Corticoide en Tb
15
7/28/2019 Corticoide en Tb http://slidepdf.com/reader/full/corticoide-en-tb 1/15 www.thelancet.com/infection Vol 13 March 2013 223 Articles Corticosteroids for prevention of mortality in people with tuberculosis: a systematic review and meta-analysis Julia A Critchley, Fiona Young, Lois Orton, Paul Garner Summary Background The effects of corticosteroids are systemic, but their benefits in tuberculosis are thought to be organ specific, with clinicians using them routinely to treat some forms of tuberculosis (such as meningitis), but not others. We aimed to assess the effects of steroids on mortality attributable to all forms of tuberculosis across organ systems. Methods We did a systematic review and meta-analysis to estimate the effi cacy of steroids for the prevention of mortality in all forms of tuberculosis, and to quantify heterogeneity in this outcome between affected organ systems. We searched the Cochrane Infectious Diseases Group trials register, the Cochrane Central Register of Controlled Trials, Medline, Embase, and Literatura Latino-Americana e do Caribe em Ciências da Saúde (LILACS) for studies published up to Sept 6, 2012, and checked reference lists of included studies and relevant reviews. We included all trials in people with tuberculosis in any organ system, with tuberculosis defined clinically or microbiologically. There were no restrictions by age, comorbidity, publication language, or type, dose, or duration of steroid treatment. We used the Mantel-Haenszel method to summarise mortality across trials. Findings We identified 41 eligible trials, 18 of which assessed pulmonary tuberculosis. 20 of the 41 trials (including 13 of those for pulmonary tuberculosis) were done before the introduction of modern rifampicin-containing antituberculosis chemotherapy. Meta-analysis stratified by affected organ systems identified no heterogeneity; steroids reduced mortality by 17% (risk ratio [RR] 0·83, 95% CI 0·74–0·92; I ² 0%), consistent across all organ groups. In a sensitivity analysis that only included trials that used rifampicin-containing regimens, the results were similar (RR 0·85, 95% CI 0·74–0·98; I ² 21%). A sensitivity analysis in pulmonary tuberculosis that excluded trials with high potential risks of bias suggested a slight benefit, but the point estimate was closer to no effect and the difference was not significant (RR 0·93, 95% CI 0·60–1·44). Interpretation Steroids could be effective in reducing mortality for all forms of tuberculosis, including pulmonary tuberculosis. However, further evidence is needed since few recent trials have assessed the effectiveness of corticosteroids in patients with pulmonary tuberculosis. Funding UK Department for International Development. Introduction About 8·7 million incident cases of tuberculosis occur annually, and the disease causes nearly 1·4 million deaths each year. 1,2 Despite effective treatments, tuber- culosis incidence and mortality remain very high in some regions, partly because of HIV infection, poverty, population ageing and migration, multidrug resistance, 3 disruption of health systems, 1,4 and the rise in some non- communicable diseases such as diabetes. 5–7 The burden of disease is also increasing because of population growth. 4 In clinical care, one enduring question is whether to use corticosteroids routinely in addition to antituberculosis drugs. The inflammatory response to infection damages tissues and treatment with steroids might counter this effect. However, steroids can make people vulnerable to other infections, could worsen the outcome of infection with Mycobacterium tuberculosis, and pharmacokinetic interactions between antituber- culosis drugs (particularly rifampicin) and steroids have been documented. 8–12 Although some investigators might argue that the effects of steroids are specific to the particular organ infected, it is equally plausible that a common underlying pathological mechanism of the host’s inflammatory response at least partly contributes to the disease process, and that the effects of steroids in one organ system might therefore have implications for management of other forms of the disease. 13,14 Previous Cochrane systematic reviews have examined corti- costeroids in specific organ systems for tuberculous pleurisy, 15 pericarditis, 16 and meningitis, 17 and we have recently completed a systematic review of corticosteroids for pulmonary tuberculosis (unpublished). Results have shown clear effects on mortality in meningitis, a statistically non-significant effect in pericarditis (for which the analysis was very underpowered), and possible short-term clinical benefits in pulmonary tuberculosis. We aimed to assess the effect of steroids on mortality attributable to all forms of tuberculosis across organ systems, with careful examination of results within and between organ systems, to attempt to provide some insights into the best treatments and directions for future research. Lancet Infect Dis 2013; 13: 223–237 Published Online January 29, 2013 http://dx.doi.org/10.1016/ S1473-3099(12)70321-3 See Comment page 186 Division of Population Health Sciences and Education, St George’s, University of London, London, UK (Prof J A Critchley DPhil); Institute of Health and Society, Newcastle University, Newcastle upon Tyne, UK (F Young PhD); Department of Public Health and Policy, Institute of Psychology, Health and Society, University of Liverpool, Liverpool, UK (L Orton PhD); and International Health Group, Liverpool School of Tropical Medicine, Liverpool, UK (Prof P Garner MD) Correspondence to: Prof Julia Critchley, Division of Population Health Sciences and Education, St George’s, University of London, Cranmer Terrace, London SW17 0RE, UK [email protected]
-
Upload
pamela-wheelock -
Category
Documents
-
view
228 -
download
0
Transcript of Corticoide en Tb

