
Clinical Services Plan for Geriatric Medicine - HNHB LHIN · June 30th, 2009. Dear Sir/madam Re:...
86
June 30 th , 2009 Dear Sir/madam Re: Clinical Services Plan for Geriatric Medicine Please find enclosed the proposals from the geriatric Planning Advisory Group. We have had numerous meetings in large and small groups and in the end submit four different but related proposals. We chose to submit like this because we do not feel that we have the resources to provide comprehensive Geriatric Services LHIN wide at this point. Background To explain our situation we would like to provide some background. Geriatrics is a essentially a specialty that deals with the care of frail older adults. Geriatricians provide comprehensive assessments of older adults and assess medical problems, cognition, mood, function, supports and risk factors. Traditionally geriatricians work in teams of health care professionals that would include nurses, occupational therapists, physiotherapists, speech language pathologists, dietitians, pharmacists and social workers. Comprehensive care plans are developed in consultation with these various health care professionals. In Ontario, Geriatricians were funded thorough Regional Geriatric programs. There are five, each attached to a Medical school. They were funded in this order Hamilton, Toronto, Ottawa, London and Kingston. When they were funded, the monies were given to hospitals. So traditionally Geriatricians were attached to hospitals and were seen as tertiary care services like cardiac surgery or burn units. So, as a result, geriatricians worked almost exclusively in hospital in consult services, inpatient assessment units and/or outpatient departments. Today we see the legacy of that funding situation. In this LHIN 80% of Geriatricians are located in Hamilton, working in hospitals and for the most part they are all attached to the university. There is currently no funding in place for community geriatricians. There are some services given out side of Hamilton like Greater Niagara General Hospital because the hospital has provided funding for this program. Currently, Geriatricians work in these programs where resources are provided. They have no way of expanding these programs to work with primary health teams, to increase outpatient clinics, to expand outreach services or to provide specialty clinics like falls, dementia or continence clinics because they have no resources. Geriatricians can only work where resources are provided and stop working if these programs or services are withdrawn.
Transcript of Clinical Services Plan for Geriatric Medicine - HNHB LHIN · June 30th, 2009. Dear Sir/madam Re:...

June 30th, 2009
Dear Sir/madam
Re: Clinical Services Plan for Geriatric Medicine
Please find enclosed the proposals from the geriatric Planning Advisory Group.
We have had numerous meetings in large and small groups and in the end submit four different but
related proposals. We chose to submit like this because we do not feel that we have the resources to
provide comprehensive Geriatric Services LHIN wide at this point.
Background
To explain our situation we would like to provide some background. Geriatrics is a essentially a specialty
that deals with the care of frail older adults. Geriatricians provide comprehensive assessments of older
adults and assess medical problems, cognition, mood, function, supports and risk factors. Traditionally
geriatricians work in teams of health care professionals that would include nurses, occupational
therapists, physiotherapists, speech language pathologists, dietitians, pharmacists and social workers.
Comprehensive care plans are developed in consultation with these various health care professionals.
In Ontario, Geriatricians were funded thorough Regional Geriatric programs. There are five, each
attached to a Medical school. They were funded in this order Hamilton, Toronto, Ottawa, London and
Kingston. When they were funded, the monies were given to hospitals. So traditionally Geriatricians
were attached to hospitals and were seen as tertiary care services like cardiac surgery or burn units.
So, as a result, geriatricians worked almost exclusively in hospital in consult services, inpatient
assessment units and/or outpatient departments. Today we see the legacy of that funding situation. In
this LHIN 80% of Geriatricians are located in Hamilton, working in hospitals and for the most part they
are all attached to the university. There is currently no funding in place for community geriatricians.
There are some services given out side of Hamilton like Greater Niagara General Hospital because the
hospital has provided funding for this program.
Currently, Geriatricians work in these programs where resources are provided. They have no way of
expanding these programs to work with primary health teams, to increase outpatient clinics, to expand
outreach services or to provide specialty clinics like falls, dementia or continence clinics because they
have no resources. Geriatricians can only work where resources are provided and stop working if these
programs or services are withdrawn.

Geriatricians are anxious to provide services outside of Hamilton and outside the traditional silos where
they have been forced to work for decades now. Geriatricians have been communicating together for
months in anticipation of this proposal. In addition to inviting our own membership, we also invited key
stakeholders to help us with our planning. In collaboration with our partners we developed a Discussion
Document that addressed demographic, utilization and some preliminary ideas on specialized geriatric
service delivery models. We then used a Delphi consensus process to determine what areas we would
like to develop as a priority. Then we met for a day workshop with an external facilitator (Dr. C. Powell)
and developed four priority areas;
1. Family Health teams – shared care model 2. Outreach – “atHome” program 3. Transitional care program 4. Video conferencing (via OTN)
At the strategic workshop we divided into teams and developed proposals for each of these areas. We wanted to focus on programs that could be applied throughout the LHIN in cities, small towns and rural areas. We wanted to assess people in their own environment, in their own homes or in their family doctors’ offices. Unlike traditional tertiary care services that are located in large teaching hospitals, these services go to where the patient is, to provide services where the person is, when they need it and what they need. Rather then propose a centralized intake process, we recommend the best approach will be to have multiple access points for referrals. Each portal will employ a standardized approach using common care processes and common screening and assessment forms. This will facilitate improved overall communication across programs, reduce system redundancy and allow for data to be collected so evaluation and benchmarking activities can be initiated. These proposals do not replace existing services. They build on existing services and attempt to enrich them and provide a focus and integration of services that is currently lacking. Geriatricians want to work with CCAC, Family health teams and Community health Centres. These four proposals represent our efforts to expand specialty services throughout the LHIN. We have provided a common template for sections 2 for the four proposed areas. While we have provided four different proposals to expand specialty services we recognize more needs to be done and obviously we would be happy to meet with your staff to discuss an overall strategy for expanding specialty services throughout the LHIN. The main limitation to this right now is the lack of specialist geriatricians, nurses and allied health care professionals to work in these teams. No matter what the strategy, it will have to be gradual and incremental. So these proposals represent the strategies offered by the Regional Geriatric Program central to expand these specialty services throughout the LHIN. Sincerely Dr. W. Molloy Chair, Regional Geriatric Program central David Jewell Director, Regional Geriatric Program central
Re: Geriatric Clinical Services Delivery Model Diagram for HNBH LHIN
This diagram provides an overview of our current and future service models
Current Inpatient services – largely Hamilton based
Geriatric Consult Service
Geriatric Rehabilitation and Assessment
Current Outpatient Services – largely Hamilton based
Geriatric Outpatient Clinic
Geriatric Outreach
Geriatric Day Hospital
This new HNHB model links the acute care system with 4 new model enhancements:
1. Transitional care – expedited discharge with strong prevention of readmission program elements.
2. Primary Care – Development of a shared care model between primary care and geriatrics. This will provide increased assessment and treatment expertise among physicians and allied health in Family Health Teams. Transitional care will link with primary care.
3. atHome Program – This geriatric outreach service will be highly responsive to clients in emergency, identify those at risk in the home and put in place prevention measures to help improve independent living. This program will link closely with Transitional care and Primary – shared care model.
4. Video conferencing – will improve clinical access to services. Video conferencing will begin to address lack of access to clinical services in rural areas. A number of geriatricians have already begun to link with Family Health Teams and other sites.

Geriatric Clinical Services Delivery Model HNHB LHIN
EDUCATION ‐ TRAINING – CAPACITY BUILDING
LOW RISK
HIGH RISK
Admission to Acute Care
ACUTE CARE
Geriatric Inpatient Consultation
Geriatric Assessment & Rehabilitation
Units
Transitional Care
CCAC‐based APN
transitional coach to
provide patient/caregiver
self‐care training
Specialty Geriatric Community Services
atHome Program: Outreach Team
Home Visits
Inpatient & Outpatient Geriatric
Assessments
Training/Capacity Building
Video
Conferencing
Outpatient Geriatric Assessment clinics & Day Hospitals
PRIMARY CARE (FHTs & CHCs)
Shared Care Model
LOW Vulnerability HIGH Vulnerability Frailty Severity
Outpatient Geriatric Assessment & Consultation
Outreach Team Home Visits


HAMILTON NIAGARA HALDIMAND BRANT
LOCAL HEALTH INTEGRATION NETWORK
CLINICAL SERVICES PLANNING PROJECT
At Home Geriatric IP Outreach
PLANNING ADVISORY GROUP MEETING GUIDE

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
1. Complete Template #1. Describe the strengths and challenges within the existing health care system in addressing population health care needs for the PAG’s patient/client population. Primers for discussion: ‘Summary of Community Values and Preferences’ (Appendix A), ‘Criteria for PAG Service Delivery Models’ (Appendix B) and ‘Guiding Principles for PAG Service Delivery Models’ (Appendix C).
Template #1: Strengths and Challenges within the Current System in Addressing Population Needs PAG Name:
At Home Program
Outreach Specialized Geriatric Services for Frail Older Adults
PAG Facilitator
Dr. W. Molloy, Mary‐Lou van der Horst
Strengths and Challenges
Introduction
This proposal describes a LHIN wide program that will provide quicker access to Geriatricians, geriatric assessments and coordinated specialized
geriatric services. The geriatric assessments use a risk‐based management model and standardized tools and processes. In addition, for frail older
adults who cannot attend geriatric assessments within the outpatient settings due to health and functional issues or who are at risk of maintaining
themselves/their health will be offered geriatric assessments within their own home.
Goal: The goal is to keep these frail older adults at home and help them maintain their independence, reduce unnecessary admissions to
acute care, and avoid premature admissions to long‐term care.
Innovative: The atHOme program is distinct from and complementary to current services like FHTs and CCACs operating in the community.
It offers timely and efficient access to complex services for complex patients. Highly skilled teams of health care professionals are trained to
deal with complex frail older adults. It can be accessed by doctors, CCACs and other community agencies who have health and functional
concerns about community‐dwelling frail older adults.
FINAL: At Home Geriatric Outreach 7 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
Urban and Rural Settings: The atHOme program is designed to work in urban and rural settings. It is an excellent model for rural settings
and small towns.
Comprehensive Geriatric Assessments: Evidence‐Based and Knowledge Informed
Comprehensive Geriatric Assessments that use standardized tools and processes have been shown to reduce mortality, morbidity and reduce costs
when used appropriately in the care of frail older adults. This program targets a specific group of older adults – those who are frail and vulnerable
to changes in their health ‐ which represent a substantial portion of people over the age of 85 and to a lesser degree those over the age of 65.
At Risk Frail Older Adults
Typically these patients will be frail, elderly, and have some of the following risk criteria:
Multiple admissions or ER visits (frequent users), falling, non‐compliant with medications/polypharmacy, poor nutritional status due to not eating/food selection/lack of food, refusing help in the home, poor ambulation, confusion, incontinent of bladder/bowels, and at risk of hospitalization and/or premature institutionalization (long‐term care).
In the Home Assessments
The first step is a telephone screening conversation by an advanced practice nurse to determine if this person meets the criteria for an in‐home
assessment. If the person fits the criteria, the urgency is assessed next. The urgency will be ranked from low to high and a home assessment
arranged based on this ranking. All Home Assessments will use standardized assessment measures including history, medications, systems review,
physical exam, psychosocial assessment, functional assessment, cognition, mood, home safety/environment, and risk assessments. The assessment
will be client‐focused and culturally sensitive. This assessment will be recorded electronically and will be part of a larger data base. The next step is
a Case Conference with the interprofessional/ interorganizational team and the Geriatrician. Less complex cases may not be seen by the
Geriatrician. More complex cases will be reviewed and a determination made if a home visits needed or if the person can be seen in the outpatient
setting.
FINAL: At Home Geriatric Outreach 8 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
The Inter‐professional and Inter‐organizational Team
This inter‐professional and inter‐organizational team will have nurses and other health care providers such as occupational therapists and physical
therapists. We would also include Community Care Access Centre (CCAC), Family Health Team (FHT) and Community Health Centre (CHC) staff on
the team to facilitate interorganizational collaboration and speed up turnaround times for home supports. The patient, family and caregivers are an
important and critical part of this team. We also will consult with speech language pathology, dietitians, pharmacists and other health care
providers based on the care needs. Technology will be used to promote interorganizationl collaborative care. For example, if there are geographical
barriers, primary care providers will be invited to attend care conferencences via videoconference.
