
Colangiopatie autoimmuni ed epatiti autoimmuni, malattie ... · Colangiopatie autoimmuni ed epatiti...
101
Colangiopatie autoimmuni ed epatiti autoimmuni, malattie prevalenti nella donna Annarosa Floreani Dept. of Surgery, Oncology and Gastroenterology, University of Padova 16 settembre 2017
Transcript of Colangiopatie autoimmuni ed epatiti autoimmuni, malattie ... · Colangiopatie autoimmuni ed epatiti...

Colangiopatie autoimmuni ed epatiti
autoimmuni, malattie prevalenti nella donna
Annarosa FloreaniDept. of Surgery, Oncology and Gastroenterology,
University of Padova
16 settembre 2017
Annarosa Floreani, MD, Dept. of Surgery, Oncology and Gastroenterology, University of Padova, Italy
Declares to have participated over the last 12 months in the Advisory Committee of the PBC Group
sponsored by Intercept
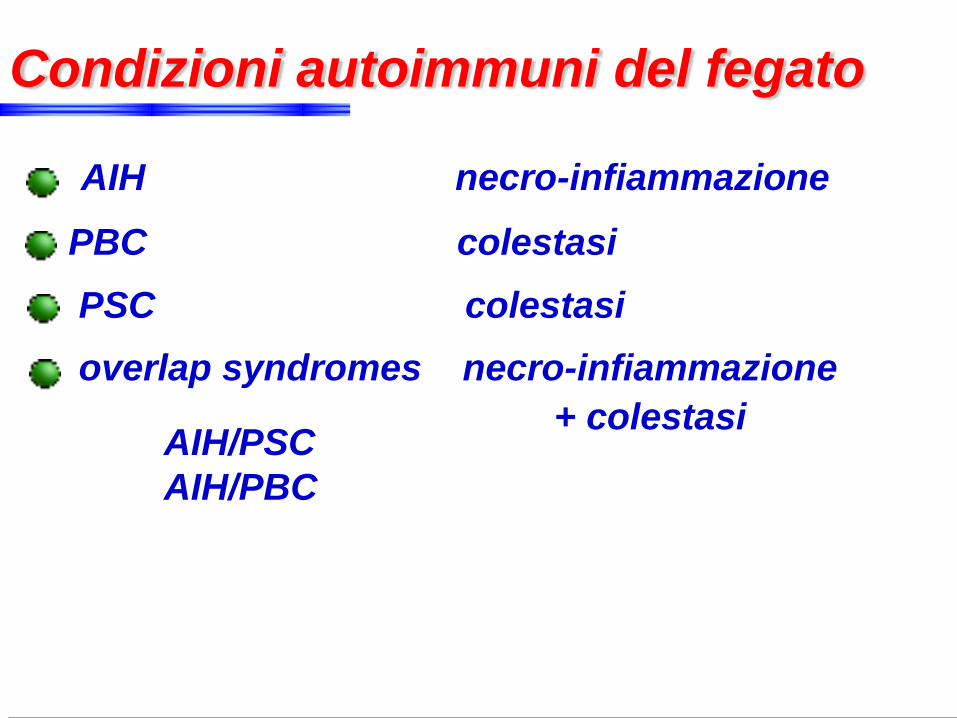
Condizioni autoimmuni del fegato
AIH necro-infiammazione
PBC colestasi
PSC colestasi
overlap syndromes necro-infiammazione
+ colestasi AIH/PSC
AIH/PBC
predisposizione genetica
fattori triggers (agenti infettivi, farmaci, tossici)
difetti dell’immunoregolazione
Eziopatogenesi
B
Co- stimuli
Class I
Class II
K
TSTS
APC
P
TNF-aIFN-g
M
TCTC
TH2TH2
TH0
cellLiver
IL-1IL-1
B
Co- stimuliCo- stimuli
Class I
Class II
IL-2IL-2
IL-12IL-12
K
TsTs
IL-4IL-4IL-10IL-10
APC
P
TNF-aTNF-aIFN-gIFN-g
MIFN-gIFN-g
TcTc
Th2Th2
cellLiver
IL-4IL-4
Th0
Th1
B
Co- stimuli
Class I
Class II
K
TSTS
APC
P
TNF-aIFN-g
M
TCTC
TH2TH2
TH0
cellLiver
IL-1IL-1
B
Co- stimuliCo- stimuli
Class I
Class II
IL-2IL-2
IL-12IL-12
NK
TsTr
IL-4IL-4IL-10IL-10
APC
P
TNF-aTNF-aIFN-gIFN-g
M
IFN-gIFN-g
TcTc
Th2Th2
cellLiver
IL-4IL-4
Th0
Th1
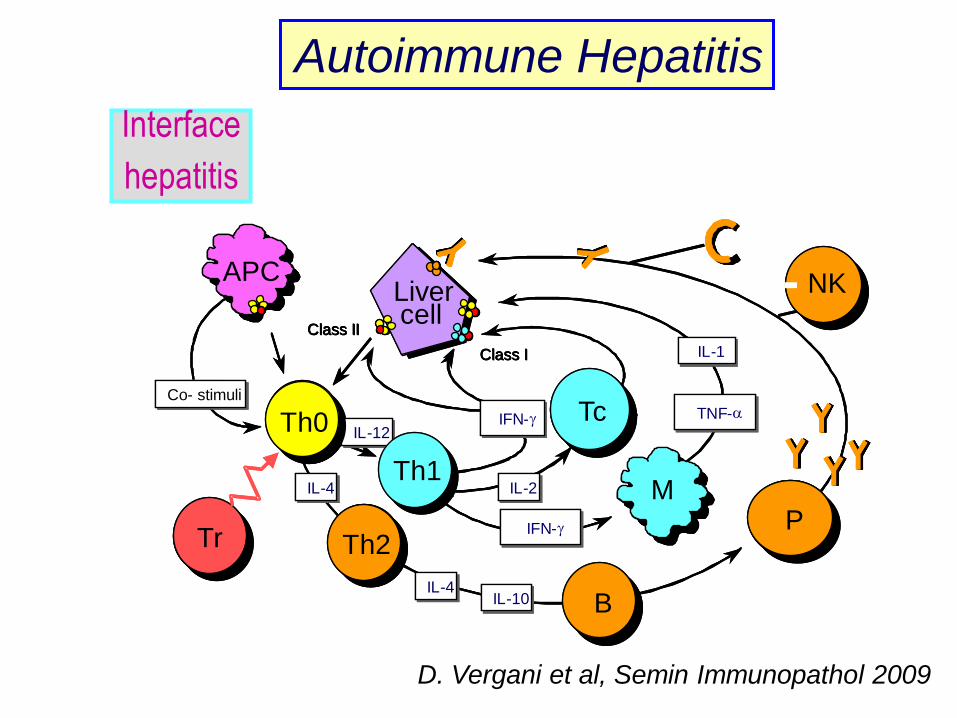
Autoimmune Hepatitis
Interface
hepatitis
D. Vergani et al, Semin Immunopathol 2009

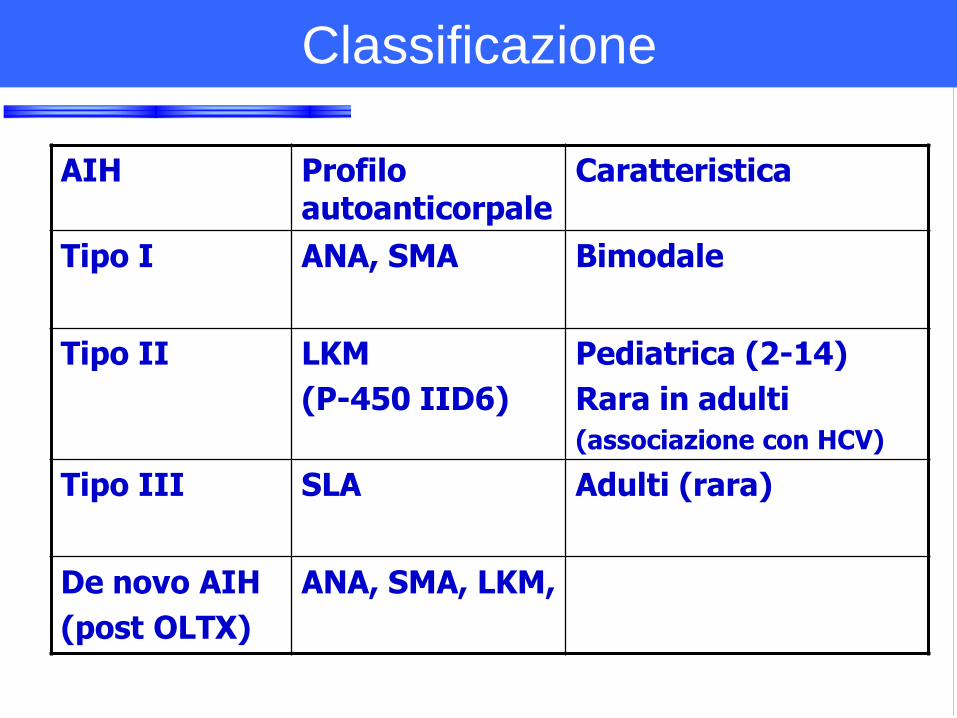
AIH Profilo autoanticorpale
Caratteristica
Tipo I ANA, SMA Bimodale
Tipo II LKM
(P-450 IID6)
Pediatrica (2-14)
Rara in adulti
(associazione con HCV)
Tipo III SLA Adulti (rara)
De novo AIH
(post OLTX)
ANA, SMA, LKM,
Classificazione
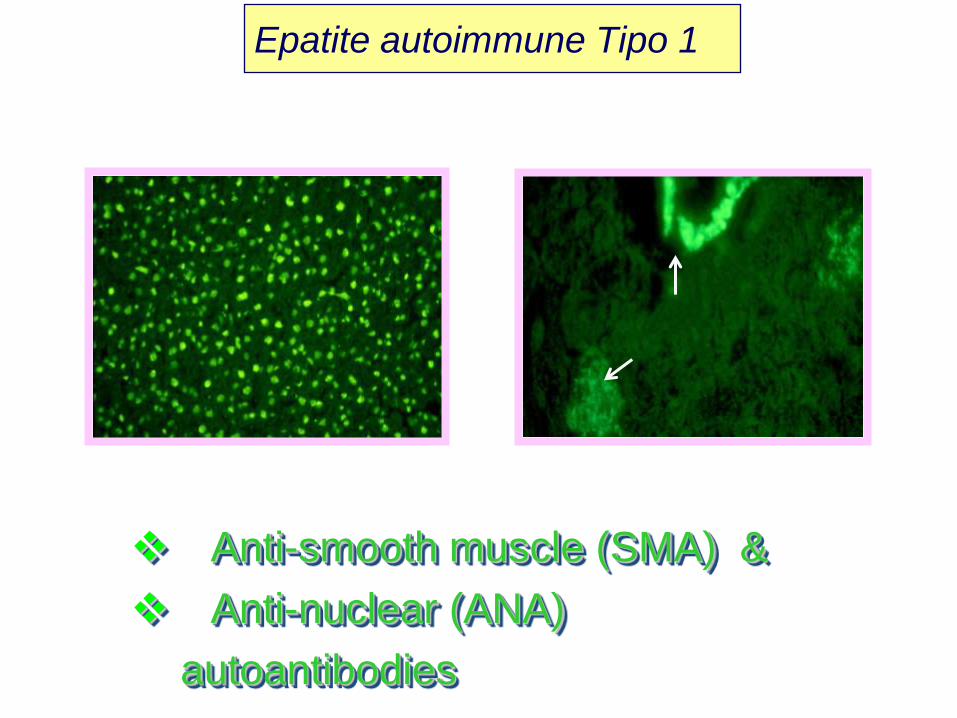
Anti-smooth muscle (SMA) &
Anti-nuclear (ANA)
autoantibodies
Epatite autoimmune Tipo 1
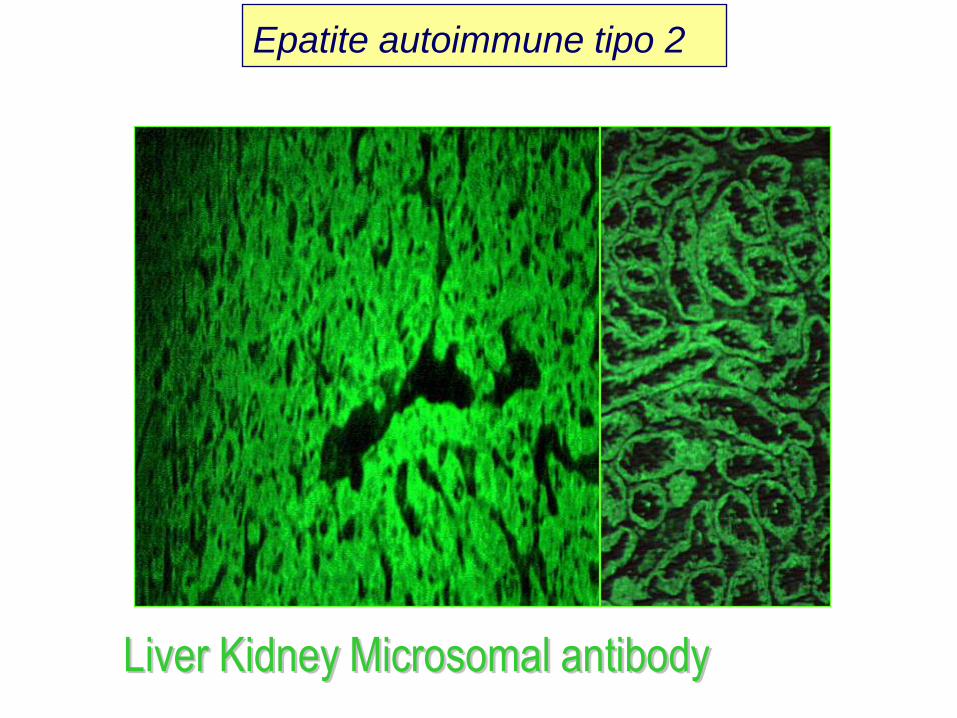
Liver Kidney Microsomal antibody
Epatite autoimmune tipo 2
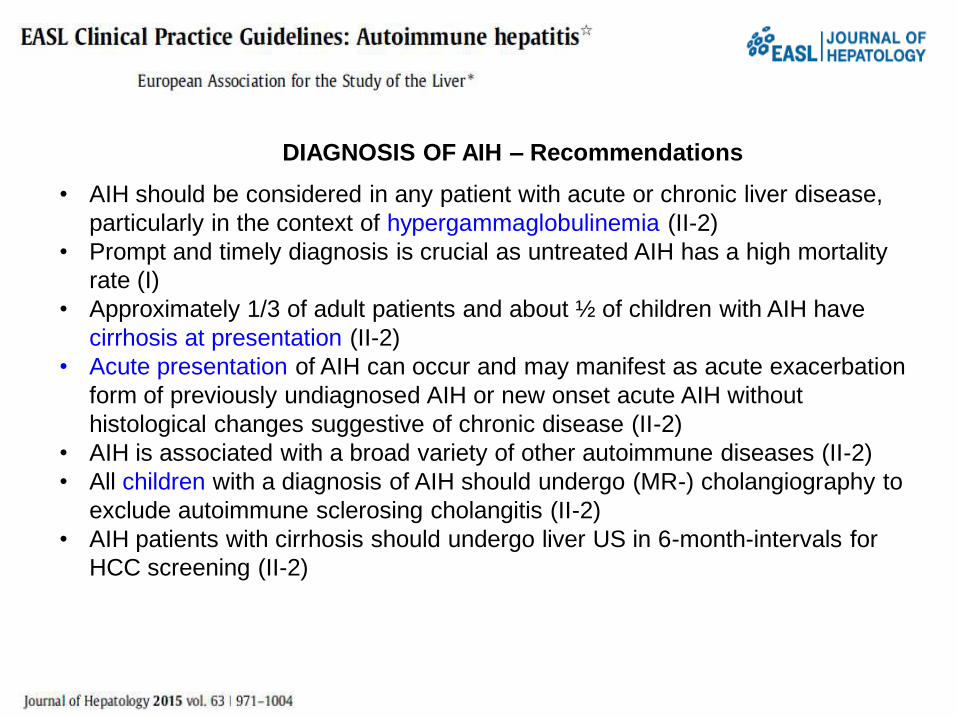
DIAGNOSIS OF AIH – Recommendations
• AIH should be considered in any patient with acute or chronic liver disease,
particularly in the context of hypergammaglobulinemia (II-2)
• Prompt and timely diagnosis is crucial as untreated AIH has a high mortality
rate (I)
• Approximately 1/3 of adult patients and about ½ of children with AIH have
cirrhosis at presentation (II-2)
• Acute presentation of AIH can occur and may manifest as acute exacerbation
form of previously undiagnosed AIH or new onset acute AIH without
histological changes suggestive of chronic disease (II-2)
• AIH is associated with a broad variety of other autoimmune diseases (II-2)
• All children with a diagnosis of AIH should undergo (MR-) cholangiography to
exclude autoimmune sclerosing cholangitis (II-2)
• AIH patients with cirrhosis should undergo liver US in 6-month-intervals for
HCC screening (II-2)
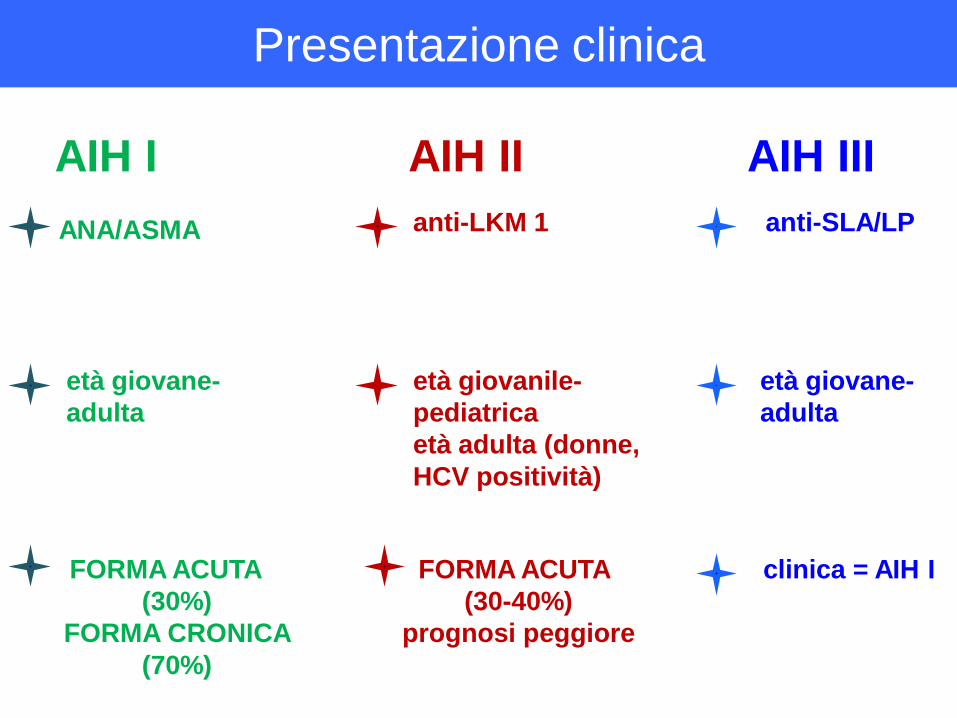
AIH I
FORMA ACUTA
(30%)
FORMA CRONICA
(70%)
ANA/ASMA
età giovane-
adulta
AIH II
anti-LKM 1
età giovanile-
pediatrica
età adulta (donne,
HCV positività)
FORMA ACUTA
(30-40%)
prognosi peggiore
AIH III
anti-SLA/LP
età giovane-
adulta
clinica = AIH I
Presentazione clinica
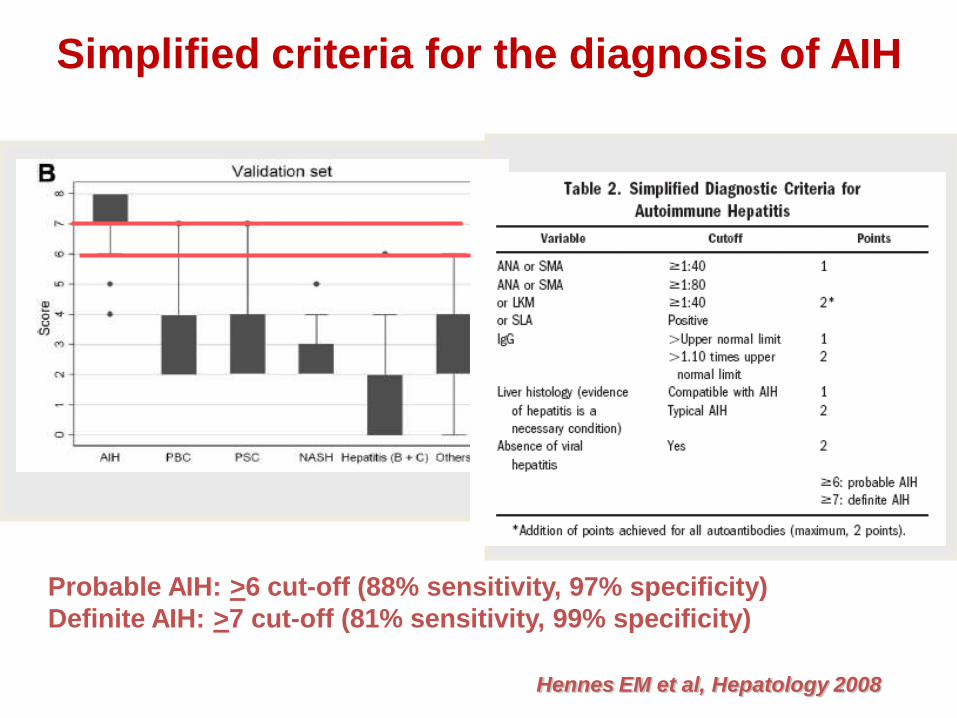
Simplified criteria for the diagnosis of AIH
Probable AIH: >6 cut-off (88% sensitivity, 97% specificity)
Definite AIH: >7 cut-off (81% sensitivity, 99% specificity)
Hennes EM et al, Hepatology 2008
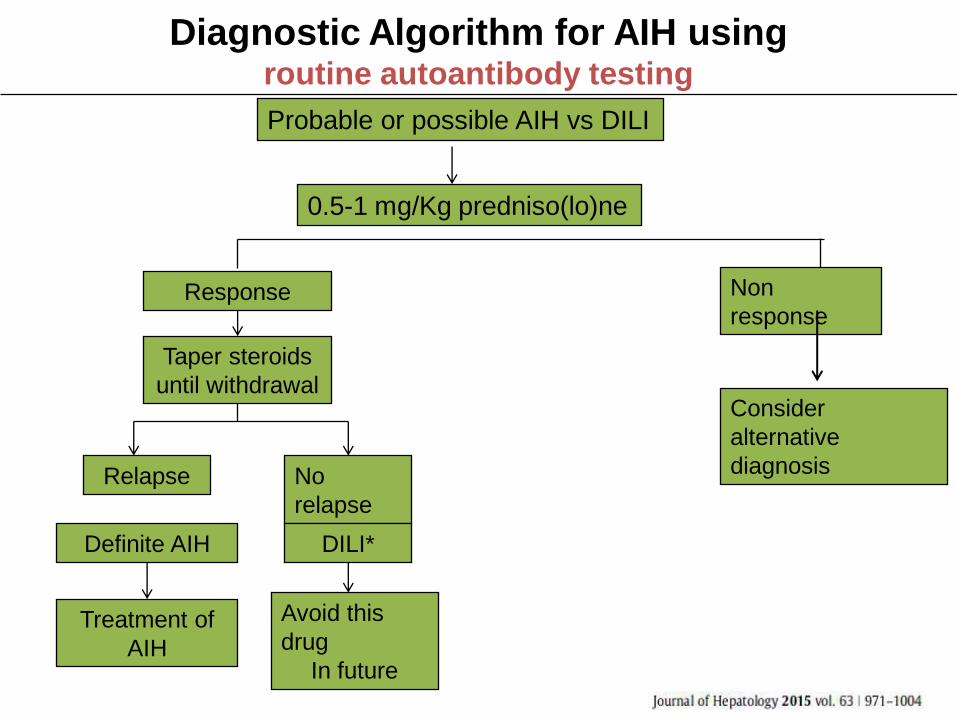
Diagnostic Algorithm for AIH usingroutine autoantibody testing
Probable or possible AIH vs DILI
0.5-1 mg/Kg predniso(lo)ne
Response
Relapse
Treatment of
AIH
Avoid this
drug
In future
Consider
alternative
diagnosis
Non
response
No
relapse
DILI*Definite AIH
Taper steroids
until withdrawal