7/28/2019 Corticoide en Tb
http://slidepdf.com/reader/full/corticoide-en-tb 1/15www.thelancet.com/infection Vol 13 March 2013 223
Articles
Corticosteroids for prevention of mortality in people with
tuberculosis: a systematic review and meta-analysis Julia A Critchley, Fiona Young, Lois Orton, Paul Garner
SummaryBackground The effects of corticosteroids are systemic, but their benefits in tuberculosis are thought to be organspecific, with clinicians using them routinely to treat some forms of tuberculosis (such as meningitis), but notothers. We aimed to assess the effects of steroids on mortality attributable to all forms of tuberculosis across organsystems.
Methods We did a systematic review and meta-analysis to estimate the effi cacy of steroids for the prevention of mortality in all forms of tuberculosis, and to quantify heterogeneity in this outcome between affected organsystems. We searched the Cochrane Infectious Diseases Group trials register, the Cochrane Central Register of Controlled Trials, Medline, Embase, and Literatura Latino-Americana e do Caribe em Ciências da Saúde (LILACS) for
studies published up to Sept 6, 2012, and checked reference lists of included studies and relevant reviews. Weincluded all trials in people with tuberculosis in any organ system, with tuberculosis defined clinically or microbiologically. There were no restrictions by age, comorbidity, publication language, or type, dose, or durationof steroid treatment. We used the Mantel-Haenszel method to summarise mortality across trials.
Findings We identified 41 eligible trials, 18 of which assessed pulmonary tuberculosis. 20 of the 41 trials (including13 of those for pulmonary tuberculosis) were done before the introduction of modern rifampicin-containingantituberculosis chemotherapy. Meta-analysis stratified by affected organ systems identified no heterogeneity; steroidsreduced mortality by 17% (risk ratio [RR] 0·83, 95% CI 0·74–0·92; I ² 0%), consistent across all organ groups. In asensitivity analysis that only included trials that used rifampicin-containing regimens, the results were similar (RR 0·85, 95% CI 0·74–0·98; I ² 21%). A sensitivity analysis in pulmonary tuberculosis that excluded trials with highpotential risks of bias suggested a slight benefit, but the point estimate was closer to no effect and the difference wasnot significant (RR 0·93, 95% CI 0·60–1·44).
Interpretation Steroids could be effective in reducing mortality for all forms of tuberculosis, including pulmonarytuberculosis. However, further evidence is needed since few recent trials have assessed the effectiveness of corticosteroids in patients with pulmonary tuberculosis.
Funding UK Department for International Development.
IntroductionAbout 8·7 million incident cases of tuberculosis occurannually, and the disease causes nearly 1·4 milliondeaths each year.1,2 Despite effective treatments, tuber-culosis incidence and mortality remain very high insome regions, partly because of HIV infection, poverty,population ageing and migration, multidrug resistance,3 disruption of health systems,1,4 and the rise in some non-
communicable diseases such as diabetes.5–7
The burdenof disease is also increasing because of populationgrowth.4 In clinical care, one enduring question iswhether to use corticosteroids routinely in addition toantituberculosis drugs. The inflammatory response toinfection damages tissues and treatment with steroidsmight counter this effect. However, steroids can makepeople vulnerable to other infections, could worsen theoutcome of infection with Mycobacterium tuberculosis,and pharmacokinetic interactions between antituber-culosis drugs (particularly rifampicin) and steroids havebeen documented.8–12 Although some investigatorsmight argue that the effects of steroids are specific to the
particular organ infected, it is equally plausible that acommon underlying pathological mechanism of thehost’s inflammatory response at least partly contributesto the disease process, and that the effects of steroids inone organ system might therefore have implications formanagement of other forms of the disease.13,14 PreviousCochrane systematic reviews have examined corti-costeroids in specific organ systems for tuberculous
pleurisy,15
pericarditis,16
and meningitis,17
and we haverecently completed a systematic review of corticosteroidsfor pulmonary tuberculosis (unpublished). Results haveshown clear effects on mortality in meningitis, astatistically non-significant effect in pericarditis (forwhich the analysis was very underpowered), and possibleshort-term clinical benefits in pulmonary tuberculosis.We aimed to assess the effect of steroids on mortalityattributable to all forms of tuberculosis across organsystems, with careful examination of results within andbetween organ systems, to attempt to provide someinsights into the best treatments and directions forfuture research.
Lancet Infect Dis 2013;
13: 223–237
Published Online
January 29, 2013
http://dx.doi.org/10.1016/
S1473-3099(12)70321-3
See Comment page 186
Division of Population Health
Sciences and Education, St
George’s, University of London,
London, UK
(Prof J A Critchley DPhil);
Institute of Health and Society,
Newcastle University,
Newcastle upon Tyne, UK
(F Young PhD); Department of
Public Health and Policy,
Institute of Psychology, Health
and Society, University of
Liverpool, Liverpool, UK
(L Orton PhD); and
International Health Group,
Liverpool School of Tropical
Medicine, Liverpool, UK
(Prof P Garner MD)
Correspondence to:
Prof Julia Critchley, Division of
Population Health Sciences and
Education, St George’s,University of London, Cranmer
Terrace, London SW17 0RE, UK

7/28/2019 Corticoide en Tb
http://slidepdf.com/reader/full/corticoide-en-tb 2/15
Articles
224 www.thelancet.com/infection Vol 13 March 2013
MethodsSearch strategy and selection criteriaWe did a systematic review and meta-analysis to assessthe effi cacy of steroids in the prevention of mortalityattributable to all forms of tuberculosis across organsystems. We attempted to identify all relevant trials,irrespective of language or publication status. Wesearched several electronic databases, covering all datesfrom the creation of each database up to Sept 6, 2012: theCochrane Infectious Diseases Group trial register, theCochrane Central Register of Controlled Trials, Medline(accessed via PubMed), Embase, and Literatura Latino-Americana e do Caribe em Ciências da Saúde (LILACS). Allsearches were designed and executed by a skilledinformation scientist. We contacted authors for furtherinformation or clarification when necessary, and con-
tacted authors of registered, unpublished trials in anattempt to identify studies that were in progress. Ourinitial search consisted of the terms “tuberculosis” and“corticosteroids” and related terms (including the namesof specific steroid drugs; appendix p 1). Each search termwas used in combination with a highly sensitive searchstrategy for the retrieval of trials developed by TheCochrane Collaboration.18 We also manually checked thereference lists of all the studies identified by the abovemethods and of relevant reviews. Our systematic reviewand meta-analysis is reported in accordance with thepreferred reporting items for systematic reviews andmeta-analyses (PRISMA) guidelines.19
Eligibility criteriaOur objective was to estimate the effect of adjunctivecorticosteroid use on mortality in patients with any formof tuberculosis. We included all relevant randomisedcontrolled trials or quasi-randomised controlled trials(clinical trials that used predictable methods of patientallocation such as alternate allocation) published beforeSept 6, 2012. We decided to include trials that were notrandomised because most trials on this subject are notrecent and were done before the methodologicaladvantages of randomisation were fully recognised.20
Trials that included people with any form of tuberculosis(defined clinically or microbiologically) were eligible.There were no restrictions on studies with respect to age
groups, settings, disease types, or coexistence of HIV orother illnesses. The interventions could be a cortico-steroid of any dose, duration, or mode of administration,compared with a placebo or no steroid. We includedcorticotropin because, although it is not a corticosteroid,it causes an increase in the body’s production and releaseof corticosteroids and thus works in the same way ascorticosteroid treatment. All comparison groups werealso treated with an antimicrobial combination regimenfor tuberculosis that was recognised internationally asappropriate at the time the trial was done.21 We includeddeath from all causes during treatment and up to12 months follow-up (or longer if data were available) as
an outcome. Trials were excluded only if they did notreport on mortality. The methods were defined inadvance in a protocol (appendix pp 2–8). The onlydeviation from the protocol was that we were not able toconsider other (morbidity) outcomes across all forms of tuberculosis.
Data extractionTwo investigators (JAC plus FY or LO) independentlychecked the citations retrieved by the search strategy. Theauthors, institutions, or journals were not masked fromthe investigators. Abstracts that did not provide enoughinformation with respect to the inclusion and exclusioncriteria were retrieved for assessment of the full text. Weobtained full versions of all potentially relevant papers, andeligibility was assessed with a form based on the inclusion
criteria. Two investigators (JAC plus FY or LO) alsoindependently assessed articles for eligibility and extracteddata with a piloted data extraction form. They crosschecked the data and settled discrepancies by discussion.We contacted seven study authors by letter or email to askfor additional details, although only one replied. Dataextracted included demographic characteristics (age, sex,and ethnic origin); period and geographical location of thestudy; method of diagnosis of tuberculosis; organ systemor systems affected; corticosteroid type, dose, and duration;antimicrobial treatment given; mortality from all causes;and details of any adverse events reported.
Risk of bias was assessed in accordance with thePRISMA recommendations. Two investigators (JAC plus
FY or LO) independently assessed the risk of bias of eachtrial in terms of generation of allocation sequence,allocation concealment, masking, and loss to follow-upand other exclusions. We classified generation of allo-cation sequence and allocation concealment as adequate,inadequate, or unclear.22 We classified follow-up as ad-equate if follow-up information was available for at least85% of participants. We described masking as unclear(not mentioned in the paper, likely to be open—ie, allparties aware of treatment), single (the allocatedintervention is masked from one of either theparticipants, care provider, or assessor—we specifywhich where possible), double (trial uses a placebo or adouble-dummy technique such that the participant and
either the care provider or assessor do not know whichtreatment is given), or triple (the allocated intervention ismasked from the patient, care provider, and outcomeassessors).
Statistical analysisWe analysed the data with RevMan (version 5.2). Weused the Mantel-Haenszel method to calculate riskratios with 95% CIs to summarise mortality acrosstrials. We assessed heterogeneity between the trials withthe χ² test with a 10% level of statistical significance andwith the I ² test. In the absence of substantialheterogeneity within or between different tuberculosis
See Online for appendix

