
Cynthia Natiello, ARNP Seattle VA - mtsaacn.org · Tobacco use, SOB or DOE as presenting ......
75
Cynthia Natiello, ARNP Seattle VA
Transcript of Cynthia Natiello, ARNP Seattle VA - mtsaacn.org · Tobacco use, SOB or DOE as presenting ......

Cynthia Natiello, ARNPSeattle VA

Coronary Artery Bypass Graft (CABG)
Valve Replacement
MAZE Procedure
TMR
Aortic Aneurysm Repair
Heart Transplant
CAD single or multivessel Significant LM > 50%, widow makerRefractory anginaAngina with injury/ST elevation or
ischemia/ST depression LV dysfunction, proximal LAD LV failure/cardiogenic shock d/t CAD Perforation of coronary artery after PCI
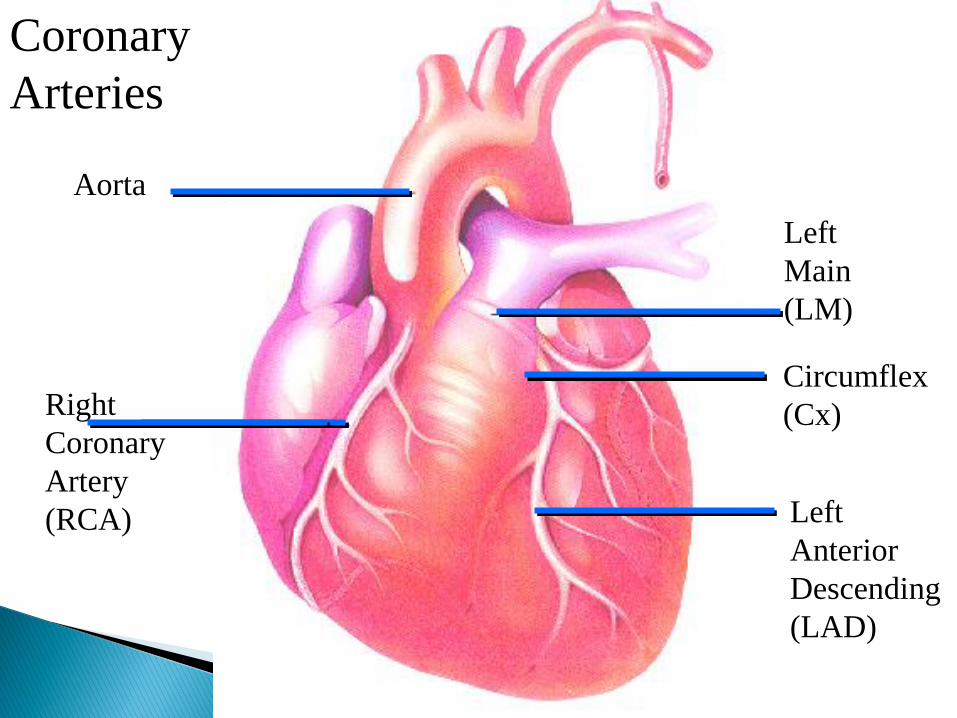
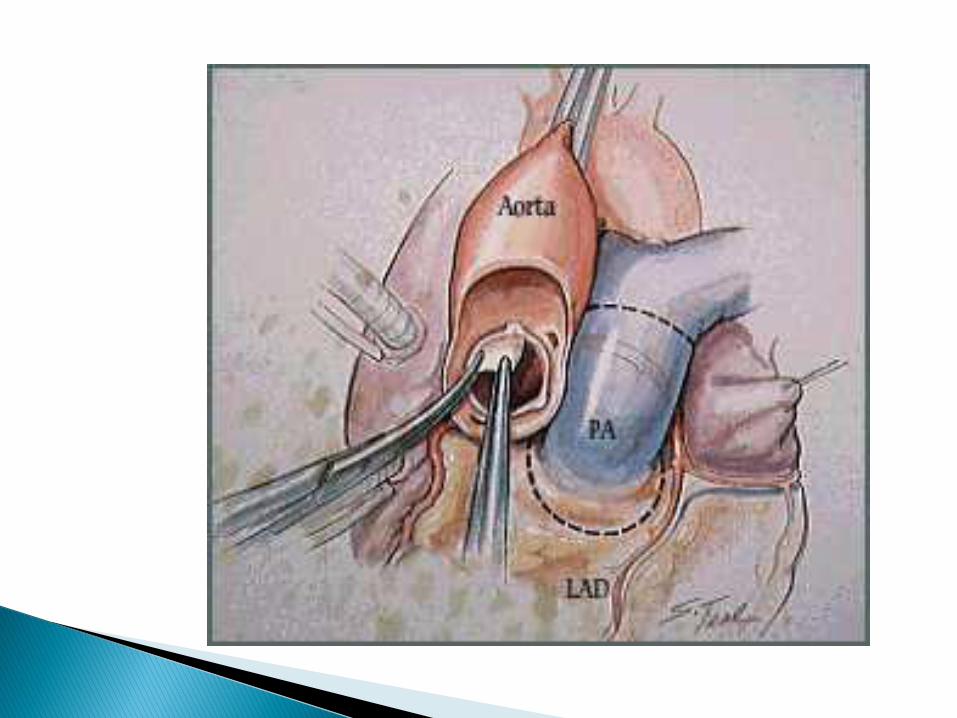
Aorta
Right
Coronary
Artery
(RCA) Left
Anterior
Descending
(LAD)
Circumflex
(Cx)
Left
Main
(LM)
Coronary
Arteries
Cardiac catheterization:Angina, presence or lack of CADDelineates anatomy & targets
Echocardiogram:Murmurs, suspicion of valvular diseaseR or L ventricular dysfunctionEjection fraction 55% nl.
History & physical including social & family
EKG
CXR PA & Lat
Type & Cross x 4 U PRBCs & 6u w/4u FFP if redo
Labs:
-CBC, coags, chemistry, BNP
-Urinalysis
-LFTs Anesthesiologist Consults with specialty teams
Carotid Duplex:
Age > 65, PVD, TIA/CVA, presence of carotid bruit
Pulmonary Function Tests:
Tobacco use, SOB or DOE as presenting symptoms, exam findings, pulmonary disease
DENTAL
Clearance for valve or graft placement
(e.g. aortic aneurysm repair)
Rationale: Oral disease can cause
endocarditis of a new valve (a catastrophic p/op situation)