Therapeutic options for AIH remission according to the AASLD guidelines

Therapeutic options for AIH remission according to the EASL guidelines
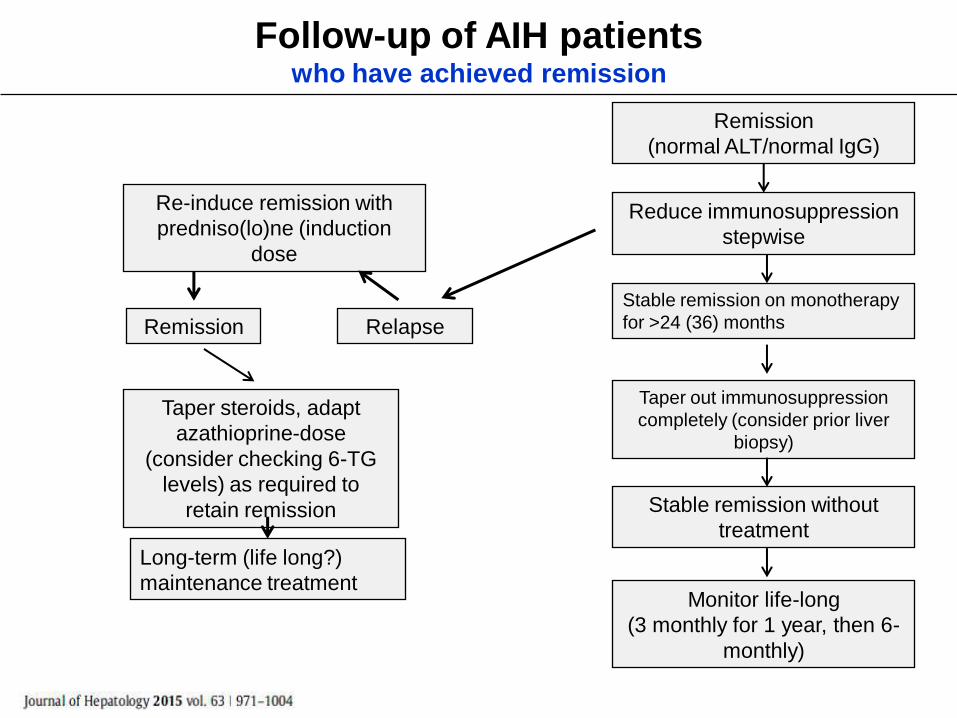
Follow-up of AIH patients who have achieved remission
Remission
Stable remission on monotherapy
for >24 (36) months
Reduce immunosuppression
stepwise
Remission
(normal ALT/normal IgG)
Taper steroids, adapt
azathioprine-dose
(consider checking 6-TG
levels) as required to
retain remission
Relapse
Taper out immunosuppression
completely (consider prior liver
biopsy)
Stable remission without
treatment
Monitor life-long
(3 monthly for 1 year, then 6-
monthly)
Re-induce remission with
predniso(lo)ne (induction
dose
Long-term (life long?)
maintenance treatment

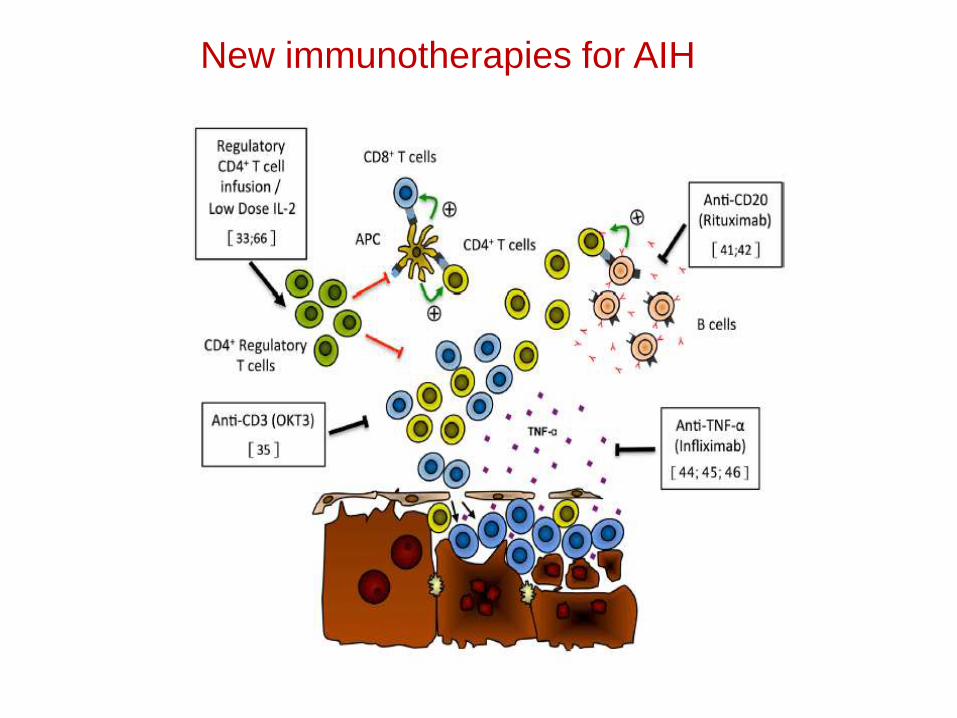
New immunotherapies for AIH
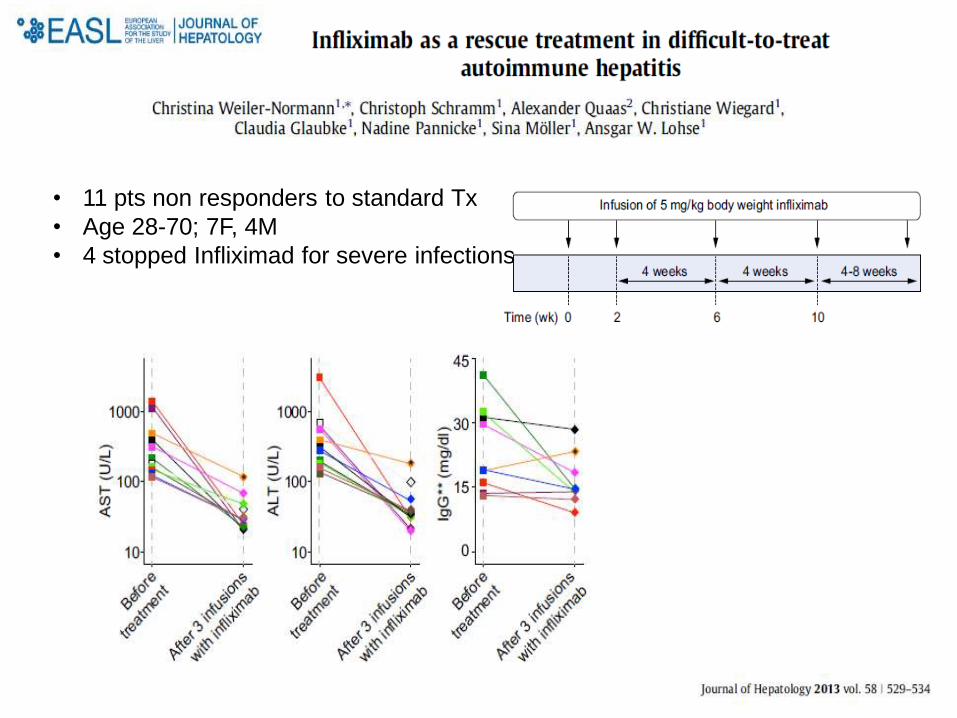
• 11 pts non responders to standard Tx
• Age 28-70; 7F, 4M
• 4 stopped Infliximad for severe infections
Liver Transplantation
End-stage liver disease
– Complications of portal hypertension
– Hepatocellular carcinoma
Fulminant liver disease
– Acute liver injury
– Acute decompensation superimposed on chronic liver injury
Results
– 5 yr pt and graft survival: 80-90%
– Recurrence: 15-40%
– Higher rates of acute and chronic rejection
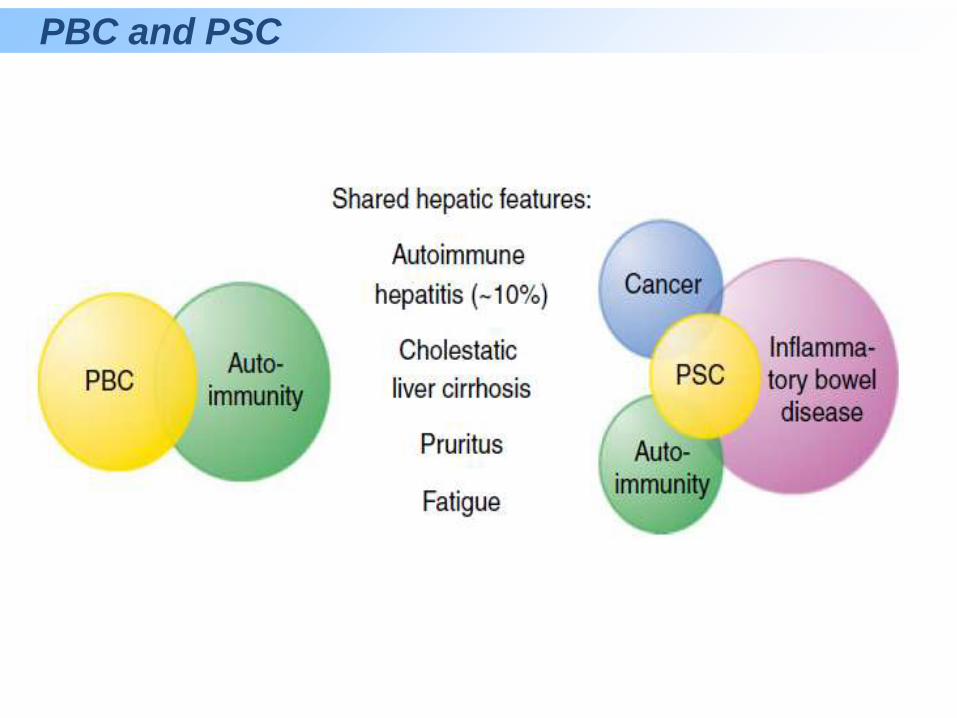
PBC and PSC
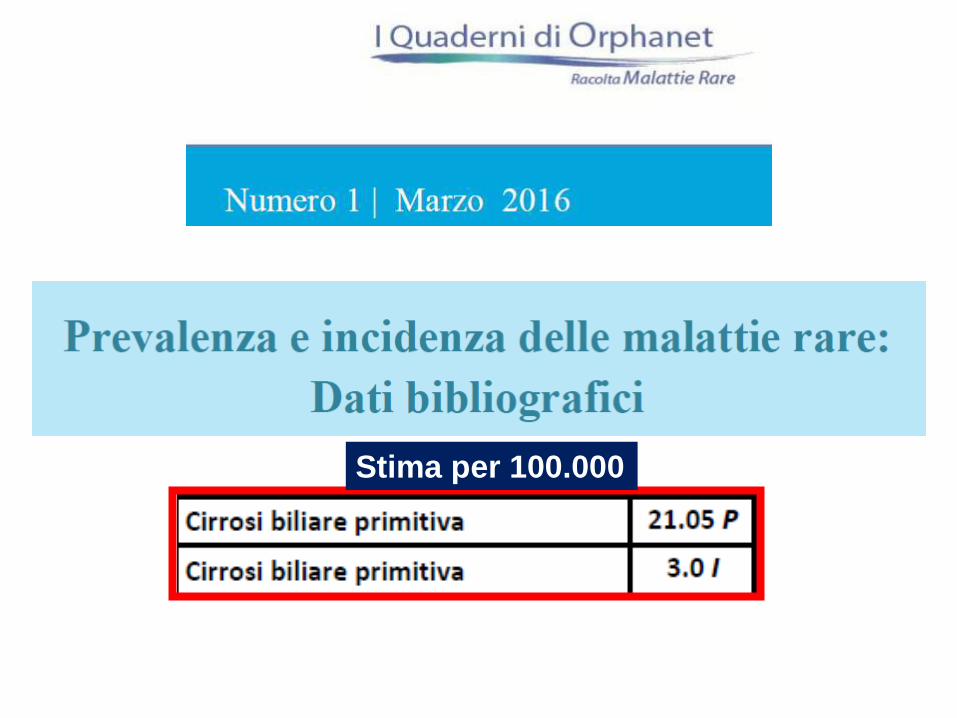
Stima per 100.000
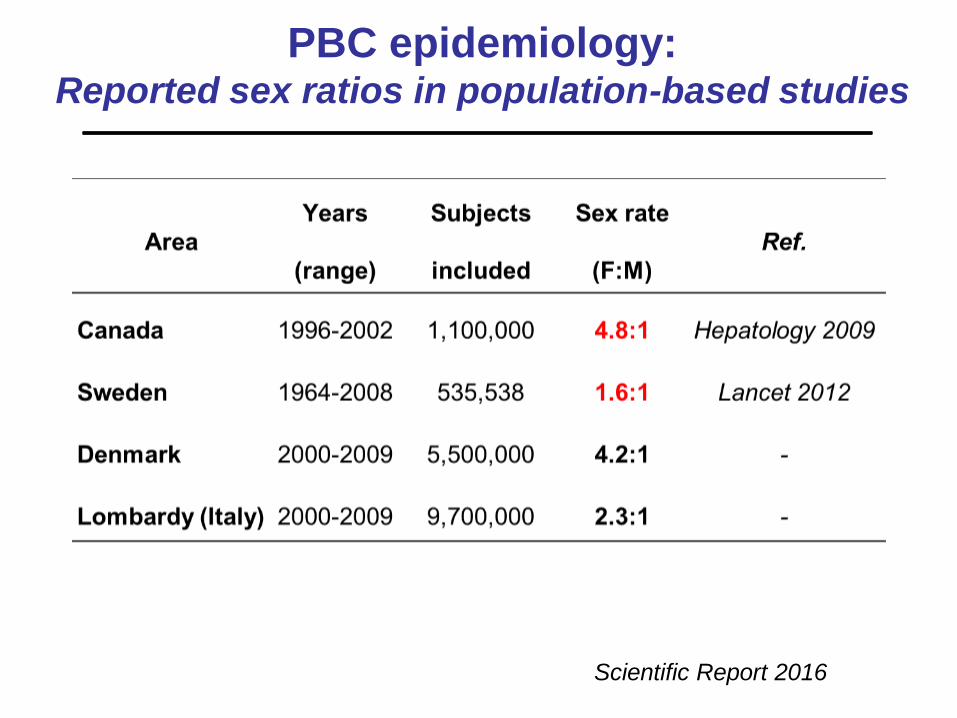
PBC epidemiology: Reported sex ratios in population-based studies
Scientific Report 2016
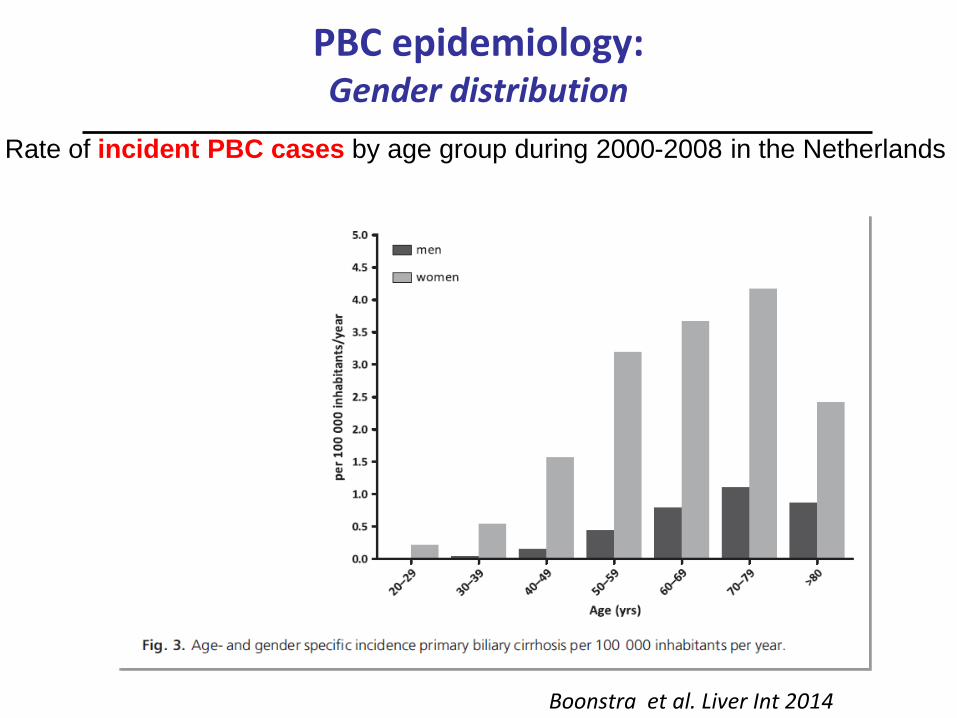
PBC epidemiology: Gender distribution
Rate of incident PBC cases by age group during 2000-2008 in the Netherlands
Boonstra et al. Liver Int 2014

Lombardia population
Inhabitants (about
10.000.000)
M:F PBC RATIO = 1:2
Denmark population
Inhabitants (about
5.500.000)
M:F PBC RATIO = 1:4
Scientific Report 2016

Global PBC Study Group
Dallas
Edmonton
Seattle
Toronto
Rochester
Birmingham
London
Paris
Barcelona
Leuven
Amsterdam
&
Rotterdam
MilanPadua
W.J. Lammers, MD PhD
> 20 centers world-wide - European and North American medical centers> 20 centers world-wide - European and North American medical centers
Acknowledgments
All members of the Global PBC Study Group
Networking story in PBC
2011 2012
Swiss PBC
Austro-German
PBC
2016-17
ERN-RARE
LIVEREuropean Reference
Network
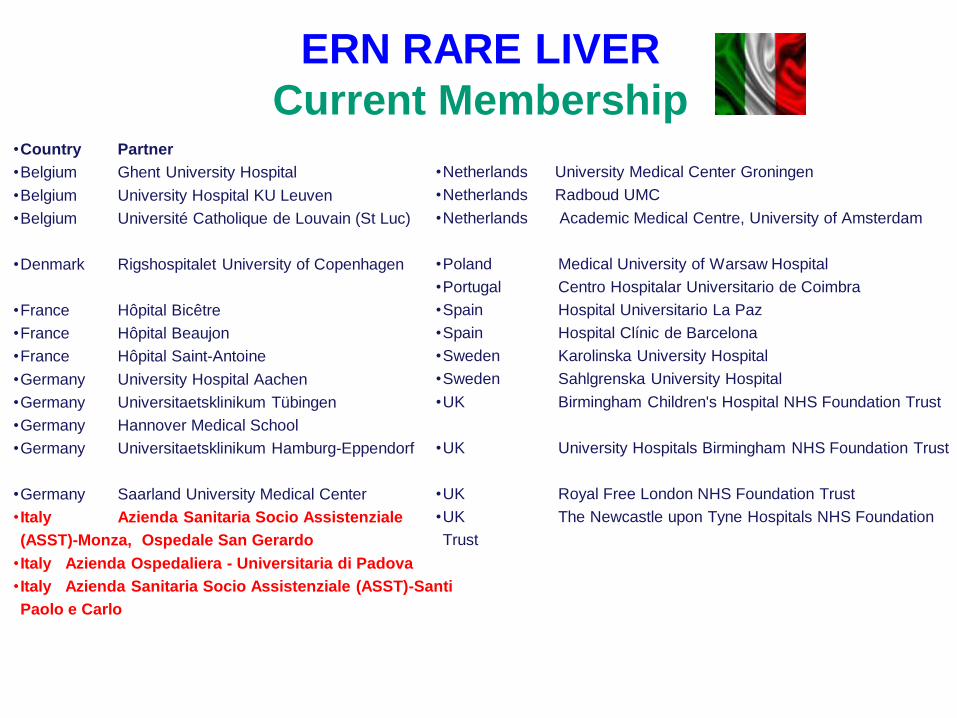
ERN RARE LIVER
Current Membership•Country Partner
•Belgium Ghent University Hospital
•Belgium University Hospital KU Leuven
•Belgium Université Catholique de Louvain (St Luc)
•Denmark Rigshospitalet University of Copenhagen
•France Hôpital Bicêtre
•France Hôpital Beaujon
•France Hôpital Saint-Antoine
•Germany University Hospital Aachen
•Germany Universitaetsklinikum Tübingen
•Germany Hannover Medical School
•Germany Universitaetsklinikum Hamburg-Eppendorf
•Germany Saarland University Medical Center
• Italy Azienda Sanitaria Socio Assistenziale
(ASST)-Monza, Ospedale San Gerardo
• Italy Azienda Ospedaliera - Universitaria di Padova
• Italy Azienda Sanitaria Socio Assistenziale (ASST)-Santi
Paolo e Carlo
•Netherlands University Medical Center Groningen
•Netherlands Radboud UMC
•Netherlands Academic Medical Centre, University of Amsterdam
•Poland Medical University of Warsaw Hospital
•Portugal Centro Hospitalar Universitario de Coimbra
•Spain Hospital Universitario La Paz
•Spain Hospital Clínic de Barcelona
•Sweden Karolinska University Hospital
•Sweden Sahlgrenska University Hospital
•UK Birmingham Children's Hospital NHS Foundation Trust
•UK University Hospitals Birmingham NHS Foundation Trust
•UK Royal Free London NHS Foundation Trust
•UK The Newcastle upon Tyne Hospitals NHS Foundation
Trust

