Conquest - Spring 2008
28
CONQUEST V O L U M E 2 2 I S S U E 4 S P R I N G 2 0 0 8 TRACKING FORERUNNER GENES
-
Upload
md-anderson-cancer-center -
Category
Documents
-
view
215 -
download
2
description
Cover story: scientists have identified forerunner genes, whose activation paves the way for silencing tumor-suppressing genes and jump-starts cancer development.
Transcript of Conquest - Spring 2008
CONQUESTV O L U M E 2 2 I S S U E 4S P R I N G 2 0 0 8
CONONO QQQNQN UQUQ ESUESU TV O L U M E 2 2 I S S U E 4S P R I N G 2 0 0 8
TRACKING FORERUNNERGENES

m i S S i O N
The mission of
The University of Texas
M. D. Anderson Cancer Center
is to eliminate cancer in Texas,
the nation, and the world through
outstanding programs that
integrate patient care, research and
prevention, and through education
for undergraduate and graduate
students, trainees, professionals,
employees and the public.
V i S i O N
We shall be the premier
cancer center in the world,
based on the excellence of our
people, our research-driven
patient care and our science.
We are Making Cancer History.
C O r E V a L U E S
CaringBy our words and actions,
we create a caring environment for everyone.
integrityWe work together to merit
the trust of our colleagues and those we serve.
discoveryWe embrace creativity and
seek new knowledge.
On the Cover:Bogdan Czerniak, M.D., Ph.D., and colleagues have identified and charted the location of key forerunner genes, which drive the initial growth of precancerous cells and set in motion the beginning stages of cancer.
Check out the Conquest Web site at www.mdanderson.org/conquest
2 FRONTLINE
One More Reason Not to Smoke
1 9 PROFILE
Ernest T. Hawk, M.D.
1 6 SYMPTOM RESEARCH
Steps to Validation
2 FRONTLINE
One More Reason Not to Smoke
2 4 MOVING FORWARD
Moira Podgurski
2 2 CANCER BRIEFINGS
ASPIRE Kicks Butt
Reducing Cancer Risk Naturally
1 9 PROFILE
Ernest T. Hawk, M.D.
1 6 SYMPTOM RESEARCH
Steps to Validation
F E A T U R E S
8
14
5
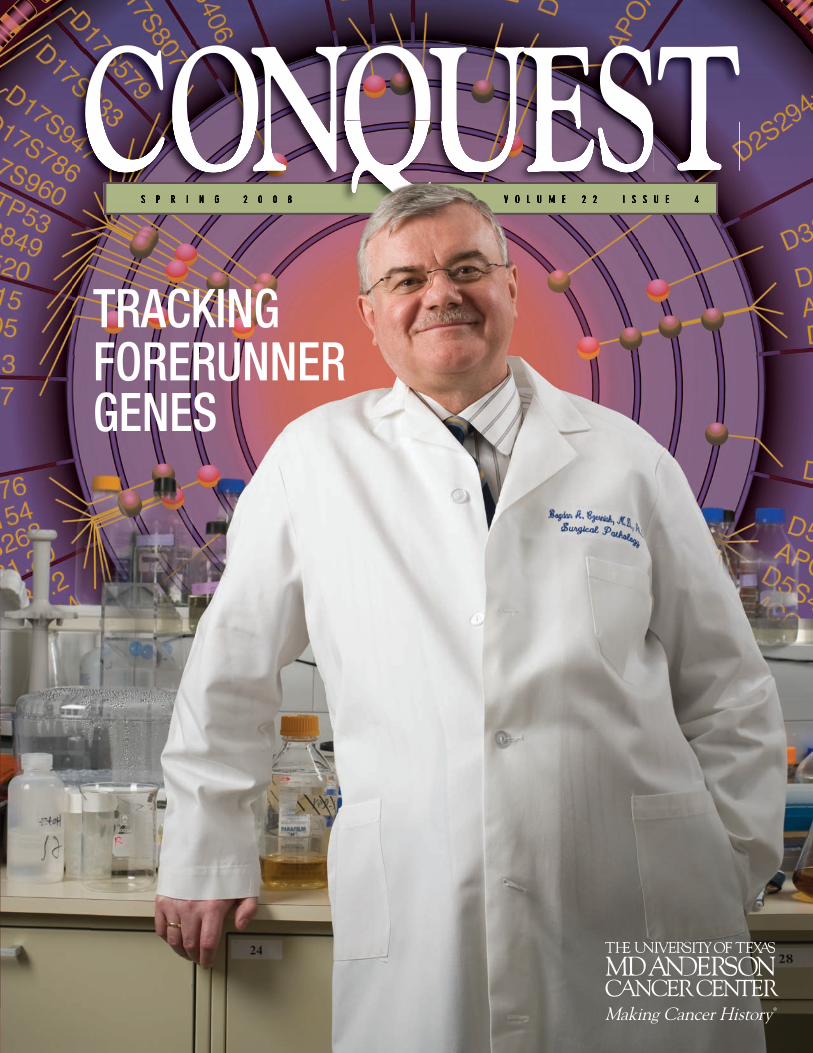
CANCER’S IGNITION SWITCH
Scientists have identified forerunner genes, whose
inactivation paves the way for the silencing
of tumor-suppressing genes and jump-starts
cancer development.
CONTENTSS p r i N g 2 0 0 8
C O N Q U E S T
LIFE IS FULL OF ADVENTURES
One Saturday every month, elementary school children come to
M. D. Anderson to learn everything from how to package medicine
to what goes on in the operating room.
A PERSONAL INVESTMENT
David H. Koch’s $18 million gift will bring together
basic, translational and clinical scientists to
rapidly move scientific findings to patients with
genitourinary cancers.

2
C O N Q U E S T
S P R I N G 2 0 0 8 FRONTLINE
“This is the first study to identify a common genetic vari-ant that influences the risk for developing lung cancer,” says lead author Chris Amos, Ph.D., professor in M. D. Anderson’s Department of Epidemiology. The variants are present in about one-half of the Caucasian population studied.
The paper, reported in the April 2 online edition of Nature Genetics, is one of three published by Nature this spring from three unique teams that have identified the same genetic location as being associated with increased lung cancer risk. The findings are a major step forward in identifying those at high risk for non-small cell lung cancer and for understanding how smoking and genetic factors interact to cause the disease.
“The major risk factor for developing lung cancer is cigarette smoking,” Amos says. “What we don’t understand is why some long-term smokers develop lung cancer and others don’t. There are so many different cancer-causing compounds in tobacco smoke that it’s hard to separate them, and we don’t fully understand the mechanisms that cause lung cancer.”
While all smokers and former smokers are at higher risk for lung cancer, less than 20 percent of these “ever smokers” eventually develop the disease. “We need to get a better handle on how genetic factors increase risk and what molecular pathways are involved in development of lung cancer,” Amos says.
Growing body of evidenceThe research team, comprising scientists from
M. D. Anderson, Johns Hopkins University, and the Institute for Cancer Research and the University of Cambridge in the United Kingdom, pinpointed two spots of genetic variation on chromosome 15.
The two variants are single-nucleotide polymorphisms (SNPs, pronounced “snips”), places in the human genome that vary by a single DNA chemical building block or nucleotide. Scientists found that individuals who have ever smoked and who have one or two copies of either of these SNPs have increased risks ranging from 28 percent to 81 percent of developing lung cancer.
The team’s findings also might provide support for a growing body of evidence suggesting that nicotine, long known as the prime addictive compound in cigarettes, might also play a direct causative role in the development of lung cancer.
There are five genes in the area of chromosome 15 where the two, risk-raising SNPs were identified, Amos explains. Of those, three are nicotine acetylcholine receptor genes that encode proteins that serve as docking sites to which nicotine can bind.
“Once bound, these receptors set in motion a cascade of signals. Nicotine is known to activate cell proliferation, new blood vessel development and growth factors while up-regulating several signaling pathways. If these are indeed causal genes, that will be of great interest,” Amos says.
ONe MORe ReaSON NOt tO SMOke
If you smoke, or have ever smoked, read on.a team led by M. D. anderson scientists discovered that two commonly inherited genetic variations are associated with an increased risk of lung cancer for smokers and former smokers.

a team led by Chris
amos, Ph.D., and
Margaret Spitz, M.D.,
has identified specific
genes that increase
lung cancer risk and
which may explain how
smoking and genetic
factors interact to
cause the disease.
Another potential causative gene in the area is one that encodes a component of the proteasome, which degrades other proteins. The function of the fifth gene has yet to be identified.
Further studies with additional SNPs in African-American populations who show different SNP patterns may help to define which of these five genes causes lung cancer. Collaborations with scientists representing both M. D. Anderson’s Lung Specialized Programs of Research Excellence grant and the Robert J. Kleberg, Jr. and Helen C. Kleberg Center for Molecular Markers will evaluate whether these SNPs influence expression of any of these five genes in lung cancers and normal lung tissue, according to Amos.
An exhaustive searchAmos and senior co-author Margaret Spitz, M.D., chair
of M. D. Anderson’s Department of Epidemiology, conceived the study, which follows on evidence from epidemiological research indicating a two-fold increase in lung cancer risk for first-degree relatives of lung cancer patients.
To pinpoint genetic variations, the team conducted a series of genome-wide association studies, first genotyping 317,498 different SNPs among 1,154 former and current smokers who developed lung cancer and were seen at M. D. Anderson and 1,137 matched ever-smoker controls in Houston.
This first phase of the study narrowed the search to 10 SNPs, which were then genotyped in 711 additional cases and 632 controls from the same Houston population to identify the final two SNPs. A second replication phase was conducted among 2,013 ever-smoker lung cancer cases and 3,062 controls in the United Kingdom.
To minimize confusion among risk factors and to increase the study’s ability to pinpoint genetic effects, controls were matched to lung cancer cases according to smoking behav-ior, age and sex. Former smokers were matched by years since they stopped smoking. The study was performed first in Caucasians to minimize the effect of ethnic genetic variation.
3

The team carefully analyzed its findings to exclude the possibility that the elevated risk from the two SNPs was attributable to their asso-ciation with heavier smoking. They reported that the study showed a weak effect (of these two SNPs) on smoking behaviors and an extremely significant effect on lung cancer risk, whether or not adjustment for smoking behavior was made during the analysis.