Network of Geriatric Services
The atHome Program will be part of the Regional Geriatric Program‐Central which encompasses a wide range of geriatric services including
Geriatric Assessment Units, Geriatric Rehabilitation, consultation services, outreach teams, outpatient clinics, and day hospital programs. This
program will interface with existing programs such as Adult Day Programs, Community Support Services, various community associations and
governmental associations such as Veterans Affairs, Hospices, Palliative Care, and cultural groups.
Education
This program offers excellent opportunities for all health care providers to learn from each other and gain continued learning through the Regional
Geriatric Program – Central’s linkages with McMaster University.
Follow Up
Follow up will be done by CCAC and primary health teams. The atHome Team will remain available for consultation and follow‐up support.
FINAL: At Home Geriatric Outreach 9 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
2. Complete Template #2: Describe the leading factors that are most likely to increase or decrease the demand for health care by the PAG’s patient/client population by 2013. For each of these factors, indicate whether it will have a modest or significant impact on the future demand for health care. And, list factors that may influence the demand for care beyond 2013
At Home Geriatric Outreach Program
As of 2006, the HNHB LHIN was home to over 200,000 seniors aged 65 years and older; the largest number of seniors of all LHINs. In 2006,
seniors 65 years of age and older represented 15.8% of the total HNHB LHIN population, compared to 13.6% for all of Ontario.
Twenty‐nine percent (29%) of seniors aged 65+ live alone in HNHB communities, higher than the provincial average of 27%. Within HNHB the highest proportions of seniors living alone are found in St. Catharines (33%) and Brantford (33%) and the lowest proportion in Wainfleet (19%).
Seniors living alone may be at greater risk of social isolation. The lack of social support among the elderly contributes to poor health status and the need for formal and institutional care.
Approximately 27.7% of seniors in the HNHB LHIN live alone (See Table 2). Seniors living alone may be at greater risk of social isolation. The
lack of social support among the elderly contributes to poor health status and the need for formal and institutional care. i A recent Statistics
Canada studyii demonstrated that the vast majority of seniors remain in the community as their health care needs increase. Between 1981‐
2001 the proportion of Canadians aged 65+ living in health care institutions remained at about 7%; in 2001, approximately one‐third of
Canadians age 85+ lived in an institutional care setting. Among seniors living in the broader community, the Ministry of Health and Long‐
Term Care estimates that relatives, friends and volunteers provide about 80% of support to seniors with needs.
The majority of seniors that live in the HNHB LHIN live within Hamilton and Niagara (See Figure 1). In terms of absolute numbers, Hamilton
and Niagara are each home to over 74,000 seniors 65 years of age and older, and together represent 72% of the total HNHB LHIN population
over 65 years of age.
Significant impact
on future demand
for health care
FINAL: At Home Geriatric Outreach 10 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
At Home Geriatric Outreach Program
Population aging presents significant challenges to the health care system in Ontario. Not the least of these is the fact that 82% of seniors
have one or more chronic health condition and 43% have three or more chronic conditions. This latter group is at risk of becoming frail.
Frailty, characterized by complex bio‐psycho‐social and functional problems, is associated with increased health system usage and puts
seniors at risk of loss of the capacity for independent living and lowered quality of life (Wolff et al, 2002). Within the aging demographic,
frailty may be the fastest growing issue across the province and particularly in northern regions and outside high‐density urban areas
(Manuel & Schultz, 2001).
The ageing of the Baby Boomers will be the main driver of the increased number of people who are 65 years and over. These numbers will
increase by 50% over the next 10‐15 years. Improved life expectancy will also see the numbers of people aged 80 years and over double
during the next two decades. As we live longer we are likely to see an increasing proportion of people with age related medical disorders
such as neurodegenerative disorders, depression and mental health problems (Hopkins & Hopkins, 2005).
A key contributor to the increase in severe disability experienced by those over 80 is growth of neurological conditions, which result in
disorders of memory, cognition, behaviour, motor and sensory functioning, mobility and balance. These neurodegenerative diseases are
often slowly progressive and they have not, so far, been amenable to prevention or delayed onset, as have other disorders such as heart
attacks and stroke. While there is no strong evidence that the incidence of these diseases is changing, their prevalence is rising rapidly as
more people are living longer. We can expect the systemic disorders to be overtaken by neurodegenerative diseases as the major cause of
death in older people during the coming decades and also the major cause of severe disability.
People will come out of hospital with the capacity to get better and it will be important that the health system has a strong focus on
restorative and preventative measures. The demand for rehabilitation and other services following these acute events will certainly increase.
In response to these trends we may benefit from a hospital sector that plays a greater role in preventing acute admissions to hospitals and
delivers more services in the community.
FINAL: At Home Geriatric Outreach 11 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
At Home Geriatric Outreach Program
The Dementia Epidemic: In Ontario, dementia is the leading cause of disability for those over 60 years of age causing more years lived with disability than stroke, cardiovascular disease and all forms of cancer (Alzheimer Society of Ontario, 2007). It is expected that by 2010, 175,000 Ontarians will be living with dementia; this will increase by almost 127% by 2020 (Hopkins & Hopkins, 2005). Table 1 presents the estimated incidence of dementia in the HNHB LHIN for 2006. Ageing demographics will have a significant impact on human resource planning and development in all professions working in many health
care contexts across the circle of care (McKnight et al. 2003). Providing care to this expanding population of frail seniors requires both an
increase in the numbers of care providers, capacity building across various health care sectors, and restructuring of how and where we
deliver care. Our skill sets require expertise in three broad competencies ‐ geriatrics, inter‐professional practice and inter‐organizational
collaboration.
Table 1: Estimated Incidence of Dementia in the HNHB LHIN, by County and Age Group, 2006.
Age Group
Geography 60‐64 65‐69 70‐74 75‐79 80‐84 85+
Total
(60+)
Brant 31 50 93 173 291 533 1,171
Burlington 45 73 134 238 391 667 1,548
Haldimand‐Norfolk 31 48 86 148 242 438 994
Hamilton 125 207 386 742 1,242 1,968 4,670
Niagara 121 204 378 704 1,201 1,997 4,605
HNHB LHIN 353 583 1,077 2,005 3,367 5,603 12,988
Ontario 2,984 4,872 8,578 15,146 24,486 42,003 98,069
Source: Statistics Canada, 2006 Census; Dementia Age Relative risk: 60 1%; 65 2%; 70 4%; 75 8%; 80 16%; 85+ 32%. Source:
Significant impact
on future demand
for health care
Significant impact
on future demand
for health care
FINAL: At Home Geriatric Outreach 12 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
At Home Geriatric Outreach Program
Competence in geriatrics is required because the clinical presentations of frail seniors are unique and include the ‘geriatric giants’ of
dementia, delirium, falls, continence and poly‐pharmacy. These often co‐exist in complex ways. Competence in inter‐professional practice is
required because the complexities of these clinical presentations are such that optimal care requires an interdisciplinary team. Inter‐
professional teamwork, as outlined in the recently published Health Force Ontario, Inter‐professional Care: Blueprint for Action (Oandasan &
Closson, 2007), is the care delivery method of choice in caring for frail seniors (Geriatrics Interdisciplinary Advisory Group, 2006). Finally,
competence in inter‐organizational collaboration is required because the management of frail seniors requires the sharing of care across
many organizational boundaries from primary and community based care to emergency and hospital‐based services.
Significant impact
on future demand
for health care
Advancement in technology and how we communicate with each other
Based on this aging population and HR challenges we need to develop e – health strategies such as video conferencing, maximize electronic
record sharing such as clinical connect, standardize all documentation processes to facilitate data collection, evaluation and reduce
redundant assessment practices that are a further burden on staff and patients and families. Common forms and tools will create more
effective practice and help different teams start communicating AS ONE. Common documentation will facilitate rapid and improved transfer
of information. Capacity building will be much easier and bench marking will be attainable.
Patients/clients need to assume more responsibility for their care. Work has been done using patient passports and best practice needs to
be implemented using principles from the chronic disease model, e.g., flag prevention measures, telephone follow up to reinforce messages
etc.
Video conferencing is now being tested by geriatricians and office space has been secured. Geriatricians will be among a very small group in
the province of Ontario to actually use video conferencing for clinical purposes. We are just beginning to understand the full ramifications of
this technology.
Significant impact
on future demand
for health care
FINAL: At Home Geriatric Outreach 13 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
At Home Geriatric Outreach Program
How services are offered
As frail seniors decondition rapidly in hospitals e.g., loosing muscle mass, delirium, infections etc., it is imperative that services are designed
that prevent admission and re‐admission and help people live longer in their homes with a good quality of life. The specialty of geriatrics can
not tackle this problem single handedly. Using a collaborative model, we propose developing a shared care model with family health teams
and community health centres. Building expertise in geriatrics across the continuum with targeted specialist support will help multi‐
disciplinary groups identify seniors at risk. We need to equip primary care settings to be responsive to seniors at risk so they can provide
time sensitive support to hospital discharges or seniors presenting in emergency who can return home with expedited clinical support.
Having a flexible team that can provide outpatient and at home outreach services is critical. Many seniors in our LHIN live in isolated
situations and are at risk.
Best practice
We know that targeted care to frail seniors makes a difference in health outcomes. Evidence indicates that interdisciplinary teams on an
inpatient and outpatient basis is important. Comprehensive Geriatric Assessment targeted at frail seniors responds to immediate issues and
prevents other medical conditions from worsening. Home visits will improve overall functioning and help seniors live more independently.
Teaching seniors more about their health and how to manage their care more proactively is a integral part of the care process. Already, we
have positive results in the Transitional Care program through Dr. G. Heckman that shows teaching frail seniors is effective and helps them
stay out of hospital. Using communication strategies like providing patients a copy of their treatment plan, having them bring their patient
passport to all health care appointments is an important health information tool. This will introduce evidence based practice for meeting the
needs of aging population
Significant impact
on future demand
for health care
Significant impact
on future demand
for health care
Significant impact
on future demand
for health care
FINAL: At Home Geriatric Outreach 14 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
At Home Geriatric Outreach Program
What factors are expected to influence the demand for health care beyond 2013?
Practice of geriatric care is clustered in urban centres, primarily Hamilton
Rapidly growing older adult population with shortage of geriatric specialty trained health care professionals across all sectors of health care including primary
care and community.
Movement of older adults to retirement communities, often smaller towns with poorly established geriatric health services and limited family and
transportation
Finite number of Long Term Care beds
FINAL: At Home Geriatric Outreach 15 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
Template #3: Components of an Ideal Service Delivery Model
PAG Name
Geriatric Outreach Service: At Home ‐ Home First.
Geriatric outreach team for Frail Elders
PAG Facilitator
Dr. W. Molloy, Mary‐Lou van der Horst
Component of service delivery
model
Services associated with this component of the
model
Clinical and non‐clinical interdependencies (e.g.,
DI, lab, other programs/services, other PAGs) Linkages to community services
Health Promotion/Disease
Prevention
The referral is triaged immediately and risk of not
managing at home is assessed. For an at home
visit, the assessment is comprehensive covering
physical, emotional, social, psychological and
functional aspects. Assess‐ ment in the home
setting provides unique information of the person’s
current health and functional status and risk.
Interorganizational collaboration is important to
helping maintain the older adults staying in their
home Health issues that may become problematic
in the future are addressed. At the same time this
program promotes family education. If a person
cannot or will not come to an out patient clinic,
they will qualify for an outreach visit.
Direct link to:
- CCAC including Placement Coordination Services, Home Care services, Adult Day care , community association such as Alzheimer Society, Diabetes Association; FHTs/CHCs and family doctors, Labs; Outpatient clinics, other services
The assessment will provide a blue print for
action. Working within an interprofessional
interorganizational network, decisions will be
made about which services are most appropriate
so services are offered in a more timely and more
efficient way. As much as possible, promote one
stop shopping for the patient and family.
