 57
-
58
Prem
ature V
entricu
lar Co
ntractio
n: R
-on
-T P
hen
om
eno
n
T
he P
VC
s occu
r so early th
at they fall o
n th
e T w
ave of th
e preced
ing
beat.
T
hese P
VC
s occu
r du
ring
the refracto
ry perio
d o
f the ven
tricles, a vuln
erable p
eriod
becau
se the
cardiac cells h
ave no
t fully rep
olarized
.
ECGS
Rate:D
epen
ds o
n rate o
f un
derlyin
g rh
ythm
Rh
ythm
:Irregu
lar wh
enever a P
VC
occu
rsP
Waves:N
on
e associated
with
the P
VC
PR
Interval :N
on
e associated
with
the P
VC
QR
S:W
ide (>0.10 sec), b
izarre app
earance
Cl in
ical T ip:In
acute isch
emia, R
-on
-T p
hen
om
eno
n m
ay be esp
ecial ly dan
gero
us b
ecause th
e ven-
tricles may b
e mo
re vuln
erable to
ventricu
lar tachycard
ia (VT
) or ven
tricular fib
rillation
(VF).
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 58
-
Prem
ature C
on
traction
: Interp
olated
PV
C
T
he P
VC
occu
rs betw
een tw
o reg
ular co
mp
lexes; it may ap
pear san
dw
iched
betw
een tw
o n
orm
alb
eats.
An
interp
olated
PV
C d
oes n
ot in
terfere with
the n
orm
al cardiac cycle.
59
ECGS
Interpolated PVC
Rate:D
epen
ds o
n rate o
f un
derlyin
g rh
ythm
Rh
ythm
:Irregu
lar wh
enever a P
VC
occu
rsP
Waves:N
on
e associated
with
the P
VC
PR
Interval :N
on
e associated
with
the P
VC
QR
S:W
ide (>0.10 sec), b
izarre app
earance
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 59
-
60
Ven
tricular Tach
ycardia (V
T): M
on
om
orp
hic
In
mo
no
mo
rph
ic VT, Q
RS
com
plexes h
ave the sam
e shap
e and
amp
litud
e.
ECGS
Ra t e :1 0 0 2 5 0 b
pm
Rh
y t hm
:Reg
ula r
P W
aves:No
ne o
r no
t associated
with
the Q
RS
PR
Interval:N
on
eQ
RS
:Wid
e (>0.10 sec), bizarre ap
pearan
ce
Cl in
ical T ip:I t is im
po
rtant to
con
firm th
e presen
ce or ab
sence o
f pu
lses becau
se mo
no
mo
rph
ic VT
may b
e perfu
sing
or n
on
perfu
sing
.
Cl in
ical T ip:M
on
om
orp
hic V
T w
i l l pro
bab
ly deterio
rate into
VF o
r un
stable V
T if su
stained
and
no
ttreated
.
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 60
-
Ven
tricular Tach
ycardia (V
T): P
olym
orp
hic
In
po
lymo
rph
ic VT, Q
RS
com
plexes vary in
shap
e and
amp
litud
e.
Th
e QT
interval is n
orm
al or lo
ng
. 61
ECGS
Ra t e :1 0 0 2 5 0 b
pm
Rh
ythm
:Reg
ular o
r irregu
larP
Waves:N
on
e or n
ot asso
ciated w
ith th
e QR
SP
R In
terval:No
ne
QR
S:W
ide (>0.10 sec), b
izarre app
earance
Cl in
ical T ip:I t is im
po
rtant to
determ
ine w
heth
er pu
lses are presen
t becau
se po
lymo
rph
ic VT
may
be p
erfusin
g o
r no
np
erfusin
g.
Clin
ical Tip:C
on
sider electro
lyte abn
orm
alities as a po
ssible cau
se.
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 61
-
62
Torsad
e de P
oin
tes
T
he Q
RS
reverses po
larity and
the strip
sho
ws a sp
ind
le effect.
Th
is rhyth
m is an
un
usu
al variant o
f po
lymo
rph
ic VT
with
lon
g Q
T in
tervals.
In Fren
ch th
e term m
eans tw
isting
of p
oin
ts.
