Concept of Spondyloarthritis (SpA) - UMF IASI 2015 · PDF filePatient‘s history...
78
“Juvenile SpA” Reactive Arthritis Arthritis associated with Ulcerative Colitis/ Crohn’s Disease Psoriatic Arthritis Undifferentiated SpA Acute anterior Uveitis Ankylosing Spondylitis Concept of Spondyloarthritis (SpA) 1 www.asas-group.org 1
Transcript of Concept of Spondyloarthritis (SpA) - UMF IASI 2015 · PDF filePatient‘s history...

“Juvenile SpA”
Reactive
Arthritis
Arthritis
associated with
Ulcerative Colitis/
Crohn’s Disease
Psoriatic
Arthritis
Undifferentiated
SpA
Acute
anterior
Uveitis
Ankylosing
Spondylitis
Concept of Spondyloarthritis (SpA)
1 www.asas-group.org
1

2
Amor Classification Criteria for Spondyloarthritis
Amor B et al. Rev Rhum Mal Osteoartic 1990;57:85-89 2

3
ESSG-Classification Criteria
(European Spondylarthropathy Study Group)
Dougados M et al. Arthritis Rheum 1991;34;1218 3

Good response to NSAIDs
Symptoms
Imaging
Lab
Patient‘s history
Inflammatory
back pain
ESR/CRP
Spondyloarthritis:
Characteristic Parameters Used for Diagnosis-I
4 4

Genetics
Predisposing/concomitant diseases
Infection* psoriasis Uveitis
*positive staining for Chlamydia in synovial membrane1
Spondyloarthritis-Characteristic
Parameters Used for Diagnosis II
1. Schumacher HR et al. Arthritis Rheum 1988; 31:937-46
Spondyloarthritis:
Characteristic Parameters Used for Diagnosis-II
HLA-B27
positive
family
history
Crohn‘s
5 5

6

SpA and HLA-B27
Disease Approximate Prevalence of HLA-B27 (%)
AS 90
Reactive arthritis (ReA) 40-80
Juvenile spondyloarthropathy 70
Enteropathic spondyloarthropathy 35-75
Psoriatic arthritis 40-50
Undifferentiated spondyloarthropathy 70
Acute anterior uveitis 50
Aortic incompetence with heart block 80
Khan MA. Ann Intern Med 2002;136(12):896-907

Spondyloarthropathies: group of
disorders characterized by:
Inflammatory axial spine involvement
Asymmetrical peripheral arthritis
Enthesopathy
Inflammatory eye disease
Mucocutaneous features
Rheumatoid factor negative
High frequency of HLA B27 antigen
Familial aggregation

Predominantly Axial
SpA
Ankylosing Spondylitis
Non-radiographic
axial SpA
Predominantly Peripheral
SpA
Reactive arthritis
Psoriatic Arthritis
Arthritis with inflammatory
bowel disease
Undifferentiated SpA
Concept of Spondyloarthritides (SpA)
9 9

Time (years)
Back pain Back pain
Radiographic
sacroiliitis
Back pain
Syndesmophytes
Radiographic stage
Axial Spondyloarthritis
Non-radiographic stage
Sacroiliitis on MRI
Rudwaleit M et al. Arthritis Rheum. 2005;52:1000-8.
Modified New York Criteria 1984
10 10
Ankylosing spondylitis

ASAS Classification Criteria for Axial Spondyloarthritis
(SpA)
Rudwaleit M et al. Ann Rheum Dis 2009;68 777-83
In patients with ≥3 months back pain and age at onset <45 years
#SpA features
• inflammatory back pain
• arthritis
• enthesitis (heel)
• uveitis
• dactylitis
• psoriasis
• Crohn‘s/colitis
• good response to NSAIDs
• family history for SpA
• HLA-B27
• elevated CRP
Sacroiliitis on imaging*
plus
≥1 SpA feature#
HLA-B27
plus
≥2 other SpA features#
OR
*Sacroiliitis on imaging
• active (acute) inflammation on MRI highly suggestive of sacroiliitis associated with SpA
• definite radiographic sacroiliitis according to mod NY criteria
n=649 patients with back pain;
Sensitivity: 82.9%, Specificity: 84.4%
Imaging alone: Sensitivity: 66.2%, specificity: 97.3%
Clinical arm alone: Sensitivity: 56.6%, specificity: 83.3%
11 11

