Coronary Heart #1
40
coronaryheart.com Using Magnetic Fields to fix Atrial Fibrillation “Especially for Cardiac Cath, EP, and Non-Invasive Departments” June / July 06 International Double Issue EDUCATION, CONFERENCES + more... Medtronic Endeavor DES Product Focus Lab Staff Performing Angiograms E M P L O Y M E N T LAB VISITS Epworth Hospital, Australia East Surrey Hospital, UK UK Australia New Zealand Special Feature
-
Upload
cardiologyhd -
Category
Documents
-
view
217 -
download
2
description
June/July 2006 Edition
Transcript of Coronary Heart #1

coronaryheart.com
Using Magnetic Fields to fi x Atrial Fibrillation
“Especially for Cardiac Cath, EP, and Non-Invasive
Departments”
June / July 06 International Double IssueJune / July 06 International Double Issue
EDUCATION,CONFERENCES
+ more...
Medtronic Endeavor DES Product Focus
coronaryheart.com
Lab Staff Performing Angiograms
EMP
LO
YMENT
LAB VISITSEpworth Hospital, AustraliaEast Surrey Hospital, UK
UK
Australia
New Zealand
Special Feature

www.siemens.com/medical
M-Z
91
7-1
-76
00 Proven Outcomes in Cardiology. Caring for
more patients, over a longer period of time, with
fewer resources. Impossible? On the contrary: We can
prove it. With integrated solutions that create a seamless
cardiology workflow. Where images and data are retrieved
instantaneously. Where cutting-edge technology enables
absolute precision. Where clinicians are free to provide
the best care possible. These are the Proven Outcomes
that are transforming the delivery of health care. Today.
We see a way to reduce cardiac cath lab reportturnaround times from 48 hours to 15 minutes
Proven OutcomesHelping cardiologists make 24 hours work like 48.
Siemens Medical Solutions that help
Results may vary. Data on file.
98257_M-Z917_A4_eng.qxd 17.05.2006 13:49 Uhr Seite 1

CONTENTS
ContentsCORONARYHEART
June / July 2006
CORONARY HEART ™ 3
Administrators Managers Cardiologists Nurses Radiographers Physiologists Echocardiographers
04 Welcome Editorial
05 Latest News‘April - May 2006’
09 Recent News‘Jan - Apr 2006’
14 Product Focus‘Medtronic Endeavor’
15 Special Feature‘Coronary Angiography Technician’
18 Australia Lab Visit‘Epworth Hospital’
22 UK Lab Visit‘East Surrey Hospital’
25 EP Education‘Wolff Parkinson White Syndrome’
30 Radiographer Education‘Cath Lab Angles’
32 Conferences‘Plan your holidays around some of these conferences’
36 CardiologyLanguages‘Learn German’
38 Employment‘Make a new start from one of our job listings’
34 Global Heart Reports‘Latest cardiac health reports from around the world’
35 Healthy Heart‘Our chef shows you how to cook healthily’
04 Welcome
THIS EDITION
© Philips
www.siemens.com/medical
M-Z
91
7-1
-76
00 Proven Outcomes in Cardiology. Caring for
more patients, over a longer period of time, with
fewer resources. Impossible? On the contrary: We can
prove it. With integrated solutions that create a seamless
cardiology workflow. Where images and data are retrieved
instantaneously. Where cutting-edge technology enables
absolute precision. Where clinicians are free to provide
the best care possible. These are the Proven Outcomes
that are transforming the delivery of health care. Today.
We see a way to reduce cardiac cath lab reportturnaround times from 48 hours to 15 minutes
Proven OutcomesHelping cardiologists make 24 hours work like 48.
Siemens Medical Solutions that help
Results may vary. Data on file.
98257_M-Z917_A4_eng.qxd 17.05.2006 13:49 Uhr Seite 1
East Surrey Hospital Cath Lab VisitEast Surrey Hospital Cath Lab VisitPage: 22
Ambient Experience Cath LabAmbient Experience Cath LabPage: 9

W elcome to the fi rst edition of Coronary Heart™, being distributed to virtually all cardiac catheterisation labs, electrophysiology labs, and
non-invasive departments in the UK, Australia, and New Zealand. Th e aim of this and future editions of Coronary Heart™ is to provide managers and staff with the latest product / medical news, and techniques employed by other departments around the world. Many cardiologists have also shown great interest in this publication as a refreshing alternative.
In order to become one of the most popular cardiology departmental magazines in the world, we require interesting articles from you related to your fi eld in cardiology. Tell us about the techniques your department uses, the studies you have completed, or just contact us to do a review of your department.
Th e issue you are now reading is a combined June / July Double Issue, due to last minute events beyond our control involving our fi rst Printer and Web Design fi rm. Th e challenges faced are now solved with the employment of a more reliable and professional Printer (Prometheus Press), and the completion of our website. And now with a committed team of editors, Coronary Heart™ is at last open for business.
Th e main edition (such as this) will be released bi-monthly, with a separate Recruitment Only edition being distributed on alternate months. Th e next edition released in August will be a Main edition.
Coronary Heart™ is an independent publication by Coronary Heart Publishing and is not affi liated with any organisation or association.
WELCOME
Welcome Editorial
Coronary Heart Publishing Ltd145 - 157 St John Street
London, EC1V 4PYUnited Kingdom
Phone: +44 (0) 207 788 7967Fax: +44 (0) 207 160 9334
Visit us online at www.coronaryheart.com
Director/Chief EditorTim Larner
Clinical EditorDr Rodney Foale (UK)
Consulting EditorsDr Richard Edwards (UK)
Ian Wright (UK)
ADVERTISING
Media kits are available online
CIRCULATION
460 Departments in the UK, Australia, and New Zealand
+ over 60 Industry Professionals
Copyright 2006 by Coronary Heart Publishing Ltd. All rights reserved.
Material may only be reproduced by prior arrangement and with due acknowledgment of
Coronary Heart Publishing.Th e publication of an advertisement or product
review does not imply that a product is recommended by Coronary Heart Publishing Ltd.
Disclaimer:Coronary Heart™ should never be regarded as an authoritative peer reviewed medical journal. Coronary Heart™ has been designed as a guide only, to inform readers who work in the cardiology environment about latest news stories and the diff erent techniques used by others around the world. Whilst all care is taken in reviewing articles obtained from various companies and contributors, it is not possible to confi rm the accuracy of all statements. Th erefore it is the reader’s responsibility that any advice provided in this publication should be carefully checked themselves, by either contacting the companies involved or speaking to those with skills in the specifi c area. Readers should always recheck claims made in this publication before employing them in their own work environment. Opinions expressed by contributors are their own and not necessarily those of their institution, Coronary Heart Publishing Ltd or the editorial staff .
Register Online to get your own
free copy
Tim LarnerDirector, Chief Editor
elcome to the fi rst edition of Coronary Heart™, being distributed to virtually all cardiac catheterisation labs, electrophysiology labs, and
non-invasive departments in the UK, Australia, and New Zealand. Th e aim of this and future editions of Coronary Heart™ is to provide managers and staff with the latest product / medical news, and techniques employed by other departments around the world. Many cardiologists have also shown great interest in this publication as a refreshing alternative.
elcome to the fi rst edition of Coronary Heart™, being distributed to virtually all cardiac catheterisation labs, electrophysiology labs, and
non-invasive departments in the UK, Australia, and New Zealand. Th e aim of this and future editions of Coronary Heart™ is to provide managers and staff with the latest product / medical news, and techniques employed by other departments around the world. Many cardiologists have also shown great interest in this publication as a refreshing alternative.
Tim�
Clinical Editor
Dr Rodney Foale, FRCP. FACC. FESC. FCSANZ.Clinical Director, Surgery, Cardiovascular Sciences and Critical Care. SMHT.
COVER PHOTO (from left): Smitha Sivasdasan, Kate Reed, & Paula Gontan, from Epworth Hospital Cath Lab, Melbourne, Australia. Photo by Catriona McRoy.
4 CORONARY HEART ™

LATEST NEWS
Latest News EXPRESS READ
GE Releases New Laptop Size Ultrasound Series
GE is introducing four new clinically specialized ultrasound systems to address
healthcare providers’ growing demand for sophisticated, real-time imaging at the point of care. GE’s Compact Series is a new and revolutionary line of ultrasound products that places the power and imaging capabilities of a high-performance, 400-pound system into a laptop-size design.
Visit www.gehealthcare.com for more information
St Jude Gain FDA & CE Mark Approval For EP Products
St Jude Medical announced US FDA approval of its Safi re™ Ablation Catheter, and FDA
clearance and European CE Mark for its Inquiry™ Optima™ PLUS Steerable Diagnostic Catheter.
Visit www.sjm.com for more information
Cardiac Systems with Distance Wireless Telemetry
Medtronic announced FDA approval of the Concerto™/Virtuoso™
line of implantable cardiac devices, Medtronic’s next generation of cardiac rhythm disease management products.
Th e Concerto cardiac resynchronization therapy-defi brillator (CRT-D) and Virtuoso implantable cardioverter defi brillator (ICD) are the fi rst implantable cardiac devices available with Medtronic’s proprietary Conexus™ Wireless Telemetry, developed using the Medical Implant Communications Service (MICS, 402-405 MHz). Using the MICS band enables reliable communication between the implanted device and clinician programmers and patient home
monitoring units.
Advantages: At implant, there is no need for the programmer head to enter the sterile implant fi eld, and in-offi ce visits may be simplifi ed when they’re needed, as the physician can interrogate patients’ devices via wireless telemetry without the need for surface electrodes.
Visit www.medtronic.com for more information
BIOTRONIK Release Pacemaker to Last 11+ Years
BIOTRONIK has introduced to the market the Talos pacemaker in combination
with Setrox S lead off ering longevity greater than 11 years due to its energy-effi cient technology.
Consultant Cardiologist Dr. David Lefroy, Lead Clinician for Cardiac Electrophysiology & Pacing in the
Directorate of Cardiac Sciences at the Hammersmith Hospitals in London, UK, was the Physician responsible for the fi rst worldwide implant of the Talos.
Dr. Lefroy stated, “A system of such longevity can be a great benefi t to both patients and the NHS. Quite a few patients need to undergo several pacemaker implant procedures over the decades for device changes. For the aff ected patient, this is often something of a stressful situation, and for the health care system, an increasingly expensive one.”
Visit www.biotronik.com for more information
EXPRESS READEXPRESS READEXPRESS READ
informationpacemaker implant procedures over informationpacemaker implant procedures over
CORONARY HEART ™ 5

LATEST NEWS
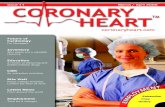
Latest NewsMagnetically Guided Catheter Zaps Atrial Fibrillation
Robotic device appears to be more precise than conventional catheter ablation devices
A remotely-controlled catheter device guided by magnetic fi elds provides a safe and
practical method for delivering radio frequency ablation treatment in the hearts of patients with atrial fi brillation, according to a new study in the April 4, 2006, issue of the Journal of the American College of Cardiology. “Based on our experience with remote navigation and ablation technology, a new era in interventional electrophysiology is beginning as magnetic, very soft catheters can be navigated in the heart more precisely and safely than manual catheters without risk of major complications, even in less experienced centres,” said Carlo Pappone, M.D., Ph.D. from the Department of Electrophysiology, San Raff aele University Hospital in Milan, Italy.
Atrial fi brillation is an abnormal heart rhythm in which the upper chambers of the heart fl utter, and do not pump blood normally. If the condition cannot be managed with medications, some patients are treated with radio frequency ablation. Th e technique uses a high energy pulse to destroy a small area of heart muscle cells, in order to prevent them from conducting nerve signals that trigger fi brillation.
Typically the radio frequency pulse is emitted by from the tip of a catheter threaded through blood vessels into the heart until it is positioned next to the target area. Conventional catheters are somewhat stiff , so they can be pushed and pulled through blood vessels, and their tips can be curled and pointed by an operator standing by the patient. Th e device tested in this trial uses a very soft, limp tip that has a magnet on the end. Rather than manually pointing the catheter tip, the operator of this device uses a computer to control a magnetic fi eld that robotically moves the catheter
tip. Th e principle is the same as a compass needle pointing to magnetic north; allowing this device to steer the magnetic catheter in three dimensions to a target visualized on 3-D scans of the patient’s heart.
“Catheter ablation for atrial fi brillation is now an important treatment for this common disorder, but the current strategy of manual catheter manipulation is highly operator-dependent, with a long and variable learning curve and a great potential for both ineffi cacy and complications
Th e Siemens AXIOM Artis dFC™ with the Stereotaxis Niobe® Magnetic Navigation System
6 CORONARY HEART ™