ECGS
Rate:200250 b
pm
Rh
ythm
:Irregu
larP
Waves:N
on
eP
R In
terval :No
ne
QR
S:W
ide (>0.10 sec), b
izarre app
earance
Cl in
ical T ip:To
rsade d
e po
intes m
ay deterio
rate to V
F or asysto
le.
Clin
ical T ip:
Frequ
ent cau
ses are dru
gs th
at pro
lon
g th
e QT
interval, an
d electro
lyte abn
orm
alitiessu
ch as h
ypo
mag
nesem
ia.
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 62
-
Ven
tricular Fib
rillation
(VF)
C
hao
tic electrical activity occu
rs with
no
ventricu
lar dep
olarizatio
n o
r con
traction
.
Th
e amp
litud
e and
frequ
ency o
f the fib
rillatory activity can
defin
e the typ
e of fib
rillation
as coarse,
med
ium
, or fin
e. Sm
all baselin
e un
du
lation
s are con
sidered
fine; larg
e on
es are coarse.
63
ECGS
Rate:In
determ
inate
Rh
ythm
:Ch
aotic
P W
aves:No
ne
PR
Interval :N
on
eQ
RS
:No
ne
Cl in
ical T ip:T
here is n
o p
ulse o
r cardiac o
utp
ut. R
apid
interven
tion
is critical . Th
e lon
ger th
e delay,
the less th
e chan
ce of co
nversio
n.
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 63
-
64
Pu
lseless Electrical A
ctivity (PE
A)
T
he m
on
itor sh
ow
s an id
entifiab
le electrical rhyth
m, b
ut n
o p
ulse is d
etected.
T
he rh
ythm
may b
e sinu
s, atrial, jun
ction
al, or ven
tricular.
P
EA
is also called
electrom
echan
ical disso
ciation
(EM
D).
ECGS
Rate:R
eflects un
derlyin
g rh
ythm
Rh
ythm
:Reflects u
nd
erlying
rhyth
mP
Waves:R
eflects un
derlyin
g rh
ythm
PR
Interval :R
eflects un
derlyin
g rh
ythm
QR
S:R
eflects un
derlyin
g rh
ythm
Cl in
ical T ip:P
oten
tial causes o
f PE
A are trau
ma, ten
sion
pn
eum
oth
orax, th
rom
bo
sis (pu
lmo
nary o
rco
ron
ary), cardiac tam
po
nad
e, toxin
s, hyp
o- o
r hyp
erkalemia, h
ypo
volem
ia, hyp
oxia, h
ypo
glycem
ia,h
ypo
therm
ia, and
hyd
rog
en io
n (acid
osis).
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 64
-
Asysto
le
E
lectrical activity in th
e ventricles is co
mp
letely absen
t.65
ECGS
Ra t e :N
on
eR
hy t h
m:N
on
eP
Waves:N
on
eP
R In
terval:No
ne
QR
S:N
on
e
Cl in
ical T ip:R
ule o
ut o
ther cau
ses such
as loo
se leads, n
o p
ow
er, or in
sufficien
t sign
al gain
.
Cl in
ical T ip:S
eek to id
entify th
e un
derlyin
g cau
se as in P
EA
. Also
, search to
iden
tify VF.
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 65
-
66
Atrio
ventricu
lar (AV
) Blo
cks
A
V b
locks are d
ivided
into
three categ
ories: first, seco
nd
, and
third
deg
ree.
First-Deg
ree AV
Blo
ck
ECGS
Rate:D
epen
ds o
n rate o
f un
derlyin
g rh
ythm
Rh
ythm
:Reg
ular
P W
aves:No
rmal (u
prig
ht an
d u
nifo
rm)
PR
Interval :P
rolo
ng
ed (>0.20 sec)
QR
S:N
orm
al (0.060.10 sec)
Cl in
ical T ip:U
sual ly a first-d
egree A
V b
lock is b
enig
n, b
ut i f asso
ciated w
ith an
acute M
I i t may lead
to fu
rther A
V d
efects.
Clin
ical Tip:
Often
AV
blo
ck is caused
by m
edicatio
ns th
at pro
lon
g A
V co
nd
uctio
n; th
ese inclu
de
dig
oxin
, calcium
chan
nel b
lockers, an
d b
eta blo
ckers.
