D. Integri n - 1 File Download
30
Item: 1 of 5 1 • M k -<:J 1>- Jil QIO: 30 69 ..L ar Previ ous Next Lab fli!l tu es Not es Calc ulator • 1 . 2 • 3 ·4 • 5 A 5-year-old girl is brought to the pediatrician because of generalized edema. Laboratory testing reveals proteinuria of 5 g/day, and podocyte foot process appear sho•·tened and thinner than usual when visualized with electron microscopy of a kidney biopsy . Disruption of which of the following components of the filtration barrier is contributing to this patient's proteinuria? : A. Brush border B. Endothelial cell C. Heparan sulfate D. Integrin E. Type IV collagen a s 8 Lock Suspend End Bl ock •
Transcript of D. Integri n - 1 File Download

Item: 1 of 5 ~ 1 • M k -<:J 1>- Jil ~· !:';-~ QIO: 3 069 ..L a r Prev ious Next Lab fli!ltues Notes Calcula t o r
• 1
. 2
• 3
· 4
• 5
A 5-year-old girl is brought to the pediatrician because of generalized edema. Laboratory testing reveals proteinuria of 5 g/day, and podocyte
foot process appear sho•·tened and thinner than usual when visualized with electron microscopy of a kidney biopsy.
Disruption of which of the following components of the filtration barrier is contributing to this patient's proteinuria?
: A. Brush border
B. Endothelial cell
C. Heparan sulfate
D. Integrin
E. Type IV collagen
a s 8 Lock Suspend End Block
•

Item: 1 of 5 ~ . I • M k <:] t> al ~· ~ QIO: 3069 .l. ar Previous Next lab 'lifllues Notes Calculator
1
. 2
• 3
. 4
• 5
The correct answer is C. 470fo chose this.
The g lomerular filtration barrier is composed of endothelial cells, g lomerular basement membrane, and epithelial podocytes. It is responsible for the filtration of plasma according to size, shape, and net charge. The d istances between the podocyte foot processes (filtration slits), the pores of the g lomerular basement membrane, and the fenestrations between the endothelial cells limit the size and shape of the filtrate. The negatively
charged heparan sulfate in the g lomerular basement membrane prevents negatively charged molecules, such as albumin, from being filtered into the urine. This patient has minimal change d isease manifested by nephrotic syndrome, in which the negatively charged heparan sulfate is lost, thereby allowing plasma protein to be lost in the urine. Podocyte foot process effacement is often seen on electron microscopy in minimal change d isease as well, though the role of this finding in the pathophysiology of the d isease is less clear. Podocyte Nephrotic syndrome Glomerular basement membrane Basement membrane Heparan sulfate Minimal change disease Albumin Protein Epithelium
Blood plasma Electron microscope Glomerulus Urine Endothelium Glomerulus (kidney) Blood proteins Renal function Cell membrane Biological membrane
A is not correct. 90fo chose this.
A brush border is characteristic of the proximal tubules and refers to the thickened appearance of the apical surface of these tubules due to the presence of microvilli covered by a dense g lycocalyx . It is not part of the g lomerulus and is not affected in minimal change d isease. Glycocalyx Microvillus Minimal change disease Glomerulus (kidney) Cell membrane Nephron Proximal convoluted tubule Anatomical terms of location Glomerulus
B is not correct. 190/o chose this.
The endothelial cell, as explained below, makes up part of the g lomerular filtration barrier. However, it is intact in minimal change d isease. Endothelium Minimal change disease Glomerulus (kidney) Glomerulus Renal function
0 is not correct. 11 Ofo chose this.
Integrins are transmembrane proteins that serve as cell adhesion molecules, allowing cells to adhere to the underlying extracellular matrix. In leu kocyte adhesion deficiency type 1, a deficiency in ~ -2 integ rin resu lts in an inability on the part of leu kocytes to adhere to the endothelium for transmigration into the tissue, resu lting in recu rrent infections. Integrins are not involved in the g lomerular filtration barrier and play no role in the etiology of minimal change d isease. Extracellular matrix Integrin Endothelium White blood cell Cell adhesion molecule Cell adhesion Transmembrane protein Etiology Protein Glomerulus Extracellular
E is not correct. 140/o chose this.
Type IV collagen is the collagen component of the basement membrane and is not compromised in nephrotic syndrome. When mutated, however, it g ives rise to a form of basement membranopathy known as Alport syndrome. This syndrome is characterized by lens d isplacement, •
6 s 0 lock Suspend End Block

Item: 1 of 5 ~ . I • M k <:] t> al ~· ~ QIO: 3069 .l. ar Previous Next lab 'lifllues Notes Calculator
1
. 2
• 3
. 4
• 5
A is not correct. 90fo c hose t his.
A brush border is characteristic of the proximal tubules and refers to the thickened appearance of the apical surface of these tubules due to the presence of microvilli covered by a dense g lycocalyx . It is not part of the g lomerulus and is not affected in minimal change d isease. Glycocalyx Microvillus Minimal change disease Glomerulus (kidney) Cell membrane Nephron Proximal convoluted tubule Anatomical terms of location Glomerulus
B is not correct. 190/o c hose t his.
The endothelial cell, as explained below, makes up part of the g lomerular filtration barrier. However, it is intact in minimal change d isease. Endothelium Minimal change disease Glomerulus (kidney) Glomerulus Renal function
0 is not correct. 11 Ofo c hose t his.
Integrins are transmembrane proteins that serve as cell adhesion molecules, allowing cells to adhere to the underlying extracellular matrix. In leu kocyte adhesion deficiency type 1, a deficiency in 13-2 integ rin resu lts in an inability on the part of leu kocytes to adhere to the endothelium for transmigration into the tissue, resu lting in recu rrent infections. Integrins are not involved in the g lomerular filtration barrier and play no role in the etiology of minimal change d isease. Extracellular matrix Integrin Endothelium White blood cell Cell adhesion molecule Cell adhesion Transmembrane protein Etiology Protein Glomerulus Extracellular
E is not correct. 140/o c hose t his.
Type IV collagen is the collagen component of the basement membrane and is not compromised in nephrotic syndrome. When mutated, however, it g ives rise to a form of basement membranopathy known as Alport syndrome. This syndrome is characterized by lens d isplacement, cataracts, and nerve deafness and is associated with hematuria. Alport syndrome Nephrotic syndrome Hematuria Collagen Basement membrane Type IV collagen Hearing loss Sensorineural hearing loss Cataract
Bottom Line :
In minimal change d isease, with d isruption of negatively charged heparan sulfate, negatively charged albumin is no longer repelled and protein is lost in the urine. This d isruption can be seen on electron microscopy as podocyte effacement and manifests as edema, proteinuria, and hyperlipidemia. Podocyte Minimal change disease Proteinuria Hyperlipidemia Heparan sulfate Albumin Protein Electron microscope Edema Urine Microscopy
6 s 0 lock Suspend End Block