The genetic variations might help identify smokers at higher lung cancer risk who would be the best candidates for screening. And they may be useful to gauge the risk of other smoking-related cancers, such as cancers of the esophagus, bladder, head and neck, and pancreas. A similar genome-wide study of African-American smokers is planned.
Invaluable supportResearch was funded principally by the National Cancer Institute
(NCI) of the National Institutes of Health (NIH). The Kleberg Center for Molecular Markers, the Flight Attendants Medical Research Institute and the Allan J. Lerner Fund also helped support the study.
Genotyping was conducted by the Center for Inherited Disease Research, which is funded by an NIH contract to Johns Hopkins University, and in the laboratory of Xifeng Wu, M.D., Ph.D., professor in M. D. Anderson’s Department of Epidemiology, as well as at the Institute for Cancer Research in the United Kingdom.
Lung cancer patients and controls for the Texas components of the study came from a 17-year M. D. Anderson lung cancer epidemiological study, which was funded by NCI and led by Spitz.
“We’re very indebted to the patients who’ve participated in the study,” Spitz says. “There’s no immediate benefit to the patients them-selves, but they willingly agree to participate in our research and their help has been invaluable. Being able to conduct this analysis should be useful to future generations who develop lung cancer.”
— Scott Merville
Did You Know?
Lung cancer is the leading cause of death
among men and women, killing more than
160,000 Americans annually and millions
worldwide. Non-small cell lung cancer makes
up 85 percent of all lung cancer cases.
FRONTLINEFRONTLINEWith Di Zhang’s help, Xifeng Wu, M.D., Ph.D., (right) and colleagues conducted a series of genome-wide association studies that
pinpointed the location of two common genetic variations associated with an increased risk of lung cancer.
Source: American Cancer Society
4
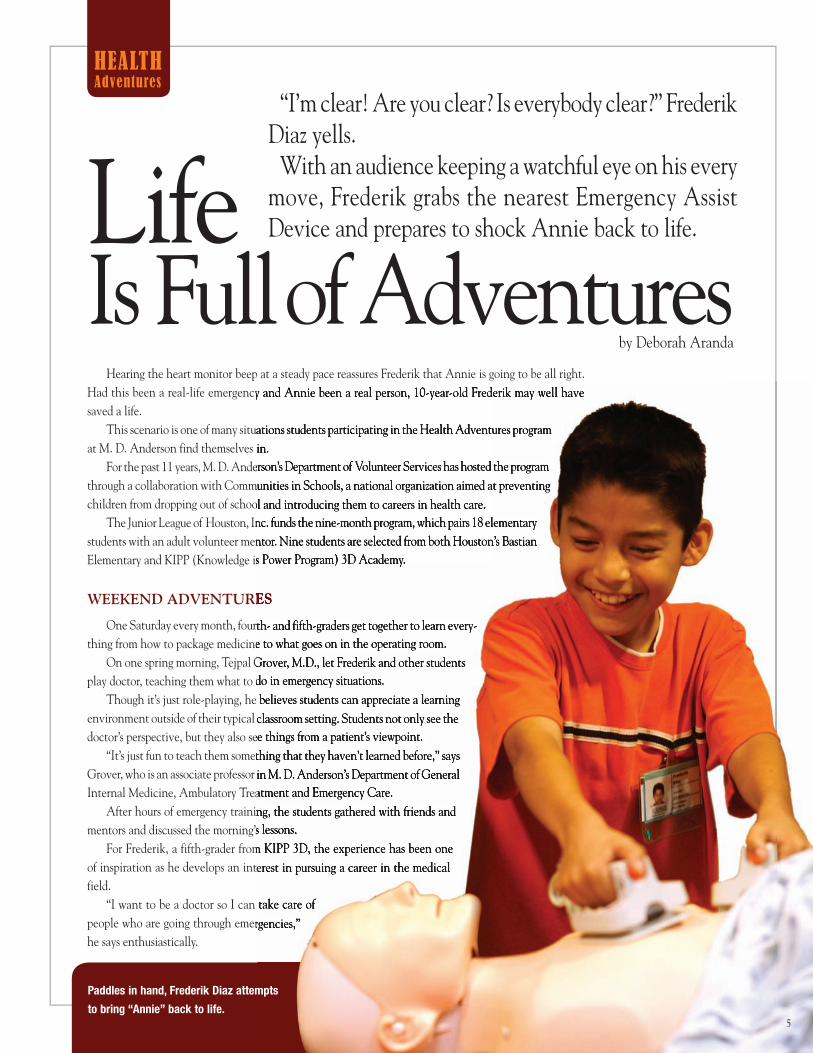
Hearing the heart monitor beep at a steady pace reassures Frederik that Annie is going to be all right.Had this been a real-life emergency and Annie been a real person, 10-year-old Frederik may well have saved a life.
This scenario is one of many situations students participating in the Health Adventures program at M. D. Anderson find themselves in.
For the past 11 years, M. D. Anderson’s Department of Volunteer Services has hosted the program through a collaboration with Communities in Schools, a national organization aimed at preventing children from dropping out of school and introducing them to careers in health care.
The Junior League of Houston, Inc. funds the nine-month program, which pairs 18 elementary students with an adult volunteer mentor. Nine students are selected from both Houston’s Bastian Elementary and KIPP (Knowledge is Power Program) 3D Academy.
wEEkENd adVENTUrES
One Saturday every month, fourth- and fifth-graders get together to learn every-thing from how to package medicine to what goes on in the operating room.
On one spring morning, Tejpal Grover, M.D., let Frederik and other students play doctor, teaching them what to do in emergency situations.
Though it’s just role-playing, he believes students can appreciate a learning environment outside of their typical classroom setting. Students not only see the doctor’s perspective, but they also see things from a patient’s viewpoint.
“It’s just fun to teach them something that they haven’t learned before,” says Grover, who is an associate professor in M. D. Anderson’s Department of General Internal Medicine, Ambulatory Treatment and Emergency Care.
After hours of emergency training, the students gathered with friends and mentors and discussed the morning’s lessons.
For Frederik, a fifth-grader from KIPP 3D, the experience has been one of inspiration as he develops an interest in pursuing a career in the medical field.
“I want to be a doctor so I can take care of people who are going through emergencies,” he says enthusiastically.
“I’m clear! Are you clear? Is everybody clear?” Frederik Diaz yells.
With an audience keeping a watchful eye on his every move, Frederik grabs the nearest Emergency Assist Device and prepares to shock Annie back to life.Life
Is Full of Adventuresby Deborah Aranda
HealtH
adventures
Had this been a real-life emergency and Annie been a real person, 10-year-old Frederik may well have
This scenario is one of many situations students participating in the Health Adventures program at M. D. Anderson find themselves in.
For the past 11 years, M. D. Anderson’s Department of Volunteer Services has hosted the program through a collaboration with Communities in Schools, a national organization aimed at preventing children from dropping out of school and introducing them to careers in health care.
The Junior League of Houston, Inc. funds the nine-month program, which pairs 18 elementary students with an adult volunteer mentor. Nine students are selected from both Houston’s Bastian Elementary and KIPP (Knowledge is Power Program) 3D Academy.
wEEkENd adVENTUrES
One Saturday every month, fourth- and fifth-graders get together to learn every-thing from how to package medicine to what goes on in the operating room.
On one spring morning, Tejpal Grover, M.D., let Frederik and other students play doctor, teaching them what to do in emergency situations.
Though it’s just role-playing, he believes students can appreciate a learning environment outside of their typical classroom setting. Students not only see the doctor’s perspective, but they also see things from a patient’s viewpoint.
“It’s just fun to teach them something that they haven’t learned before,” says Grover, who is an associate professor in M. D. Anderson’s Department of General Internal Medicine, Ambulatory Treatment and Emergency Care.
After hours of emergency training, the students gathered with friends and mentors and discussed the morning’s lessons.
For Frederik, a fifth-grader from KIPP 3D, the experience has been one of inspiration as he develops an interest in pursuing a career in the medical
“I want to be a doctor so I can take care of people who are going through emergencies,”
Paddles in hand, Frederik Diaz attempts
to bring “annie” back to life.5

Coming into their own
Cindy Shursen, Health Adventures program coordinator at M. D. Anderson, has seen how students have flourished in the program, which was initiated by the American Society of Directors of Volunteer Services in 1996, and is now offered in hospitals throughout the United States.
“The kids really come out of their shells,” she says. “Some of the kids that come in are really shy at first, then as they progress through the program, they begin asking questions and volunteering for participation.”
The program is a good fit for students who have an interest in the medical field, but also for those who may be having trouble academically, Shursen says.
During the school year, students are introduced to different areas throughout the hospital and have a day of activities planned for each visit. Before their final Saturday stop in the emergency room, they already had spent time with nurses, pharmacists, child life specialists, and physical and occupational therapists, and learned about sterile processing, radiation oncology and laboratory medicine.
On the last day of the program, mentors and site hosts unite, making it a special one to remember.
“I’ll make books for the kids with famous motivational quotes that they get to keep,” Shursen says. “We have a graduation ceremony and hand out diplomas. At the end of the ceremony, the kids toss their caps. Every year it’s a lot of fun and extremely rewarding.”
Something more to gain
Students aren’t the only ones benefiting from the Health Adventures program. Medical professionals and volunteers also have gained something valuable — the satisfaction of making a difference in a child’s life.
That’s been the case for Osvaldo Gomez, who’s been a volunteer mentor for the past five years.
“It’s so critical for kids to have caring adults in their lives, and some of these kids go home to a very challenging environment,” he says. “They’re bringing a lot of challenges to the program already, so to be a part of their lives for these nine months is very important to me. That’s one of the reasons I got involved.”
Gomez, a human resources specialist at M. D. Anderson, says the program has contributed to his learning about the diverse world of medicine.
“I get a chance to experience and see things within the hospital that I wouldn’t normally see as an employee, like the operating room, rehabilitation center or radiology,” he says. “I read about them, I work with some of the staff involved, but this program really gives me a chance to be in the middle of seeing first-hand what these areas are all about.”
Sally Fernandez, nurse manager for the Emergency Center, has been a work-site host since the program started. Motivating
HealtH
adventures
Brittany Cisneros (right) gets her blood pressure
checked as Alondra Ortiz waits her turn.
Below, Brittany teams with her mentor Laurie Elmore
in the laboratory to conduct several experiments.
6
students to keep attending school has been an enjoyable experience for her. “It’s always great to help them stay in school and get them excited about continuing their studies. Get them focused, not off track,” she says.
