

Daniel J. Hettich March, 2013 - American Health … · Daniel J. Hettich March, 2013 2...
20
1 Medicare Value-Based Purchasing for Hospitals: A New Era in Payment Daniel J. Hettich March, 2013 2 Introduction: Evolution of Medicare as a Purchaser Evolution of Medicare as a Purchaser • Cost reimbursement ― rewards more services but capped at “reasonable costs” • Prospective payment ― Flat fee; incentives for efficiency but still rewards volume • Value based purchasing (VBP) ― adds incentives for quality of services ― Foundation in Inpatient Quality Reporting Program, began in 2005, which withheld 2% of payments for failing to report performance on quality measures
Transcript of Daniel J. Hettich March, 2013 - American Health … · Daniel J. Hettich March, 2013 2...

1
Medicare Value-Based Purchasing for Hospitals: A New Era in Payment
Daniel J. Hettich
March, 2013
2
Introduction: Evolution of Medicare as a PurchaserEvolution of Medicare as a Purchaser
• Cost reimbursement
― rewards more services but capped at “reasonable costs”
• Prospective payment
― Flat fee; incentives for efficiency but still rewards volume
• Value based purchasing (VBP)
― adds incentives for quality of services
― Foundation in Inpatient Quality Reporting Program, began in 2005, which withheld 2% of payments for failing to report performance on quality measures

2
3
4
VBP Program Concept
• Set aside a pool from existing Medicare PPS dollars
― Funded through reductions in base operating DRG per discharge payment reductions
― 1% in FY2013 up to 2% in FY2017 forward― Estimated pool for FY 2013 = $917
• Redistribute the pool among PPS hospitals based on their performance on certain quality measures
― as compared to other hospitals
― as compared to each hospital’s prior performance
• Create incentives to improve quality—race to the top

3
5
Who Participates in VBP Program?
• All “subsection (d) hospitals”• Exempt or excluded hospitals― IPPS-excluded hospitals ― Payment reduction under IQR― Cited for health or safety deficiencies during
performance period (CMS’s policy requires immediate jeopardy citations noted on at least two Form CMS-2567s issued after a State survey)
― Puerto Rico hospitals― Maryland hospitals (temporary exemption)― Need to have minimum # of cases (e.g., at least 100
HCAHPS surveys)
6
Components of the VBP Program
• Four Primary components
― 1. The Measures
― 2. The Performance Standards
― 3. The Score
― 4. The Payment

4
7
VBP Measures
• Must be listed on HospitalCompare for at least one year prior to use
• Quality Measures divided into differently weighted buckets or “domains”
• Two domains for FFY 2013:
― Process of Care (70%) and Patient Satisfaction (HCAHPS) (30%)
8
12 Clinical Process of Care Measures
Weighted Value of Each Domain
8 Patient Experience of
Care Dimensions
2013 Hospital VBP Domains and Measures
Source: CMS

5
9
Performance Standards: How Will Hospitals Be Evaluated?
Improvement vs. Achievement
Source: CMS
10
Threshold v. Benchmark
Source: CMS