7/28/2019 Corticoide en Tb
http://slidepdf.com/reader/full/corticoide-en-tb 3/15

7/28/2019 Corticoide en Tb
http://slidepdf.com/reader/full/corticoide-en-tb 4/15

7/28/2019 Corticoide en Tb
http://slidepdf.com/reader/full/corticoide-en-tb 5/15

7/28/2019 Corticoide en Tb
http://slidepdf.com/reader/full/corticoide-en-tb 6/15

7/28/2019 Corticoide en Tb
http://slidepdf.com/reader/full/corticoide-en-tb 7/15

7/28/2019 Corticoide en Tb
http://slidepdf.com/reader/full/corticoide-en-tb 8/15

7/28/2019 Corticoide en Tb
http://slidepdf.com/reader/full/corticoide-en-tb 9/15
Articles
www.thelancet.com/infection Vol 13 March 2013 231
organ systems, we estimated the pooled risk reductionin mortality by use of a fixed-effect model by tuberculosisorgan system and then across all forms of tuberculosis.We did a subgroup analysis according to whether thetreatment regimen contained rifampicin. Sensitivityanalyses excluded trials that were based on non-randomised methods of allocation, the small pulmonarytuberculosis trial23 that excluded deaths shortly afterrandomisation, and trials in HIV-positive patients. Wealso used funnel plots to examine any evidence of publication bias or other biases associated with trialsize. We attempted to summarise the incidence of anyserious adverse events (those defined by the trial authorsas serious or that necessitated a change in ordiscontinuation of treatment).
Role of the funding sourceThe sponsor of the study had no role in study design,data collection, data analysis, data interpretation, orwriting of the report. The corresponding author had fullaccess to all the data in the study and had finalresponsibility for the decision to submit for publication.
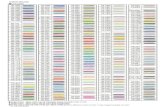
ResultsWe identified 41 trials (comprising 3560 patients whoreceived steroids and 2982 patients in control groups)that met our inclusion criteria, of which 18 were inpatients with pulmonary tuberculosis,23–41 nine were inpatients with meningitis,42–51 seven were in patients withpleurisy,52–58 six were in patients with pericarditis,59–64 and
one was in patients with peritonitis65
(table; figure 1). Most of the studies (23) were reported before 1990, andtherefore did not use modern antituberculosis treatmentregimens. All of the trials took place in hospitals—mostlymajor tertiary referral centres. Methodological qualityvaried, and was often not well reported. Most of thestudies did not report the details of allocationconcealment. Most were described as double-blind ortriple-blind, or had some outcomes masked from out-come assessors, but masking was not always adequatelydescribed (classified as unclear). Attrition rates weregenerally low (complete reporting of mortality is oftenbetter than for other outcomes), but trials were onaverage very small. In one trial,23 the investigator excluded
deaths that occurred in the first 12 h after randomisation(table); we did sensitivity analyses that first includedthese patients and then excluded the trial altogether.
The types of steroids used, and their doses and durationwere highly variable. Reporting of regimens used wasalso variable—not all trials described the tapering dosesin detail, or the precise duration of treatment. More thanhalf of the included trials (21 of 41) used prednisolone(almost all orally).25,26,29–31,34,38–42,49,50,52,53,55,56,59,62–64 Doses variedfrom 4 mg daily to 60 mg daily, and duration varied from30 days to 15 weeks. A further nine trials usedprednisone;27,28,33,35,37,43,54,58,61,65 doses varied from 0·75 mg/kgper day to 60 mg/day, and durations ranged from 9 to
17 weeks. Two studies used methylprednisolone; oneorally36 (48 mg/day, 4 weeks duration) and oneintravenously47 (1 g per day [if heavier than 50 kg] or20 mg/kg per day, for 5 days). Five trials,44–48 all in patientswith tuberculous meningitis, used dexamethasone. Thedoses and durations used in these studies were moreconsistent than in the trials that used other steroids,although these also showed substantial variation (dosesranged from 2·25 mg/day to 16 mg/day and durations
ranged from 4 to 8 weeks). Intravenous corticotropin wasgiven in five trials: three used doses of 200–300 mg perday;23,24,62 one27,28 used 60 international units every 4 days,tapered over 13 weeks; and one60 used a 16 h drip on days11–14 at 0·5 units/kg up to maximum of 50 units (unitswere not defined). Two trials used intravenoushydrocortisone (one60 at 4 mg/kg every 24 h; and one57
with a dose of 150–250 mg) and two used triamcinolone(one32 at 0·11 mg/kg, tapered over 10 weeks; and one 61 with a 200 mg dose of intrapericardial triamcinolonehexacetonide). Several trials used more than one type of steroid.27,28,47,60,61 In all these cases, the trialists themselvesor we combined data from both steroid arms since there
57 records identified throughdatabase searches
114 records screened
53 records excluded
61 full-text articles assessed for eligibility
20 full-text articles excluded8 case series2 studies in which all patients
received steroids2 studies for which we were unable
to contact the authors to verifyeligibility (both Russian language)
1 cross-over study1 review article1 included patients with diseases
other than tuberculosis1 had controls that were not
concurrent with cases1 used adjunctive thalidomide,
not steroid1 did not report numbers of patients1 trial was not randomised and had
very different numbers intreatment and control groups
1 compared two different steroids
41 studies included in qualitative synthesis
41 studies included in quantitative
synthesis (meta-analysis)
57 additional records identifiedthrough other sources
Figure 1: Study selection