According to Shursen, students in higher-grade levels are more prone to quit school, which is why the Health Adventures program focuses on elementary school-age children. The goal is to reach students early and get them excited about staying in school and seeing what career opportunities are available to them.
Like Frederik, 12-year-old David Espinoza feels fortunate to be in such a program. “I learned how to take care of people and what to do if they had a heart attack or were on the ground,” he says. “I like this program. We’re lucky that we’re here.”
Future plans for the Health Adventures program include having a reunion for mentors and past students involved. “This program continues to evolve every year,” Shursen says.
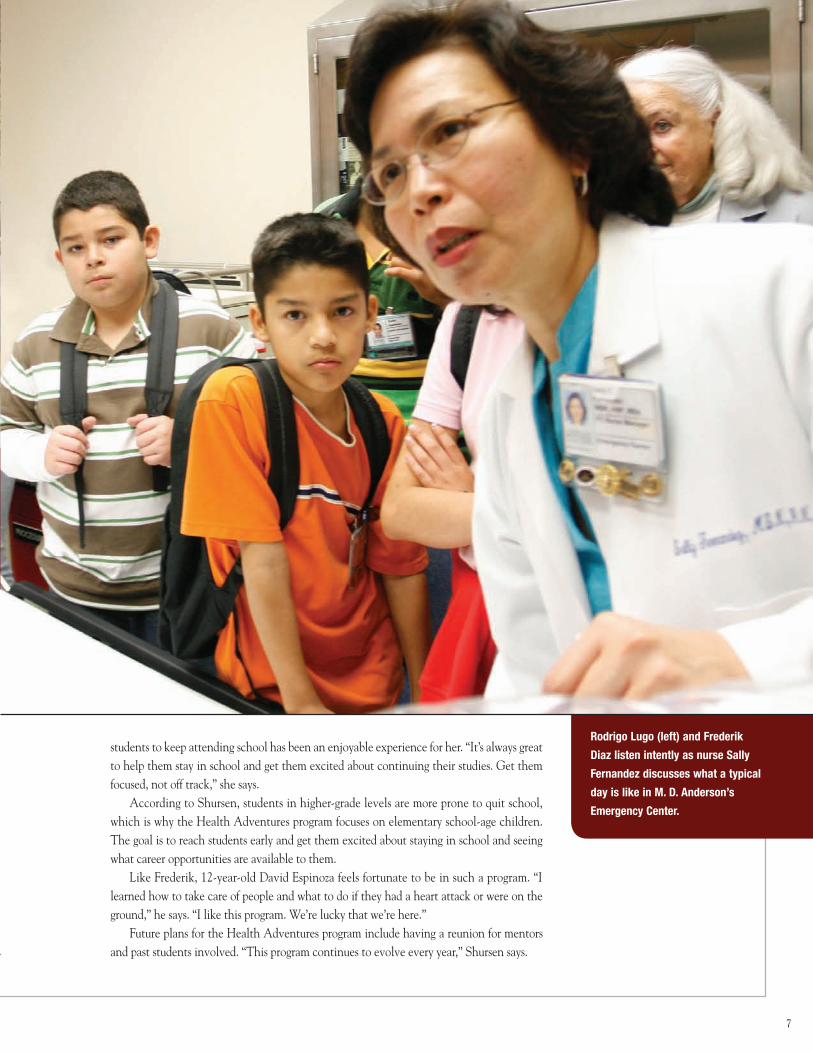
Rodrigo Lugo (left) and Frederik
Diaz listen intently as nurse Sally
Fernandez discusses what a typical
day is like in M. D. Anderson’s
Emergency Center.
7

CANCER’S IGNITION SWITCH
Forerunner genes pave way for cancer
M. D. Anderson Pathology Professor Bogdan Czerniak, M.D., Ph.D., and colleagues are exposing this journey with a unique map — one so complex and finely detailed that it pinpoints an organ’s normal, transitional and cancerous cells in a way that also depicts how cells arrive at a cancerous destination.
The key finding from a decade of bladder cancer research is the existence of what Czerniak calls “forerunner genes,” whose inactivation paves the way for the silencing of tumor-suppressing genes, thus jump-starting cancer development.
“Forerunner genes are the ignition key that starts the engine of carcinogenesis,” Czerniak says. While the transition of normal cells into cancer has long been believed to involve activation of oncogenes and silencing of tumor-suppressing genes, forerunner genes drive the initial growth of precancerous cells.
“Discovery of these genes opens an entirely new field of investigation to identify bio-markers for the early identification and prevention of cancer,” he says. They also provide a new set of potential targets for therapies to prevent or treat cancer.
His technique, called whole organ histologic and genetic mapping, superimposes maps of genetic variation over a detailed map of the organ’s terrain as revealed by microscopic study of its tissue, or its histology.
EarLY dETECTiON, bLaddEr CaNCEr aNd bEYONd
Czerniak’s mapping technique and findings are the first of their kind, says T. Sudhir Srivastava, Ph.D., chief of the Cancer Biomarkers Research Group, Division of Cancer Prevention of the National Cancer Institute (NCI).
“Identifying genes involved in precancerous development has been an arduous task, primarily for lack of a systematic approach to discovering them and the non-availability of quality tumor specimens for discovery,” Srivastava says. “Dr. Czerniak has overcome these difficulties by utilizing the resources available at M. D. Anderson and employing the gene-mapping expertise of his group to uniquely characterize chromosomal regions involved in genomic imbalances, particularly those involved in progression of precancerous conditions to clinically aggressive bladder cancer.
Long before cancer threatens health, long before it’s even detectable as cancer, normal cells stealthily are going bad. Identifying these precancerous changes during “the invisible stage” of a cell’s path to malignancy could make a huge difference in cancer prevention and treatment.
by Scott Merville
8

Bogdan Czerniak, M.D., Ph.D.,
and his colleagues have
developed a unique map that
pinpoints an organ’s normal,
transitional and cancerous
cells in a way that also depicts
how cells arrive at a cancerous
destination.
9
“These findings will accelerate development of clinically useful biomarkers for the early detection, surveillance and clinical management of bladder cancer,” adds Srivastava, who leads NCI’s Early Detection Research Network, which partially funds Czerniak’s work.
There’s good reason to believe the team’s research will apply to other cancers. Lung and oral cancers are similar to bladder cancer, Czerniak notes. All are cancers of the epithelium, the tissue that lines the surfaces and cavities of the body’s organs. Epithelial cancers, or carcinomas, make up 80 percent of all cancers.
They have found that two forerunner genes, that lead to the development of bladder cancer when they are silenced, also are quieted to varying degrees in lung, breast, blood and common pediatric malignancies.
It’s hard to be fIrst
The intense methods used in bladder cancer provide a model approach to address other cancers. There are new forerunner genes, new keys to the ignition, to be found.
At first, Czerniak expected to discover more crucial parts to the engine — new tumor-suppressors that are damaged or shut down, allowing cancerous cells to flourish. Instead, experimental data kept guiding Czerniak’s team back to the genomic neighbor-hoods of known tumor-suppressing genes, but not to the suppressors themselves.
Following the evidence in bladder cancer specimens, the team narrowed its search to several genes located near — one is actually inside — an important common tumor-suppressing gene known as RB1, which is shut down in many cancers. Researchers then demonstrated that two of these genes are silenced before RB1 is stifled.
These findings and the techniques used to reach them were so cutting-edge that publication took an agonizing four years. “Our initial publication was rejected by everyone, all of the major journals,” Czerniak says. “We hope that this is over.”
Reviewers at the prestigious Proceedings of the National Academy of Sciences (PNAS) finally embraced the forerunner gene paper enthusiastically and it was pub-lished last year. “But that paper is just the tip of the mountain,” he says.
‘the most precIous pIece of scIentIfIc work’
Jim Crawford, M.D., Ph.D., editor of Laboratory Investigation, a member of the Nature Publishing Group, will publish more of the mountain, devoting about one-half of the July issue to a “megapaper” that covers the team’s research to date.
“We’ve basically cleared out the issue for this paper,” says Crawford, who also is professor and chair of the University of Florida College of Medicine’s Department of Pathology, Immunology and Laboratory Medicine. Devoting that much space to a single paper is highly unusual, but Crawford is convinced it’s worthwhile. Czerniak notes that Crawford was one of the few editors who understood and supported the team’s early work. After the PNAS paper was published, the two discussed publication of a comprehensive article in Laboratory Investigation.
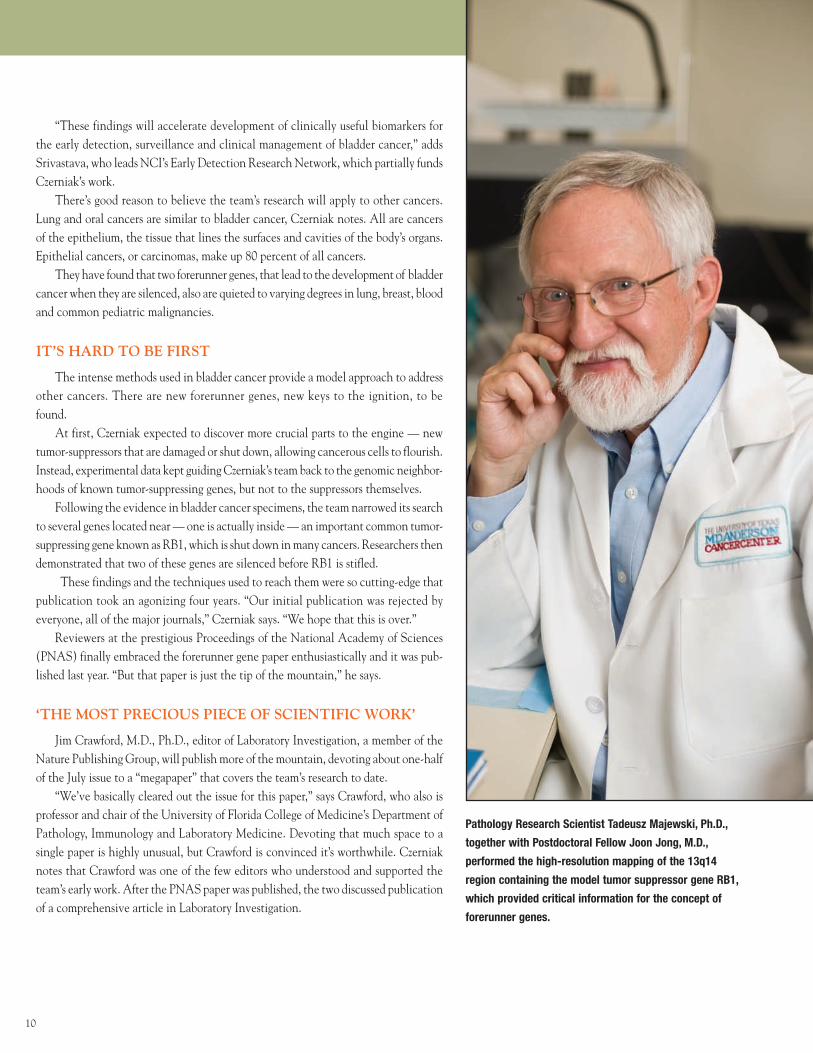
Pathology Research Scientist Tadeusz Majewski, Ph.D.,
together with Postdoctoral Fellow Joon Jong, M.D.,
performed the high-resolution mapping of the 13q14
region containing the model tumor suppressor gene RB1,
which provided critical information for the concept of
forerunner genes.
