D D Sleep Disordered Breathing and Dentistry Sleep Disordered Breathing and Dentistry National...
88
D Sleep Disordered Sleep Disordered Breathing Breathing and Dentistry and Dentistry National Primary Oral National Primary Oral Health Care Conference Health Care Conference August 9, 2005 August 9, 2005 Atlanta, Georgia Atlanta, Georgia
-
Upload
claud-ernest-underwood -
Category
Documents
-
view
227 -
download
3
Transcript of D D Sleep Disordered Breathing and Dentistry Sleep Disordered Breathing and Dentistry National...
DD Sleep Disordered BreathingSleep Disordered Breathing
and Dentistryand Dentistry Sleep Disordered BreathingSleep Disordered Breathing
and Dentistryand Dentistry
National Primary Oral Health National Primary Oral Health Care ConferenceCare ConferenceAugust 9, 2005August 9, 2005
Atlanta, GeorgiaAtlanta, Georgia
National Primary Oral Health National Primary Oral Health Care ConferenceCare ConferenceAugust 9, 2005August 9, 2005
Atlanta, GeorgiaAtlanta, Georgia
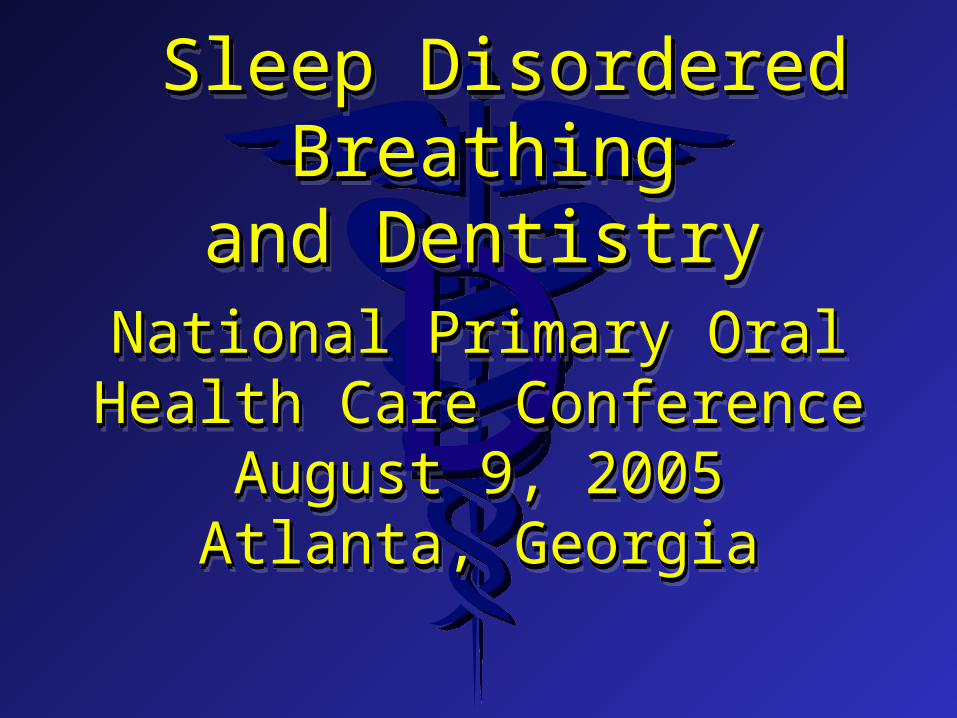
DDOral cavityOral cavityTongue3Tongue3UvulaUvulaNasal cavityNasal cavityPharynxPharynxGenioglossusGenioglossusTensor VeliTensor Veli*Soft tissue*Soft tissuetubetube
Anatomy of Upper AirwayAnatomy of Upper Airway
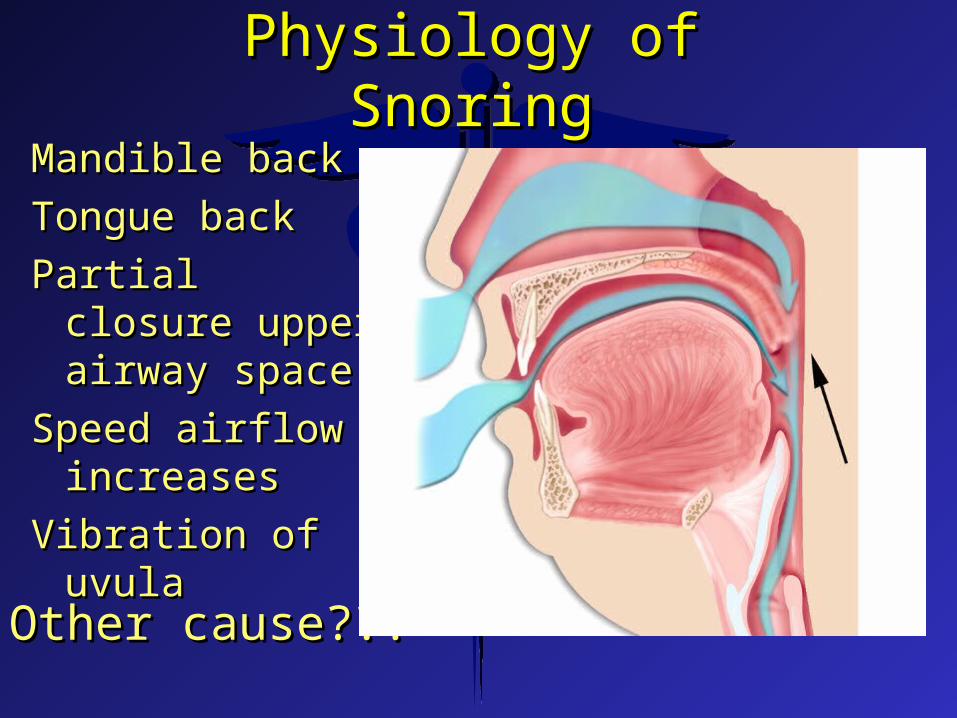
DDPhysiology of SnoringPhysiology of Snoring
Mandible backMandible back
Tongue backTongue back
Partial closure Partial closure upper airway upper airway spacespace
Speed airflow Speed airflow increasesincreases
Vibration of uvulaVibration of uvula
* Other cause???* Other cause???
DDSnoring DemographicsSnoring Demographics
z 40 - 60% over 50 years snore40 - 60% over 50 years snorez Males twice as likely as femalesMales twice as likely as femalesz Overweight / neck size Overweight / neck size
z Males 17” or greaterMales 17” or greaterz Females 16” or greaterFemales 16” or greater

DDSnoring SignificanceSnoring SignificanceSnoring SignificanceSnoring Significance
z Snorers awaken their partners and Snorers awaken their partners and occasionally themselves by the occasionally themselves by the loudness of their snoring resulting in loudness of their snoring resulting in loss of sleep (to be discussed later) loss of sleep (to be discussed later)
z 10 - 20 % have a Severe Upper 10 - 20 % have a Severe Upper Airway Sleep Disorder!Airway Sleep Disorder!