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 66
-
Seco
nd
-Deg
ree AV
Blo
ckTyp
e I(M
ob
itz I or W
enckeb
ach)
P
R in
tervals beco
me p
rog
ressively lon
ger u
ntil o
ne P
wave is to
tally blo
cked an
d p
rod
uces n
o Q
RS
com
plex. A
fter a pau
se, du
ring
wh
ich th
e AV
no
de reco
vers, this cycle is rep
eated.
67
ECGS
Blocked beatX
Rate:D
epen
ds o
n rate o
f un
derlyin
g rh
ythm
Rh
ythm
: Atrial: reg
ular; ven
tricular: irreg
ular
P W
aves:No
rmal (u
prig
ht an
d u
nifo
rm), m
ore P
waves th
an Q
RS
com
plexes
PR
Interval :P
rog
ressively lon
ger u
nti l o
ne P
wave is b
locked
and
a QR
S is d
rop
ped
QR
S:N
orm
al (0.060.10 sec)
Cl in
ical T ip:T
his rh
ythm
may b
e caused
by m
edicatio
n su
ch as b
eta blo
ckers, dig
oxin
, and
calcium
chan
nel b
lockers. Isch
emia in
volvin
g th
e righ
t coro
nary artery is an
oth
er cause.
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 67
-
68
Seco
nd
-Deg
ree AV
Blo
ckTyp
e II (M
ob
itz II)
C
on
du
ction
ratio (P
waves to
QR
S co
mp
lexes) is com
mo
nly 2:1, 3:1, o
r 4:1, or variab
le.
QR
S co
mp
lexes are usu
ally wid
e becau
se this b
lock u
sually in
volves b
oth
bu
nd
le bran
ches.
ECGS
Rate:A
trial: usu
ally 60100 bp
m; ven
tricular: slo
wer th
an atrial rate
Rh
ythm
:Atrial: reg
ular; ven
tricular: reg
ular o
r irregu
larP
Waves:N
orm
al (up
righ
t and
un
iform
); mo
re P w
aves than
QR
S co
mp
lexesP
R In
terval :No
rmal o
r pro
lon
ged
bu
t con
stant
QR
S:M
ay be n
orm
al , bu
t usu
al ly wid
e (>0.10 sec) if the b
un
dle b
ranch
es are invo
lved
Cl in
ical T ip:
Resu
lting
brad
ycardia can
com
pro
mise card
iac ou
tpu
t and
lead to
com
plete A
V b
lock.
Th
is rhyth
m o
ften o
ccurs w
ith card
iac ischem
ia or an
MI.
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 68
-
69
ECGS
Th
ird-D
egree A
V B
lock
C
on
du
ction
betw
een atria an
d ven
tricles is totally ab
sent b
ecause o
f com
plete electrical b
lock at o
rb
elow
the A
V n
od
e. Th
is is kno
wn
as AV
disso
ciation
.
Co
mp
lete heart b
lock is an
oth
er nam
e for th
is rhyth
m.
Rate:A
trial: 60100 bp
m; ven
tricular: 4060 b
pm
if escape fo
cus is ju
nctio
nal,
-
70
Bu
nd
le Bran
ch B
lock (B
BB
)
E
ither th
e left or th
e righ
t ventricle m
ay dep
olarize late, creatin
g a w
ide o
r no
tched
QR
S
com
plex.
ECGS
Notched QRS
Ra t e :D
epen
ds o
n r a te o
f un
de r ly in
g r h
y thm
Rh
ythm
:Reg
ular
P W
aves:No
rmal (u
prig
ht an
d u
nifo
rm)
PR
Interval:N
orm
al (0.120.20 sec)Q
RS
:Wid
e (>0.10 sec) with
a no
tched
app
earance
Cl in
ical T ip:B
un
dle b
ranch
blo
ck com
mo
nly o
ccurs in
coro
nary artery d
isease.
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 70
-
Artificial C
ardiac P
acemak
ers
Artificial p
acemakers electro
nically stim
ulate th
e heart in
place o
f the h
earts ow
n p
acemaker.
P
acemakers m
ay be p
reset to stim
ulate th
e hearts activity co
ntin
uo
usly o
r interm
ittently.