10

Crawford agreed to accommodate one huge paper, including supplemental data and figures used with permission from the PNAS paper. “A person should be able to
read this paper and know the whole story,” Crawford says. The resulting paper was too large to transmit electronically and
had to be sent via FedEx. “When I received this paper I had the feeling I was holding the most precious piece of scientific work that I would ever touch in my career,” Crawford says.
Czerniak notes this research is a massive undertaking, involving multistep genetic screenings, followed by validation studies of initial findings, which required plenty of bladder, blood and urine specimens.
Studies of gene expression, sequencing and a regulatory chemical process called methylation, along with functional studies of what candidate
genes do and epidemiological analyses were required in the final steps of forerunner gene identification.
“Our collaborators, both inside and outside the institution, are superstars in their fields,” Czerniak says.
Faculty from six M. D. Anderson departments contributed to the Laboratory Investigation paper, and over the years, Czerniak’s team has collaborated with 15 departments. Internationally known researchers from Baylor College of Medicine in Houston, Creighton University in Omaha, Neb., The University of Texas Southwestern Medical Center in Dallas, the International Institute of Molecular and Cell Biology in Warsaw, Poland, and the Sunnybrook and Women’s College Health Science Center in Toronto made major contributions.
mappInG the terraIn
It all starts with the surgically removed cancerous organ. In this case, it’s the bladder. Microscopic analysis of the entire organ creates a map of the bladder’s terrain. Areas of normal tissue are noted along with areas of precancerous plaques and lesions, and the tumor or tumors.
Taking the forerunner gene paper as an example, the team mapped the tissue of five bladders with cancer in the organ’s lining.
Next, they employed 787 DNA markers to identify chromosomal regions that display genetic variations of interest. By superimposing the low-resolution map of genetic varia-tion over the geographic map of the organ’s tissue, they identified regions associated with two different types of precursor lesions.
In one type, a genetic change is obvious, but unaccompanied by notable change in a cell’s appearance or composition — its phenotype. In the second case, striking genetic change was accompanied by signs of cellular abnormality called dysplasia and development of carcinoma in situ, cancer that remains limited to its tissue of origin. Dysplasia and carcinoma in situ progress to higher grade, invasive cancer.
F o r e r u n n e r g e n e s p a v e w a y f o r c a n c e r
read this paper and know the whole story,” Crawford says.
multistep genetic screenings, followed by validation studies of initial findings, which required plenty of bladder, blood and urine specimens.
Studies of gene expression, sequencing and a regulatory chemical process
Did You Know?The greatest risk factor for
bladder cancer is smoking.
Smokers are more than
twice as likely to get bladder
cancer as nonsmokers.
Smoking causes nearly
one-half of the deaths from
bladder cancer among men
and slightly more than a
quarter in women.
Source: American Cancer Society
Three Steps to IgnitionInactivation of forerunner genes leading to the silencing of a major tumor-suppressing gene, RB1, leads to the establishment and proliferation of bladder cancer.
Here’s how this happens:
First: Everyone has two versions of each gene,
one from each parent. Initially, one version of both
the forerunner and the RB1 gene is inactivated by
large deletions of DNA. The deletions in RB1 and its
neighboring region are seen in about one-half of all
epithelial bladder cancers.
Second: The remaining forerunner gene is inactivated
by hypermethylation, the attachment of methyl
chemical groups to spots on the gene that shut it down.
This process is associated with expansion of
low-grade tumors.
Third: The remaining RB1 gene is inactivated, most
commonly by a mutation, a step associated with
advancement to high-grade tumors.
11
F o r e r u n n e r g e n e s p a v e w a y f o r c a n c e r
Additional analysis narrowed the chromosomal areas to portions of six chromo-somes. These six sites were confirmed by testing multiple markers of genetic loss found in those chromosomal regions in the urine and blood of 32 bladder cancer patients and 31 disease-free patients with a history of bladder cancer. Genetic losses from at least one of the six regions were found in 98 percent of patients. In 82 percent of the cases, two to five chromosomal regions were involved.
“This told us that genetic losses in those regions were frequent in bladder cancers and that those regions may harbor genes critical to cancer development,” Czerniak says.
fOrErUNNErS fOUNd
The team then chose the 13q14 region on chromosome 13, which they knew harbored the tumor-suppressor RB1 gene, for high-resolution genetic analysis to identify candidate genes. The initial mapping data indicated that inactivation of RB1 wasn’t associated with growth advantage of early in situ precancerous lesions and suggested that other genes in the region may be involved.
Their earlier organ-wide genomic analysis employed microsatellite markers. These are very short stretches of repeat base pairs of nucleotides, which are the building blocks of DNA. For a more refined analysis of genes around RB1, the team used single-nucleotide polymorphisms, or SNPs, as markers. SNPs are points in the genome that vary by a single DNA nucleotide.
Researchers examined 92 SNPs mapping to a region around the RB1 gene in 84 paired samples of bladder tumors and blood DNA. This high-resolution genetic analysis pointed to the same section of the chromosome that whole organ histologic and genetic mapping had identified with expansion of abnormal cells.
Three genes in that segment were targeted for additional analysis. Two were found to be inactivated before RB1 loses its function during tumor development.
Researchers found that a neighboring gene called ITM2b was silenced by methyla-tion, which is the attachment of methyl chemical groups to places on the gene that shut the gene down. In bladder cancer tumors and cancer cell lines, this gene was methylated 40 percent of the time. Methylation is an epigenetic effect, meaning it regulates gene expression without changing a gene’s DNA.
ThE SmOkiNg CONNECTiON
A gene known as P2RY5 located inside a portion of the RB1 gene was affected by a number of single-nucleotide variations. A case-control study of one of the gene’s variant forms was conducted using blood DNA from 790 bladder cancer patients and 712 controls matched for age and gender. The study, conducted by Xifeng Wu, M.D., Ph.D., professor in M. D. Anderson’s Department of Epidemiology, found that the specific variation was present in 2.78 percent of patients.
Wu’s study also found that every single patient with this P2RY5 polymorphism who also smoked developed bladder cancer. Smoking is the most important risk factor in bladder cancer and thought to be involved in one-half of all cases.
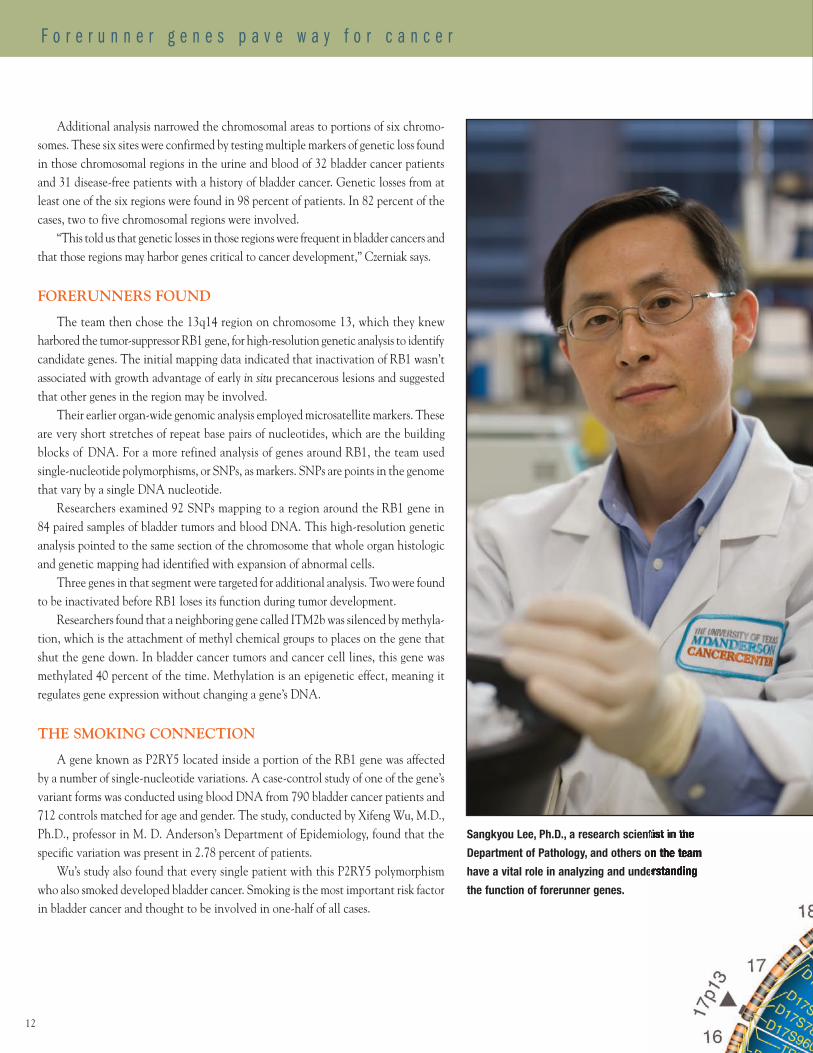
Sangkyou Lee, Ph.D., a research scientist in the
Department of Pathology, and others on the team
have a vital role in analyzing and understanding
the function of forerunner genes.