7/28/2019 Corticoide en Tb
http://slidepdf.com/reader/full/corticoide-en-tb 10/15
Articles
232 www.thelancet.com/infection Vol 13 March 2013
Pulmonary
Angel et al24 (1960)
Bell et al25 (1960)
Bilaçeroğlu et al26 (1999)
British Tuberculosis Association27,28 (1961 and 1963)
De Alemquer23 (1955)
Halleck29 (1965)
Horne30 (1960)
Johnson et al31 (1965)
Keidan and Todd32 (1961)
Malik and Martin33 (1969)
Marcus et al34 (1962)
Mayanja-Kizza et al35 (2005)
McLean36 (1963)
Nemir et al37 (1967)
Park et al38 (1997)
Toppett et al39 (1990)
Tuberculosis Research Centre40 (1983)
Weinstein and Koler41 (1959)
Subtotal
Heterogeneity: χ²=10·48, df=9 (p=0·31); I²=14%. Test for overall effect: Z=1·30 (p=0·20)
Meningitis
Chotmongkol et al42 (1996)
Escobar et al43 (1975)
Girgis et al44 (1991)
Kumarvelu et al45 (1994)
Lardizabal and Rexas46 (1998)
Malhotra et al47 (2009)
O'Toole et al48 (1969)
Schoeman et al49 (1997)
Thwaites et al50/Török et al51 (2004/2011)
Subtotal
Heterogeneity: χ²=9·06, df=8 (p=0·34); I²=12%. Test for overall effect: Z=2·55 (p=0·01)
Pleurisy
Bang et al52 (1997)
Elliott et al53 (2004)
Galarza et al54 (1995)
Lee et al55 (1998)
Lee et al56 (1999)
Mathur et al57 (1960)
Wyser et al58 (1996)
Subtotal
Heterogeneity: NA. Test for overall effect: Z=0·44 (p=0·66)
Pericarditis
Hakim et al59 (2000)
Lepper and Spies et al60 (1963)
Reuter et al61 (2006)
Schrire62 (1959)
Strang et al63 (1987)
Strang et al64 (1988)
Subtotal
Heterogeneity: χ²=0·89, df=3 (p=0·83); I²=0%. Test for overall effect: Z=1·91 (p=0·06)
Peritonitis
Singh et al65 (1969)
Subtotal
Heterogeneity: NA. Test for overall effect: NA
Total (all organ systems)
Heterogeneity: χ²=22·43, df=23 (p=0·49); I²=0%. Test for overall effect: Z=3·35 (p=0·0008)
Test for subgroup differences: χ²=1·81, df=3 (p=0·61), I²=0%
Events n Events n
Steroid group Control group Risk ratio (95% CI) Weight
0
1
0
3
2
2
1
7
0
0
0
17
0
0
0
0
0
2
35
5
22
72
5
4
17
6
4
121
256
0
36
0
0
0
0
0
36
5
6
0
0
88
27
0
0
354
0
0
0
1
9
2
1
14
0
1
0
14
0
1
0
0
0
1
44
2
23
79
7
6
13
9
13
128
280
0
39
0
0
0
0
0
39
10
7
0
0
1116
44
0
0
407
Not estimable
3·07 (0·13–73·32)
Not estimable
3·08 (0·32–29·16)
0·21 (0·05–0·78)
0·51 (0·07–3·62)
1·03 (0·07–16·28)
0·48 (0·21–1·09)
Not estimable
0·35 (0·01–8·32)
Not estimable
1·23 (0·64–2·34)
Not estimable
0·34 (0·01–8·15)
Not estimable
Not estimable
Not estimable
1·92 (0·18–20·52)
0·77 (0·51–1·15)
2·59 (0·54–12·29)
0·86 (0·56–1·33)
0·85 (0·68–1·05)
0·75 (0·28–1·98)
0·67 (0·21–2·12)
0·64 (0·36–1·14)
0·73 (0·39–1·37)
0·26 (0·09–0·76)
0·93 (0·78–1·12)
0·85 (0·75–0·96)
Not estimable
0·92 (0·65–1·32)
Not estimable
Not estimable
Not estimable
Not estimable
Not estimable
0·92 (0·65–1·32)
0·50 (0·19–1·28)
0·85 (0·29–2·45)
Not estimable
Not estimable
0·79 (0·34–1·83)0·55 (0·25–1·24)
0·65 (0·41–1·01)
Not estimable
Not estimable
0·83 (0·74–0·92)
0·1%
0·2%
2·2%
0·6%
0·2%
3·4%
0·4%
3·3%
0·4%
0·2%
11·2%
0·5%
5·8%
19·6%
1·6%
1·4%
4·2%
2·1%
3·3%
30·8%
69·3%
9·3%
9·3%
2·4%
1·7%
2·5%3·6%
10·2%
100·0%
54
45
91
116
14
1108
87
52
8
46
49
93
10
58
17
15
261
51
2175
29
52
145
20
29
61
11
63
274
684
50
97
57
21
32
25
34
316
29
119
33
14
62105
362
23
23
3560
50
46
87
119
13
566
90
50
8
48
51
94
11
59
17
14
269
49
1641
30
47
135
21
29
30
12
54
271
629
33
97
60
19
50
25
36
320
29
118
24
14
67116
368
24
24
2982
10·2 5 200·05
Favours steroid Favours control
Figure 2: Prevention of
mortality with steroid use
for tuberculosis, stratified by
organ system affected
Error bars show 95% CIs. Risk
ratios and weights were
derived according to the
Mantel-Haenszel fixed effect
model. df=degrees of freedom.