Latest News LATEST NEWS
in inexperienced hands. Robotic navigation may increase the ability of inexperienced operators to perform this procedure easily and safely, as it is most dependent on a well-trained team rather than on a single operator,” Dr. Pappone said.
Since catheter procedures of this type require frequent use of X-rays to track the location of the target and the catheter tip, another advantage of remote navigation is that the operator can work from a shielded control room, rather than having to stand next to the
patient for several hours while wearing protective lead aprons.
Th is fi rst trial of the robotic magnetic navigation system in patients with atrial fi brillation involved 40 participants whose conditions were not adequately controlled by medication. After encountering some diffi culties in the fi rst three patients, the researchers said the remaining procedures went smoothly. In all, the catheter tip was successfully guided by magnetic navigation to the target and radio frequency ablation was applied in 38 of the 40 study participants. Th ere were no reported complications during the procedures.
“Based on our results, we believe that incorporation of remote navigation and ablation in the electrophysiology laboratory may represent a true revolution regardless of age and experience of the operators leading to a seismic change in electrophysiologic paradigms for many laboratories worldwide. People always have had a love/hate relationship with robots, but this psychological barrier must be overcome. After performing more than 10,000 procedures with manually defl ectable catheters, I have become enthusiastic for this emerging fi eld,” Dr. Pappone said.
E. Kevin Heist, M.D., Ph.D. from Massachusetts General Hospital in Boston, who was not connected with this study, said even though catheter ablation is more successful than medical treatment for atrial fi brillation, the conventional procedure can be long and diffi cult.
“Catheter ablation as currently practiced with hand held, manually defl ected catheters is a long procedure, typically 3 to 5 hours, has a long learning curve, and has a signifi cant risk of procedural complications and of recurrent atrial fi brillation after the
procedure. Robotic catheter navigation with a magnet-tipped catheter directed by large, computer directed magnets can provide more precise catheter control as compared to manual catheter manipulation. Th is has the potential, as yet unproven, to shorten the procedure, reduce the length of the learning curve, and perhaps to improve the outcomes of the procedure and reduce complications,” Dr. Heist said.
Dr. Heist said future trials will be needed to directly compare robotic navigation to conventional manually operated catheters in regard to procedural safety and effi cacy.
Mitchell N. Faddis M.D., Ph.D. from the Washington University School of Medicine in St. Louis, Missouri, who was not involved with this study, helped develop the remote magnetic navigation system the researchers used.
“Th e work of Pappone et al. is extremely exciting to me as the culmination of this work, and to the cardiology community in general as a potential important technical advance in the treatment of atrial fi brillation,” Dr. Faddis said.
Dr. Faddis said this new system should be easier to master, as well as being more precise, than conventional catheter ablation.
“Because of computer control, the effi ciency of the procedure may improve. By the end of the 40 patient cohort of Pappone et al., procedures were routinely performed in less than an hour. Th is will likely have an important impact on the complication rate for the procedure which is likely aff ected by procedure duration,” he said.
Visit www.stereotaxis.com for information on this device
Siemens press picture
CORONARY HEART ™ 7

Latest NewsLATEST NEWS
Taller People More Likely to Develop Atrial Fibrillation
Study is the fi rst to show that stature infl uences atrial fi brillation risk
Analysis of data from a registry of patients with left ventricular dysfunction indicates that
height is an independent risk factor for an arrhythmia of the upper chambers of the heart, according to a new study in the April 18, 2006, issue of the Journal of the American College of Cardiology. “Tall stature is a potent risk for the development of atrial fi brillation and is independent of other clinical risk factors. Indeed, the male predominance of atrial fi brillation appears to be explained by the diff erence in height between men and women,” said Jonathan J. Langberg, M.D. from Emory University in Atlanta, Georgia.
Atrial fi brillation is the most common sustained cardiac arrhythmia. During an episode, the upper chambers of the heart fl utter instead of pumping blood eff ectively. Th e incidence increases as people age, with a prevalence of more than 5 percent in patients over the age of 65 years.
Th e size of the left atrium of the heart is known to be associated with atrial fi brillation, so the researchers wanted to see if bigger people have a higher risk of atrial fi brillation.
“It is well known that small animals do not develop atrial fi brillation, while
those larger than humans, particularly horses, seem to be quite susceptible. I also encountered a string of very tall patients, most of whom were former basketball players, with lone atrial fi brillation,” Dr. Langberg said.
Th e researchers, including fi rst author Ibrahim R. Hanna, M.D., reviewed data on 25,268 enrolled in the ADVANCENT registry. ADVANCENT is a prospective, longitudinal, multicenter, observational registry designed to collect and report data on the histories, diagnostics, therapies, and interventions for patients with left ventricular dysfunction (ejection fraction ≤ 40 percent). Th ey separated the patients by height into four groups each for men and women and then
compared atrial fi brillation rates.
Th e patients in the tallest quartile group had an atrial fi brillation prevalence that was 32 percent higher than those in the shortest quartile. Extrapolating from this result indicates that every 16 centimetres (about 6 inches) increase in height is associated with a 50 percent
increase in the chance of developing atrial fi brillation.
“Tall patients may need more aggressive attempts to attenuate risk factors. Controlled trials should evaluate stature in treatment and control arms,” Dr. Langberg said.
He noted that this study just used a snapshot of the health information of the patients at a single point in time, although the patients of course reached their adult height long before they were likely to develop atrial fi brillation. And while all the subjects in this study were patients with impaired left ventricular function, Dr. Langberg speculates that the same results would be found in other groups.
Professor Michael Feneley, M.D., F.R.A.C.P., F.A.C.C. from St Vincent’s
Hospital in Sydney, Australia, who was not connected with this study, pointed out that height is not a modifi able risk
factor.
“Although the paper supports previous evidence of a relationship
between atrial size and atrial fi brillation, there is no therapeutically applicable outcome from the study,
because you can’t alter your height as a risk factor for atrial
fi brillation!” Prof. Feneley said.
the heart, according to a new study in the April 18, 2006, issue of the Journal of the American College of Cardiology.
Atrial fi brillation is the most common sustained cardiac arrhythmia. During an episode, the upper chambers of the heart fl utter instead of pumping blood eff ectively. Th e incidence increases as people age, with a prevalence of more than 5 percent in patients over the age
Th e size of the left atrium of the heart
fi brillation, so the researchers wanted to see if bigger people have a higher risk of
do not develop atrial fi brillation, while
the heart, according to a new study in the April 18, 2006, issue of the Journal of the American College of Cardiology.
Atrial fi brillation is the most common sustained cardiac arrhythmia. During an episode, the upper chambers of the heart fl utter instead of pumping blood
people age, with a prevalence of more than 5 percent in patients over the age
Th e size of the left atrium of the heart
fi brillation, so the researchers wanted to see if bigger people have a higher risk of
do not develop atrial fi brillation, while
compared atrial fi brillation rates.
Th e patients in the tallest quartile group had an atrial fi brillation prevalence that was 32 percent higher than those in the shortest quartile. Extrapolating from this result indicates that every 16 centimetres (about 6 inches) increase in height is associated with a 50 percent
Professor Michael Feneley, M.D., F.R.A.C.P., F.A.C.C. from St Vincent’s
Hospital in Sydney, Australia, who was not connected with this study, pointed out that height is not a modifi able risk
factor.
“Although the paper supports previous evidence of a relationship
between atrial size and atrial fi brillation, there is no therapeutically applicable outcome from the study,
because you can’t alter your height as a risk factor for atrial
fi brillation!” Prof. Feneley said.
The taller you are, the more
susceptible to atrial fibrillation
8 CORONARY HEART ™

RECENT NEWS
Recent News
February 22, 2006
Claimed by Philips, the ‘world’s fi rst Ambient Experience Cath Lab’ is now
open at the Catharina Hospital in Eindhoven, the Netherlands.
Advantages for patients: Heart patients can be distracted from the Cath Lab procedure by choosing a favourite visual theme that can be viewed on LCD panels on the ceiling. Th e theme is accompanied by coloured lighting that illuminates the walls and by a sound and scent that also represent the theme. All these senses together make the environment a comforting and calming atmosphere for the patient, reducing anxiety.
Advantages for medical staff : Using diff use light, any shadows or
refl ections on monitors are eliminated. Furthermore, equal light distribution makes the room very relaxing and soothing to doctor’s eyes.
Th e ambient experience design concept from Philips aims to improve the workfl ow of physicians considerably and reduce anxiety of heart patients undergoing catheterization. Initial tests show that the Ambient Experience design concept
is leading to faster diagnoses, lower radiation doses and calmer patients.
“Th e fi rst experiments already proved this to be a very important investment for our hospital. Th is might even result in less radiation, as our fi rst experiments already have shown. My colleagues and I are also very pleased how this ambient Cath Lab takes into account the sometimes diffi cult working conditions we as physicians encounter – extremely long working hours where concentration and patient focus are essential,” says cardiologist Jacques Koolen of the Catharina Hospital, Eindhoven.
Gerard Kleisterlee, CEO of Royal Philips Electronics: “Hospitals fi nd themselves in an increasingly competitive environment needing to diff erentiate”.
Visit www.medical.philips.com for info
World’s First ‘Ambient Experience’ Cardiology Suite
Image provided courtesy Philips
Philips completes acquisition of Witt Biomedical CorporationApril 27, 2006
Royal Philips Electronics announced that it has completed
its acquisition of Witt Biomedical Corporation, the largest independent supplier of haemodynamic monitoring and clinical reporting systems used in cardiology catheterization laboratories (Cath Labs). Under the terms of the agreement, which was announced on March 8, 2006, Philips acquired Witt Biomedical for USD 165 million. As a result of the transaction, Witt Biomedical will be fi nancially consolidated with immediate eff ect within the Cardio/Vascular X-Ray business of
Philips’ Medical Systems division.
Visit www.medical.philips.com for information
Image provided courtesy Philips
CORONARY HEART ™ 9

RECENT NEWS
Recent NewsBoston Scientific Completes Combination with Guidant
“We look forward to realizing the substantial benefits of combining Boston Scientific & Guidant”
Boston Scientific Corporation announced that it has completed its combination with Guidant
Corporation, creating a global leader in cardiovascular devices and one of the largest medical technology companies in the world. In a related transaction before the closing of the Boston Scientific- Guidant transaction, Guidant and Abbott closed the acquisition by Abbott of Guidant’s vascular intervention and endovascular businesses.
“This is a momentous day for the employees and stockholders of the new Boston Scientific, as well as for thousands of physicians and millions of patients around the world,” said Pete Nicholas, Chairman of Boston
Scientific. “As we begin this new chapter in Boston Scientific’s history, we are committed to building on our long, mutual tradition of technological innovation that helps physicians provide life-saving treatments to their patients. We are also committed to maintaining a culture that values initiative, creativity and collaboration -- and that recognizes the talents and contributions of people who make a difference for our company and our customers.”
“We are looking forward to realizing the substantial benefits of combining Boston Scientific and Guidant,” said Jim Tobin, President and Chief Executive Officer of Boston Scientific. “The new Boston Scientific will be a broadly diversified medical technology company that we believe will command a market valuation closer to our peers and generate significant upside potential for our stockholders. We are confident the integration will proceed smoothly, and we extend a warm welcome to the Guidant employees who are joining us. I know that together we can and we will build a successful future.”
Visit www.bostonscientific.com for more information
Abbott Completes Acquisition Of Guidant Vascular Business
Combination Of Abbott’s And Guidant’s Vascular Organizations Creates Leading Vascular Devices Business
Abbott today announced it has completed the acquisition of Guidant’s vascular business,
which, combined with Abbott’s current vascular business, creates one of the leading global vascular devices companies. This acquisition was made in connection with Boston Scientific’s
acquisition of Guidant Corporation.“The acquisition of Guidant’s vascular business builds on our broad-based business strategy to develop leading positions in attractive health care markets – shaping Abbott for greater balance and strengthening our business mix and breadth of pipeline opportunities,” said Miles D. White, chairman and chief executive officer, Abbott.
“The combined Abbott and Guidant business offers a broad line of leading coronary and endovascular products, a pre-eminent sales force, and global manufacturing operations, as well as a state-of-the-art R&D organization, which is developing innovative technologies and devices such as the XIENCE™ V and ZoMaxx™ drug-eluting stents,” White said. “Our newly expanded vascular organization has the tools and the talent to transform the way physicians treat vascular disease, impacting the lives of millions of patients around the world.”
Visit www.abbott.com for more information
Boston Scientific controls Guidant’s Cardiac Rhythm Management and Cardiac
Surgery business, whilst Abbott controls Guidant’s Vascular
Intervention and Endovascular Solutions business
The Guidant Take-overApril 21, 2006
Boston Scientific’s Corporate Headquarters in Natick, Massachusetts
Courtesy Boston Scientific Corp.
10 CORONARY HEART ™