DDSevere Upper Airway Severe Upper Airway
Sleep DisordersSleep Disorders
Upper Airway Resistant Syndrome Upper Airway Resistant Syndrome (Tx – Same as OSA)(Tx – Same as OSA)
Obstructive Sleep Apnea (OSA)Obstructive Sleep Apnea (OSA)

DDObstructive Sleep ApneaObstructive Sleep Apnea(OSA)(OSA)
DDObstructive Sleep ApneaObstructive Sleep ApneaObstructive Sleep ApneaObstructive Sleep Apnea
z Complete or almost complete reduction in Complete or almost complete reduction in airflow through the upper airway lasting airflow through the upper airway lasting for more than 10 seconds, resulting in for more than 10 seconds, resulting in severe oxygen depletion leading to medical severe oxygen depletion leading to medical problemsproblems
z Causes - Tongue, obesity, inflammation of Causes - Tongue, obesity, inflammation of any soft tissues in the upper airway any soft tissues in the upper airway (tonsils, adenoids), polyps, tumors, etc(tonsils, adenoids), polyps, tumors, etc
z Demographics - 4% of adult middle-aged Demographics - 4% of adult middle-aged males and 2% of femalesmales and 2% of females
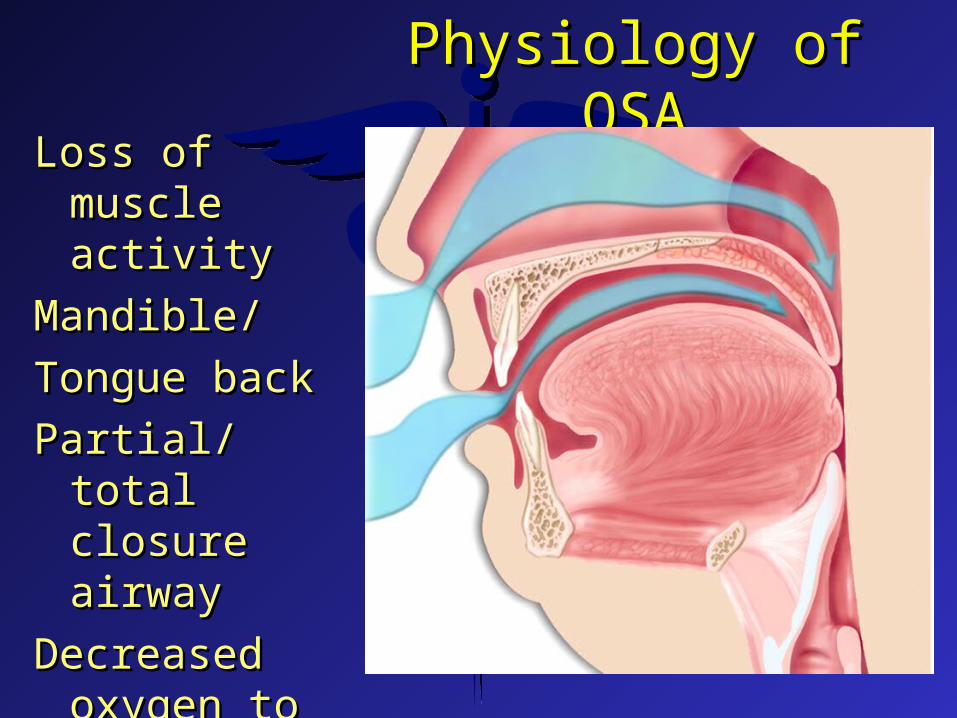
DDPhysiology of OSAPhysiology of OSA
Loss of muscle Loss of muscle activityactivity
Mandible/Mandible/
Tongue backTongue back
Partial/total Partial/total closure airwayclosure airway
Decreased oxygen Decreased oxygen to lungsto lungs
Blood oxygen Blood oxygen desaturationdesaturation

DDPatients With OSAPatients With OSA
z Snore loudlySnore loudlyz Stop breathing - snort to start againStop breathing - snort to start againz ChokeChokez Suffer from acid refluxSuffer from acid refluxz Toss and turnToss and turnz Wake up frequentlyWake up frequentlyz Daytime sleepinesDaytime sleepines
DDSignificance of OSASignificance of OSA
z Loss of air to lungs may happen many Loss of air to lungs may happen many times per hour times per hour
z Blood oxygen drops below the 90% level Blood oxygen drops below the 90% level causing the patient to arouse to breathcausing the patient to arouse to breath
z Arousal causes loss of sleep, daytime Arousal causes loss of sleep, daytime sleepiness, decreased production, sleepiness, decreased production, increased accidents, etc.increased accidents, etc.
z May cause medical problems ranging May cause medical problems ranging from mild to from mild to “life threatening”“life threatening”
DDMedical ResponsibilityMedical ResponsibilityMedical ResponsibilityMedical Responsibility
z Diagnosis and determine presence and Diagnosis and determine presence and severity of an UASD - “Sleep Study”severity of an UASD - “Sleep Study”
z Determine treatmentDetermine treatmentz Treat patient or refer for oral deviceTreat patient or refer for oral device
Dental ResponsibilityDental ResponsibilityDental ResponsibilityDental Responsibilityz Recognize and referRecognize and referz Provide support when requestedProvide support when requested

DDPhysician Treatment OptionsPhysician Treatment Options
z Behavior modificationBehavior modificationz SurgerySurgeryz MedicationsMedicationsz CPAPCPAPz Oral devicesOral devices
DDBehavior ModificationBehavior Modification
z Sleep on side rather than backSleep on side rather than backz Avoid alcohol late in day and evening (CNS Depressant)Avoid alcohol late in day and evening (CNS Depressant)z Minimize use of sedativesMinimize use of sedativesz Weight lossWeight loss
Long term success poorly documentedLong term success poorly documented

DDSurgical ProceduresSurgical Procedures
z UPPP - UvuloPalatoPharyngoPlastyUPPP - UvuloPalatoPharyngoPlastyz LAUP - Laser-Assisted Uvula-PalatoplastyLAUP - Laser-Assisted Uvula-Palatoplastyz High Frequency Radio Waves to uvulaHigh Frequency Radio Waves to uvulaz Tonsillectomy, adenoidectomyTonsillectomy, adenoidectomyz Tracheostomy - life saving procedureTracheostomy - life saving procedurez Craniofacial operations - Maxillomandibular Craniofacial operations - Maxillomandibular
Advancement, Hyoid liftAdvancement, Hyoid lift