Item: 1 of 5 ~ 1 • M k -<:J I> ~ £!1}>' !!":-~ a r • QIO: 3 069 ..L Prev ious Next Lab lues Notes Calcula t o r
1
. 2
• 3
· 4
• 5
Glomerular filtration barrier
Nephritic syndrome
Acute poststreptococcal glomerulonephritis
Responsible for filtration of plasma according to size and charge selectivity.
Composed of: • Fenestrated capillary endothel ium
Basement membrane with trpe IV collagen chains and heparan sulfate Epithelial layer consisting of podoc) te foot processes ·
FA17 p 551 .2
Charge barrier-all 3 layers contain 8 charged gi)COproleins preventing<±> charged molecule entry (eg, albumin). ize barrier-fenestrated capillary epithelium (pre,ent entrr of> 100 nm molecules/blood cells); podocyte foot processes interpose "it h basement membrane; slit diaphragm (prevent entr\" of molecules> 50-60 nm).
'
FA17 p 564.1
f\cphrltic syndrome= Inflammatory process. When glomeruli are in\"Oived, leads to hematuria and RBC casts in urine. Associated with azotemia, oliguria, hypertension (due to salt retention), proteinuria.
LM-glomeruli en larged and hypercellular fl. I F'-("starry sky") granular appearance
("lumpy-bumpy") (E) due to lgC, l g~ l , and C3 deposition along GB~I and mesangium.
EY!-subepithelial immune complex (IC) humps.
lost frequently seen in children. Occurs - 2-4 weeks after group A streptococcal infection of pharynx or skin. Resolves spontaneously. Type II [ h) persensitivity reaction.
Presents with peripheral and periorbital edema, cola-colored urine, h)-pertension.
,, .. . '
a s 8 Lock Suspend End Block
•
Item: 1 of 5 ~ 1 • M k -<:J 1>- Jil ~· !:';-~ QIO: 3 069 ..L a r Prev ious Next Lab fli!ltues Notes Calcula t o r
1
. 2
• 3
· 4
• 5
Rapidly progressive (crescentic)
glomerulonephritis
Diffuse proliferative glomerulonephritis
lgA nephropathy (Berger disease)
LM and IF - crescent moon shape . Crescents
consist of fibrin and plasma proteins (eg, C3b) with glomerular parietal cells, monoc) tes,
macrophages. Se,·eral disease processes may resuh in this
pattern, in particular: • Goodpasture syndrome-type II
hypersensiti,ity reaction; antibodies to
CBl\1 and akeolar basement membrane -+ linear lF
Granulomatosis with polyangiitis {Wegener)
~1icroscopic Polyangiit is
Often due to SLE or membranoproliferative glomerulonephritis.
LM-"wire looping" of capillar ies. EM-subendothelial and sometimes
intramembranous IgG-bascd ICs often with
C3 deposition. lF -granular.
LM-mesangial proliferation. E~~l-mesangiai!C deposits. 114_ l l'r.1_h ... C"Arl rr A~nn.C' ;f (' ; ..... rnJ!It.C''lnn: ...... ,
I
Poor prognosis. Rapidly deteriorating renal function (days to ,,·eeks).
11ematuria/hemoptrsis. Treatment: emergent plasmapheresis.
PR3-ANCA/c-Al CA. Pauci-immune (no lg/C3
deposition). l\IPO-ANCA/p-ANCA. Pauci-immune (no Ig/C3
deposition).
A common cause of death in SLE {think "wire
lupus"). DPCr and MPC often present as
nephrotic syndrome and nephritic syndrome concurrently.
Episodic gross hematuria that occurs
concurrently" ith respiratory or Gltracl ;n(A,...t-;n.n(' {1,...,.1 ; (' C'ArrAf-Ar) hu l"nn,..I'\C"'l ) l;n;nnc-\
a s 8 Lock Suspend End Block

Item: 1 of 5 ~ 1 • M k -<:J 1>- Jil ~· !:';-~ QIO: 3 069 ..L a r Prev ious Next Lab fli!ltues Notes Calcula t o r
1
. 2
• 3
· 4
• 5
Nephrotic syndrome
Minimal change disease (lipoid nephrosis)
Focal segmental glomerulosclerosis
FA17 p566.1
I\ephrO tic syndrome-massi'e prO teinuria {> 3.5 glday) with hypoalbuminemia, resulting
edema, hyperlipidemia. Frothy urine" ith fatly casts. Due to podocyte damage disrupting
glomerular filtration charge barrier. \llay be 1° {eg, direct sclerosis of podocytes) or 2° {systemic
process [eg, diabetes] secondarily damages podocytes). Associated with hypercoagulable state {eg,
thromboembolism) due to antithrombin ( T ) Ill loss in urine and t risk of infection {due to loss of
immunoglobulins in urine and soft tissue compromise by edema).
Se,·ere nephritic syndrome may present with nephrotic S}lldrome features {nephritic-nephrotic
syndrome) if damage to C B I is severe enough to damage charge barrier.
LM-normal glomeruli {lipid may be seen in PCT cells).
IF8. EM-effacement of foot processes t'J.
LM-segmental sclerosis and hyalinosis : .
IF - often 8, but may be<±> for nonspeci Fie focal
deposits of Ig r, C3, C l. EM -effacement of foot process similar to
minimal change disease.
\!lost common cause of nephrotic S)lldrome in children. Often 1° (idiopathic) and ma) be
triggered by recent infection, immunization, immune stimulus. Rarely, may be zo to
lymphoma (eg, cytokine-mediated damage). I 0
disease has excellent response to corticosteroids.
Mo~t common cause of nephrotic syndrome in
African Americans and Hispanics. Can be ]0
{idiopathic) or zo to other conditions {eg, H IV
infection, sickle cell disease, heroin abuse,
massive obesity, interferon treatment, chronic
kidney disease due to congenital malfom1ations).
1° disease has inconsistent response to steroids. ~lay progress to chronic renal disease.
T , , •·rr ... ... ' . . r• n
a s 8 Lock Suspend End Block
•

Item: 2 of 5 ~ 1 • M k -<:J 1>- Jil ~· !:';-~ QIO: 3 052 ..L a r Prev ious Next Lab fli!ltues Notes Calcula t o r
1
. 2
• 3
· 4
• 5
Two weeks after recovering from a viral illness, a 5-year-old boy presents to the physician with frothy urine as well as periorbital and lower
extremity edema. The physician wants to empirically begin steroid therapy, but the parents first want to obtain a diagnosis. A kidney biopsy shows no evidence of renal pathology.
What other aberration would be expected in this patient?
A. Azotemia
B. Decreased cardiac output
C. Hematuria
D. Hyperlipidemia
E. Hypertension
a s 8 Lock Suspend End Block
•

Item: 2 of 5 ~ . I • M k <:] t> al ~· ~ QIO: 3052 .l. ar Previous Next lab 'lifllues Notes Calculator
1
2
• 3
. 4
• 5
The correct answer is 0. 550/o chose this.
This is a classic presentation for minimal change d isease (MCD}, the most common cause of nephrotic syndrome in children . Typically, nephrotic syndrome is accompanied by proteinuria, hypoalbuminemia, and hyperlipidemia. The lower protein levels in the serum decrease oncotic pressure, which leads to extracellular fluid leaving the plasma and subsequent edema. The liver ramps up production of proteins, resu lting in a secondary hyperlipidemia. The loss of antithrombin III can also resu lt in a hypercoagulable state, though this is more common in other nephrotic syndromes such as membranous nephropathy. No changes are evident in the kidneys under light microscopy, but electron microscopy reveals loss of epithelial foot processes. MCD is often associated with viral and parasitic infections, d rugs, tumors, and even some allergies to food, dust, and pollen . Transient proteinuria is the most common cause of proteinuria in children . Unlike MCD, which is considered persistent proteinuria, it on ly occu rs du ring the inciting problem and resolves afterward . The proteinuria will resolve within 48 hours if it is due to exercise and will resolve within 10-14 days if due to a fever. Other causes of transient proteinuria in children include viral exposu re, seizures, and congestive heart failure .
Nephrotic syndrome Hypoalbuminemia Minimal change disease Oncotic pressure Hyperlipidemia Antithrombin Membranous glomerulonephritis Heart failure
Congestive heart failure Proteinuria Edema Thrombophilia Blood plasma Protein Electron microscope Extracellular fluid Kidney disease liver Kidney
Serum (blood) Epithelium Epileptic seizure Allergy Fever Optical microscope Parasitism Virus Microscopy Coagulation
A is not correct. 140/o chose this.
Azotem ia is an excess of nitrogenous wastes in the blood and is a characteristic of nephritic syndrome. It would not be a likely consequence of minimal change d isease, although occasionally fluid loss into the interstitium and/or a high tubular cell protein load can lead to decreased renal function . Nephritic syndrome Minimal change disease Azotemia Protein Renal function Nephron Nephritis Interstitial fluid Kidney
B is not correct. 60/o chose this.
Decreased cardiac output can be seen in congestive heart failure and would lead to pulmonary edema, as well as edema in the lower extrem ities, but would not be an associated sequela of minimal change d isease. Card iac output would most likely stay constant due to a compensatory increase in heart rate (recall the equation CO= SV x HR}. Sequela Minimal change disease Heart failure Congestive heart failure Pulmonary edema Cardiac output Edema Heart rate
C is not correct. 150/o chose this.
Hematu ria is characteristic of nephritic syndrome. Causes of nephritic syndrome in children include lgA nephropathy, Henoch-Schon lein purpura, hemolvtic uremic svndrome. and ooststreotococcal a lomeruloneoh ritis . Hematu ria is seen in uo to 20% of children with minimal chanae d isease
6 s 0 lock Suspend End Block