Recent NewsRECENT NEWS
TOSHIBA INFINIX DP-i/FD2 DEBUTS AT ACCMarch 12, 2006
New System Features Two Flat Panel Detectors for Improved Cardiac Imaging
As a leading developer of technologies that improve the delivery of cardiac care,
Toshiba America Medical Systems, Inc. (TAMS) is debuted its new Infi nixTM DP-i/FD2 vascular X-ray system at the America College of Cardiology’s (ACC) 55th Annual Scientifi c Session in Atlanta, March 11-14, 2006. Designed as one system that operates like two, the Infi nix DP-i/FD2 is equipped with two fl at panel detectors (FPD).
Designed with one eight-inch by eight-inch fl oor mounted cardiac C-arm and one 12-inch by 16-inch ceiling mounted C-arm, the system enables physicians to obtain the high quality images needed to perform both detailed peripheral vascular work and coronary studies without compromise for more effi cient, comprehensive patient care. In addition, the system’s design allows clinicians to perform both coronary and vascular studies on the same table without moving the patient, saving time and increasing overall patient comfort.
“Developing products that improve the patient experience and increase the quality of medical care is a top priority for Toshiba,” said
Don Volz, director, Vascular X-ray Business Unit, TAMS. “With the Infi nix DP-i/FD2, both patients and clinicians benefi t from the system’s ability to perform uncompromised cardiovascular procedures in a single room. In addition, the resulting high quality images featuring precise anatomical detail enable more accurate diagnoses.”
Th e Infi nix also off ers a dual-PC processing system architecture, which permits background image processing and archiving without interrupting the exam. Th is powerful processing can be used with either the eight-by-eight or the 12-by-16-inch FPD. Th e system allows 20 frames per second fl uoroscopy as a tableside option, reducing the patient dose routinely by 25 percent without compromising image quality. Additionally, the Windows®-based operating system provides an intuitive user interface familiar to most operators. Both the triple focus liquid-metal bearing tube for peripheral exams and the dual-focus tube for cardiac exams have a 3.0 million anode heat capacity. Th is rating eliminates delays and increases throughput.
Visit www.medical.toshiba.com for more information
Biosense Webster & Siemens AllianceMarch 16, 2006
Biosense Webster, a Johnson & Johnson company, and
Siemens Medical Solutions announced a strategic alliance giving Biosense Webster exclusive worldwide rights to distribute Siemens’ state-of-the-art cardiac catheters, ACUSON AcuNav™ ultrasound catheters, to electrophysiologists. Siemens will continue to distribute AcuNav ultrasound catheters to interventional cardiologists through its own sales force. Th e two companies also agreed to co-develop future products.
“Biosense Webster’s expertise in the fi eld of electrophysiology and Siemens’ leadership in ultrasound is an ideal combination to help develop future technologies,” said Vivek Y. Reddy, M.D., of the Mass General Hospital in Boston.
images needed to perform both detailed peripheral vascular work and coronary studies without compromise for more effi cient, comprehensive patient care.
allows clinicians to perform both
and increase the quality of medical Siemens press pictureTh e AcuNav™ Ultrasound Catheter
CORONARY HEART ™ 11

Recent NewsRECENT NEWS
GE Conducts Global Cardiac Ultrasound Research at Winter OlympicsFebruary 16, 2006
GE Healthcare and the Olympic Committees from the U.S., Italy and
China, have collaborated on a new clinical study to examine athletes’ hearts in an eff ort to gain new insights into techniques for diagnosing and treating heart disease.
Research leader Malissa Wood, MD at Massachusetts General Hospital and researcher at Harvard Medical School explained, “Past research has shown that abnormalities can develop in endurance athletes’ hearts after exercise. Such changes like stiff ening of the heart are similar to changes found in the earliest phases of coronary heart disease. We hope that the fi ndings of this study will allow physicians to use new methods to more precisely diagnose and follow
the treatment of heart disease and heart failure in everyone from Olympic athletes to the patients we see every day.”
Currently, many professional sport organizations and Olympic teams undergo regular cardiovascular screenings to understand their cardiovascular health and assess risk factors for sudden cardiac death.
GE Healthcare provided some of the world’s most advanced miniaturized ultrasound systems at the Torino Games. Th ese systems - the Vivid i for cardiovascular assessment and the LOGIQ Book used primarily for
musculoskeletal screening - provided sports medicine professionals
with a means to track overall cardiac and musculoskeletal fi tness of an athlete over the course of their training
regimen and also ensured advanced healthcare to
the athletes at the Torino 2006
Olympic Winter Games.
GE’s Vivid i ultrasound system
off ers the functionality and high performance
of larger-scale systems, but in a portable and
wireless design that weighs only 10 pounds. Th e system
makes it possible for patients to receive full diagnostic exams
anywhere, as opposed to being transported to an imaging lab in
a hospital. In addition, physicians can wirelessly transfer fi les from the system to other physicians for instant consultation.
GE’s LOGIQ Book XP is a lightweight, portable ultrasound system that enables
real-time diagnosis anywhere – even the ice rink or locker room. Designed for a modern, all digital healthcare environment, the LOGIQ Book XP allows clinicians to share information for consultation and to archive results electronically.
Visit www.gehealthcare.com for more information
Olympic ski photo provided courtesy LaPresse
China, have collaborated on a new clinical study to examine athletes’ hearts in an eff ort to gain new insights into techniques for diagnosing and treating heart disease.
Research leader Malissa Wood, MD at Massachusetts General Hospital and researcher at Harvard Medical School explained, “Past research has shown that abnormalities can develop in endurance athletes’ hearts after exercise. Such changes like
the LOGIQ Book used primarily for musculoskeletal screening - provided
sports medicine professionals with a means to track overall cardiac and musculoskeletal fi tness of an athlete over the course of their training
healthcare to the athletes at
the Torino 2006 Olympic Winter
Games.
GE’s Vivid i ultrasound system
off ers the functionality and high performance
of larger-scale systems, but in a portable and
wireless design that weighs only 10 pounds. Th e system
makes it possible for patients to receive full diagnostic exams
anywhere, as opposed to being transported to an imaging lab in
a hospital. In addition, physicians
China, have collaborated on a new clinical study to examine athletes’ hearts in an eff ort to gain new insights into techniques for diagnosing and treating heart disease.
Research leader Malissa Wood, MD at Massachusetts General Hospital and researcher at Harvard Medical School explained, “Past research has shown that abnormalities can develop in endurance athletes’ hearts
the LOGIQ Book used primarily for musculoskeletal screening - provided
sports medicine professionals with a means to track overall cardiac and musculoskeletal fi tness of an athlete over the course of their training
Olympic Winter Games.
GE’s Vivid i ultrasound system
off ers the functionality and high performance
of larger-scale systems, but in a portable and
wireless design that weighs only 10 pounds. Th e system
makes it possible for patients to receive full diagnostic exams
anywhere, as opposed to being transported to an imaging lab in
Heart Attack Patients Better with Cypher than BMSMarch 12, 2006
According to data presented during a late-breaking
clinical trials session at the 2006 American College of Cardiology Scientifi c Session, the CYPHER® Sirolimus-eluting Coronary Stent reduced the risk of target vessel failure (TVF) by almost half in patients who suff ered a heart attack (AMI) compared to those who were treated with the current standard of care (balloon angioplasty and a bare metal stent [BMS]).
At one year post implantation of the CYPHER® Stent, the study found that patients given the CYPHER® Stent were 49 percent less likely to experience TVF than those given a BMS. Results were from the TYPHOON study.
Visit www.cordis.com for more information
12 CORONARY HEART ™

Recent NewsRECENT NEWS
World’s FirstBioabsorbable DES Trial BeginsMarch 9, 2006:
Guidant Corporation announced enrolment of the fi rst patient in
a fi rst-in-man clinical trial designed to evaluate the safety of a fully bioabsorbable everolimus eluting stent platform for the treatment of coronary artery disease.
“We are excited about our bioabsorbable drug eluting stent program, which is aligned with Guidant’s strategy of leveraging bioabsorbable technologies to provide innovative site-specifi c therapy for the
treatment of heart disease,” stated John M. Capek, Ph.D., president, Vascular Intervention, Guidant Corporation.Th e fi rst implant was performed by a team headed by Drs. John Ormiston and Mark Webster at Auckland City Hospital, New Zealand. Th e ABSORB trial will enrol up to 60 patients in Belgium, Denmark, France, New Zealand, Poland and Th e Netherlands.
Visit www.guidant.com for more info
Siemens Unveil their Most Advanced CTMarch 3, 2006:
Siemens has pushed the technical and clinical boundaries of CT with this latest innovation, the
Somatom Defi nition, which is faster than every beating heart and capable of imaging full cardiac detail with as much as 50 percent less radiation exposure compared to traditional CT scans.
Th is is an entirely new category of CT scanner technology – dual source computed tomography (DSCT). Th is is due to the utilization of two sources and two detectors. Traditional 64-slice scanners only use one source and one detector.
Setting new standards in cardiac diagnosis, the Somatom Defi nition will image patients with high or irregular heart rates, or even arrhythmia, without beta blocker medications that have been previously needed to slow a patient’s heart. Th e system also enables physicians to better identify and characterize plaque, an early indicator of heart disease.
Th e Somatom Defi nition has enhanced capabilities they claim were not
previously available from any type of diagnostic imaging technology, which are expected to lead to new breakthroughs in clinical research. Th ese capabilities include scanning with two diff erent X-ray energies simultaneously, which allow physicians to better diff erentiate, characterize, isolate and distinguish bone, soft tissue and fl uid. With 0.33 seconds per rotation, electrocardiogram- (ECG) synchronized imaging can be performed with 83-millisecond temporal resolution, independent of the heart rate, resulting in motion free cardiac images.
Th e fi rst Somatom Defi nition was installed at the University of Erlangen (Germany) in October 2005. “Siemens’ newest CT system provides very valuable clinical information for patients presenting in our department with acute chest pain and suspicion of coronary artery disease,” said Dr. Stephan Achenbach, associate professor of Cardiology, University of Erlangen. “We expect that the Somatom Defi nition will have
a signifi cant role in even the most demanding environments, such as emergency departments,” added Prof. Werner Bautz, chairman of Radiology, University of Erlangen, Germany.
Visit www.medical.siemens.com for more information
isolate and distinguish bone, soft tissue and fl uid. With 0.33 seconds per rotation, electrocardiogram- (ECG) synchronized imaging can be performed with 83-millisecond temporal resolution, independent
resulting in motion free
Erlangen (Germany)
“Siemens’ newest CT
patients presenting in our department with
suspicion of coronary artery disease,” said Dr. Stephan Achenbach, associate professor of Cardiology, University of Erlangen. “We expect that the Somatom Defi nition will have
isolate and distinguish bone, soft tissue and fl uid. With 0.33 seconds per rotation, electrocardiogram- (ECG) synchronized imaging can be performed with 83-millisecond temporal resolution, independent
resulting in motion free
artery disease,” said Dr. Stephan Achenbach, associate professor of Cardiology, University of Erlangen. “We expect
Siemens press picture
CORONARY HEART ™ 13

Product FocusPRODUCT INFORMATION
Medtronic Endeavor Drug Eluting Stent
Th e long awaited arrival of Medtronic’s drug eluting stent, the Endeavor™ is fi nally here. Although in some
countries it is still under investigational use we will give you a brief run down on the facts and fi gures.
Platform:
Th e popular Driver coronary stent system provides the platform for the Endeavor™. Already popular with physicians for its manoeuvrability and ease of use, the Driver is a cobalt alloy stent, meaning it is denser and stronger than traditional stainless steel stents, whilst having thinner struts.
Drug:
Licensed by Abbott Laboratories to Medtronic, the drug code named ABT-578 (zotarolimus), is believed to reduce restenosis in clogged arteries by preventing smooth cell proliferation. It achieves this by blocking the function of the cell cycle regulatory protein, mTOR, stopping the growth of new tissue.
Polymer:
Th e delivery matrix for the stent is coated with a Phosphorylcholine (PC) polymer, licensed from Abbott Laboratories, called PC Technology™. It is designed to slowly release the drug into the arterial wall.
Delivery System:
Th e Endeavor Drug Eluting Coronary Stent is intended to be released on Rapid Exchange, Over-the-Wire (USA), and Multi-Exchange technologies for International markets.
Trials:
Th ese trials have been undertaken at various sites to determine the eff ectiveness of the Endeavor™ in reducing coronary artery restenosis.
Endeavor I: Safety and effi cacy of Endeavor™ in de novo coronary lesions in native coronary arteries. Results: A 24-month target lesion revascularization (TLR) rate of 2.0 percent, and no additional cases of stent thrombosis in the 97 study patients who received follow-up over the second 12-month period.
Endeavor II: Compared the Endeavor™ stent to the traditional Medtronic Driver bare metal stent. Results: Demonstrated no observed cases of stent thrombosis between nine and 12 months in either study arm. A 12-month TLR rate of 6.0 percent for Endeavor™ patients, compared to 13.2 percent in the Driver control group.
Endeavor III: Compares the Endeavor™ against the Cypher™ drug-eluting stent marketed by Cordis Corporation, a Johnson & Johnson company. Results: Showed that Endeavor provides clinical and angiographic outcomes consistent with previous Endeavor trials and with no statistical diff erents between Endeavor and Cypher.
Endeavor IV: Compares the Endeavor™ against the TAXUS™ Paclitaxel-Eluting Coronary Stent System from Boston Scientifi c Corporation. Results: Still enrolling.
Medtronic Endeavor Drug-Eluting StentCourtesy Medtronic, Inc.
Medtronic Endeavor Drug-Eluting StentCourtesy Medtronic, Inc.
14 CORONARY HEART ™

