Clinical Trials on Multiple Myeloma in Chinacme-utilities.com/mailshotcme/Material for...
43
Clinical Trials on Multiple Myeloma in China Wenming Chen Beijing Chaoyang Hospital Capital Medical University Multiple Myeloma Research Center of Beijing
Transcript of Clinical Trials on Multiple Myeloma in Chinacme-utilities.com/mailshotcme/Material for...

Clinical Trials on Multiple Myeloma in China
Wenming Chen
Beijing Chaoyang Hospital
Capital Medical University
Multiple Myeloma Research Center of Beijing

Current situation of anti-myeloma drugs
Available Reimbursement Indication
Melphalan oral:x iv: x Transplant
Bortezomib NDMM, RRMM
Ixazomib RRMM
Carfilzomib Trail closed, will be approved on 2020
Thalidomide off-label
Lenalidomide NDMM,RRMM, Mainten
Pomalidomide will be approved on 2019
Daratumumib will be approved on 2019
Isatuximab on trial
Selinexor on trial
CAR-T Ongoing Phase I-II trial: 3 IIS: >10
TRAIL Phase III on goning

Circularly Permuted TNF-Related Apoptosis-Inducing Ligand
(TRAIL,CPT) for the treatment of RRMM

Recombinant human TRAIL-induced apoptosis
TRAIL: TNF-Related Apoptosis-Inducing LigandDR: death receptor DcR: Decoy receptor OPG: osteoprotegerin

Modified CPT monomer structureWild type TRAIL monomer structure
Structure of CPT
CPT—Circularly Permuted TRAIL
N-terC-ter
N-ter
C-ter
Flexible linker
Advantages of CPT
⚫ more potent anti-tumor activity in preclinical studies compared with wild type
TRAIL
⚫ longer half-life than recombinant human Apo2L/TRAIL in human

Nude mice with established RPMI-8226(left) or NCI-H460(right) xenografts were
given CPT or wtTRAIL as an i.p. bolus for 10 consecutive days (n=6-8/group).
Results shown(plot) are mean values.
Anti-myeloma activity of CPT
in vivo: more potent anti-myeloma tumor activity in mouse xenograftmodels compared with wild type TRAIL (wtTRAIL)
0 5 10 15 20 25
0
500
1000
1500
2000
2500
3000
3500
4000
Tum
or si
ze (m
m3 )
Days
control
CPT15mg/kg
CPT3mg/kg
wtTRAIL15mg/kg
CPT/TRAIL

CPT for RRMM: Phase I Trial
Study design
−Open-label, single agent, dose escalation studies
−Observe overall safety, PK, Preliminary efficacy studies
2.5mg /kg/d×14d
1.7mg /kg/d×14d
1.0mg /kg/d×14d
Phase Ia: Advanced solid tumor and
hematologic cancers (N=28)
15mg /kg/d×5d
10mg /kg/d×5d
8.0mg /kg/d×5d
6.5mg /kg/d×5d
5.0mg /kg/d×5d
Phase Ib: Refractory/Relapsed Multiple
Myeloma (N=29)
Am J Hematol, 2014, 89: 1037-42

Phase Ib:Efficacy Results In RRMM patients
*Efficacy evaluable patients
Response Rates: assessments were based EBMT criteria.
Response
Rate
5,6.5mg/kg
(n=9)8, 10mg/kg
(n=12)15mg/kg
(n=6)Total*
(n=27)
CR & nCR, n(%) 0 0 1(16.67) 1(3.70)
PR, n(%) 0 3 (25) 1(16.67) 4(14.81)
MR, n(%) 3 (33.33) 0 1 (16.67) 4(14.81)
CR+PR, n(%) 0 3 (25) 2 (33.33) 5(18.52)
CR+PR+MR, n(%) 3 (33.33) 3 (25) 3 (50) 9(33.33)
Am J Hematol, 2014, 89: 1037-42

Phase Ⅰ:Treatment-related Adverse Events
Well tolerated, No DLT were found
AE, %Phase I
(N=28+29)
ALT 24.56%
AST 22.80%
Fever 17.54%
Fatigue 12.28%
Nausea 7.02%
Vomiting 10.53%
Leukopenia 12.28%
Anorexia 5.26%
Rash 3.51%
Tumor Lysis Syndrome 1.75%
Am J Hematol, 2014, 89: 1037-42