DD
DDz The most effective acceptable surgical The most effective acceptable surgical
treatment of OSA (excluding tracheostomy)treatment of OSA (excluding tracheostomy)z Success rates of 96%, 97%, 98% and 100% Success rates of 96%, 97%, 98% and 100%
reported in the literaturereported in the literaturez Caution – Reports of devitalization of teeth Caution – Reports of devitalization of teeth
cause by surgical procedurescause by surgical procedures
Maxillomandibular Advancement Maxillomandibular Advancement (MMA)(MMA)
Maxillomandibular Advancement Maxillomandibular Advancement (MMA)(MMA)
Prinsell JR. Maxillomandibular advancement (MMA) in a Site-Prinsell JR. Maxillomandibular advancement (MMA) in a Site-Specific treatment approach for obstructive sleep apnea: A Specific treatment approach for obstructive sleep apnea: A surgical approach. Sleep Breath. 2000;4:147-54.surgical approach. Sleep Breath. 2000;4:147-54.
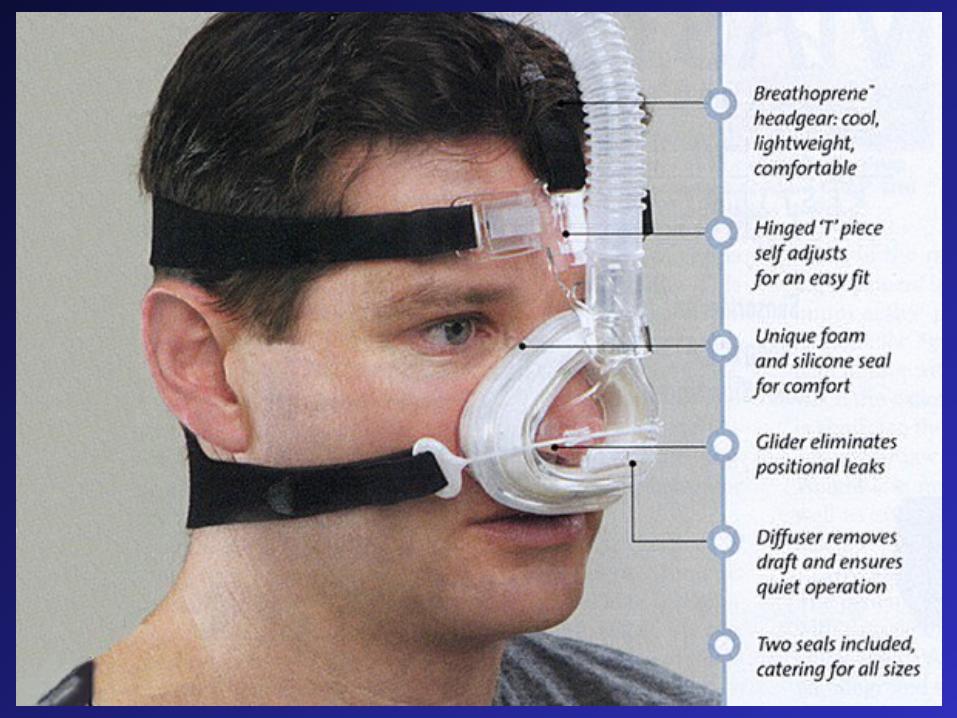
DDContinuous Positive Air Continuous Positive Air
Pressure - CPAPPressure - CPAPz Most effective of all treatment modalitiesMost effective of all treatment modalitiesz Patient must wear mask while sleepingPatient must wear mask while sleepingz Very noisy equipment, uncomfortableVery noisy equipment, uncomfortablez Equipment not easily portableEquipment not easily portablez Compliance poorCompliance poor
DD
DDMedicationsMedications
z Only for those patient who are not Only for those patient who are not good candidates for CPAP, Oral good candidates for CPAP, Oral Devices or Surgical Procedures Devices or Surgical Procedures
z Should not be considered by Should not be considered by dentistrydentistry
DDOral DeviceOral DeviceHow and WhatHow and What
Oral DeviceOral DeviceHow and WhatHow and What

DD

DD

DDz Snoring/OSA caused by loss of airway spaceSnoring/OSA caused by loss of airway spacez Most oral devices advance the mandibleMost oral devices advance the mandiblez This pulls the genioglossus forward This pulls the genioglossus forward z This pulls the tongue forwardThis pulls the tongue forwardz Upper airway space is regainedUpper airway space is regainedz Snoring/OSA diminished or eliminatedSnoring/OSA diminished or eliminatedz Others simply keep the tongue protrudedOthers simply keep the tongue protruded
How Does An Oral Device Work?How Does An Oral Device Work?How Does An Oral Device Work?How Does An Oral Device Work?
DDAll Dental Patients Should be All Dental Patients Should be Evaluated for a Potential Sleep Evaluated for a Potential Sleep
DisorderDisorder
All Dental Patients Should be All Dental Patients Should be Evaluated for a Potential Sleep Evaluated for a Potential Sleep
DisorderDisorder

DDDiagnosing Snoring / OSADiagnosing Snoring / OSA
z Medical historyMedical historyz Sleep historySleep historyz Extended dental examination including TMJ Extended dental examination including TMJ
evaluationevaluationz Epworth Sleepiness ScaleEpworth Sleepiness Scalez Preliminary diagnosisPreliminary diagnosisz Referral for medical evaluation (sleep study)Referral for medical evaluation (sleep study)
DDz Snore loudlySnore loudlyz Stop breathing - snort to start againStop breathing - snort to start againz ChokeChokez Suffer from acid refluxSuffer from acid refluxz Toss and turn during sleepToss and turn during sleepz Wake up frequentlyWake up frequentlyz Have daytime sleepinessHave daytime sleepiness
Quality of Sleep QuestionsQuality of Sleep Questions

DD1.1. Weight Compared to Year Ago?Weight Compared to Year Ago?
2. Ever Treated for Nasal Congestion 2. Ever Treated for Nasal Congestion
3. 3. Neck CircumferenceNeck Circumference
4. Alcohol/Sedatives- How Often?4. Alcohol/Sedatives- How Often?
5. 5. Tired/Sleepy During the Day?Tired/Sleepy During the Day?
6. Sleep Position - Back, sides, stomach6. Sleep Position - Back, sides, stomach
Questions I’ll AskQuestions I’ll Ask
DD6.6. Frequency and loudness of snoringFrequency and loudness of snoring7.7. Previous Sleep Studies or Past Previous Sleep Studies or Past
Treatment for Snore Problems?Treatment for Snore Problems?8.8. Do You Ever Awaken Gasping for Do You Ever Awaken Gasping for
Air?Air?9.9. Ever Been Told That You Stop Ever Been Told That You Stop
Breathing While You Sleep?Breathing While You Sleep?
Questions I’ll AskQuestions I’ll Ask

DDHow much air space is present?How much air space is present?
z Open fairly wide and slightly protrude your tongueOpen fairly wide and slightly protrude your tonguez Grade - I, II, or IIIGrade - I, II, or III
(Jamieson AO, Becker PM. Snoring: its evaluation (Jamieson AO, Becker PM. Snoring: its evaluation and treatment. Hospital Medicine. March 1996)and treatment. Hospital Medicine. March 1996)