SPECIAL FEATURE
by Maria Whitehead and Jenny LavenderHull and East Yorkshire Hospitals NHS Trust, UK
Introduction
In this article we will discuss the Hull experience of why we decided to introduce the role of coronary angiography practitioner. We will include the stages we went through to gain approval within our organisation and how we set the program up including the training needs. We will evaluate the reality of the role highlighting the advantages and disadvantages and discuss our plans for future development.
Background
Hull is a tertiary centre providing interventional cardiology services for a population of 1.2 million. We perform 2000 coronary angiograms per annum. Our cardiology services are currently split between three sites, which poses us quite a challenge in terms of medical staffi ng. Th is has been further increased by the European Working Time Directives reducing the availability of cardiology SpRs in the cath lab and the new Consultant contracts, which has reduced the fl exibility of the Cardiologists to backfi ll empty cath lab sessions.
Th ese issues led to our cath labs being under utilised and we were struggling to meet the National Service Framework Target waiting times for coronary angiography.
Our service manager and clinical director for cardiology considered that a solution to the problem could be to train non medical practitioners to perform coronary angiography.
Setting up a program
Who
We acknowledged that any of the three professional groups within the cath lab with the relevant experience could be trained equally eff ectively. However within our cardiac cath labs, our nurses and radiographers are dedicated, permanent staff whereas our cardiac physiologists work on a rotational basis and already have their own specialist areas of practice.
Experience
We enrolled a senior cardiac nurse and a senior radiographer to undertake training, each with around 10 year’s cath lab experience. Obviously an extensive knowledge of the procedure, equipment selection, potential problems and the ability to manage them is essential.
Introducing the role of Coronary Angiography Practitioner
and radiographers are dedicated, them is essential. and radiographers are dedicated, permanent staff whereas our cardiac physiologists work on a rotational basis and already have their own specialist areas of practice. The traditional roles of
lab professionals may be changing
CORONARY HEART ™ 15

SPECIAL FEATURE (cont...)
Supporting Documentation
We prepared the following documentation prior to commencing the role;
A proposal for the role including the benefi ts to the organisation.Job description and person specifi cation.Competency based training and assessment program utilising the Skills for Health (2005) competencies for coronary heart disease.Written schemes of work including a protocol for undertaking the procedure.Risk assessments.
A high volume centre
You must have the opportunity to perform enough procedures to regularly maintain your skills without aff ecting the training opportunities of the cardiology SpR’s. A minimum of 100 cases per annum is recommended for each practitioner.
•
•
•
•
•
Support
Support from senior management is essential to drive the program. Our service manager for cardiology undertook most of the ground work in terms of taking the proposal to the following stakeholders;
CardiologistsClinical GovernanceDirector of NursingRadiology service managerRadiation Protection AdvisorTrade UnionsMedical DirectorTrustboard
To obtain agreement from all the stakeholders including obtaining the written medical indemnity took 8 months in total.
Initially we did not have support from all our Cardiologists but as the benefi ts became evident the support grew rapidly.
Training
During the time we spent waiting for approval to commence training, we utilised the time to undertake some role swapping. Th is enhanced the skills of the nurse in terms of producing quality radiographic views and images. Th e radiographer was able to enhance her skills in scrubbing and haemostasis and to undertake in house Intermediate Life Support, peripheral cannulation and the administration of intravenous drugs.
Th e only formal training we were required to undertake was the IRMER (Ionising Radiation Medical Exposure Regulations) certifi cate which we did in house, along side our medical colleagues.
Our training plan was to work along side a Cardiologist for 50 procedures and be closely supervised for a further 50 procedures. We each did 2 sessions per week (10 procedures) initially, but in real terms it took 5 months to complete our training.
Our radiographer training was interrupted by pregnancy after her fi rst 70 procedures, but we consider that a suffi cient number of procedures were undertaken to demonstrate our theory that each profession could perform equally as well.
How does it work in reality?
We are required to ensure that the Cardiologist who is covering the list is on site prior to commencement. Th eir location is usually in the outpatient’s clinic or in their administration session, this enables them to be in the cath lab within 5 minutes if necessary.
Th e practitioner will complete the full list of angiograms, completing a provisional report for each patient. Th e selection criteria for practitioner led
Coronary Angiography Practitioner
16 CORONARY HEART ™

SPECIAL FEATURE (cont...)
angiography are that the patients are elective, stable and suitable for femoral access. 95% of our elective angiograms are performed via the femoral route using 4 or 5 french systems. At the end of the session, the Cardiologists will review all the fi lms, the management plans will be discussed and the patients medications are reviewed. Th e practitioner will then discuss the outcome with the patient and complete any referral documentation.
Negative aspects
Th ere was no funding identifi ed for this role prior to commencing training and we were informed that as this was a pilot role there may not be a post at the end of the training period.
Our posts were not backfi lled which meant that we had to undertake our very demanding current roles in addition to undertaking our training. Our posts including the extended role of coronary angiography practitioner are yet to be banded satisfactorily in line with Agenda for Change.
Benefi ts
We have signifi cantly improved the utilisation of our cath labs and have reduced our waiting times from 9 months to 4 months. We have reduced patient cancellations by 10% because of the fl exibility of a practitioner being available for example when there is sickness, urgent meetings, leave.
Th e routine medical workload is alleviated to allow Consultant Cardiologists to undertake complex coronary intervention and assist the possible introduction of primary PCI.Obviously for the organisation there is a huge cost saving due to eliminating the need to pay medical staff for carrying out extra sessions.
Evaluation
We are now almost 2 years into sustaining this new role. Th e coronary angiography practitioners in our organisation have performed almost 700 procedures in that time. We collect and examine our audit data 6 monthly looking specifi cally at success rates, screening times, complications and diagnostic quality. Initially we compared our data with that of our Cardiology Specialist Registrars as a benchmarking exercise and found the outcomes to be very similar.
Our original intention was to have a dedicated role of coronary angiography practitioner but as we have progressed we have recognised that a fl exible, more balanced role is more benefi cial to all parties. We continue with our original roles and backfi ll sessions when necessary and only when there is no SpR to fi ll the session. For anyone to carry out coronary angiography on a full time basis would we suggest, become rather monotonous. From a practitioners point of view it has been a very enjoyable challenge that has enhanced job satisfaction. Th e new challenges for year 2 have been to progress to radial procedures and to include more complex procedures such as patients with previous CABG. From a patients point of view we have received very positive feedback.
Th e future
We have a new cardiothoracic centre due to open in 2007/2008 with a further increase in cath lab capacity. It has been useful to explore new ways of working and hopefully the introduction of this role will provide an attractive cath lab career ladder, improving our recruitment and retention prospects and we aim to expand our team of coronary angiography practitioners.
Coronary Angiography Practitioner
We would like to hear your
comments on this article.
Email your thoughts, positive or
negative, and we’ll try to
publish them in the next
issue.
Write to us at:
CORONARY HEART ™ 17

CATH LAB VISIT
Epworth Hospital
The Epworth Foundation is a not for profi t organisation and is Australia’s largest multi-campus
group, located in Melbourne, Victoria; the southernmost state in Australia.
It comprises of 4 campuses, Epworth Hospital Richmond, Epworth Eastern Box Hill, Epworth Rehabilitation Brighton, and the Transitional Living centre in Brunswick. It currently has 829 beds, 23 operating theatres and 5 catheter labs, employs 2844 staff and has 1477 accredited doctors.
In 2006, Freemasons Hospital will join the Epworth Foundation making it the largest and busiest private hospital group in metropolitan Melbourne with
a total of 1131 beds.
Epworth Hospital, Richmond
Th e Epworth Hospital is renowned
both locally and internationally for its cutting edge technology and standards of clinical excellence. It was the fi rst private hospital in Victoria to provide open heart surgery, and robotics surgery in the southern hemisphere.
AUSTRALIA
ADDRESS
STAFF
MAP
13 Nurses3 Radiographers2 Orderlies (Porters)2 Receptionists11 Cardiac Physiologists (from Non-Invasive Dept)
Cardiac Cath LabEpworth Hospital89 Bridge RoadRichmondVictoria, 3121Australia
18 CORONARY HEART ™

CATH LAB VISIT (cont...)
Epworth Hospital
CORONARY HEART ™ 19
Cardiovascular Intervention Suite
Th e Cardiovascular Intervention Suite at Epworth Hospital is one of Australia’s largest interventional facilities comprising of 4 labs. It consists of 2 cardiac labs, a dedicated vascular lab and a dedicated electrophysiology lab. Th e Suite attended to approximately 4300 patients and carried out about 5400 procedures in 2005. Th e Intervention Suite generally operates between the hours of 7am to 7pm Mondays to Fridays with a 24 hour acute service for PCI. A Saturday morning elective session is available on request
Cardiac Labs
Th e 2 cardiac Labs are equipped with the GE Innova 2000 digital system, the fi rst cath lab in Victoria to do so and is supported by the Mac-Lab Haemodynamic monitoring, the Centricity Cardiology Data Management system and the Vepro Image Archival system. Th e labs carry out about 2900 procedures that include coronary angiograms, ASD/PFO closures, PCI and, Rotational Atherectomy. About 800 PCI’s are done annually.
Vascular Lab
Th is is the fi rst dedicated vascular lab in Australia and the procedures are carried out by Vascular Surgeons. Th e surgeons performed about 1560 procedures in 2005. Th ese include femoral angiograms, angioplasty and stenting, renal and carotid stenting, ovarian vein and other vessel embolisations and endoluminal repair of Abdominal Aortic Aneurysm’s (AAA). Th e Vascular lab did 118 AAA repair cases in 2005 and is expected to reach 130 in 2006. It is one of the busiest Abdominal Aneurysm repair labs in the world. Th e imaging equipment used in this lab is the GE Advantx LCV.
continued......Lab Photography: Catriona McRoy
Kate Reed (Senior Radiographer) in the common Control Room which divides the two cath labs.
Headsets are used to communicate with cardiologists and nurses behind the lead screen during cases.
The Cardiac Physiologist sits on the right.

CATH LAB VISIT (cont...)
Epworth Hospital
20 CORONARY HEART ™
Electrophysiology Lab
The electrophysiology lab was established in September 2002 and is one of only two private dedicated EP labs in Australia. It is equipped with a 56 channel EP-WorkMate system and an EPT 1000XP generator for ablations. The lab carried out 879 procedures in 2005 comprising electrophysiology studies, ablations, reveal, pacemaker, AICD and bi-vent device implants. The lab hopes to acquire a 3-D Mapping system sometime in the future. The imaging equipment used in this lab is the GE Advantx LU.
Staffing
The Cath Lab Suite currently has 21 permanent staff members, comprising
a unit manager, 13 registered nurses, 3 radiographers, 1 full-time and a part-time receptionist, and 2 orderlies (porters). The staff are further complemented by 11 cardiac physiologists in the cardiac and electrophysiology labs whom rotate down from the Non-Invasive Department.
The Unit Manager, Mr Letch Krishnan, is assisted by 3 team leaders and a senior radiographer. One of the team leaders has an education portfolio and is responsible for all education, training, development and competencies in the unit.
Education and Training
The nurses undergo supervised competency based training in cardiac, vascular, and electrophysiology interventions. They also undergo an anaesthetics and recovery education program with clinical placement in the Operating Theatre Suite, adjacent to the main department.
The Cath Lab Suite carried out 336 cases under general anaesthesia in 2005 and these patients are recovered in the cath lab by the cath lab nurses. Other compulsory competencies include Basic Life Support, Advanced Life Support ECG, Intravenous cannulation, cardiac pacing, and intra aortic balloon pump management.
Multi-skilling is an important aspect of staff education and training in the suite. Radiographers assist in managing the inventory, learn from the nurses to scrub assisting the doctor, and scouting during the procedures. They also monitor the patients ECG and other physiological parameters and record all the equipment used during the cases.
All doctors working in the Cath Lab Suite undergo a course on radiation safety resulting in a Radiation Safety Licence being awarded at the end of the course. This allows them to operate the
Lab 1: The Director of Cardiology, Dr Ron Dick performing a coronary angiogram
EP /Pacemaker LabFrom left: Cameron McCormack
(Tech) & Dr Bruno Martin

