COGNITIVE THERAPY Slides created by Barbara A. Cubic, Ph.D. Professor Eastern Virginia Medical...
68
COGNITIVE THERAPY COGNITIVE THERAPY Slides created by Slides created by Barbara A. Cubic, Ph.D. Barbara A. Cubic, Ph.D. Professor Professor Eastern Virginia Medical School Eastern Virginia Medical School To accompany To accompany Current Psychotherapies 10 Current Psychotherapies 10
-
Upload
flora-harvey -
Category
Documents
-
view
226 -
download
5
Transcript of COGNITIVE THERAPY Slides created by Barbara A. Cubic, Ph.D. Professor Eastern Virginia Medical...

COGNITIVE THERAPYCOGNITIVE THERAPY
Slides created bySlides created by
Barbara A. Cubic, Ph.D.Barbara A. Cubic, Ph.D.ProfessorProfessor
Eastern Virginia Medical SchoolEastern Virginia Medical School
To accompany To accompany
Current Psychotherapies 10Current Psychotherapies 10

Learning ObjectivesLearning Objectives This presentation will focus on:
• Principles of learning and cognitive theory relevant to psychotherapy
• History of cognitive therapy
• Overview of cognitive therapy
• Commonly used CT techniques
• Creative applications of CT

Basic Concepts of CTBasic Concepts of CT

Basic Concepts Basic Concepts Cognitive therapy focuses
primarily on how information is processed.
Behavioral techniques and cognitive restructuring techniques are utilized to elicit change.

Cognitive ModelCognitive Model Processing of information is vital for
survival. Survival systems are:
• Cognitive• Behavioral• Affective • Motivational
Each system is comprised of structures.• Schemas

ModesModes Information is processed through networks of
cognitive, affective, motivational, and behavioral schemas.
Primal modes are evolutionary-based, universal, tied to survival (e.g. anxiety) and operational almost continuously in some cases (e.g. personality disorders) while other modes are minor and under conscious control.
Primal modes include primal thinking, which is rigid, absolute, automatic, and biased.
Conscious intentions can override primal thinking.
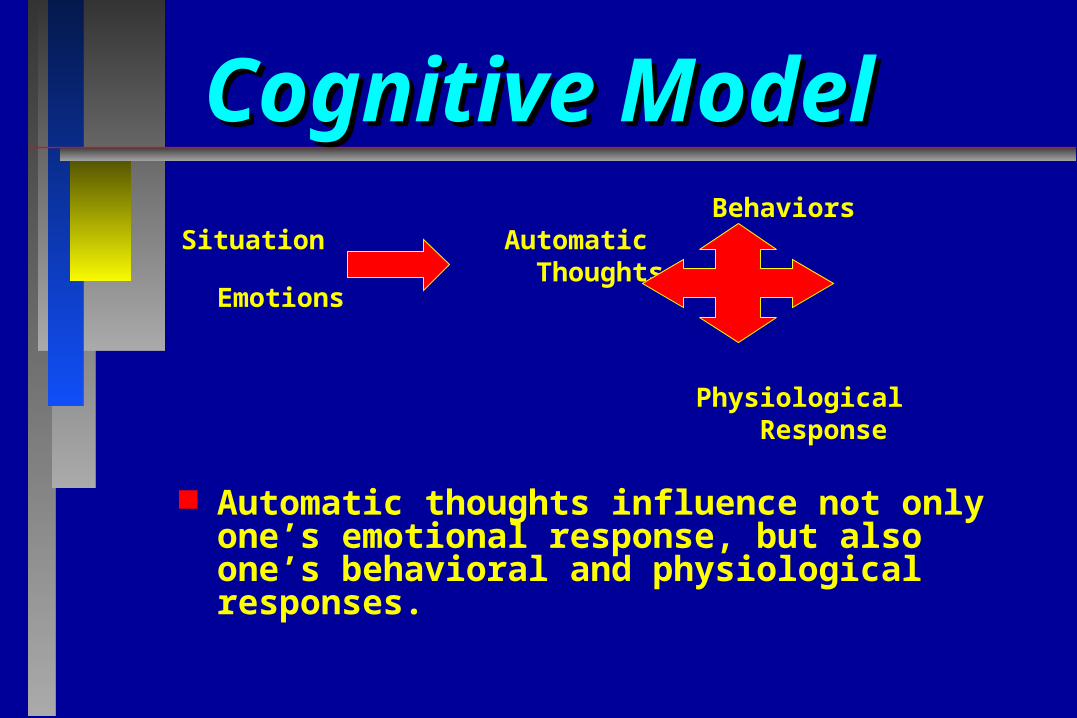
Cognitive ModelCognitive Model
BehaviorsSituation Automatic
ThoughtsEmotions
Physiological Response
Automatic thoughts influence not only one’s emotional response, but also one’s behavioral and physiological responses.