Sangkyou Lee, Ph.D., a research scientist in the
Department of Pathology, and others on the team
have a vital role in analyzing and understanding
12
Working with Henry Lynch, M.D., an expert in cancer genetics and professor and chair of Preventive Medicine at Creighton University School of Medicine, the team followed up earlier evidence that P2RY5 mutations might be inherited variations — what scientists call germline mutations — as opposed to variations caused by damage to existing DNA.
Genetic analysis of a family in Lynch’s research that has been plagued by a variety of cancers for generations showed that their tumors had only mutant P2RY5 genes. The genetic transmission pattern in the family indicated an association between inherited mutations of P2RY5 and cancer development.
“It was whole-organ mapping that led us to these inherited P2RY5 mutations,” Czerniak notes.
EXCiTiNg TimES ahEad
This exhaustive, detailed scrutiny of a portion of one chromosome is what’s in store for the five other chromosomal regions identified by the whole organ map. In fact, the entire genome will get the high-resolution treatment.
The whole organ genetic and histologic mapping procedure is a useful model for hunting down forerunner genes in other types of cancer, particularly because many cancers share damage or inactivation of common tumor-suppressing genes.
The forerunner genes identified in bladder cancer were analyzed for their expres-sion, methylation and sequence in 62 cell lines derived from major groups of common cancers. Of the cell lines tested, forerunner gene expression was reduced in 63 percent of the cases and ITM2b was methylated in 42 percent.
While forerunner gene down-regulation was identified in lung, breast, blood and pediatric malignancies, the genes were strongly expressed in colon and liver cancers. This makes sense, researchers note, because those two cancers don’t rely on inactiva-tion of RB1 to thrive.
Czerniak remains excited by what’s to come. “It took us 10 years to get where we are now. With the new high-throughput technology now available, we’ll complete a high-resolution genetic map of the entire genome for bladder cancer in the next two or three years.”
Joe Gray, Ph.D., director of the Life Sciences Division of the Lawrence Berkeley National Laboratory, which is managed by the University of California, notes that researchers have made great progress identifying genomic and epigenetic aberrations that drive the initiation, invasion and metastasis of cancer.
“Dr. Czerniak and colleagues have now added an important three-dimensional histological context to cancer genomics that guides the identification of initiat-ing events and promises to provide insights into how specific genomic aberrations contribute to distinct stages of tumor progression,” Gray says. “This approach should contribute substantially to our understanding of the functions of epigenetic and genomic aberrations in cancer.”
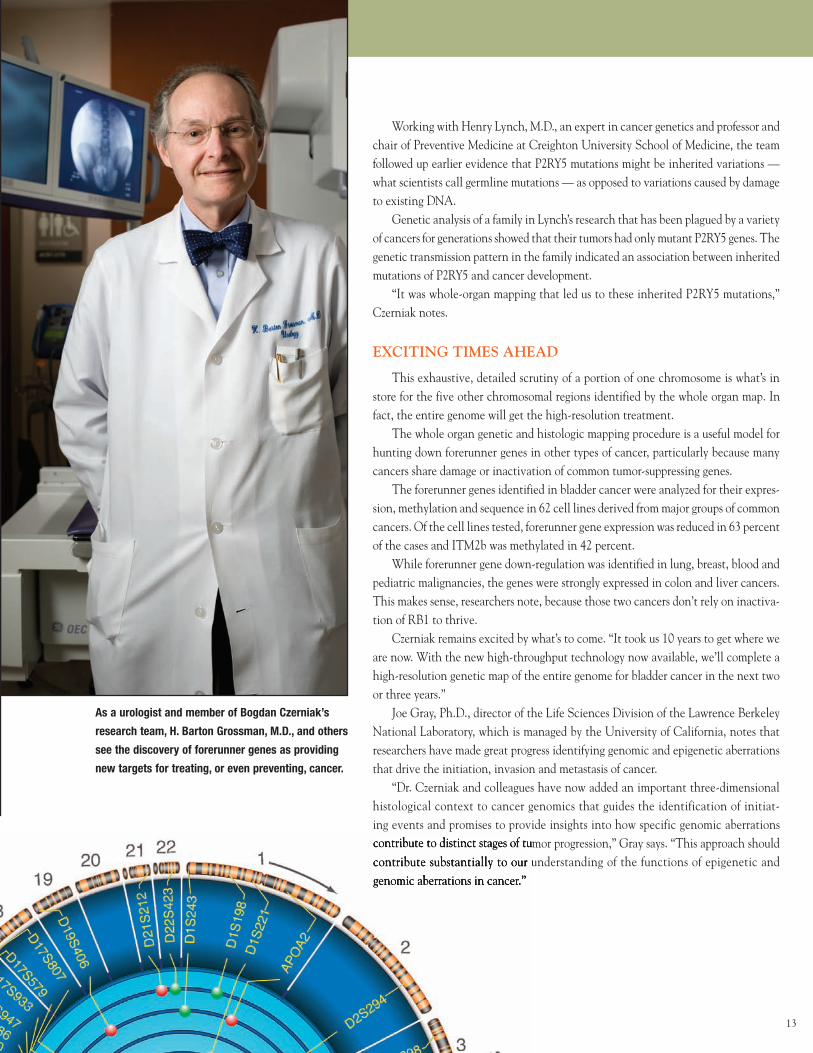
as a urologist and member of Bogdan Czerniak’s
research team, H. Barton Grossman, M.D., and others
see the discovery of forerunner genes as providing
new targets for treating, or even preventing, cancer.
contribute to distinct stages of tumor progression,” Gray says. “This approach should contribute substantially to our understanding of the functions of epigenetic and genomic aberrations in cancer.”
13
Through a combination of inspiration and compassion, Koch is touching thousands of lives with the more than $500 million in philanthropic gifts he’s made to a variety of orga-nizations and programs that further cancer research, enhance medical centers and support educational institutions, as well as to programs that sustain arts and cultural institutions.
Most recently, he’s given $18 million to M. D. Anderson to create the David Koch Center for Applied Research in Genitourinary Cancers.
Under the direction of Koch’s oncologist, Christopher Logothetis, M.D., chair of the Department of Genitourinary Medical Oncology, the Koch Center will bring together basic, translational and clinical scientists to rapidly move scientific findings to patients with diseases such as prostate cancer, which Koch has battled for many years.
“The idea behind the Koch Center is to create a unique infrastructure that enables us to take abundant discovery and move it more efficiently and more reliably into human studies,” Logothetis says. “The Koch Center will create a shared environment where researchers in basic science, applied science and all the fields with which we interact can obtain and analyze data the same way, use the same scientific language, establish strict project management deadlines and stay goal-oriented.”
This approach also allows the Koch Center to create a “memory.”
“Each time we do a study in humans or in animals, it will be recorded in such a way that allows us to retrieve the data to see how it relates to the next study,” Logothetis explains.
Should a scientist leave the institution, Logothetis notes, his or her work will be preserved so that it remains available to investigators worldwide.
Koch attributes his passion for supporting prostate cancer research to his own experience with the disease.
A Personal Investment by DeDe DeStefano
Dedicated, generous, hardworking and passionate, David H. Koch embodies success not only by being one of the principal owners of Koch Industries, Inc., the world’s largest privately held company, but also by the impact he’s making on mankind.
David H. Koch’s $18 million gift will help support basic and translational research in the study and treatment of genitourinary cancers.
14

“I’ve been living with prostate cancer for 15 years and have been under the care of Dr. Logothetis,” Koch says. “I’m a survivor, and I have tremendous sympathy for others who have this disease. When you’re up close and personal with prostate cancer, you become a crusader. My wife and I have three young children, and I have great aspirations to live long enough to see all of them graduate from college. My children are tremendous incentives.”
Prostate cancer is the most common type of cancer diagnosed in American men, other than skin cancer. It’s second only to lung cancer as the leading cause of cancer death in men.
“We’re humbled by the trust that our patients, such as David Koch, place in us for their care and by their gifts to the institution, and we feel especially compelled to deliver results,” Logothetis says. “They drive us and give us a sense of responsibility just as much as a peer-reviewed grant.”
Koch has supported M. D. Anderson for many years, having served on its Board of Visitors since 1999. He and his wife, Julia, also have given financially to the institution for more than a decade. In addition, they support the cancer center by opening their home to guests who are interested in hearing about M. D. Anderson. In 2007 and 2008, the Kochs hosted educational dinners designed to raise awareness of the research, patient care, education and prevention programs ongoing at M. D. Anderson.
Koch Industries, Inc. owns a diverse group of companies with about $90 billion in revenues, 80,000 employees and a presence in nearly 60 countries. Familiar Koch company brands include STAINMASTER® carpet, LYCRA® spandex, Quilted Northern® tissue and Dixie® cups.
“I feel extraordinarily blessed to be one of the principal owners of Koch Industries,” Koch says. “The outstanding growth of my family company has been largely due to the heroic efforts of our executives and employees and has enabled me to be very generous to many worthwhile institutions.”
In 2004, Koch received a presidential appointment to the National Cancer Advisory Board of the National Cancer Institute. He serves on more than 20 nonprofit boards.
During a follow-up appointment, David Kirkman got a chance to catch up with Christopher Logothetis, M.D., and learn about the creation and naming of the David Koch Center for Applied Research in Genitourinary Cancers, which Logothetis directs.
15

Those who practice this specialized field are psychometricians, and their science is psychometrics, the study of the design and analysis of tests and questionnaires. Besides standardized tests, psychometricians also play a prominent role in the construction of patient-reported assessment tools for cancer-related clinical trials, such as symptom burden outcome.
Tito Mendoza, Ph.D., assistant professor in M. D. Anderson’s Department of Symptom Research, is one such psychometrician. Along with Charles Cleeland, Ph.D., chair of the department, he’s worked with researchers and health care professionals across the institution to assess the reliability and validity of tools that measure the symptom burden of cancer patients.
Recently published are the results of an investigation into the overall symptoms of head and neck cancers. The M. D. Anderson Symptom Inventory-Head and Neck (MDASI-HN) is a study he worked on with principal investigator David I. Rosenthal, M.D., professor in the Department of Radiation Oncology and director of Head and Neck Translational Research.
phYSiCiaN wiTh a miSSiON
When he arrived at M. D. Anderson six years ago, Rosenthal brought with him a deep concern about the symptom burden his patients experienced as a result of treatment.