Item: 2 of 5 ~ . I • M k <:] t> al ~· ~ QIO: 3052 .l. ar Previous Next lab 'lifllues Notes Calculator
1
2
• 3
. 4
• 5
Azotem ia is an excess of nitrogenous wastes in the blood and is a characteristic of nephritic syndrome. It would not be a likely consequence of minimal change d isease, although occasionally fluid loss into the interstitium and/or a high tubular cell protein load can lead to decreased renal function . Nephritic syndrome Minimal change disease Azotemia Protein Renal function Nephron Nephritis Interstitial fluid Kidney
B is no t correct. 6 0/o c hose this.
Decreased cardiac output can be seen in congestive heart failure and would lead to pulmonary edema, as well as edema in the lower extrem ities, but would not be an associated sequela of minimal change d isease. Card iac output would most likely stay constant due to a compensatory increase in heart rate (recall the equation CO = SV x HR}. Sequela Minimal change disease Heart failure Congestive heart failure Pulmonary edema Cardiac output Edema Heart rate
C is no t correct. 1 50/o c hose this.
Hematu ria is characteristic of nephritic syndrome. Causes of nephritic syndrome in children include lgA nephropathy, Henoch-Schon lein purpura, hemolytic uremic syndrome, and poststreptococcal g lomeruloneph ritis . Hematu ria is seen in up to 20% of children with minimal change d isease and up to one-th ird of adults. Hematuria Nephritic syndrome IgA nephropathy Minimal change disease Hemolytic-uremic syndrome Glomerulonephritis Kidney disease Immunoglobulin A
Nephritis Purpura Streptococcus Nephron Hemolysis
E is no t correct. 100/o c hose this.
Hypertension is a characteristic of nephritic syndrome. Hypertension is seen in up to 30% of children with minimal change d isease. Nephritic syndrome Minimal change disease Hypertension Nephron Nephritis
Botto m Line :
Symptoms of proteinuria, hypoalbuminemia, and hyperlipidemia in a child are consistent with minimal change d isease. The kidney appears normal on light microscopy. Hypoalbuminemia Proteinuria Minimal change disease Hyperlipidemia Kidney Optical microscope Microscopy
6 s 0 lock Suspend End Block

Item: 2 of 5 ~ 1 • M k -<:J 1>- Jil ~· !:';-~ QIO: 3 052 ..L a r Prev ious Next Lab fli!ltues Notes Calcula t o r
1
2
• 3
· 4
• 5
Nephrotic syndrome
Minimal change disease (lipoid nephrosis)
Focal segmental glomerulosclerosis
FA17 p566.1
f\ephrO tic syndrome-massi\e prO teinuria (> 3.5 glday) with hypoalbuminemia, resulting
edema, h) perlipidemia. Frothy urine" ith fatly casts. Due to podocyte damage disrupting
glomerular filtration charge barrier. \ ,lay be 1° (eg, direct sclerosis of podocytes) or 2° (systemic
process [eg, diabetes] secondarily damages podocytes). Associated with hypercoagulable state (eg,
thromboembolism) due to antithrombin ( T ) Ill loss in urine and t risk of infection (due to loss of
immunoglobulins in urine and soft tissue compromise by edema).
Se,·ere nephritic syndrome may present with nephrotic S}lldrome features (nephritic-nephrotic
syndrome) if damage to CBl\1 is severe enough to damage charge barrier.
LM-normal glomeruli (lipid may be seen in PCT cells).
we. EM-effacement of foot processes tl
LM-segmental sclerosis and hyalinosis : .
IF- often 8, but may be® for nonspecific focal
deposits of Ig !, C3, C l. E If-effacement of foot process sim ilar to
minimal change disease.
\tfost common cause of nephrotic S)lldrome in children. OFten 1° (idiopathic) and ma) be
triggered by recent infection, immunization, immune stimulus. Rarely, may be zo to
lymphoma (eg, cytokine-mediated damage). I 0
disease has excellent response to corticosteroids.
Most common cause of nephrotic syndrome in
African Americans and Hispanics. Can be !0
(idiopathic) or zo to other conditions (eg, H IV
infection, sickle cell disease, heroin abuse,
massive obesity, interferon treatment, chronic
kidney disease due to congenitalmalfom1ations).
)0 disease has inconsistent response to steroids. ~Jay progress to chronic renal disease.
a s 8 Lock Suspend End Block
•

Item: 2 of 5 ~ 1 • M k -<:J 1>- Jil ~· !:';-~ QIO: 3 052 ..L a r Prev ious Next Lab fli!ltues Notes Calcula t o r
1
2
• 3
· 4
• 5
Nephritic syndrome
Acute poststreptococca I glomerulonephritis
Rapidly progressive (crescentic) glomerulonephritis
FA17 p 564.1
J\ephrltic syndrome= InAammatory process. When glomeruli are involved, leads to hematuria
and RBC casts in urine. Associated with azotemia, oliguria, hypertension (due to salt retention),
proteinuria.
u.,J-glomerul i enlarged and h) percellular f'J. IF' -("starry sky") granular appearance
("lumpy-bumpy") [lJ due to lgC, lg \ I, and C3 deposition along GB I and mesangium.
E~1-subepithelial immune complex (IC)
humps.
LM and IF - crescent moon shape [j. Crescents
consist of fibrin and plasma proteins (eg, C3b) with glomerular parietal cel ls, monocytes,
macro phages. Several d isease processes may result in this
pallern, in particular: • Goodpasture syndrome-type II
hrpersensitivity reaction; antibodies to
CBM and alveolar basement membrane -+ linear IF
lost frequently seen in children. Occurs
- 2-4 weeks after group A streptococcal infection of pharynx or skin. Resolves
spontaneous!). Type Ill h) persensiti' it~
reaction. Presents with peripheral and periorbital edema,
cola-colored urine, hypertension.
Positi,·e strep titers/serologies, ~ complement
b·cls (C3) due to consumption.
Poor prognosis. Rapidly deteriorating renal function (days to weeks).
llematuria/hemoptysis. Treatment: emergent plasmapheresis.
Granulomatosis with oolvanl!iitis (Weeener) PR3-ANCA/c-AJ CA. Pauci-immune (no [f!/C3
a s 8 Lock Suspend End Block
•