PBC/HCV
• 14/170 (8%)
• At presentation, the HCV-infected PBC group had significantly lower levels of ALP, GGT, and IgM than the AMA+ or AMA- PBC patients (p<0.01).
• Increased risk for HCC
• 9/76 (11.8%)
• PBC/HCV+ vs PBC/HCV- 1:3
• HCV+ significantly higher Child-Pugh and MELD
• Higher incidence of HCC
• No difference in survival
Floreani A et al. AJG 2003 Chen W-H et al, Ann Hepatol 2013
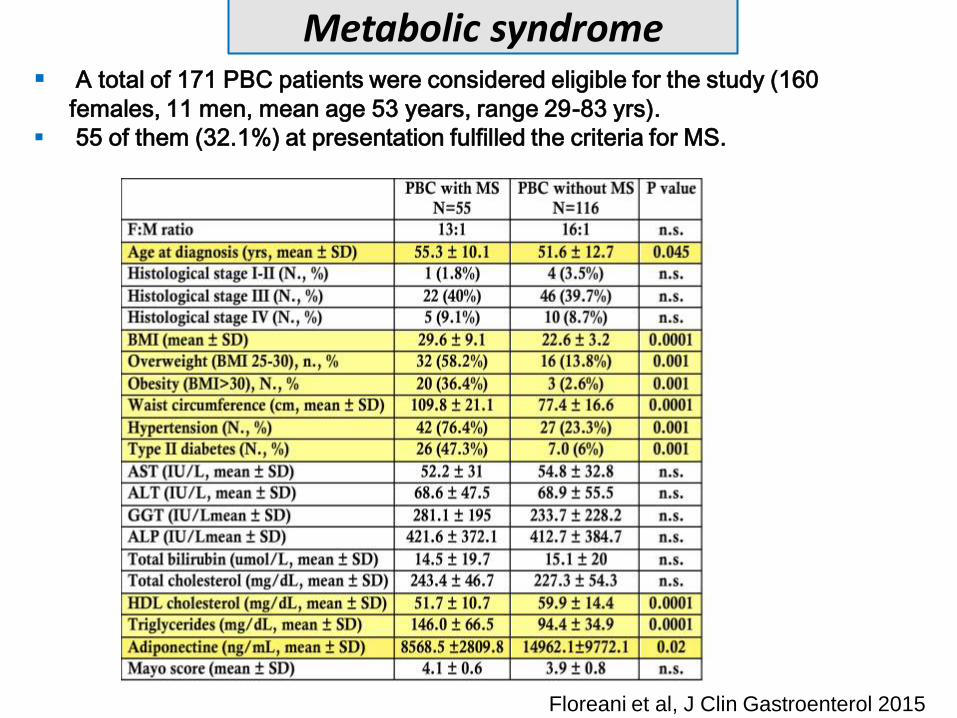
A total of 171 PBC patients were considered eligible for the study (160
females, 11 men, mean age 53 years, range 29-83 yrs).
55 of them (32.1%) at presentation fulfilled the criteria for MS.
Metabolic syndrome
Floreani et al, J Clin Gastroenterol 2015
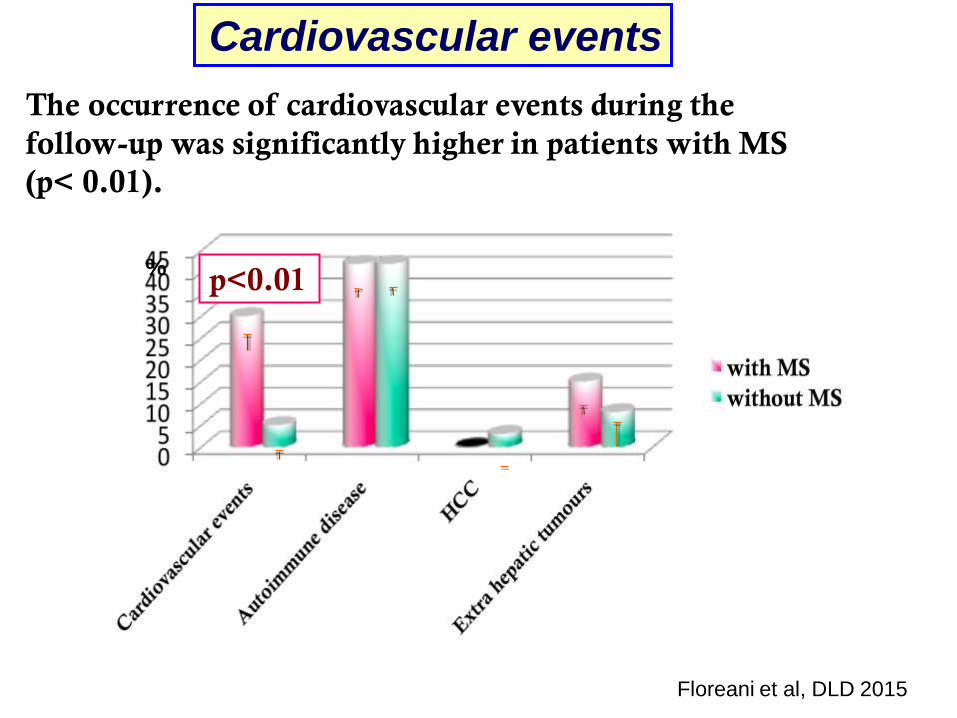
The occurrence of cardiovascular events during the
follow-up was significantly higher in patients with MS
(p< 0.01).
p<0.01%
Cardiovascular events
Floreani et al, DLD 2015
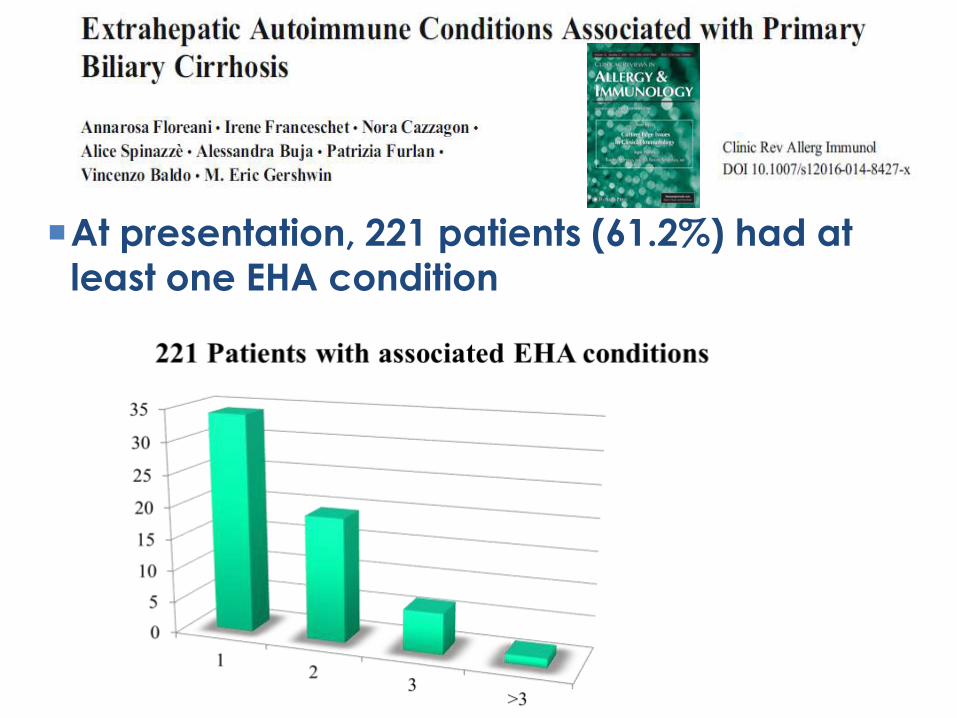
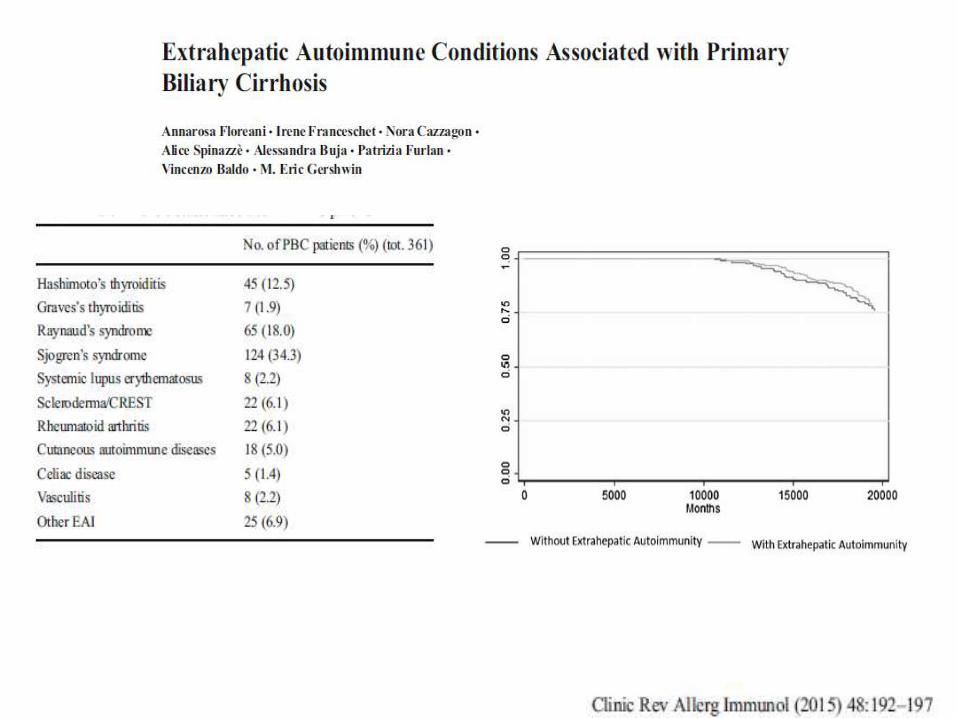
At presentation, 221 patients (61.2%) had at
least one EHA condition
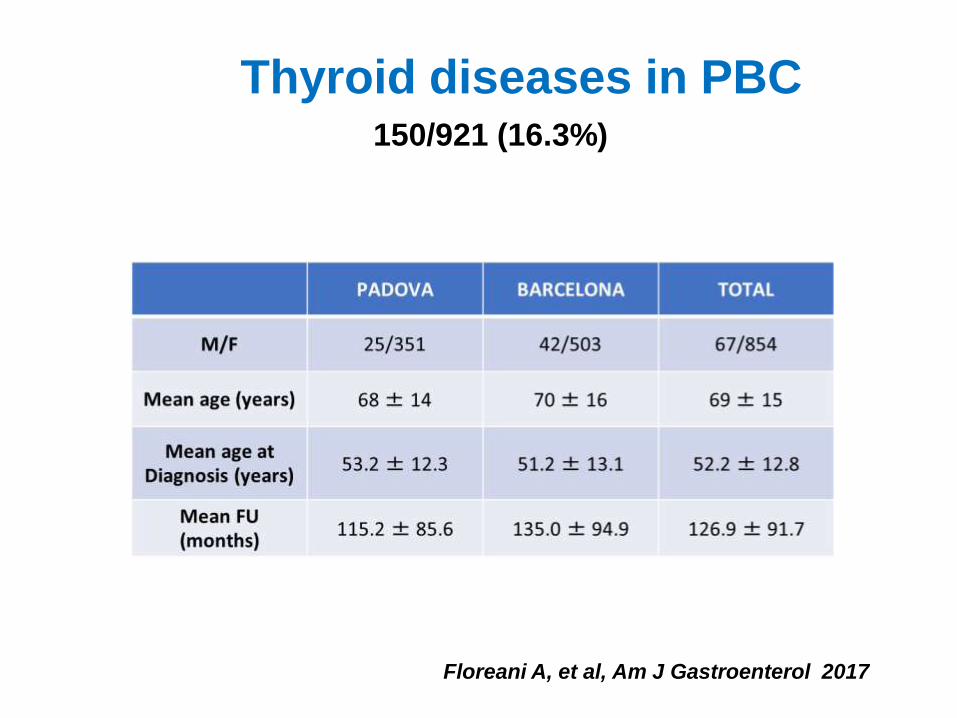
Thyroid diseases in PBC
Floreani A, et al, Am J Gastroenterol 2017
150/921 (16.3%)
5

Primary endpoint: achieving alkaline phosphate (ALP) <1.67x ULN and a ≥15% reduction in ALP and a total bilirubin ≤ULN
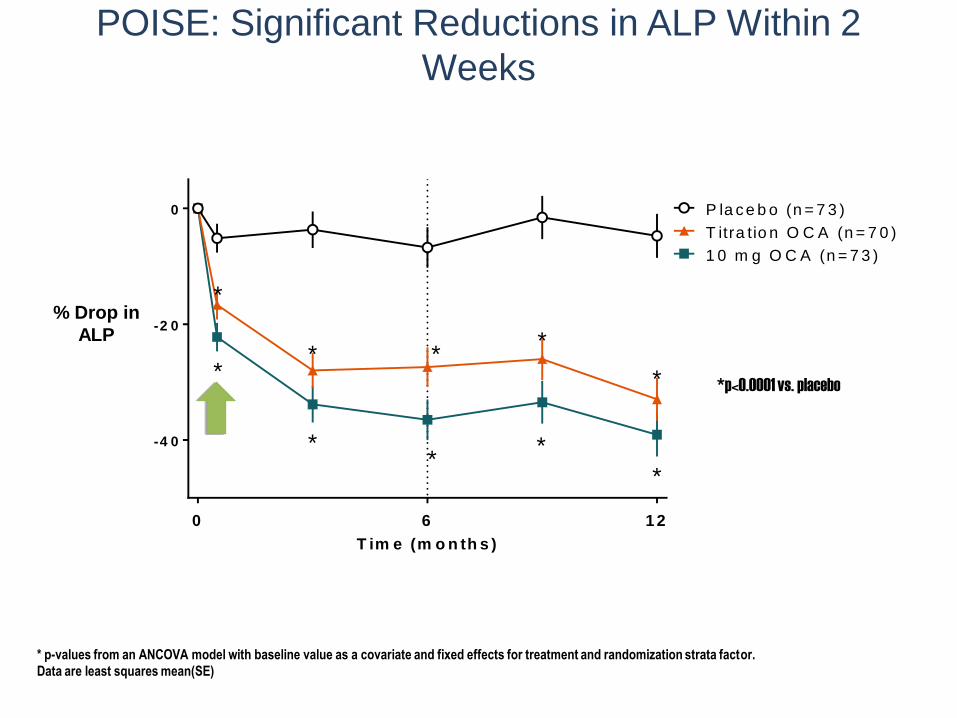
POISE: Significant Reductions in ALP Within 2
Weeks
* p-values from an ANCOVA model with baseline value as a covariate and fixed effects for treatment and randomization strata factor.
Data are least squares mean(SE)
*p<0.0001 vs. placebo
T im e (m o n th s )
% A L P
-4 0
-2 0
0 P la c e b o (n = 7 3 )
T itra tio n O C A (n = 7 0 )
1 0 m g O C A (n = 7 3 )
0 6 1 2
*
*
*
* *
*
*
*
*
*
% Drop in
ALP
Re
sp
on
de
rs
(%
)
0 .5 3 6 9 1 2 O L E
3
O L E
6
O L E
9
O L E
1 2
O L E
1 5
O L E
1 8
0
2 0
4 0
6 0
8 0
P la c e b o U D C A , n
O C A 5 -1 0 m g U D C A , n
O C A 1 0 m g U D C A , n
M o n th s
D o u b le -B lin d P h a s e
R a n d o m iz e d T r e a tm e n t
O p e n -L a b e l E x te n s io n
A ll R e c e iv e O C A
5 m g T it r a t io n
***
***
***
***
***
***
***
***
*** ***
D B T r e a tm e n t G r o u p
7 3 7 37 3 7 3 7 3
5 9 5 96 4 6 0 5 5 5 5
7 0 6 27 07 0 6 07 0 6 37 0 6 2 5 7 5 7
7 3 6 17 37 3 5 97 3 6 47 3 5 9 5 8 5 9
P la c e b o p a t ie n t s s t a r t e d O C A d u r in g t h e o p e n - la b e l e x t e n s io n , n
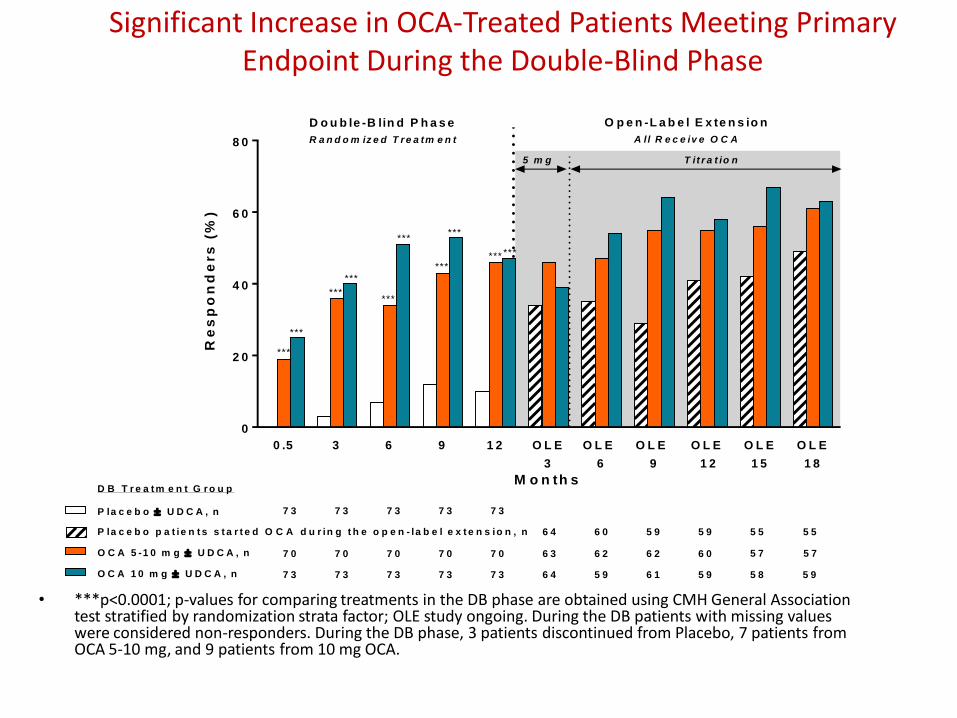
Significant Increase in OCA-Treated Patients Meeting Primary Endpoint During the Double-Blind Phase
• ***p<0.0001; p-values for comparing treatments in the DB phase are obtained using CMH General Association test stratified by randomization strata factor; OLE study ongoing. During the DB patients with missing values were considered non-responders. During the DB phase, 3 patients discontinued from Placebo, 7 patients from OCA 5-10 mg, and 9 patients from 10 mg OCA.
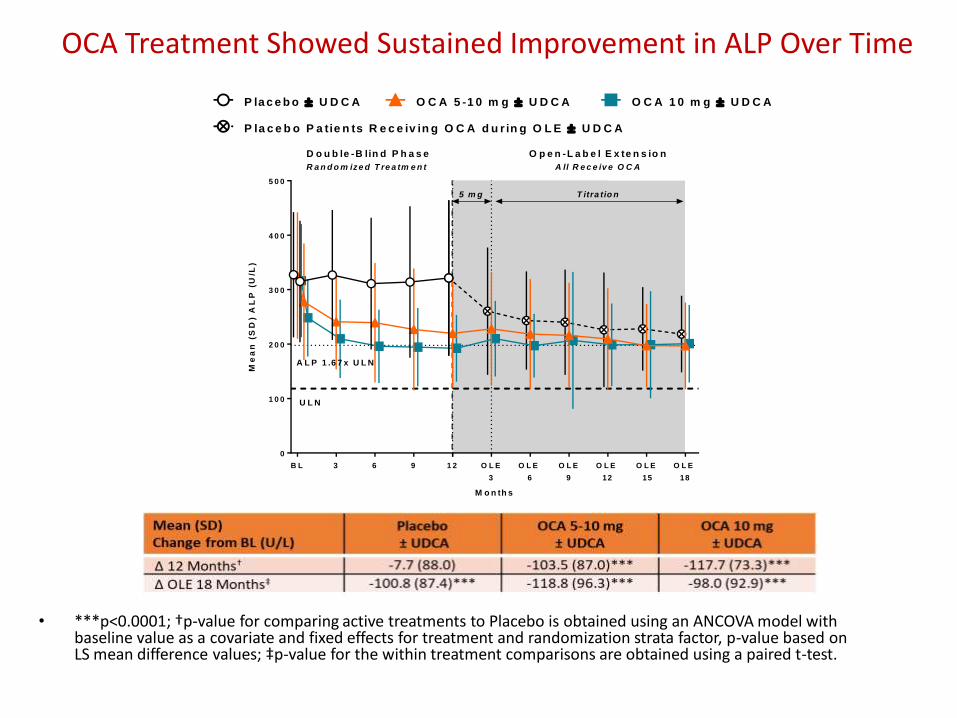
OCA Treatment Showed Sustained Improvement in ALP Over Time
• ***p<0.0001; †p-value for comparing active treatments to Placebo is obtained using an ANCOVA model with baseline value as a covariate and fixed effects for treatment and randomization strata factor, p-value based on LS mean difference values; ‡p-value for the within treatment comparisons are obtained using a paired t-test.
3 6 9 1 2
0
1 0 0
2 0 0
3 0 0
4 0 0
5 0 0
M o n th s
Me
an
(S
D)
AL
P (
U/L
)
B L
A L P 1 .6 7 x U L N
O L E
3
O L E
6
O L E
12
U L N
5 m g T itra tio n
D o u b le -B lin d P h a s e
R a n d o m iz e d T re a tm e n t
O p e n -L a b e l E x te n s io n
A ll R e c e iv e O C A
O L E
9
O L E
15
O L E
18
O C A 5 -1 0 m g U D C AP la c e b o U D C A O C A 1 0 m g U D C A
P la c e b o P a tie n ts R e c e iv in g O C A d u r in g O L E U D C A
3 6 9 1 2
4
6
8
1 0
1 2
1 4
1 6
2 0
2 4
2 8
M o n th s
Me
an
(S
D)
To
tal
Bil
iru
bin
(u
mo
l/L
)
B L O L E
3
O L E
6
O L E
9
O L E
12
D o u b le -B lin d P h a s e
R a n d o m iz e d T re a tm e n t
O p e n -L a b e l E x te n s io n
A ll R e c e iv e O C A
U L N
5 m g T itra tio n
O L E
15
O L E
18
P la c e b o U D C A O C A 5 -1 0 m g U D C A O C A 1 0 m g U D C A
P la c e b o p a tie n ts re c e iv in g O C A d u r in g O L E U D C A
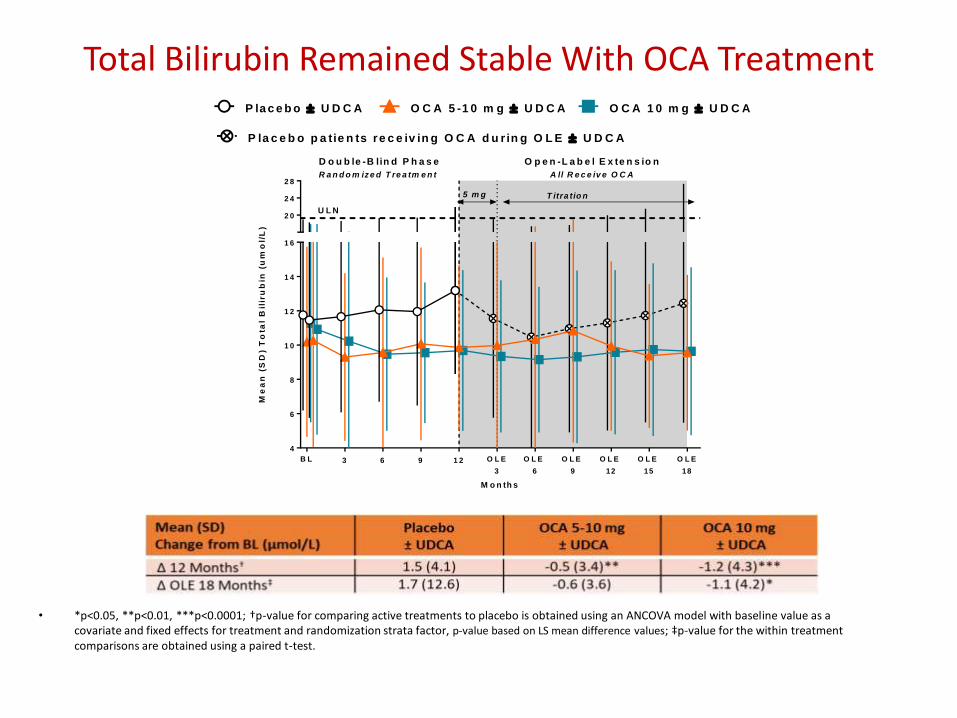
Total Bilirubin Remained Stable With OCA Treatment
• *p<0.05, **p<0.01, ***p<0.0001; †p-value for comparing active treatments to placebo is obtained using an ANCOVA model with baseline value as a covariate and fixed effects for treatment and randomization strata factor, p-value based on LS mean difference values; ‡p-value for the within treatment comparisons are obtained using a paired t-test.