DDGrade IGrade I
The tonsillar pillars, soft palate, and uvula The tonsillar pillars, soft palate, and uvula can be seen, with at least 5 mm between the can be seen, with at least 5 mm between the tip of the uvula and the base of the tonguetip of the uvula and the base of the tongue
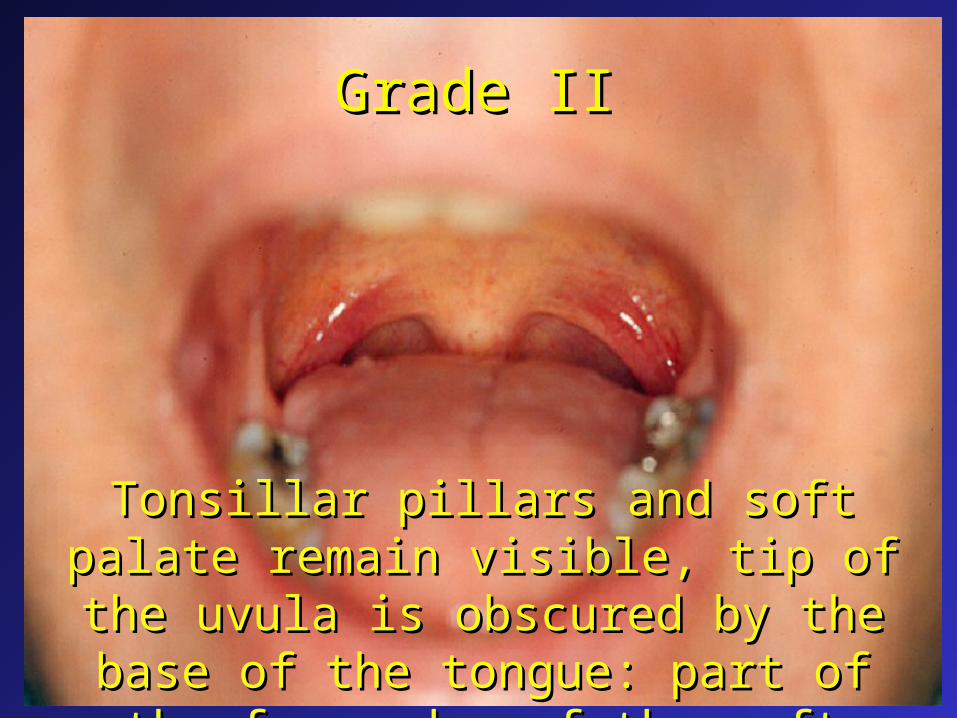
DDGrade IIGrade II
Tonsillar pillars and soft palate remain Tonsillar pillars and soft palate remain visible, tip of the uvula is obscured by the visible, tip of the uvula is obscured by the base of the tongue: part of the free edge of base of the tongue: part of the free edge of
the soft palate is still visiblethe soft palate is still visible
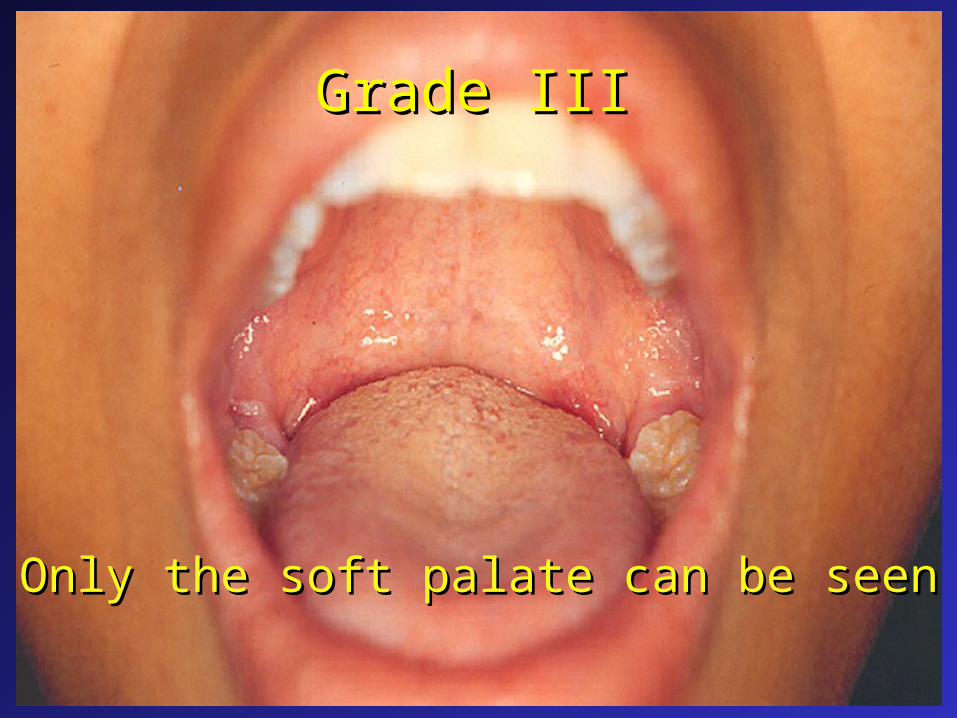
DDGrade IIIGrade III
Only the soft palate can be seenOnly the soft palate can be seen
DDEpworth Sleepiness ScaleEpworth Sleepiness Scale
z Likeliness to doze off or fall asleep in certain Likeliness to doze off or fall asleep in certain situations versus to just feeling tired situations versus to just feeling tired
z Use the following scale to choose the most Use the following scale to choose the most appropriate number for each situation: appropriate number for each situation:
z Likeliness to doze off or fall asleep in certain Likeliness to doze off or fall asleep in certain situations versus to just feeling tired situations versus to just feeling tired
z Use the following scale to choose the most Use the following scale to choose the most appropriate number for each situation: appropriate number for each situation:
0 = would never doze 0 = would never doze 1 = slight chance of dozing 1 = slight chance of dozing 2 = moderate chance of dozing 2 = moderate chance of dozing 3 = high chance of dozing3 = high chance of dozing
DDPreliminary DiagnosisPreliminary Diagnosis
z Snoring only Snoring only z Snoring and potential upper airway Snoring and potential upper airway
sleep disorder sleep disorder z Definite disorder – OSA or UARSDefinite disorder – OSA or UARS
DDOral Devices for TreatingOral Devices for Treating
Snoring and Snoring and Obstructive Sleep ApneaObstructive Sleep Apnea