12
ASAS Classification Criteria for Peripheral
Spondyloarthritis (SpA)
Rudwaleit M et al. Rheum Dis 2011;70:25-31 (with permission) 12

Symptoms at presentation determine which
pathway
Apply ASAS Criteria
for Axial SpA1
Apply ASAS Criteria
for Peripheral SpA2
Purely peripheral
symptoms at time of
presentation*
Axial ± peripheral
symptoms at time of
presentation
*Past inflammatory back pain allowed
1Rudwaleit et al. Ann Rheum Dis 2009;68:777-783. 2Rudwaleit et al. Ann Rheum Dis 2011;70:25-31. 13 13

14
ASAS Classification Criteria for Spondyloarthritis
(SpA)
Rudwaleit M et al. Ann Rheum Dis 2011;70:25-31 (with permission 14

Ankylosing Spondylitis

16
Ankylosing Spondylitis (AS)
– AS is a chronic, progressive immune-mediated inflammatory disorder that results in ankylosis of the vertebral column and sacroiliac joints
– The spine and sacroiliac joints are the common affected sites
– Chronic spinal inflammation (spondylitis) can lead to fusion of vertebrae (ankylosis)
1 Taurog JD. et al. Harrison‘s Principles of Internal Medicine, 13 th Ed. 1994: 1664-67.

• Peak onset between 20 and 30 years
• Form of spondyloarthritis (cause inflammation around site of ligament insertion into bone) and association with HLA-B27
• Prevalence as high as 5% in adults with chronic low back pain
• Male to female ratio 2-3:1
• B27 is pozitive in 90-95% of AS.
• B27 pozitive individuals have a 2-5% chance of developing AS
•
Epidemiology

Pathogenesis
• ?development in genetically predisposed individuals, triggered by an environmental factor eg gastro-intestinal infection: Klebsiella pneumoniae
• Reactive arthritis has a similar pathogenesis whereby Chlamydia trachomatis, Yersinia enterocolitica, Shigella flexneri, Campylobactor jejuni, Salmonella typhymurium have been implicated.

Pathogenesis
• There is a high incidence of GI mucosal inflammation (both symptomatic and asymptomatic), this raises the possibility that the gut, with breakdown of the mucosal lining is a triggering event.
• Activated T-cells and macrophages found at sites of inflammation with expression of IL-1β, tnf-α and IF-γ. These inflammatory cytokines cause erosion of cortical bone, new bone formation and loss of bone mass

AS: Characteristic Pathologic Features
Sieper J. Arthritis Res Ther 2009;11:208
Elewaut D & Matucci MC. Rheumatology 2009;48:1029-1035
• Chronic inflammation in:
– Axial structures (sacroiliac joint, spine, anterior chest
wall, shoulder and hip)
– Possibly large peripheral joints, mainly at the lower limbs
(oligoarthritis)
– Entheses (enthesitis)
• Bone formation particularly in the axial joints
Inflammation
Disease activity
Structural damage
Syndesmophytes formation

Clinical Features of AS
Skeletal Axial arthritis (eg, sacroiliitis and spondylitis)
Arthritis of ‘girdle joints’ (hips and shoulders)
Peripheral arthritis uncommon
Others: enthesitis, osteoporosis, vertebral,
fractures, spondylodiscitis, pseudoarthrosis
Extraskeletal Acute anterior uveitis
Cardiovascular involvement: aortic regurgitation,
conduction abnormalities
Pulmonary involvement: apical fibrobullous
disease
Cauda equina syndrome
Enteric mucosal lesions
Amyloidosis

Symptoms • Chronic systemic inflammatory disease involving axial
skeleton of younger patients
• Develops in second/third decade
• Typically dull aching pain of insidious onset in lower lumber/ buttock region
• Early morning stiffness and nocturnal pain
• Stiffness improves with exercises and recurs after periods of inactivity
• Some patients present with painful hips, shoulders, asymmetrical arthritis of lower limbs prior to spinal involvement
• Cervical and thoracic pain and stiffness is frequent

23

Inflammatory back pain - characteristics
• insidious onset before age 40
• persistence for at least 3 months
• accentuation of back pain at night
or after prolonged rest
• back pain improves with exercise

Buttock pain

Physical Exam: Reduced range of
motion: Schober test



14.10.2014 29
“ skier position”