CATH LAB VISIT (cont...)
Epworth Hospital
CORONARY HEART ™ 21
x-ray equipment in the suite.
Th e staff in the cath lab are given opportunities to attend both local and international meetings as part of their on-going professional development with generous support of study leave, registration and other related expenses.
Recognition
Th e Cath Lab Suite is highly regarded both in Australia and internationally. It is a preferred reference site to many corporate businesses and is a frequent venue for live meetings, workshops, and conferences, and plays host to many renowned international speakers.
Visit www.epworth.org.au for further hospital details.
The Cath Lab Day WardComplete with overhead televisions
Nurses from left: Paula Gontan, Denise Lark (“Angel at Work”), and Smitha Sivasdasan
WHY MELBOURNE?
Set on the shores of Port Phillip Bay, the second largest city in Australia (3.6 million) boasts a lively cosmopolitan culture. The city centre itself is located 5km from the bay and sits on the northern banks of the Yarra River, popular with rowers and tourist ferries. Melbourne is host to the F1 Grand Prix, and the Australian Open Tennis and in March 2006, hosted the Commonwealth Games. Beautiful parks, golden beaches, and friendly locals, will make all visitors fall in love.
What’s Great to See?
Federation SquareOpened in 2002 on the banks of the Yarra, this public space fuses art and architecture. Visit for great cafes and Australian art.
NewQuayMelbourne’s newest dining & shopping precinct, 1km from the CBD situated right on the waterfront. Experience great food, and great views.
Melbourne Cricket GroundTh is incredible 97,000 seat stadium is the home of Australian Rules Football (AFL), and for 90 days over summer hosts the cricket.
•
•
•

CATH LAB VISIT
East Surrey Hospital Cath Lab StaffBack Row (from left): Rachel King (nurse), Caroline Pinney (Nurse Unit Manager), Hafiza Abbas (Superintendant Radiographer), Analy Castro (Radiographer). Front Row (from left): Janet Townsend (Nurse), Emma Thompson (Nurse).
East Surrey Hospital
22 CORONARY HEART ™
East Surrey Hospital is part of the Surrey and Sussex Healthcare NHS Trust, and is located in
the town of Redhill, on the southern outskirts of London. Th e Cath Lab was built in 2004 in a newly constructed wing to the hospital and contains all the latest cardiac equipment expected for a non-PCI centre.
Th e department is staff ed by a very friendly team of cardiologists, nurses, radiographers, and physiologists, whom work extremely well together, ensuring any problems or delays are kept to a minimum. Patients are also happy, as shown by the overfl owing board of “Th ankyou” cards in the staff room.
Th e Cath Lab Unit Manager, Caroline Pinney spoke with Coronary Heart™ about how the department works, and their goals for the future.
1) Cath Lab size?
We have one lab and a six bedded day ward. Next door to the lab is a twenty-six bedded cardiology ward incorporating a six bedded high dependency area and an eight bedded CCU.
2) Staff Numbers and Roles?
We have seven nursing staff who are responsible for the preparation of the patient for the procedure. Th e nurse also acts as a scrub nurse and a
runner nurse during the procedure. Th ey are also responsible for removing the sheath post procedure and the recovery of the patient. Th e nurse also holds a pre – assessment clinic each morning for patients prior to their procedure. We have two radiographers both of them are shared with radiology. We currently have four cardiac physiologists who have a dual role in the cardiac department. Four cardiology consultants each operate one day in the lab.
3) Staff Cross-Training?
Our staff are currently not cross trained and we do not plan to do any cross training at this time.
UNITED KINGDOM
STAFF
ADDRESS
IMAGING
MAP
7 Nurses2 Radiographers4 Cardiac Physiologists4 Cardiologists
Cardiac Cath LabEast Surrey HospitalCanada AvenueRedhill, RH1 5RHSurreyUnited Kingdom
1x GE Innova 2100

CATH LAB VISIT (cont...)
East Surrey Hospital
continued...
CORONARY HEART ™ 23
4) Roles for Radiographers, and Cardiac Physiologists?
The radiographer is responsible for driving the camera, moving the table, and injecting the LV. They also have a role in teaching and education around radiation protection issues. The cardiac physiologist is responsible for all the monitoring in the lab.
5) Types of Procedures?
We perform diagnostic angiograms and implant permanent pace makers. We also provide an area for a TOE list and carry out emergency procedures such as insertion of a temporary wire of pericardial drain.
6) Procedures per year?
Approximately 1000.
7) Day Cases?
Where possible all diagnostic angiograms are performed as day cases.
8) Private Cases?
We do not perform private cases.
9) Angioplasty (PCI) future plans?
We hope to commence our angioplasty service in June 2006.
10) Surgical Back-up for the Department?
There are no cardiac theatres on site. Patients are transferred to one of three tertiary centres in the event that they require further intervention, either St Georges, Royal Sussex or the Heart.
11) Alliances with other Hospitals for Treatment?
We have an agreement with the three tertiary centres mentioned before to refer for PCI and surgery and complicated high risk procedures.
12) Haemostasis Management?
We have several methods of managing haemostasis. The method used depends on the patients and their medical and social circumstances. We currently use
closure devices, femstops, Neptune pads and manual pressure.
13) New Procedures Implemented into the Lab?
We are currently following an accelerated recovery procedure for patients having their sheath removed using a femstop device. The recovery time for those patients who are eligible has been reduced from 4hrs to 1.5hrs.
14) Inventory Management?
We perform a weekly stock check. All the stock is managed on a spreadsheet. Commonly ordered stock is ordered via telephone and delivered within 24hrs, other items are ordered via the internet.
15) Measures Implemented to Cut Costs in the Lab?
No specific measures have been introduce, we are all aware of budgetary constraints and are careful with stock.
The spacious and well organised Lab with the GE Innova 2100 Digital Detector, and LCD monitors.
The modern cardiology wing and decking overlooking a pond which is home to
protected birdlife.

CATH LAB VISIT (cont...)
East Surrey HospitalWHY SURREY?
The County of Surrey is located in southern England, on the outskirts of the UK’s capital city, London. The population of over one million people, spread throughout the region, are surrounded by lush countryside, dotted with old english villages, stately homes, and medieval churches. Many people move to this region for its beauty and relaxed culture, whilst still being close enough to commute into London. Redhill is located just south of the M25, close to London’s Gatwick Airport, and 30min by train to London.
Nearby Villages & Landmarks
Reigate (circa 1150)Th is traditional market town is located just to the south of the North Downs, and is famous for Th e Old Town Hall built in 1708, and the Reigate Windmill (world’s only used for worship).
Guildford Castle (circa 1066)Th is was the only Royal Castle in Surrey, with the original wooden defences replaced with stone in the 12th century. Today only the Tower Keep remains, surrounded by a beautiful park.
Nearby Pursuits
Paragliding and Hang GlidingMountain BikingHikingVariety of Watersports
•
•
••••
24 CORONARY HEART ™
16) Training for New Employees?
New nursing staff s receive a set of competencies on arrival to the unit and an information booklet about procedures performed in the Angiosuite. Th ey work towards those competencies with an assigned mentor spending time in each area of the department as well as orientation to the hospital as a whole.
17) Continuing Education Programs for Staff ?
Staff are encouraged to attend all in-house training supplied by the trust including the mentorship programme and the clinical leadership programme. Further education is also available through Guildford University for some staff each year.
18) Competency Checks for Staff once Employed?
Competencies are signed by the senior nurse or doctor depending on which area of training is being assessed.
19) Challenges Setting up a New Department?
It is always a challenge setting up a new service but all the challenges have been a good learning experience.
20) Best Part of Working at East Surrey Hospital Cath Lab?
It is wonderful to be part of a committed multi-disciplinary team.
The modern six-bedded Cath Lab day ward at the end of a busy day

EP EDUCATION
An Introduction to Wolff Parkinson White Syndrome Written by Ian Wright
St Mary’s Hospital, London, UK
“WPW syndrome is present in approximately three in every 2,000 people”
In 1930 Wolff , Parkinson and White fi rst described the syndrome that bears
their name as “bundle-branch block with short P-R interval in healthy young people prone to paroxysmal tachycardia.” We now know that the condition is caused by one or more strands of myocardial tissue, known as accessory pathways, which bridge the atrio-ventricular (AV) ring that electrically isolates atria from ventricles. In the normal heart the AV ring is bridged only by the His bundle arising from the AV node - this forms the sole route for an impulse to pass from atria to ventricles (other connections having been severed during foetal development of the heart valves).
Th e presence of this extra pathway (or “bypass tract”) explains the features that defi ne WPW syndrome and is present in approximately three in every 2,000 people.
An important role of the AV node is to slow impulses on route from atria to ventricles, allowing optimal time for ventricular fi lling. By comparison accessory pathways conduct very rapidly. Th is manifests on the ECG as a short P-R interval.
Rapid conduction of the impulse around the ventricles by the specialised conduction system results in the narrow QRS complexes seen on a normal ECG. As accessory pathways connect to non-specialised myocardial cells that conduct slowly, activation of the ventricles via such pathways results in a broad initial QRS - the delta wave seen in WPW patients.
1.
2.
AV nodal conduction eventually catches up and the QRS changes from broad to narrow. Th is activation of the ventricles from two diff erent routes produces the characteristic fusion complex that characterises WPW syndrome (see Fig 2).
Patients with this ECG appearance are said to have a manifest accessory pathway. With the knowledge available at the time Wolff , Parkinson and White incorrectly described this ECG appearance as bundle branch block.
Figure 1: 12 Lead ECG in WPW
Figure 2
CORONARY HEART ™ 25

EP EDUCATION (cont...)
WPW Syndrome
Th e presence of an accessory pathway provides the substrate for Atrio-Ventricular Re-entrant Tachycardia (AVRT). Th is is an endless loop of activation circling between atrium and ventricle, utilising the AV node/His bundle and the pathway. Th ese circuits are possible in two opposite directions – from atrium to ventricle via the pathway, returning via the AV node (antidromic AVRT) or atrium to ventricle via the AV node, returning via the pathway (orthodromic AVRT). Slow conduction away from the pathway means antidromic AVRT is broad complex (it looks similar to ventricular tachycardia) whilst rapid distribution of the impulse by the specialised conduction system means orthodromic AVRT is narrow (in the absence of rate-related bundle-branch block). Orthodromic AVRT is by far the more common (Fig. 3).
3.
As atrial impulses approach the AV node faster and faster, it responds by conducting slower and slower. Th is is called decremental conduction and is displayed by the AV node more than other heart tissue. Because of this the AV node acts as a gatekeeper – protecting the ventricles from unwanted and potentially dangerous rhythms arising in the atria, such as atrial fi brillation (AF). Accessory pathways however, pass on incoming signals however fast, without slowing the impulse (“all or nothing” conduction). If a patient with WPW goes into AF, the ventricles may be exposed to very rapid signals that the AV node would normally fi lter out. Th e rate of this bombardment is determined by the refractory period of the pathway and if this is short, the stimulation may be suffi cient to provoke polymorphic VT or VF. Consequently, untreated WPW carries a small increased risk of sudden death. Young patients and those experiencing syncope are considered more at risk.
4.
Th e word Ortho means “right” or “correct” (as in orthodontics - “correct teeth”) whilst dromic means route, way, path. I fi nd this helps me remember which is which – the AV conduction via the AV node is the “correct” route of anterograde conduction, hence in orthodromic AVRT the anterograde limb of the circuit is the AV node.
Concealed Accessory Pathways
Some patients have pathways that only conduct from ventricle to atrium. Th ese pathways do not show up on the resting ECG, which is normal, and such patients are said to possess a concealed accessory pathway. Th ey do not have WPW syndrome but may still suff er from palpitations caused by orthodromic AVRT (see below).
26 CORONARY HEART ™

EP EDUCATION (cont...)
WPW Syndrome
An ECG of WPW with AF is quite memorable. It shows a rapid, broad complex, irregular tachycardia. The differential diagnosis is AF with WPW, or polymorhic VT. In contrast to the constantly changing complexes seen in polymorhic VT, AF with
WPW presents with a fairly consistent QRS morphology (Fig. 4). This presentation is known as pre-excited AF. It is impossible in patients with a truly concealed pathway who do not share the increased risk of sudden death that accompanies WPW.
Figure 3
Figure 4
Pre-excited AF
CORONARY HEART ™ 27