Cognitive ModelCognitive Model In other words, the relationship is bi-
directional (all systems act together as a mode).• Thoughts influence biological, affective,
behavioral (and motivational) processes.• Simultaneously biology, emotions, behavior
(and motivation) influence thoughts.
Therefore biological treatments can change thoughts and CBT can change biological processes.

Cognitive ModelCognitive Model We all have cognitive vulnerabilities (i.e. core
beliefs) which predispose us to interpret information in a certain way.
These vulnerabilities are developed early. When these beliefs are rigid, negative, and
ingrained we are predisposed to pathology. Core beliefs give rise to conditional
assumptions (i.e. rules for living) as we mature.

Cognitive ModelCognitive Model
Behaviors
Situation Automatic
Thoughts Emotions
Underlying Physiological
Beliefs Response
Automatic thoughts are influenced by these underlying core beliefs and conditional assumptions

Cognitive ModelCognitive Model
Withdrawal
Relationship
Breakup He doesn’t want me Depressed
I’m worthless SNS Reaction
I’m unlovable Poor Sleep

Cognitive ShiftsCognitive Shifts In various types of psychopathology,
there is a systematic bias toward selectively interpreting information in a certain manner.

Characteristics of CTCharacteristics of CT Practical Symptom-focused Empirically-derived techniques Requires patient collaboration. Acknowledges underlying precursors
of symptoms (schemas), but present-oriented.
Case conceptualization drives treatment.

Roles of the CT TherapistRoles of the CT Therapist Conceptualize the patient in cognitive Conceptualize the patient in cognitive
terms.terms. Structure the sessions.Structure the sessions. Use collaborative empiricism and Use collaborative empiricism and
guided discovery to:guided discovery to:
• Specify problems and set goals.Specify problems and set goals.
• Teach the patient CT techniques. Teach the patient CT techniques.

CT Strategies CT Strategies Collaborative empiricism Guided discovery Deactivation of dysfunctional
modes:• Deactivate them.• Modify their content and structure.• Construct more adaptive modes to
neutralize them.

Comparing CT to Comparing CT to Other TherapiesOther Therapies

Compared with PsychoanalysisCompared with Psychoanalysis Both assume behavior influenced by beliefs
outside awareness. CT focuses on:
• Linkages among symptoms, conscious beliefs and current experiences.
• Little concern with unconscious feelings or repressed emotions.
• Minimal focus on childhood issues except in terms of assessment or when addressing core beliefs.
CT is highly structured and short-term (12-16 weeks) whereas psychoanalysis is long-term and unstructured.
CT therapist actively collaborates with patient.

CT Compared with REBTCT Compared with REBTCT REBT
Thoughts Labeled
Dysfunctional Irrational
Reasoning Used Inductive Deductive
Beliefs Associated with Psychopathology
Cognitive specificity for disorders
Core set of irrational beliefs
View of the Problem
Functional Philosophical
Therapist’s Approach
More collaborative
More confrontational

Compared to Behavior Compared to Behavior TherapyTherapy
CT is very different from applied behavioral analysis.
CT is the most commonly practiced form of cognitive behavior therapy (CBT).• CBT: An overarching term to represent therapies
that integrate cognitive and behavioral theories and techniques.
CT sees the individual as more active rather than passive in change process.
CT stresses expectations, interpretations and reactions.

History of Cognitive TherapyHistory of Cognitive Therapy

Cognitive TherapyCognitive Therapy Developed by Aaron T. Beck,
M.D.• Investigated “anger turned
inward” psychoanalytic concept in 1960s and found evidence for negative cognitions.
Bandura, Ellis, Mahoney, and Meichenbaum were all influential and developing their approaches simultaneously.