• Chest expansion: expansion of less than 2.5cm abnormal (5cm considered normal)
• Sacroiliac joint tenderness
• Hip joint involvement
• Peripheral joint involvement (dactylitis- “sausage toes”)
Physical Examination

Peripheral manifestations
Enthesitis Peripheral arthritis Dactylitis
AS: Signs and Symptoms
50% patients with
enthesitis1
1Cruyssen BV et al. Ann Rheum Dis 2007;66:1072-1077 2Sidiropoulos PI et al. Rheumatology 2008;47:355-361
Up to 58% patients
ever had arthritis1
Mch smaller number
of patients

Why are Dactylitis and Enthesitis Important?
The first abnormality to appear in swollen joints associated with
spondyloarthropathies is an enthesitis2
Likelihood of erosions is higher for digits with dactylitis than
those without1
1Brockbank. Ann Rheum Dis 2005;62:188-90; 2McGonagle et al. The Lancet 1998;352.

Enthesopathy
Erosion
New bone

Heel tendonitis in AS

AS: Extra-skeletal Signs and Symptoms
Other common symptoms seen during the early stages of disease
include:
• Anorexia
• Malaise
• Low grade fever
• Weight loss
• Fatigue
1Missaoui B. et al. Ann Readapt Med Phys 2006;49:305-8, 389-391
Linden VD et al. Chapter 10. In: Firestein, Budd, Harris, McInnes, Ruddy and Sergent, eds. Kelley’s
Textbook of Rheumatology: Spondyloarthropathies. 8th ed. Saunders Elsevier;2009:p.1176
Fatigue is a frequent complaint
of patients with AS1

AS: Extra-articular Manifestations
Extra-articular manifestations Prevalence in AS
Patients (%)
Anterior uveitis 30-50
IBD 5-10
Subclinical inflammation of the gut 25-49
Cardiac abnormalities
Conduction disturbances
Aortic insufficiency
1-33
1-10
Psoriasis 10-20
Renal abnormalities 10-35
Lung abnormalities
Airways disease
Interstitial abnormalities
Emphysema
40-88
82
47-65
9-35
Bone abnormalities
Osteoporosis
Osteopenia
11-18
39-59
Elewaut D & Matucci MC. Rheumatology 2009;48:1029-1035
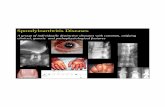
Terminal ileitis
Anterior uveitis
Cardiac
abnormalities

Recurrent Iritis caused Synechiae (adhesions
between the lens and iris)
Acute anterior uveitis: occurs in 25-40% of patients
- Presents as acute unilateral pain, photophobia, and blurring of vision

• ESR and CRP typically elevated
• HLA-B27: present in 8% of population, prevalence in HLA-B27 positive population is only 5%
• Normocytic, normochromic anemia
Laboratory Tests

X Ray:
• Widening, erosions, sclerosis, or ankylosis of sacroiliac joint
• Early signs: squaring of vertebral bodies due to anterior and posterior spondylitis
• Late stages: proliferative changes, anterior atlantoaxial subluxation
MRI: more sensitive- can use in patients who do not have sacroiliitis on plain radiographs (can see “bone marrow edema”)
Imaging

Sacroiliitis: Scoring System • Grade 0 : Normal
• Grade 1: Suspicious changes
• Grade 2: Minimal Change. Localized erosions or sclerosis not altering joint width
• Grade 3: Definite moderate to severe change, with one or more of the following:
• Erosions; Sclerosis; Joint Space Widening; Joint Space Narrowing; Partial ankylosis
• Grade 4: Severe. Total Ankylosis
SpA Characteristic XRAY
change
Erosions
Osteitis (Sclerosis)
Bridging Syndesmophytes
Ankylosis of joints

Symmetrical Sacroiliitis Ankylosing Spondylitis
(abnormal) (abnormal)

42
Sacroiliitis Grade 3 Bilaterally
42


Sacroiliitis grade II
bilat.
Sclerosis Erosions

45
Definition of Positive MRI-SI Joint
ASAS handbook, Ann Rheum Dis 2009;68 (Suppl II) (with permission) 45

How to Define Active Inflammatory Lesions (‘positive MRI‘)
of the Sacroiliac Joint
• The presence of definite subchondral bone marrow edema/osteitis
highly suggestive of sacroiliitis is mandatory.
• The presence of synovitis, capsulitis, or enthesitis only without
subchondral bone marrow edema/ osteitis is compatible with but
not sufficient for making a diagnosis of active sacroiliitis.
Rudwaleit M et al, Ann Rheum Dis 2009;68:1520-27
• STIR images are usually sufficient to detect active (acute) inflammatory
lesions; exception: synovitis (not detectable with STIR only).
• Amount of signal required
– If there is 1 signal (lesion) only, this should be present on at least 2
slices. If there is more than 1 signal on a single slice, 1 slice may be
enough.
46 46