Phase II
Trial-1:
CPT monotherapy for
RRMM (N=27)
Trial-2:
CPT plus Thalidomide for
RRMM(N=43)
Objectives: safety, efficacy
Patients: Refractory or Relapsed MM
Trial-3:
CPT plus Thalidomide
and Dexamethasone (TD)
for RRMM (N=71)
CPT FOR RRMM: Phase II Trial
Cancer Chemother Pharmacol. 2017,79(6):1141-1149Am J Clin Oncol. 2018,41(10):1008-1014

Trial-3: CPT in combination with Thalidomide and Dexamethasone (TD) for RRMM (N=71)
− Design: multi-center, open-Label, Randomized and Controlled
− Inclusion criteria: relapsed and/or refractory multiple myeloma , received at least 2
prior anti-MM therapy.
− Intervention: CPT+TD vs TD
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19 – 28
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19 - 28
CPT 10mg/kg
Thalidomide 150mg
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19 – 28
Dexamethasone 40mg
Phase II: Trial-3 (CPT+TD vs TD)
Cancer Chemother Pharmacol. 2017,79(6):1141-1149

Efficacy results
Phase II: Trial-3 (CPT+TD vs TD)
Best Response(EBMT)(n=71)
CPT+TD
(n=47)
TD
(n=24)
Efficacy-evaluable patients 41 23
nCR, n(%) 7(17.1) 0(0)
PR, n(%) 11(26.8) 6(26.1)
MR, n(%) 7(17.1) 1(4.3)
nCR+PR, n(%) 18(43.9) 6(26.1)
nCR+PR+MR, n(%) 25(61.0) 7(30.4)
PFS (n=71), Median(95% CI) 6.7(3.3~10.1) 3.1(1.7~4.5)
Cancer Chemother Pharmacol. 2017,79(6):1141-1149

Kaplan-Meier curves of progression-free survival (PFS)
Phase II: Trial-3 (CPT+TD vs TD)
Cancer Chemother Pharmacol. 2017,79(6):1141-1149

Safe and well tolerated of CPT in combination with TD therapies
Table 1. Incidences of adverse events (Safety population)Adverse events (AEs), n (%)b CPT+TD (N=47) TD (N=24)
Any grades Grade 3 or 4 Any grades Grade 3or 4
Hematologic AEsNeutropenia 22 (46.8) 7 (14.9) 12 (50.0) 6 (25.0)Leukopenia 18 (38.3) 3 (6.4) 9 (37.5) 3 (12.5)Decreased Haemoglobin 13 (27.7) 3 (6.4) 11 (45.8) 8 (33.3)Thrombocytopenia 9 (19.1) 5 (10.6) 5 (20.8) 5 (20.8)
Non-hematologic AEsIncreased ALT 22 (46.8) 4 (8.5) 2 (8.3) 0Increased AST 13 (27.7) 5 (10.6) 0 0Hypocalcaemia 12 (25.5) 3 (6.4) 0 0Lung infection 11 (23.4) 4 (8.5) 6 (25.0) 4 (16.7)Fever 11 (23.4) 0 4 (16.7) 1 (4.2)Hypokalemia 9 (19.1) 3 (6.4) 1 (4.2) 0Increased LDH 8 (17.0) 2 (4.3) 1 (4.2) 0
Serious adverse events (SAEs), n (%)c
Any event 8 (17.0) 6 (25.0)aAEs were evaluated independent of the relation to the treatment. bAEs with an incidence ≥15% among
patients in either study group were listed. cAll SAEs were listed.
Phase II: Trial-3 (CPT+TD vs TD)
Cancer Chemother Pharmacol. 2017,79(6):1141-1149

Summary
1. CPT showed more potent activity and longer half life compared
with wtTRAIL
2. Safe and well tolerated
3. Definite efficacy for refractory/relapsed MM as mono-therapy.
4. Definite Dose-Response Relationship.
5. CPT+TD, show superior efficacy compared with TD

Study of CPT or Placebo plus Thalidomide and Dexamethasone
in Relapsed and/or Refractory Multiple Myeloma
Phase III trial
− A Multicenter, Randomized, Double-Blind, Controlled Phase 3 study
− Enrollment: 417 patients, received at least 2 prior line therapy
− Study start date: March 2017
Study completion date: Q2 2019
− Primary endpoint: PFS
Ongoing trial