Item: 3 of 5 ~ 1 • M k -<:J 1>- Jil ~· !:';-~ QIO: 3455 ..L a r Prev ious Next Lab fli!ltues Notes Calcula t o r
1
2
• 3
· 4
• 5
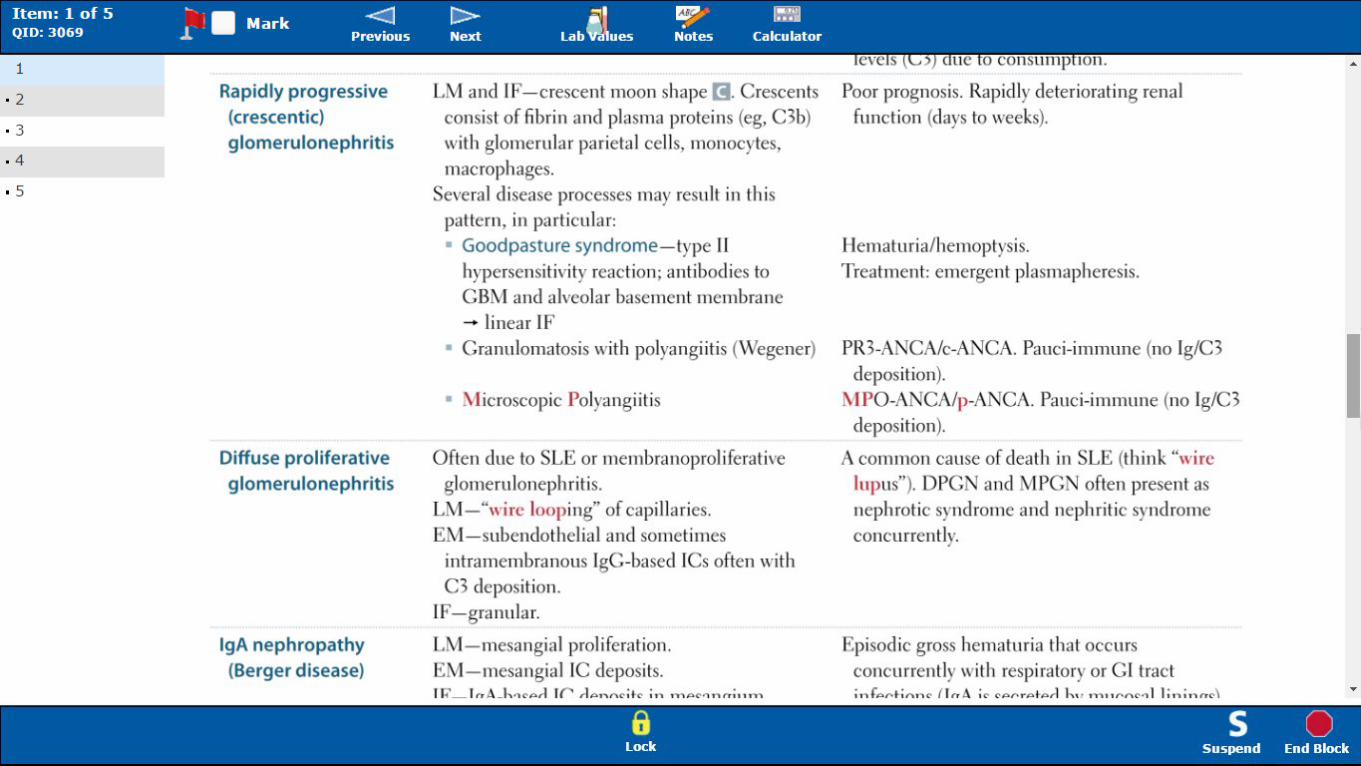
A 35-year-old man suffering from an upper respiratory infection presents to the emergency depa•·tment with complaints of severe muscle
aches, urinary frequency, and "strange-colored urine." He has been drinking large amounts of orange and grapefruit juice in an effort to
combat his cold . His previous medical history is significant only for recently beginning treatment with a statin drug for high cholesterol. His
serum creatinine level is 2.0 mg/dl. A histologic section ofthe patient's kidney is shown in the image.
Which of the following is the most likely diagnosis?
: A. Acute tubular necrosis
a s 8 Lock Suspend End Block
•
Item: 3 of 5 ~ 1 • M k -<:J I> ~ £!1}>' !!":-~ a r • QIO: 3455 ..L Prev ious Next Lab lues Not es Calculat o r
1
2
• 3
· 4
• 5
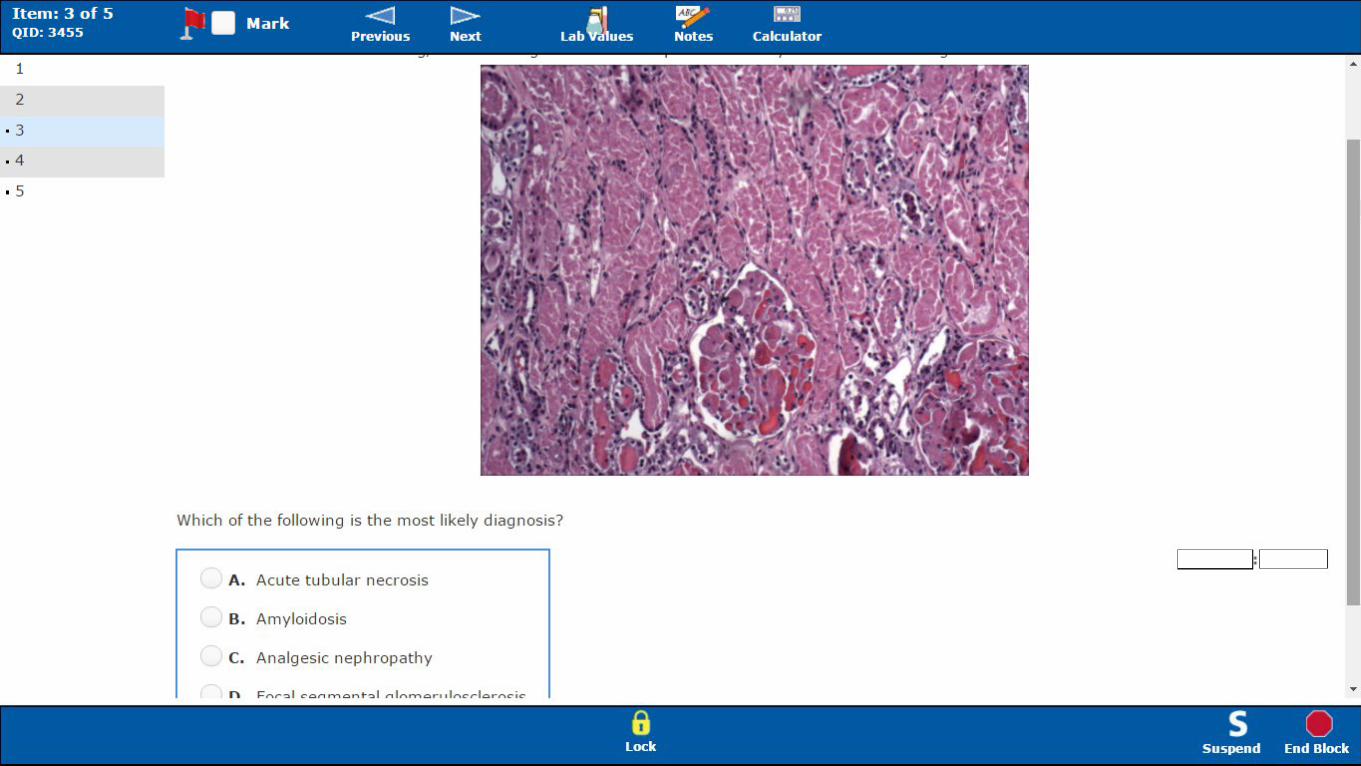
Which of the following is the most likely d iagnosis?
A . Acute tubular necrosis
B. Amyloidosis
C. Analgesic nephropathy
:
a s 8 Lock Suspend End Block
•
Which of the following is the most likely d iagnosis?
: A. Acute tubular necrosis
B. Amyloidosis
C. Analgesic nephropathy
D. Focal segmental glomerulosclerosis
E. Pyelonephritis
a s 8 Lock Suspend End Block