DDOral Devices IndicationsOral Devices IndicationsOral Devices IndicationsOral Devices Indications
Recommended for snoring and mild Recommended for snoring and mild to moderate sleep apnea if CPAP to moderate sleep apnea if CPAP unsuccessful.unsuccessful.
Practice parameters for the treatment of Practice parameters for the treatment of snoring and obstructive sleep apnea with snoring and obstructive sleep apnea with oral devices. An American Sleep oral devices. An American Sleep Disorders Association Report. Sleep. Disorders Association Report. Sleep. 1995;18(6):511-131995;18(6):511-13
DDProblems with MADs after long term Problems with MADs after long term
use (3 years or more)use (3 years or more)Problems with MADs after long term Problems with MADs after long term
use (3 years or more)use (3 years or more)z Minor jaw/facial, tooth, muscle pain – 40% Minor jaw/facial, tooth, muscle pain – 40% z Xerstomia – 30%Xerstomia – 30%z Very Satisfied – 82%Very Satisfied – 82%z Satisfied – 15%Satisfied – 15%z Painless but irreversible change in Painless but irreversible change in
occlusion - 26%occlusion - 26%
GT, Sohn JW, Hong CN. Treating obstructive sleep GT, Sohn JW, Hong CN. Treating obstructive sleep apnea and snoring: assessment of an anterior mandibular apnea and snoring: assessment of an anterior mandibular positioning device. J Am Dent Assoc. 2000;131:765-71.positioning device. J Am Dent Assoc. 2000;131:765-71.

DDCLINICAL IMPLICATIONSCLINICAL IMPLICATIONSCLINICAL IMPLICATIONSCLINICAL IMPLICATIONS
z Patients with mild-to-moderate OSA Patients with mild-to-moderate OSA who receive a two-piece, adjustable who receive a two-piece, adjustable MAD should be informed that 50 MAD should be informed that 50 percent of patients quit using the percent of patients quit using the device in a three-year period and device in a three-year period and some will experience shifts in their some will experience shifts in their occlusion.occlusion.

DDDevice Treatment OptionsDevice Treatment Options
Tongue Retaining Device (TRD)Tongue Retaining Device (TRD)
Mandibular Advancement Device (MAD)Mandibular Advancement Device (MAD)
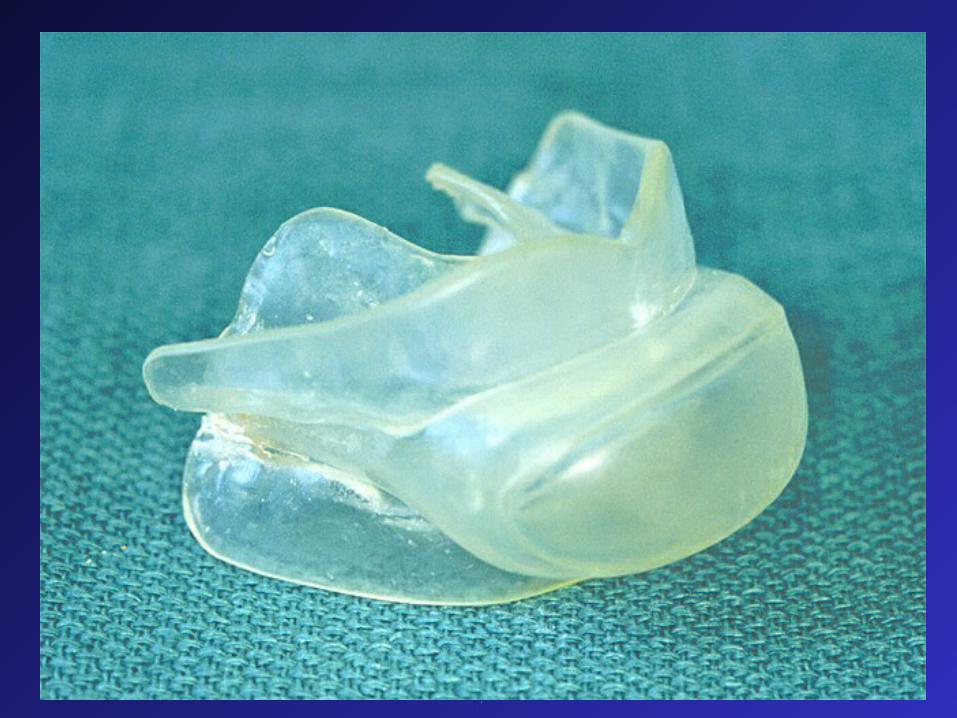
DDTongue Retaining DeviceTongue Retaining Device
(TRD)(TRD)Tongue Retaining DeviceTongue Retaining Device
(TRD)(TRD)
Laboratory fee - $150Laboratory fee - $150
DDIndications for TRDsIndications for TRDsIndications for TRDsIndications for TRDs
z Edentulous patientsEdentulous patientsz Patients with potential Patients with potential
temporomandibular joint problemstemporomandibular joint problems
Problems with TRDsProblems with TRDsProblems with TRDsProblems with TRDsz Sore tongueSore tonguez Tongue elongationTongue elongation
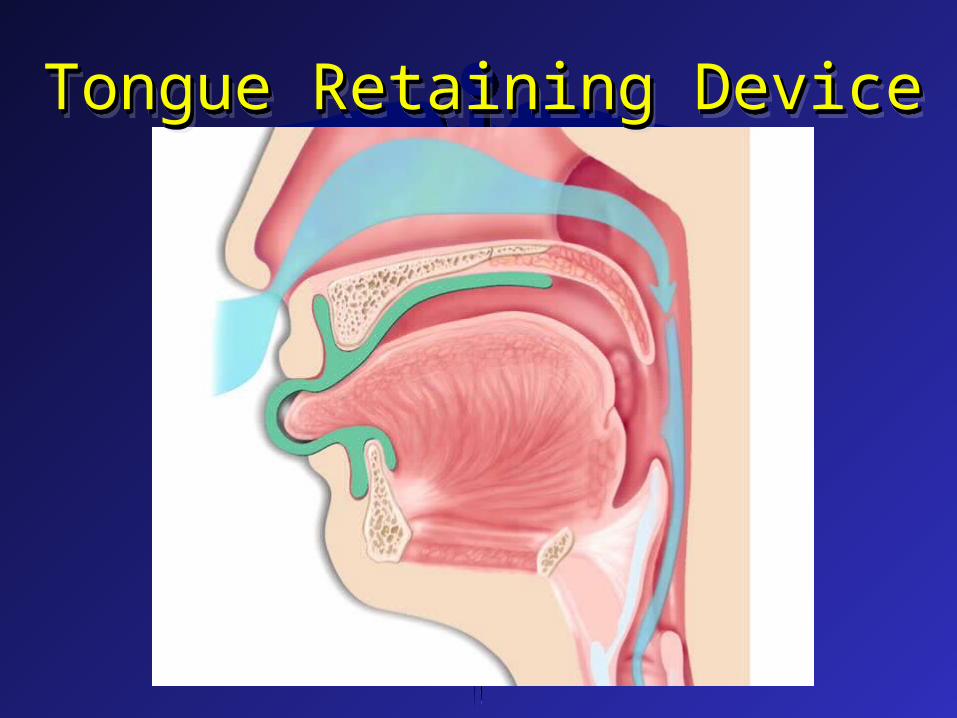
DDTongue Retaining DeviceTongue Retaining DeviceTongue Retaining DeviceTongue Retaining Device