Temp
orary P
acemaker
P
aces the h
eart thro
ug
h ep
icardial, tran
sveno
us, o
r transcu
taneo
us ro
utes. T
he p
ulse g
enerato
r islo
cated extern
ally.
Perm
anen
t Pacem
aker
Its circu
itry sealed in
an airtig
ht case, th
e pacem
aker is imp
lanted
in th
e bo
dy. It u
ses sensin
g an
dp
acing
device lead
s.
Sin
gle-C
ham
ber P
acemaker
O
ne le a d
is pla c e d
in th
e he a r t a n
d p
a c e s a s ing
le he a r t c h
a mb
e r (e ithe r a tr iu
m o
r v e ntr ic le ).
Du
a l-Ch
amb
e r Pa c e m
a k e r
O
ne lead is placed in the right atrium and the other in the right ventricle. The atrial electrode generates a spike that
should be followed by a P w
ave, and the ventricular electrode generates a spike followed by a w
ide QR
S com
plex.
Pacem
aker Mo
des
Fixed
rate (asynch
ron
ou
s): Disch
arges at a p
reset rate (usu
al ly 7080 bp
m) reg
ardless o
f the
patien
ts ow
n electrical activity.
D
eman
d (syn
chro
no
us): D
ischarg
es on
ly wh
en th
e patien
ts heart rate d
rop
s belo
w th
e pacem
akersp
reset (base) rate.
Clin
ical Tip:P
atients w
ith p
acemakers m
ay receive defib
rillation
, bu
t avoid
placin
g th
e defib
rillator
pad
dles o
r pad
s closer th
an 5 in
ches to
the p
acemaker b
attery pack.
71
ECGS
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 71
-
72
Artificial C
ardiac P
acemak
ersECGS
Pacem
aker C
od
esC
ham
ber
Ch
amb
er R
espo
nse to
Pro
gram
mab
le R
espo
nse to
P
acedS
ensed
Sen
sing
Fun
ction
sTach
ycardia
A =
Atriu
mV
=
Ventricle
D =
Du
al (atrium
an
d ven
tricle)O
=
No
ne
Ar t if icial P
acemak
er Rh
ythm
Ra t e
Va r ie s a c c or d
ing
to p
r e s e t pa c e m
a k e r r a te . R
hy t h
mR
egu
la r for a s y n
c hr o
no
us p
a c e ma k e r ; ir r e g
ula r fo
r de m
a nd
pa c e m
a k e r un
le s s 1 0 0 %p
a c e d w
ith n
o in
tr ins ic b
e a ts .P
waves
No
ne p
rod
uced
by ven
tricular p
acemaker. S
inu
s P w
aves may b
e seen b
ut are u
nrelated
toQ
RS
. Atrial o
r du
al-cham
ber p
acemaker sh
ou
ld h
ave P w
aves follo
win
g each
atrial spike.
PR
Interval
None for ventricular pacer. A
trial or dual-chamber pacem
aker produces constant PR intervals.
QR
SW
ide (>0.10 sec) fo
l low
ing
each ven
tricular sp
ike in a p
acemaker rh
ythm
. Th
e patien
tso
wn
electrical activity may g
enerate a Q
RS
com
plex th
at loo
ks differen
t from
the p
acedQ
RS
s. I f atrial ly paced
on
ly, the Q
RS
may b
e with
in n
orm
al l imits.
A =
Atriu
mV
=
Ventricle
D =
Du
al (atrium
and
ventricle)
O =
No
ne
T =
Trigg
ers pacin
gI
=In
hib
its pacin
gD
=
Du
al (trigg
ersan
d in
hib
its)O
=
No
ne
P =
Basic p
rog
rams
(rate and
ou
tpu
t)M
=
Mu
ltiple p
rog
rams
C =
Co
mm
un
ication
(i.e., telemetry)
R =
Rate resp
on
seO
=
No
ne
P =
Pacin
gS
=
Sh
ock
D =
Du
al (pace
and
sho
ck)O
=
No
ne
Clin
ical T ip:O
nce an
imp
ulse is g
enerated
by th
e pacem
aker, it app
ears as a spike, eith
er abo
ve or
belo
w th
e baselin
e (isoelectric lin
e), on
the E
CG
. Th
e spike in
dicates th
at the p
acemaker h
as fired.