The assessment is comprehensive
and provides a portal to
appropriate services. The atHome
Program will function much like a
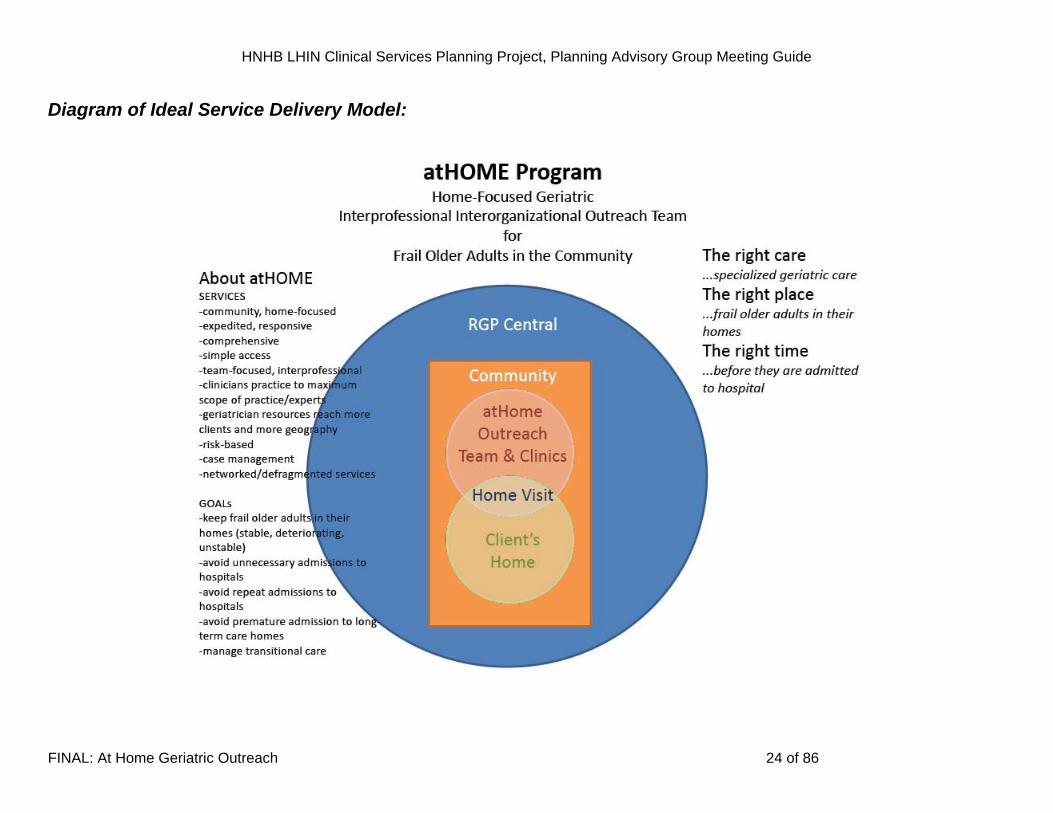
“traffic controller” so the patient
can get the right care in the right
place at the right time and ideally
in the home…This is client‐
centered and needs based…The
care plan will be comprehensive
and recom‐mends where the
person can get needed services
e.g. FHT, Cardiology, Day
Care…We maximize links to all
community services;
Community Support agencies :
‐ MS, CNIB, Meals on Wheels, Life
line, Catholic Family Services,
Parkinson’s Society, faith‐based
organizations, etc
FINAL: At Home Geriatric Outreach 16 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name
PAG Facilitator
Geriatric Outreach Service: At Home ‐ Home First. Dr. W. Molloy, Mary‐Lou van der Horst Geriatric outreach team for Frail Elders
Component of service delivery Services associated with this component of the Clinical and non‐clinical interdependencies (e.g.,
model model DI, lab, other programs/services, other PAGs) Linkages to community services
Primary Care/prehospital care
This program responds to primary care and keeps
the focus at the primary care level and out of
hospital. It aims to keep people in the community
and use community based services. If the person
does not have a family doctor, they can be referred
from a walk in clinic. It links directly with CCAC and
can take referrals from CCAC case managers
directly. In fact, the intent is to take referrals from a
variety of access points to maximize accessibility
such as family doctors, other programs, community
agencies, self‐referral for those who don’t have
family doctor, etc. Using a common triage and
screen ‐ing process and assessment tools, patients
can be referred from different programs – all using
the same documents and processes of care.
Patients have access to interdisciplinary teams (OT,
PT, SLP,) through family health teams and
Community Health Centers. Referrals will be
accepted for those who don’t have family doctor’s.
The people in the home (care‐giver network) now
become involved directly in the care planning
process.This program is linked to academics in
research and education. Should an admission occur
to hospital this info‐rmation is available in the
hospital data base.
The people in the home (caregiver network –
patient and family) now become involved directly
in the care planning process.
This program provides assessment in an
outpatient clinic for those who can access them
or in the home for those who can’t go to an
outpatient clinic. It promotes the interface of
community programs. It fosters inter‐
organizational collaboration with different
associations (Mental Heath, Veterans Affairs,
cultural organizations, Parkinson’s Society,
diabetes) so an integrated care plan can be
developed in the “home”. E Health transmits and
exchanges information with the different
programs and agencies. Each person in the circle
of care has access to this information.
In this program, the locus of care
is patient and family the home .
For patients receiving geriatric
assessments in their home, they
will have a chart in their home
listing the different care programs
and contact people in the care
team. If patients are receiving
home care and have a current
chart in the home, the atHome
Program will collaborate to ensure
they their information is part of
the cart. See non‐acute section
for further information.
This type of communication hub
creates home based linkage to
community services
FINAL: At Home Geriatric Outreach 17 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name
PAG Facilitator
Geriatric Outreach Service: At Home ‐ Home First. Dr. W. Molloy, Mary‐Lou van der Horst Geriatric outreach team for Frail Elders
Component of service delivery Services associated with this component of the Clinical and non‐clinical interdependencies (e.g.,
model model DI, lab, other programs/services, other PAGs) Linkages to community services
Hospital Care
– Acute and non‐acute
All of the information gained in the atHome
geriatric assessment and follow up in the
community will be available to the hospital. The
patient chart from the home will help facilitate
improved understanding of the assessment,
medications and overall community care plan. If
the patient needed elective surgery then a
comprehensive assessment would already be done
and it would be shared with the hospital staff. The
chart in the home would have the assessment data
in the chart and they can bring this with them to
the hospital if they are going for any assessment
e.g. Cardiology outpatients, ER visit. If the patient
arrives in the ER and has never been reviewed by
the outreach team, the ER doctors can connect
with the atHome team to get an urgent assessment
to allow for discharge thereby preventing
admission to ER. The atHome team will have the
capacity to do different levels of responses e.g. the
ER staff can do a trigger/urgent referral to allow
the atHome staff to organize an urgent referral
next day and prevent admission. If the person has
been seen, the ER team will contact the atHOme
team and arrange for immediate follow up. There
will be an urgent response in the home to prevent
The key is to have information to hospital staff
available so they are aware of all the assessment
data and the care plan.
“Share rather than duplicate”
Hospital staff:
The hospital staff can access a wealth of clinical
information so they will be aware of what was
happening in the community before the person
came to hospital. The broad network of
information is richer and more comprehensive
then the information that the CCAC alone can
currently provide. The atHome outreach team
will provide richer medical and health
information from dedicated specialist teams
directly to hospital staff. The hospital staff will
know what careproviders are involved in this
person’s care in the community. This will increase
linkages between the hospital team, transitional
care program and the community services.
The atHome Outreach Team is
available to the hospital staff to
provide support and information
about various geriatric and
community support services.
Because the CCAC and FHTs are
part of the atHome Team, they
can expedite such linkages and
work to assist the hospital to plan
for earlier return home. The
atHome Team is part of the larger
RGPc network of specialized
geriatric and related community
services.
FINAL: At Home Geriatric Outreach 18 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name
PAG Facilitator
Geriatric Outreach Service: At Home ‐ Home First. Dr. W. Molloy, Mary‐Lou van der Horst Geriatric outreach team for Frail Elders
Component of service delivery Services associated with this component of the Clinical and non‐clinical interdependencies (e.g.,
model model DI, lab, other programs/services, other PAGs) Linkages to community services
hospital admission.
The atHome outreach team
The atHome outreach team is the portal to
community services and a quick and easy access
point for patients to understand the geriatric and
community services. Linkage to CCAC for ongoing
care in the home is facilitated by the outreach
team. The team collaborates with the CCAC and
in hospital staff to provide the appropriate home
care services to facilitate discharge. Upon
discharge from the acute care setting the team
immediately follows up in the home to provide
for seamless transfer by enriching and
broadening the interface between the hospital
and community services. This will minimize the
risk of readmission to hospital and ER through
guidance on appropriate care approaches to frail
older adults and their geriatric syndrome and
chronic disease issues.
FINAL: At Home Geriatric Outreach 19 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name
PAG Facilitator
Geriatric Outreach Service: At Home ‐ Home First. Dr. W. Molloy, Mary‐Lou van der Horst Geriatric outreach team for Frail Elders
Component of service delivery Services associated with this component of the Clinical and non‐clinical interdependencies (e.g.,
model model DI, lab, other programs/services, other PAGs) Linkages to community services
Non‐acute Hospital Care
The team will link with in patient rehabilitation,
slow paced rehabilitation, complex continuing care,
palliative care, convalescent care, day hospital
programs when appropriate. Non acute services
available can also be accessed as appropriate.
People who have gone through these programs will
all be referred to this outreach team on discharge
to follow up in the community
The atHome Outreach Team is available to the
hospital staff to provide support and information
about various geriatric and community support
services that the patient has accessed and/or
currently using. Any Geriatric Assessment,
laboratory, test or services information that the
atHOme team has can be quickly accessed and
shared.
In this program the locus of care is
in the home so each person will
have a chart in their home listing
the different care programs and
contact people in the care team.
Teams members will use lap tops
in the home to fill out the
standardized assessment process
using reliable and validated
instruments. A copy of the
assessment and care plan is left in
the home to be accessed by family
and caregivers in the home. In this
way the information is directly
communicated.
FINAL: At Home Geriatric Outreach 20 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name
PAG Facilitator
Geriatric Outreach Service: At Home ‐ Home First. Dr. W. Molloy, Mary‐Lou van der Horst Geriatric outreach team for Frail Elders
Component of service delivery Services associated with this component of the Clinical and non‐clinical interdependencies (e.g.,
model model DI, lab, other programs/services, other PAGs) Linkages to community services
Post‐Hospital Care
If a person is discharged, then this team will have
access to hospital records to review the
investigations treatments etc. Nurses and
physicians on the teams will be able to determine
what happened during the hospital stay. A referral
to the Transitional Care program may be made.
If the older adult was a patient of the atHome
Program prior to admission and communication is
maintained during hospitalization/transition care,
care back to the community will be seamless and
simple.
If the older is newly referred to the atHome
Program, the Outreach Team will assist with
return home.
The atHome Outreach Team is
available to the hospital staff to
provide support and information
about various geriatric and
community support services.
Because the CCAC and FHTs are
part of the atHome Team, they
can expedite such linkages and
work to assist the hospital to plan
for the return home. The atHome
Team is part of the larger RGPc
network of specialized geriatric
and related community services.
The interorganizational
component of the team allows for
coordinated return home care and
services.
FINAL: At Home Geriatric Outreach 21 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name
PAG Facilitator
Geriatric Outreach Service: At Home ‐ Home First. Dr. W. Molloy, Mary‐Lou van der Horst Geriatric outreach team for Frail Elders
Component of service delivery Services associated with this component of the Clinical and non‐clinical interdependencies (e.g.,
model model DI, lab, other programs/services, other PAGs) Linkages to community services
Community‐based Acute Care
This team will triage assessments first over the
phone when the referral is made. The second step
is when the assessment is made in the home, the
team will determine if there is significant issues
that can be managed in the home with appropriate
assessment and treatment e.g. pneumonia,
congestive heart failure. cellulitis, to prevent
hospital admission. If necessary the person would
facilitate hospital admission to bypass emergency,
e.g., directly to the Geriatric Assessment unit or
palliative care or CCC. The team will determine the
level of urgency and develop an appropriate care
plan. For example, consider a person with
pneumonia. The physicians diagnoses, treats and
the person is followed by a nurse daily and may be
managed in the community. This program could
easily be integrated with the transitional care
program or assume responsibility for those patients
who finish with the transitional care program.
