CPC:38 year-old AIDS patient with brain and pulmonary lesions Gregory M. Lucas, MD PhD Division of...
26
CPC:38 year-old AIDS patient with brain and pulmonary lesions Gregory M. Lucas, MD PhD Division of Infectious Diseases
-
Upload
adam-campbell -
Category
Documents
-
view
214 -
download
0
Transcript of CPC:38 year-old AIDS patient with brain and pulmonary lesions Gregory M. Lucas, MD PhD Division of...

CPC:38 year-old AIDS patient with brain and pulmonary lesions
Gregory M. Lucas, MD PhD
Division of Infectious Diseases

Could a viral CNS infection present this way?
• Herpes viruses – CMV, VZV, HSV can affect the CNS
• Typical picture is encephalitis often with ventriculitis
• CSF usually abnormal
• CNS mass lesions not seen
• Couldn’t explain pulmonary findings

Initial approach to an AIDS patient with brain lesions
No mass effect, no enhancement with IV contrast
• HIV encephalopathy• Progressive multifocal leukoencephalopathy (PML)
Mass effect, enhancement with IV contrast
• Abscess• Malignancy

Differential diagnosis of contrast-enhancing CNS lesions in an AIDS patient
Abscess• Toxoplasmosis• Cryptococcosis, dimorphic
fungi (histoplasmosis, coccidioidomycosis)
• Pyogenic abscess (Staph, Strep, polymicrobial)
• Tuberculosis• Nocardiosis• Filamentous fungi• Neurocysticercosis
Malignancy• Primary CNS lymphoma• Non-CNS cancer
metastatic to brain

Toxoplasma gondii • Cats are definitive host, many other animals
incidental host• Seroprevalence in Baltimore ~10%• Disease in AIDS is reactivation of latent infection
Pro Con• Most common cause of brain lesions
in AIDS patients
• Multiple ring-enhancing lesions typical (basal ganglia, corticomedullary junction cerebrum and cerebellum)
• Toxo IgG negative
• Lung lesions atypical

CNS toxoplasmosis

Yeast: H. capsulatum (C. neoformans) • Found worldwide, but geographical variation in intensity
of exposure• Lung – fungemia – CNS involvement in 10-20% (usually
meningitis)• Histoplasma antigen testing from serum or urine highly
accurate in disseminated disease
Pro Con• May produce nodular lung infiltrates • CRAG negative
• Brain abscesses rare with Histo



Pyogenic brain abscess • Classification
– Extension from sinuses or ear, – “Metastatic” – typically multiple– trauma or post-operative
• S. aureus, Streptococci, anaerobic organisms
Pro Con• Could pulmonary lesions be septic
emboli?• High-grade bacteremia should have
been readily detected
• No association with AIDS

Mycobacterium tuberculosis • Infects 1/3 of global population• Transition from latent to active disease occurs in 10% of HIV
co-infected patients per year• CNS involvement
– Meningitis – prominent basilar meningeal enhancement– Tuberculomas – often multiple, solid-appearing grossly, often
accompanied by meningitis– Tuberculous abscess – quite rare, large, solitary, multiloculated
Pro Con• Appealing explanation for lung-brain
involvement
• ETOH and drug dependence increases likelihood of exposure
• AFB smears (induced sputum) negative at outside hospital
• No meningitis

Tuberculomas

Nocardiosis • “Higher-order” bacteria, gram-positive branching
filaments, usually acid-fast• Ubiquitous environmental saprophytes• Defects in cell-mediated immunity important risk factor• Manifestations
– Cutaneous infections (nodular lymphangitis, mycetoma)– Pulmonary – disseminated (usually N. asteroides)
Pro Con• Lung-brain involvement common
• Pulmonary nodular infiltrates common
• No cavities or pleural effusion

Acid fast stain of N. asteroides

Nocardia pulmonary infection in transplant patient

Nocardia brain abscess

Rhodococcus equi• Gram-positive, weakly acid-fast rod• May be mistaken for a “diptheroid” contaminant• Causes pneumonia in foals• Present in soil, 1/3 infected have exposure to horses• In immunocompromised humans it presents as a TB mimic –
indolent, upper-lobe, cavitary• Difficult to treat
Pro Con• Dissemination to brain can occur • Rare
• No horse exposure
• Pulmonary infiltrates with R. equi typically upper lobe cavities

Filamentous fungi: Aspergillus, Pseudallescheria, zygomycosis• Neutrophil defects strongest risk factor for invasive aspergillosis–bone
marrow transplant, chronic granulomatous disease (CGD)– Other risk factors – steroids, alcoholism
• Lung or sinuses typical portal of entry– Dissemination to brain common, never meningitis
• Unusual in AIDS patients – very advanced disease, relative neutropenia, steroid use
• Notable aspect of pathogenesis is angioinvasion
Pro Con• Lung involvement with dissemination
to brain a hallmark of filamentous fungi
• “Wedge” shaped pulmonary infiltrates characteristic
• ?PE
• Rare complication in AIDS
• WBC 11,380 at presentation making neutropenia unlikely