Clin
ical Tip:A
pacem
aker is in cap
ture w
hen
a spike p
rod
uces an
EC
G w
ave or co
mp
lex.
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 72
-
Sin
gle-C
ham
ber P
acemaker R
hyth
mA
trial
73
ECGS
Pace
make
r spike
Pa
cem
aker spike
Sin
gle -C
ham
be r P
a c e ma k e r R
hy t h
m
Ven
t r ic ula r
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 73
-
74
Du
al-Ch
amb
er Pacem
aker Rh
ythm
A
trial and
Ven
tricular
ECGS
Atrial pacemake
r spikeV
entricular pacem
aker spike
No
tes :
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 74
-
Pa c e m
a k e r F a ilur e t o
Ca p
t ur e
75
ECGS
Pacem
aker M
alfun
ction
sM
alfun
ction
Reaso
nFailu
re to p
aceP
acemaker sp
ikes are absen
t. Th
e cause m
ay be a d
ead b
attery, a disru
ptio
n in
the
con
nectin
g w
ires, or im
pro
per p
rog
ramm
ing
.Failu
re to cap
ture
Pacem
aker spikes are p
resent, b
ut n
o P
wave o
r QR
S fo
llow
s the sp
ike. Turn
ing
up
the p
acemakers vo
ltage o
ften co
rrects this p
rob
lem. Lead
wires sh
ou
ld also
be
checked
a d
islod
ged
or b
roken
lead w
ire may n
ot d
eliver the n
eeded
energ
y.Failu
re to sen
seT
he p
acemaker fires b
ecause it fails to
detect th
e hearts in
trinsic b
eats, resultin
g in
abn
orm
al com
plexes. T
he cau
se may b
e a dead
battery, d
ecrease of P
wave o
r QR
Svo
ltage, o
r dam
age to
a pacin
g lead
wire. O
ne serio
us p
oten
tial con
sequ
ence m
ayb
e an R
-on
-T p
hen
om
eno
n.
Oversen
sing
Th
e pacem
aker may b
e too
sensitive an
d m
isinterp
ret mu
scle mo
vemen
t or o
ther
events in
the card
iac cycle as dep
olarizatio
n. T
his erro
r resets the p
acemaker in
ap-
pr o
pr ia te ly , in
c r e a s ing
the a m
ou
nt o
f time b
e for e th
e ne x t d
is c ha r g
e .
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 75
-
76
Pacem
aker Failure to
Sen
seECGS
Pa c e m
a k e r Ov e r s e n
s ing
2142_Tab02_032-079.qxd 9/12/09 3:00 PM Page 76
-
Artifact
A
rtifacts are EC
G d
eflection
s caused
by in
fluen
ces oth
er than
the h
earts electrical activity.
Loo
se Electro
des
77
ECGS
Ba s e lin
e Va r ie s W
it h R
e s pir a t io
n
2142_Tab02_032-079.qxd 9/12/09 3:01 PM Page 77
-
78
60-Cycle In
terference
ECGS
Re g u la r R-R in te rv a ls
Mu
s c le Ar t ifa c t
Clin
ical Tip:N
ever con
fuse m
uscle artifact w
ith A
-fib if th
e rhyth
m is reg
ular.
2142_Tab02_032-079.qxd 9/12/09 3:01 PM Page 78
-
Notes:79
ECGS
2142_Tab02_032-079.qxd 9/12/09 3:01 PM Page 79
-
12-LEAD
80
The 12-Lead ECG
A standard 12-lead ECG provides views of the heart from 12 different angles.This diagnostic test helps to identify pathological conditions, especially bun-dle branch blocks and T wave changes associated with ischemia, injury, andinfarction. The 12-lead ECG also uses ST segment analysis to pinpoint thespecific location of an MI.
The 12-lead ECG is the type most commonly used in clinical settings.The following list highlights some of its important aspects:
The 12-lead ECG consists of the six limb leadsI, II, III, aVR, aVL, andaVFand the six chest leadsV1, V2, V3, V4, V5, and V6.
The limb leads record electrical activity in the heart's frontal plane.This view shows the middle of the heart from top to bottom.Electrical activity is recorded from the anterior-to-posterior axis.