DDKelgaugeKelgauge

DD

DD
DD

DD
DDTRD FindingsTRD FindingsTRD FindingsTRD Findings
z Altered the timing of the inspiratory Altered the timing of the inspiratory genioglossus (GG) activity and the onset of genioglossus (GG) activity and the onset of inspiration effortinspiration effort
z Oxygen desaturation index dropped to Oxygen desaturation index dropped to fewer than 10 events/ h in 75% of patients fewer than 10 events/ h in 75% of patients
z Significantly improved the blood oxygen Significantly improved the blood oxygen saturation level in infants saturation level in infants
z Helped patients with mild to moderate Helped patients with mild to moderate OSA; however, patients with more severe OSA; however, patients with more severe OSA may also be treated effectivelyOSA may also be treated effectively

DDMandibular Advancement Mandibular Advancement
DevicesDevicesMandibular Advancement Mandibular Advancement
DevicesDevicesz Fixed - $100 - 500Fixed - $100 - 500z Adjustable - $300 - 800Adjustable - $300 - 800
DDFabrication of an “Adjustable” Fabrication of an “Adjustable” Laboratory Fabricated Device Laboratory Fabricated Device

DDPractice CR toPractice CR tomaximum protruded maximum protruded
positionposition

DD

DD

DD

DDPatient closingPatient closing
in the in the pre-selected pre-selected
protrudedprotrudedpositionposition
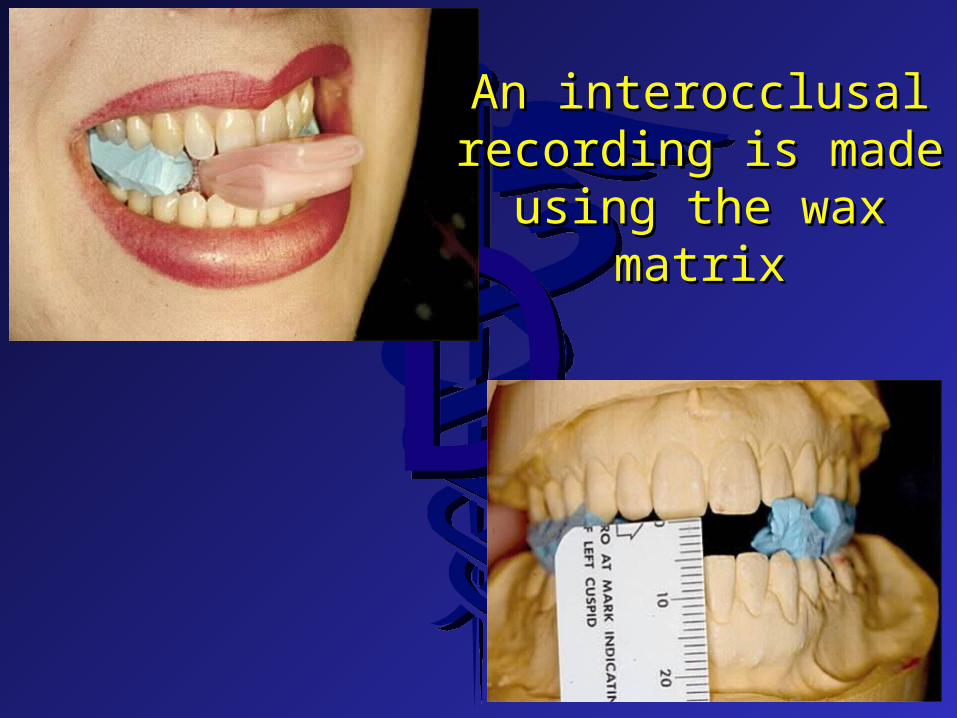
DDAn interocclusalAn interocclusal
recording is maderecording is madeusing the waxusing the wax
matrixmatrix

DD

DD

DD

DD

DDAdjustment of the Adjustment of the
device mustdevice mustbe made be made
depending on device depending on device fabricatedfabricated
DDPatient instructions for adjustmentPatient instructions for adjustment(depends on device but typical):(depends on device but typical):
Patient instructions for adjustmentPatient instructions for adjustment(depends on device but typical):(depends on device but typical):
z No adjust for first 3 nights to allow patient No adjust for first 3 nights to allow patient to become accustom to deviceto become accustom to device
z Protrude device 0.25 mm per night for 3 – Protrude device 0.25 mm per night for 3 – 4 nights, stop, check for improvement4 nights, stop, check for improvement
z Protrude device 0.25 mm per night for 3 – Protrude device 0.25 mm per night for 3 – 4 nights, stop, check for improvement4 nights, stop, check for improvement
z Continue until symptoms are relieved or Continue until symptoms are relieved or reduced or TMJ symptoms developreduced or TMJ symptoms develop

DDEvaluationEvaluationEvaluationEvaluation
z Following relief of symptoms allow patient Following relief of symptoms allow patient to wear device for 2 – 4 weeksto wear device for 2 – 4 weeks
z Have patient wear a Pulse Oximetry device Have patient wear a Pulse Oximetry device and determine success of treatmentand determine success of treatment
z Continue adjustments and followup Pulse Continue adjustments and followup Pulse Oximetry or Oximetry or
z Refer to Physician for reevaluation Refer to Physician for reevaluation (2(2ndnd polysomnography) polysomnography)
DD
DDPatient Should ExpectPatient Should Expect
z Lips will be very dry - lip balmLips will be very dry - lip balmz Difficulty going to sleep for a few nightsDifficulty going to sleep for a few nightsz Lots of saliva - on pillowLots of saliva - on pillowz Teeth may become sensitive - seek care Teeth may become sensitive - seek care
immediately - usually slight adjustmentimmediately - usually slight adjustment

DDz For approximately 20 minutes upon For approximately 20 minutes upon
awakening teeth will not close together - awakening teeth will not close together - don’t force closure don’t force closure - no treatment- no treatment
z TMJ discomfort - May be sore for a few TMJ discomfort - May be sore for a few minutes during early adjustment, must be minutes during early adjustment, must be relieved by moving mandible posteriorlyrelieved by moving mandible posteriorly
Patient Should ExpectPatient Should Expect

DDz Device for treatment of snoring and/or OSADevice for treatment of snoring and/or OSAz Cease wearing and return to dentist immediately Cease wearing and return to dentist immediately
if any problems developif any problems developz Device may only be partially successfulDevice may only be partially successfulz May cause existing dental restorations to May cause existing dental restorations to
loosened or failloosened or failz Device may increase severity of an existing OSADevice may increase severity of an existing OSA
Consent Form Before TreatingConsent Form Before Treating