PublicationsNo. Time Journal Title
1 2018Hematology
2018,23(9):620-625.
Synergistic effects of rmhTRAIL and 17-AAG on
the proliferation and apoptosis of multiple myeloma cells
2 2017Cancer Lett
2017 Mar 28;389:70-77.
Rocaglamide breaks TRAIL-resistance in human multiple myeloma and
acute T-cell leukemia in vivo in a mouse xenogtraft model.
3 2018Med Sci Monit
2018;24:2550-2561.
Effects of Recombinant Circularly Permuted Tumor Necrosis Factor (TNF)-
Related Apoptosis-Inducing Ligand (TRAIL) (Recombinant Mutant Human
TRAIL) in Combination with 5-Fluorouracil in Human Colorectal Cancer
Cell Lines HCT116 and SW480
4 2016 Exp HematolEffects and mechanism of arsenic trioxide in combination with rmhTRAIL
in multiple myeloma
5 2015 Onco Targets TherGefitinib upregulates death receptor 5 expression to mediate rmhTRAIL-
induced apoptosis in Gefitinib-sensitive NSCLC cell line
6 2015 Clin LabNovel Molecular Regulators of Tumor Necrosis Factor-Related Apoptosis-
Inducing Ligand (TRAIL)-Induced Apoptosis in NSCLC Cells
7 2019 On submitEffects and mechanism of Bortezomib in combination with rmhTRAIL in
refractory multiple myeloma

CAR-T cell from Legend: LCAR-B38M
Zhao WH, J Hematol Oncol. 2018 Dec 20;11(1):141

CAR-T cell from Legend: LCAR-B38M
LCAR-B38M was composed of a human CD8 alpha signal peptide (CD8α SP),
BCMA-targeting domain consisting of two different VHHs (single-domain antibody,
clones VHH1 and VHH2), human CD8 alpha hinge and transmembrane domain
(CD8α hinge + TM), human 4-1BB cytoplasmic domain, and a human CD3 zeta
cytoplasmic domain (CD3ζ)
Zhao WH, J Hematol Oncol. 2018 Dec 20;11(1):141

Legend (LCAR-B38M) Study in XiAn
• Prior lines of therapy: 3±2
• ECOG: ≥2: 16%
• Cyclophosphamide: 300mg/m2
• Dose: 0.5×10e6/kg
• 57 patients treated
• ORR 88%
• sCR:68%
• CRS: 90%; ≥3= 7%
• mPFS : 15m
NCT03090659
Zhao WH, J Hematol Oncol. 2018 Dec 20;11(1):141

Zhao WH, J Hematol Oncol. 2018 Dec 20;11(1):141
Legend (LCAR-B38M)
hydrothorax

Exploratory trial of a biepitopic CAR T-targeting B cell
maturation antigen in relapsed/refractory multiple
myeloma
Jie Xua,1, Li-Juan Chenb,1, Shuang-Shuang Yanga,1, Yan Suna,1, Wen Wua, Yuan-Fang Liua, Ji Xu b, Yan Zhuangc, Wu Zhanga,
Xiang-Qin Wenga, Jing Wua, Yan Wanga, Jin Wanga, Hua Yana, Wen-Bin Xua, Hua Jiangc, Juan Duc, Xiao-Yi Dingd, Biao Lid,
Jun-Min Lia, Wei-Jun Fuc, Jiang Zhua, Li Zhue, Zhu Chena,2, Xiao-Hu (Frank) Fane,2, Jian Houc,2, Jian-Yong Lib,2, Jian-Qing
Mia,2, and Sai-Juan Chena,2
aState Key Laboratory of Medical Genomics, Shanghai Institute of Hematology, National Research Center for Translational Medicine, Ruijin Hospital
affiliated with Shanghai Jiao Tong University School of Medicine, 200025 Shanghai, China; bDepartment of Hematology, Jiangsu Province Hospital, First
Affiliated Hospital of Nanjing Medical University, 210029 Nanjing, China; cDepartment of Hematology, Changzheng Hospital, The Second Military
Medical University, 200003 Shanghai, China; dDepartment of Radiology and Nuclear Medicine, Ruijin Hospital affiliatedwithShanghai JiaoTong
University School of Medicine, 200025 Shanghai, China; and eNanjing Legend Biotech, 210008 Nanjing, China
Contributed by Zhu Chen, December 17, 2018 (sent for review November 19, 2018; review
Xu J, et al. PNAS, 2019 Apr 15
Legend (LCAR-B38M)