This service will link to community services as
appropriate and facilitate referrals to specialty
clinics. Ultimately we will determine which
patients can come to outpatients and which ones
will need in home assessment. This program
interfaces with all the other specialty Geriatric
services. This includes dementia clinics, falls
clinics, referrals to Osteo clinics etc
The atHome Outreach Team is
available to community
agencies/services to provide
support and information about
various geriatric and community
support services. Because the
CCAC and FHTs are part of the
atHome Team, they can also assist
with community linkages. The
atHome Team is part of the larger
RGPc network of specialized
geriatric and related community
services and knowledge about
these agencies.
FINAL: At Home Geriatric Outreach 22 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name
PAG Facilitator
Geriatric Outreach Service: At Home ‐ Home First. Dr. W. Molloy, Mary‐Lou van der Horst Geriatric outreach team for Frail Elders
Component of service delivery Services associated with this component of the Clinical and non‐clinical interdependencies (e.g.,
model model DI, lab, other programs/services, other PAGs) Linkages to community services
Community‐based Non‐Acute
Care
Please refer to information contained within the
following boxes above:
- Health promotion/disease prevention - Primary Care/prehospital care
Please refer to information contained within the
following boxes above:
- Health promotion/disease prevention - Primary Care/prehospital care
Please refer to information
contained within the following
boxes above:
- Health promotion/ disease prevention
- Primary Care/ prehospital care
FINAL: At Home Geriatric Outreach 23 of 86
HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
Diagram of Ideal Service Delivery Model:
FINAL: At Home Geriatric Outreach 24 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
FINAL: At Home Geriatric Outreach 25 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
FINAL: At Home Geriatric Outreach 26 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
FINAL: At Home Geriatric Outreach 27 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
Template #4. Assess and Describe the PAG service delivery model using the HNHB LHIN Criteria PAG Name: Geriatric Outreach Service: At Home Geriatric Outreach Team for Frail Elders
Domain Criteria Assessment Description
Strategic Fit Alignment with LHIN priorities
for health improvement
- Promotes Aging in Place - Promotes better health management of complex health issues (chronic diseases) of frail older adults who
are the largest proportion of health care system users - Decreases unnecessary visits to ERs - Decreases unnecessary admissions to hospitals - Expedites discharges from transitional care - Averts premature admission to long‐term care homes
Alignment with trends in
health care needs and system
transformation
- Addresses the increasing usage demands being placed on the health care system by older adult consumers (increased life expectancy and diseases associated diseases of longevity)
- Provides greater access by more older adults to finite and often geographically distant geriatric expertise (geriatrician) and related specialty services
- Promotes more efficient use of finite geriatrics services - Promotes a standardized approach to geriatric assessment of frail older adults across the LHIN - Promotes use of evidence‐based best practices in geriatric care - Provides access to a network of established geriatric and related services
Population Health Health status (clinical
outcomes & QOL)
- Improved management of frail older adults chronic diseases and their related functional and cognitive consequences
- Promoting “at home” geriatric services and “remaining at home” care, life enhancing strategies becomes the focus of care, ensures it is client‐centred, and deals with health issues that ensure the older adult’s quality of life is recognized and maintained
FINAL: At Home Geriatric Outreach 28 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name: Geriatric Outreach Service: At Home Geriatric Outreach Team for Frail Elders
Domain Criteria Assessment Description
Prevalence - Targeting frail older adults (25% of those older adults over 80) – largest consumers of health care - Burdened with diseases of longevity (chronic diseases and their debilating effects)
Health promotion & disease
prevention
- For frail older adults the focus is not so much on disease prevention or health promotion but rather on health maintenance (e.g, disease stabilization) and minimizing health declines (e.g, minimize functional losses)
- Promotes Aging in Place
Client‐focus - atHome has the client at the centre of its program model - all assessments are client‐focused and include the family/care givers - client, family and caregivers are included as part of the atHome Outreach Team - link with the Aging at Home Strategy
Partnerships - the atHome Program has an “interorganizational” focus and collaborates networks with existing community organizations and hospitals directly and through the Regional Geriatric Program Central
- FHTs and CCAC will be part of the core membership of the outreach team
System Values
Community Engagement
- the atHome Program has an “interorganizational” focus and collaborates with networks with existing community organizations and hospitals directly and through the Regional Geriatric Program Central
- FHTs and CCAC will be part of the core membership of the outreach team - Several atHome teams will be developed to serve a specific geographic area and will draw team
membership from the local area, connect with local organizations and resources
FINAL: At Home Geriatric Outreach 29 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name: Geriatric Outreach Service: At Home Geriatric Outreach Team for Frail Elders
Domain Criteria Assessment Description
Innovation
- The atHOme program is distinct from and complementary to current services like FHTs and CCACs operating in the community.
- It offers timely and efficient access to complex services for complex patients. - Highly skilled teams of health care professionals across the LHIN are trained to deal with complex frail older
adults. - It can be accessed by doctors, CCACs and other community agencies who have health and functional
concerns about community‐dwelling frail older adults - The atHOme program is designed to work in urban and rural settings. - It is an excellent model for rural settings and small towns. - It is based on a highly successful pilot project in the Niagara area with Dr. W. Molloy and a team of geriatric
specialty trained health care professionals. It is not offered anywhere else in the LHIN and funding on the Niagara pilot project is due to end.
Equity
- Will be available to urban, small town and rural communities - All communities will have access to specialized geriatric services and geriatricians - All frail older adult can qualify especially those who cannot leave their homes but are able to stay within
them - Anyone or any agency can refer, no requirement to have a family doctor
FINAL: At Home Geriatric Outreach 30 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name: Geriatric Outreach Service: At Home Geriatric Outreach Team for Frail Elders
Domain Criteria Assessment Description
Efficiency (operational) - Promoted through use of team format - Promoted through use of a triage decision‐making process - Promoted through case management and immediate handling of geriatric issues by the team and
appropriate referral of very complex cases to the Geriatrician (not all frail older adults need to see the Geriatrician but can benefit from the geriatric assessment provided by the team with appropriate referral to necessary services)
Access
- Improved access to Geriatricians and specialty trained geriatric health care professionals - Improved access for smaller towns and rural areas - Improved access through the use of technology such as video conferencing/assessments - Reach frail older adults within their homes who cannot go to a hospital outpatient clinic
Quality - Promote the use of standardized assessment tools and processes across the LHIN - Promote the use of evidence‐based and best practices in geriatric care - Hire only geriatric specialty trained health care providers - Timely service provision - Patient and family satisfaction
System Performance
Sustainability
- Able to implement very quickly due to the linkages within the system, knowledge of who and where the geriatric health care professionals are, linkages to the RGP and academia, linkages to FHTS and CCACs, linkages to many geriatric focused organizations
- Will require additional funding to sustain some of the roles within the atHome Outreach Team
FINAL: At Home Geriatric Outreach 31 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name: Geriatric Outreach Service: At Home Geriatric Outreach Team for Frail Elders
Domain Criteria Assessment Description
Integration
- Focus is on interprofessional and interorganizational collaboration - Focus is on expansion of geriatrician and geriatric specialty services to more frail older adults but through
better model design and system efficiencies - Promote consistent approach to assessment and care coordination for frail older adults
FINAL: At Home Geriatric Outreach 32 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
3. Complete Template #5. Describe the pre‐requisites, enablers and challenges to implementation of the ideal service model.
Template #5: Description of Pre-requisites, Enablers and Challenges to Implementation: Category Pre‐requisites Enablers Challenges
Policy/legislation Frail older adults do not need a family
doctor to access atHome Outreach
Program
LHIN
Regional Geriatric Program Central
Specialized Geriatric Services
CCAC
FHTs
Resources (e.g., human, fiscal, capital,
etc.)
Geriatricians
Geriatric specialty trained health care
professionals
Funding support for new positions
within the atHome Program,
Geriatrician services funding via
teleconferencing
Community readiness
Partners have collaborated on various
geriatric care issues in the past
Established geriatric services network
Services
Enhancement of geriatric outreach
services
RGPCentral
FHT
CCAC
LHIN
Niagara is only area in this LHIN that
has piloted a similar model
FINAL: At Home Geriatric Outreach 33 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
Partnerships/linkages
Partnerships and networks are well
established
Formalize outreach partnership
FINAL: At Home Geriatric Outreach 34 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
HAMILTON NIAGARA HALDIMAND BRANT
LOCAL HEALTH INTEGRATION NETWORK
CLINICAL SERVICES PLANNING PROJECT
Primary Care Family Health Team
PLANNING ADVISORY GROUP MEETING GUIDE
FINAL: At Home Geriatric Outreach 35 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
Complete Template #1. Describe the strengths and challenges within the existing health care system in addressing population health care needs for the PAG’s patient/client population. Primers for discussion: ‘Summary of Community Values and Preferences’ (Appendix A), ‘Criteria for PAG Service Delivery Models’ (Appendix B) and ‘Guiding Principles for PAG Service Delivery Models’ (Appendix C).
Integrating specialty geriatric services in primary care:
Background
Seniors represent the fastest growing age group in the Haldimand Norfolk Hamilton Brant, Local Integrated Health Network (HNHB LIHN)1. Volume and complexity of care is increasing. Primary care practitioners will provide the majority of care.
Family physicians have identified inadequate training, lack of confidence to manage frail elderly and limitations with the primary care model as barriers to provision of comprehensive geriatric care 2, 3. Limitations with the traditional organization of primary care include; focus on acute problems that are managed in short (average 7 minutes) unprepared visits, without consistent planned follow up4.
Specialized geriatric services in the HNHB LIHN are largely hospital based, located in urban areas (Hamilton, Niagara, Brantford and St. Catharines). Continuity and accessibility of care is fragmented between community and hospital settings, limited to urban areas and fraught by referral delays up to six months with limited emphasis on capacity building in the community.
Objective
This project proposes a shared care model that integrates specialized geriatric services within primary care. The target population is community dwelling seniors
at risk of functional decline, institutionalization and or hospitalization. This complimentary interface between primary care and specialized geriatric medicine
addresses limitations of accessibility, capacity and system organization barriers to provide the most appropriate care, when needed, in a familiar and accessible
location to seniors.
Integrating specialized geriatric medicine within primary care distributes specialized geriatric services throughout the LIHN.
A shared care approach extends the traditional role of the consultant to include capacity building among primary care providers.
FINAL: At Home Geriatric Outreach 36 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
Case finding, consistent use of standardized tools for comprehensive geriatric assessment combined with planned follow up visits that focus on evidence based
interventions addresses current organization limitations with respect to provision of comprehensive geriatric care in primary care.
Goal
The goal of this project is to support community dwelling seniors to maintain independence in their ‘home’. It is anticipated that targeting this vulnerable
population prior to functional decline will improve home and driving safety, decrease emergency department visits, increase average age of long term care
admission and decrease alternate level of care placement. The ultimate goal is to provide comprehensive geriatric care to all frail seniors in the HNHB LIHN.
Plan
The initial phase of this project focuses on multidisciplinary family health teams (FHTs) that are poised to provide inter‐professional, comprehensive team based
geriatric care for community dwelling frail elderly. This represents an innovative shift in family health team focus by integrating chronic disease management
into a population approach The next step will be to adapt the model to community health centres as well as non‐FHT group and solo practices according to
expertise and resources in these settings. The ultimate goal is to integrate and extend specialty geriatric services into all models of primary care throughout the
LIHN.
This project builds on the experience of a pilot study funded by the Department of Family Medicine, McMaster University5 in collaboration with the Hamilton
Family Health Team, Division of Geriatric Medicine, McMaster University, Alzheimer’s Society of Hamilton and Halton and the HNHB Community Care Access
Centre.
The goal of this pilot project is to: provide comprehensive geriatric care for frail elderly patients attending McMaster Family Health Team, Stone church Family
Health Centre, enhance expertise among primary care providers and family medicine residents, foster interprofessional collaboration among allied health care
providers and strengthen inter‐organizational partnerships with community resources.