DDIs Insurance Coverage Is Insurance Coverage
Available? Yes and NoAvailable? Yes and Noz Yes - medical insurance coverage is Yes - medical insurance coverage is
possible for treatment of a possible for treatment of a diagnosed sleep diagnosed sleep apnea condition.apnea condition. Very hard to collect Very hard to collect
z No - medical insurance coverage for a No - medical insurance coverage for a snoring onlysnoring only problem problem
z No - dental insurance coverage for eitherNo - dental insurance coverage for either
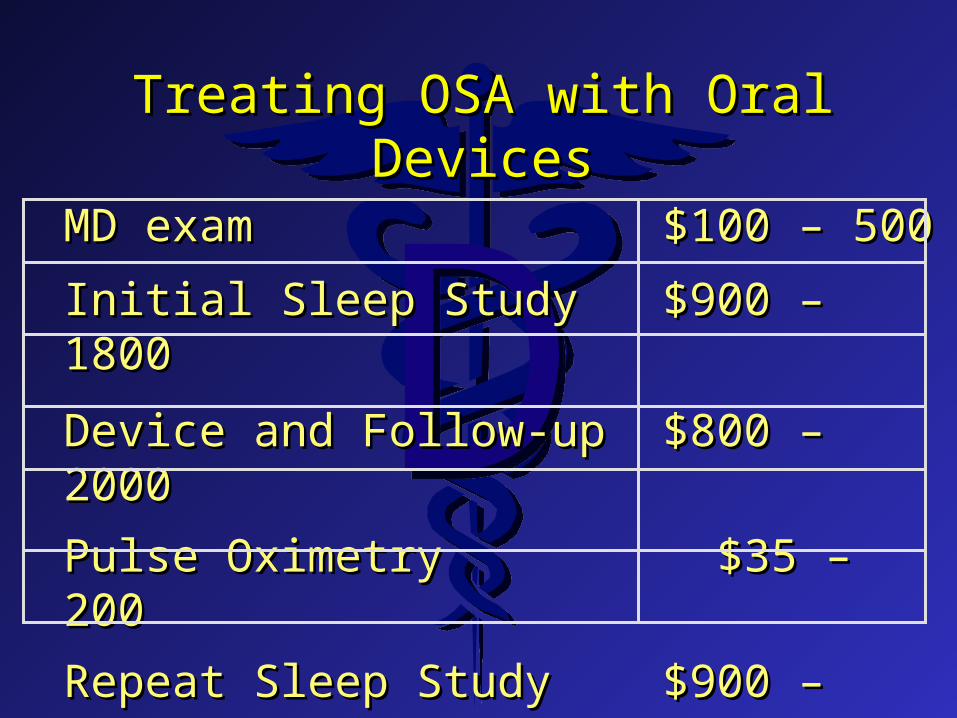
DDTreating OSA with Oral DevicesTreating OSA with Oral Devices
MD examMD exam $100 – 500$100 – 500
Initial Sleep StudyInitial Sleep Study $900 – 1800$900 – 1800
Device and Follow-upDevice and Follow-up $800 – 2000$800 – 2000
Pulse OximetryPulse Oximetry $35 – 200 $35 – 200
Repeat Sleep StudyRepeat Sleep Study $900 – 1800$900 – 1800
TotalTotal $2735 $2735 –– 6300 6300
DDSleep Disorders in Infants Sleep Disorders in Infants and Childrenand Children
Sleep Disorders in Infants Sleep Disorders in Infants and Childrenand Children
DDPrevalence in Infants and ChildrenPrevalence in Infants and ChildrenPrevalence in Infants and ChildrenPrevalence in Infants and Children
z 3 – 12% snore3 – 12% snorez 1 – 10% have OSA1 – 10% have OSA
When do problems occurWhen do problems occurWhen do problems occurWhen do problems occurz Snoring – 22.7 monthsSnoring – 22.7 monthsz Apnea – 34.7 monthsApnea – 34.7 months
DDSymptoms - 352 OSA children exhibited : Symptoms - 352 OSA children exhibited : Symptoms - 352 OSA children exhibited : Symptoms - 352 OSA children exhibited : z Chronic mouth breathing (84%)Chronic mouth breathing (84%)z Otitis media (middle ear infection) (64%)Otitis media (middle ear infection) (64%)z Sinusitis (56%)Sinusitis (56%)z Sore throat (51%)Sore throat (51%)z Choking (47%)Choking (47%)z Daytime drowsiness (42%) Daytime drowsiness (42%) z Less observed symptoms included poor school Less observed symptoms included poor school
performance, enuresis (bed wetting), poor performance, enuresis (bed wetting), poor appetite and/or weight gain, dysphagia, and appetite and/or weight gain, dysphagia, and vomiting. vomiting.

DDWhat Do Studies Show?What Do Studies Show?What Do Studies Show?What Do Studies Show?
z 7% of the children were habitual snorers and 7% of the children were habitual snorers and exhibited a higher prevalence of difficulty in exhibited a higher prevalence of difficulty in breathing, observed apneas, restless sleep, and breathing, observed apneas, restless sleep, and nocturnal enuresis than non-snorers nocturnal enuresis than non-snorers
z Subjects were more likely to fall asleep while Subjects were more likely to fall asleep while watching television and in public places and watching television and in public places and were hyperactive were hyperactive
DDz The presence of asthma and hay fever The presence of asthma and hay fever
increased the likelihood of habitual snoring increased the likelihood of habitual snoring with exposure to cigarette smoking at home with exposure to cigarette smoking at home
z Primary snoring was corrected with Primary snoring was corrected with adenotonsillectomy resulting in weight gain adenotonsillectomy resulting in weight gain and a restoration of normal growth and a restoration of normal growth
z 26% of children with mild symptoms of 26% of children with mild symptoms of Attention-Deficit/Hyperactivity Disorder Attention-Deficit/Hyperactivity Disorder (ADHD) also demonstrate OSA as observed (ADHD) also demonstrate OSA as observed during polysomnography testingduring polysomnography testing
DDz Almost 25% of OSA children had clinically Almost 25% of OSA children had clinically
significant behavioral sleep problems such as significant behavioral sleep problems such as sleep walking and nightmares as well as a greater sleep walking and nightmares as well as a greater incidence of daytime externalizing behavior incidence of daytime externalizing behavior problems problems
z Children 11 to14 years of age who were Children 11 to14 years of age who were diagnosed as being sleep deficient exhibited diagnosed as being sleep deficient exhibited lowered self-esteem, significantly lower grades lowered self-esteem, significantly lower grades and higher levels of depressive symptoms than and higher levels of depressive symptoms than those students registering more normal sleep those students registering more normal sleep duration duration