History of Cognitive TherapyHistory of Cognitive Therapy
Major influences were: Major influences were: 1.1. Phenomenological Phenomenological
approachesapproaches
2.2. Structural theory Structural theory and depth and depth psychologypsychology
3.3. Cognitive Cognitive psychologypsychology

Current Status of CTCurrent Status of CT

Research on the Research on the Cognitive ModelCognitive Model
Cognitive specificity hypothesis (i.e., distinct cognitive profile for each disorder) supported for many disorders.• Negatively biased interpretations have been
found in all forms of depression.• Support for cognitive triad, negatively biased
cognitive processing of stimuli and identifiable dysfunctional beliefs in depression.
• Danger-related bias demonstrated in anxiety disorders.

Cognitive Therapy Cognitive Therapy and Medicationand Medication
Studies generally show CT to be equivalent to psychotropic medications for depression, bulimia and some anxiety disorders.
Generally, research suggests the combination of the two approaches is superior to either used in isolation.
CT shows longer efficacy (less relapse) and increased likelihood of continuing gains when treatment is discontinued.

Current Status of CTCurrent Status of CT Controlled studies shown efficacy of CT
with:• Depression• Panic disorder• Social phobia• Generalized anxiety disorder• Substance abuse• Eating disorders• Marital problems• Schizophrenia• OCD• PTSD

CT Assessment Measures CT Assessment Measures Beck Depression Inventory-II (BDI-II) Beck Anxiety Inventory Beck Hopelessness Scale (score of
> 9 predictive of eventual suicide) Beck Scale for Suicidal Ideation Many others

Resources in CTResources in CT Center for Cognitive Therapy (U/Penn) and
Beck Institute are the major training sites (both in Philadelphia).
Multiple other training sites in the United States and internationally:• Cognitive Therapy and Research • Journal of Cognitive Psychotherapy• Academy of Cognitive Therapy
(www.academyofct.org)

Understanding the Understanding the TheoryTheory
Behind CT Behind CT

Cognitive Case Cognitive Case ConceptualizationConceptualization

Personality Dimensions:Personality Dimensions:Styles of BehavingStyles of Behaving
Sociotropy (social dependence):• Become depressed following
disruption of relationship(s).
• Organized around closeness, nurturance, and dependence.

Personality Dimensions:Personality Dimensions:Styles of BehavingStyles of Behaving
Autonomy:• Become depressed after defeat or
failure to attain a desired goal.
• Organized around independence, goal setting, self-determination, and self-imposed obligations.

Problematic ThinkingProblematic Thinking
Extreme Broad Catastrophic Negative Unscientific Pollyannaish
Idealistic Demanding Judgmental Comfort Seeking Obsessive Confusing
Problematic thinking is very:
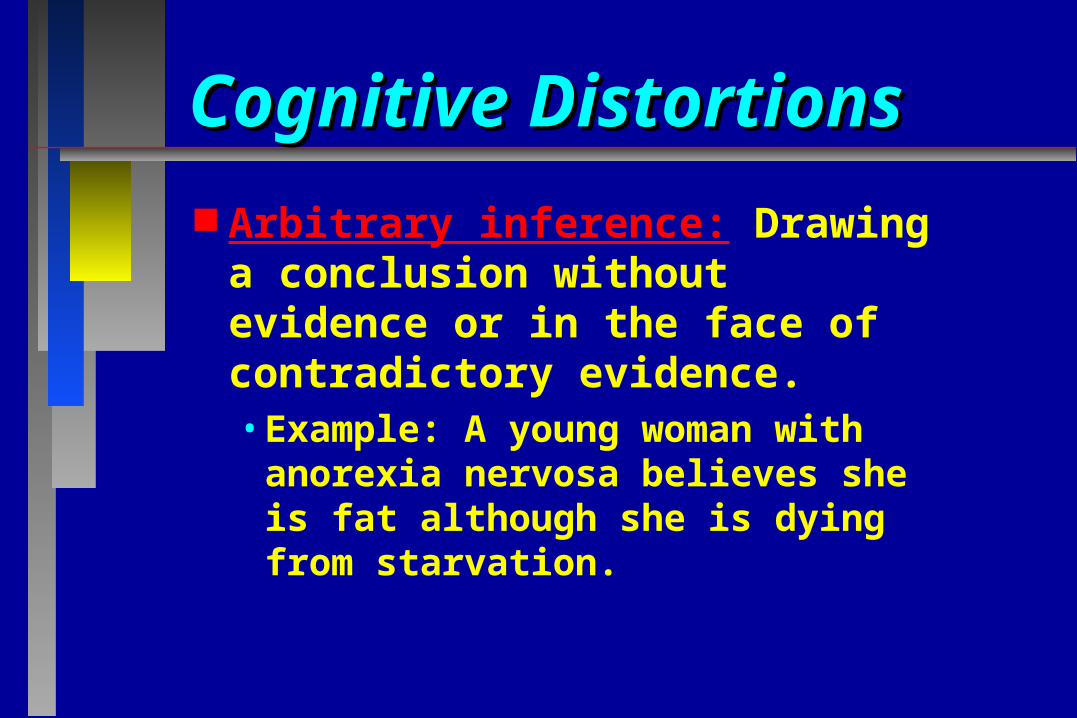
Cognitive DistortionsCognitive Distortions
Arbitrary inference: Drawing a conclusion without evidence or in the face of contradictory evidence.• Example: A young woman with
anorexia nervosa believes she is fat although she is dying from starvation.