7/28/2019 Corticoide en Tb
http://slidepdf.com/reader/full/corticoide-en-tb 11/15
Articles
www.thelancet.com/infection Vol 13 March 2013 233
were no significant differences in results for mortality orother reported outcomes.
Mortality was lower in patients who were given steroidsfor every included tuberculosis organ system (figure 2);the overall reduction in mortality with steroids was 17%(risk ratio [RR] 0·83, 95% CI 0·74–0·92). We noted nosignificant heterogeneity between trials within orbetween organ systems (I² within organ systems:pulmonary 14%, meningitis 12%, pericarditis 0% [I² could not be calculated for pleurisy]; between organsystems 0%). Funnel plot analysis did not show anyevidence of publication bias or other biases (appendixp 9). The sensitivity analysis that excluded non-randomised trials32,33,57,62,65 gave an almost identical result(since only one death occurred in any of the five non-randomised trials). De Alemquer’s23 small pulmonary
tuberculosis trial from the 1950s omitted six patientsrandomly assigned to study groups who all died within12 h of randomisation—four in the steroid group (of whom two apparently died before the start of steroidtreatment) and two in the control group. The death ratewas very high in this trial because of the severity of illness at recruitment. Reinstatement of these six patientsin a sensitivity analysis did not substantially affect thepoint estimate or 95% CI for the pulmonary tuberculosisstratum (RR before reinstatement 0·77, 0·51–1·15; RRafter reinstatement 0·78, 95% CI 0·54–1·14). Exclusionof the De Alemquer trial altogether, together withexclusion of the non-randomised trials, increased thepooled RR to 0·93 (0·60–1·44).
Adverse events from corticosteroid treatment of tuberculosis have been summarised in the relevant
Pulmonary
Bilaçeroğlu et al26 (1999)
Mayanja-Kizza et al35 (2005)
Park et al38 (1997)
Toppett et al39 (1990)
Tuberculosis Research Centre40 (1983)
Subtotal
Heterogeneity: NA. Test for overall effect: Z=0·62 (p=0·53)
Meningitis
Chotmongkol et al42 (1996)
Kumarvelu et al45 (1994)
Lardizabal and Rexas46 (1998)
Malhotra et al
47
(2009)Schoeman et al49 (1997)
Thwaites et al50/Török et al51 (2004/2011)
Subtotal
Heterogeneity: χ²=8·78, df=5 (p=0·12); I²=43%. Test for overall effect: Z=1·84 (p=0·07)
Pleurisy
Bang et al52 (1997)
Elliott et al53 (2004)
Galarza et al54 (1995)
Lee et al55 (1998)
Lee et al56 (1999)
Wyser et al58 (1996)
Subtotal
Heterogeneity: NA. Test for overall effect: Z=0·44 (p=0·66)
Pericarditis
Hakim et al
59
(2000)Reuter et al61 (2006)
Strang et al63 (1987)
Strang et al64 (1988)
Subtotal
Heterogeneity: χ²=0·58, df=2 (p=0·75); I²=0%. Test for overall effect: Z=1·98 (p=0·05)
Total (all organ systems)
Heterogeneity: χ²=12·61, df=10 (p=0·25); I²=21%. Test for overall effect: Z=2·23 (p=0·03)
Test for subgroup differences: χ²=3·23, df=3 (p=0·36), I²=7·1%
Events n Events n
Steroid group Control group Risk ratio (95% CI) Weight
0
17
0
0
0
17
5
5
4
174
121
156
0
36
0
0
0
0
36
50
8
8
21
230
0
14
0
0
0
14
2
7
6
1313
128
169
0
39
0
0
0
0
39
100
11
16
37
259
Not estimable
1·23 (0·64–2·34)
Not estimable
Not estimable
Not estimable
1·23 (0·64–2·34)
2·59 (0·54, 12·29)
0·75 (0·28–1·98)
0·67 (0·21–2·12)
0·64 (0·36–1·14)0·26 (0·09–0·76)
0·93 (0·78–1·12)
0·85 (0·72–1·01)
Not estimable
0·92 (0·65–1·32)
Not estimable
Not estimable
Not estimable
Not estimable
0·92 (0·65–1·32)
0·50 (0·19–1·28)Not estimable
0·79 (0·34–1·83)
0·55 (0·25–1·24)
0·61 (0·37–0·99)
0·85 (0·74–0·98)
5·3%
5·3%
0·7%
2·6%
2·3%
6·6%5·3%
48·8%
66·4%
14·8%
14·8%
3·8%
4·0%
5·8%
13·6%
100·0%
91
93
17
15
132
348
29
20
29
6163
274
476
50
97
57
21
32
34
291
2933
62
105
229
1344
87
94
17
14
129
341
30
21
29
3054
271
435
33
97
60
19
50
36
295
2924
67
116
236
1307
10·2 5 200·05
Favours steroid Favours control
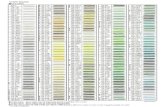
Figure 3: Subgroup analysis of trials that used rifampicin-containing antituberculosis regimens
Error bars show 95% CIs. Risk ratios and weights were derived according to the Mantel-Haenszel fixed effect model. df=degrees of freedom.

7/28/2019 Corticoide en Tb
http://slidepdf.com/reader/full/corticoide-en-tb 12/15
Articles
234 www.thelancet.com/infection Vol 13 March 2013
Cochrane reviews.15–17 Generally, adverse events havebeen poorly reported (eg, many trials only report thenumber of events but not the trial group in which theyoccurred). However, no difference has been reported inthe incidence of serious adverse events betweencorticosteroid and control groups. In one trial,40 steroidsgiven with a suboptimum antituberculosis treatmentregimen (in which rifampicin was not given and patientshad disease that was resistant to both streptomycin andisoniazid) resulted in an unfavourable response totreatment.
The results from trials that used rifampicin-containingantituberculosis regimens were analysed as a subgroup,since regimens with this drug are more effective thanolder regimens (figure 3). No trials assessed the use of rifampicin for tuberculous peritonitis, and only one
tuberculous pleurisy study53
that used rifampicinreported any deaths; therefore subgroup analyses werenot feasible for these organ systems. For pulmonarytuberculosis, only five of the 18 trials took place after theintroduction of rifampicin-containing regimens,26,35,38–40 and of these only one reported any deaths. 35 The RR of mortality from this one trial was 1·23 (95% CI 0·64–2·34).However, this trial was done in patients with pulmonarytuberculosis who were also infected with HIV. Thepooled RR for mortality from the earlier pulmonarytuberculosis trials that used non-rifampicin regimenswas 0·57 (0·34–0·97). After exclusion of the small trial23 in which all deaths shortly after randomisation had beenexcluded, the pooled RR from these early pulmonary
tuberculosis trials was 0·72 (0·40–1·29).For tuberculous meningitis and pericarditis, weidentified no substantial differences in the resultsstratified by rifampicin regimens. For tuberculousmeningitis, the pooled RR from three early trials43,44,48 thatused non-rifampicin regimens was 0·84 (0·70–1·01).The pooled RR from six trials42,45–47,49–51 that usedrifampicin-containing regimens was 0·85 (0·72–1·01).Similarly for tuberculous pericarditis, the pooled RRfrom two early trials60,62 that used non-rifampicinregimens was 0·85 (0·29–2·45), and the pooled RR fromfour more recent trials59,61,63,64 that used rifampicin-containing regimens was 0·61 (0·37–0·99).
Pooling the results of trials of rifampicin-containing
regimens only (21 trials, n=2651 patients [1344 whoreceived steroids and 1307 controls]) across all organsystems, the overall reduction in risk of mortality is verysimilar to that for all 41 trials (0·85, 95% CI 0·74–0·98, I ²21%; figure 3).
Three small, recent trials35,53,59 enrolled patients whowere infected with both tuberculosis (pulmonary tuber-culosis, tuberculous pleurisy, or tuberculous pericarditis)and HIV. No differences in mortality were detected inany of these trials, although all were underpowered forthis outcome (pulmonary tuberculosis RR 1·23, 95% CI0·64–2·34;35 tuberculous pleurisy 0·92, 0·65–1·32;53 andtuberculous pericarditis 0·50, 0·19–1·2859). Exclusion of
these three trials in a sensitivity analysis made littledifference to the overall pooled RR (0·81, 0·72–0·91) orthe RR for tuberculous pericarditis (0·69, 0·42–1·15), butthe risk reduction for pulmonary tuberculosis increasedand became significant (0·57, 0·34–0·97). Fortuberculous pleurisy, the trial with patients co-infectedwith HIV was the only one to report any events. Inanother trial in patients with tuberculous meningitis,about a third of enrolled patients were also infected withHIV, and the preplanned subgroup analysis showed nodifference in outcomes for patients co-infected withHIV.50 Investigators of another trial61 in patients withtuberculous pericarditis also reported no differences inoutcomes for patients infected with HIV compared withpatients without HIV infection, but this trial was small(n=57) and had substantial losses to follow-up.
DiscussionOverall, corticosteroids resulted in a significant andclinically important reduction in mortality, whatever theorgan group affected. The overall reduction in mortalityfrom steroid use was 17% (RR 0·83, 95% CI 0·74–0·92).Although effects on mortality have previously beenshown for tuberculous meningitis17 and pericarditis,16 there has been uncertainty with respect to pulmonarytuberculosis and other forms of extrapulmonarytuberculosis such as tuberculous pleurisy.15 The exactmechanisms of the benefit from steroids are not clear,but are related to the host response to the tuberculosispathogen (including excessive inflammation), and so
effects in one organ system might well be relevant toothers with respect to mortality outcomes. Recentresearch suggests that genetic variation at the LTA4H gene affects the development of mycobacterialpathogenesis66,67 and that corticosteroids could affecttuberculosis outcomes through interruption of myco-bacterial pathogenesis mechanisms, rather than actingonly by suppressing the immune response. Thissuggestion lends support to the idea that an effect mightbe present across all organ systems.
The key strengths of our review include the com-prehensive search for trials irrespective of language ordate of publication. We have also addressed the benefit of steroids for all forms of tuberculosis. This point is
especially important for pulmonary tuberculosis, aboutwhich the evidence is older and has been largely ignoredin recent guidelines and research prioritisations.68 Theuse of rifampicin was a major breakthrough inantituberculosis chemotherapy; several randomisedcontrolled trials done about 30–40 years ago had highcure rates after short treatment periods, even when drugswere given intermittently.69 We therefore also did asubgroup analysis for trials that used rifampicin-basedregimens.
The limitations of our review relate to the trials, whichwere generally small and done some years ago, whenreporting of methods was less stringent than it is