EP EDUCATION (cont...)
WPW Syndrome
Ablation of WPW
Since the late 1980s radio-frequency (RF) energy, delivered via a steerable catheter, has been used to destroy accessory pathways by heating. A successful ablation cures the patient of AVRT and removes the increased risk of sudden death. It also converts the QRS complexes to normal (Fig 5). Th e procedure is performed in an EP lab where diagnostic catheters are placed in strategic positions within the heart and the location of the pathway deduced from the sequence of intra-cardiac signals. Pathways may present around the mitral valve (left-sided pathways) or tricuspid valve (right-sided pathways). Pathways close to the AV node can be diffi cult to treat due to the increased risk of damaging this important structure. Cryo-ablation (freezing), which appears to have certain safety advantages, can be employed to treat these pathways.
© Ian Wright, 2006.
Figure 5: This is the same patient as fig 1 but after successful ablation
28 CORONARY HEART ™

coronaryheart.com
Conferences 2006CONFERENCES
CORONARY HEART ™ 33
October 5-7Annual General Meeting of the Irish Cardiac SocietyLocation: Killarney, Co. Kerry, IrelandWebsite: www.irishcardiacsociety.com
October 15-1921st Scientific Meeting of International Society of HypertensionLocation: Fukuoka, JapanWebsite: www.congre.co.jp
October 21-24Acute Cardiac CareLocation: Prague, Czech RepublicWebsite: www.escardio.org
October 21-25Canadian Cardiovascular SocietyLocation: Vancouver, BC, CanadaWebsite: www.ccs.ca
October 22-27TCT 2006: Transcatheter CardiovascularTherapeuticsLocation: Washington DC, USAWebsite: www.tct2006.com
LIST YOUR CARDIAC
CONFERENCEHERE FREE
Email the details to:[email protected]
October 26-28Autumn Congress of the Netherlands Society of CardiologyLocation: Ermelo, NetherlandsWebsite: www.cardiologie.nl
November 1-4New Cardiovascular HorizonsLocation: New Orleans, Louisiana, USAWebsite:www.newcvhorizons.com
December 3-719th World Diabetes CongressLocation: Cape Town, South AfricaWebsite: www.idf2006.org
December 6-9EuroEcho 10Location: Prague, Czech RepublicWebsite: www.euroecho.org
Conferences 2006
CORONARY HEART ™
LIST YOUR CARDIAC
CONFERENCEHERE FREE
Email the details to:[email protected]
October 26-28Autumn Congress of the Netherlands Society of CardiologyLocation:Website: www.cardiologie.nl
November 1-4New Cardiovascular HorizonsLocation:Louisiana, USAWebsite:www.newcvhorizons.com
December 3-719th World Diabetes CongressLocation: Cape Town, South AfricaWebsite: www.idf2006.org
December 6-9EuroEcho 10Location:RepublicWebsite: www.euroecho.org
MEDICAL IMAGING
RAO 30 / CAU 20
CORONARY HEART ™ 31
RAO 30 / CAU 20
Objective:
This angle is used primarily to demonstrate the Left Main and the Circumflex arteries, and is the best view for demonstrating the proximal Obtuse Marginal branch. The Left Anterior Descending artery is also seen however is often overlapped by the Diagonal branches. Acquisition time should be long enough to obtain adequate contrast filling of the distal arteries, and if necessary pan to the anatomical right to visualise collateral filling of the Right Coronary artery. Visualising the right coronary artery filling distally may assist Cardiologist of the possible lesion length occurring in that artery.
Alternatives:
More CAU (eg. RAO 30 / CAU 40):
This decreases the foreshortening of the proximal circumflex improving visualisation. The distal circumflex can be foreshortened and overlapped by distal branches. Foreshortening of the LAD occurs mid /distal with overlap of the diagonal branches.
Less CAU (eg. RAO 30 / CAU 10):
Increases foreshortening of proximal circumflex, however improves visualisation distally by separating the distal branches. The obtuse marginal is often overlapped by large septals from the LAD or diagonal branches.
More RAO (eg. RAO 40 / CAU 20):
This separates the diagonal branches further from the LAD, demonstrating them inferior to the LAD. This view can also improve visualisation of the mid / distal Obtuse Marginal branch
Less RAO (eg. RAO 10 / CAU 20):
This separates the diagonal branches further from the LAD, demonstrating them superior to the LAD.
CORONARY HEART ™ 31
RAO 30 / CAU 20
LM Left Main
LAD Left Anterior Descending
D1 Diagonal
LCX Circumflex
OM1 ObtuseMarginal 1
RAO 30 / CAU 20
More RAO (eg. RAO 40 / CAU 20):
This separates the diagonal branches further from the LAD, demonstrating them inferior to the LAD. This view can also improve visualisation of the mid / distal Obtuse Marginal
This separates the diagonal branches further from the LAD, the LAD.
CORONARY HEART ™
Left Main
Left Anterior Descending
Diagonal
Circumflex
ObtuseMarginal 1
EP EDUCATION
An Introduction to Wolff Parkinson White Syndrome Written by Ian Wright
St Mary’s Hospital, London, UK
CORONARY HEART ™ 27
“WPW syndrome is present in approximately three in every 2,000 people”
In 1930 Wolff, Parkinson and White first described the syndrome that bears
their name as “bundle-branch block with short P-R interval in healthy young people prone to paroxysmal tachycardia.” We now know that the condition is caused by one or more strands of myocardial tissue, known as accessory pathways, which bridge the atrio-ventricular (AV) ring that electrically isolates atria from ventricles. In the normal heart the AV ring is bridged only by the His bundle arising from the AV node - this forms the sole route for an impulse to pass from atria to ventricles (other connections having been severed during foetal development of the heart valves).
The presence of this extra pathway (or “bypass tract”) explains the features that define WPW syndrome and is present in approximately three in every 2,000 people.
An important role of the AV node is to slow impulses on route from atria to ventricles, allowing optimal time for ventricular filling. By comparison accessory pathways conduct very rapidly. This manifests on the ECG as a short P-R interval.
Rapid conduction of the impulse around the ventricles by the specialised conduction system results in the narrow QRS complexes seen on a normal ECG. As accessory pathways connect to non-specialised myocardial cells that conduct slowly, activation of the ventricles via such pathways results in a broad initial QRS - the delta wave seen in WPW patients.
1.
2.
AV nodal conduction eventually catches up and the QRS changes from broad to narrow. This activation of the ventricles from two different routes produces the characteristic fusion complex that characterises WPW syndrome (see Fig 2).
Patients with this ECG appearance are said to have a manifest accessory pathway. With the knowledge available at the time Wolff, Parkinson and White incorrectly described this ECG appearance as bundle branch block.
Figure 1: 12 Lead ECG in WPW
Figure 2
Wolff Parkinson Written by Ian WrightSt Mary’s Hospital, London, UK
CORONARY HEART ™
AV nodal conduction eventually catches up and the QRS changes from broad to narrow. This activation of the ventricles from two different routes produces the characteristic fusion complex that characterises WPW
Patients with this ECG appearance are said to have a manifest accessory pathway. With the knowledge available at the time Wolff, Parkinson and White incorrectly described this ECG appearance as bundle branch block.
Figure 1: 12 Lead ECG in WPW
SPECIAL FEATURE (cont...)
CORONARY HEART ™ 19
angiography are that the patients are elective, stable and suitable for femoral access. 95% of our elective angiograms are performed via the femoral route using 4 or 5 french systems. At the end of the session, the Cardiologists will review all the films, the management plans will be discussed and the patients medications are reviewed. The practitioner will then discuss the outcome with the patient and complete any referral documentation.
Negative aspects
There was no funding identified for this role prior to commencing training and we were informed that as this was a pilot role there may not be a post at the end of the training period.
Our posts were not backfilled which meant that we had to undertake our very demanding current roles in addition to undertaking our training.
Our posts including the extended role of coronary angiography practitioner are yet to be banded satisfactorily in line with Agenda for Change.
Benefits
We have significantly improved the utilisation of our cath labs and have reduced our waiting times from 9 months to 4 months. We have reduced patient cancellations by 10% because of the flexibility of a practitioner being available for example when there is sickness, urgent meetings, leave.
The routine medical workload is alleviated to allow Consultant Cardiologists to undertake complex coronary intervention and assist the possible introduction of primary PCI.Obviously for the organisation there is a huge cost saving due to eliminating the need to pay medical staff for carrying out extra sessions.
Evaluation
We are now almost 2 years into sustaining this new role. The coronary angiography practitioners in our organisation have performed almost 700 procedures in that time. We collect and examine our audit data 6 monthly looking specifically at success rates, screening times, complications and diagnostic quality. Initially we compared our data with that of our Cardiology Specialist Registrars as a benchmarking exercise and found the outcomes to be very similar.
Our original intention was to have a dedicated role of coronary angiography practitioner but as we have progressed we have recognised that a flexible, more balanced role is more beneficial to all parties. We continue with our original roles and backfill sessions when necessary and only when there is no SpR to fill the session. For anyone to carry out coronary angiography on a full time basis would we suggest, become rather monotonous.
From a practitioners point of view it has been a very enjoyable challenge that has enhanced job satisfaction. The new challenges for year 2 have been to progress to radial procedures and to include more complex procedures such as patients with previous CABG. From a patients point of view we have received very positive feedback.
The future
We have a new cardiothoracic centre due to open in 2007/2008 with a further increase in cath lab capacity. It has been useful to explore new ways of working and hopefully the introduction of this role will provide an attractive cath lab career ladder, improving our recruitment and retention prospects and we aim to expand our team of coronary angiography practitioners.
Coronary Angiography Practitioner
We would like to hear your
comments on this article.
Email your thoughts,positive or
negative, and we’ll try to
publish them in the next
issue.
Write to us at:
Coronary Angiography PractitionerCoronary Angiography Practitioner
We would like to hear your
comments on
negative, and
publish them
SPECIAL FEATURE
by Maria Whitehead and Jenny LavenderHull and East Yorkshire Hospitals NHS Trust, UK
CORONARY HEART ™ 17
Introduction
In this article we will discuss the Hull experience of why we decided to introduce the role of coronary angiography practitioner. We will include the stages we went through to gain approval within our organisation and how we set the program up including the training needs. We will evaluate the reality of the role highlighting the advantages and disadvantages and discuss our plans for future development.
Background
Hull is a tertiary centre providing interventional cardiology services for a population of 1.2 million. We perform 2000 coronary angiograms per annum. Our cardiology services are currently split between three sites, which poses us quite a challenge in terms of medical staffing. This has been further increased by the European Working Time Directives reducing the availability of cardiology SpRs in the cath lab and the new Consultant contracts, which has reduced the flexibility of the Cardiologists to backfill empty cath lab sessions.
These issues led to our cath labs being under utilised and we were struggling to meet the National Service Framework Target waiting times for coronary angiography.
Our service manager and clinical director for cardiology considered that a solution to the problem could be to train non medical practitioners to perform coronary angiography.
Setting up a program
Who
We acknowledged that any of the three professional groups within the cath lab with the relevant experience could be trained equally effectively. However within our cardiac cath labs, our nurses and radiographers are dedicated, permanent staff whereas our cardiac physiologists work on a rotational basis and already have their own specialist areas of practice.
Experience
We enrolled a senior cardiac nurse and a senior radiographer to undertake training, each with around 10 year’s cath lab experience. Obviously an extensive knowledge of the procedure, equipment selection, potential problems and the ability to manage them is essential.
Introducing the role of Coronary Angiography Practitioner
them is essential.
The traditional roles of lab professionals may be changing
by Maria Whitehead and Jenny LavenderHull and East Yorkshire Hospitals NHS Trust, UK
Experience
We enrolled a senior cardiac nurse and a senior radiographer to undertake training, each with around 10 year’s cath lab experience. Obviously an extensive knowledge of the procedure, equipment selection, potential problems and the ability to manage them is essential.
Coronary Angiography Coronary Angiography
them is essential.
The traditional roles of lab professionals may be changing
Product FocusPRODUCT INFORMATION
Medtronic Endeavor Drug Eluting Stent
The long awaited arrival of Medtronic’s drug eluting stent, the Endeavor™ is finally here. Although in some
countries it is still under investigational use we will give you a brief run down on the facts and figures.
Platform:
The popular Driver coronary stent system provides the platform for the Endeavor™. Already popular with physicians for its manoeuvrability and ease of use, the Driver is a cobalt alloy stent, meaning it is denser and stronger than traditional stainless steel stents, whilst having thinner struts.
Drug:
Licensed by Abbott Laboratories to Medtronic, the drug code named ABT-578 (zotarolimus), is believed to reduce restenosis in clogged arteries by preventing smooth cell proliferation. It achieves this by blocking the function of the cell cycle regulatory protein, mTOR, stopping the growth of new tissue.
Polymer:
The delivery matrix for the stent is coated with a Phosphorylcholine (PC) polymer, licenced from Abbott Laboratories, called PC Technology™. It is designed to slowly release the drug into the arterial wall.
Delivery System:
The Endeavor Drug Eluting Coronary Stent is intended to be released on Rapid Exchange, Over-the-Wire (USA), and Multi-Exchange technologies for International markets.
Trials:
These trials have been undertaken at various sites to determine the effectiveness of the Endeavor™ in reducing coronary artery restenosis.
Endeavor I: Safety and efficacy of Endeavor™ in de novo coronary lesions in native coronary arteries. Results: A 24-month target lesion revascularization (TLR) rate of 2.0 percent, and no additional cases of stent thrombosis in the 97 study patients who received follow-up over the second 12-month period.
Endeavor II: Compared the Endeavor™ stent to the traditional Medtronic Driver bare metal stent. Results: Demonstrated no observed cases of stent thrombosis between nine and 12 months in either study arm. A 12-month TLR rate of 6.0 percent for Endeavor™ patients, compared to 13.2 percent in the Driver control group.
Endeavor III: Compares the Endeavor™ against the Cypher™ drug-eluting stent marketed by Cordis Corporation, a Johnson & Johnson company. Results: Showed that Endeavor provides clinical and angiographic outcomes consistent with previous Endeavor trials and with no statistical differents between Endeavor and Cypher.
Endeavor IV: Compares the Endeavor™ against the TAXUS™ Paclitaxel-Eluting Coronary Stent System from Boston Scientific Corporation. Results: Still enrolling.
CORONARY HEART ™ 15
Medtronic Endeavor Drug-Eluting StentCourtesy Medtronic, Inc.
Medtronic Endeavor Drug-Eluting StentCourtesy Medtronic, Inc.
The delivery matrix for the stent is coated with a Phosphorylcholine (PC) polymer, licenced from Abbott Laboratories, called PC Technology™. It is designed to slowly release the drug into the arterial wall.
Delivery System:
The Endeavor Drug Eluting Coronary Stent is intended to be released on Rapid Exchange, Over-the-Wire (USA), and Multi-Exchange technologies for International markets.
These trials have been undertaken at various sites to determine the effectiveness of the Endeavor™ in reducing coronary artery restenosis.
Safety and efficacy of Endeavor™ in de novo coronary lesions in native coronary arteries. 24-month target lesion revascularization (TLR) rate of 2.0 percent, and no additional cases of stent thrombosis in the 97 study patients who received follow-up over the second 12-
Compared the Endeavor™ stent to the traditional Medtronic Driver bare metal stent. Demonstrated no observed cases of stent thrombosis between nine and 12 months in either study arm. A 12-month TLR rate of 6.0 percent for Endeavor™ patients, compared to 13.2 percent in the Driver control group.
Compares the Endeavor™ against the Cypher™ drug-eluting stent marketed by Cordis Corporation, a Johnson & Johnson company. Endeavor provides clinical and angiographic outcomes consistent with previous Endeavor trials and with no statistical differents between Endeavor and Cypher.
Compares the Endeavor™ against the TAXUS™ Paclitaxel-Eluting Coronary Stent System from Boston Scientific Corporation.
Latest NewsLATEST NEWS
CORONARY HEART ™ 13
World’s FirstBioabsorbable DES Trial BeginsMarch 9, 2006:
Guidant Corporation announced enrolment of the first patient in
a first-in-man clinical trial designed to evaluate the safety of a fully bioabsorbable everolimus eluting stent platform for the treatment of coronary artery disease.
“We are excited about our bioabsorbable drug eluting stent program, which is aligned with Guidant’s strategy of leveraging bioabsorbable technologies to provide innovative site-specific therapy for the
treatment of heart disease,” stated John M. Capek, Ph.D., president, Vascular Intervention, Guidant Corporation.The first implant was performed by a team headed by Drs. John Ormiston and Mark Webster at Auckland City Hospital, New Zealand. The ABSORB trial will enrol up to 60 patients in Belgium, Denmark, France, New Zealand, Poland and The Netherlands.
Visit www.guidant.com for more info
Siemens Unveil their Most Advanced CTMarch 3, 2006:
Siemens has pushed the technical and clinical boundaries of CT with this latest innovation, the
Somatom Definition, which is faster than every beating heart and capable of imaging full cardiac detail with as much as 50 percent less radiation exposure compared to traditional CT scans.
Setting new standards in cardiac diagnosis, the Somatom Definition will image patients with high or irregular heart rates, or even arrhythmia, without beta blocker medications that have been previously needed to slow a patient’s heart. The system also enables physicians to better identify and characterize plaque, an early indicator of heart disease.
The Somatom Definition has enhanced capabilities not previously available from any type of diagnostic imaging technology, which are expected to lead to new breakthroughs in clinical research. These capabilities include scanning with two different X-ray energies simultaneously, which allow physicians to better differentiate,
characterize, isolate and distinguish bone, soft tissue and fluid. With 0.33 seconds per rotation, electrocardiogram- (ECG) synchronized imaging can be performed with 83-millisecond temporal resolution, independent of the heart rate, resulting in motion free cardiac images.
The first Somatom Definition was installed at the University of Erlangen (Germany) in October 2005. “Siemens’ newest CT system provides very valuable clinical informationfor patients presenting in our department with acute chest pain and suspicion of coronary artery disease,” said Dr. Stephan Achenbach, associate professor of Cardiology, University of Erlangen. “We expect that the Somatom Definition will have a significant role in even the most demanding environments, such as emergency departments,”
added Prof. Werner Bautz, chairman of Radiology, University of Erlangen, Germany.
Visit www.medical.siemens.com for more information
treatment of heart disease,” stated John
Siemens press picture
treatment of heart disease,” stated John M. Capek, Ph.D., president, Vascular Intervention, Guidant Corporation.The first implant was performed by a team headed by Drs. John Ormiston and Mark Webster at Auckland City Hospital, New Zealand. The ABSORB trial will enrol up to 60 patients in Belgium, Denmark, France, New Zealand, Poland and The Netherlands.
Visit www.guidant.com for more info
added Prof. Werner Bautz, chairman of Radiology, University of Erlangen, Germany.
Visit www.medical.siemens.com for more information
treatment of heart disease,” stated John
Vol 1: Ed 1 International EditionVol 1: Ed 1 International Edition
coronaryheart.comJune 2006
“Especially for Cardiac Cath, EP, and Non-Invasive
Departments”
Using Magnetic Fields to fix Atrial Fibrillation
Lab Staff Performing Angiograms
Medtronic Endeavor DES Product Focus
EDUCATION &CONFERENCES
+ more...
EMP
LO
YMENT
Special Feature
LAB VISITSEpworth Hospital, AustraliaEast Surrey Hospital, UK
UK
Australia
New Zealand
MEDIA KIT 2006
Special Prices...
30% off* August 2006 issue.
(* does not apply to Buyers Guide Listing and New Products in-use)
For details contact:[email protected]
The new magazine designed for managers and staff working in cardiac cath / EP labs, and non-invasive departments.Distributed to UK, Australia, and NZ.
2006
coronaryheart.com
RecruitmentAdvertising Rates
Special Prices...
AdministratorsManagersCardiac NursesCardiac PhysiologistsEchocardiographersRadiographersCardiac IndustryOther Cardiac Professions
••••••••
AUSTRALIA
UNITED KINGDOM
NEW ZEALAND
AUSTRALIA
50% off August 2006 issue.
25% off September 2006 issue.
For details contact:[email protected]
2006200620062006200650% off August 2006
25% off September
2006200620062006200650% off August 2006
Like to Advertise?
Download our Media Kits
Onlinecoronaryheart.com