Sustained Reduction In Markers of Hepatic Damage: AST and ALT
• Reductions in AST and ALT are statistically significant (p<0.05) for all OCA -treated groups in the DB phase† and all groups in the OLE phase‡
• †p-value for comparing active treatments to placebo is obtained using an ANCOVA model with Baseline value as a covariate and fixed effects for treatment and randomization strata factor, p-value based on LS mean difference values; ‡p-value for the within treatment comparisons are obtained using a paired t-test.
3 6 9 1 2
0
2 0
4 0
6 0
8 0
1 0 0
M o n th s
Me
an
(S
D)
AS
T (
U/L
)
B L O L E
3
O L E
6
O L E
9
O L E
12
5 m g T itra tio n
D o u b le -B lin d P h a s e
R a n d o m iz e d T re a tm e n t
O p e n -L a b e l E x te n s io n
A ll R e c e iv e O C A
O L E
15
O L E
18
O C A 5 -1 0 m g U D C AP la c e b o U D C A O C A 1 0 m g U D C A
P la c e b o p a tie n ts re c e iv in g O C A d u r in g O L E U D C A
3 6 9 1 2
0
2 0
4 0
6 0
8 0
1 0 0
M o n th s
Me
an
(S
D)
AL
T (
U/L
)B L O L E
3
O L E
6
O L E
9
O L E
12
5 m g T itra tio n
D o u b le -B lin d P h a s e
R a n d o m iz e d T re a tm e n t
O p e n -L a b e l E x te n s io n
A ll R e c e iv e O C A
O L E
15
O L E
18
AST (U/L) ALT (U/L)
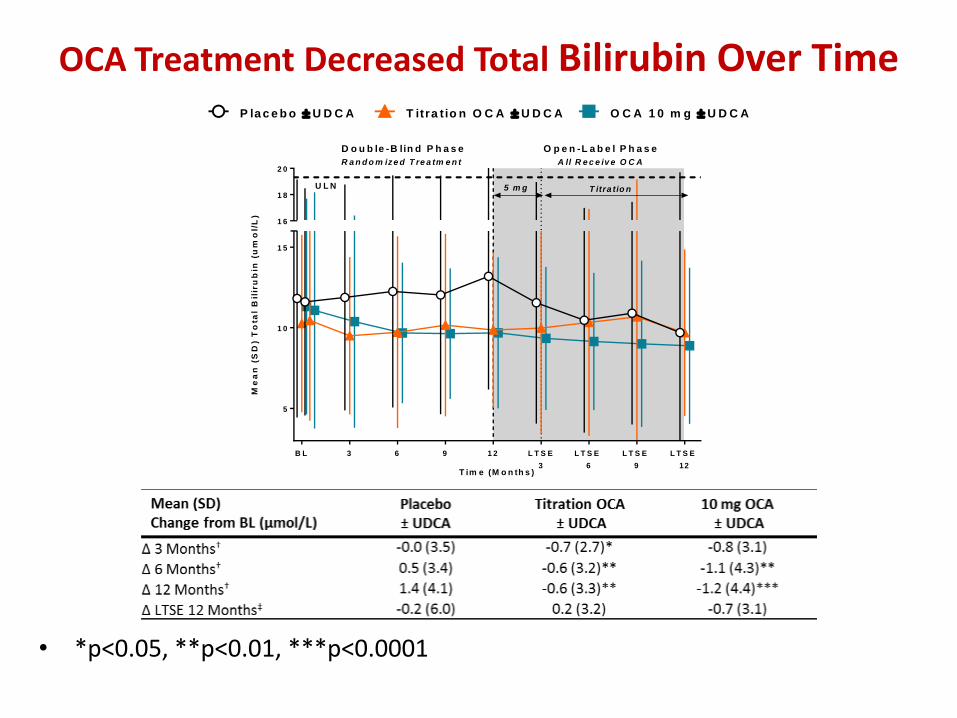
OCA Treatment Decreased Total Bilirubin Over Time
• *p<0.05, **p<0.01, ***p<0.0001
3 6 9 1 2
5
1 0
1 5
1 6
1 8
2 0
T im e (M o n th s )
Me
an
(S
D)
To
tal
Bil
iru
bin
(u
mo
l/L
)
B L L T S E
3
L T S E
6
L T S E
9
L T S E
12
D o u b le -B lin d P h a s e
R a n d o m iz e d T re a tm e n t
O p e n -L a b e l P h a s e
A ll R e c e iv e O C A
U L N 5 m g T itra tio n
P la c e b o U D C A T itra t io n O C A U D C A O C A 1 0 m g U D C A
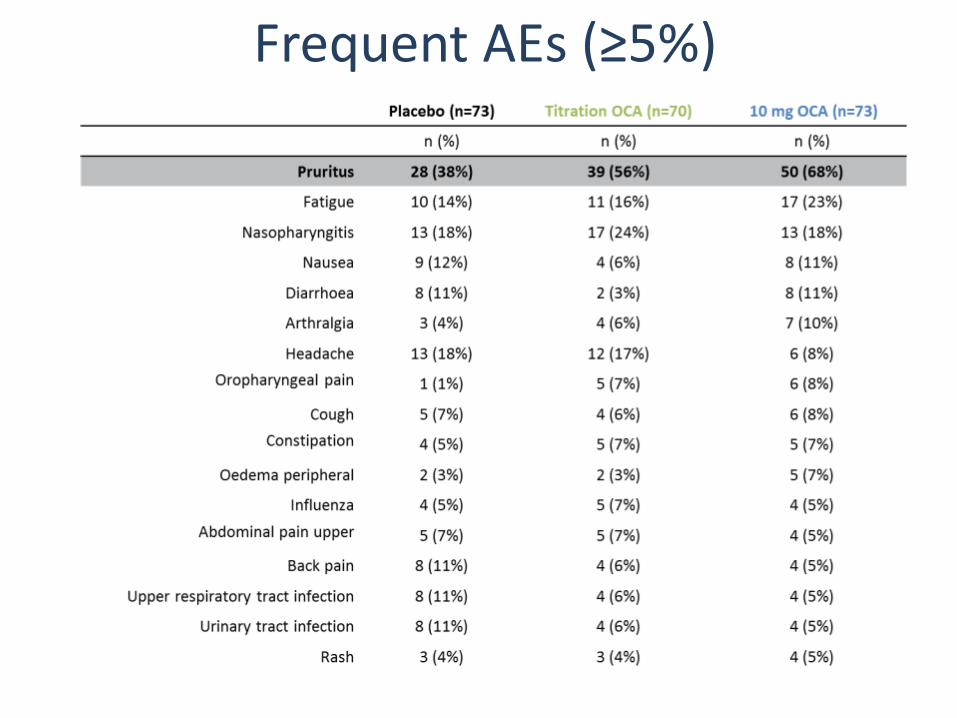
Frequent AEs (≥5%)
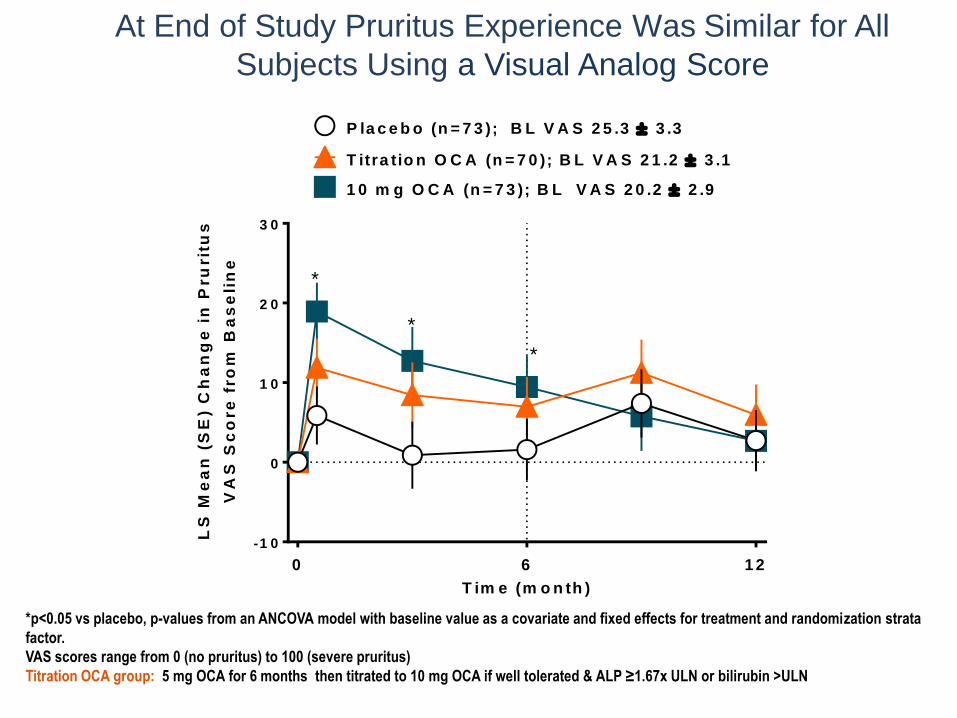
At End of Study Pruritus Experience Was Similar for All
Subjects Using a Visual Analog Score
T im e (m o n th )
LS
Me
an
(S
E)
Ch
an
ge
in
Pru
rit
us
VA
S S
co
re
fro
m B
as
eli
ne
-1 0
0
1 0
2 0
3 0
P la c e b o (n = 7 3 ); B L V A S 2 5 .3 3 .3
0 6 1 2
T itra tio n O C A (n = 7 0 ); B L V A S 2 1 .2 3 .1
1 0 m g O C A (n = 7 3 ); B L V A S 2 0 .2 2 .9
*
*
*
*p<0.05 vs placebo, p-values from an ANCOVA model with baseline value as a covariate and fixed effects for treatment and randomization strata
factor.
VAS scores range from 0 (no pruritus) to 100 (severe pruritus)
Titration OCA group: 5 mg OCA for 6 months then titrated to 10 mg OCA if well tolerated & ALP ≥1.67x ULN or bilirubin >ULN
La Determina dell’AIFA n. 1392/2017 è stata pubblicata in Gazzetta Ufficiale (GU Serie Generale n.196 del 23-08-2017)
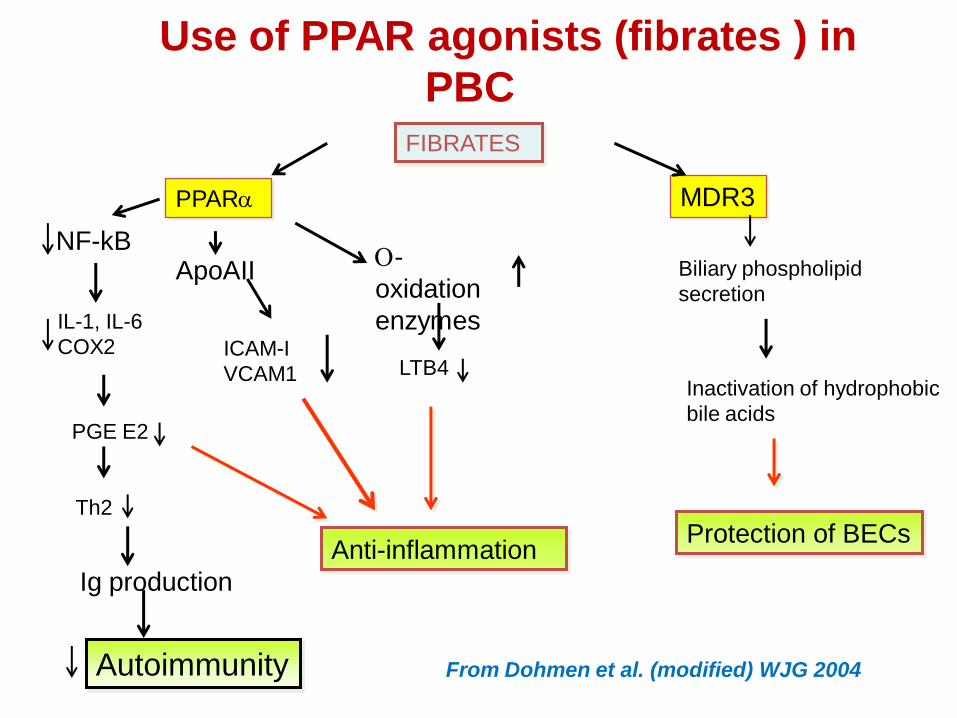
FIBRATES
MDR3PPARa
O-
oxidation
enzymes
LTB4
ApoAII
ICAM-I
VCAM1
Anti-inflammation
Biliary phospholipid
secretion
Inactivation of hydrophobic
bile acids
Protection of BECs
NF-kB
IL-1, IL-6
COX2
PGE E2
Th2
Ig production
Autoimmunity From Dohmen et al. (modified) WJG 2004
Use of PPAR agonists (fibrates ) in
PBC PBC
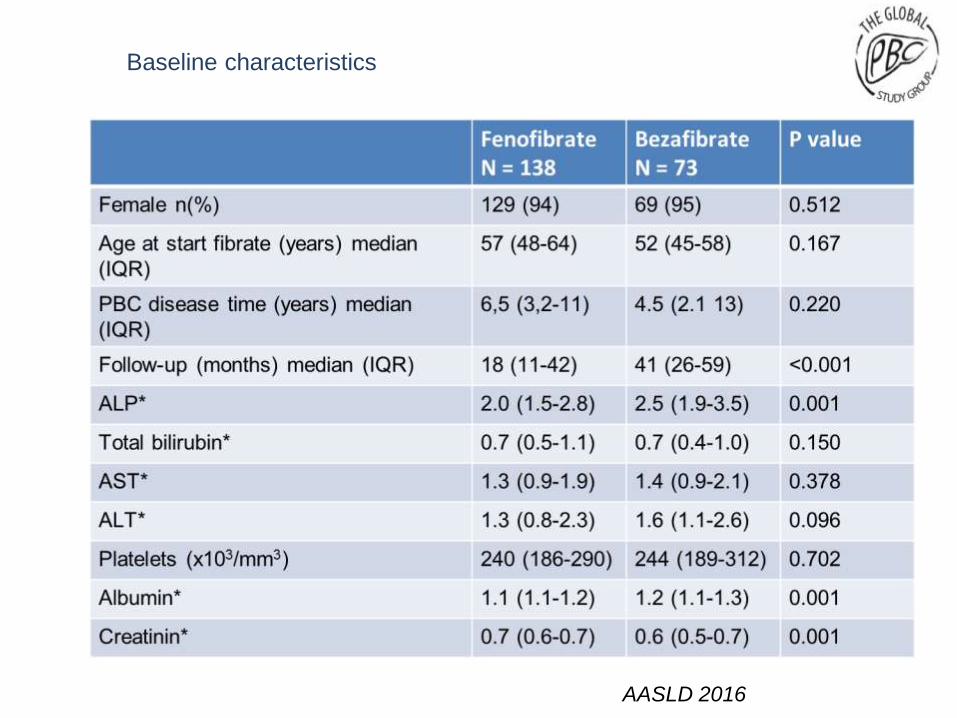
Baseline characteristics
AASLD 2016
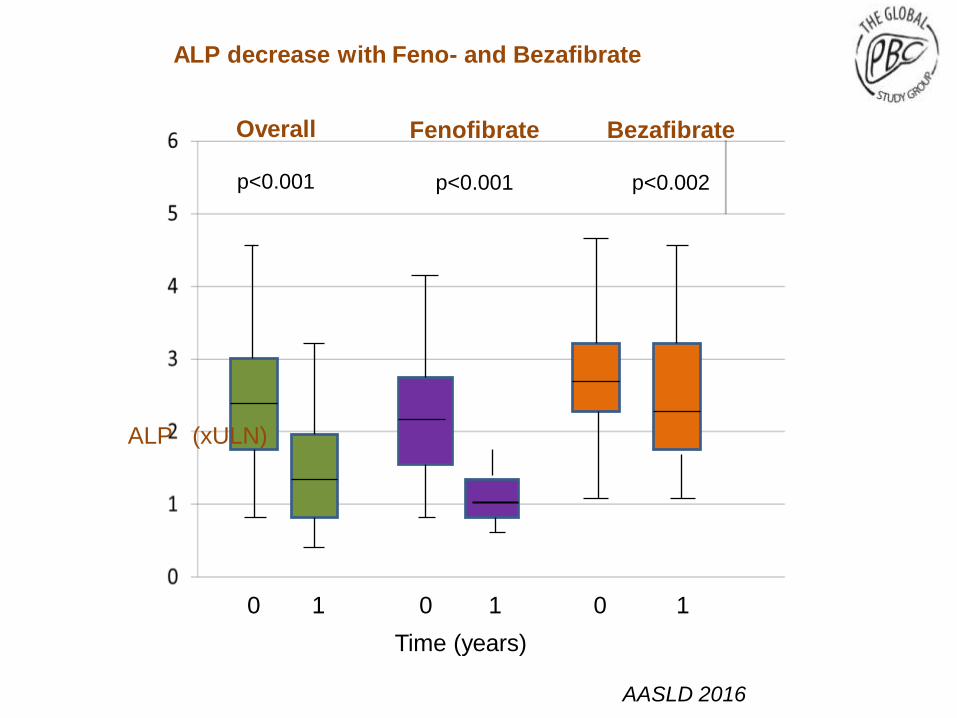
0 1 0 1 0 1
Overall
p<0.001
Fenofibrate
p<0.001
Bezafibrate
p<0.002
ALP decrease with Feno- and Bezafibrate
Time (years)
AASLD 2016
ALP (xULN)
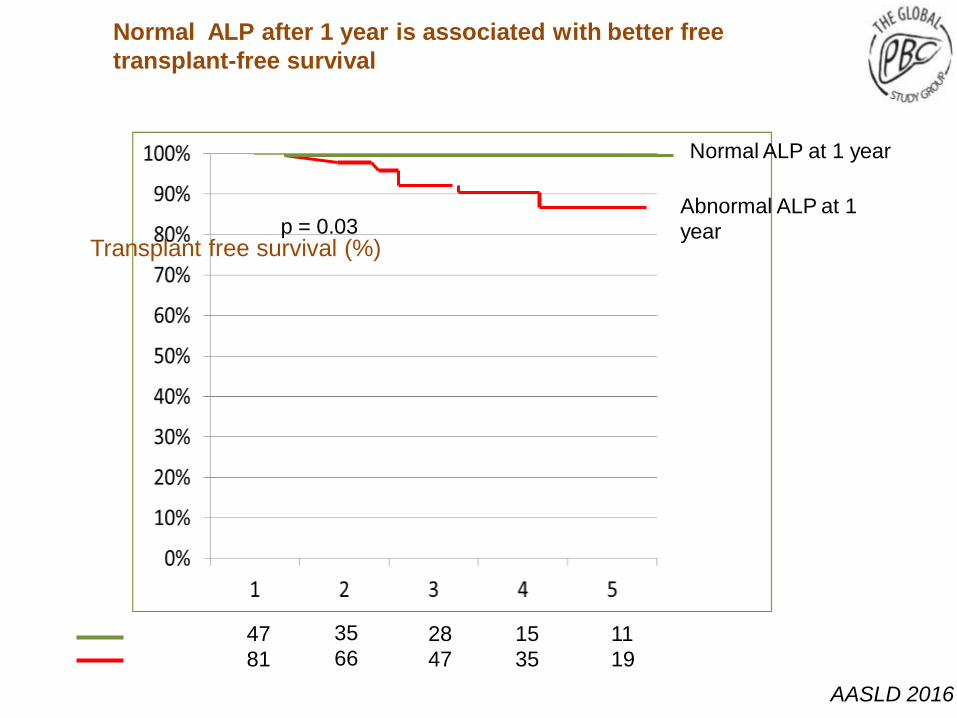
Normal ALP after 1 year is associated with better free
transplant-free survival
Normal ALP at 1 year
Abnormal ALP at 1
year
47
81
35
6628
47
15
35
11
19
p = 0.03Transplant free survival (%)
AASLD 2016
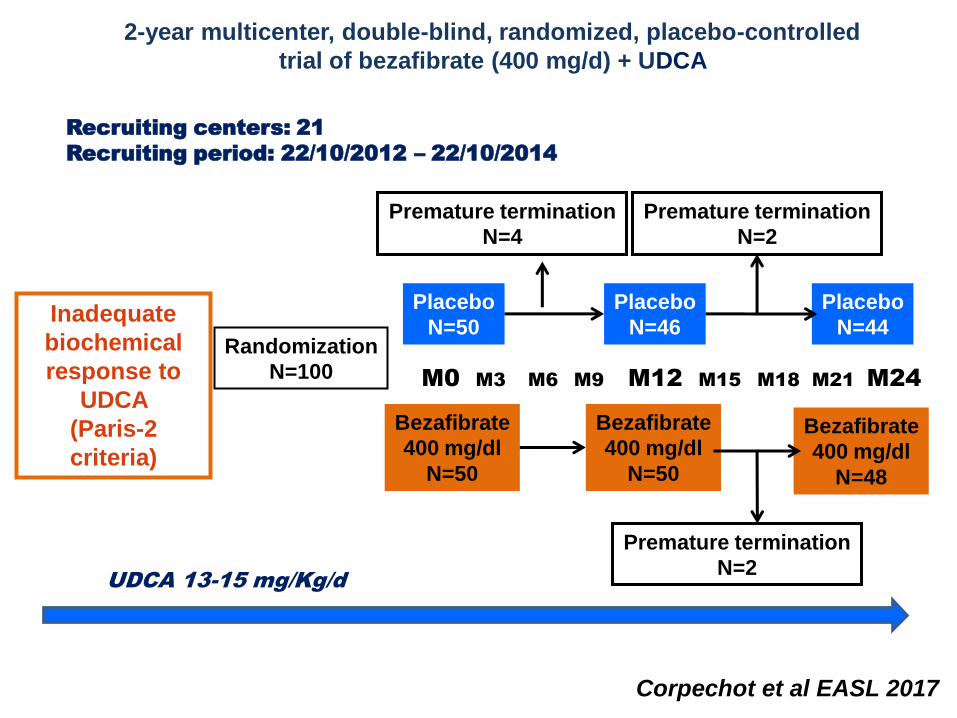
2-year multicenter, double-blind, randomized, placebo-controlled
trial of bezafibrate (400 mg/d) + UDCA
Corpechot et al EASL 2017
Inadequate
biochemical
response to
UDCA
(Paris-2
criteria)
Randomization
N=100
Premature termination
N=4
Bezafibrate
400 mg/dl
N=50
Placebo
N=46
Placebo
N=44
Bezafibrate
400 mg/dl
N=50
Bezafibrate
400 mg/dl
N=48
Placebo
N=50
Premature termination
N=2
Premature termination
N=2
Recruiting centers: 21
Recruiting period: 22/10/2012 – 22/10/2014
UDCA 13-15 mg/Kg/d
M0 M3 M6 M9 M12 M15 M18 M21 M24
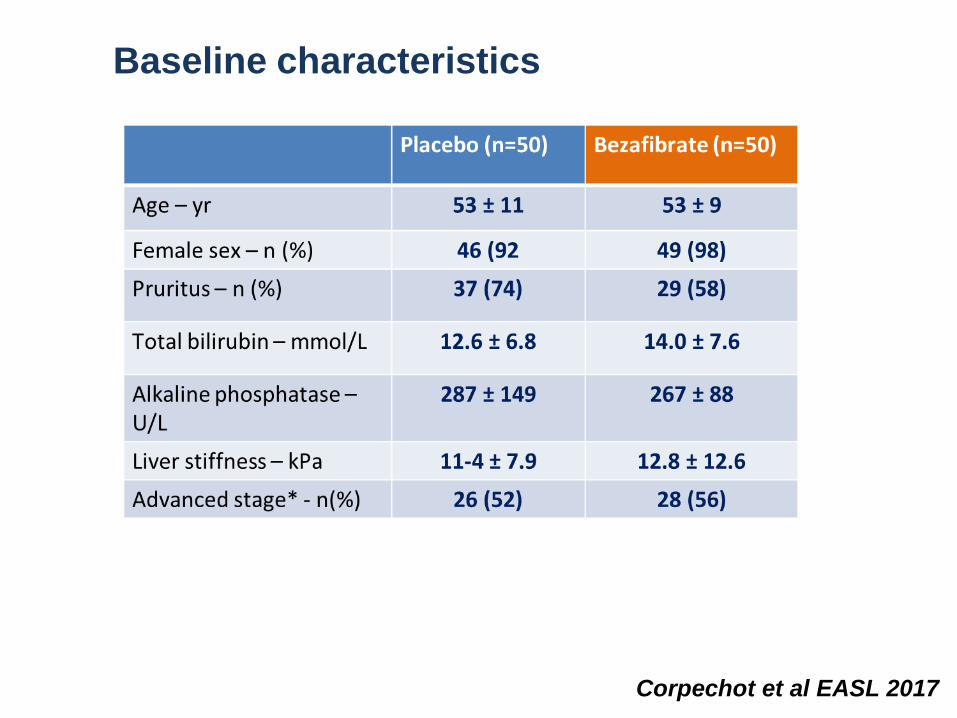
Baseline characteristics
Corpechot et al EASL 2017
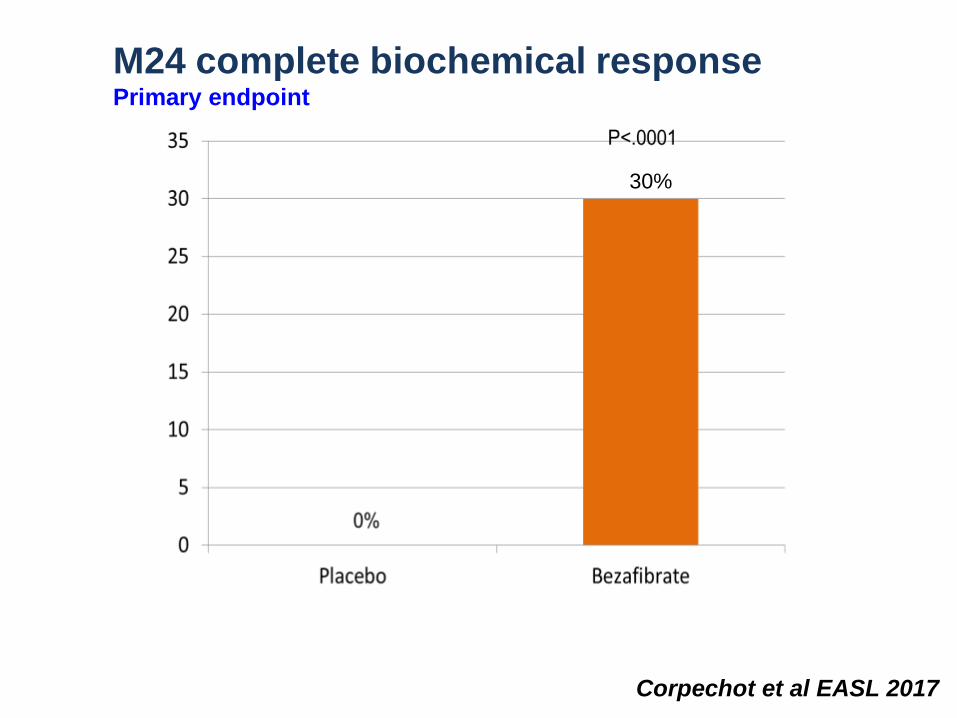
M24 complete biochemical responsePrimary endpoint
Corpechot et al EASL 2017
30%
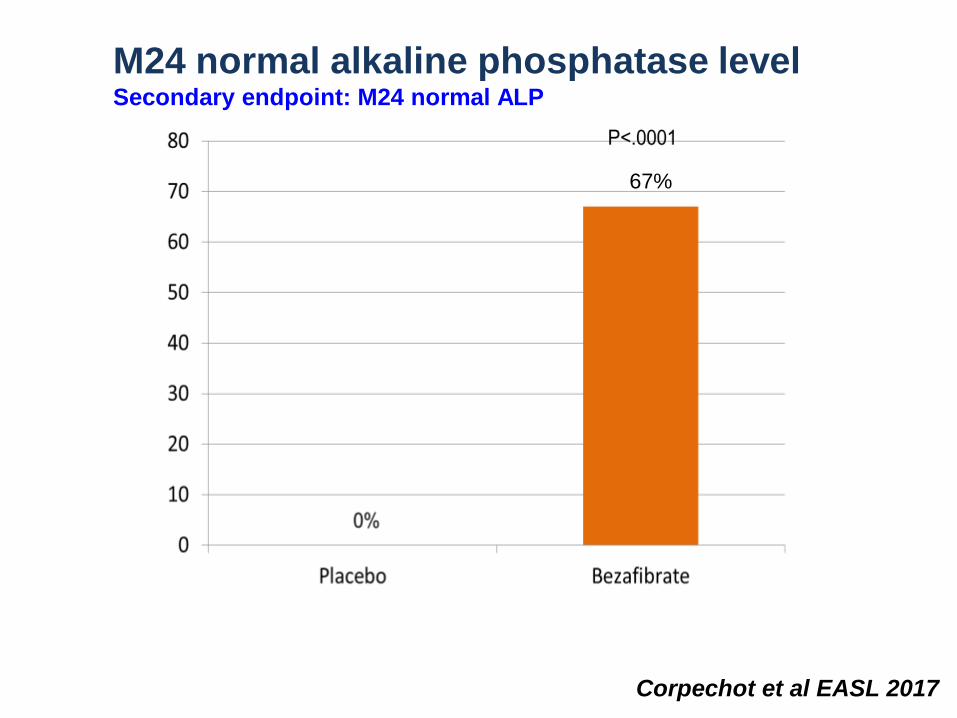
M24 normal alkaline phosphatase levelSecondary endpoint: M24 normal ALP
Corpechot et al EASL 2017
67%
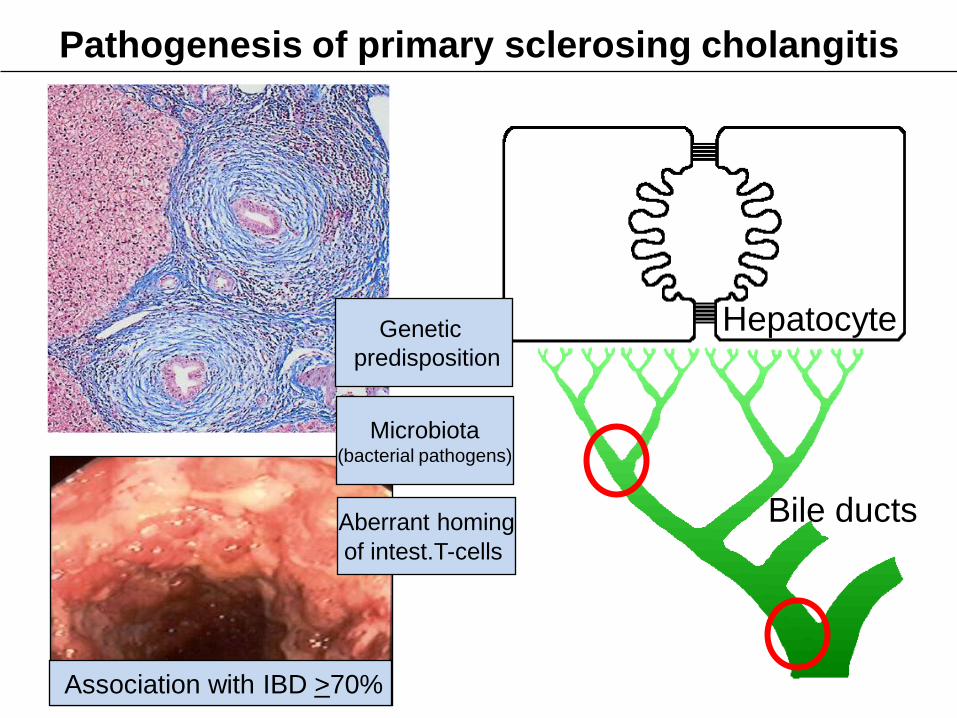
Genetic
predisposition
Association with IBD >70%
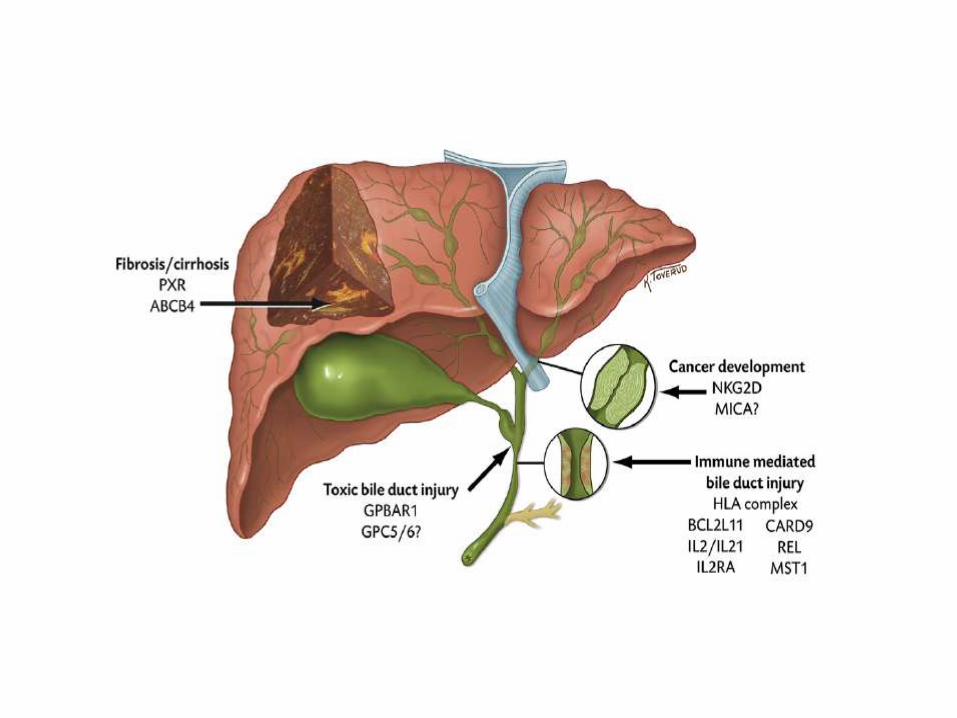
Pathogenesis of primary sclerosing cholangitis
Hepatocyte
Bile ducts
Microbiota(bacterial pathogens)
Aberrant homing
of intest.T-cells