Syndesmophytes, apophyseal joint fusion, disc
peripheral ossification (AS)

Ankylosing Spondylitis
“Bamboo Spine”
Repeated process of healing and bone
formation leads to formation of
syndesmophytes
‘bone bridges’
ACR Slide Collection on the Rheumatic Diseases; 3rd edition. 1994.

Ankylosing Spond. Left: squaring of vertebra, Rt:
ant. longitudinal lig.calcification

Ankylosing Spondylitis: Bamboo spine ,ossification
follow the contour of intervertebral discs

Bamboo spine:
1. Syndesmophyte
2. “rail”=the ossification of
the posterior apophyseal joints
3.” wire”= ossification of the
ligaments

14.10.2014 52

Ankylosing Spondylitis: calcaneal spur and erosion

Plantar periostitis seen in AS

Unilateral sacroiliitis

AS: A Debilitating Rheumatic Disease
Over time, joints in the spine can fuse together and cause a fixed, bent-forward posture
1Linden VD et al. Chapter 10. In: Firestein, Budd, Harris, McInnes, Ruddy and Sergent, eds. Kelley’s
Textbook of Rheumatology: Spondyloarthropathies. 8th ed. Saunders Elsevier;2009:p.1171 2 Braun J & Sieper. J Rheumatology 2008;47:1738-40
AS patients have an important
impact on health care and non
health-care resource utilization,
resulting in a mean total cost
(direct and productivity) of about
$6700 to $9500/year/patient1
More than 30% of patients
carry a heavy burden of
disease and have a decreased
QoL2

57
Modified New York Criteria for Ankylosing Spondylitis
(1984)
van der Linden et al. Arthritis Rheum. 1984 Apr;27(4):361-8. 57

Reiter's syndrome
Rheumatoid arthritis
Gonococcal arthritis
Psoriatic arthritis
Age Young Middle Young Middle
Gender Male>female Female>male Female>male No effect
Onset Abrupt Insidious Abrupt Insidious
Joint numbr Oligoarthritis Polyarthritis Monoarthritis or oligoarthritis
Oligoarthritis
Symmetry of arthritis
No Yes No No
Sausage digits
Yes No No Yes
Back pain Yes No No Yes
Urethritis Yes No Yes No
Skin lesions Palms and soles in 10 percent
Subcutaneous nodules
Pustular, nodular or vesicular
Psoriasis
Gonococcus No No Yes No

59

• Symptomatic relief
• Restore function
• Prevent joint damage
• Prevent spinal fusion (prevent progressive bony erosions and ankylosis of the spine)
• Minimize extraspinal and extraarticular manifestations
• Prevent complications of spinal disease
Goals of Therapy

• Global pain
• Axial pain
• Degree and duration of morning stiffness
• Activities that are limited
• ESR or CRP are useful as laboratory parameters of active disease
Assessment of disease activity

• Hip arthritis
• Dactylitis
• Poor efficacy of NSAIDs
• High ESR
• Limitation in ROM of lumbar spine
• Oligoarthritis
• Onset less than 16 years of age
Prognostic Indicators


Treatment
Treat symptoms with NSAIDs
Physical therapy,stretching and exercises to preserve spine and joints function
Maintain good posture
Sulfasalazine,Methotrexate used ,found beneficial (in peripheral disease)
Anti TNF drugs emerging role
Prevent eye complications by early recognition and treatment

14.10.2014 65

Management recommendations
66 66

ASAS-Recommendations for the treatment of AS Patients
with TNF-Blockers
Diagnosis: fulfillment of the mod. New York criteria for
AS or the ASAS criteria for axial SpA
Failure of standard treatment:
• at least 2 NSAIDs over 4 weeks (in total)
• one local steroid injection if appropriate
• normally a therapeutic trial of a DMARD,
preferably sulfasalazine (not mandatory)
High disease activity: BASDAI ≥4
Predominant
peripheral
manifestations
Positive expert opinion based on parameters such as:
• Positive CRP/ESR
• Positive MRI
• Radiological Progression
• Clinical examination
plus
Predominant axial manifestations
van der Heijde et al. Ann Rheum Dis 2011:905-8.