Implications
Data gathered from this initiative will inform future programming and resource distribution based on the needs d. For example
References
1. Hospital Discharge data. Population Health Planning Database. Ontario Ministry of Health and Long-Term Care 2. Rueben DB et al. Restructuring primary care practices to manage geriatric syndromes. The ACOVE-2 intervention. Journal of American
Geriatric Society 2003; 51: 1787-1793.
FINAL: At Home Geriatric Outreach 37 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
3. Grimshaw JM, Shirran L, Thomas R et al. Changing provider behaviour. An overview of systematic review of interventions. Med Care 2001: 39:2-45
4. Kates N. Shared mental health care. The way ahead. Canadian Family Physician 2002; 48: 853-855 5. Feasibility of a collaborative care intervention between specialized geriatric medicine and family health team providers. 2008. Department of
Family Medicine. McMaster University. Project n progress
Template #1: Strengths and Challenges within the Current System in Addressing Population Needs Integration of specialty geriatric medicine services within primary care
PAG Facilitator: Dr. A. Moore, Dr. D. Cowan
Strengths Challenges
Strengths within the primary care system to facilitate this project include:
The target group of this proposal is frail older adults living in the community who are at risk of functional decline, hospitalization, and institutionalization in long term care homes.
This project proposes collaboration between specialized geriatric services (SGS)
and primary care. The initial phase proposes a shared care model with family
health teams. Subsequent stages will extend to community health centres, non
FHT group and solo practices with the ultimate goal of integrating SGS in
primary care across the LIHN.
A comprehensive and accessible primary care network in the HNHB LHIN. More than 95% of residents over 65 years of age have family doctors (significantly higher than the Ontario Average).
Concentrated core of FHT’s with multidisciplinary teams poised to provide appropriate care for the complex needs of community dwelling frail elderly (about 25% of family doctors work in family health teams).
Challenges within the primary care system to facilitate this project include: Volume
200,000 seniors, fastest growing age group, largest number of seniors in all 14
LIHN populations in Ontario.
Complexity
Seniors living with more than one chronic condition is increasing. 55% of
Ontarians suffer from two or more chronic conditions
Primary care challenges
Primary care practitioners provide the majority of care for elderly living in the
community. Family physicians have identified inadequate training, lack of
confidence and resources to manage complex frail elderly.
The traditional organization of primary care which emphasizes triage and
FINAL: At Home Geriatric Outreach 38 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
Minimal wait times to see Family Doctors vs specialized geriatric services
Family doctors provide the majority of care for the aged.
Relationship between geriatric medicine specialists and family doctors is an
opportunity for capacity building.
Highly dedicated staff
Patient satisfaction
Academic affiliations (some providers)
Opportunity for early intervention, health promotion, disease prevention, risk
reduction (eg vitamin D, exercise program, prevention of falls and social
isolation – risk of depression, medication management, driving and home
safety assessment) potentially leading to decreased emergency department
visits, alternate level of care placement and increased average age at
admission to long term care.
Opportunities for advanced planning (health, shelter, finances)
Early experience with shared care model integration of specialized geriatric
medicine in primary care (collaboration project between the Department of
Family Medicine, McMaster University, Hamilton Family Health Team,
Alzheimer’s Society, Community Care Access Centre).
patient flow, focuses on acute problems that are managed in short (average 7
minutes) unprepared visits without consistent after care. This practice is
incongruent with the needs of frail elderly.
Advanced care planning is minimally addressed in primary care and represents
the ideal opportunity for these discussions.
Wide variety of primary care models (family health teams, community health
centres, family health groups, fee for service, solo and group practices).
Delayed access to consultant services (geriatric medicine, rehabilitation
services, orthopedics, internal medicine).
Access to MRIs
Communication delays and gaps with specialists – Lack of shared health
electronic record
Access to marginalized immigrant, aboriginal, socially isolated and
disadvantaged seniors
FINAL: At Home Geriatric Outreach 39 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
Strengths within specialized Geriatric Medicine system to facilitate this
project include:
Highly dedicated staff
Academic affiliations (education and training health care professionals)
History of relationships with Family doctors
Hospital based services – full scope of medical programs available
Existence of partnerships; i.e., (HHSC, SJH, etc…)
Linkages and collaboration with community resources (CCAC, DVA, AS)
Challenges within the specialized geriatric medicine system to facilitate this
project include:
Inconsistent access to specialized geriatric medicine services
Largely hospital based, urban centred
Prolonged wait times to access specialized geriatric medicine services (up to 6
months)
High ALC rates
Lack of access to alternatives to hospital admission
Delayed access to consultant services (geriatric medicine, rehabilitation
services, orthopedics, internal medicine)
Access to MRIs
Communication delays and gaps – Lack of shared health electronic record
FINAL: At Home Geriatric Outreach 40 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
4. Complete Template #2: Describe the leading factors that are most likely to increase or decrease the demand for health care by the PAG’s patient/client population by 2013. For each of these factors, indicate whether it will have a modest or significant impact on the future demand for health care. And, list factors that may influence the demand for care beyond 2013
Template #2: Factors Most Likely to Increase or Decrease the Future Demand for Health Care:
Same as previous information in template 2
FINAL: At Home Geriatric Outreach 41 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
5. Complete Template #3. Describe the key components of an ideal service delivery model for the PAG’s target population.
Template #3: Components of an Ideal Service Delivery Model PAG Name
Integration of specialty geriatric medicine services within primary care
PAG Facilitator
Component of service
delivery model
Services associated with this component of the
model
Clinical and non‐clinical interdependencies
(e.g., DI, lab, other programs/services, other
PAGs) Linkages to community services
Health Promotion/Disease
Prevention
- Patient and family educational materials
Collaboration with case manager at CCAC regarded self efficacy for client in the home. Capacity building‐Educational events for the Family Health Teams
Patient Passport
Public Education
Professional Continuing Education - Resource specialists/CCAC case
managers on site - Needs assessment from clients and
families related to gaps in knowledge
- Referrals from outpatient and Home visits assessments to specialists, organizations and CCAC
- Case finding – Referrals from Health Team to specialists, continence advisors, bone density testing
- University Education
- Links to community groups e.g. Alzheimer Society
– First Link program,
counseling and
education, respite care,
CCAC, legal services,
seniors Drop‐In
centres
FINAL: At Home Geriatric Outreach 42 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name PAG Facilitator
Integration of specialty geriatric medicine services within primary care
Component of service
delivery model
Services associated with this component of the
model
Clinical and non‐clinical interdependencies
(e.g., DI, lab, other programs/services, other
PAGs) Linkages to community services
Primary Care /
Pre‐hospital Care
- This program provides service in the persons local community (FD office, CHC or home) care is locally accessible in a familiar setting.
- Supports self care and independent living at home as long as possible by treating medical social, psychological and functional needs
- Efficiency is maximized by working with local resource network (CCAC, Alzheimer Society, DVA, meals on wheels) no duplication of services, engagement of appropriate services.
- Given comprehensiveness of assessment this responds to diverse needs and individual client characteristics.
- Specialized Geriatric Services (e.g., newly proposed atHome Program’s geriatric outreach team to assist with diversion from hospital, ER admission) response to primary care request for
- Similar to out patient visit
- Links to current community services, back to the referrer and to new community support organizations
- e.g. other consultants, Alzheimer Society
CCAC (home care,
day care, LTC)
FINAL: At Home Geriatric Outreach 43 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name PAG Facilitator
Integration of specialty geriatric medicine services within primary care
Component of service
delivery model
Services component of the
model
Clinical and non‐clinical interdependencies
(e.g., DI, lab, other programs/services, other
PAGs) Linkages to community services
associated with this
clinic or home visit - Referrers are family physicians, CCAC,
etc. - Add mechanism to deal with patients
who do not have a family physician - Consult note has an educational
component and is shared with patient and family
Tele health is starting in some areas and will be expanded
Local geriatric clinics
Case management model so clients have a primary worker who is accountable for overall coordination of care
Visiting specialists - Eventual incorporation of physician
assistants
Acute Hospital Care
- Prevent admission to acute hospital care by increasing resources in the community
- Link with Transitional Care and proposed atHome geriatric outreach program to prevent readmission. Handoff from the transitional program
- Similar to out patient visit - Link with CCAC or other CHC services
- Link to RGPc network of geriatric service providers
- Link to proposal/atHome
FINAL: At Home Geriatric Outreach 44 of 86
HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name PAG Facilitator
Integration of specialty geriatric medicine services within primary care
Component of service
delivery model
Services
model
Clinical and non‐clinical interdependencies
(e.g., DI, lab, other programs/services, other
PAGs) Linkages services
associated with this component of the
to community
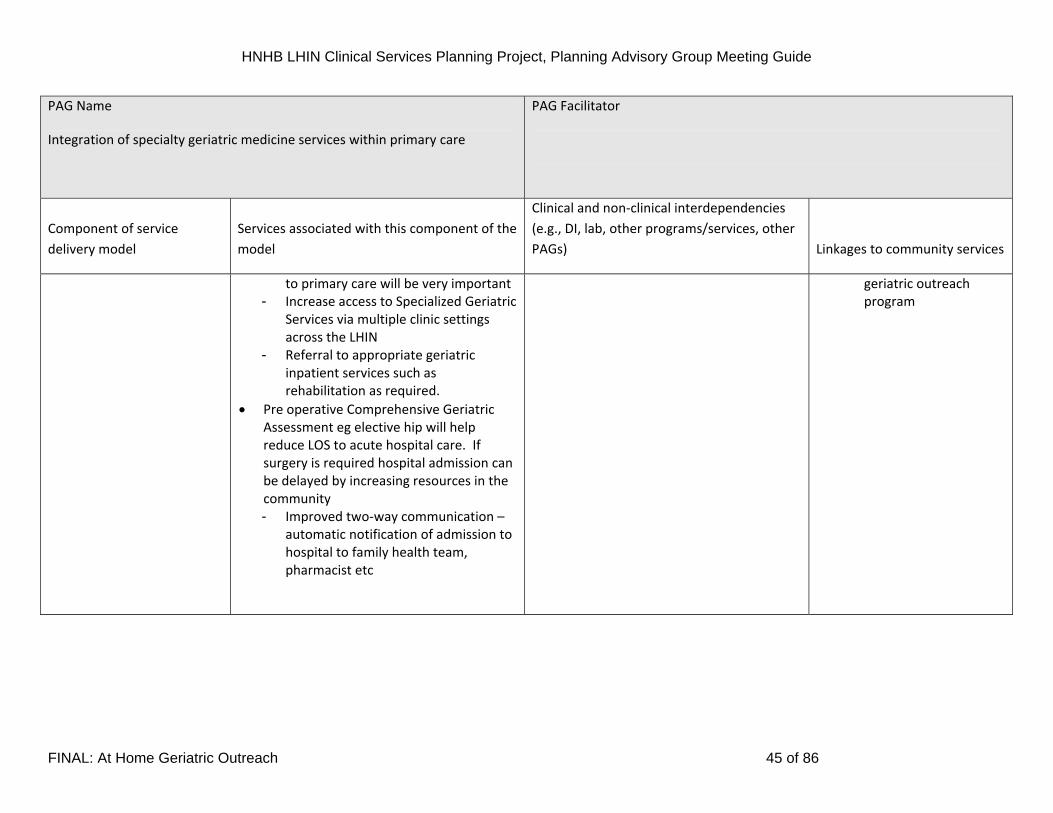
to primary care will be very important - Increase access to Specialized Geriatric
Services via multiple clinic settings across the LHIN
- Referral to appropriate geriatric inpatient services such as rehabilitation as required.
Pre operative Comprehensive Geriatric Assessment eg elective hip will help reduce LOS to acute hospital care. If surgery is required hospital admission can be delayed by increasing resources in the community - Improved two‐way communication –
automatic notification of admission to hospital to family health team, pharmacist etc
geriatric outreach program
FINAL: At Home Geriatric Outreach 45 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name PAG Facilitator
Integration of specialty geriatric medicine services within primary care
Component of service
delivery model
Services associated with this component of the
model
Clinical and non‐clinical interdependencies
(e.g., DI, lab, other programs/services, other
PAGs) Linkages to community services
Non‐acute Hospital Care
- Increase referrals to CCAC and community support programs to help people manage at home
- Hospital admission to rehab, geriatric assessment unit, day hospital, OT, PT, SLP, physiatrist
- Similar to out patient visit
- Discharge planning - Need for expedited
follow up on frail seniors
- Linkage with outreach/outpt programs/day hospitals
Post‐Hospital Care
- Support for “precarious discharge” patients (e.g. transitional care).