PSC and Genetic Associations
• Integration of Genetics and Environment?
Karlsen et al. J Hepatol 2015;62:S6–S14.
Environmental risk factors
• Not well understood!
• Smoking is protects against ulcerative colitis, and
this is also seen in patients who have both PSC
and colitis
• Two independent studies have suggested a
negative association between coffee
consumption and PSC.
Lammert et al Clin Gastroenterol Hepatol 2014; 12:1562-8
Andersen IM et al Clin Gastroenterol Hepatol 2014; 12: 1019-28.
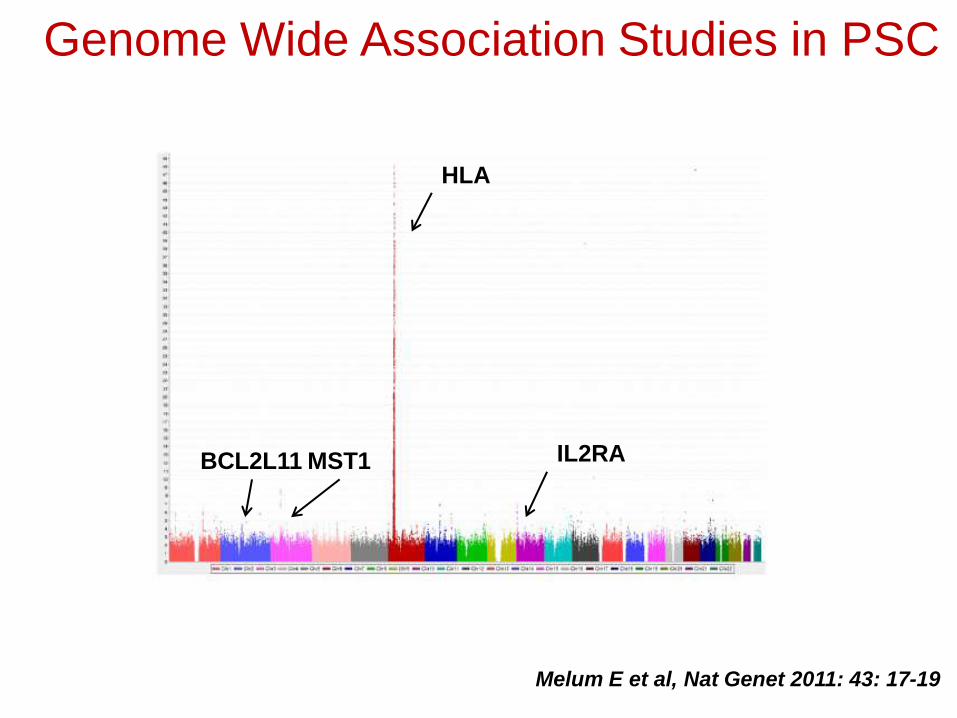
Genome Wide Association Studies in PSC
HLA
IL2RABCL2L11 MST1
Melum E et al, Nat Genet 2011: 43: 17-19
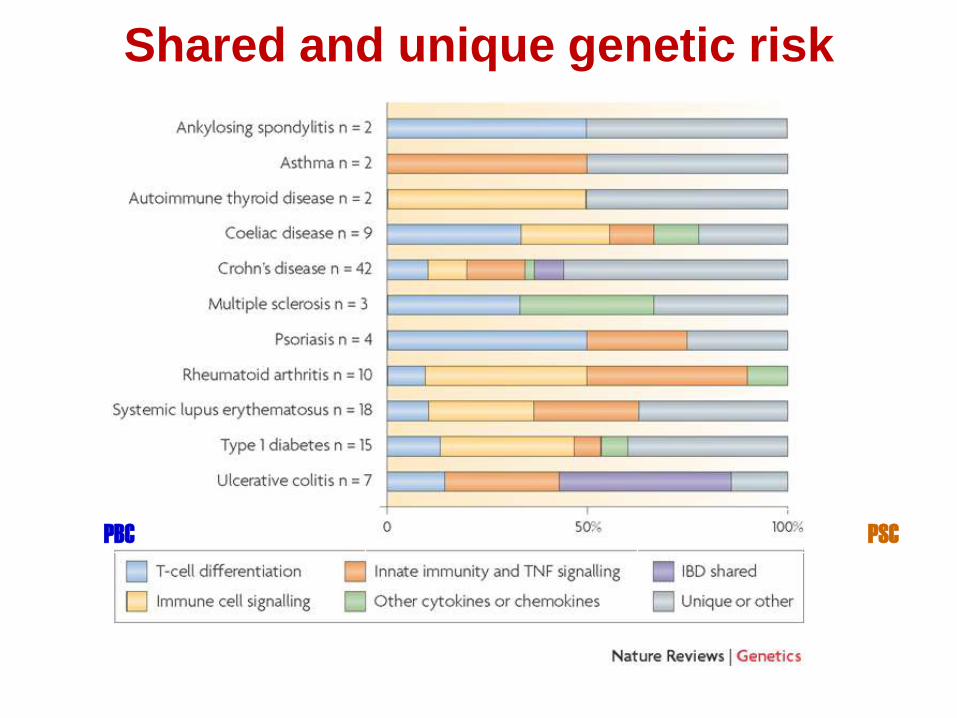
Shared and unique genetic risk
PBC PSC