BETA BLOCKERSImportant! Should be continued
ACEI/ARBSDC 1-2 days pre-op, peri-operative hypotension
WARFARIN
DC 5 days pre-op, bridge w/LMWH, bleeding
PLAVIX
DC 5-7 days prior, bleeding
ASPIRIN continue

INSULIN & METFORMINHold am dose, NPO & hypoglycemia
STATINS continue
ANTIBIOTICSCefazolin 1-2 gm & Vancomycin 1 gm
CHLORHEXIDINE SCRUB/MUPIROCIN

Median
Sternotomy
Endovascular Vein Harvesting

Coronary Artery Bypass Graft Surgery (CABG)

Purpose: Decreases O2 demand
Surgical Indications:
Pre or post/op MI, weaning from CPB,
maintenance of graft patency
Contraindications:
Aortic regurgitation, thoracic & abdominal aortic aneurysm, severe PVD, bleeding
Preload- degree of myocardial stretch created by venous return , the load placed on the cardiac muscles before contraction. For the ventricles, the amount of volume at the end of diastole 4-12mmHg.
Afterload-the force that opposes ventricular ejection & resistance of the arterioles,

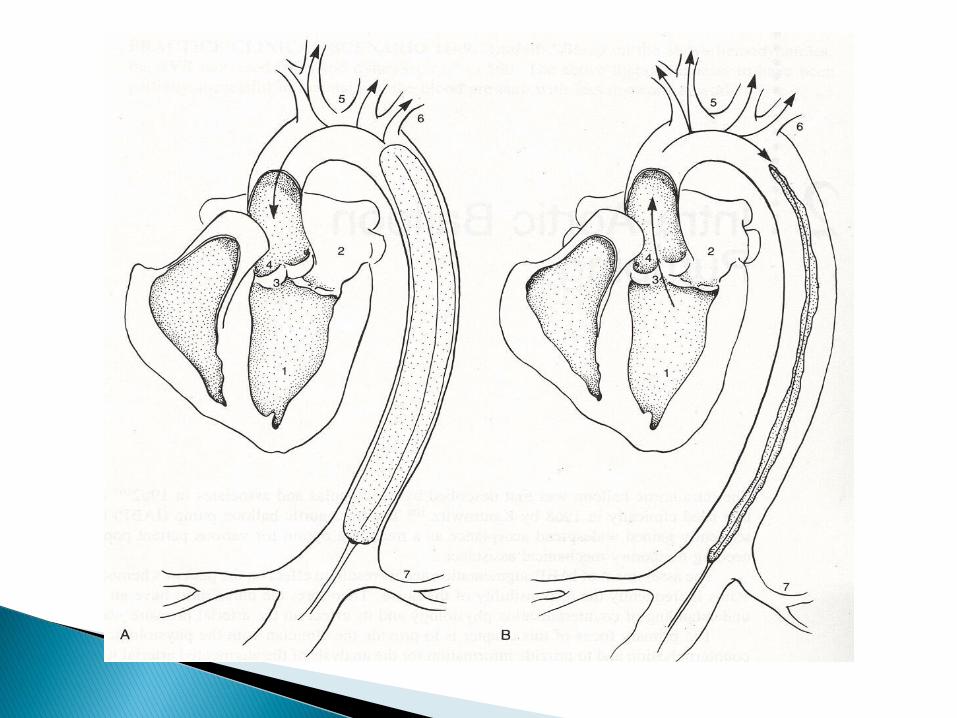
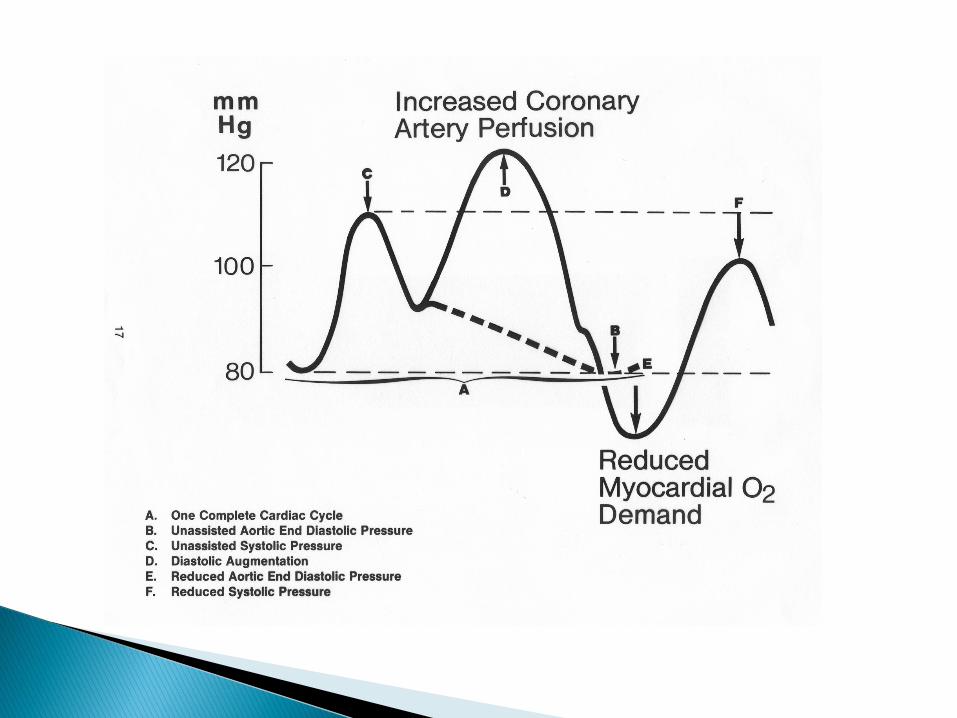
Inflation:
Increases coronary blood flowIncreases diastolic pressureIncreases systemic perfusion
Deflation:
Decreases after load
IVC phase shortenedIncreases stroke volumeEnhances cardiac output
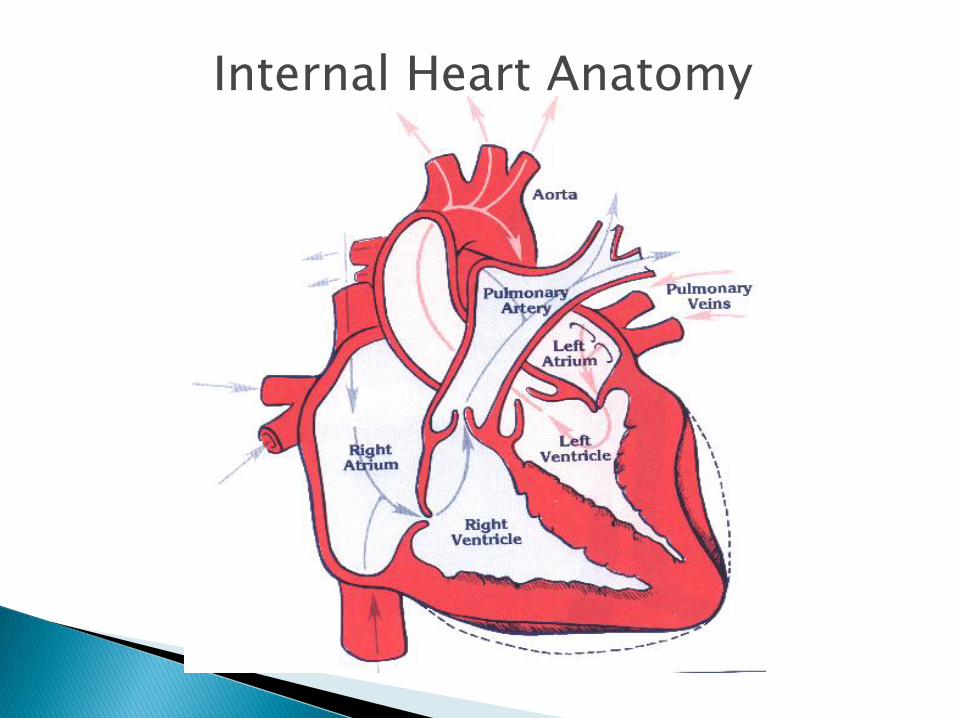
Internal Heart Anatomy