7/28/2019 Corticoide en Tb
http://slidepdf.com/reader/full/corticoide-en-tb 13/15
Articles
www.thelancet.com/infection Vol 13 March 2013 235
nowadays. Nevertheless, almost all of the trials includedwere randomised, and had little loss to follow-up for themortality outcome. Most were also masked. Few of thetrials were adequately powered and many did not usemodern combination antituberculosis therapies, par-ticularly the more effective rifampicin-containing regi-mens; this limitation was especially true for the trials inpulmonary tuberculosis. No evidence from other organsystems (particularly tuberculous meningitis andpericarditis) suggested that the recent trials differedsubstantially in terms of their mortality outcomescompared with the older trials. No statistical hetero-geneity was evident between or within affected organsystems, although the statistical power to detect hetero-geneity was low for pulmonary tuberculosis since fewdeaths were reported in most of the studies.
Most of the trials took place before the HIV era, and inrecent trials people with HIV have often been excluded,which means that we have been unable to assess effi cacyin the subgroup of tuberculosis patients who are infectedwith HIV. Similarly, most trials were done before the eraof multidrug-resistant tuberculosis. As such, we iden-tified no convincing evidence that corticosteroids affectoutcomes in drug-resistant tuberculosis, although onetrial40 showed a worse outcome with prednisolone only ina subgroup with a suboptimum (non-rifampicin)treatment regimen and drug resistance to bothstreptomycin and isoniazid.
The results for trials in pulmonary tuberculosis,although not statistically significant, are consistent with
a reduction in mortality with steroids. In the overallcontext of all trials of steroids in tuberculosis and nodetectable heterogeneity, this effect is important.
We have considered only one outcome—mortality—inour meta-analysis, since this is the only outcome that canbe appropriately summarised across different affectedorgan systems. In our recent systematic review of pulmonary tuberculosis (unpublished), we identifiedsome evidence of statistically significant short-termclinical and radiological benefits from adjunctive steroidtreatment, including substantial reduction in time todefervescence and in time spent in hospital, from aminority of the studies included (most of the trials didnot report on these outcomes). However, in the longer
term there were no significant differences in radiographicor clinical outcomes. New clinical trials of corticosteroidsin patients with pulmonary tuberculosis (both infectedand uninfected with HIV) are needed to assess whetherthese clinical benefits remain in the era of modern anti-tuberculosis chemotherapy. Based on the event rate inthe existing trials for pulmonary tuberculosis, at least10 000 patients would be needed for a new trial to beadequately powered for mortality.
Not many serious side-effects were reported, and theirfrequency did not differ substantially with adjunctivesteroid use; however, adverse events are notoriouslypoorly reported in trials,70 particularly in older studies. If
more widespread use of adjunctive corticosteroids isadvocated, the rapid rise of drug-resistant tuberculosisworldwide and the inability of most laboratories to detectdrug resistance within a clinically useful timeframe is asafety concern.
The benefit-to-risk ratio from adjunctive corticosteroiduse thus needs to be more accurately assessed in newtrials and cohort studies and by use of reporting systemsfor adverse events. Our analysis suggests a benefit fromsteroids that seems to be consistent across organsystems. Even in the absence of contemporary data forrifampicin-based regimens for treatment of pulmonarytuberculosis, if this result shows a true systemic effectacross organ systems, it provides indirect evidence tosuggest that steroids could be of benefit in pulmonarytuberculosis.
ContributorsJAC obtained data, developed methods, did analyses, and wrote theprotocol and the report. FY and LO obtained data and commented onanalyses and the report. PG conceived the research question, helped todevelop the methods and protocol, and helped with analyses anddrafting of the report.
Conflicts of interest
We declare that we have no conflicts of interest.
Acknowledgments
This research was partly funded by the UK Department for InternationalDevelopment (PO 5242). We thank Mike Clarke for comments oninterpretation and Vittoria Lutje, who did the electronic searches.
References 1 WHO. Global tuberculosis report 2012. Geneva: World Health
Organization, 2012.
2 Raviglione M, Marais B, Floyd K, et al. Scaling up interventions to
achieve global tuberculosis control: progress and newdevelopments. Lancet 2012; 379: 1902–13.
3 Migliori GB, Dara M, de Colombani P, Kluge H, Raviglione MC.Multidrug-resistant tuberculosis in Eastern Europe: still on theincrease? Eur Respir J 2012; 39: 1290–01.
4 WHO. Tuberculosis (fact sheet no 104). Geneva: World HealthOrganization. http://www.who.int/mediacentre/factsheets/fs104/en/ (accessed Feb 5, 2011).
5 Creswell J, Raviglione M, Ottmani S, et al. Tuberculosis andnoncommunicable diseases: neglected links and missedopportunities. Eur Respir J 2011; 37: 1269–82.
6 Stevenson CR, Critchley JA, Forouhi NG, et al. Diabetes and therisk of tuberculosis: a neglected threat to public health? Chronic Illn 2007; 3: 228–45.
7 Stevenson CR, Forouhi NG, Roglic G, et al. Diabetes andtuberculosis: the impact of the diabetes epidemic on tuberculosisincidence. BMC Public Health 2007; 7: 234.
8 Bergrem H, Refvem OK. Altered prednisolone pharmacokinetics
in patients treated with rifampicin. Acta Med Scand 1983;213: 339–43.
9 Edwards OM, Galley JM, Courtenay-Evans RJ, Hunter J, Tait AD.Changes in cortisol metabolism following rifampicin therapy.Lancet 1974; 304: 549–51.
10 Kaojarern S, Supmonchai K, Phuapradit P, Mokkhavesa C,Krittiyanunt S. Effect of steroids on cerebrospinal fluid penetrationof antituberculous drugs in tuberculous meningitis.Clin Pharmacol Ther 1991; 49: 6–12.
11 Sarma GR, Kailasam S, Nair NG, Narayana AS, Tripathy SP. Effectof prednisolone and rifampin on isoniazid metabolism in slow andrapid inactivators of isoniazid. Antimicrob Agents Chemother 1980;18: 661–66.
12 Wagay AR, Singhal KC, Bhargava R. Alteration in the levels of pyrazinamide in pleural fluid following simultaneousadministration of prednisolone in patients of tubercular pleuraleffusion. Indian J Physiol Pharmacol 1990; 33: 259–62.