Genetics of PSC
Henriksen et al, 2014
Liver-Gut Axis
• The liver continuously receives blood coming from
the intestines
• Carries bacterial products, toxins, nutrition
• Abnormalities in the intestine might trigger
inflammation in the liver
– Abnormal composition of the microbiome
(organisms living in the intestines)
– Are these bacteria causing PSC or responding
to the different cause?
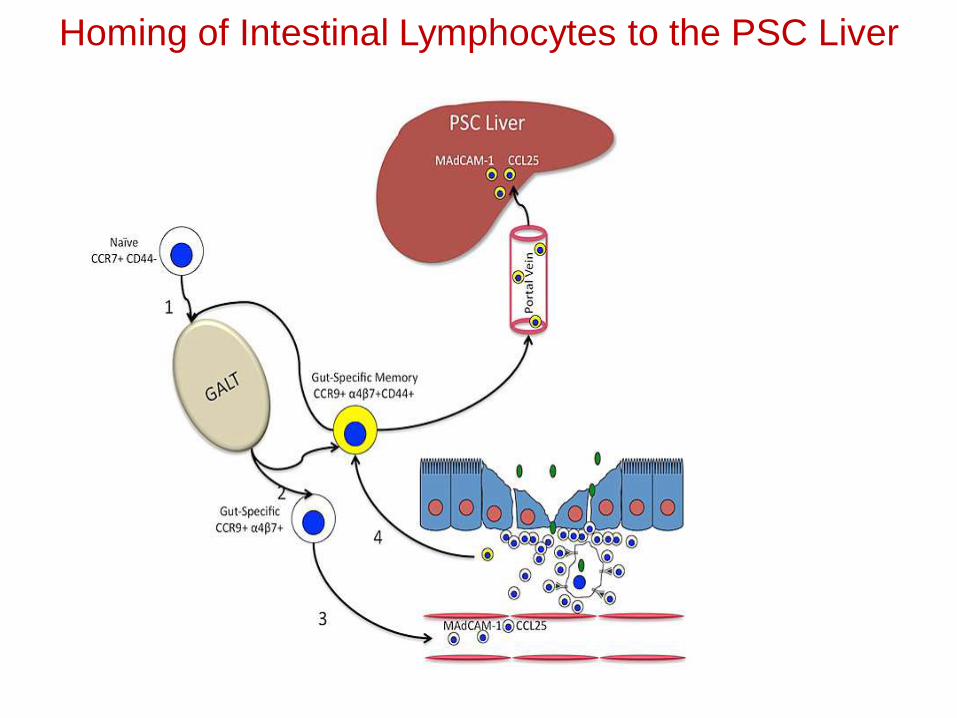
Homing of Intestinal Lymphocytes to the PSC Liver
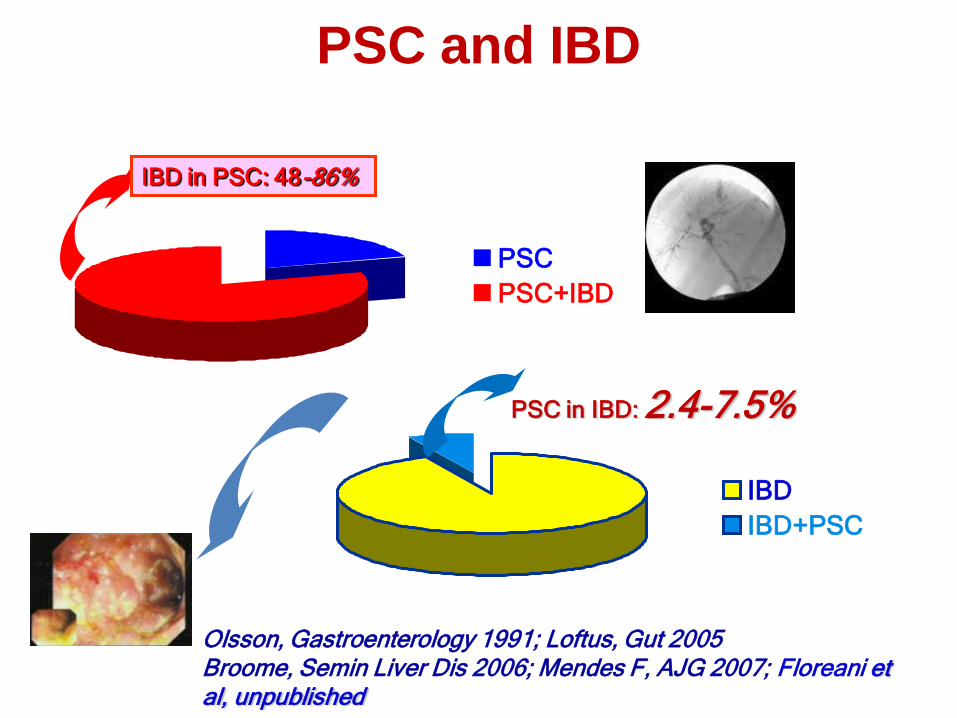
Olsson, Gastroenterology 1991; Loftus, Gut 2005Broome, Semin Liver Dis 2006; Mendes F, AJG 2007; Floreani et al, unpublished
PSC
PSC+IBD
IBD in PSC: 48-86%
IBD
IBD+PSC
PSC in IBD: 2.4-7.5%
PSC and IBD

International PSC Study Group
PATIENT AGE, SEX, AND INFLAMMATORY BOWEL DISEASE
PHENOTYPE ASSOCIATE WITH COURSE OF PRIMARY
SCLEROSING CHOLANGITIS
T.J. Weismüller1,2, J.A. Talwalkar3, C.Y. Ponsioen4, D.N. Gotthardt5, H.-U. Marschall6, S. Naess7, K. Holm7, R.K. Weersma8, K.N. Lazaridis3, J.
Fevery9, P.J. Trivedi10, C. Schramm11, O. Chazouilleres12, T. Müller13, M. Farkkila14, S. Almer15,16, S. Pereira17, A.L. Mason18, A. Floreani19, P.
Milkiewicz20, C. Levy32, H. Harley21, A. Pares22, L. de Vries4, C.N. Manser23, D. Huynh21, E. Rauws4, G. Dalekos24, N. Gatselis24, C. Berg25, H. Lenzen2,
M. Benito de Valle6, M. Imam3, G. Kirchner26, P. de Leuw27, V. Zimmer28, L. Fabris19, F. Braun29, P.L. Jansen4, G.M. Hirschfield10, M. Marzioni30, P.
Invernizzi31, B.D. Juran3, C.P. Strassburg1,2, U. Beuers4, M.P. Manns2, E. Schrumpf7, T.H. Karlsen7, A. Bergquist16, K.M. Boberg7
International PSC Study Group
1Department of Internal Medicine 1, University of Bonn, Bonn, Germany 2Department of Gastroenterology, Hepatology and Endocrinology, Hannover
Medical School, Hannover, Germany, 3Division of Gastroenterology and Hepatology, Mayo Clinic, Rochester, MN, United States, 4Department of
Gastroenterology and Hepatology, Academic Medical Center, Amsterdam, Netherlands, 5Department of Internal Medicine, University Hospital of
Heidelberg, Heidelberg, Germany, 6Department of Molecular and Clinical Medicine, Sahlgrenska Academy,University of Gothenburg, Gothenburg,
Sweden, 7Norwegian PSC Research Center, Oslo University Hospital Rikshospitalet, Oslo, Norway, 8Department of Gastroenterology and Hepatology,
University Medical Center Groningen and University of Groningen, Groningen, Netherlands, 9Department of Hepatology, University Hospital
Gasthuisberg, Leuven, Belgium, 10NIHR Biomedical Research Unit and Centre for Liver Research, University of Birmingham, Birmingham, United
Kingdom, 111st Department of Medicine, University Medical Center Hamburg-Eppendorf, Hamburg, Germany, 12Service d'Hépatologie, Hôpital Saint
Antoine, Assistance Publique-Hôpitaux de Paris,Faculté de Médecine Pierre et Marie Curie, Paris, France, 13Department of Internal Medicine,
Hepatology and Gastroenterology, Charité Universitätsmedizin Berlin, Berlin, Germany, 14Division of Gastroenterology, Department of Medicine,
Helsinki University Central Hospital, Helsinki, Finland, 15Gastroenterology & Hepatology, Linköping University, Linköping, 16Division of
Gastroenterology and Hepatology, Karolinska University Hospital Huddinge, Karolinska Institutet, Stockholm, Sweden, 17UCL Institute for Liver and
Digestive Health, London, United Kingdom, 18Division of Gastroenterology and Hepatology, University of Alberta, Edmonton, AB, Canada,
19Department of Surgical, Oncological and Gastroenterological Sciences, University of Padova, Padova, Italy, 20Liver Unit and Liver Research
Laboratories, Pomeranian Medical University, Szczecin, Poland, 21Department of Gastroenterology and Hepatology, Royal Adelaide Hospital,
Adelaide, SA, Australia, 22Liver Unit, Hospital Clínic, University of Barcelona, Barcelona, Spain, 23Division for Gastroenterology and Hepatology,
University Hospital Zurich (USZ), Zürich, Switzerland, 24Department of Medicine and Research Laboratory of Internal Medicine, University Hospital of
Larissa, University of Thessaly, Larissa, Greece, 25Department of Gastroenterology, Hepatology, and Infectiology, Medical Clinic, University of
Tübingen, Tübingen, 26Department of Internal Medicine I, University Hospital of Regensburg, Regensburg, 27Department of Internal Medicine 1,
Johann Wolfgang Goethe-University Hospital, Frankfurt, 28Saarland University Medical Center, Homburg, 29UKSH, Campus Kiel, Kiel, Germany,
30Department of Gastroenterology, Università Politecnica delle Marche, Ancona, Italy, 31 Center for Aotoimmune Liver Diseases, Humaitis Clinical and
Research Center, Rozzano (MI), Italy, 32Center for Liver Diseases University of Miami, Miami, Florida, United States
Gastroenterology, 2017
• International, Multicenter, Retrospective, Observational Study
• Inclusion criteria:
– all patients diagnosed between 1/1/1980 and 12/31/2010 with one of the following diagnoses:
• PSC
• small-duct-PSC
• PSC with features of AIH
• PSC with features of IgG4-assoc. cholangitis
• Exclusion criteria: secondary causes of sclerosing cholangitis
Study design
Gastroenterology, 2017
• 25 Parameters:
- demographic data: date of birth, gender, date of death/last follow-up, liver-tx
- PSC: date of main diagnosis, subtype of PSC, IgG4
- IBD: date of diagnosis, subtype of IBD (MC/CU/Ind. Col.), date of colectomy,
indication for colectomy
- malignancy: colorectal malignancy, hepatobiliary malignancy (CCA, GBC,
HCC, pancreatic carcinoma)
• Endpoints: overall-survival, transplant-free survival, malignancy-free survival
• Statistics: Mann-Whitney-U-Test, Kaplan-Meier, log-rank, Cox Regression
Study design
Gastroenterology, 2017
Gastroenterology, 2017
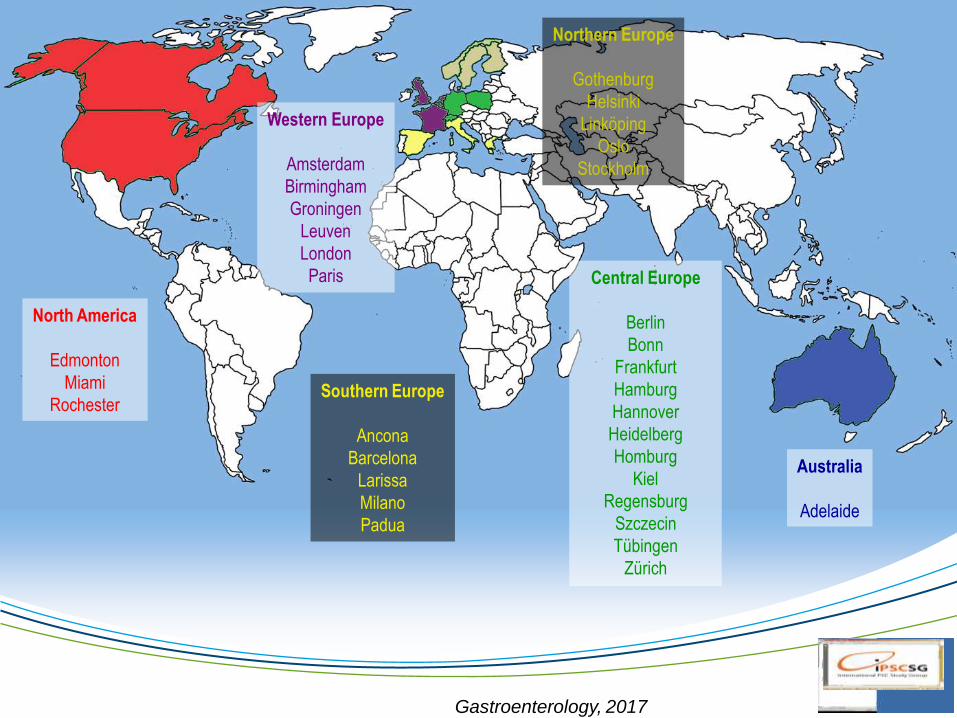
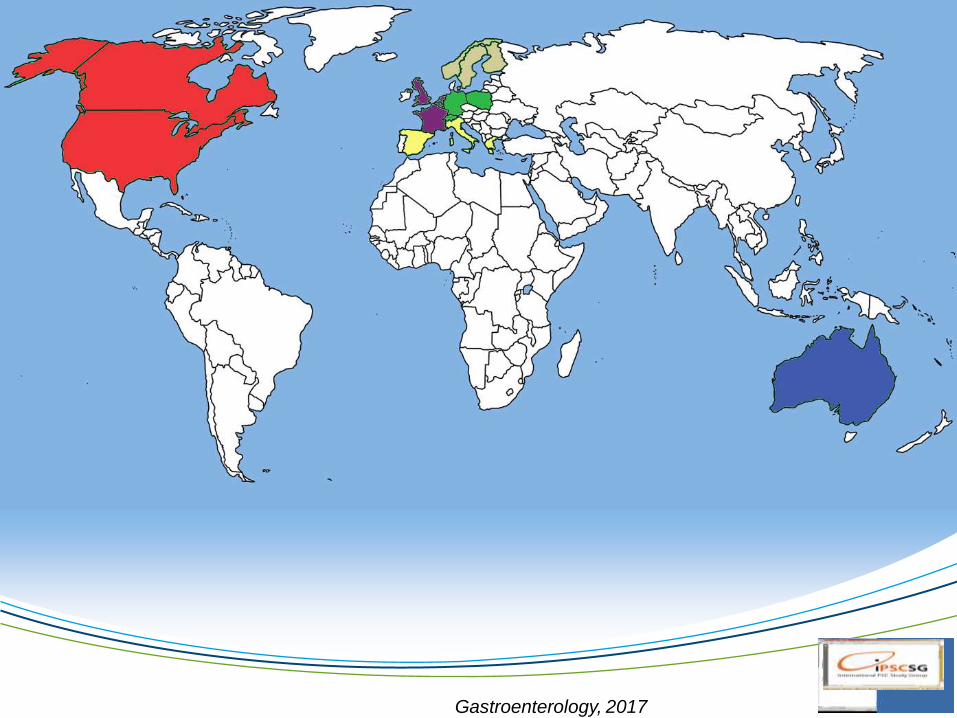
North America
Edmonton
Miami
Rochester
Western Europe
Amsterdam
Birmingham
Groningen
Leuven
London
Paris
Southern Europe
Ancona
Barcelona
Larissa
Milano
Padua
Australia
Adelaide
Northern Europe
Gothenburg
Helsinki
Linköping
Oslo
Stockholm
Central Europe
Berlin
Bonn
Frankfurt
Hamburg
Hannover
Heidelberg
Homburg
Kiel
Regensburg
Szczecin
Tübingen
Zürich
Gastroenterology, 2017
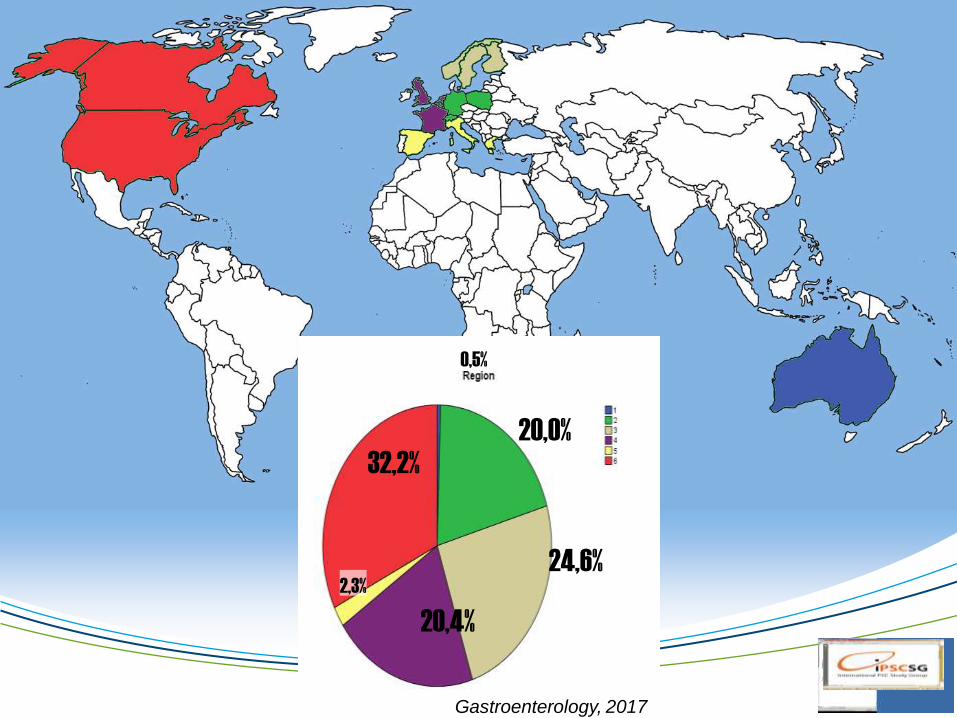
20,0%
24,6%
20,4%
2,3%
32,2%
0,5%
Gastroenterology, 2017
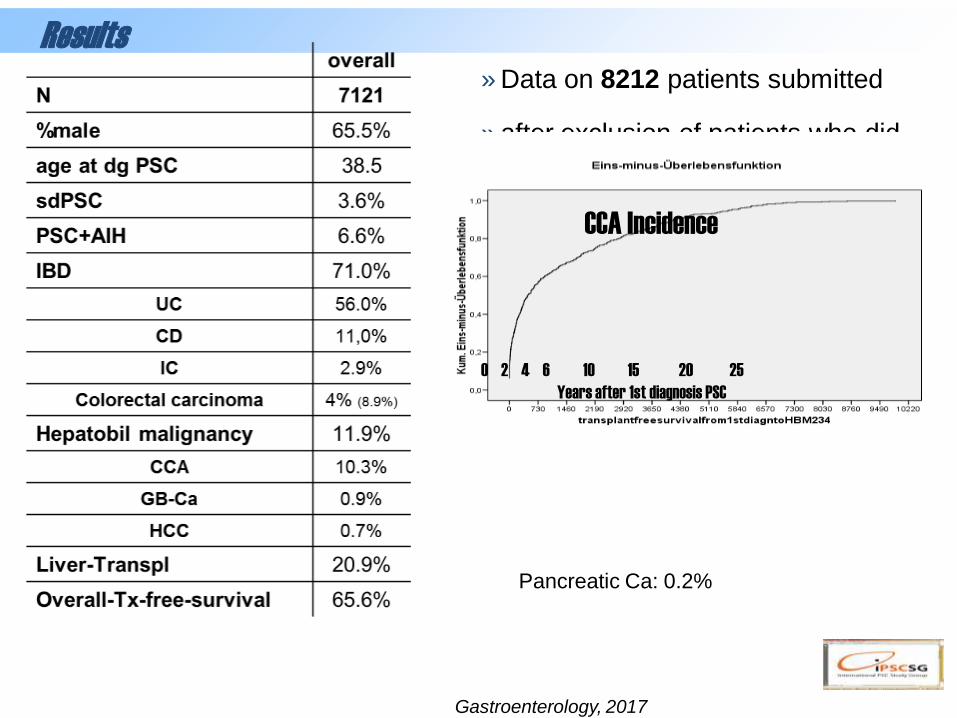
Results
» Data on 8212 patients submitted
» after exclusion of patients who did
not meet the inclusion criteria or
had insufficient follow-up
information 7121 patients remained
» Mean follow-up time: 21 years
Pancreatic Ca: 0.2%
0 2 4 6 10 15 20 25
Years after 1st diagnosis PSC
CCA Incidence
Gastroenterology, 2017