Indications:Stenosis-narrow valve or unable to open fully
Insufficiency-too wide and unable to close completely
S/S: AS-DOE/SOB, syncopeAI-fatigue, dyspnea, dizzinessMVP-asymptomatic, chest pain MR-tachycardia, dyspnea, orthopnea
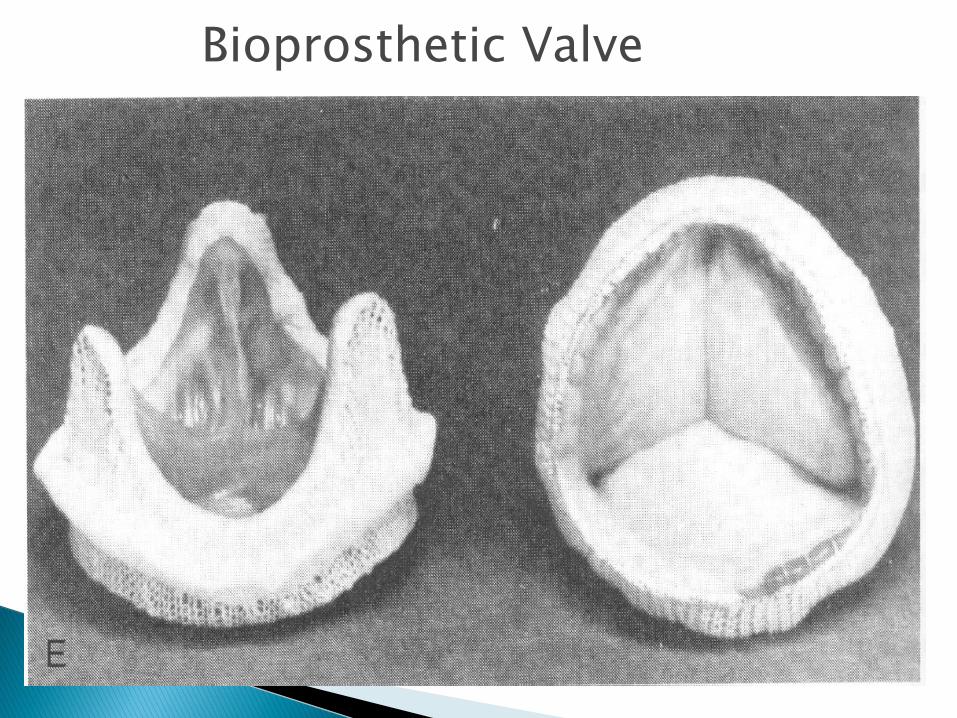
Bioprosthetic Valve