Item: 3 of 5 ~ 1 • M k -<:J 1>- Jil ~· !:';-~ QIO: 3455 ..L a r Prev ious Next Lab fli!ltues Not es Calculat or
1
2
3
· 4
• 5
The correct a ns wer is A. 660/o chose this.
This patient is suffering from acute tubular necrosis (ATN) as a result of
rhabdomyolysis brought on by statin use. Myoglobin released by the muscles is toxic to the kidney tubule cells, especially those of the proximal tubule. In the image shown
here, all of the tubules are necrotic with sloughed pink epithelial cells and debris and loss of nuclear detail. It is commonly associated with oliguria, but ATN actually manifests with increased urine output in SO% of patients. Rhabdomyolysis is an adverse effect of statins that is more likely with higher doses of statins. In addition, statins are metabolized by cytochrome P-450 enzymes. The grapefruit juice inhibited the P-450 enzymes, so that the risk of rhabdomyolysis was increased by increasing statin levels above normal. Statin Rhabdomyolysis Myoglobin Oliguria Acute tubular necrosis Proximal convoluted tubule
Cytochrome P450 Kidney Nephron Urine Necrosis Epithelium Grapefruit Adverse effect
Metabolism Grapefruit juice Anatomical terms of location Enzyme
B is not correct. lQO/o c hose this.
Amyloidosis has a number of causes, but it is characterized histologically by deposits of cotton-candy-like material in the blood vessel walls and the glomeruli. Blood vessel Amyloidosis Glomerulus Glomerulus {kidney) Histology
C is not correct. solo chose this.
Analgesic nephropathy is a type of tubulointerstitial nephritis that is associated with the long-term use of nonsteroidal antiinflammatory drugs
{NSAIDs). The histologic appearance shows interstitial fibrosis and inflammation . Even if the patient has been taking over-the-counter cold
remedies {which often contain NSAIDs), it usually takes many years of high- level exposure to develop this condition . Analgesic Interstitial nephr'tis Nonsteroidal anti - inflammatory drug Analgesic nephropathy Anti-inflammatory Kidney disease Nephritis Over-the-counter drug
Inflammation Fibrosis Histology Interstitial fluid
a s 8 Lock Suspend End Block
•

Item: 3 of 5 ~ 1 • M k -<:J 1>- Jil ~· !:';-~ QIO: 3455 ..L a r Prev ious Next Lab fli!ltues Not es Calculat or
1
2
3
· 4
• 5
• I I • I t I -
Amyloidosis has a number of causes, but it is characterized histologically by deposits of cotton-candy- like material in the blood vessel walls and the glomeruli. Blood vessel Amyloidosis Glomerulus Glomerulus (kidney) Histology
C is n o t correct . soto chose this .
Analgesic nephropathy is a type of tubulointerstitial nephritis that is associated with the long-term use of nonsteroidal antiinflammatory drugs
(NSA!Ds). The histologic appearance shows interstitial fibrosis and inflammation. Even if the patient has been taking over- the-counter cold
remedies (which often contain NSAIDs), it usually takes many years of high-level exposure to develop this condition. Analgesic I te stitial nephritis Nonsteroidal anti-inflammatory drug Analgesic neph o tl f Ant -·nflammatory Kidney disease Nephritis Over-the-counter drug
Inflammation Fibrosis Histology Interstitial fluid
D is not correct. 120/o chose t his .
Focal segmental glomerulosclerosis (FSGS) is unlikely in this patient because it does not have an acute onset. Patients present with nephrotic
signs and symptoms, including edema, massive proteinuria, hypoalbuminemia, and hyperlipidemia. FSGS is also associated with patients with
hepatitis B, C, HIV, SLE, or vasculitis. It is recognized histologically by the sclerosis of parts of a minority of the glomeruli. Hypoalbuminemia Proteinuria Hyperlipidemia Hepatitis B Focal segmental glomerulosclerosis Glomerulus (kidney) Vasculitis Glomerulus Edema HIV
Glomerulosclerosis Systemic lupus erythematosus Hepatitis Histology
E is not correct. 4 0/o c hose this .
Pyelonephritis is usually caused by an ascending infection. It is characterized by tubular necrosis, as seen here, but it is seen on a background of inflammation, with numerous neutrophils present in the tubule lumen. Pyelonephritis Neutrophil Acute tubular necrosis Necrosis Inflammation Lumen (anatomy) Nephron
Bottom Line:
Acute tubular necrosis manifests with tubule cell detachment from basement membrane and sloughing of cells into the lumen. It is associated with statin use. Statin Acute tubular necrosis Basement membrane Necrosis Lumen (anatomy) Nephron
a s 8 Lock Suspend End Block
•

Item: 3 of 5 ~ 1 • M k -<:J 1>- Jil ~· !:';-~ QIO: 3455 ..L a r Prev ious Next Lab fli!ltues Notes Calcula t o r
1
2
3
· 4
• 5
FA17 p 572.2
Acute tubular necrosis lost common cause of acute J..idney injur) in hospitalized patients. Spontaneously resoh-es in
Acute kidney injury (acute renal failure)
Prerenal azotemia
many cases. Can be fatal, especially during initial oliguric phase. f FEI'\a. Key findin g: granular {"muddy brown") casts 3 stages:
l. Inciting event 2 . .Vlaintenancc phasc-oliguric; lasts 1-3 weeks; risk of hyperkalemia, metabolic acidosis,
uremta 3. Recm·ery phase- polyuric; BU ' and serum creatinine fall; risk of hypokalemia
Can be caused by ischemic or nephroto-.: ic injury: lschemic-2° to l renal blood flo,, (eg, h} potension, shock, sepsis, hemorrhage, llF). Rcsuhs in death of tubular cells that may slough into tubular lumen : (PCT and thick ascending limb are highly susceptible to injury).
ephrotoxic-2° to injury rcsuhing from toxic substances (cg, aminoglycosides, radiocontrast agents, lead, cisplatin, ethrlene glycol), crush injury (myoglobinuria}, hemoglobinuria. PCT is particularly susceptible to injury.
FA17 p 571 .2
Acute kidney injury is defined as an abrupt decline in renal function as measured by f creatinine and f BU1 or by oliguria/anuria.
Due to l RBF (eg, hypotension) - l CFR. la+/1120 and BUt retained by kidney in an attempt to l"ni'\(;P n..:,:a cnlttnlP - t Rt f /l"rf.a 'llinin l) r'lfin / R.I J i~ rP~h('nrhPrl I"I"P!l lininP ~ ~ nnt \ !lnl'l 1 ~[,(.
a s 8 Lock Suspend End Block
•

Item: 3 of 5 ~ 1 • M k -<:J 1>- Jil ~· !:';-~ QIO: 3455 ..L a r Prev ious Next Lab fli!ltues Notes Calcula t o r
1
2
3
· 4
• 5 Consequences of renal
failure
Serum BUN/Cr > 20
Inability to make urine and excrete nitrogenous wastes.
Consequences (~lAD II U:\GER}: \tetabolic Acidosis
Dyslipidemia (especial!) t trigl)cericlcs)
l lyperkalemia
Uremia- clinical syndrome marked b) t BUt :
I\'ausea and anorexia
• Pericarditis
• Asterixis
Encepha I opal hy
Platelet dysfunction
~a+/H20 retention (HF', pulmonary edema, hypertension}
G rowth retardation and dcvclop111cntal delay
E rythropoietin fai lure (anem ia)
Renal osteodystrophy
< 15
> 2% (se,·ere)
Varies
FA17 p 571 .3
2 forms of renal failure: acute (cg, AT N) and
chronic (cg, hypertension, diabetes mellitus, congenital anomalies).
a s 8 Lock Suspend End Block
•

Item: 4 of 5 ~ 1 • M k -<:J 1>- Jil ~· !:';-~ QIO: 3 066 ..L a r Prev ious Next Lab fli!ltues Notes Calcula t o r
1
2
3
. 4
• 5
A 35-year-old woman presents to the emergency department because of right flank pain that sta•·ted 1 day prior. She states she has also had i•A] feelings of nausea and pain with urination during this same time period . The patient's past medical history includes diabetes mellitus, A
hyperlipidemia, and hypertension . Vital signs reveal a temperature of 101.7° F, heart rate of 94/min, respiratory rate of 16/min, and a blood
pressure of 130/90 mm Hg . On examination, the patient appears lethargic and has costovertebral tenderness along her right flank. Laboratory results were obtained and were significant for WBC casts in the urine.
Which of the following is the most prominent cell type found in the infiltrate of the involved organ?
: A. Macrophage
B. Monocyte
C. Plasma cell
D. Polymorphonuclear leukocytes
E. T lymphocyte
a s 8 Lock Suspend End Block
•