Results
Gastroenterology, 2017
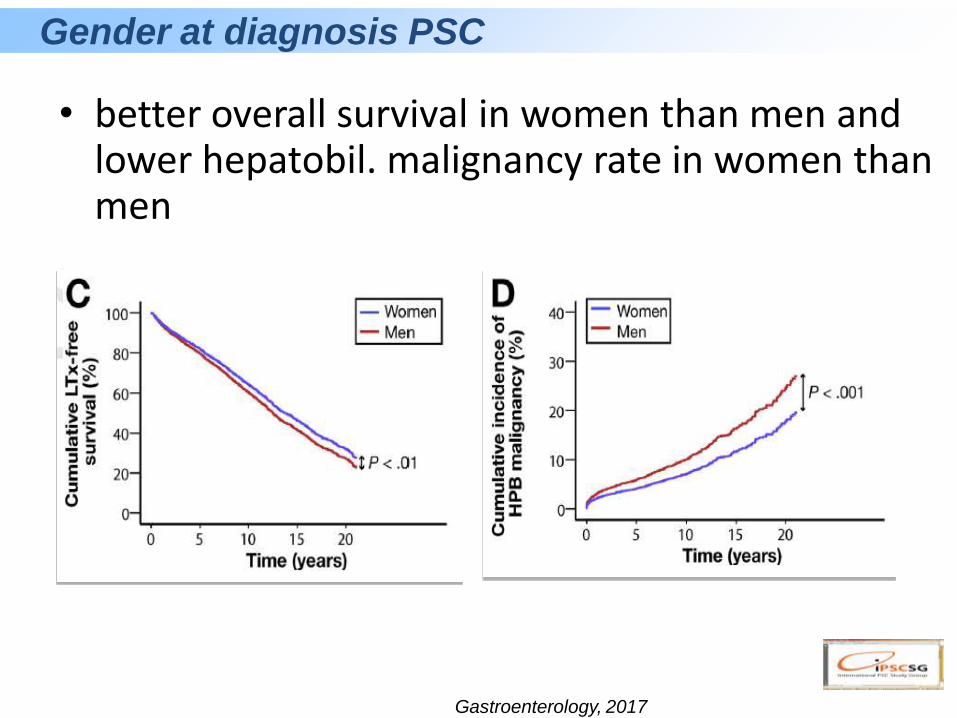
• better overall survival in women than men and lower hepatobil. malignancy rate in women than men
Gender at diagnosis PSC
Gastroenterology, 2017
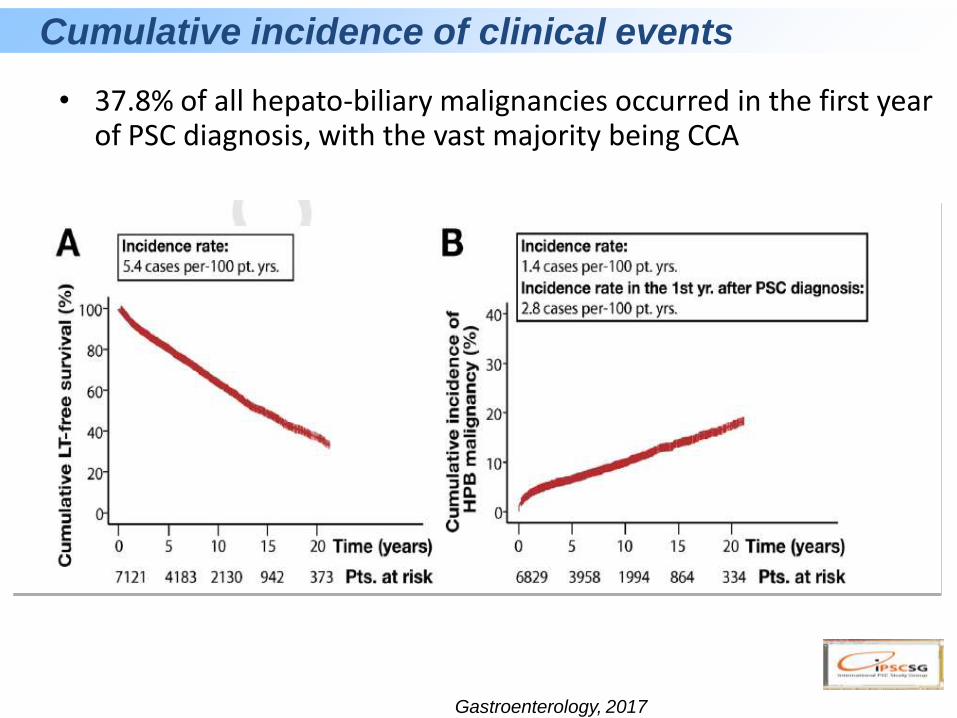
• 37.8% of all hepato-biliary malignancies occurred in the first year of PSC diagnosis, with the vast majority being CCA
Cumulative incidence of clinical events
Gastroenterology, 2017
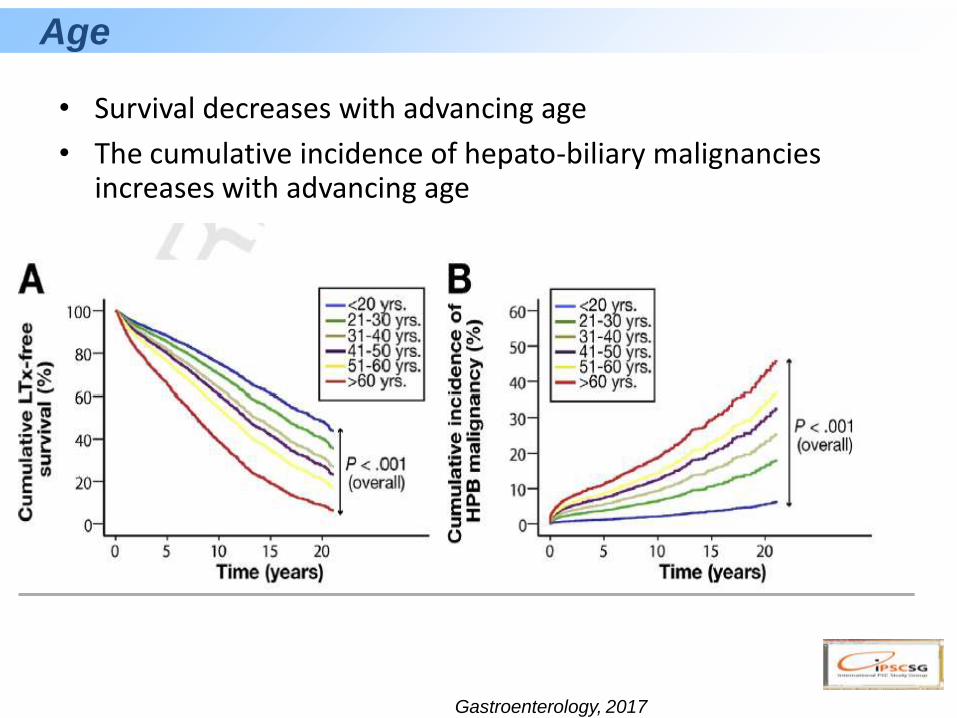
• Survival decreases with advancing age
• The cumulative incidence of hepato-biliary malignancies increases with advancing age
Age
Gastroenterology, 2017

• Better overall survival and lower hepatobil. malignancy rate in patients with small-duct PSC
• Mean age at dg PSC: sdPSC 39years, PSC 41years(p=0.064)
Small-duct disease, and AIH/PSC vs. classical PSC
Gastroenterology, 2017
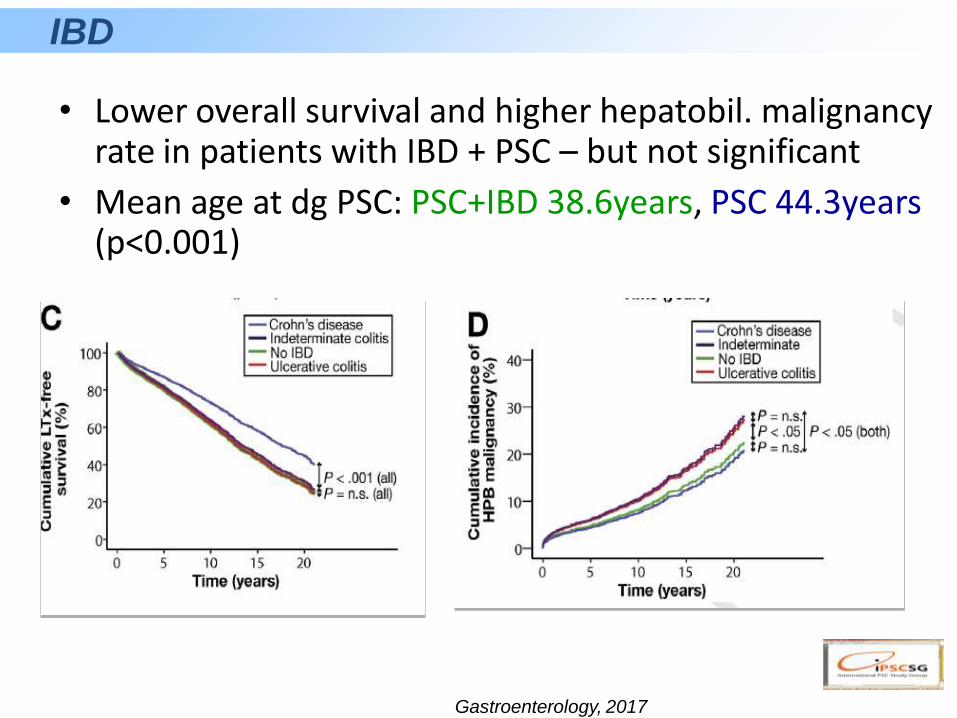
• Lower overall survival and higher hepatobil. malignancy rate in patients with IBD + PSC – but not significant
• Mean age at dg PSC: PSC+IBD 38.6years, PSC 44.3years(p<0.001)
IBD
Gastroenterology, 2017
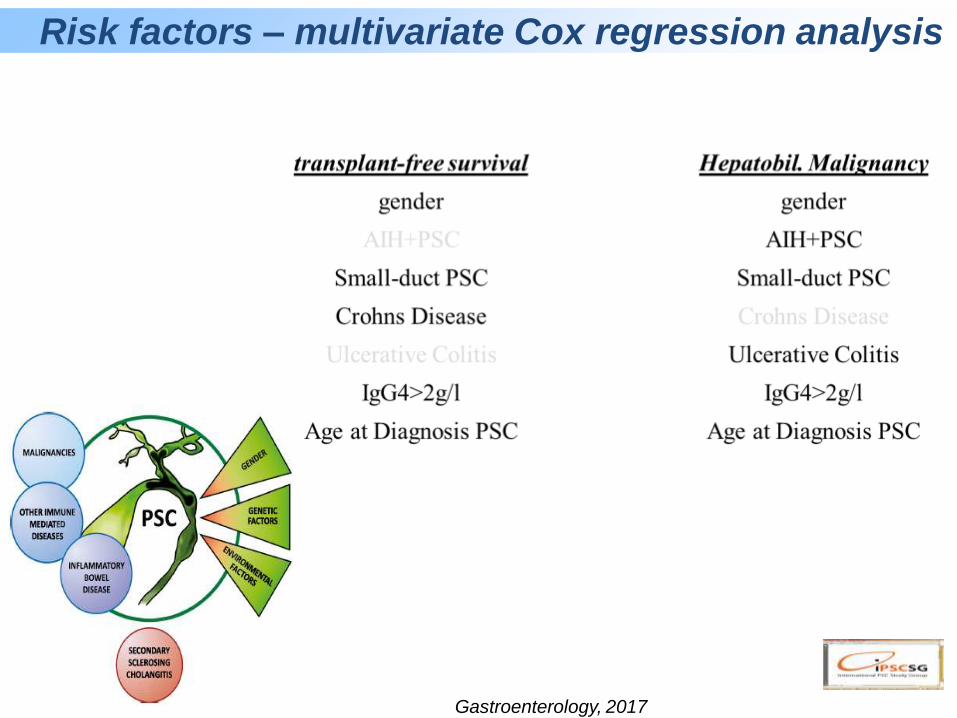
Risk factors – multivariate Cox regression analysis
Gastroenterology, 2017
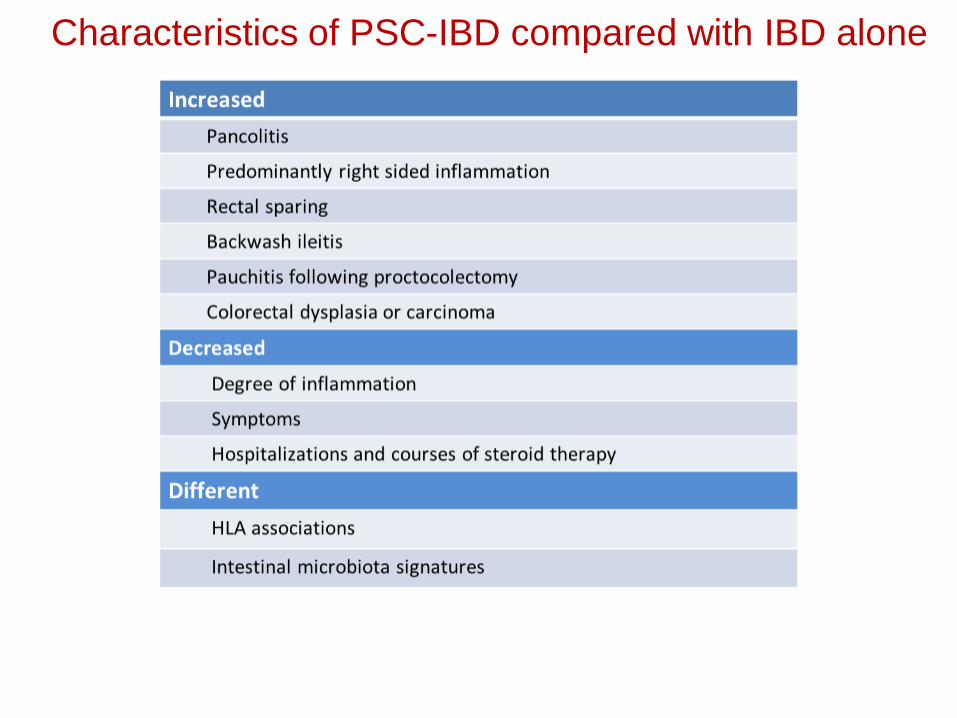
Characteristics of PSC-IBD compared with IBD alone
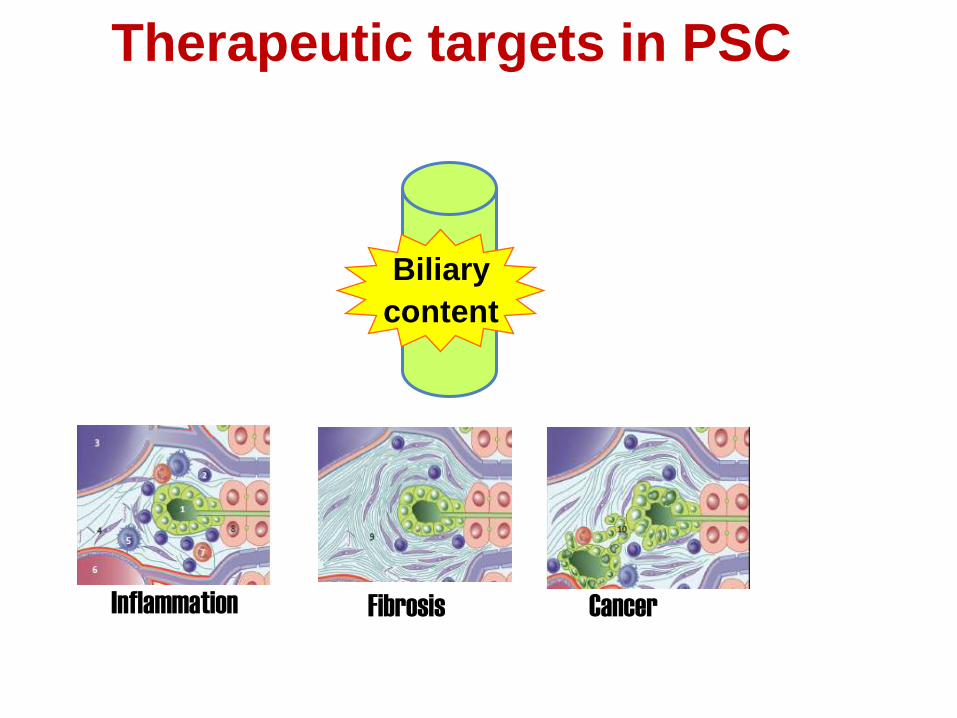
Biliary
content
Inflammation Fibrosis Cancer
Therapeutic targets in PSC
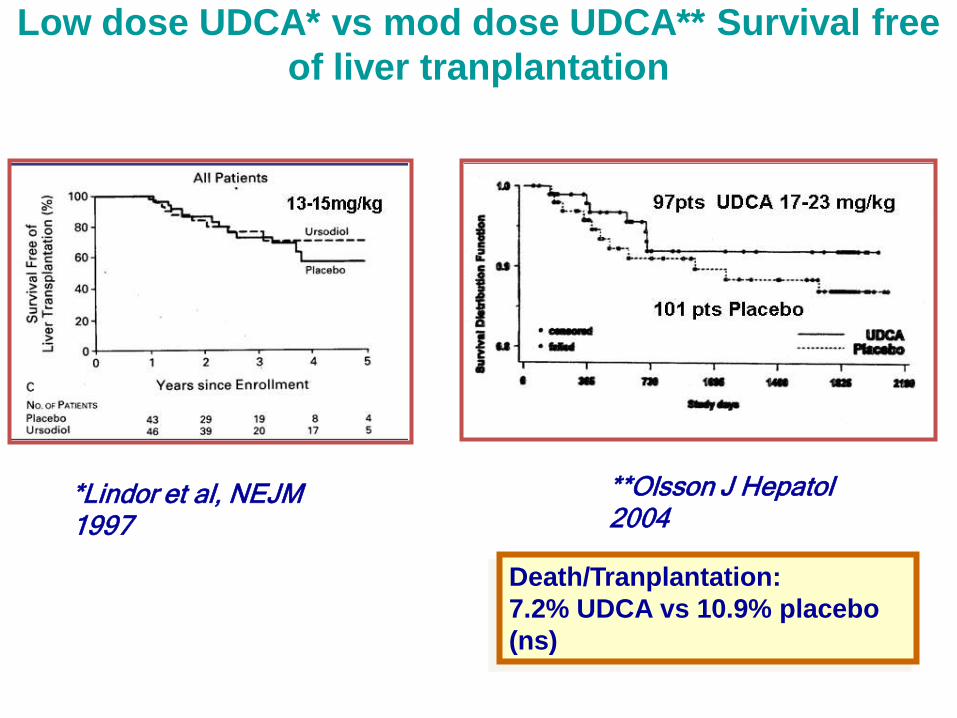
Low dose UDCA* vs mod dose UDCA** Survival free
of liver tranplantation
*Lindor et al, NEJM 1997
**Olsson J Hepatol 2004
Death/Tranplantation:
7.2% UDCA vs 10.9% placebo
(ns)
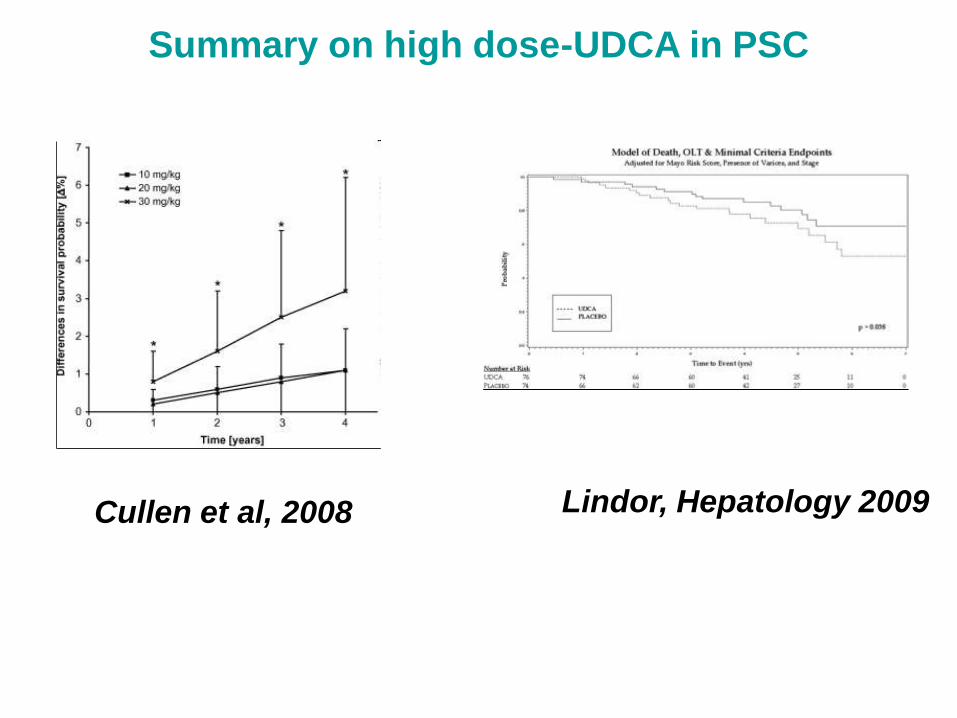
Summary on high dose-UDCA in PSC
Cullen et al, 2008 Lindor, Hepatology 2009