While successful advances have been made in the treatment of head and neck cancers over the last 10-15 years, the acute toxicity can be significant and also cause long-term functional impairment whose symptoms are not well understood. This is especially true for patients with cancers, such as those of the oropharynx (the soft palate at the back of the mouth, the base of the tongue and tonsils), many of whom underwent operations in the past. Today, standard treatment for them consists of combining chemotherapy as a sensitizer to intensify the effect of radiation on the tumor and to kill more cancer cells.
While cancer control and survival rates are excellent, and the organs are numerically preserved, certain functions, such as swallowing, may be impaired.
StePS tO VaLIDatION
by Sandi Stromberg
Have you ever wondered who develops standardized tests, like the Scholastic Aptitude Test for getting into college or the Graduate Record Exam for graduate school?
How do they know what questions measure knowledge or intelligence?
And how can they calculate what constitutes a passing score that says a person has the ability to follow a course of study?
Editor’s Note:
Active in pain research for many years and instrumental in developing the Brief Pain
Inventory now used in most clinical trials, Charles Cleeland, Ph.D., chair of M. D. Anderson’s
Department of Symptom Research, knew the importance of measuring and attending to
patients’ symptom distress long before it became a concern for federal agencies.
“Now, the U.S. Food and Drug Administration is asking for more rigor in the assessment
of symptoms and other patient-reported outcomes,” he says. “It wants more systematic and
validated measures of symptoms that are both relevant and intelligible to patients.”
M. D. Anderson has been a leader in this field through the institution’s symptom
inventories, collaborative studies in which health care professionals across the institution
collect solid, scientific evidence that can be used to design interventions to relieve the
symptom burden caused by cancer and its treatments.
This is the third article in a series.
16
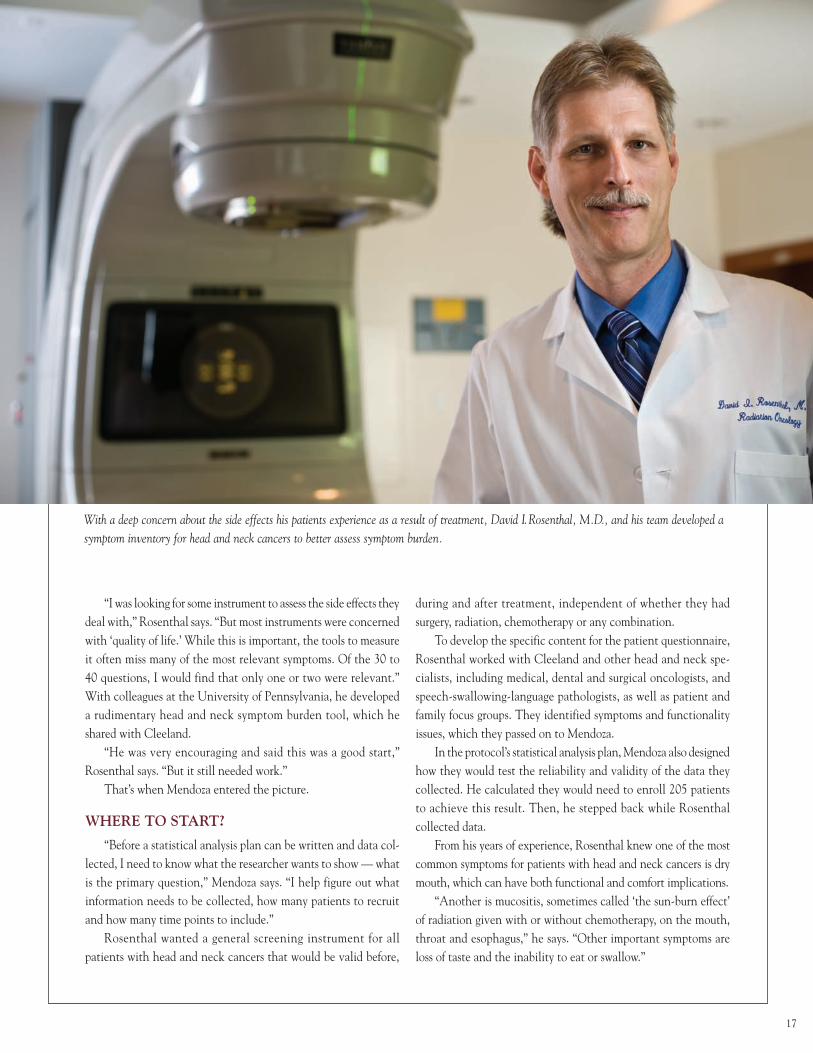
With a deep concern about the side effects his patients experience as a result of treatment, David I.Rosenthal, M.D., and his team developed a symptom inventory for head and neck cancers to better assess symptom burden.
“I was looking for some instrument to assess the side effects they deal with,” Rosenthal says. “But most instruments were concerned with ‘quality of life.’ While this is important, the tools to measure it often miss many of the most relevant symptoms. Of the 30 to 40 questions, I would find that only one or two were relevant.” With colleagues at the University of Pennsylvania, he developed a rudimentary head and neck symptom burden tool, which he shared with Cleeland.
“He was very encouraging and said this was a good start,” Rosenthal says. “But it still needed work.”
That’s when Mendoza entered the picture.
whErE TO STarT?
“Before a statistical analysis plan can be written and data col-lected, I need to know what the researcher wants to show — what is the primary question,” Mendoza says. “I help figure out what information needs to be collected, how many patients to recruit and how many time points to include.”
Rosenthal wanted a general screening instrument for all patients with head and neck cancers that would be valid before,
during and after treatment, independent of whether they had surgery, radiation, chemotherapy or any combination.
To develop the specific content for the patient questionnaire, Rosenthal worked with Cleeland and other head and neck spe-cialists, including medical, dental and surgical oncologists, and speech-swallowing-language pathologists, as well as patient and family focus groups. They identified symptoms and functionality issues, which they passed on to Mendoza.
In the protocol’s statistical analysis plan, Mendoza also designed how they would test the reliability and validity of the data they collected. He calculated they would need to enroll 205 patients to achieve this result. Then, he stepped back while Rosenthal collected data.
From his years of experience, Rosenthal knew one of the most common symptoms for patients with head and neck cancers is dry mouth, which can have both functional and comfort implications.
“Another is mucositis, sometimes called ‘the sun-burn effect’ of radiation given with or without chemotherapy, on the mouth, throat and esophagus,” he says. “Other important symptoms are loss of taste and the inability to eat or swallow.”
17
ENSURING RELIABILITY AND VALIDITY
The first thing Mendoza tested was reliability.“Reliability means that if you ask patients about a symptom at one
point, they give you the same answer at the second point, if nothing in the patient’s condition changes. For example, if you take your tem-perature with a thermometer, unless you develop a fever, you should get a similar result a few days later. If you don’t, your thermometer isn’t reliable. A variation, or noise, is coming from somewhere else. It’s like trying to hear a conversation above some ambient noise that we need to get rid of to understand the conversation.”
Next, Mendoza measured validity. To analyze data collected by Rosenthal and his colleagues for the MDASI-HN, he chose three validity measures: construct validity, known groups and concurrent validty. (See sidebar)
Of reliability and validity, Mendoza says they used three forms of validity because it’s more important. “You can have a reliable tool, but if it isn’t relevant or valid, it’s not very helpful.”
WHAT THEY LEARNED
“One thing we noticed in our trials is that some patients get a lot of mucus in their throat,” Rosenthal says. “It’s a significant symptom that hadn’t been reported before. Yet, mucus in the throat can be so copious that some patients’ entire lives are focused on management of secretions. They’re constantly gargling, suctioning. They can’t sleep. They gag and regurgitate.”
Counting this discovery, the study identified nine head and neck cancer-specific symptoms, separate from the 13 core MDASI symptoms that may be experienced by any cancer patient (see Conquest, Summer 2007). They’re mouth and throat sores, problems with tasting food, constipation, problems with teeth or gums, skin pain, burning or rash, difficulty with voice or speech, mucus in the mouth or throat, choking or coughing, and difficulty chewing or swallowing.
Not only were they able to validate the MDASI-HN, but also in a subsequent study where they compared it with the quality-of-life Functional Assessment of Cancer Therapy-Head and Neck, it provided a better measure of the severity of radiation-induced mucositis.
Since validation, the tool has been incorporated into some clinical trials. However, hopes are that when technology allows, the MDASI-HN will become an integral part of a patient’s electronic medical record as M. D. Anderson researchers work toward under-standing symptom burden and finding interventions to treat and ultimately prevent debilitating side effects for cancer survivors.
Simple Measures, Valid Results
Tito Mendoza, Ph.D., assistant professor in
M. D. Anderson’s Department of Symptom Research,
used the following methods to validate specific
symptoms experienced by patients with head and
neck cancers.
Construct Validity: This method helps deter-
mine underlying factors — latent constructs not
directly measurable but that can be observed with
indicators. For example, a family’s socioeconomic
status (SES) can’t be directly measured, but we can
measure a host of variables such as the parents’ occu-
pation, education level and income that may represent
SES. In the MDASI-HN, two factors were identified:
(1) mouth sores, tasting, constipation, teeth and gum
problems, and skin pain; and (2) voice and speech
difficulties, choking, coughing, chewing, swallowing
and mucus. Each set of items indicated high levels
of reliability.
Known Group Validity: Using the Eastern
Cooperative Oncology Group (ECOG) performance
status, one measure of how ill the patient is, as the
grouping variable, patients with poor ECOG per-
formance status reported severe symptoms on the
MDASI-HN. On the other hand, patients with good
ECOG performance status (healthier patients) had
fewer and less severe symptoms.
Concurrent Validity: This measures how well
the MDASI-HN correlates with another test that
measures something similar, such as the SF12 from the
Rand Corporation. The overlap in results between
the two tools provided another element of validity.
If patients have good health status, they should have
less symptom burden, and vice versa.
In the summer issue, the series continues with a look at
M. D. Anderson’s recent alliance with AstraZeneca and the
new opportunities for symptom research it provides.
18
Ernest T. Hawk, M.D.
Ernest T. Hawk, M.D.
P R O F I L E :
His enthusiasm for medicine evolved from an early desire “to help people,” but Ernest T. Hawk, M.D., didn’t decide how best to do so until he began exploring cancer at the molecular level.
“In the late 1980s, I became fascinated by the molecular biology revolution. As I learned more about how cancer develops, I got increasingly interested in prevention, especially chemoprevention. Today, I’m more excited than ever about the great impact that prevention can have on everyone’s life,” he explains.