6
11
Scoring
• Achievement― 10 pts for meeting or exceeding the benchmark― 0 pts for performing below threshold― 1-9 on a linear scale between the threshold and
benchmark• Improvement― Similar formula to achievement score― 0 pts if below hospital’s own baseline score; 1-9
pts on a linear scale if above baseline score; 10 pts for meeting national benchmark
12
Performance period
Baseline period •0429
7
.8163•
Achievement Range
Improvement Range
Hospital A earns 6 points for achievementHospital A earns 7 points for improvementHospital A score = higher of achievement or improvement = 7 points
ScoreScore
1 2 3 4 5 6 7 8 9 10
0 1 2 3 4 5 6 7 8 9 10
Sample VBP Score for Process Measure
Measure: AMI-7a-Fibrinolytic Therapy
.9191 •
Benchmark
• • •• • • • • ••
•Achievement
Threshold
.6548 Achievement Range
• • • • • • • • •• •
•••
7
13
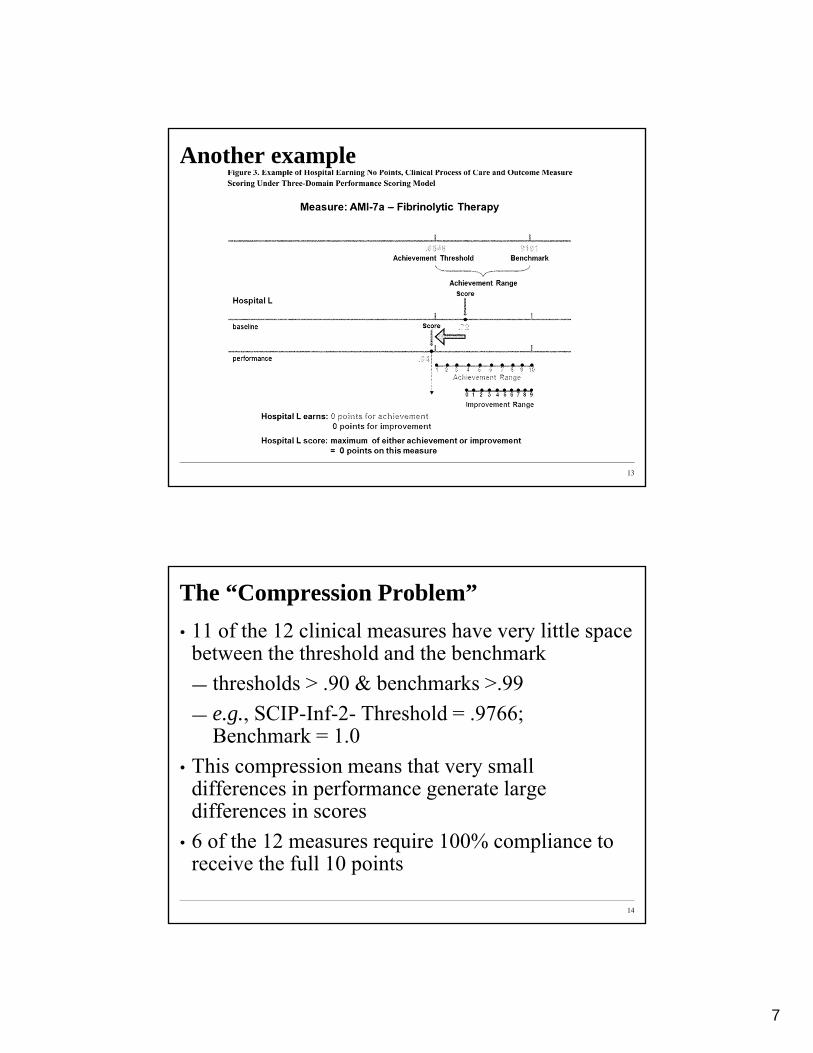
Another example
14
The “Compression Problem”
• 11 of the 12 clinical measures have very little space between the threshold and the benchmark
― thresholds > .90 & benchmarks >.99
― e.g., SCIP-Inf-2- Threshold = .9766; Benchmark = 1.0
• This compression means that very small differences in performance generate large differences in scores
• 6 of the 12 measures require 100% compliance to receive the full 10 points

8
15
Clinical Process of Care Domain
Performance Standards based on National Measure Rates
Source: CMS
16
HCAHPS Scores
• Must report minimum of 100 surveys
• Eight dimensions are weighted equally
• Achievement - 0-10 points
• Improvement - 0-9 points
• Formulas are similar to process scores
• Can also achieve up to 20 points for “consistency”
• Total = sum larger of achievement or improvement for each measure + consistency score

9
17
HCAHP Floor, Threshold and Benchmark Scores
(76 Fed. Reg. 26490, 26519)
New York Times Op-Ed, March 15, 2012

10
19
2014 VBP Program
• New Outcome Domain for FFY 2014:
― Process of Care (45%), HCAHPS (30%), Outcome measures (30-day mortality for AMI, HF, and PN) (25%)
20
Added Outcome Domain to 2014 VBP Program
(76 Fed. Reg. 74122, 74536)

11
21
2014 Baseline and Performance Periods
(76 Fed. Reg. 74122, 74535)
22
Posted on Hospital Compare for at Least a Year?• CMS had initially finalized a policy to have 4 domains in
2014 and two additional outcome measures (HAC and AHRQ outcome measures).
• CMS revised its finalized policy, however. • Effective dates of the HAC, AHRQ, and Medicare
spending per beneficiary measures are suspended― Rationale: data on these measures will not have been
made publicly available on Hospital Compare for at least one year prior to these dates
― Policy: CMS will publicly post hospital performance on all candidate measures on Hospital Compare for at least one year prior to the time when the performance period for those measures would start.

12
23
• Adding two new measures to the outcome domain:— CLABSI: (Central Line-Associated Blood
Stream Infection measure) which is an HAI measure that assesses the rate of bloodstream infection or clinical sepsis among ICU patients
— AHRQ PSI composite measure (PSI-90) which is a composite measure of patient safety indicators developed and maintained by AHRQ.
2015 VBP Outcome Measures
24
• Significant concerns raised by commenters regarding reliability of some measures especially the mortality measures
• CMS replied: “We do not believe that focusing on the individual measure’s reliability, to the exclusion of its contribution to the reliability of the TPS, is the sole criterion for assessing the appropriateness of adopting measures to the Hospital VBP Program.”
• “Moderate reliability for the majority of hospitals” appears to be sufficient for CMS
• CMS did, however, increase the case minimum from 10 cases to 25 cases for the mortality measures.
2015 VBP Outcome Measures (cont.)