Item: 4 of 5 ~ . I • M k <:] t> al ~· ~ QIO: 3066 .l. ar Previous Next lab 'lifllues Notes Calculator
1
2
3
4
• 5
The correct answer is 0. 730/o chose this.
The presence of WBC casts in the urine ind icates that this is acute pyelonephritis and not j ust a lower urinary tract infection (UTI } . Pyelonephritis is an acute infection of the renal parenchyma that most often resu lts from an ascending prog ression of a UTI from the bladder. The most frequently involved pathogen is Escherichia coli. Other clinical manifestations of pyelonephritis include dysu ria, urinary frequency, urgency, fever, chills, and nausea and vomiting . A common physical exam finding seen with pyelonephritis is costovertebral tenderness. The presence of WBC casts in the urine ind icates involvement of the kidney, making it a case of pyelonephritis. Acute pyelonephritis, like most acute phases of inflammation, is characterized by a predom inance of polymorphonuclear leu kocytes. It should be noted that the presence of WBCs alone (without casts) would be ind icative of an infection in the lower urinary tract. Urinary tract infection Pyelonephritis Dysuria Escherichia coli Parenchyma Urinary system Urine White blood cell Urinary bladder Kidney Nausea Pathogen
Granulocyte Frequent urination Vomiting Inflammation Physical examination Infection Costovertebral angle tenderness Fever
A is not correct. 100/o chose this.
After 2-3 days, neutrophils are replaced by monocytes, macrophages, plasma cells, and lymphocytes as part of chronic inflammation . Macrophages are longer lived than neutrophils and are capable of proliferating and phagocytosing larger particles. Macrophage Neutrophil lymphocyte Phagocytosis Monocyte Blood plasma Plasma cell Inflammation Chronic inflammation
B is not correct. 60/o chose this.
A monocyte has a kidney-shaped nucleus and d ifferentiates into a macrophage in tissue; it is seen in chronic inflammation . Macrophage Monocyte Inflammation Cell nucleus Chronic inflammation
C is not correct. 4 0fo chose this.
A plasma cell has a d ock-faced chromatin d istribution . B lymphocytes d ifferentiate into plasma cells, which then produce large amounts of antibody. They are a component of humoral immunity. Humoral immunity Blood plasma Chromatin Antibody lymphocyte B cell Plasma cell Humorism Immunity (medical)
E is not correct. ]Ofo chose this.
T lymphocytes are the key component of cell -mediated immunity and are not the primary cell in acute inflammation . Cell-mediated immunity lymphocyte T cell Inflammation Immunity (medical)
6 s 0 lock Suspend End Block

Item: 4 of 5 ~ 1 • M k -<:J 1>- Jil ~· !:';-~ QIO: 3066 ..L a r Prev ious Next Lab fli!ltues Notes Calculat or
1
2
3
4
• 5
chills, and nausea and vomiting. A common physical exam finding seen with pyelonephritis is costove•·tebral tenderness. The presence of WBC
casts in the urine indicates involvement of the kidney, making it a case of pyelonephritis. Acute pyelonephritis, like most acute phases of
inflammation, is characterized by a predominance of polymorphonuclear leukocytes. It should be noted that the presence of WBCs alone (without casts) would be indicative of an infection in the lower urinary tract. Urinary tract nfection Pyelonephritis Dysuria Escherichia coli Parenchyma Urinary system Urine White blood cell Urinary bladder Kidney Nausea Pathogen
Granulocyte F equent urination Vomiting Inflammation Physical examination Infection Costovertebral angle tenderness Fever
A is not correct . lOO/o chose this.
After 2-3 days, neutrophils are replaced by monocytes, macrophages, plasma cells, and lymphocytes as part of chronic inflammation.
Macrophages are longer lived than neutrophils and are capable of proliferating and phagocytosing larger particles. Mac ophage Neutroph. Lymphocyte Phagocytosis Monocyte Blood plasma Plasma eel Inflammation Chrome inflammation
B is not correct. 60/o chose this.
A monocyte has a kidney-shaped nucleus and differentiates into a macrophage in tissue; it is seen in chronic inflammation. Macrophage Monocyte Inflammation Cell nucleus Chronic inflammation
C is not correct. 4 0/o chose this.
A plasma cell has a clock-faced chromatin distribution. B lymphocytes differentiate into plasma cells, which then produce large amounts of antibody. They are a component of humoral immunity. Humoral immunity Blood plasma Chromatin Antibody lymphocyte B cell Plasma cell Humorism Immunity (medical)
E is not correct. JOfo c hose this.
T lymphocytes are the key component of cell-mediated immunity and are not the primary cell in acute inflammation . Cell-mediated immunity lymphocyte T cell Inflammation Immunity (medical)
Bottom Line:
The presence of WBC casts in a patient with a UTI indicates acute pyelonephritis, which is characterized histologically by polymorphonuclear cells. Pyelonephritis Histology
a s 8 Lock Suspend End Block
•
t