Prosthetic
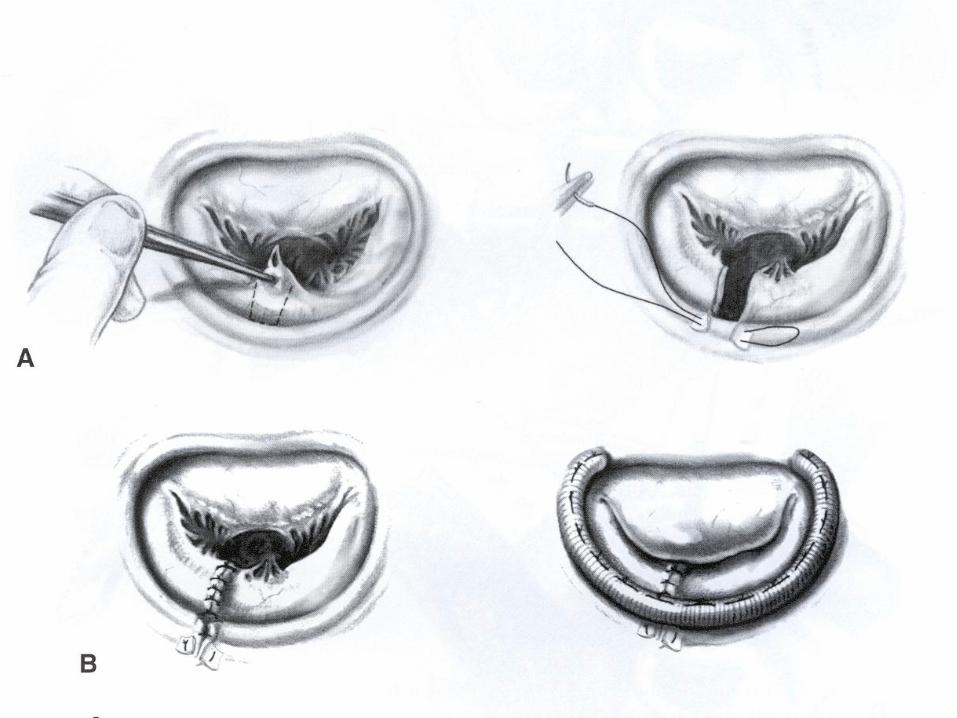
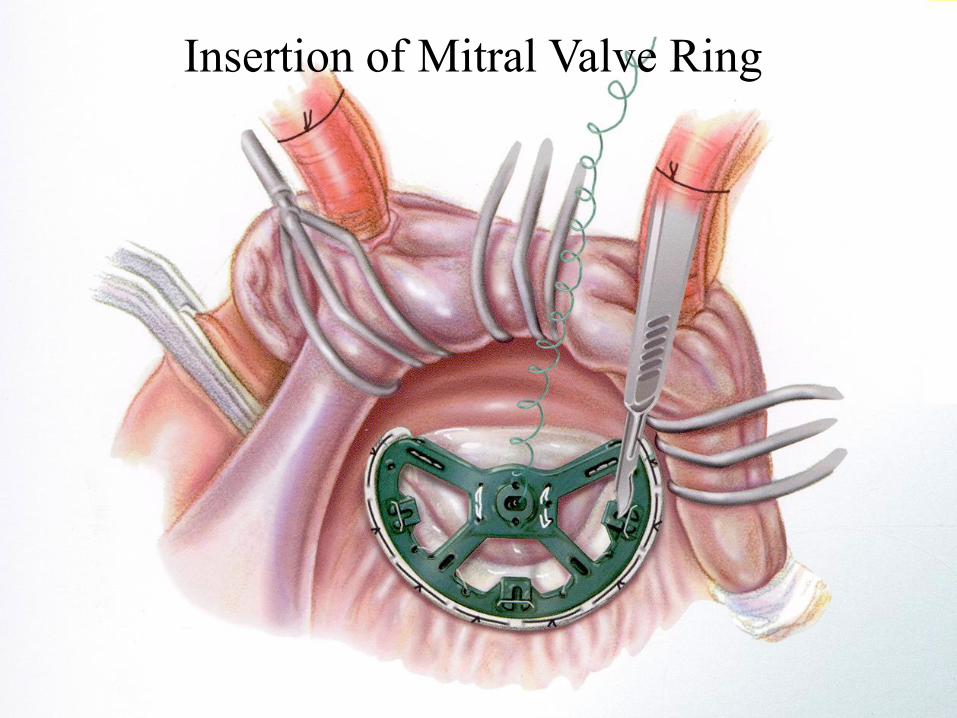
Insertion of Mitral Valve Ring

Bioprosthetic/Porcine
Aortic INR none, ASA 81mg
Mitral INR 2.0-3.0, x 3 mo., 81mg ASA
Prosthetic/Mechanical-chronic
Aortic INR 2-0-3.0, ASA 81mgMitral INR 2.5-3.5, ASA 81mg
ACCP Evidence based clinical practice guidelines, 8th
ed. 2008

Treats AF
Laser treatment for AF, creates a maze of new electrical pathways so that impulsescan travel easily through the heart.
P/op complications: Bradycardia-permanent pacemaker, bleeding
Anticoagulation for 3 months

Treats refractory unstable angina
CO2 laser drills holes in epicardial wall
at rest
Increases oxygenated blood flow &
stimulates new blood vessel growth
Alpha receptors:Vascular smooth muscle, alpha 1 vaso-
constriction (pressor effect), alpha 2 dilatation, NE > Epi
Beta receptors:Beta 1 heart, increases rate & force of
contraction (inotrope effect), NE = EpiBeta 2, vascular smooth muscle, dilatation,
Epi > NE
Norepinephrine (Levophed)
Sympathometic w/largely alpha 1-increasing SVR & BP, .01-.1 mcg/min, little beta 1-increasing contractility & pulse
Epinephrine
Strong beta 1 contractility-increasing CO & pulse, .01-.3 mcg/kg/min, low doses beta 2-dilatation, high doses alpha 1-increasing vasoconstriction & BP
Vasopressin
Potent vasoconstrictor, increases SVR & BP, .01-.1unit/min