- Shared care model will offer a variety of clinical settings. High risk patients will be seen promptly. This will help reduce hospital and LTC admissions. This will also provide a discharge location as hospital teams will have more confidence that referrals will be picked up quickly for frail clients.
- Having multiple teams in various primary care settings is an enhancement of the current outreach program
- CCAC - Community support
services - Transitional care - Primary care
FINAL: At Home Geriatric Outreach 46 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name PAG Facilitator
Integration of specialty geriatric medicine services within primary care
Component of service
delivery model
Services associated with this component of the
model
Clinical and non‐clinical interdependencies
(e.g., DI, lab, other programs/services, other
PAGs) Linkages to community services
Community‐based Acute
Care / Community‐based
Non‐Acute Care
Patient Passport
Transitional care coach
Reintroduce links between family health team and CCAC case management
Enhanced community rehabilitation services
Inpatient assessment to identify patients who
need rapid follow‐up assessment
- CCAC and community support services
FINAL: At Home Geriatric Outreach 47 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
Diagram of Ideal Service Delivery Model: Integrated Specialty Geriatric Services Within Primary Care
FINAL: At Home Geriatric Outreach 48 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
Template #4. Assess and Describe the PAG service delivery model using the HNHB LHIN Criteria PAG Name – Integration of specialty geriatric medicine services within primary care
Domain Criteria Assessment Description
Strategic Fit Alignment with LHIN
priorities for health
improvement in response
to the demographic
imperative
- Decrease readmissions to hospital and visits to Emergency Departments - Improve Aging in Place - Improve access to services - Aligned with Chronic Disease Management model (self efficacy, self care, education) - Health promotion and prevention – target specific interventions such as memory loss,
depression, falls risk, confusion re: polypharmacy
Alignment with trends in
health care needs and
system transformation
- System of services, standard assessment forms and common care path approaches - Connecting individuals to services and improving collaboration amongst service providers - Will build on Best Practice - Use of shared care models - Access to other team resources
Health status (clinical
outcomes & QOL)
- Improved health and quality of life
Prevalence - targeting of frail older adults eg 25% of over 80’s
Population Health
Health promotion &
disease prevention
- Will target those at risk of falls, declining functional status, memory loss etc. Will build in strategies to help people learn more about their health so they take on more responsibility
-
FINAL: At Home Geriatric Outreach 49 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name – Integration of specialty geriatric medicine services within primary care
Domain Criteria Assessment Description
Client‐focus - Yes, bringing service to the client at home. Link with “aging at home” services - Use of circle of care approach, drawing in extended family, church and significant others - Will reach those who are marginalized due to physical disability or lack of transportation - Will have improved access to staff who speak different languages and will promote cultural
sensitivity based on client population characteristics
Partnerships - Pts, families and informal supporters - Multiple partnerships; - Community organizations – e.g. formal (CCAC) and informal (Alzheimer Society) - Sectors (primary care, acute care, community care) - Professions (OT, PT, SLP)
System Values
Community Engagement - Will be responsive to diverse needs and in corporate approaches to care and education that is appropriate
- Will improve proximity to care as lack of transportation will not exclude people from expert care - Teams in rural areas may need to be made up of a different mix of disciplines compared to
urban/academic centres. Rural areas will collaborate with a smaller set of organizations. We will be sensitive to the needs and strengths nested in each “community” area
- Resources will be more efficient if a “shared care” approach is used. Tremendous capacity building
- Ongoing focus groups will be required with senior citizens to help develop age friendly health promotion and prevention strategies and a review of how each “communities” constellation of services are working together. Care issues will be addressed through this ongoing feedback loop from consumers. The Hamilton Council on Aging (HCOA) is very diverse and has agreed to help develop this form of engagement with consumers of health care. The HCOA will help us link with other seniors groups in other areas of the LHIN
FINAL: At Home Geriatric Outreach 50 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name – Integration of specialty geriatric medicine services within primary care
Domain Criteria Assessment Description
Innovation - Enhancement of current service with outreach workers using a shared care model - This service will be responsive using different interventions such as telephone reminders,
assessing priority visits for those screened at high risk, assessing self efficacy skills etc -
Equity - Reach frail seniors who cannot travel to current service sites - Address travel/transit challenges (particularly in rural regions of the LHIN) -
Efficiency (operational) - Yes – shared care models - Screening by trained staff will allow specialists to see those at high risk while other patient
referrals may be managed by team members or referred to other community programs. This model will ensure those most at need will be seen by the specialist. This will also allow the specialist to see more patients at clinics when team members have already completed a battery of tests with a preliminary assessment in place
Access ‐ improved access through multiple clinic sites and home visits
Quality - Quality assurance component - Patient and family satisfaction
Sustainability
‐ This model can be implemented very quickly. All that is required is clinic space, access to appropriate
staff and basic infrastructure needs
System Performance
Integration
‐ This outreach model will promote more consistency of care with common approaches, common
assessment documentation and linkage with transitional care and primary care settings. Continuity of
care is known to improve overall patient care
FINAL: At Home Geriatric Outreach 51 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
6. Complete Template #5. Describe the pre‐requisites, enablers and challenges to implementation of the ideal service model.
Template #5: Description of Pre-requisites, Enablers and Challenges to Implementation: Category Pre‐requisites Enablers Challenges
Policy/legislation Policy will address access variation to
specialized geriatric services LHIN
wide
Agreements accountability, locus of
care
Criteria for intake
Model evaluation, definition of
outcome measures
Standardized assessment tools to
allow evaluation/audit LHIN wide
Developed –Hamilton Family Health
care mental health policy agreements
in alignment with current legislation
(Seniors health initiative in family
health team)
Large resource of evidence based
quality indicators (some tools
developed locally)
Adaptation to models of primary care
delivery across LHIN
Resources (e.g., human, fiscal, capital,
etc.)
Distribution of specialized geriatric
team based expertise from hospital
(urban) to community (urban and
rural)
Recruitment / Training physician and
allied health.
Financial and human resources
Interprofessional communication
Inter‐organizational communication
Well established hospital based
multidisciplinary geriatric teams
Highly skilled providers
Expertise in collaboration
CCAC
FHTs
Hospitals
Experience community based geriatric
multidisciplinary medicine teams (role
definition, scope of practice,
communication, electronic medical
records, remuneration)
FINAL: At Home Geriatric Outreach 52 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
Co‐located team based care facilitates
communication
enhances continuity of care between
specialist, and community providers
(family doctors, allied
Community readiness
Ongoing communication will be
required with all stakeholders
patients, family, care givers, primary
care providers, specialized geriatric
medicine providers, community
resource organizations, community
partners (Hamilton Family Health
Team),
Recognition of need has been
identified, preliminary experience
Familiarity with shared care model
(mental health shared care model
HFHT)
History of collaboration between
stakeholdes; patients, primary care,
specialized geriatric providers,
community organizations and
partners)
Current initiatives:
Shared care model with specialized
geriatric medicine in primary care
(Collaboration between Hamilton
Family Health Team, Department of
Family Medicine, McMaster
University, AS, CCAC)
Patient health passport
Widely variable models of primary
care delivery across the LHIN
(variation in resources of space,
human, remuneration)
development of patient health
passport
FINAL: At Home Geriatric Outreach 53 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
Services
Survey and identify process for
linkages between services (eg.acute
care, LTC primary care, community
resources, transitional care, ‘at home'
program,
Clinical services with established
efficacy
Under utilization, duplication of
services, variable awareness of
resources and services
Coordination of services will require
communication, accountability.
Partnerships/linkages
Engage, communicate build on
current linkages among
stekeholders/partners (CCAC AS DVA
CNIB meals on wheels etc),
survey needs and identify strategies
to maximize resources and linkages to
avoid under utilization and
duplication of resources and services
Well established relationships
collaborative partnerships among
stakeholders (patients family, care
givers, primary care providers
specialized geriatric providers,
community partners)
FINAL: At Home Geriatric Outreach 54 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
HAMILTON NIAGARA HALDIMAND BRANT
LOCAL HEALTH INTEGRATION NETWORK
CLINICAL SERVICES PLANNING PROJECT
Transitional Care
PLANNING ADVISORY GROUP MEETING GUIDE
FINAL: At Home Geriatric Outreach 55 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
Complete Template #1. Describe the strengths and challenges within the existing health care system in addressing population health care needs for the
PAG’s patient/client population. Primers for discussion: ‘Summary of Community Values and Preferences’ (Appendix A), ‘Criteria for PAG Service Delivery
Models’ (Appendix B) and ‘Guiding Principles for PAG Service Delivery Models’ (Appendix C).
Template #1: Strengths and Challenges within the Current System in Addressing Population Needs PAG Name Transitional Care PAG Facilitator Dr. George Heckman
Strengths and Challenges
Introduction PAG – Geriatrics (frailty and chronic disease)
Almost 15% of Canadians are aged 65 years or over, and the greatest proportional population increase is occurring among octogenarians (StatsCan 01). The
rising numbers of older persons is expected to cause a significant strain on health care budgets, as the burden of chronic disease increases with age (Rapoport et
al, 2004). Chronic disease management (CDM) approaches have focused on improving outcomes for persons with major chronic illnesses such as diabetes
mellitus, heart failure or chronic obstructive pulmonary disease. However, such approaches perpetuate a system of care silos that focus on individual conditions
as if they occur in isolation, a model that is unsuitable to the growing number of seniors who suffer from multiple concurrent comorbidities. In Canada, over 40%
of persons aged 80 years and over report three or more chronic illnesses (Rapoport et al, 2004). In addition to these chronic illnesses, increasing numbers of
seniors are also afflicted by age‐associated disabilities and geriatric syndromes such as frailty, functional decline, disability, falls, incontinence, and
psychogeriatric disorders such as cognitive impairment, depression and anxiety. In the 2003 Canadian Community Health Survey of 28617 adults aged 65 years
and over, 4% of men and 4% of women aged 65 to 74 years required assistance in at least one basic activity of daily living (BADL), and 9% of men and 18% of
women required assistance in at least one instrumental activity of daily living (IADL) (Gilmour 05). Among men and women aged 85 years and over, these figures
rose to 20% and 23% for BADLs and 46% and 65% for IADLs, respectively.The economic impact of these geriatric syndromes is equivalent to that of major chronic
illnesses (Gilmour & Park, 2005; Cigolle et al, 2007; Levy & Muller, 2006; Rubenstein, 2006; Fillit & Hill, 2005; AHA 2002; Szczech & Lazar, 2004).
FINAL: At Home Geriatric Outreach 56 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
Introduction to Geriatrics – Frailty and chronic disease management model
Frailty can be understood as a state of increased vulnerability to adverse health outcomes due to age‐related decreases in physiologic reserve, and is most often,
but not exclusively, found in older persons (Bergman 2007). Frailty bears many similarities to major chronic diseases, as it is more common with age, and leads
to disability, increased health resource utilization, and mortality. Perhaps less widely appreciated is that frailty can be a direct consequence of poorly managed
chronic diseases such as heart failure, COPD, or diabetes. Moreover, just like these chronic diseases, frailty can be successfully managed. Numerous randomized
clinical trials demonstrate that comprehensive geriatric care can reduce mortality, improve function, cognition and quality of life, and prevent hospitalization
and institutionalization into long‐term care facilities, in a manner that can be cost‐effective. Yet, despite this evidence, the management of frailty in our current
health care system remains disjointed and inadequate.