Item: 4 of 5 ~ 1 • M k -<:J 1>- Jil ~· !:';-~ QIO: 3 066 ..L a r Prev ious Next Lab fli!ltues Notes Calcula t o r
1
2
3
4
• 5
Pyelonephritis
Acute pyelonephritis
Chronic pyelonephritis
FA17 p 570.2
Neutrophils infiltrate renal interstitium · . Affect~ cortex with relati,·e sparing of glomeruli/vessels. Presents with fe,·ers, Aank pain (costovertebral angle tenderness), nausea/vomiting, chills.
Causes include ascending UTI (E coli is most common), hematogenous spread to kidney. Presents with vVBCs in urine+/- \VBC casts. CT \\Ould sho" striated parenchymal enhancement
Risk factors include indwelling urinar> catheter, urinary tract obstruction, vesicoureteral reAu;\, diabetes mellitus, pregnancy.
Complications include chronic pyelonephritis, renal papillar)' necrosis, perinephric abscess, u roseps1s.
Treatment: antibiotics.
The result of recurrent episodes of acute pyelonephritis. Typically requires predisposition to infection such as vesicourctcral rcAux or chronically obstructing kidney stones.
Coarse, asymmetric corticomedullary scarring, blunted calyx. Tubules can contain eosinophilic casts resembling thyroid tissue (thyroidization of kidney).
Xanthogranulomatous pyelonephritis-rare; gross!)' orange nodules that can mimic tumor nodules; characterized by widespread kidney damage due to granulomatous tissue conta ining foamy macrophages . ...
a s 8 Lock Suspend End Block
•
Item: 4 of 5 ~ . I • M k <:] t> al ~· ~ QIO: 3066 .l. ar Previous Next lab 'lifllues Notes Calculator
1
2
3
4
• 5
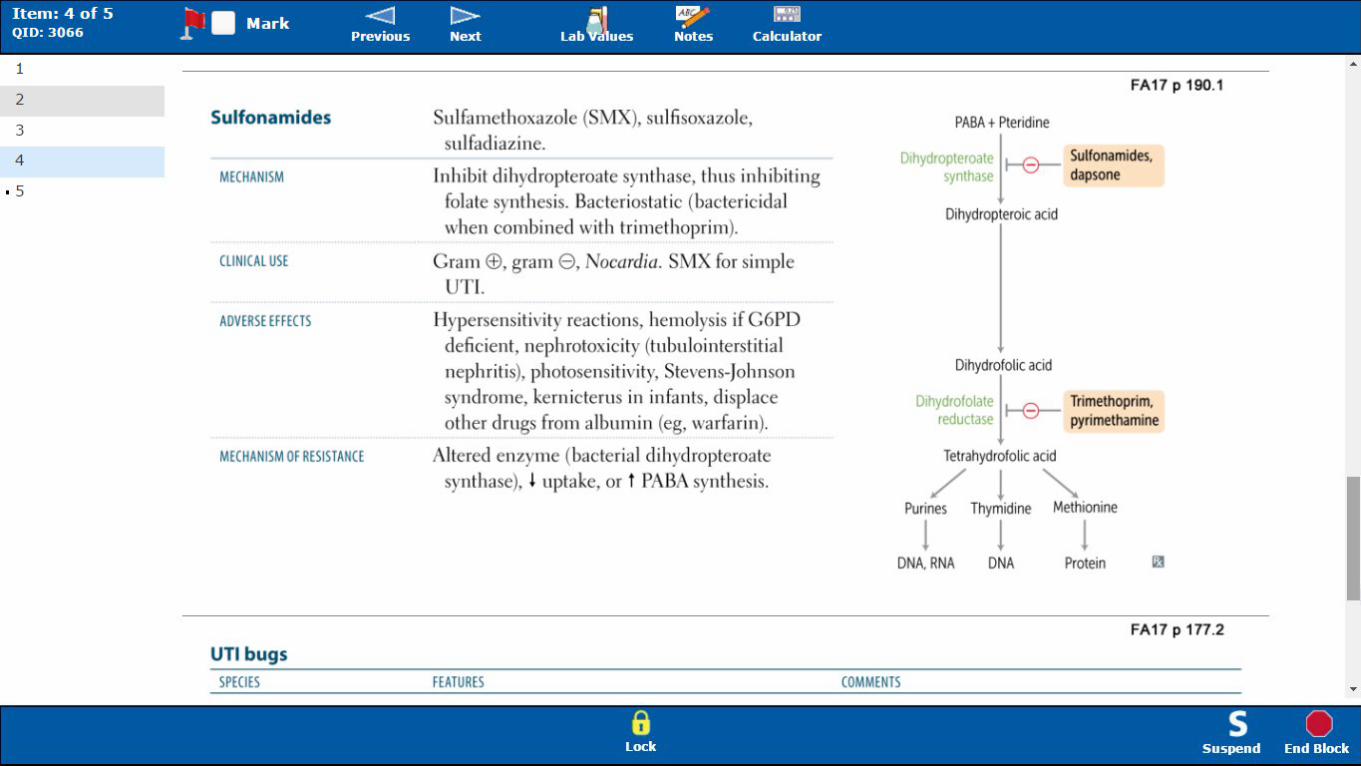
Sulfonamides
MECHANISM
CLINI CAL USE
ADVERSE EFFECTS
MECHANISM OF RESISTANCE
UTI bugs
SPECIES
Sulfamethoxazolc (SMX), sulfisoxazole, sulfadiazine.
T n h ibit dihydropteroate synthase, thus in hibiti ng fola te synthesis. Bacteriostatic (bactericida I when combined with tri methoprim).
Gram<±'>, gram 8 , 1 ocardia. SMX for simple UTI.
Hypersensitivity reactions, hemolysis if G6PD deficient, neph rotoxicit}' (tubu lointerstitial nephritis), photosensitivi ty, Stevens-Johnson syndrome, kern icterus in infants, displace other drugs from albumi n (eg, warfarin).
Altered enzyme (bacterial dihydroptcroatc synthase), £ uptake, or t PABA synthesis.
FEATURES
FA17 p 190.1
PABA+ Pteridine
D1hydropteroatt 11-0-- Sulfonamides, S'<nthase dapsone
Dihydropteroic acid
Dihydrofolic acid
D1hyd ofolate 11-0-- Trimethoprim, reductase pyrimethamine
Tetrahydrofolic acid
/!~ Purines Thymidine Methionine
! ! ! DNA. RNA DNA Protein
FA17 p 177.2
COMMENTS
6 s 0 lock Suspend End Block

Item: 4 of 5 ~ . I • M k <:] t> al ~· ~ QIO: 3066 .l. ar Previous Next lab 'lifllues Notes Calculator
1
2
3
4
• 5
UTI bugs
SPECIES
Escherichia coli
Staphylococcus saprophyticus
Klebsiella pneumoniae
Serratia marcescens
Enterococcus
Proteus mirabilis
Pseudomonas aeruginosa
synthase), l uptake, or t PABA synthesis.
FEATURES
Leading cause of UTI. Colonies show green metall ic sheen on EMB agar.
2nd leading cause of UTI in sexually active women.
3rd leading cause of UTJ. Large mucoid capsule and viscous colonies.
Some strains produce a red pigment; often nosocomial and drug resistant.
Often nosocomia l and drug resistant.
Nlotil ity causes "swarming" on agar; produces urease; associated with struvitc stones.
Blue-green pigment and fruity odor; usually nosocomial and drug resistant.
/! Purines Thymidine
~ Methionine
l l ! DNA. RNA DNA Protein
FA17 p 177.2
COMMENTS
Diagnostic markers: <±> Leukocyte esterase = evidence of WBC
activit)'· <±> itrite test = reduction of urinary nitrates
by bacterial species (eg, E coli). <±> Urease test = urease-producing bugs (eg,
S saprofJhyticus, Proteus, Klebsiella).
6 s 0 lock Suspend End Block

Item: 5 of 5 ~ 1 • M k -<:J 1>- Jil ~· !:';-~ QIO: 3 0 74 ..L a r Prev ious Next Labfli!llues Notes Calcula t o r
1
2
3
4
• 5
A 67-year-old man is admitted to the hospital because of gastrointestinal bleeding seconda•·y to dive•·ticulosis. He notes massive
gastrointestinal bleeding present for 1 day. In addition to his chief complaint, he feels lightheaded and dizzy . Physical examination reveals dry mucous membranes and flat jugular veins.
Which of the following groups of cells would be expected to increase their secretion based on this patient's condition?
A. Distal convoluted tubule
B. Glomerular capillaries
C. Juxtaglomerular cells
D. Macula densa
E. Proximal convoluted tubule
a s 8 Lock Suspend End Block
•

Item: 5 of 5 ~ . I • M k <:] t> al ~· ~ QIO: 3074 .l. ar Previous Next lab 'lifllues Notes Calculator
1
2
3
4
5
The correct answer is C. 790fo chose this.
In response to this patient's hypovolemia, the ren in -angiotensin -aldosterone mechanism will be activated to preserve more sodium ion and water in an attempt to return to a euvolem ic state. Add itionally, decreased sodium delivery to the macula densa or increased sympathetic tone can stimulate the ren in -angiotensin -aldosterone system . The cells responsible for secreting renin are the juxtaglomerular cells, which are specialized s mootiJ mus cle cells located in the wall of the afferent arteriole just before it enters the glomerulus. Ren in catalyzes the conversion of angiotensinogen (produced in the liver) to angiotensin L Ang iotensin -converting enzyme, which is produced in the renal and pulmonary endotheliu m, converts angiotensin I to angiotensin IL Ang iotensin II has a number of effects includ ing increasing sympathetic activity, stimulating sodium and chloride retention and potassium excretion, and triggering arteriolar vasoconstriction; all of which increase blood pressure. Add itionally it d irectly causes an increase in production of aldosterone and ADH. Aldosterone increases sodium and chloride retention and potassium excretion, and ADH causes increased water reabsorption in the collecting duct. Both increase blood pressure through volume expansion. Angiotensinogen Macula densa Arteriole Hypovolemia Aldosterone Afferent arterioles Renin Vasoconstriction Enzyme Juxtaglomerular cell Angiotensin
Endothelium Angiotensin II Glomerulus (kidney) Glomerulus Collecting duct system Smooth muscle tissue Renin-angiotensin system Sodium Blood pressure
Sympathetic nervous system Vasopressin Angiotensin I Angiotensin-converting enzyme Autonomic nervous system Catalysis Fluid balance liver Ion Potassium
Excretion Chloride
A is not correct. 3 0fo chose this.
The d istal convoluted tubule is also in close apposition to the g lomerulus. The continuation of the ascending thick limb of the loop of Hen le becomes the first part of the d istal convoluted tubule as it enters the cortex and lies in the angle of the efferent and afferent arterioles at the vascu lar pole of the g lomerulus. Distal convoluted tubule loop of Henle Afferent arterioles Glomerulus Glomerulus (kidney) Vascular pole Arteriole Nephron Anatomical terms of location
B is not correct. 2 0/o chose this.
The g lomerular capillaries are found within the g lomeruli and have no specialized cells for hormone secretion to regu late blood pressure. They act as part of a filtration barrier. Glomerulus (kidney) Glomerulus Capillary Blood pressure Hormone
0 is not correct. 120/o chose this.
The macu la den sa is an area of tightly packed cells in the d istal convoluted tubule that is in contact with the juxtaglomerular cells . These cells can most reliablv be d istinau ished bv their location lie. closest to the a lomerular vascu lar oole\. Macula densa cells function as the sodium ion sensors
6 s 0 lock Suspend End Block