Hawk says that he’s “thrilled” to be the new leader of M. D. Anderson’s far-reaching cancer prevention efforts.
“The opportunities to help elevate cancer prevention to the next level are just fantastic here,” notes Hawk, who in November 2007 was appointed vice president and head of the Division of Cancer Prevention and Population Sciences.
Before coming to M. D. Anderson, Hawk spent nearly 15 years at the National Cancer Institute (NCI) in Bethesda, Md. Upon finishing a three-year cancer prevention fellowship at NCI, he was one of the first clinically oriented oncologists asked to join a research group there. He held several key administra-tive posts while conducting chemoprevention research focused on nonsteroidal anti-inflammatory drugs and COX-2 inhibitors. Some of his research involved collaborating with experts at M. D. Anderson to design and conduct landmark chemopreven-tion clinical trials.
“Even though I knew about many of M. D. Anderson’s achievements in cancer prevention, I’m more impressed every day by the breadth and depth of the research and the commit-ment to educate the public and health care professionals about the enormous potential of prevention,” Hawk says.
❖
A native of Detroit, Hawk excelled in academics. As valedictorian of his high school graduating class, he received a full scholarship to Wayne State University, where he earned a bachelor’s degree with high distinction in biological sciences.
“My parents, who both worked in the auto industry, were proud that I was the first in the family to go to college and then delighted when I was accepted to Wayne State’s School of Medicine. That’s where I saw my first cancer patients and became interested in cancers of the gastrointestinal tract,” Hawk recalls.
by Mary Jane Schier
19

Ernest T. hawk, m.d.P R O F I L E :
After receiving his medical degree in 1985, Hawk completed an internship and internal medicine residency at Emory University’s affiliated hospitals in Atlanta. While working as a staff physician at the Atlanta Veterans Affairs Medical Center and Grady Memorial Hospital for three years, he enjoyed treating patients but was “increasingly intrigued” about emerging molecular biology research.
In 1991, Hawk was accepted for a two-year clinical fellowship in medical oncology at the University of California School of Medicine, San Francisco. That academic center was then home to J. Michael Bishop, M.D., and Harold E. Varmus, M.D., who shared the 1989 Nobel Prize in Physiology or Medicine for discovering the first human oncogene. Their findings about how cancer begins at the molecular level and other scientific discoveries influenced Hawk’s changing interest from treating malignancies to preventing them.
The 1993-1996 period provided pivotal experiences for Hawk. During the initial part of his cancer prevention fellowship at NCI, he earned a master’s degree in epidemiology and biostatistics at Johns Hopkins University School of Hygiene and Public Health.
“Learning the quantitative methods needed to conduct translational research and clinical trials was stimulating, and soon I was immersed in the development of new agents for promising targets and planning how best to incorporate novel intermediate endpoints into clinical trials,” remembers Hawk, who after the fellowship was invited to join NCI’s Chemoprevention Branch.
In 1997, Hawk was promoted to medical officer for the Chemoprevention Branch. Two years later, his research group was split into four, including the Gastrointestinal and Other Cancers Research Group that he headed. In 2002, he received the NCI Research Award for Distinguished Achievement in Cancer Prevention.
Four years ago, he was asked to direct the NCI’s Office of Centers, Training and Resources. In that position, he coordinated a portfolio of grants involving cancer centers, translational research and training, totaling more than $500 million. He also chaired the Translational Research Working Group that was developing a strategic plan for the nation’s investment in translational cancer science.
Hawk smiles as he says, “I loved working as a public servant and thought I’d be at NCI for the rest of my professional career. However, there are unparalleled opportunities at M. D. Anderson to advance all aspects of cancer research and to ensure that cancer prevention is not just a promising theory but an increasingly compelling component of our clinical approach to the disease.”
As the new leader of M. D. Anderson’s cancer prevention programs, Hawk makes daily exercise a top priority.
20
During the last decade, Hawk enjoyed chemoprevention research collaborations and co-authored journal articles with several faculty members at M. D. Anderson, among them Bernard Levin, M.D., previous head of the Division of Cancer Prevention and Population Sciences, who retired in fall 2007.
“I look forward to building on Dr. Levin’s successes and strengthen-ing our spectrum of prevention programs,” Hawk states.
His early plans include developing an effective database and com-puterized tracking system for all cancer prevention research projects and services.
“Hopefully, within a year, we’ll have a new system to better char-acterize our activities. We need to describe each project with regard to its scientific goals, its translational potential and the population that it intends to benefit, such as healthy individuals, people at elevated risks due to familial history or lifestyle choices, cancer survivors and so on,” Hawk explains. “This initiative should stimulate our faculty, staff, potential research participants and others to always think about where our research is going in a very tangible manner.”
Hawk also intends to initiate a simple mnemonic, or memory aid — termed the ABCs for clinical trials — which he helped create at NCI. “A” stands for preventive agents; “B” for intermediate biomarkers of efficacy; “C” for cohorts of people at risk; “D” for clinical trial design; and “E” for endpoints of clinical efficacy.
“By focusing on enhancements in one or more of these critical elements, clinical research can be accelerated,” he says, “and time is everyone’s most precious resource.”
Hawk anticipates broadening prevention research by working closely with John DiGiovanni, Ph.D., chair of M. D. Anderson’s Department of Carcinogenesis and director of the Virginia Harris Cockrell Cancer Research Center in Smithville, Texas, and Garth Powis, D.Phil., director of M. D. Anderson’s Center for Targeted Therapy in the Red and Charline McCombs Institute for the Early Detection and Treatment of Cancer.
“Our goal for these collaborations is to discover, develop and bring to clinical trials an array of chemoprevention drugs and biologic agents that can attack molecular defects inside early cancer cells and correct malfunctions in precancerous cells long before clinical symptoms occur,” he notes.
❖
Getting adjusted to who works where across M. D. Anderson’s Main and South campuses has been “challenging,” but Hawk says he appreciates “how helpful everyone has been.”
He’ll also feel more settled once his family moves to Houston. For now, he commutes frequently to see his wife, Diana, whom he met in the seventh grade, and their three children: Christiana, 14; Melina, 13; and Grant, 9. His mother also lives with the family in a small rural community about 35 miles from Baltimore.
Besides heading the Division of Cancer Prevention and Population Sciences, Hawk is ad interim chair of the Department of Clinical Cancer Prevention. He serves as deputy editor for Cancer Prevention Research and senior editor for Cancer Epidemiology, Biomarkers and Prevention. Over the years, he’s contributed to more than 90 journal articles and 12 books. His research has led to two patent applications.
Looking ahead, Hawk is concerned about the shortage of scien-tists and clinicians devoted to cancer prevention as well as resources necessary for translating the most promising prevention discoveries into widespread use.
“I firmly believe that our division has the capacity to be the definitive resource for educating the public and health care profes-sionals about state-of-the-art practices in cancer prevention and the critical role that research plays,” he says. “We must work harder than ever to assure we can be a dynamic training group for future genera-tions of researchers and practitioners committed to cancer prevention as well as the broader mission of improving overall health.”
Hawk counts on Executive Assistant Cheri McClellan to keep track of his busy schedule.
21
ASPIRE Internet Site Kicks Butt
What better way to mark the 13th annual National Kick Butts Day than to announce plans to expand use of M. D. Anderson’s ASPIRE Internet site to students nationwide through collaborations with state education and health agencies.
ASPIRE — A Smoking Prevention Interactive Experience — is an evidence-based, multi-media tobacco prevention and cessation Internet site for middle and high school kids. The site integrates interactive video game-like components, customized messages, graphics, animation and streaming video to capture the interest of both nonsmoking and smoking teens.
“Nearly 4,000 youth under the age of 18 start smoking daily,” says Alexander Prokhorov, M.D., Ph.D., professor in the Department of Behavioral Science at M. D. Anderson. “We created ASPIRE because ‘Just Say No’ wasn’t good enough anymore.”
Through situations teens readily relate to — dating, stress from school and sports — ASPIRE addresses the long-term and short-term consequences of tobacco use, including changes in physical appearance and physiological processes. The Internet site speaks to teenagers on their terms and emphasizes that addiction is dependence, appealing to their desire to be independent and to make decisions on their own, Prokhorov says.
Students who used ASPIRE reported reduced number of ciga-rettes smoked, stronger anti-smoking beliefs and lower temptations to smoke. To date, the ASPIRE Internet site has had more than 30,000 visitors from 66 countries.
An initial e-campaign targeting 97 school districts in 32 states in North America was launched in late 2007. From those efforts, the
Arkansas Department of Health, the Kentucky Cancer Program and the North Carolina Department of Public Health all have plans under way to use ASPIRE in schools throughout their states. A similar partnership with the Houston Independent School District that utilizes ASPIRE to complement anti-smoking lesson plans in physical education and health classes will serve as a model for future collaborations.
“This marks the first concerted effort to provide a national platform in which ASPIRE can reach our nation’s teens,” says Kathy Hill, com-munications specialist in the Department of Behavioral Science, who is leading ASPIRE’s national rollout. “The response we received from this first push was very promising, and we look forward to continuing discussions with several states that expressed interest in adopting ASPIRE into their school’s curriculums.”
ASPIRE is available free of charge to school districts, state health departments, teachers and parents nationwide. Anyone may access the program by visiting www.mdanderson.org/aspire.
ASPIRE is funded by the National Cancer Institute and the George and Barbara Bush Endowment for Innovative Cancer Research.