The chest leads record electrical activity in the heart's horizontalplane. This transverse view shows the middle of the heart from left toright, dividing it into upper and lower portions. Electrical activity isrecorded from either a superior or an inferior approach.
Measurements are central to 12-lead ECG analysis. The height anddepth of waves can offer important diagnostic information in certainconditions, including MI and ventricular hypertrophy.
The direction of ventricular depolarization is an important factor indetermining the axis of the heart.
In an MI, multiple leads are necessary to recognize its presence anddetermine its location. If large areas of the heart are affected, thepatient can develop cardiogenic shock and fatal arrhythmias.
ECG signs of an MI are best seen in the reciprocal, or reflecting,leadsthose facing the affected surface of the heart. Reciprocal leadsare in the same plane but opposite the area of infarction; they show a"mirror image" of the electrical complex.
Prehospital EMS systems may use 12-lead ECGs to discover signs ofacute MI, such as ST segment elevation, in preparation for in-hospitaladministration of thrombolytic drugs.
After a 12-lead ECG is performed, a 15-lead, or right-sided, ECG maybe used for an even more comprehensive view if the right ventricle orthe posterior portion of the heart appears to be affected.
2142_Tab03_080-093.qxd 9/12/09 2:15 PM Page 80
-
81
12-LEAD
R Wave Progression
Normal ventricular depolarization in the heart progresses from rightto left and from front to back.
In a normal heart, the R wave becomes taller and the S wave smalleras electrical activity crosses the heart from right to left. This phenom-enon is called R wave progression and is noted on the chest leads.
Alteration in the normal R wave progression may be seen in left ventric-ular hypertrophy, COPD, left bundle branch block, or anteroseptal MI.
V1 V2 V3V4
V5
V6
Leftlung
Rightlung
NNoorrmmaall RR wwaavvee pprrooggrreessssiioonn iinn cchheesstt lleeaaddss VV11VV66
2142_Tab03_080-093.qxd 9/12/09 2:15 PM Page 81
-
12-LEAD
82
Electrical Axis Deviation
The electrical axis is the sum total of all electrical currents generatedby the ventricular myocardium during depolarization.
Analysis of the axis may help to determine the location and extent ofcardiac injury, such as ventricular hypertrophy, bundle branch block,or changes in the position of the heart in the chest (e.g., from preg-nancy or ascites).
The direction of the QRS complex in leads I and aVF determines theaxis quadrant in relation to the heart.
30
0180
90
90
30
60120
150
150
III II
I
aVF
aVR aVL
II
aVF
I
aVF
aVF
I
aVF
Normal A
xis
Right Axis Deviation
Axi
s De
viation
Extrem
e Righ
t Left Axis Deviation
EElleeccttrriiccaall aaxxiiss ooff tthhee hheeaarrtt..
CClliinniiccaall TTiipp:: Extreme right axis deviation is also called indeterminate,"no man's land," and "northwest."
2142_Tab03_080-093.qxd 9/12/09 2:15 PM Page 82
-
83
12-LEAD
Ischemia, Injury, and Infarction in Relation to the Heart
Ischemia, injury, and infarction of cardiac tissue are the three stages result-ing from complete blockage in a coronary artery. The location of the MI iscritical in determining the most appropriate treatment and predicting prob-able complications. Each coronary artery delivers blood to specific areas ofthe heart. Blockages at different sites can damage various parts of theheart. Characteristic ECG changes occur in different leads with each typeof MI and can be correlated to the blockages.
Anterior wall
Anterior view
LLooccaattiioonn ooff MMII bbyy EECCGG LLeeaaddss
I lateral aVR V1 septal V4 anterior
II inferior aVL lateral V2 septal V5 lateral
III inferior aVF inferior V3 anterior V6 lateral
Lateral wall
Septal wall Inferior wall
Anterior view Posterior view
CClliinniiccaall TTiipp:: Lead aVR may not show any change in an MI.
CClliinniiccaall TTiipp:: An MI may not be limited to just one region of the heart.For example, if there are changes in leads V3 and V4 (anterior) and leads I,aVL, V5, and V6 (lateral), the MI is called an anterolateral infarction.
2142_Tab03_080-093.qxd 9/12/09 2:15 PM Page 83
-
12-LEAD
84
Progression of an Acute Myocardial Infarction
An acute MI is a c