MEDICAL IMAGING
RAO 10
RAO 10
Objective:
Th is angle is usually taken as the fi rst image in the series. Engaging the left coronary system usually occurs in AP, however the catheter seen in the distal aorta usually overlaps the left main artery, possibly obscuring a narrowing. As soon as the catheter is engaged, the radiographer (or whoever is moving the detector) should immediately angle RAO to clear the left main of the distal catheter. Th is is usually 10 degrees however can sometimes be as much as 20 degrees. If necessary, consult your cardiologist for initial projections greater than 15 degrees.
Th is projection is good for a quick assessment of the left main artery, however can be slightly foreshortened and overlapped by the proximal circumfl ex. It is good for the mid circumfl ex and obtuse marginal branch. Th e proximal circumfl ex is diffi cult to visualise due to foreshortening, as it is seen end on as it bifurcates from the left main artery. Th e LAD is diffi cult to visualise due to overlapping by the diagonal branches.
Alternatives:
More RAO (eg. RAO 30):
Left main becomes completely overlapped by the circumfl ex. Th e LAD is perpendicular the detector in this view however is often overlapped along its length by diagonals and septals
Less RAO (eg. AP):
Demonstrates the proximal left main free from overlap however suff ers from foreshortening. Th is view is good for demonstrating the mid / distal circumfl ex. Th e proximal LAD and circumfl ex are overlapped, with the obtuse marginal often overlapping the mid / distal LAD. Beware that the catheter seen in the descending aorta often obscures the left main / proximal LAD.
RAO 10
LM Left Main
LAD Left Anterior Descending
D1 Diagonal
LCX Circumflex
OM1 Obtuse Marginal 1
30 CORONARY HEART ™

RAO 30 / CAU 20MEDICAL IMAGING
RAO 30 / CAU 20
Objective:
Th is angle is used primarily to demonstrate the Left Main and the Circumfl ex arteries, and is the best view for demonstrating the proximal Obtuse Marginal branch. Th e Left Anterior Descending artery is also seen however is often overlapped by the Diagonal branches. Acquisition time should be long enough to obtain adequate contrast fi lling of the distal arteries, and if necessary pan to the anatomical right to visualise collateral fi lling of the Right Coronary artery. Visualising the right coronary artery fi lling distally may assist Cardiologist of the possible lesion length occurring in that artery.
Alternatives:
More CAU (eg. RAO 30 / CAU 40):
Th is decreases the foreshortening of the proximal circumfl ex improving visualisation. Th e distal circumfl ex can be foreshortened and overlapped by distal branches. Foreshortening of the LAD occurs mid /distal with overlap of the diagonal branches.
Less CAU (eg. RAO 30 / CAU 10):
Increases foreshortening of proximal circumfl ex, however improves visualisation distally by separating the distal branches. Th e obtuse marginal is often overlapped by large septals from the LAD or diagonal branches.
More RAO (eg. RAO 40 / CAU 20):
Th is separates the diagonal branches further from the LAD, demonstrating them inferior to the LAD. Th is view can also improve visualisation of the mid / distal Obtuse Marginal branch
Less RAO (eg. RAO 10 / CAU 20):
Th is separates the diagonal branches further from the LAD, demonstrating them superior to the LAD.
RAO 30 / CAU 20
LM Left Main
LAD Left Anterior Descending
D1 Diagonal
LCX Circumflex
OM1 Obtuse Marginal 1
CORONARY HEART ™ 31
RAO 30 / CAU 20
CORONARY HEART ™ 31
RAO 30 / CAU 20

Conferences 2006CONFERENCES
32 CORONARY HEART ™
June 14-17CardioStim 2006Location: Nice, FranceWebsite: www.cardiostim.fr
June 17-20Heart Failure CongressLocation: Helsinki, FinlandWebsite: www.escardio.org
June 28-30Cardio Alex 2006Location: Alexandria, Egypt Website: www.cardioalex.com
July 6-7Stress Echo at King’sLocation: London, UKWebsite: www.stressechoatkings.com
July 7Symposium on Cardiovascular Disease in WomenLocation: London, UKEmail: [email protected]
July 14-16ASUM NZ Branch 2006 Annual ConferenceLocation: Napier, New ZealandWebsite: www.asum.com.au
July 19-21XII Congress of SOLACILocation: Porto Alegre, BrazilWebsite: www.solaci-sbhci2006.org
August 4-754th ASM of the Cardiac Society of Australia and New ZealandLocation: Canberra, AustraliaWebsite: www.csanz.edu.au
August 10-12Australian Cardiac Rehabilitation Association 16th Annual ConferenceLocation: Melbourne, AustraliaContact: [email protected]
August 12-13Advanced Angiography 2006 - LIVELocation: National Heart Centre, SingaporeWebsite: www.singlivecourse.com
September 2-6World Congress of Cardiology 2006Location: Barcelona, SpainWebsite: www.worldcardio2006.org
September 9-13Cardiovascular and Interventional Radiological Society of Europe (CIRSE)Location: Rome, ItalyWebsite: www.cirse.org

Conferences 2006-2007CONFERENCES
CORONARY HEART ™ 33
September 15-17ASUM 2006 Annual Scientifi c MeetingLocation: Melbourne, AustraliaWebsite: www.asum.com.au
September 19-21Heart Rhythm CongressLocation: Birmingham, UKWebsite: www.ukheartrhythm.org.uk
September 20-23CCT 2006 Complex Catheter TherapeuticsLocation: Kobe, JapanWebsite: www.cct.gr.jp
October 5-7Annual General Meeting of the Irish Cardiac SocietyLocation: Killarney, IrelandWebsite: www.irishcardiacsociety.com
October 21-24Acute Cardiac CareLocation: Prague, Czech RepublicWebsite: www.escardio.org
October 22-27TCT 2006: Transcatheter Cardiovascular TherapeuticsLocation: Washington DC, USAWebsite: www.tct2006.com
LIST YOUR CARDIAC
CONFERENCEHERE FREE
Email the details to:[email protected]
October 27-28British Society of Echocardiography Annual Clinical & Scientifi c MeetingLocation: Bournemouth, UKWebsite: www.bsecho.org
Nov 26 - Dec 1RSNA 2006Location: Chicago, USAWebsite: www.rsna.org
December 6-9EuroEcho 10Location: Prague, Czech RepublicWebsite: www.euroecho.org
January 24-26Advanced Angioplasty 2007Location: London, UKWebsite: www.advancedangioplasty.co.uk