68
Bath Ankylosing Spondylitis Disease Activity Index (BASDAI)
• The BASDAI is measured using the following VAS (0 to 10 cm) of subject self-assessments:
Garrett S, et al. J Rheumatol. 1994;21:2286–2291.
• Fatigue
• Spinal pain
• Joint pain
• Enthesitis
• Inflammation
– Duration morning stiffness
– Severity morning stiffness

69

70
TNFα PATHOGENIC IMPLICATIONS IN AS
Toussirot and Wendling, 1994. Gratacos, 1994.Cannete et al. 1997. Grom et al.1996.Braun et al. 1995
Biopsy o the sacroiliac joint
• Higher level of TNF-α in the serum
• Overasserting of TNF-α in the synovial tissue of the SIJ

71
INFLIXIMAB (REMICADE)
– Chimeric monoclonal antibody
– Made of the constant region of the G1 human Ig to which the variable region of a murine Ig with high specificity for TNF-α of which it was fixed.

72
14.10.2014 7
2
INFLIXIMAB (REMICADE®)
• dose: 5 mg/kg body weight, in perfusion, in weeks So, S2, S6 and later once at 8 weeks.
• Ankylosing Spondylitis Study for the Evaluation of Recombinant Infliximab Therapy (ASSERT)
• Insufficient response: the dose is risen up to maximum 10 mg/kg
body weight or
the dosing interval can be diminished to 4-6 weeks

73
ADALIMUMAB (HUMIRA)
• Fully-human monoclonal antibody
• Specific binding to TNFα
• Dual mechanism of action:
– neutralization of TNFα
– rapid removal of TNFα from circulation

74
ETANERCEPT (ENBREL)
• A molecule made of 2 extracellular regions that connect the p75 receptor of the TNFα connected to the Fc of G1 human Ig.
• Binds TNFα and TNFβ.

75
14.10.2014 7
5
ADALIMUMAB (HUMIRA®)
• dose: 40 mg, subcutaneously, at 2 weeks
ETANERCEPT (ENBREL®)
• dose: 50mg/week, subcutanously

76
ANTI-TNF-α – BIOLOGICAL THERAPY
• Before of the beginning of the treatment it is obligatory to:
– Screen for tuberculosis: tuberculin test (PPD) and chest X-ray
– Screen for viral infection: B and C hepatitis, HIV
– Exclusion of neoplasia and demyelination diseases
– Exclusion of asociate autoimmune phenomena (anti ds DNA antibodies)

77
BIOLOGICAL THERAPY MAIN EXCLUSION CRITERIA/CONTRAINDICATIONS
• Pregnancy /breast-feeding
• Autoimmune diseases associated : systemic lupus erythematosus and multiple sclerosis
• Severe chronic heart failure (class III/IV NYHA)
• Demyelinating diseases
• Optical Neuritis
• Tuberculosis: active infection or a history of tuberculosis or positive PPD test
• Cancer, personal history of neoplasia (except neoplasia without recurrence for ≥ 10 years)
• Active/chronic/recurrent infections (infection with HBV, HCV, HIV)
• Septic arthritis (≤ 12 months)
• Infection of joint prostheses (≤ 12 months-if the prosthesis is extracted or is on an indefinite period - if the prosthesis remains in situ)

78 BIOLOGICAL THERAPY - MAIN SIDE EFFECTS
• Acute side effects of intravenous perfusion: fever, headache, pruritus, urticaria, hypotension, dyspnoea - infliximab;
• Infections - tuberculosis relapse - all anti-TNF-α biological agents;
• Hypersensitivity of delayed type: myalgia, arthralgia, erythema, oedema;
• Autoimmune Phenomena: human antichimeric antibodies (HACA), antinuclear antibodies (ANAs), anti-double-stranded DNA autoantibodies (lupus-like phenomena)-infliximab;
• Cardio-vascular events: worsening of heart failure, arrhythmias;
• Digestive manifestations: nausea, diarrhea;
• Neurological manifestations: demyelinating syndromes;
• Hematological manifestations: leucopenia, anemia, thrombocytopenia;
• Neoplasias, lymphomas.