Milrinone
Increases CI & contractility, decreases SVR, 0.25-0.75mcg/kg/min
Dopamine
Increases contractility, C.O., SVR & P, .5-20mcg/kg/min
Dobutamine
Increases contractility, CO & mild increase in SVR, 2-15 mcg/kg/min,
NTG
Smooth muscle relaxant, low doses, 5-200 mcg/min,), reduces preload, higher doses reduces afterload, used after CABG to prevent LIMA vasospasm, decreases BP
Nitroprusside
Decreases SVR, reduces afterload, increases BP, .3-5mcg/kg/min
Insulin Serum glucose 100-140 mg/dL
w/continuous infusionDiabetic & non-diabeticContinue 72 hrs or until taking PO, then
SQDecreases mortality & morbidityDecreases p/op infections
Amiodarone…
Systolic blood pressure (SBP) 60-90mmHg
Cardiac Index (CI) 2.2-4.4L/min
Central Venous Pressure (CVP) 10-15mmHg
Pulmonary capillary wedge pressure (PCWP) 10-15mmHg
Systemic Vascular Resistance (SVR) 800-1200
Mean Arterial Pressure (MAP) 70-100mmHg
Cardiac Output (CO) 4-8L/min

Air, fluid or blood from pleural space
H2O seal chamber-nl rise & fall w/respiration, air leak w/persistent bubbling, ok w/coughing
Cessation of drainage-clotted, kinked
Pain @ insertion site w/inspiration-improperly placed, interferes w/deep breathing
Assess for SQ air & s/s infection
Bloody drainage > than or equal to 200ml/hr, hemorrhage/shock

Epicardial Pacing Wires
Monitor for dysrhythmias
Separate & insulate grounding pins
Gloves when manipulating or cleaningwires
No electric shavers Shower after wires are removedRemoval in supine, steady slow gentle
tension uncoils wire, 24h before DCMonitor for S/S of cardiac tamponade, rare

Arrhythmias
Bleeding/HIT
Cardiac tamponade
Hypothermia
Pulmonary
complications
Cardiogenic shock
Hypo/hypertension Renal dysfunction Infection CNS complications GI complications Hyperglycemia/DM Electrolyte
imbalance
Afib-common, 20-30% cardiac surgeries, > 50% valve surgery, older pts, atrial arrhythmias, lung disease, R CAD, long cross clamp time, hypothermia
Ventricular-less common 1%, hypoxemia, acid-base imbalance, acute MI
Heart blocks-valve & MAZE
Treatments:Correct K+ and Mg++, medications,temporary pacing

Atrial Fibrillation Increases risk of p/op ventricular arrhythmias
Treat prophylactically:Metoprolol 25-50 mg PO bidMagnesium 2 gm IV after CPB & POD #1Amiodarone started in OR & converted
to PO 150 mg, then 60mg/h x 8 hrs, then 30mg/h x 16h then 400 mg PO bid x 1 week

Causes:Heparin intra-op, long case, redo surgery, p/o anticoagulation
Treatments:Blood products, IVF, medications, apply PEEP, re-explore chest 1-3%
Type 1
Common w/i 48 hrs, PLT ct 100.00
Type 2
PLT decrease by 50% 5-10d
Treatment
Stop heparin, start IV lepirudin or argatroban

Precordial fullness, pain, dyspnea, anxiety,
cyanosis, altered LOC, feeling of
impending doom
Beck’s triad: hypotension, distended neck
veins, muffled heart tones
Falling UOP
Tachycardia to PEA

Hemodynamic changes:
High equalizing pressures RA, PCW, LA
Narrowing pulse pressure
Fall in CI
CXR shows widening mediastinum
Tranesophageal echo

Widening of
mediastinum
Kouchoukos, N T Aneurysms of the Ascending Aorta,
pg227 In Glenn’s Thoracic and Cardiovascular Surgery
Diagnosis: CXR
Treatment
Declot chest tube
Volume-NS, Albumin, blood products
Pericardiocentesis
Open chest @ bedside
Return to OR
<36 C to ICU
Increases SVR & BP, atrial & ventricular
arrhythmias, shivering decreases O2 &
increases CO2, Plt dysfunction
Nitroprusside & propofol for vasodilatation
Apply body warming air blankets-BAIR Hugger

Common:
Pleural effusion
Pneumonia
HF
Pneumothorax
Less common:
PE
Hemothorax
Paralyzed diaphragm-phrenic nerve