(A) LCAR-B38M was composed of a human CD8 alpha signal peptide (CD8α SP), BCMA-targeting domain consisting of two
different VHHs (single-domain antibody, clones VHH1 and VHH2), human CD8 alpha hinge and transmembrane domain
(CD8α hinge + TM), human 4-1BB cytoplasmic domain, and a human CD3 zeta cytoplasmic domain (CD3ζ) (see Materials
and Methods for details).
(B and C) Measurements of LCAR-B38M gene-modified T cells assessed by means of qPCR assay in peripheral blood of
patients treated with cyclophosphamide/fludarabine combination conditioning and three-infusion CAR T delivery (B) or
cyclophosphamide conditioning and one-infusion CAR T delivery (C).
CAR-T cell from Legend: LCAR-B38M
Xu J, et al. PNAS, 2019 Apr 15

Xu J, et al. PNAS, 2019 Apr 15

Xu J, et al. PNAS, 2019 Apr 15
Legend (LCAR-B38M)
17 patients
treated
Prior lines of
therapy: 4.6
15/17 response
--13 CR
--4/5 EM disease
progressed

• Progression-free survival (PFS) rates of 82.4% at 6 mo and 52.9% at 12 mo (Fig. 2F)
• The 1-y overall survival (OS) rate was 82.3% (Fig. 2G) Xu J, et al. PNAS, 2019 Apr 15

Xu J, et al. PNAS, 2019 Apr 15

Xu J, et al. PNAS, 2019 Apr 15

Research on the safety, tolerability, pharmacokinetics and
efficacy of autologous CAR-BCMA T cells (CT053) for relapsed
and/or refractory multiple myeloma
Unpublished data, only for academic communication

CT053: Fully-human BCMA CAR-T Therapy
Size exclusion chromatograms of anti-BCMA antibodies in scFv_Fcform
High Percentage of Monomer Ratio of CT053 scFv

Potent in vivo Antitumor Activities of CT053 CAR T

CT053 CAR-BCMA T Study Design
Screening
Lymphodepletion
CAR-BCMA T manufacturing ( ~14 Day)
Infusion
F: fludarabine
C: cyclophosphamide
W: week
M: Month
Apheresis
Baseline
ICF
F+C
D-5 ~ -3
D0
W2 W4 W8 W12 M4 M5 M6 M9 M12 M18 M24W1
Main follow-up period Follow-up period
Treatment

Key Eligibility Criteria
• 18 -79 years of age
• Relapsed and/or refractory myeloma after at least 2 prior standard lines of therapy
• Subjects must be positive for BCMA per flow cytometry analysis or pathological exam.
• Estimated survival time > 12 weeks
• Have measurable disease on study entry
• ECOG performance status of 0-2
• WBC ≥ 1.5×109/L and PLT ≥ 45×109/L; serum creatinine ≤ 1.5 ULN; ALT ≤ 2.5 ULN,and AST ≤ 2.5 ULN

CT053 CAR-BCMA-T Cell Infusion
◼ Cell infusion dose in 24 patients: 0.5 – 1.8 ×108 transduced T-cells
✓ 1st patient: 0.5 ×108 cells (0.86 ×106/kg)
✓ 2nd patient: 1.8 ×108 cells (1.98 ×106/kg)
✓ 17th patient: 1.0×108 cell (2.04×106/kg)
✓ 21 patients: 1.5 ×108 (1.94-3.57×106/kg)
◼ Infusion was finished within 2 – 20 min
◼ No infusion related reactions were reported
◼ Second infusion:
✓ Pt 2 received the 2nd dose infusion 2.0×108 cell
✓ Pt 5 received the 2nd dose infusion 1.5×108 cell
✓ Pt 4 received the 2nd dose infusion 1.5×108 cell

Subjects(N=24) Without EM infiltration(N=13) With EM infiltration(N=11)Age (year)* 60.2 (38.5-70.0) 56.3 (39.5-67.2) 63.4 (38.5-70.0)Male/Female 13/11 7/6 6/5
Body Surface Area (m2)* 1.7 (1.3-2.1) 1.7 (1.4-1.9) 1.6 (1.3-2.1)
Time since diagnosis (year)* 3.5 (0.3-10.8) 4.3 (1.1-10.8) 2.9 (0.3-5.9)
IgG λ/IgA κ/λ light chains/IgA λ/IgG κ 12/6/2/2/2 7/3/1/1/1 5/3/1/1/1
ECOG
0-1 16 (66.7%) 10 (76.9%) 6 (54.5%)
2 6 (25.0%) 3 (23.1%) 3 (27.3%)
3 2 (8.3%) 0 (0.0%) 2 (18.2%)
ISS
I 4 (16.7%) 2 (15.4%) 2 (18.2%)
II 11 (45.8%) 4 (30.8%) 7 (63.6%)
III 9 (37.5%) 7 (53.8%) 2 (18.2%)
BCMA positivity (%)* 91.3 (30.4-99.8) 90.5 (58.5-99.8) 95.7 (30.4-99.5)No. of prior regimens excluding bridging therapy 4.5 (2.0-12.0) 6.0 (3.0-12.0) 4.0 (2.0-8.0)
PIs 24(100%) 13(100%) 11(100%)
IMiDs 22(91.7%) 13(100%) 9(81.8%)
PIs and IMiDs 22(91.7%) 13(100%) 9(81.8%)
Monoclonal antibody 5(20.8%) 4(30.8%) 1(9.1%)
Stem cell transplantation 10(41.7%) 7(53.8%) 3(27.3%)
Patient’s Characteristics