Item: 5 of 5 ~ . I • M k <:] t> al ~· ~ QIO: 3074 .l. ar Previous Next lab 'lifllues Notes Calculator
1
2
3
4
5
A is not correct. 30fo c hose t his.
The d istal convoluted tubule is also in close apposition to the g lomerulus. The continuation of the ascending thick limb of the loop of Hen le becomes the first part of the d istal convoluted tubule as it enters the cortex and lies in the angle of the efferent and afferent arterioles at the vascular pole of the g lomerulus. Distal convoluted tubule loop of Henle Afferent arterioles Glomerulus Glomerulus (kidney) Vascular pole Arteriole Nephron Anatomical terms of location
B is not correct. 20/o c hose t his.
The g lomerular capillaries are found within the g lomeruli and have no specialized cells for hormone secretion to regu late blood pressure. They act as part of a filtration barrier. Glomerulus (kidney) Glomerulus Capillary Blood pressure Hormone
0 is not correct. 1 20/o c hose t his.
The macula den sa is an area of tightly packed cells in the d istal convoluted tubule that is in contact with the juxtaglomerular cells . These cells can most reliably be d istingu ished by their location (ie, closest to the g lomerular vascular pole}. Macula densa cells function as the sodium ion sensors in the j uxtaglomerular complex. These cells can sense a decreased sodium ion concentration in the d istal tubules (such as with hypovolemia) and relay that information to the j uxtaglomerular cells . The cells of the macula den sa also release adenosine. Distal convoluted tubule Macula densa Hypovolemia Juxtaglomerular cell Glomerulus Nephron Glomerulus (kidney) Vascular pole Sodium Adenosine Ion
E is not correct. 4 0fo c hose t his.
The proximal convoluted tubule arises from the renal corpuscle and forms the urine pole, opposite to the vascular pole in the g lomeruli. It contains no specialized cells involved in hormone secretion . It can be d istingu ished by its brush border and a high mitochondrial content, as proximal tubular cells are responsible for a significant amount of solute transport. Renal corpuscle Proximal convoluted tubule Nephron Brush border Glomerulus (kidney) Glomerulus Vascular pole Urine Hormone Mitochondrion Solution Kidney
Bottom Line :
To combat hypovolemia, the body must retain sodium and can do so by releasing ren in from the juxtaglomerular cells, thereby initiating the ren in -angiotensin -aldosterone mechanism . Juxtaglomerular cells are located in the wall of the afferent arteriole. Arteriole Hypovolemia Afferent arterioles Juxtaglomerular cell Renin Sodium
6 s 0 lock Suspend End Block

Item: 5 of 5 ~ 1 • M k -<:J 1>- Jil ~· !:';-~ QIO: 3 0 74 ..L a r Prev ious Next Labfli!llues Notes Calcula t o r
1
2
3
4
5
Juxtaglomerular apparatus
Consists of mesangial cells, JC cells (modified
smooth muscle of afferent arteriole) and the
macula dcnsa (NaCI sensor, part of OCT).
JC cells secrete renin in response to 1 renal
blood pressure and t sympathetic tone (p1).
FA17 p 558.2
JCA maintains CFR via renin-angiotensin-
:! ldosterone system.
1\ lacula densa cells sense 1 l'\'aCI dclivcq to
OCT - t renin release - efferent arteriole vasoconstriction - t CFR.
P-blockers can decrease BP by inhibiting
P1-receptors of the JCA - 1 renin release.
FA17 p 558.1
Renin-angiotensin-aldosterone system
I BP (JG cells)
I Na• delivery (macula densa cells)
t sympathetic tone IP,-receptors)
v
R . A~CE _____... Bradykinin
enm -------.. A A breakdown ( // 't T y
Anaiotensmooen -- Anaiotensin I -- Anaiotensin II .
Acts at angiotensin II - -+ Vasoconstriction - -+ t BP receptor. type 1 (AT
1) on
vascular smooth muscle
Constricts efferent artenole of glomerulus
Aldosterone (adrenal cortex)
t FF to preserve renal function (GFR) in low-volume states (ie. when RBF ~ )
t Na' channel insertion and _ _. t activity of Na·/K' pump; enhances K· and H·
Creates favorable Na· gradient for
a s 8 Lock Suspend End Block
•

Item: 5 of 5 ~ 1 • M k -<:J 1>- Jil ~· !:';-~ QIO: 3 0 74 ..L a r Prev ious Next Labfli!llues Notes Calcula t o r
1
2
3
4
5
I Na• delivery (macula densa cells)
I sympathetiC tone (~1-receptors)
AngaotenSJnogen
Renin
AT II
ANP, BNP
Renin A
::.--~) v
~ Bradyk' . ACE ---+ aran A breakdown
Acts at angiotensin 11 - -+ Vasoconstriction --- I BP receptor, type 1 (AT
1) on
vascular smooth muscle
Constricts efferent artenole of glomerulus
I FF to preserve renal function (GFRI in low-volume states (ie, when RBF ~ )
Aldosterone (adrenal cortex)
I Na' channel insertion and - -+ I activity of Na·fK· pump; enhances K· and H· excretion by way of principal cell K' channels and a-intercalated cell H· ATPases
Creates favorable Na· gradient for Na' and HzO reabsorption
,_...,.. AOH (posterior ------1> I aquaporin insertion in ----+ HzD patuatary) principal cells reabsorption
---+ Na', HCOJ·· and Hp reabsorption 1 PCT Na'/H' activity (can permit contraction alkalosis)
Stimulates hypothalamus ----+ Thirst
Secreted by JG cells in response to l renal arteria l pressure, t renal sympathetic discharge (~ 1 effect}, and l 1 a+ delivery to macu la dcnsa cells.
Helps maintain blood ,-olume and blood pressure. Affects baroreceptor function; lim its reAex bradycardia, ,,·hich would normally accompany ils pressor effects.
Released from atria { lp) and ' enlricles (B P) in response to t volume; may act as a "check" on renin-angiotensin-aldosterone system; re)a,es vascular smooth muscle via cG\1 P - t GFR,
a s 8 Lock Suspend End Block
•

2
3
4
5
Angiotensinogen
Renin
AT II
ANP, BNP
ADH
Aldosterone
Renin ~ T
-----+ I Na' channel insertion and - + I activity of Na' /K' pump; enhances K· and H· excretion by way of principal cell K• channels and a-intercalated cell H· ATPases
Creates favorable Na· gradient for Na' andHp reabsorption
ADH (posteriOr -------+ I aquaporin insertion in ----+ Hp pitUitary) principal cells reabsorption
--+ Na'. HC01•• and Hp reabsorption 1 PCT Na'/H' activity (can permit contraction alkalosis)
Stimulates hypothalamus ----+ Thirst
Secreted by jG cells in response to l rena l arterial pressure, t renal sympathetic discharge (p1
effect), and l 1a+ delivery to macula clensa cells.
Helps ma intain blood volume and blood pressure. Affects baroreceptor function; lim its renex bradycardia, which would normally accompany its pressor effects.
Released from atria ( 1P) and ventricles (B IP) in response to t volume; may act as a "check" on renin-angiotensin-aldosterone system; relaxes vascular smooth muscle via cGM P - t GFR, l renin. Dilates afferent arteriole, constricts efferent arteriole, promotes natriuresis.
Primarily regulates osmolarity; a !so responds to low blood ,·olume states.
Primarily regu lates ECF volume and Na+ content; responds to low blood ,-olume states. Responds to hyperkalemia by t K+ excretion.
a s 8 Lock Suspend End Block