High dose UDCA trial
*Lindor et al, Hepatology 2009
In adult patients with PSC, we recommend
against the use of UDCA (1A). AASLD
Guidelines 2010
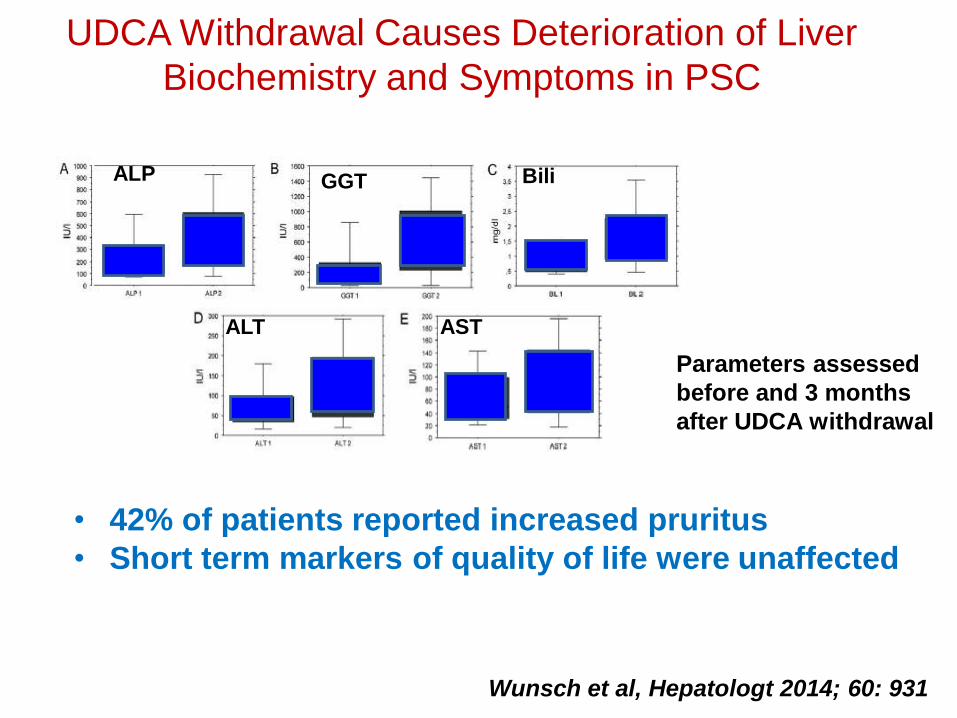
UDCA Withdrawal Causes Deterioration of Liver
Biochemistry and Symptoms in PSC
ALP GGT Bili
ALT AST
Parameters assessed
before and 3 months
after UDCA withdrawal
• 42% of patients reported increased pruritus
• Short term markers of quality of life were unaffected
Wunsch et al, Hepatologt 2014; 60: 931
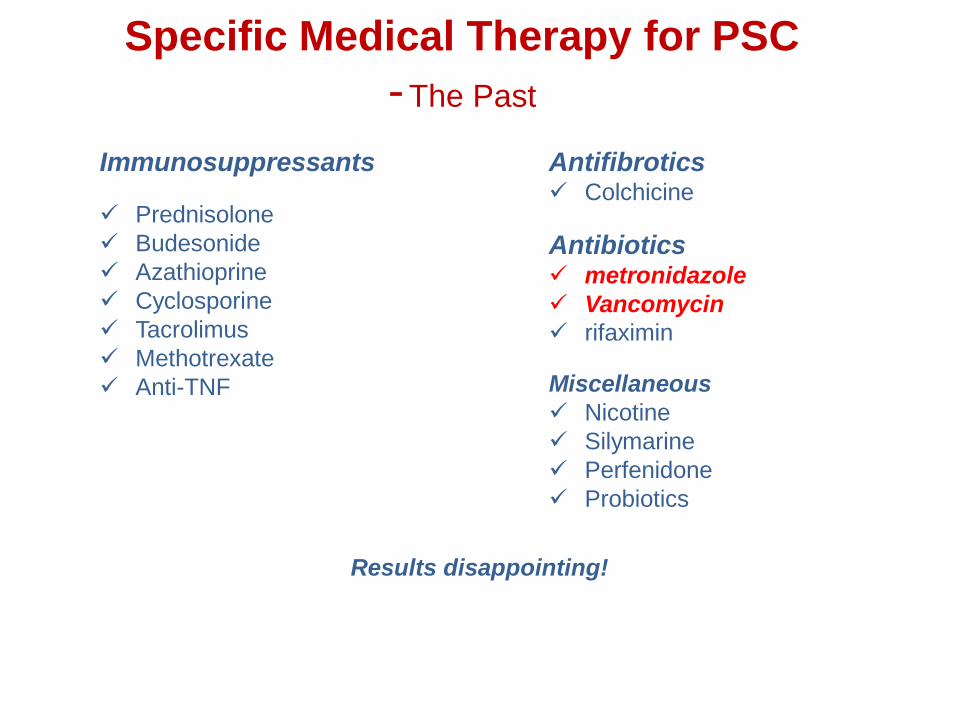
Specific Medical Therapy for PSC
-The Past
Immunosuppressants
Prednisolone
Budesonide
Azathioprine
Cyclosporine
Tacrolimus
Methotrexate
Anti-TNF
Antifibrotics Colchicine
Antibiotics metronidazole
Vancomycin
rifaximin
Miscellaneous
Nicotine
Silymarine
Perfenidone
Probiotics
Results disappointing!
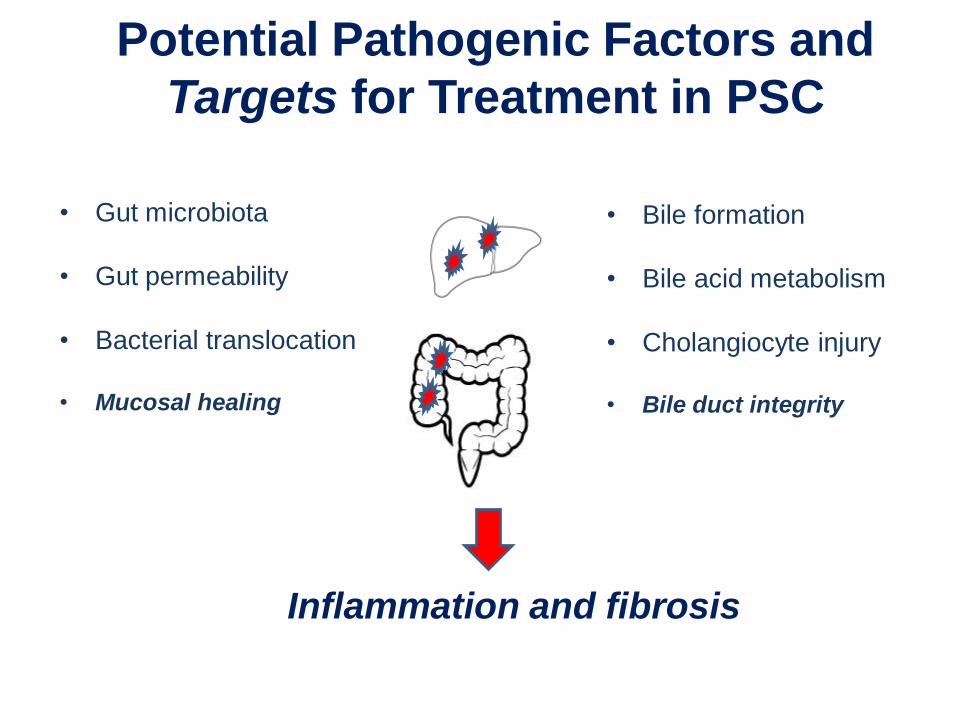
Potential Pathogenic Factors and
Targets for Treatment in PSC
• Gut microbiota
• Gut permeability
• Bacterial translocation
• Mucosal healing
• Bile formation
• Bile acid metabolism
• Cholangiocyte injury
• Bile duct integrity
Inflammation and fibrosis
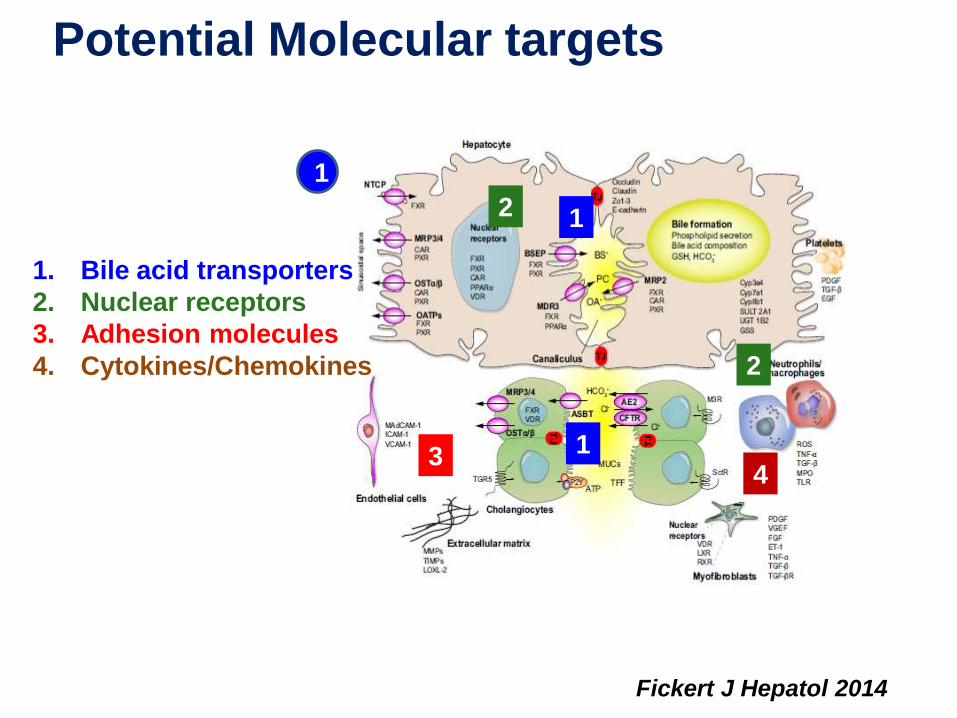
Potential Molecular targets
Fickert J Hepatol 2014
1. Bile acid transporters
2. Nuclear receptors
3. Adhesion molecules
4. Cytokines/Chemokines
1
1
1
2
2
34
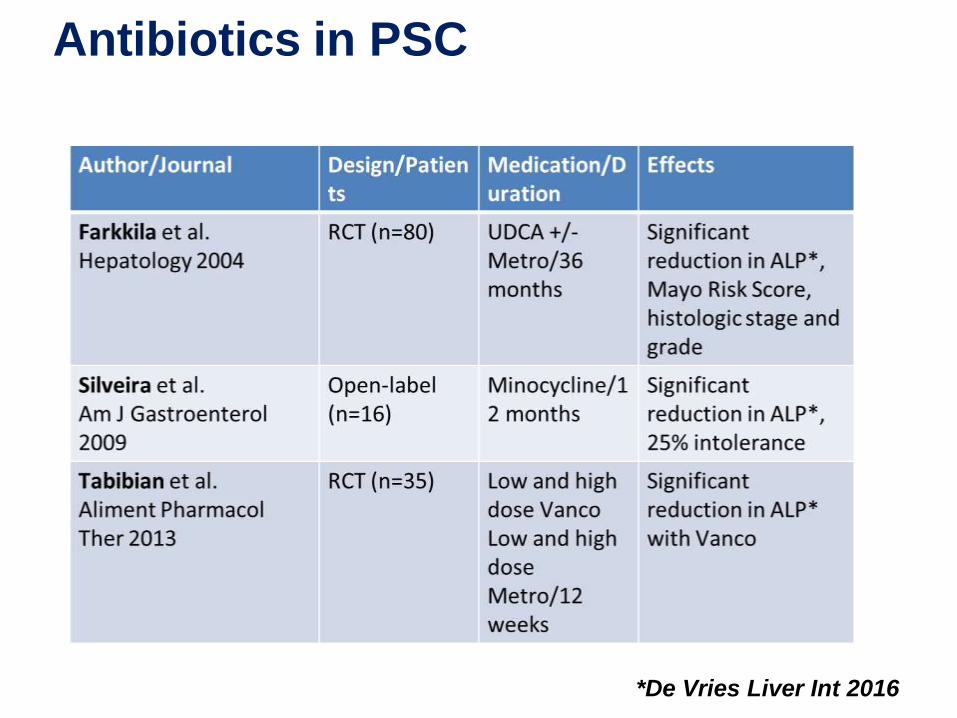
Antibiotics in PSC
*De Vries Liver Int 2016
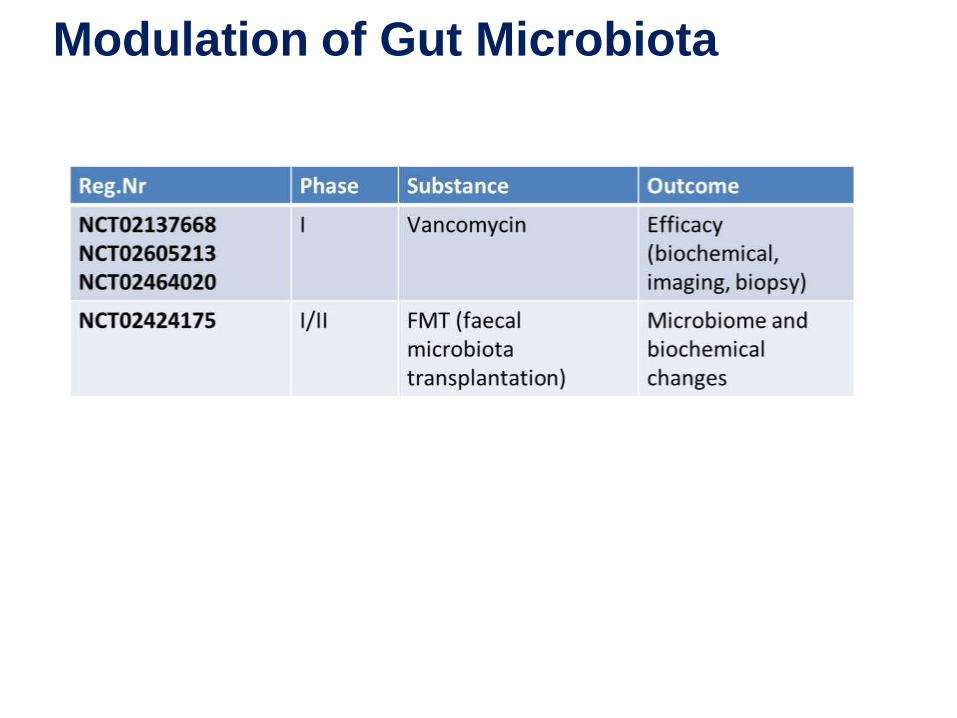
Modulation of Gut Microbiota

Modulation of Gut Microbiota
Intestinal mucosal vessels
Natalizumab
Vedolizumab
Etrolizumab
Trivedi J Autoimmun 2013
Gut-tropic
T-cell
CCR9
a4b7
CCL25MAdCAM-1
Hepatic sinusoids
BT1023 PF00547659
PF00547659
MAdCAM-1VAP-1
CCL25
VAP-1 H2O2 NfkB MAdCAM-1
Vedolizumab in PSC
• 27 pts with PSC-IBD
• Vedo 300 mg iv at weeks 0, 2, 6
• Primary endpoint 50% reduction in ALP
• 63% achieved primary endpoint
Eksteen et al. PS124 ILC 2016
HC O 3-
C l-
CF
TR
CaC
l
C l-
C l-
S ecretinAC h
ATP
ATP
P2Y AE
2
Ins P 3
Ins P 3E R
C a++
c AMP
TGR-5
+
C a++
+
P2Y
AT
P
C l-
C l-C l
-
HCO3-
HCO3-
HCO3-
HCO3-
HCO3-
HCO3-
HCO3-
HCO3-
HCO3-
HCO3-
HCO3-
HCO3-
HCO3-
HCO3-
HCO3- HCO3
-
HCO3-
HCO3-
HCO3-
HCO3-HCO3
-HCO3
-
HCO3-
HCO3-
HCO3-
HCO3-
M3R
OHHO
COOH
OHHO
COO-
HCO3- H2CO3
Apoptos is
F ibros ing / s cleros ing cholangitis
C DC A
B ile
C holang ioc yte
HC O 3
-
H 2O + C O 2
+ H+
S R
C A
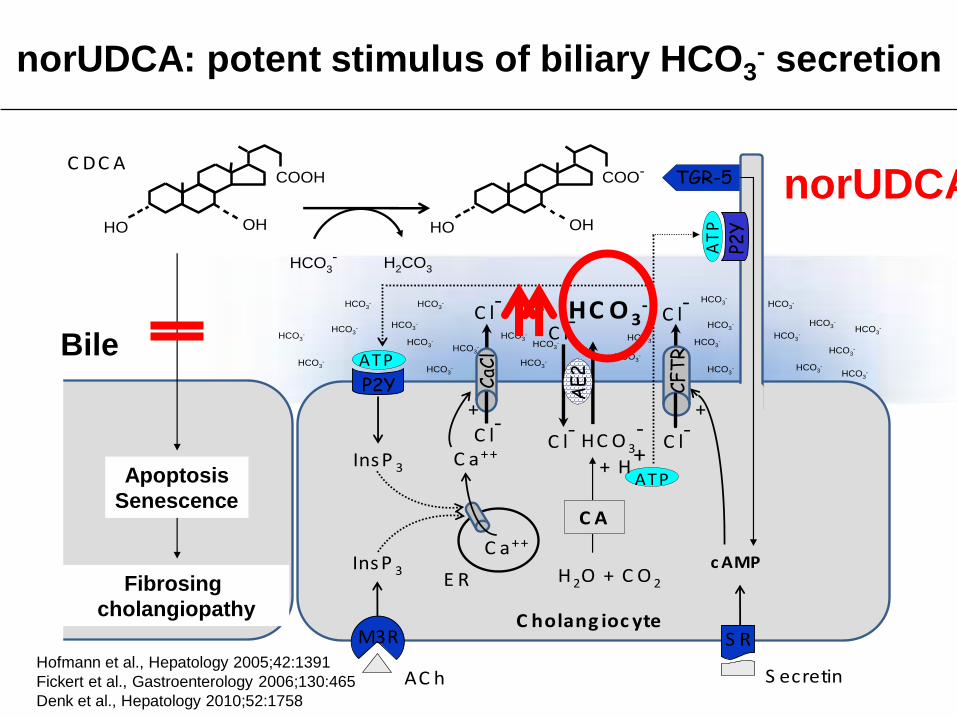
norUDCA: potent stimulus of biliary HCO3- secretion
Bile
norUDCA
Hofmann et al., Hepatology 2005;42:1391
Fickert et al., Gastroenterology 2006;130:465
Denk et al., Hepatology 2010;52:1758
Apoptosis
Senescence
Fibrosing
cholangiopathy
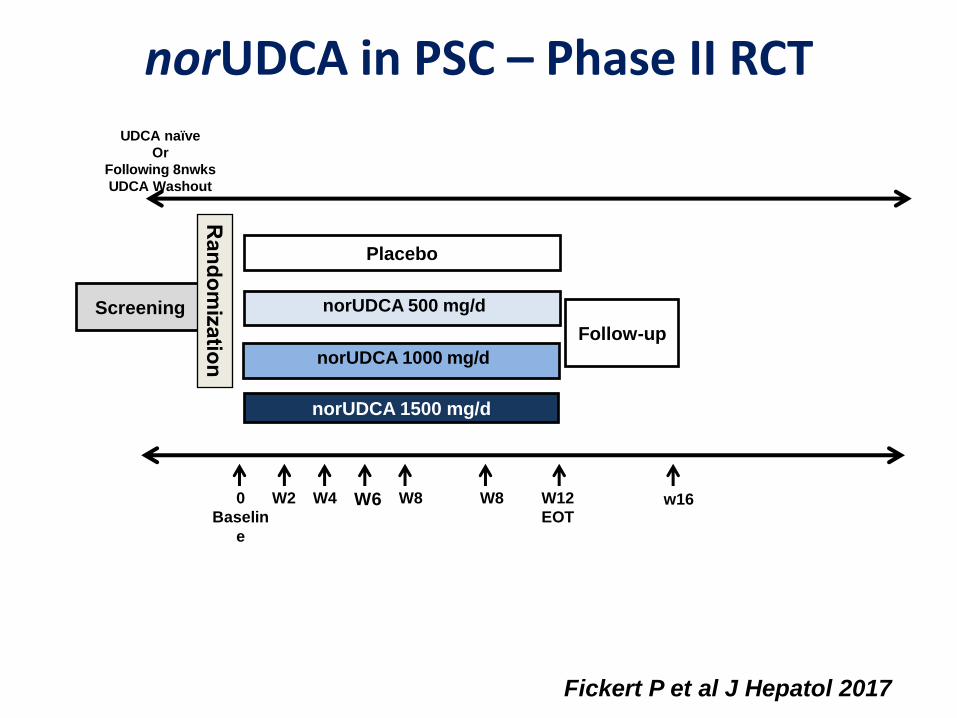
norUDCA in PSC – Phase II RCT
norUDCA 500 mg/d
Placebo
W2 W60
Baselin
e
W4
UDCA naïve
Or
Following 8nwks
UDCA Washout
norUDCA 1500 mg/d
W8 w16W8 W12
EOT
Follow-up
Screening
norUDCA 1000 mg/d
Fickert P et al J Hepatol 2017
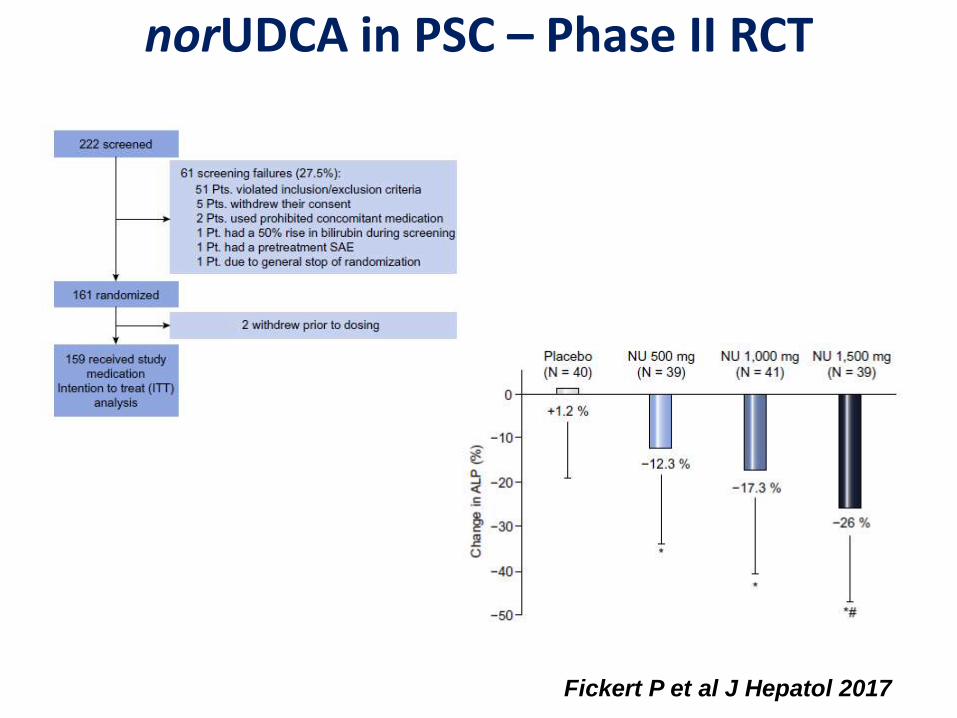
norUDCA in PSC – Phase II RCT
Fickert P et al J Hepatol 2017
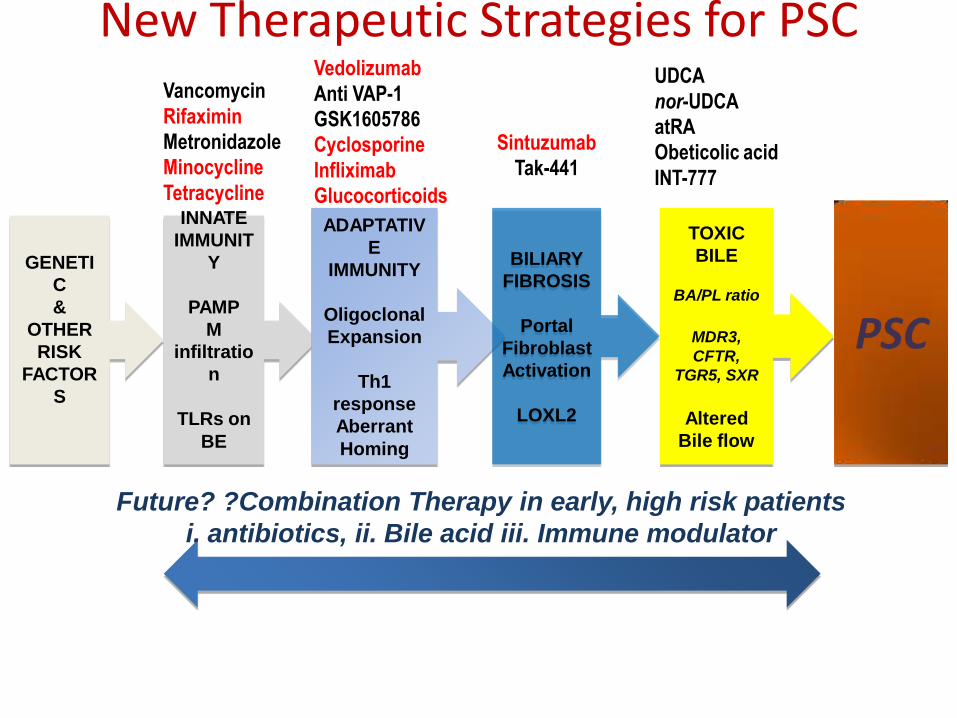
GENETI
C
&
OTHER
RISK
FACTOR
S
INNATE
IMMUNIT
Y
PAMP
M
infiltratio
n
TLRs on
BE
ADAPTATIV
E
IMMUNITY
Oligoclonal
Expansion
Th1
response
Aberrant
Homing
BILIARY
FIBROSIS
Portal
Fibroblast
Activation
LOXL2
TOXIC
BILE
BA/PL ratio
MDR3,
CFTR,
TGR5, SXR
Altered
Bile flow
PSC
Vancomycin
Rifaximin
Metronidazole
Minocycline
Tetracycline
Vedolizumab
Anti VAP-1
GSK1605786
Cyclosporine
Infliximab
Glucocorticoids
Sintuzumab
Tak-441
UDCA
nor-UDCA
atRA
Obeticolic acid
INT-777
Future? ?Combination Therapy in early, high risk patients
i. antibiotics, ii. Bile acid iii. Immune modulator
New Therapeutic Strategies for PSC



