Cognitive DistortionsCognitive Distortions
Selective abstraction: Dwelling on a single negative detail taken out of context.• Example: While on a date, you
say one thing you wish you could have said differently and now see the entire evening as a disaster.

Cognitive DistortionsCognitive Distortions
Overgeneralization: A single negative event is viewed as a never-ending pattern of defeat.• Example: Following a job interview,
an accountant does not receive the job. He/she begins thinking that they will never find a job position despite their qualifications.

Cognitive DistortionsCognitive Distortions
Magnification and/or minimization: The binocular trick. Things seem bigger or smaller than they are.• Example: An employee believes that
a minor mistake will lead to being fired.
• Example: An alcoholic believes he/she doesn’t have a problem.

Cognitive DistortionsCognitive Distortions
Personalization: Assuming personal responsibility for something for which you are not responsible.• Often seen in patients who are
sexually abused/assaulted.

Cognitive DistortionsCognitive Distortions
Dichotomous thinking: Things are seen as black and white, there is no gray or middle ground.• Things are wonderful or awful,
good or bad, perfect or a failure.

Cognitive DistortionsCognitive Distortions Mind reading: Assuming someone is
responding negatively to you without checking it out. • Example: If your husband is in a bad mood,
you assume it is your fault and don’t ask what is wrong.
Fortune teller error: Creating a negative self-fulfilling prophecy. • Example: You believe you will fail an exam
so you don’t study and fail.

Cognitive DistortionsCognitive Distortions
Emotional reasoning: You assume that your negative feeling results from the fact that things are negative. • Example: If you feel bad, then that
means the world or situation is bad. You don’t consider that your feelings are a misrepresentation of the facts.

Cognitive DistortionsCognitive Distortions Should statements: Use words
like should, must, ought rather than “it would be preferred” to guilt self.
Labeling and mislabeling: Name-calling (such as “he’s a jerk”) rather than just criticizing the behavior.

Cognitive Triad of DepressionCognitive Triad of Depression
Negative
view of

Examples of Cognitive Shifts: Examples of Cognitive Shifts: Depression vs. AnxietyDepression vs. Anxiety
Negative view of Threatening view of
Future Future
Self World Self World