DDz The early onset of alcohol, marijuana or illicit The early onset of alcohol, marijuana or illicit
drug use by the adolescent as well as an early drug use by the adolescent as well as an early onset of cigarette use by the age of 12 to 14 onset of cigarette use by the age of 12 to 14 could be significantly predicted by the could be significantly predicted by the mother’s ratings of their children’s sleep mother’s ratings of their children’s sleep problems at ages 3 to 5 years problems at ages 3 to 5 years
z Children with sleep disorders and attention Children with sleep disorders and attention deficit hyperactivity disorder had a verbal IQ deficit hyperactivity disorder had a verbal IQ (intelligence quotient) up to 20 points lower (intelligence quotient) up to 20 points lower than control subjectsthan control subjects
DDz Children with lower academic Children with lower academic
performance in middle school were more performance in middle school were more likely to have snored in early childhood likely to have snored in early childhood and have required tonsillectomy and and have required tonsillectomy and adenoidectomyadenoidectomy
z Persistent sleep disturbance is likely to Persistent sleep disturbance is likely to adversely affect cognition, mood, behavior adversely affect cognition, mood, behavior and family functionand family function
DDz Habitual snoring was significantly Habitual snoring was significantly
associated with lowered academic associated with lowered academic performances in mathematics, science and performances in mathematics, science and spelling in third grade childrenspelling in third grade children
z Infantile OSAS does occur in infants due Infantile OSAS does occur in infants due to hypertrophic adenoids and tonsils and to hypertrophic adenoids and tonsils and that among other things these infants that among other things these infants failed to gain weight failed to gain weight
DDRecognitionRecognitionRecognitionRecognition
z Of all observations made by parents, that Of all observations made by parents, that of “snoring every night”, is the most of “snoring every night”, is the most significant factor in predicting OSA significant factor in predicting OSA
z Children with sleep breathing disorders Children with sleep breathing disorders had the dolico facial pattern had the dolico facial pattern (disproportionately long face)(disproportionately long face)
z Migraine headaches may be indicative of Migraine headaches may be indicative of sleep disturbances sleep disturbances
DDRisk Factors for sleep apnea Risk Factors for sleep apnea
in children include:in children include:Risk Factors for sleep apnea Risk Factors for sleep apnea
in children include:in children include:z ObesityObesityz African-American raceAfrican-American racez Sinus problemsSinus problemsz Persistent wheezingPersistent wheezing

DDGuideline for Diagnosis of Guideline for Diagnosis of
OSASOSASGuideline for Diagnosis of Guideline for Diagnosis of
OSASOSAS1.1. All children should be screened for All children should be screened for
snoringsnoring2.2. Complex high-risk patients should be Complex high-risk patients should be
referred to a specialistreferred to a specialist3.3. Patients with cardiorespiratory failure Patients with cardiorespiratory failure
cannot await elective evaluationcannot await elective evaluation4.4. Diagnostic evaluation is useful in Diagnostic evaluation is useful in
discriminating between primary snoring discriminating between primary snoring and OSAS, the gold standard being and OSAS, the gold standard being polysomnographypolysomnography

DD5.5. Adenotonsillectomy is the first line of Adenotonsillectomy is the first line of
treatment for most children, and treatment for most children, and continuous positive airway pressure is an continuous positive airway pressure is an option for those who are not candidates option for those who are not candidates for surgery or do not respond to surgeryfor surgery or do not respond to surgery
6.6. Patients should be reevaluated Patients should be reevaluated postoperatively to determine whether postoperatively to determine whether additional treatment is requiredadditional treatment is required
Guideline for Diagnosis of Guideline for Diagnosis of OSASOSAS
Guideline for Diagnosis of Guideline for Diagnosis of OSASOSAS
DDTreatmentTreatmentTreatmentTreatment
z Children with OSA have marked increases in Children with OSA have marked increases in healthcare-related costs healthcare-related costs
z If prompt diagnosis and management are not If prompt diagnosis and management are not implemented some of these complications may not implemented some of these complications may not be completely reversible, resulting in long-lasting be completely reversible, resulting in long-lasting consequences consequences
z Adenotonsillectomy is the treatment of choice for Adenotonsillectomy is the treatment of choice for most children and continuous positive airway most children and continuous positive airway pressure may be an option for those patients who pressure may be an option for those patients who are not a candidate for surgery or who do not are not a candidate for surgery or who do not respond to surgery respond to surgery

DDz Caregivers detected a long-term improvement in Caregivers detected a long-term improvement in
quality of life following adenotonsillectomy for quality of life following adenotonsillectomy for OSA although the results were not uniform OSA although the results were not uniform
z Decreasing nasal congestion associated with Decreasing nasal congestion associated with allergic rhinitis can improve sleep in these allergic rhinitis can improve sleep in these patients and lead to improved daytime quality of patients and lead to improved daytime quality of life life
z CPAP can be effectively used in children less CPAP can be effectively used in children less than 2 years of age than 2 years of age
TreatmentTreatmentTreatmentTreatment
DDz Children with primary snoring were Children with primary snoring were unlikelyunlikely to to
develop polysomnography-confirmed OSA and develop polysomnography-confirmed OSA and therefore delayed treatment was safe therefore delayed treatment was safe
z For patients with residual problems following For patients with residual problems following adenotonsillectomy, collaboration with adenotonsillectomy, collaboration with orthodontists to improve craniofacial risk factors orthodontists to improve craniofacial risk factors should be considered should be considered
TreatmentTreatmentTreatmentTreatment

DDSummarySummarySummarySummary
z Failure to diagnose and treat these patients can Failure to diagnose and treat these patients can result in serious but usually reversible problems result in serious but usually reversible problems which may include impaired growth, which may include impaired growth, neurocognitive and behavioral dysfunction and neurocognitive and behavioral dysfunction and cardiorespiratory failure cardiorespiratory failure
z Identifying these patients may be difficult Identifying these patients may be difficult because they may not exhibit signs or symptoms because they may not exhibit signs or symptoms while awake while awake
DDOne Westbrook Corporate CenterOne Westbrook Corporate CenterSuite 920Suite 920Westchester, IL 60154Westchester, IL 60154(708) 273-9335(708) 273-9335Annual MembershipAnnual Membership $295$295Quarterly - “ADSM Report”Quarterly - “ADSM Report”Quarterly – “Sleep and Breathing”Quarterly – “Sleep and Breathing”www. dentalsleepmed.orgwww. dentalsleepmed.org
One Westbrook Corporate CenterOne Westbrook Corporate CenterSuite 920Suite 920Westchester, IL 60154Westchester, IL 60154(708) 273-9335(708) 273-9335Annual MembershipAnnual Membership $295$295Quarterly - “ADSM Report”Quarterly - “ADSM Report”Quarterly – “Sleep and Breathing”Quarterly – “Sleep and Breathing”www. dentalsleepmed.orgwww. dentalsleepmed.org
Academy of Dental Sleep MedicineAcademy of Dental Sleep Medicine