— Robin Davidson
BRIEFINGS
22
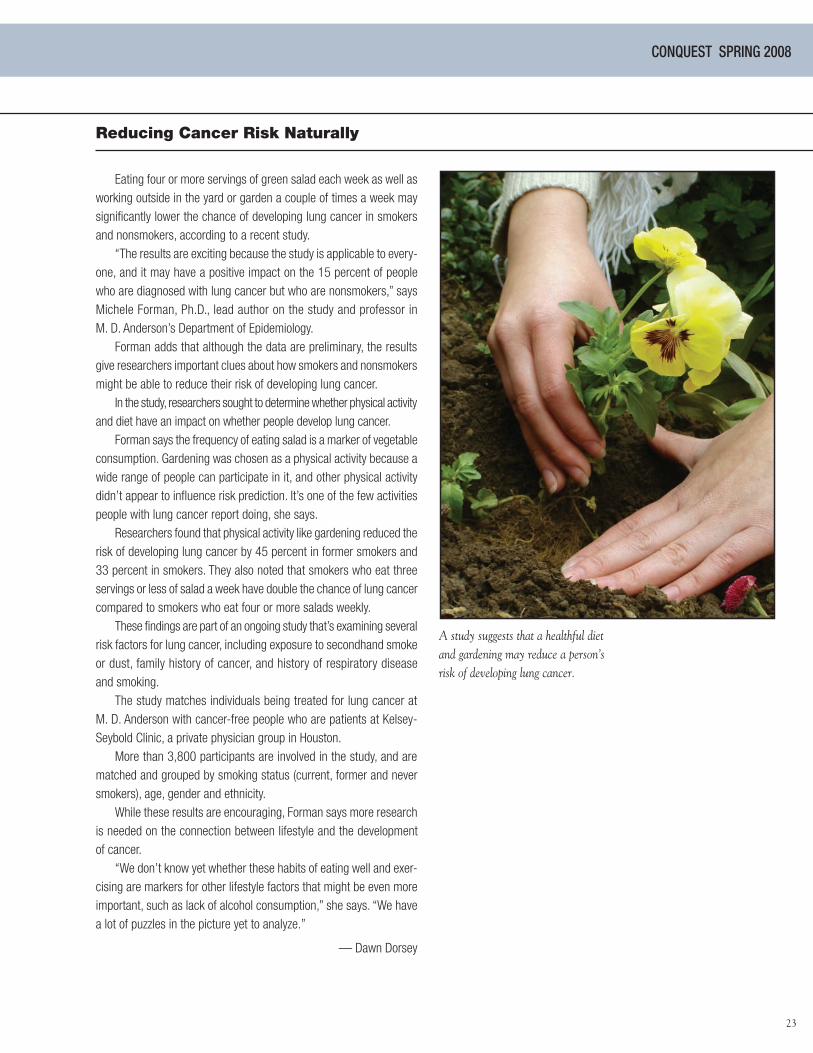
Eating four or more servings of green salad each week as well as working outside in the yard or garden a couple of times a week may significantly lower the chance of developing lung cancer in smokers and nonsmokers, according to a recent study.
“The results are exciting because the study is applicable to every-one, and it may have a positive impact on the 15 percent of people who are diagnosed with lung cancer but who are nonsmokers,” says Michele Forman, Ph.D., lead author on the study and professor in M. D. Anderson’s Department of Epidemiology.
Forman adds that although the data are preliminary, the results give researchers important clues about how smokers and nonsmokers might be able to reduce their risk of developing lung cancer.
In the study, researchers sought to determine whether physical activity and diet have an impact on whether people develop lung cancer.
Forman says the frequency of eating salad is a marker of vegetable consumption. Gardening was chosen as a physical activity because a wide range of people can participate in it, and other physical activity didn’t appear to influence risk prediction. It’s one of the few activities people with lung cancer report doing, she says.
Researchers found that physical activity like gardening reduced the risk of developing lung cancer by 45 percent in former smokers and 33 percent in smokers. They also noted that smokers who eat three servings or less of salad a week have double the chance of lung cancer compared to smokers who eat four or more salads weekly.
These findings are part of an ongoing study that’s examining several risk factors for lung cancer, including exposure to secondhand smoke or dust, family history of cancer, and history of respiratory disease and smoking.
The study matches individuals being treated for lung cancer at M. D. Anderson with cancer-free people who are patients at Kelsey-Seybold Clinic, a private physician group in Houston.
More than 3,800 participants are involved in the study, and are matched and grouped by smoking status (current, former and never smokers), age, gender and ethnicity.
While these results are encouraging, Forman says more research is needed on the connection between lifestyle and the development of cancer.
“We don’t know yet whether these habits of eating well and exer-cising are markers for other lifestyle factors that might be even more important, such as lack of alcohol consumption,” she says. “We have a lot of puzzles in the picture yet to analyze.”
— Dawn Dorsey
CONQUEST SPRING 2008
Reducing Cancer Risk Naturally
A study suggests that a healthful diet and gardening may reduce a person’s risk of developing lung cancer.
23

24
Moira and husband Jas Podgurski
by Mary Jane Schier
Moving Forward: Moira Podgurski
“I didn’t want to spoil the day for my family, so I didn’t say anything, but in the back of my mind, I kept thinking that everyone died from leukemia,” recalls Podgurski, whose three children were then seven, three and 17 months old.
The second opinion specialist she consulted said there was “nothing to do, that I might live three years.” While she and her husband, Jas, were devastated, some good friends knew about a leukemia expert at M. D. Anderson.
“That was before we had the Internet resources now available,” Podgurski says, “but I raced to the phone, got the doctor’s office and pleaded for an appointment.”
A few days later, she and Jas flew to Houston to see Kenneth B. McCredie, M.D., a pioneer in developing new drugs to treat leukemia. She enrolled in a clinical trial evaluating the biologic agent interferon, which at first she took through daily injections, then three times a week.
Although already in superb physical condition, Podgurski added yoga and meditation to her exercise routine and vegetarian lifestyle. She had started running at age 12, competed in the 1972 Olympic trials as a hurdler and has participated in many marathons.
“I approached my future with CML like I was running toward a hurdle, which you have to take one at a time. Of course, having three young children provided lots of distractions, and most days I felt good,” explains Podgurski, who’s lived in San Diego for 25 years.
After McCredie died in 1991, Podgurski met Michael J. Keating, M.D., another world leader in improving the outlook for people with leukemia. Keating became her primary specialist and would give her “ecstatic news” following a checkup at M. D. Anderson in 1997.
“When Dr. Keating called with the results of my tests, he said there was no molecular evidence of the disease, that he thought I was cured, and I should go out and live a good life,” relates Podgurski, who was in training for the Honolulu Marathon to raise money for leukemia research.
Now 11 years later, she often shares her story with newly diag-nosed leukemia patients and continues a vigorous regimen of running, race-walking five miles a day and hiking with her husband.
“I fully expect to grow old gracefully and enjoy grandchildren in the future,” Podgurski says.
Moira Podgurski doesn’t remember much about Christmas 1985 because she was “in a fog” from learning the previous day she had chronic myelogenous leukemia.

THE UNIVERSITY OF TEXAS SYSTEM BOARD OF REGENTS
H. Scott Caven, Jr., HoustonChair
James Richard Huffines, AustinVice Chair
Robert B. Rowling, DallasVice Chair
John W. Barnhill, Jr., Brenham
James D. Dannenbaum, Houston
Paul Foster, El Paso
Printice L. Gary, Dallas
Janiece M. Longoria, Houston
Colleen McHugh, Corpus Christi
Randal Matthew Camarillo, HoustonStudent Regent
Francie A. FrederickCounsel and Secretary
THE UNIVERSITY OF TEXAS SYSTEM ADMINISTRATION
Kenneth I. Shine, M.D.Chancellor Ad Interim
THE UNIVERSITY OF TEXAS M. D. ANDERSON CANCER CENTEREXECUTIVE COMMITTEE
John Mendelsohn, M.D. President
Thomas W. Burke, M.D.Executive Vice President and Physician-in-Chief
Raymond N. DuBois, M.D., Ph.D.Provost and Executive Vice President
Leon J. LeachExecutive Vice President
THE UNIVERSITY CANCER FOUNDATION BOARD OF VISITORSOFFICERS
Ernest H. CockrellChair
Marc J. ShapiroImmediate Past Chair
Nancy B. LoefflerChair-Elect
Ali A. SaberioonVice Chair
AFFILIATIONS
M. D. Anderson Cancer Center Orlando, Orlando, Florida
Centro Oncológico M. D. Anderson International España, Madrid, Spain
M. D. Anderson Clinical Care Center in the Bay Area
M. D. Anderson Radiation Treatment Centers in Bellaire, Fort Bend, Katy and The Woodlands, Texas; and Albuquerque, N.M.
Christus Spohn Stem Cell Program affiliated with M. D. Anderson Cancer Center Outreach, Corpus Christi, Texas
For information on patient services at M. D. Anderson, call askMDAnderson at 1-877-MDA-6789, or log on to www.mdanderson.org/ask
© 2008 Not printed at State expense.
Printed on recycled paper with soy-based ink.
Conquest is published quarterly by The University Cancer Foundation Board of Visitors on behalf of The University of Texas M. D. Anderson Cancer Center. All correspondence should be addressed to the Office of Public Affairs -Unit 229, M. D. Anderson Cancer Center, 1515 Holcombe Blvd., Houston, TX 77030, 713-792-0658. E-mail: [email protected]. Articles and photos may be reprinted with permission.
For information on supporting programs at M. D. Anderson Cancer Center, please contact Patrick B. Mulvey, Vice President for Development, 713-792-3450, or log on to the Development Office Web site at www.mdanderson.org/gifts.
Stephen C. Stuyck, Vice President for Public AffairsSarah Palmer, Associate Vice President for CommunicationsDavid Berkowitz, Director of Publications and Creative ServicesSandi Stromberg, Program Manager of External PublicationsEditor: Eileen A. ElligWriters: Mary Jane Schier, Deborah Aranda, Robin Davidson, DeDe DeStefano, Dawn Dorsey, Scott Merville, Sandi StrombergDesign: Michael Clarke Photography: Wyatt McSpadden, Sandy Huffaker, Ed Quinn, Cindy Shursen, F. Carter Smith
C h e c k o u t t h e C o n q u e s t We b s i t e a t w w w. m d a n d e r s o n . o r g / c o n q u e s t
The
Univ
ersi
ty o
f Tex
asM
. D. A
nder
son
Canc
er C
ente
rTe
xas
Med
ical
Cen
ter
Publ
ic A
ffairs
–22
915
15 H
olco
mbe
Blv
d.Ho
usto
n, T
exas
770
30-4
009
Addr
ess
Serv
ice
Requ
este
d
P
leas
e ch
ange
my
nam
e or
add
ress
.
I
rece
ived
a d
uplic
ate
copy
. Ple
ase
m
ake
the
nece
ssar
y co
rrec
tion.
Pl
ease
rem
ove
my
nam
e fro
m th
e
Conq
uest
mai
ling
list.
Plea
se c
heck
the
appr
opria
te b
ox a
nd re
turn
this
pag
e to
the
addr
ess
abov
e.
SPRI
NG 2
008
CONQ
UEST
Non
prof
it O
rg.
U. S
. Po
stag
e PA
IDP
erm
it N
o. 7
052
Hou
ston
, Tex
as CONQUEST