Global Heart ReportsGLOBAL HEART
Study shows deaths fromcardiovascular disease due to excess body weight
Heart Foundation to launch new healthy weight campaign
New research commissioned by the National Heart
Foundation of Australia has confi rmed thousands of Australians die from cardiovascular disease (heart, stroke and blood vessel disease) every year because they are overweight.
According to Dr Lyn Roberts, CEO – National, Heart Foundation, “Th e risk associated with cardiovascular disease as a result of carrying excess weight is real and quantifi able.”
Research undertaken by the University of Queensland’s Centre for Burden of Disease and Cost Eff ectiveness, estimates up to 7,000 Australians died in 2003 from cardiovascular disease* as a result of excess body weight. Th e study also confi rmed the connection
between excess weight, diabetes and cardiovascular disease and found 70 percent of people with diabetes died from cardiovascular disease.
Th e fi ndings have prompted the Heart Foundation to develop a practical new campaign called the Walk of Life - for all walks of life to educate Australians about the importance of walking and healthy eating to prevent unhealthy weight gain and to improve cardiovascular outcomes. Th e campaign encourages realistic lifestyle changes and provides practical resources to help the community achieve and maintain a healthy weight.
“Sedentary lifestyles and poor eating habits are placing Australians at greater risk of dying from cardiovascular disease as a result of excess weight gain,” Dr Roberts said. “Urgent action is required to curb the increasing prevalence of
excess weight and to provide assistance to those who are already overweight.”
During Heart Week (30 April - 6 May 2006), the Heart Foundation called on all sectors of the Australian community to work together to address Australia’s excess weight epidemic. Th e Walk of Life – for all walks of life campaign is an integral part of the Heart Foundation’s Healthy Weight action plan titled Addressing Australia’s Weight Problem.
Resources are available from the Heart Foundation by calling Heartline on 1300 36 27 87 or at www.
heartfoundation.com.au/walkofl ife Th ey include a new healthy weight booklet and pocket guide with further material available in the coming months.
More than 7 million Australian adults are estimated to be overweight and more than half of Australian adults are not reaching recommended levels of physical activity despite numerous studies showing that moderate intensity physical activity, on most days of the week, for about half an hour, provides maximum population health benefi ts.
“We’re working to help Australians lead healthier lifestyles, so we can reduce the incidence of cardiovascular disease, which remains the leading cause of death and a major source of disability in Australia, killing one Australian adult every ten minutes,” said Dr Roberts.
AUSTRALIA
“More than 7 million Australian adults are estimated to be overweight”
34 CORONARY HEART ™

Per Serving Nutritional InformationTotal Fat (g): 10g 16%Saturated Fat (g): 1g 7%Monounsaturated Fat (g): 6g 27%Polyunsaturated Fat (g): 2g 9%Cholesterol (mg): 25mg 8%Total Carbohydrate (g): 56g 19%Dietary Fiber (g): 4g 16%Protein (g): 12g 24%Sodium (mg): 50mg 2%Potassium (mg): 908mg 26%Calcium (mg): 64mg 6%Iron (mg): 3mg 17%Zinc (mg): 1mg 6%Vitamin C (mg): 141mg 235%Vitamin A (i.u.): 12477IU 250%Vitamin A (r.e): 1251RE 125%Vitamin B6 (mg): 7mg 36%Vitamin B12 (mcg): 1.4mcg 24%Thiamin B1 (mg): 2mg 15%Ribofl avin B2 (mg): 4mg 24%Folacin (mcg): 95mcg 24%Niacin (mg): 5mg 27%Niacin (mg): 5mg 27%
* Percent Recommended Daily Values are based on a 2000 calorie diet.
To Serve 4
Fish4 x 180g Ocean Trout Fillets (Skin On) or Atlantic Salmon
Stack1 x Sweet Potato (Peeled and sliced)1 x Zucchini (Courgette) (Cut into 5mm slices)4 x handfuls Baby Spinach (Blanch & refresh in iced water)4 x large fi eld Mushrooms (Oven Roasted with Stem off )2 x Red Capsicum (Oven Roast until golden and peel)
Balsamic Essence500ml Balsamic Vinegar1 cup Icing sugarJuice of 1 lemon
Heat a heavy pan and add 1 table spoon of Extra Virgin Olive Oil. Lay the Trout fi llets skin side down in the pan and brush the top side with olive oil. Season with salt and pepper. Place in an oven pre heated to 200c and cook for 10 minutes.Alternative to the oven is to BBQ the Fish
Using an 8cm scone cutter, pack the roasted vegetables into the inside in the above order to form a symmetrical stack and remove the cutter. Th e stacks can be put into the oven to heat at the same time as the trout.
For the Balsamic Essence, put all ingredients into a pot and reduce by half and cool. Th is is best done the day before. Pour the essence into a squeegy bottle and leave in the fridge for further use.
To ServeTake 4 main sized plates and pour on some balsamic essence. Place the stack in the centre and rest the Trout on top, skin side up. Brush the skin with olive oil to give it sheen. Garnish with Chervil sprigs and serve.
2004 Finalist in Best New Restaurant in Australia
Situated in the City of Devonport, In the beautiful State of Tasmania, Australia
www.thedeckcafe.com.au
Grilled Ocean Trout on Vegetable Stack with Balsamic EssenceGrilled Ocean Trout on Vegetable Stack
Cradle Mountain, Tasmania. A short
drive from The Deck
Healthy HeartHEALTHY HEART
CORONARY HEART ™ 35Troy Baggett, Manager & Head Chef

Cardiac DeutschLANGUAGES
English German Phonetic
Yes Ja Yarr
No Nein Nine
Don’t move. Nicht Bewegen. Nisht Beveegen
Breathe in. Einatmen. Eye-n-art-men
Hold your breath. Atem anhalten. Artem Arn-harl-ten
You can breathe. Ausatmen. Ows-art-men
Turn your head left.den Kopf nach links drehen.
den kopf nar links draa-hen
Turn your head right.den Kopf nach rechts drehen.
den kopf nar recks draa-hen
We don’t serve beer here.
Wir schenken hier kein Bier aus.
Veer shenkn he-a-ke-an beer oss
Turn your head left.den Kopf nach links drehen.
den kopf nar links draa-hen
Turn your head right.den Kopf nach rechts drehen.
den kopf nar recks draa-hen
We don’t serve beer here.
Wir schenken hier kein Bier aus.
Veer shenkn he-a-ke-an beer oss
Neuschwanstein Castle, Bavaria, Germany
Let’s LearnGerman
Every so often cardiology staff are faced with an interesting dilemma; an
inability to speak a patient’s native tongue. Some people try to employ sign language to communicate, whilst others begin shouting, with the strange belief that the patient will suddenly begin understanding English. How embarrassing!!
Here at Coronary Heart™ we have come to the rescue. Each main issue contains language assistance to help staff in the cardiac environment, with common instructions in English converted into the foreign language equivalent. For further assistance we have also included the phonetic pronunciations (how to say it). Let’s startwith German.
GERMANY
Danke schön. Auf Wiedersehen!
36 CORONARY HEART ™36 CORONARY HEART ™

Mt CookNew Zealand
Broaden YourHorizon
UK
AUSTRALIA
NEW ZEALAND
Coronary Heart’s Employment pages are distributed free monthly to Cardiac Departments and Labs in the UK, Australia, and New Zealand.
Jobs are also placed free online.
Visit coronaryheart.com and download the
Media Kit
Why advertise jobs in just one Country?
Materials Due
Publication Date
18th of each month
1st of each month
Reservations Due 15th of each month (Agency only)
Mt Cook
Media Kit
15th of each month (Agency only)
50% off Advertising*
AugustIssue
* EMPLOYMENT

View Job Ads Online
coronaryheart.com
Don’t Just Advertise Jobs in
Black & White
Add Colour at No Extra
Cost
EMPLOYMENT ADVERTISING
38 CORONARY HEART ™
UNITED KINGDOM June / July 2006
Radiographer, Band 5 or 6 (Depending on experience)
Due to the expansion of the Cardiac Angiography Service at East Surrey Hospital, a vacancy has arisen for a radiographer to join the team. We are looking for an enthusiastic radiographer, preferably with experience in diagnostic cardiac work, but training is available. This is a split role, and the successful candidate will rotate through the main Diagnostic Imaging Department, where there is the full range of modalities expected in a busy acute hospital. (CT, MRI, Nuclear Medicine)
For an Informal visit or enquiry contact Mrs. Hafiza Abba, Cardiac Superintendent Radiographer, or Andrew Millard, District Superintendent Radiographer, on 01737-231601.
Cardiac Physiologists, Band 5 or 6 (Depending on experience)
Following the expansion of the Cardiac Angiography service at East Surrey Hospital to include PCI, a vacancy has arisen for a cardiac physiologist to join the team at this busy acute hospital. We are looking for an enthusiastic individual, with a range of skills including invasive and non-invasive testing. Experience of pacing implantation and follow up would be beneficial although training would be available. The successful candidate will be required to rotate through the angiography suite and the non-invasive department.For an informal visit or enquiry contact Rachel Danvers, Chief Cardiac Physiologist, on 01737 768511 ext 2039/ 1661.
Closing date for both positions July 10, 2006.
East Surrey Hospital As seen in this Issue

Greenslopes Private Hospital“Australia’s Best Private Hospital” Awarded by the Australian Private Hospitals Association in the 2004 Hospital Award for Excellence.
Greenslopes Private Hospital is Australia’s largest private hospital & one of the fastest growing hospitals in Queensland.
At Greenslopes, we offer a diverse range of surgical specialty procedures, & with 10 operating theatres (soon to be 14) we boast state-of-the-art digitaltheatre technology.
Cardiology & Cardiothoracic NursesRegistered Nurses & Endorsed Enrolled NursesFull Time, Part Time, Flexible Short Shifts.Our peri-operative team enjoys:
• Flexible rostering• Excellent Educational opportunities (internal & external)• Opportunities for advancement• Work/life balance
Benefi ts of working at Greenslopes also include: On-site child care centre, free car parking, subsidised meals, a progressive wellness program including gymnasium, an active social club & salary packaging.
If you would like to join our team please forward your curriculum vitae, application letter including the names & contact numbers of two professional referees.If you have any further queries please call Anita on +61 7 3394 6745.
Send applications to:Anita Hoffman, Clinical Recruitment Coordinator, Greenslopes Private HospitalNewdegate Street, GREENSLOPES QLD 4120email: [email protected]
medicalENGLANDNEW ZEALANDAUSTRALIA
* Exclusive Contracts, Nationwide positions* Special Ltd Company Rates / Setup* Accommodation & Banking Advice / Accounts* Efficient, Friendly & caring service* Experienced staff who understand your needs* Work permit assistance / Visa* We pay for CRB
Join The Agency That Sets The Standards, Excellent Rates, Plus Benefits Package.
www.sonographersmedical.co.uk UK: Tel: 0845 226 1 226 E mail: [email protected]
www.sonographersmedical.co.nzEmail:[email protected]
Providing Staff to the Cardiac Industry
EchocardiographersCath Lab RadiographersCardiac Physiologists
www.sonographersmedical.com.auEmail: [email protected]: 1300 766 745
CONGRATULATIONS Coronaryheart
CONSULTING EDITORSAll Cardiac Modalities
Our mission is to provide a free educational publication to selected cardiac departments throughout the world, improving the knowledge of cardiac departments, which ultimately results in improved patient care. We aim to extend from wealthy western hospitals to the poorer third world community health centres. Free publishing available in Print or Online allows us to reach all audiences around the world.
We require volunteer consulting editors from all cardiac modalities to assist with reviewing articles before publication. So if you have previous editing / medical writing experience, or are just very knowledgable in your chosen career, we want to hear from you.
Forward your CV with references to:
Tim LarnerCoronary Heart Publishing Ltd2nd Floor145-157 St John StreetLondon, EC1V 4PYUnited Kingdomor email to: [email protected]
EMPLOYMENT ADVERTISING
CORONARY HEART ™ 39
INTERNATIONAL June / July 2006

Worked hard on a paper/article that only your colleagues get to see?Share your knowledge with everybody.
Submit it, and we may publish it. Visit the website for more details
coronaryheart.com
Worked hard on a paper/article that only your colleagues get to see?
You Submit We Review
Your Paper Goes Free!!
•
•
•
Cath / EP & Non-Invasive
Education
ManagersNurses
PhysiologistsRadiographers
Echo
Free Your Papers
Worked hard on a paper/article that only your colleagues get to see?
coronaryheart.comcoronaryheart.comWe give you
£50 if published