Illustration of the Cognitive Illustration of the Cognitive Model of AnxietyModel of Anxiety
Stimulus
(Environmental Or Internal)
Secondary appraisal:
“Risk: Resources ratio”
Reappraisals of danger, risk, resources
Behavioral inclination
(Flight, Freeze, Defend)
Affect
Anxiety, Terror
Physiological
Palpitations,Sweating,
Tension, etc.
Primary appraisal:
“Danger”
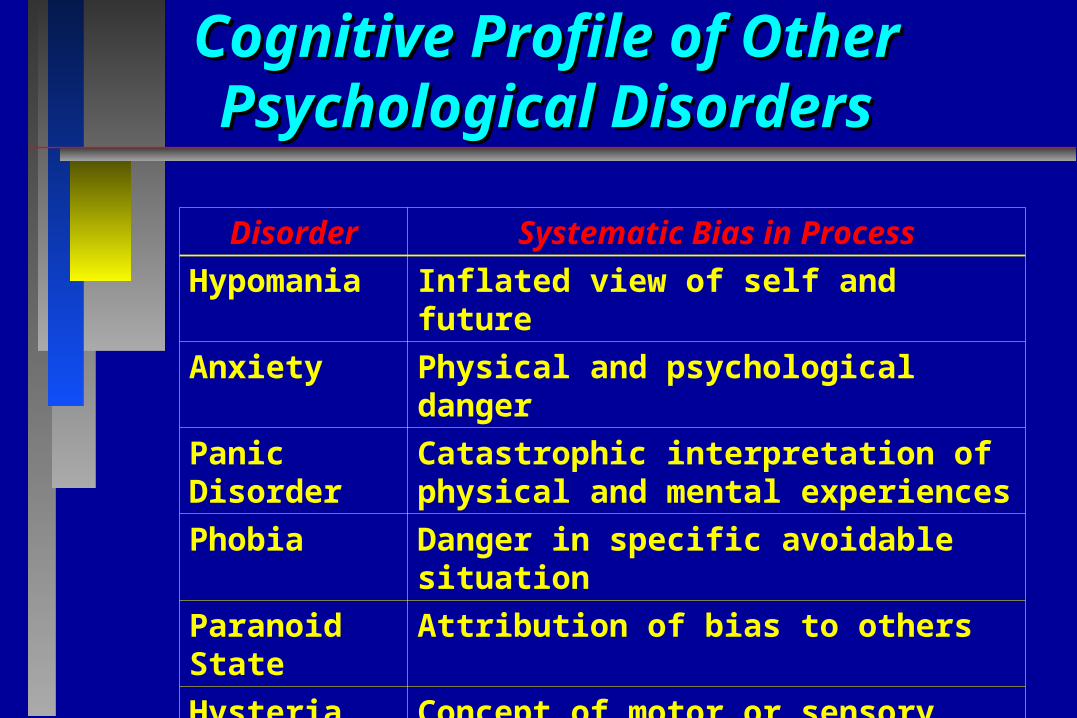
Cognitive Profile of Other Cognitive Profile of Other Psychological DisordersPsychological Disorders
Disorder Systematic Bias in Process
Hypomania Inflated view of self and future
Anxiety Physical and psychological danger
Panic Disorder
Catastrophic interpretation of physical and mental experiences
Phobia Danger in specific avoidable situation
Paranoid State
Attribution of bias to others
Hysteria Concept of motor or sensory abnormality

Cognitive Profile of Other Cognitive Profile of Other Psychological DisordersPsychological Disorders
Disorder Systematic Bias in Process
Obsession Repeated doubts about safety
Compulsion Rituals to ward off perceived Threats
Suicidal State Hopelessness; deficiencies in problem-solving
Anorexia Nervosa
Fear of being fat
Hypochondriasis Attribution of serious medical disorder

Cognitive Therapy Cognitive Therapy TreatmentTreatment

Structure of a CBT SessionStructure of a CBT Session Mood check Setting the agenda Bridging from last session Today’s agenda items Homework assignment Summarizing throughout and at end Feedback from patient

General Principles of CTGeneral Principles of CT Goal is to correct dysfunctional
thinking and help patients modify erroneous assumptions.
Patient is taught to be a scientist who generates and tests hypotheses.
Relationship between patient and therapist is collaborative.
Fundamental ConceptsFundamental Concepts Collaborative empiricism:
• Goal is to demystify therapy. Socratic dialogue:
• Questioning used to help patient come to their own conclusions.
Guided discovery:
• Therapist collaborates with patient to develop behavioral experiments to test hypotheses.

Process of TherapyProcess of Therapy Initial sessions
• Essential to build rapport.
• Focus is problem definition, goal-setting and symptom relief.
• Therapist provides psychoeducation in initial sessions.
• Behavioral interventions more prominent. Middle sessions
• Emphasis shifts from symptoms to patterns of thinking.
Termination• Expectation that therapy is time limited.

Behavioral Intervention Examples Behavioral Intervention Examples
Activity scheduling Mastery and pleasure Graded task assignment Conducting behavioral experiments
(e.g. being assertive to assess what happens)
Exposure type techniques Role plays

Weekly Activity ScheduleWeekly Activity Schedule
Mon Tue Wed Thu Fri Sat Sun
8-10 am
10-12 pm
12-2 pm
2-4 pm
4-6 pm
6-8 pm
8-10 pm
10-12 am
Patient records activities and rates them for pleasure and mastery

Weekly Activity MonitoringWeekly Activity Monitoring A self-rated chart that allows the therapist
and the patient to:• Assess how patients are spending their time.• Measure the sense of accomplishment and/or
pleasure received from various activities.• Determine which activities are occurring too
much or too little.• Evaluate automatic thoughts/emotional shifts.• Fill in specific times with planned/pleasant
activities for depressed patients or activities needed for procrastinating patients.
• Compare predicted versus actual ratings of accomplishment and pleasure.