13
25
• Adopted new “efficiency” domain with one measure: the Medicare Spending per Beneficiary (MSB)
— MSB will include all Part A and Part B payments from 3 days prior to admission through 30 days post discharge with certain exclusions
— Risk adjusted for age and severity of illness, and payments are standardized to remove differences attributable to geographic payment adjustments and other payment factors (e.g., DSH)
— Excludes high-cost outliers.
2015 VBP “Efficiency Domain”
26
2015 VBP “Efficiency Domain”–Thresholds and Benchmarks
• Proposed threshold, i.e., minimum score for a hospital to receive any achievement points for the measure, would be the “median [MSB] ratio across all hospitals during the performance period”
• Proposed benchmark to receive full 10 points would be the “mean of the lowest decile of [MSB] ratios across all hospitals during the performance period,” i.e., spending in lowest 5% of hospitals nationally
• Example: For May 15, 2010 – Feb. 14, 2011, median MSB was $17,988; benchmark $14,495

14
27
• Considered either 25 or 50 case minimum to receive a efficiency domain score
— Adopted 25 case minimum although at that level 95 percent of the time a hospital with an average underlying efficiency level (that is, 1.0) would receive a Medicare spending per beneficiary measure score between 0.81 and 1.23 (quite a range)
• CMS submitted the proposed measure to the NQF for endorsement on July 2, 2012
• CMS posted hospital performance on the Medicare Spending per Beneficiary measure on the Hospital Compare Web site on April 19, 2012
2015 VBP “Efficiency Domain”
28
2015 VBP Performance and Baseline Periods

15
29
2015 Domain Weightings
• Clinical process of care domain (20%), patient experience of care domain (HCHAP) (30%), outcome domain (30%), and the efficiency domain (MSB) (20%).
• Starting with 2015, a hospital will receive a score for the outcome domain if it has enough cases for just two out of the five outcome measures.
• In addition, scores in two out of the four domains sufficient to participate in 2015.
• CMS will reapportion the remaining domain weights so that they still total 100%.
30
• Adopted a 21-month performance period for the outcome measures, from October 1, 2012 through July 30, 2014, with a shorter baseline period of October 1, 2010 through July 30, 2011
2016 VBP Performance/Baseline Periods

16
31
Calculating Total Score
• Will only use measures that apply to the hospital
• Convert to percentage of total points available
• For FY 2013, Total Performance Score is weighted
― 70% clinical process of care
― 30% HCAHPS
32
Simulated Hospital ReportEstimated TPS Summary
Source: CMS

17
33
The Payment
• Payment Exchange Function
― CMS looked at several possibilities (linear, cube, logistic) and decided on linear
• The payment works as an adjustment to base operating DRG per discharge payment
Definition of Base DRG Amount• “Base operating DRG payment amount” will be the wage
and transfer adjusted DRG operating payment plus any applicable new technology add-on payment but excludingoutlier, IME, DSH, and low-volume payment adjustments.
• Budget neutral
34
Simulated Hospital ReportEstimated Value-Based Incentive Payment Percentage
Source: CMS

18
35
Misc. Matters• Correction process: Hospitals will have 30-days to review their
confidential claims based reports and their TPS Reports available on their QualityNet accounts and submit corrections via QualityNet― VBP exclusion determination will not be subject to correction
• Appeal process: Correction process prerequisite to appeal― Detailed technical appeal requirements (e.g., no P.O. Boxes)― The appealable issues are limited to technical errors, e.g., whether
CMS properly used the higher of the achievement/improvement points and whether each domain was weighted properly (i.e., 70%, 30%) and then properly summed in calculating the TPS
• New Measures― Proposed subregulatory process for adding and retiring measures― Rejected (preserves notice-and-comment)― Measures may be adopted for IQR and VBP at the same time
• VBP performance published on HospitalCompare
36
Tips for Improving VBP Performance• Know where your hospital stands on each selected
measure for the baseline period and identify which measures have the best rate of return. ― For example, if a hospital was at the benchmark for a
compressed measure in its baseline period, then a slight percentage change in score on that measure for the performance period could cause the hospital to lose 10 points (if it drops below the compressed threshold)
― On the other hand, it could take a very large percentage improvement to pick up less than 9 points, as an improvement score, on a measure where the hospital was well below the threshold for the benchmark period
― In that scenario, it may make sense to play defense first, before devoting resources to improvement on the latter measure

19
37
Tips for Improving VBP Performance (cont.)• Understand how discharge volume by measure
factors into the VBP score
― Each clinical performance measure has an equal weight
― An orthopedic hospital’s great performance on clinical process indicators in hundreds of surgical cases could, therefore, be offset by missing performance indicators in a handful of heart failure cases
38
Questions?


