In this submission, we propose an integrated system of clinical services to manage frailty at all levels of our health care system. These services will
complement existing inpatient consultation services and the regional Geriatric Assessment and Rehabilitation Unit at the Henderson General Hospital, by
enhancing the care of frail seniors in the community. The proposed clinical services are based upon the Chronic Disease Model, in which the majority of care
provided to seniors is at a primary care level, appropriately supported by multiple disciplines, including advanced practice nursing and other allied health
professions. In this model, specialty services, such as geriatric medicine or geriatric psychiatry, play two important roles:
1. Direct patient consultation: patients identified at the primary care level being at greatest risk of adverse events, such as institutionalization, due to
complex medical problems and / or geriatric or psychogeriatric syndromes, will undergo comprehensive geriatric assessments delivered by specialized
multidisciplinary teams that include a specialist in geriatric medicine or geriatric psychiatry.
2. Capacity building: For most patients to be cared for at the primary care level, specialists in geriatric medicine or psychiatry, as well as specialized allied
health professionals will be available to provide primary care providers educational opportunities designed to enhance their capacity to provide care to
seniors with mild to moderate frailty.
FINAL: At Home Geriatric Outreach 57 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
Introduction to Transitional Care
Over the last several decades, the average length of stay of older patients admitted to acute care hospitals with exacerbations of chronic diseases such as heart
failure or COPD has declined significantly. This trend has been associated with a parallel rise in the number of patients discharged with a particular diagnosis and
who are shortly thereafter rehospitalized with the same diagnosis. Risk factors for readmission include:
multiple functional deficits
polypharmacy, 2+ chronic health conditions
limited social support system
2+ hospitalizations in last 6 months
poor chronic disease knowledge (Naylor J Cardiovasc Nurs 00, Bowles JAGS 02, Wright Eur J Heart Fail 03; Riegel Nurs Res 07) These patients are essentially frail seniors.
In order to reduce the risk of readmissions, transitional care initiatives, based on the chronic disease management model, have been developed and evaluated.
Transitional care denotes a series of processes or actions to ensure / enhance continuity of care and collaboration between health care professionals, and thus
facilitate the safe and timely transfer of patients from one level of care (e.g., hospital) to another (e.g., primary care physician).
The core of transitional care is focused on enhancing the capacity of patients, often with the assistance of their primary informal caregivers (e.g. spouse, child),
for self‐care. The two primary components of self‐care include:
1. Self‐Maintenance: adherence to treatment and positive health practices 2. Self‐Management: active process that involves recognizing and responding to symptoms:
– recognize subtle changes in status; – evaluate their significance; – take appropriate action to avert further clinical deterioration; – evaluate effects of the action taken, and take further action is required.
Educating patients and caregivers on how to assertive and effectively navigate the health care system is a key desired outcome.
A number of randomized controlled trials have demonstrated the clinical benefits and cost effectiveness of this approach. A randomized controlled trial of 239
patients hospitalized with heart failure, aged on average 76 years and with 6 active comorbidities, evaluated an Advanced Practice Nurse (APN)‐led Self‐Care
intervention in which individualized plans of care addressing comorbidities and social issues were developed for each patient (Naylor MD J Am Geriatr Soc 04). In
addition to hospital visits, the APN visited the patient the day after discharge, and up to 7 more times during the 3 subsequent months. After a follow‐up of 1
year, the intervention results in substantially fewer heart failure deaths and rehospitalizations, as well as in fewer rehospitalizations for comorbid illnesses, at a
FINAL: At Home Geriatric Outreach 58 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
cost‐saving of $4845 per patient.
A second trial enrolled 750 pts aged on average 76 years, with various diagnoses including heart failure, stroke, coronary artery disease, arrhythmia, COPD,
diabetes mellitus, spinal stenosis, hip fracture, peripheral vascular disease, and venous thromboembolic disease (Coleman Arch Intern Med 06). The intervention
also focused on self‐care, including assistance with medications, development and maintenance of a patient‐centred and owned medical record (passport),
timely follow up with primary or specialty care, and development of a list of red flags to detect early illness decompensation and plans for response to avert a
readmission. An APN performed one home visit as well as 3 follow‐up phone calls during the subsequent 28 days. The intervention resulted in a reduction in
readmission for the index diagnosis at 6 months, and saved $500 per patient.
Finally, a randomized controlled trial enrolled 2370 pts, median age 80 and with various diagnoses including fractures, neurological disorder, cardiorespiratory
disease, and cognitive impairment (Cunliffe Age Ageing 2004; Miller Age Ageing 2005). The intervention was provided by a multidisciplinary team of allied health
professionals who provided patients and their caregivers with self‐care education, therapy and personal support following hospital discharge. The intervention
resulted in fewer total hospital days for up to one year, as well as improved performance of instrumental activities of daily living at one year, and reduced
caregiver burden during the first 3 months after hospital discharge. The intervention was associated with a savings of £1727 per patient.
Reflecting the strength of the evidence from these clinical trials, the Canadian Cardiovascular Society Heart Failure guidelines endorse the role of transitional
care programs in preventing hospital readmissions among frail older persons with heart failure (Arnold et al, Can J Cardiol 2008).
In response to this recommendation, a Transitional Care Team funded through the Aging at Home strategy, was established in Hamilton in the fall of 2008. This
team consists of Acute Care Nurse Practitioners, working in conjunction with the Hamilton Niagara Haldimand Brant Community Care Access Centre (Hamilton
branch), and targets frail older patients with heart failure or COPD and who are hospitalized at the General and McMaster sites of Hamilton Health Sciences.
Thus far, over 110 patients have been enrolled. The effect of the program on patient self‐care knowledge, functional ability, quality of life, and readmissions, as
well as on caregiver burden and quality of life, is being evaluated in a study approved by the McMaster University Research Ethics Board. Preliminary data
presented at the Annual Meeting of the Canadian Geriatrics Society in April 2009 demonstrate significant increases in patient self‐care knowledge, with no
significant decline in patient function, as well as no increase in caregiver burden. The readmission rate for both COPD and heart failure at 3 months was 18%,
which compares favourably to rates of readmission for heart failure alone reported in the literature (Phillips et al JAMA 2004).
Proposed Enhanced Program Model
This proposal builds upon the Transitional Care Model described above that has been funded through AAH. Once fully implemented, all older hospitalized
patients with mild to moderate frailty will be eligible for Transitional Care support upon discharge from hospital. Currently, patients with heart failure and COPD
are eligible. Eligible diagnoses will be expanded to include, among others, diabetes mellitus, pain, neurological disorders (e.g. Parkinson’s disease, stroke),
FINAL: At Home Geriatric Outreach 59 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
coronary artery disease, as well as the other diagnoses noted in the introduction above. Patients will be identified early during the course of hospitalization and
assessed and followed by a specially trained nurse. Upon discharge, patients will be seen within 48 hours, whereupon the self‐care education will begin. Patients
will be enrolled for at least 4 weeks, and for up to 3 months as required.
It is important to recognize that no more than half of clients served by the CCAC are referred from hospital, with the other half referred directly from primary
care or from other outpatient sources (personal communication from Dr. Jeff Poss, University of Waterloo). It is expected that a substantial proportion of these
patients will also suffer from multiple chronic diseases, and will thus also be able to benefit from the self‐care education delivered by the Transitional Care
Approach. As long‐stay CCAC clients are regularly assessed by CCAC case managers using the RAI‐HC suite of instruments, we will be able to utilize these
instruments to identify clients eligible for Transitional Care, this time with the additional aim of preventing an admission to hospital.
The RN Role
Currently in Hamilton, consistent with the literature, the RN role is provided by an Acute Care Nurse Practitioner trained in adult education as well as adult
medicine. Ultimately, the role of the ACNP will be to become a resource for the program and to train registered nurses to perform the self‐care role.
Input from Geriatric Specialists
The Transitional Care Model is essentially a primary care model for complex patients, consistent with the Chronic Disease Management approach. A certain
proportion of patients (approximately 20%) will be particularly complex and will benefit from the input of specialists in Geriatric Medicine or Geriatric Psychiatry.
Therefore, part of the initial and ongoing assessment of patients by the RN will include the use of standardized instruments to assess individual patients’ degree
of frailty and risk for subsequent adverse health outcomes. Patients at high risk will be seen in consultation by a Geriatric Medicine or Psychiatry specialist.
Please refer to the “athome outreach” and “primary care shared model” descriptions for a better understanding of how these programs relate to each other.
In addition to a direct consultative role, specialists in Geriatric Medicine and Psychiatry will assist primary care in developing the capacity to manage frail older
patients through ongoing clinical education activities, journal clubs, and workshops.
Data collection and evaluation
Data shall be collected in order to evaluate the effectiveness of the program. In addition to RAI‐HC data (as the program will run as an enhanced CCAC service),
we will utilize standardized instruments to collect data on patient self‐care knowledge, quality of life and caregiver burden. The RAI‐HC data may assist us in the
comparing the effectiveness of the program with historical control groups, as well as with other Ontario LHINs.
FINAL: At Home Geriatric Outreach 60 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
7. Complete Template #2: Describe the leading factors that are most likely to increase or decrease the demand for health care by the PAG’s patient/client population by 2013. For each of these factors, indicate whether it will have a modest or significant impact on the future demand for health care. And, list factors that may influence the demand for care beyond 2013
Template #2: Factors Most Likely to Increase or Decrease the Future Demand for Health Care:
Same as template 2 in section above
FINAL: At Home Geriatric Outreach 61 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
8. Complete Template #3. Describe the key components of an ideal service delivery model for the PAG’s target population.
Template #3: Components of an Ideal Service Delivery Model PAG Name Transitional Care PAG Facilitator Dr. George Heckman
Component of service delivery
model
Services associated with this component of the
model
Clinical and non‐clinical interdependencies (e.g.,
DI, lab, other programs/services, other PAGs) Linkages to community services
Health Promotion/Disease
Prevention
Enhancing self management
Targeted towards secondary prevention e.g
hospital admissions for indexed and other
diagnosis, adverse reactions
Pharmacy support re: medication
management, linkages to
programs to help maintain
function – falls, memory, diabetic,
continence advisors. Take actions
early on to prevent further
deterioration in health. Increase
confidence and knowledge
FINAL: At Home Geriatric Outreach 62 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Facilitator Dr. George Heckman PAG Name Transitional Care
Component of service delivery Services associated with this component of the Clinical and non‐clinical interdependencies (e.g.,
model model DI, lab, other programs/services, other PAGs) Linkages to community services
Primary Care
Identify population CHF COPD and refer
Screening to prevent from getting to the point to
be admitted to hospital
Some can be managed by primary health
Geriatrician build capacity in FHT/family physicians
–through consult and provide advice
Chronic disease management model
CCAC FHT attachments
Geriatrician
Linkages with Alzheimer’s Society
– First Link, Diabetic Management
Programs
Pharmacy home visit or med
review program
Pre‐hospital Care
FINAL: At Home Geriatric Outreach 63 of 86
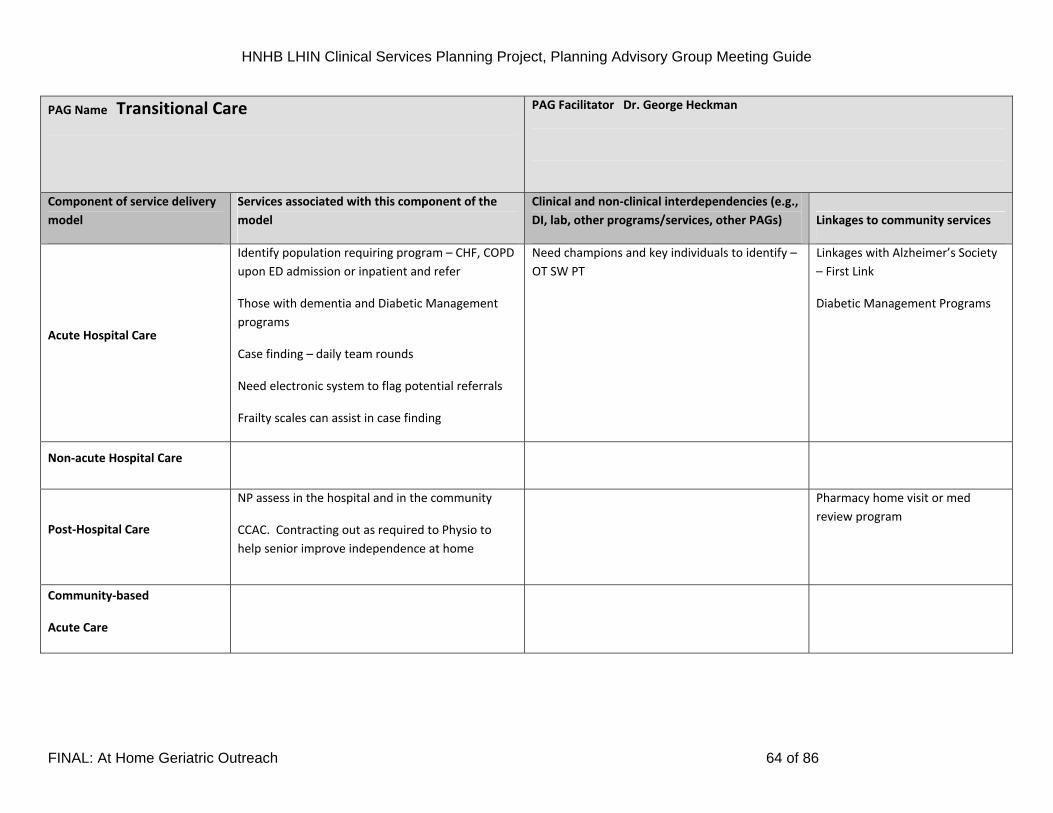
HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Facilitator Dr. George Heckman PAG Name Transitional Care
Component of service delivery Services associated with this component of the Clinical and non‐clinical interdependencies (e.g.,
model model DI, lab, other programs/services, other PAGs) Linkages to community services
Acute Hospital Care
Identify population requiring program – CHF, COPD
upon ED admission or inpatient and refer
Those with dementia and Diabetic Management
programs
Case finding – daily team rounds
Need electronic system to flag potential referrals
Frailty scales can assist in case finding
Need champions and key individuals to identify –
OT SW PT
Linkages with Alzheimer’s Society
– First Link
Diabetic Management Programs
Non‐acute Hospital Care
Post‐Hospital Care
NP assess in the hospital and in the community
CCAC. Contracting out as required to Physio to
help senior improve independence at home
Pharmacy home visit or med
review program
Community‐based
Acute Care
FINAL: At Home Geriatric Outreach 64 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Facilitator Dr. George Heckman PAG Name Transitional Care
Component of service delivery Services associated with this component of the Clinical and non‐clinical interdependencies (e.g.,
model model DI, lab, other programs/services, other PAGs) Linkages to community services
Community‐based Non‐Acute
Care
CCAC and NP – teaching self management ,
monitoring of symptoms, strategies to circumvent
exacerbation
Clinic and in home where appropriate
NP could build capacity of other personnel e.g. RNs
Education to non regulated personnel in client’s
home
Case finding
Multidisciplinary
RN complete teaching, NP LHIN wide ‐ lead building
capacity
Support to primary care
Services developed in conjunction with
clients/families, their goals and self management
needs – Client centred not service centred
Flexible duration of service e.g. longer for those
with hidden cognitive impairment,
Supportive housing project or wellness centres
Community Home to Stay programs
CCAC attachments to supportive housing settings.