Hemidiaphragm elevation

Prevention:
Early extubation, pharyngeal dysfunction from prolonged intubation-risk for aspiration pneumonia d/t dysphagia
Adequate pain medicationsPulmonary toiletingOOB w/i 12 hrs p/opMaintain CT patency & remove asapDiuresis decreases effusions, start POD
#2

Perioperative AMI is uncommon, 5%
Observations:
Assess for decreased SVR & CI/CO
Observe for ECG changes
Cardiac enzymes
Decreasing UOP, classic sign
Treatments:
Vasoactive drugs for coronary spasms
Increase filling pressures, maintain CO
If p/op AMI, return to cath lab/OR
Causes:
Pain
Anxiety
Chronic issue
Volume overload
Treatments:
Pain medications
Anxiolytics
Antihypertensive
Diuretics
Cause:
3rd spacing
Volume depletion, diuretics
Inadequate fluid intake
BB to prevent AF
Tamponade
Shock: hypovolemic, cardiogenic, septic
Treat cause
Common causes:
Pre-existing disease-CKD
Pre-op medications, ACEI/ARBs & NSAIDS
Hypotension
Cardiac catheterization dye load
P/op vasoactive meds, NE, vasopressin

Prevention/observations:
Maintain cardiac index( CI) >2.2 & MAP> 65 mm Hg
Use as little vasoactive medications aspossible
Monitor BUN, creatinineAvoid anti-inflammatories, toradolDialysis
Common Cause: Underlying lung disease, diabetes, catheters in prolonged time, poor protoplasm
Treat:Blood sugar control <140-180 mg/dLMinimal wound manipulation: remove surgical dressing 2 days, transparent occlusive dressing on graft site @ DC
Excellent hand washingMonitor incisions, WBC, temp…Blood, wound & sputum cultures, UA, Antibiotics after culture if possible
Mediastinum:
Loosely defined space between the L & R pleura, sternum & vertebrae; contains heart, great vessels, esophagus & loosely organized connective tissues
Mediastinitis: deep infection requiring surgical debridement &/or surgical repair (retrospective dx)
Systemic symptoms precede local
Fever, leukocytosis, tachycardia, general illness
Pain &/or sternal instability
Crepitus on exam
Purulent drainage &/or local cellulitis
Median detection POD #7, majority w/i 14 days, rare beyond POD #30
MSSA linked to pre operative skin flora
MRSA linked to true patient to patient transmission (nosocomial)
Treat w/antibiotics or surgical debridement

Causes:Micro-emboli, aorta, most commonCerebral hypoperfusionCarotid stenosis
Assess LOC/Neuro as soon as able
Head CT/MRI
Neurology consult
Dysphagia-ice chips, speech consult
Nausea-zofran
Constipation-colace, supp, increased activity, PT/OT
Diarrhea-stool specimen, fluids
Gastritis/GI bleed-PPIs, H2 blockers, antacids
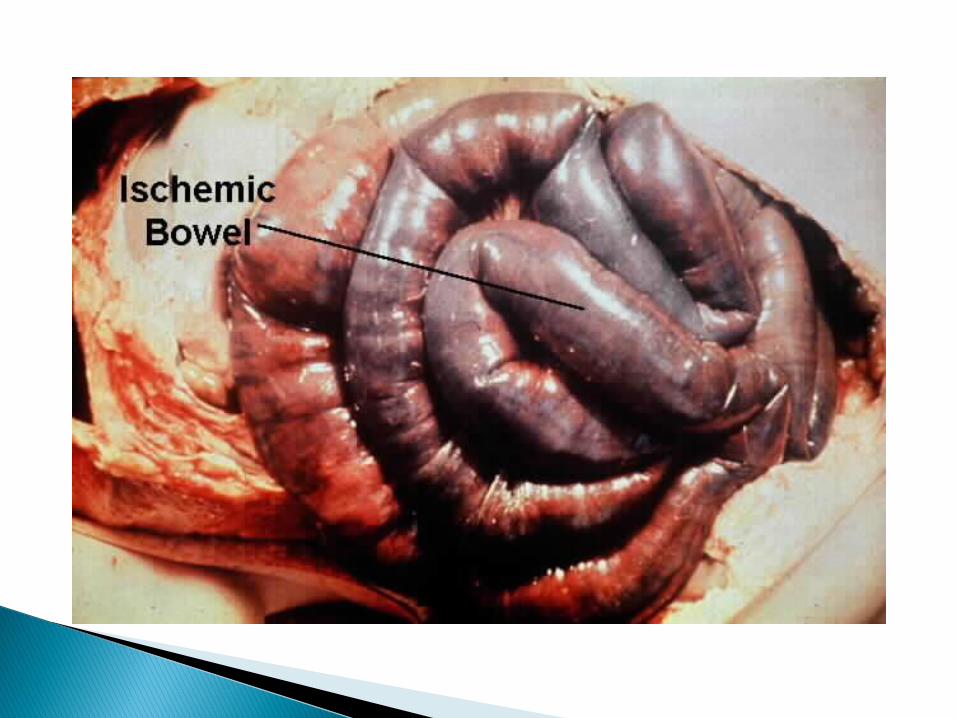
ileus-bowel rest, NGT, TPN
Emergent bowel exploration
Causes:
Pre-existing dementia, medications, pre-op anxiety/paranoia
Treatments:Re-orientRemove restraints ASAPMaximize sleeping patternsControl environmental noiseAssess/control pain-watch for hallucinationsEliminate medication offenders-narcoticsPrevent sternal injuries