Aspergillus invading blood vessel

Neurocysticercosis• Taenia solium (pork tapeworm)
– Eat pigs (undercooked) – tapeworm infection – secrete eggs– Eat poop (containing eggs) – cysticercosis (tissue infection with
parasites)
• Infection common south of the Mexican border– Accounts for 50% of adult onset seizures
Pro Con• CNS lesions in NC – typically round,
fluid filled or calcified
• Not AIDS associated
• Wouldn’t explain pulmonary process

Neurocysticercosis

Malignancies

Primary CNS lymphoma• 2nd Most common cause of ring-enhancing brain lesions
in AIDS patients in US• Unlike peripheral lymphomas – PCNSL seen exclusively
in advanced disease• Solitary lesion in 50%, multicentric in 50%• Non-Bx methods to distinguish from toxo: Toxo IgG, EBV
PCR from CSF, metabolic function scans (SPECT, PET)
Pro Con• Most common cause of enhancing
brain lesion in AIDS patients with negative toxo IgG
• Advanced immunosuppression typical
• Lung infiltrates would have to be a second process
Malignancy metastatic to brain
• Most common tumors metastasizing to brain – lung, kidney, colon, breast, melanoma
• Kaposi’s sarcoma metastasis to brain extremely rare• Peripheral lymphomas may metastasize to brain
Pro Con• PE related to hypercoagulability of
malignancy• Most common cancers metastasizing
to brain not particularly associated with AIDS
• Pulmonary lesions don’t look like metastases
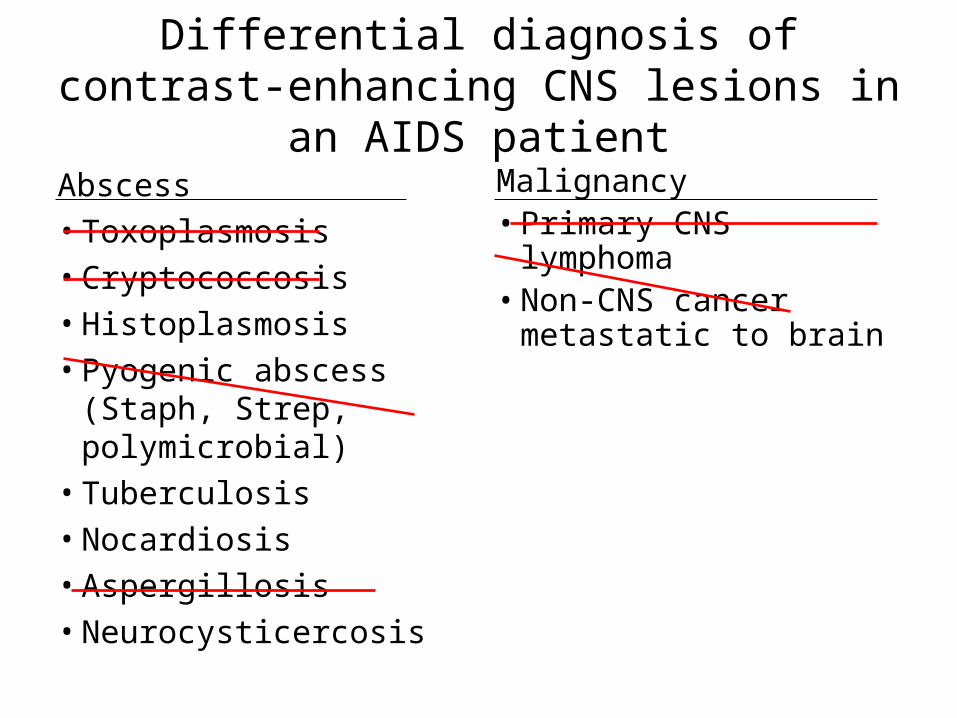
Differential diagnosis of contrast-enhancing CNS lesions in an AIDS patient
Abscess• Toxoplasmosis• Cryptococcosis• Histoplasmosis • Pyogenic abscess (Staph,
Strep, polymicrobial)• Tuberculosis• Nocardiosis• Aspergillosis• Neurocysticercosis
Malignancy• Primary CNS lymphoma• Non-CNS cancer
metastatic to brain

Clinical diagnosis
• Pulmonary aspergillosis disseminated to brain
• Nocardiosis
• Histoplasmosis
• Tuberculosis