Cognitive Interventions ExamplesCognitive Interventions Examples Elicit automatic thoughts on thought
records. Identify whether the thoughts
represent distortions in information processing.
Use Socratic questions to evaluate the thought process.
Generate alternatives in terms of how to think or how to behave differently.

Thought RecordThought RecordSituation Mood
1- 100 Automatic Thought
Evidence For AT
Evidence Against
AT
Balanced/ Alternative Viewpoint
Re-rate Mood

Eliciting Automatic ThoughtsEliciting Automatic Thoughts Basic question: What thought just went through
your mind?• Ask when an emotional shift is noted in session.• Create an emotional shift by having the patient describe
or visualize a recent situation when they felt intense emotions and then answer the question.
If patient can’t answer the question try asking:• Do you think you were thinking _____________?• If someone else was in the situation what do you think
they might have been thinking?• Were you thinking _____________ (insert something
paradoxical)?

Examples of Socratic Questions Examples of Socratic Questions What evidence supports the belief? What evidence do you have to refute it? What would your spouse, best friend, sibling (or
anyone whom you admire greatly) say in this situation?
What would you say to your spouse, best friend, or sibling if they were thinking the same thing you are?
How could you look at this situation so you would feel less depressed?
Is this view as reasonable as your first choice?

Specific Examples of Specific Examples of Socratic QuestioningSocratic Questioning
Situation: Patient feels like a bad wife. What makes you think you are a bad wife? What would a good wife have done? On a scale from 0-100, how do you rate as a
wife? Why do you place yourself there on the scale?
How does it help to call yourself a bad wife? Besides labeling yourself as a bad wife what
else could you do in this situation?

Non-Socratic QuestionsNon-Socratic Questions(Questions NOT to Use)(Questions NOT to Use)
Don’t you think most women get mad at their husbands?
Doesn’t your husband ever yell at you? I’m sure everything will work out OK,
don’t you? I think you are a good wife based on
other things you’ve told me. Could you focus on the positives?

Example: Downward Arrow Example: Downward Arrow to Obtain Less Accessible Beliefsto Obtain Less Accessible Beliefs
Situation Thoughts Emotions
Patient reports that a session hasn’t helped them.
Therapist thinks patient is right. That was a terrible session. I didn’t do anything right.
Guilty
Anxious

Example: Downward ArrowExample: Downward ArrowQuestionIf that were true, what would it mean about you?If that were true what would it mean to you?And, then what?
Response“That I had done a bad job.”“Sooner or later I would be found out.”“Everyone would know I was an imposter and incompetent.”

Setting Effective CT HomeworkSetting Effective CT Homework Make sure rationale is clear. When feasible, have patient chose the task. Personalize task to therapy goals. Begin where patient is, not where patient thinks
he/she should be. Be specific and concrete: where, when, who. Formalize the task (e.g., write on paper). Plan ahead for obstacles/trouble shoot. Practice the task in session. Review homework at beginning of each session.

Other CT TechniquesOther CT Techniques De-catastrophizing:
“What if that happened? Then what?”
Reattribution: Alternative explanations systematically examined.
Redefining: Help patient see the problem differently.
Example: “Nobody ever talks to me” becomes “I need to try to initiate conversation so other people become interested in talking to me.”
Decentering: Patient is taught to see that thoughts are just
thoughts and not “them” or “reality.”

Applications of CT: Applications of CT: Empirically Supported Empirically Supported
Meta-analyses and other recent methodologically rigorous studies have found CT to have large effect sizes for:• Major depression• Generalized anxiety disorder• Panic disorder• Social phobia• Childhood depressive and anxiety
disorders

Applications of CT: Applications of CT: Empirically SupportedEmpirically Supported
Moderate effect sizes for:• Marital problems• Anger• Childhood somatic disorders• Chronic pain
Small effect sizes for:• Schizophrenia
• Bulimia nervosa

Applications of CT: Applications of CT: Empirically SupportedEmpirically Supported
CT yields lower relapse rates than antidepressant medications and reduces the risk of symptom relapse.