IS x 10 q 1h Sternal precautions pt/familyOOB for meals & ambulate 3-4 X/day Shower if CT & pacing wires out
Monitor:Labs: Hct, WBC, PLT, Cr, K+, PT/INRDaily weight so important! S/S InfectionPain controlMedication effects

Saphenous: ACE, occlusive dsg, no SCDs
Radial: No blood pressure or lab draws from
arm, assess hand function, exercises
Monitor:
Hematoma, cellulitis, purulent drainage,
compartmental syndrome

Evaluate peripheral circulation:
aortic dissection, emboli
Evaluate renal function-malposition of catheter
Identify best augmentation, 1:1…
Observe for bleeding, Plt trauma
Monitor for arrhythmias
Monitor for infection
Pt. comfort
Protect IABP placement: skin, log rolling,
avoid leg flexion, HOB < 30 degrees

Sternal precautions-no lifting, pushing,
pulling >10lbs or driving for 6 wks
Daily walking
IS q2h x10 for 1 wk
BP, P, T
S/S infection
Incision care-no hot tubs, swimming
pools, jacuzzis
F/up Cardiac sx, Cardiologist, PCP

Aranki, S. & Aroesty, J.M. (2005) “Medical therapy to prevent perioperative complications after coronary artery bypass graft surgery” in UpToDate, www.uptodate.com. Last date of modification 10/5/2009.
Aasbo, J.D., Lawrence, A.T., et al. “Amidarone prophylaxis reduces major cardiovascular morbidity and length of stay after cardiac surgery; a meta-analysis. Annals of Internal Medicine (2005): 143:327.
Bojar, RM (2005) Manual of Perioperative Care in Cardiac Surgery. 4th
Edition. Malden, MA: Blackwell Science. Belzberg, H., & Rivkind, A. “Preoperative cardiac preparation” Chest
(1999): 115:82S-95S. Centers for Disease Control (CDC) (1999) “Recommendations for
Prevention of Surgical Site Infection” Available at www.cdc.gov.

Crystal,E., Connolly, S.J. et al. Interventions for preventing postoperative atrial fibrillation in patients undergoing heart surgery. Cochrane Database Systematic Review 2004; 106:75.
DiDomenico, R.J. & Massad, M.G. “Pharmacological strategies for Prevention of Atrial Fibrillation After Open Heart Surgery” Ann Thoracic Surg 2005: 79:728 – 40.
Handbook of Patient Care in Cardiac Surgery, 7th Ed., Lippincott Williams & Wilkins. In Books@Ovid-LVWW Doody’s CoreTitle Collections 2010.
Eagle, L.A. & Guyton, R.A. “ACC/AHA 2004 guideline update for coronary artery bypass graft surgery; a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines” Circulation (2005): 111:2014.
Jolles, H., Henry, D.A. et al. (1996) “Mediastinitis following median sternotomy; CT findings. Radiology, 201:463-6.
Maluk, V. & Macpherson, D.S. (2010) “Perioperative medication management” in UpToDate, www.uptodate.com. Last date of modification 2/17/2010.
Mangram, A.J., Horan, T.C. et al. (1999) Guideline for Prevention of Surgical Site Infection. Infection Control and Hospital Epidemiology 20:4(250-278).
Silvestry, F., (2010) “Overview of the postoperative management of patients undergoing cardiac surgery” UpToDate, www.uptodate.com. Last date of modification 9/22/10
Wiegand, D,J, Carlson, K.K. (2010) Procedure Manual for Critical Care, 6th Edition. St. Louis, MO: Elsevier Saunders.
Woods, S.L., Froelicher, E.S. et al. (2009) Cardiac Nursing, 6th
Edition. Philadelphia, PA: Lippincott Williams & Wilkins.