Treatment related AE
Number of
subjects (%) Grade 1 Grade 2 Grade 3 Grade 4 Grade 5
Cytokine release syndrome(CRS) 15(62.5%) 4 11 0 0 0
Fever 15(62.5%) 4 5 5 1 0
Neurologic toxicity*(NTX) 2(8.3%) 1 0 1 0 0
Infections and infestations 6(25%) 1 0 5 0 1
Hematological toxicity 23(95.8%) 5 9 24 46 1
Lymphocyte count decreased 18(75%) 0 0 1 17 0
White blood cell count
decreased 21(87.5%) 0 1 7 13 0
Platelet count decreased 13(54.2%) 4 3 2 4 0
Neutrophil count decreased 19(79.2%) 0 3 5 11 0
Full blood count decreased 1(4.2%) 0 0 0 1 0
Anaemia 9(37.5%) 1 1 7 0 0
Coagulopathy 2(8.3%) 0 1 1 0 0
Bone depression 2(8.3%) 0 0 1 0 1
Adverse Events of Special Interest
& Death resulting by neutropenic infections, myelosuppression and disease progression at Day 25th after infusion
*Treatment related AEs include lymphodepletion-related AEs or CAR-BCMA T-cell infusion-related AEs.
# One subject experienced both grade 3 NTX and grade 2 CRS

Efficacy Assessment
• Efficacy follow-up: 295 days (119 – 509)
• ORR is 87.5% in 24 pts who received cell infusion
• Outstanding efficacy was observed even with low dose: 0.5×108 (VGPR) persisting 378+ days, and
achieved CR on day 437, sCR on day 502.
• CR/sCR: 70.8% (17/24); VGPR and above: 83.3%(20/24)
CG6002-01001: 0.5×108 CG6002-01002: 1.8×108 CGZ001-61007: 1.0×108
• 5/6 PD subjects had baseline EM disease.
Data cut-off: 28Feb2019

Expansion and Persistence of CAR-T cells
• Detectable 1~7 days after infusion
• Peaked on 7~21 days, with the
lowest peak value at 1.5×104
copies/µg gDNA and the highest at
4.5×105 copies/µg gDNA
• Persistence at least 21~375 days
CAR T copies in subjects who experienced PD and received the second dose

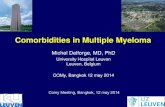
Clinical Efficacy on Extramedullary Plasmacytoma
Day 1 after CT053 treatment Day 5 after CT053 treatment Day 6 after CT053 treatment
Pt8: Male, 65yrs. MM(λ type).
Achieved CR at week 4.
lesion 2
lesion 1
lesion 2 lesion 1
lesion 2lesion 1

Lesion 1
Lesion 2
New Lesion(no neoplasm exist at base line and on week10, appear in M4, disappeared 2w thereafter)

Summary
The patients had worse clinical condition (ECOG 2/3 in 33.3% patients; 46%
with EM disease) when compared to patients in other BCMA-CAR T studies
24 subjects with R/R MM infused 0.5 - 1.8×108 CT053 cells, the dose in the 1st, 2nd
and 17th cases was 0.5×108, 1.8×108 and 1.0×108 CAR T-cells, respectively and the
other 21 subjects received a dose of 1.5×108 transduced T cells.
➢ CT053 CAR BCMA T cells conferred tolerable safety profiles (No grade 3
or higher CRS was observed)
➢ Sufficient CAR T-cell expansion and persistence observed
➢ 87.5% ORR; 83.3% of VGPR and above; 70.8% CR/sCR
Data cut-off: 28Feb2019

The safety and efficacy of autologous CAR-BCMA T cells
(CT053) for relapsed and refractory multiple myeloma
Phase I & II trial
PI: Wenming Chen
Approved by CFDA

Thank you!