7/28/2019 Corticoide en Tb
http://slidepdf.com/reader/full/corticoide-en-tb 14/15
Articles
236 www.thelancet.com/infection Vol 13 March 2013
13 Dooley DP, Carpenter JL, Rademacher S. Adjunctive corticosteroidtherapy for tuberculosis: a critical reappraisal of the literature.Clin Infect Dis 1997; 25: 872–87.
14 Cisneros JR, Murray KM. Corticosteroids in tuberculosis.Ann Pharmacother 1996; 30: 1298–303.
15 Engel ME, Matchaba PT, Volmink J. Corticosteroids for tuberculouspleurisy. Cochrane Database Syst Rev 2007; 4: CD001876.
16 Mayosi BM, Ntsekhe M, Volmink JA, Commerford PJ.Interventions for treating tuberculous pericarditis.Cochrane Database Syst Rev 2002; 4: CD000526.
17 Prasad K, Singh MB. Corticosteroids for managing tuberculousmeningitis. Cochrane Database Syst Rev 2008; 1: CD002244.
18 Lefebvre C, Manheimer E, Glanville J. Chapter 6: searching forstudies. In: Higgins JPT, Green S, eds. Cochrane handbook forsystematic reviews of interventions, version 5.0.1. Oxford: TheCochrane Collaboration, 2011.
19 Moher D, Liberati A, Tetzlaff J, Altman DG, The Prisma Group.Preferred reporting items for systematic reviews and meta-analyses:the PRISMA statement. PLoS Med 2009; 6: e1000097.
20 Odgaard-Jensen J, Vist GE, Timmer A, et al. Randomisation toprotect against selection bias in healthcare trials.
Cochrane Database Syst Rev 2011; 4: MR000012. 21 American Thoracic Society, Centers for Disease Control and
Prevention, Infectious Diseases Society of America. Treatment of tuberculosis. MMWR Morb Mortal Wkly Rep 2003; 52: 1–77.
22 Jüni P, Altman DG, Egger M. Systematic reviews in healthcare:assessing the quality of controlled clinical trials. BMJ 2001;323: 42–46.
23 De Alemquer M. Traitement de la tuberculose pulmonaire inarticulo mortis par la cortisone associée aux antibiotiques.Acta Tuberc Scand 1955; 31: 356–66.
24 Angel JH, Chu LS, Lyons HA. Corticotropin in the treament of tuberculosis. A controlled study. Arch Intern Med 1961; 108: 353–69.
25 Bell WJ, Brown PP, Horn DW. Prednisolone in the treatment of acute extensive pulmonary tuberculosis in West Africans. Tubercle 1960; 41: 341–51.
26 Bilaçeroğlu S, Perim K, Büyükşirin M, Celikten E. Prednisolone:a beneficial and safe adjunct to antituberculosis treatment?Int J Tuberc Lung Dis 1999; 3: 47–52.
27 Research Committee of the British Tuberculosis Association. Trialof corticotrophin and prednisone with chemotherapy in pulmonarytuberculosis: a two-year radiographic follow-up. Tubercle 1963;44: 484–86.
28 Research Committee of the British Tuberculosis Association. A trialof corticotrophic and prednisone with chemotherapy in pulmonarytuberculosis. Tubercle 1961; 42: 391–412.
29 Halleck S. Prednisolone in the treatment of pulmonarytuberculosis. A United States Public Health Service TuberculosisTherapy Trial. Am Rev Respir Dis 1965; 91: 329–38.
30 Horne NW. Prednisolone in treatment of pulmonary tuberculosis:a controlled trial. Final report to the Research Committee of theTuberculosis Society of Scotland. BMJ 1960; 2: 1751–56.
31 Johnson JR, Taylor BC, Morrissey JF, Jenne JW, MacDonald FM.Corticosteroids in pulmonary tuberculosis. Am Rev Respir Dis 1965;92: 376–91.
32 Keidan SE, Todd RM. Triamcinolone in primary pulmonarytuberculosis: a controlled trial. Lancet 1961; 278: 1224–27.
33 Malik SK, Martin CJ. Tuberculosis corticosteroid therapy andpulmonary function. Am Rev Respir Dis 1969; 100: 13–18.
34 Marcus H, Yoo O, Akyol T, Williams MJ. A randomized study of theeffects of corticosteroid therapy on healing of pulmonarytuberculosis as judged by clinical, roentgenographic andphysiologic measurements. Am Rev Respir Dis 1962; 88: 55–64.
35 Mayanja-Kizza H, Jones-Lopez E, Okwear A, et al. Immunoadjuvantprednisolone therapy for HIV-associated tuberculosis: a phase 2clinical trial in Uganda. J Infect Dis 2005; 191: 856–65.
36 McLean RL. The role of adrenocorticotrophic andadrenocorticosteroid hormones in the treament of tuberculosis.Ann NY Acad Sci 1963; 106: 130–47.
37 Nemir RL, Cardona J, Vaziri F, Toledo R. Prednisone as an adjunctin the chemotherapy of lymph node bronchial tuberculosis inchildhoon: a double blind study. II. Further term observation.Am Rev Respir Dis 1967; 95: 402–10.
38 Park IW, Choi BW, Hue SH. Prospective study of corticosteroid asan adjunct in the treatment of endobronchial tuberculosis in adults.Respirology 1997; 2: 275–81.
39 Toppet M, Malfroot A, Derde MP, Toppet V, Spehl M, Dab I.Corticosteroids in primary tuberculosis with bronchial obstruction.Arch Dis Child 1990; 65: 1222–26.
40 Tuberculosis Research Centre. Study of chemotherapy regimens of 5 and 7 months’ duration and the role of corticosteroids in thetreatment of sputum-positive patients with pulmonary tuberculosisin South India. Tubercle 1983; 64: 73–91.
41 Weinstein HJ, Koler JJ. Adrenocorticosteroids in the treatment of tuberculosis.N Engl J Med 1959; 260: 412–17.
42 Chotmongkol V, Jitpimolmard S, Thavornpitak Y. Corticosteroid intuberculous meningitis. J Med Assoc Thai 1996; 79: 83–90.
43 Escobar JA, Belsey MA, Dueñas A, Medina P. Mortality fromtuberculous meningitis reduced by steroid therapy. Pediatrics 1975;56: 1050–55.
44 Girgis NI, Farid Z, Kilpatrick ME, Sultan Y, Mikhail IA.Dexamethasone adjunctive treatment for tuberculous meningitis.Pediatr Infect Dis J 1991; 10: 179–83.
45 Kumarvelu S, Prasad K, Khosla A, Behari M, Ahuja GK.
Randomized controlled trial of dexamethasone in tuberculousmeningitis. Tuber Lung Dis 1994; 75: 203–07.
46 Lardizabal D, Rexas A. Dexamethasone as an adjunctive therapy inadult patients with probable TB meningitis stage II and III: an openrandomised controlled trial. Philipp J Neurol 1998; 4: 4–10.
47 Malhotra HS, Garg RK, Singh MK, Agarwal A, Verma R.Corticosteroids (dexamethasone versus intravenousmethylprednisolone) in patients with tuberculous meningitis.Ann Trop Med Parasitol 2009; 103: 625–34.
48 O’Toole RD, Thornton GF, Mukherjee MK, Nath RL.Dexamethasone in tuberculous meningitis: relationship of cerebrospinal fluid effects to therapeutic effi cacy. Ann Intern Med 1969; 70: 39–48.
49 Schoeman JF, Van Zyl LE, Laubscher JA, Donald PR. Effect of corticosteroids on intracranial pressure, computed tomographicfindings, and clinical outcome in young children with tuberculousmeningitis. Pediatrics 1997; 99: 226–31.
50 Thwaites GE, Bang ND, Dung NH, et al. Dexamethasone for the
treatment of tuberculosis meningitis in adolescents and adults.N Engl J Med 2004; 351: 1741–51.
51 Török ME, Nguyen DB, Tran TH, et al. Dexamethasone andlong-term outcome of tuberculous meningitis in Vietnamese adultsand adolescents. PLoS One 2011; 6: e27821.
52 Bang JS, Kim MS, Kwak SM, Cho CH. Evaluation of steroid therapyin tuberculous pleurisy: a prospective, randomized study.Tuberc Respir Dis 1997; 44: 52–58.
53 Elliott AM, Luzze H, Quigley MA, et al. A randomized,double-blind, placebo-controlled trial of the use of prednisolone asan adjunct to treatment in HIV-1 associated pleural tuberculosis.
J Infect Dis 2004; 190: 869–78.
54 Galarza I, Cañete C, Granados A, Estopà R, Manresa F. Randomisedtrial of corticosteroids in the treatment of tuberculous pleurisy.Thorax 1995; 50: 1305–07.
55 Lee C-H, Wang W-J, Lan R-S, Tsai Y-H, Chiang Y-C. Corticosteroidsin the treatment of tuberculous pleurisy. A double-blind,placebo-controlled, randomized study. Chest 1988; 94: 1256–59.
56 Lee BH, Jee HS, Choi JC, et al. Therapeutic effect of prednisolonein tuberculous pleurisy—a prospective study for the prevention of the pleural adhesion. Tuberc Respir Dis 1999; 46: 481–88.
57 Mathur KS, Prasad R, Mathur JS. Intrapleural hydrocortisone intuberculous pleural effusion. Tubercle 1960; 41: 358–62.
58 Wyser C, Walzl G, Smedema JP, Swart F, van Schalkwyk EM,van de Wal BW. Corticosteroids in the treatment of tuberculouspleurisy. A double-blind, placebo-controlled, randomized study.Chest 1996; 110: 333–38.
59 Hakim JG, Ternouth I, Mushangi E, Siziya S, Robertson V, Malin A.Double blind randomised placebo controlled trial of adjunctiveprednisolone in the treatment of effusive tuberculous pericarditis inHIV seropositive patients. Heart 2000; 84: 183–88.
60 Lepper MH, Spies HW. The present status of the treatment of tuberculosis of the central nervous system. Ann NY Acad Sci 1963;106: 106–23.

7/28/2019 Corticoide en Tb
http://slidepdf.com/reader/full/corticoide-en-tb 15/15
Articles
61 Reuter H, Burgess LJ, Louw VJ, Doubell AF. Experience withadjunctive corticosteroids in managing tuberculous pericarditis.Cardiovasc J S Afr 2006; 17: 233–38.
62 Schrire V. Experience with pericarditis at Groote Schuur Hospital,Cape Town: an analysis of 160 cases studied over a six-year period.S Afr Med J 1959; 33: 810–17.
63 Strang JIG, Kakaza HHS, Gibson DG, Girling DJ, Nunn AJ, Fox W.Controlled trial of prednisolone as adjuvant in treatment of tuberculous constrictive pericarditis in Transkei. Lancet 1987;330: 1418–22.
64 Strang JIG, Kakaza HHS, Gibson DG, et al. Controlled clinical trialof complete open surgical drainage and of prednisolone intreatment of tuberculous pericardial effusion in Transkei. Lancet 1988; 332: 759–64.
65 Singh MM, Bhargava AN, Jain KP. Tuberculous peritonitis—an evaluation of pathogenetic mechanisms, diagnostic proceduresand therapeutic measures. N Engl J Med 1969; 281: 1091–94.
66 Tobin DM, Vary JC Jr, Ray JP, et al. The lta4h locus modulatessusceptibility to mycobacterial infection in zebrafish and humans.Cell 2010; 140: 717–30.
67 Tobin DM, Roca FJ, Oh SF, et al. Host genotype-specific therapiescan optimize the inflammatory response to mycobacterialinfections. Cell 2012; 148: 434–46.
68 WHO. Treatment of tuberculosis guidelines, 4th edn. Geneva:World Health Organization, 2010.
69 Fox W, Ellard GA, Mitchison DA. Studies on the treatment of tuberculosis undertaken by the British Medical Research Counciltuberculosis units, 1946–1986, with relevant subsequentpublications. Int J Tuberc Lung Dis 1999; 3 (10 suppl 2): S231–79.
70 Golder S, Loke YK, Bland M. Meta-analyses of adverse effects dataderived from randomised controlled trials as compared toobservational studies: methodological overview. PLoS Med 2011;8: e1001026.