Primary Care
Geriatrician
Interdependencies with informal and formal
systems of support – consistency of approach
CHCs for Francophone, aboriginal population for
shared service delivery
Potential Enhancement – linkage
to LTC NPs to manage in the LTCH
Pharmacy home visit or med
review program
Heart Failure clinics/diabetes
programs
Academic linkages to maintain
evidence based practice
End of Life Care
Primary care, hospitals
FINAL: At Home Geriatric Outreach 65 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Facilitator Dr. George Heckman PAG Name Transitional Care
Component of service delivery Services associated with this component of the Clinical and non‐clinical interdependencies (e.g.,
model model DI, lab, other programs/services, other PAGs) Linkages to community services
System navigation
Follows national heart failure guidelines
Quality indicators – readmissions, ACOVE (quality
indicators for frail seniors)
Patients/families taught to self navigate the care
continuum, use of care passport
FINAL: At Home Geriatric Outreach 66 of 86
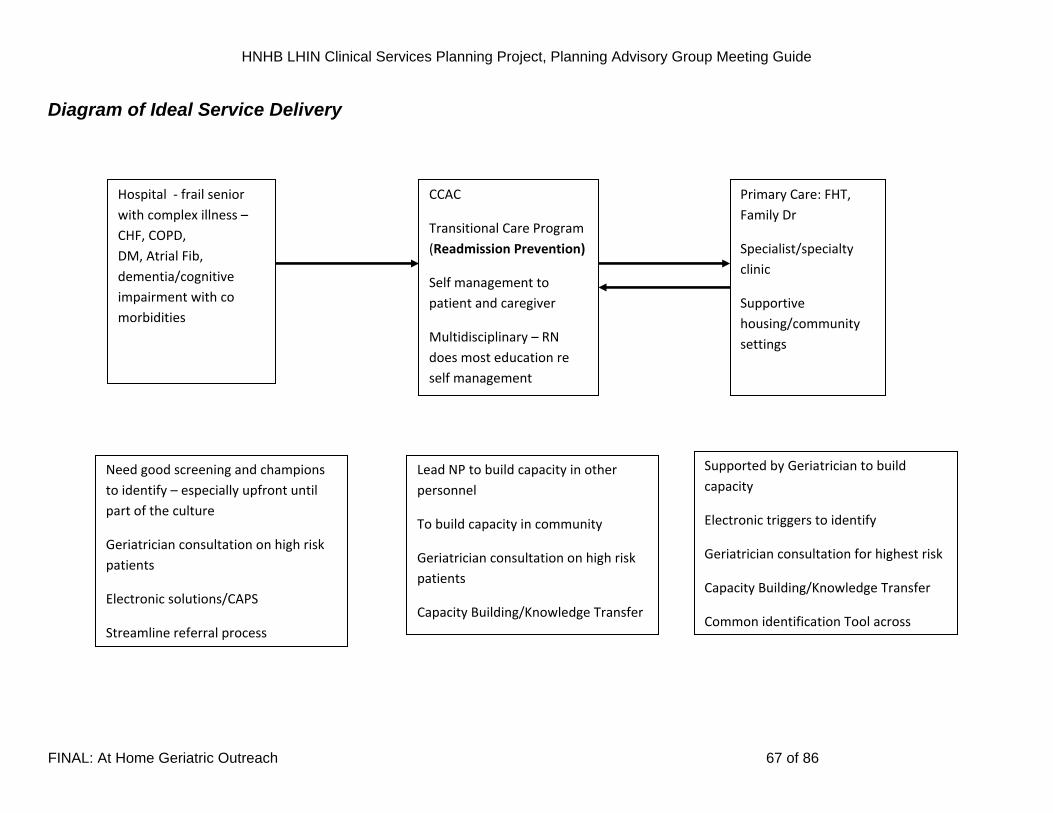
HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
Diagram of Ideal Service Delivery
Hospital ‐ frail senior
with complex illness –
CHF, COPD,
DM, Atrial Fib,
dementia/cognitive
impairment with co
morbidities
CCAC
Transitional Care Program
(Readmission Prevention)
Self management to
patient and caregiver
Multidisciplinary – RN
does most education re
self management
Primary Care: FHT,
Family Dr
Specialist/specialty
clinic
Supportive
housing/community
settings
Lead NP to build capacity in other
personnel
To build capacity in community
Geriatrician consultation on high risk
patients
Capacity Building/Knowledge Transfer
Need good screening and champions
to identify – especially upfront until
part of the culture
Geriatrician consultation on high risk
patients
Electronic solutions/CAPS
Streamline referral process
Supported by Geriatrician to build
capacity
Electronic triggers to identify
Geriatrician consultation for highest risk
Capacity Building/Knowledge Transfer
Common identification Tool across
FINAL: At Home Geriatric Outreach 67 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
Template #4. Assess and Describe the PAG service delivery model using the HNHB LHIN Criteria PAG Name: Transitional Care
Domain Criteria Assessment Description
Strategic Fit Alignment with LHIN priorities
for health improvement
ALC alleviation
DM using CDM model as part of optimal management of co‐morbidities or primary index condition
Emergency Department Diversion
CCAC able to service rural communities
Could use e‐heath solutions
Alignment with trends in
health care needs and system
transformation
Primary care reform
Addresses growing senior, frail population
Integrated approach
LHIN wide access (not limited by catchment area)
Shorter Hospital LOS – shift to community
Continuity of care
Holistic
Self efficacy/self management approach
Capacity building
Strategic partnerships
FINAL: At Home Geriatric Outreach 68 of 86
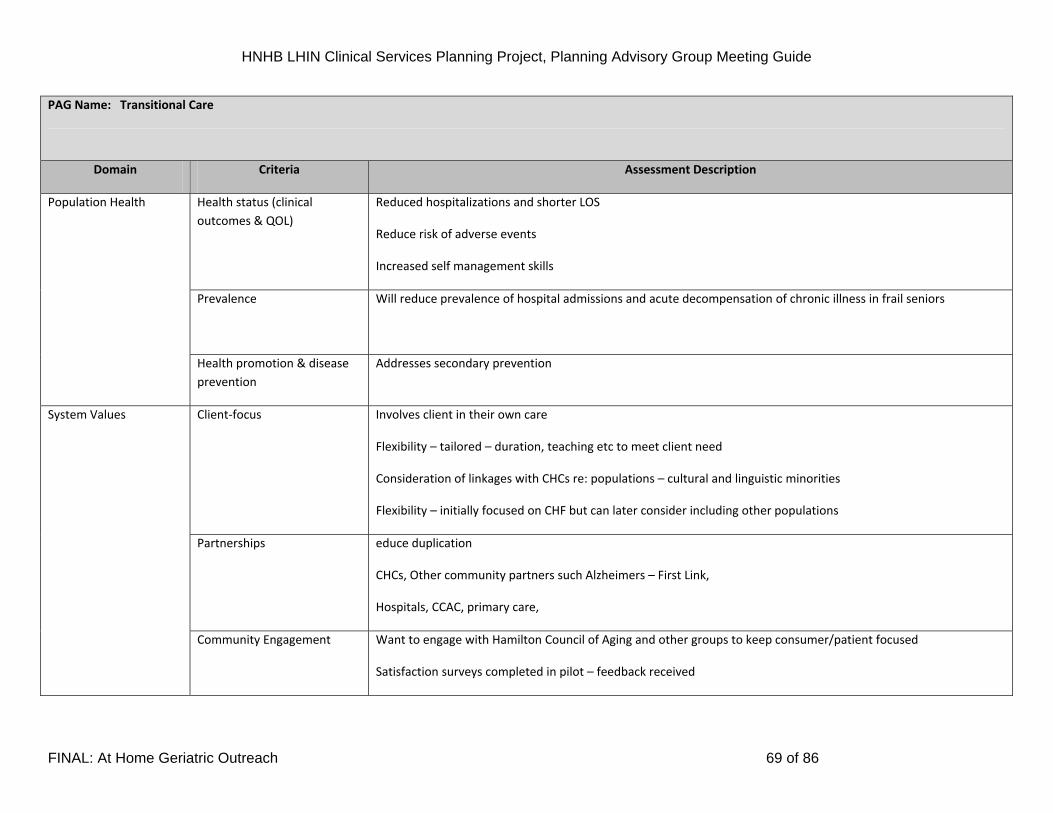
HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name: Transitional Care
Domain Criteria Assessment Description
Health status (clinical
outcomes & QOL)
Reduced hospitalizations and shorter LOS
Reduce risk of adverse events
Increased self management skills
Prevalence Will reduce prevalence of hospital admissions and acute decompensation of chronic illness in frail seniors
Population Health
Health promotion & disease
prevention
Addresses secondary prevention
Client‐focus Involves client in their own care
Flexibility – tailored – duration, teaching etc to meet client need
Consideration of linkages with CHCs re: populations – cultural and linguistic minorities
Flexibility – initially focused on CHF but can later consider including other populations
Partnerships educe duplication
CHCs, Other community partners such Alzheimers – First Link,
Hospitals, CCAC, primary care,
System Values
Community Engagement Want to engage with Hamilton Council of Aging and other groups to keep consumer/patient focused
Satisfaction surveys completed in pilot – feedback received
FINAL: At Home Geriatric Outreach 69 of 86
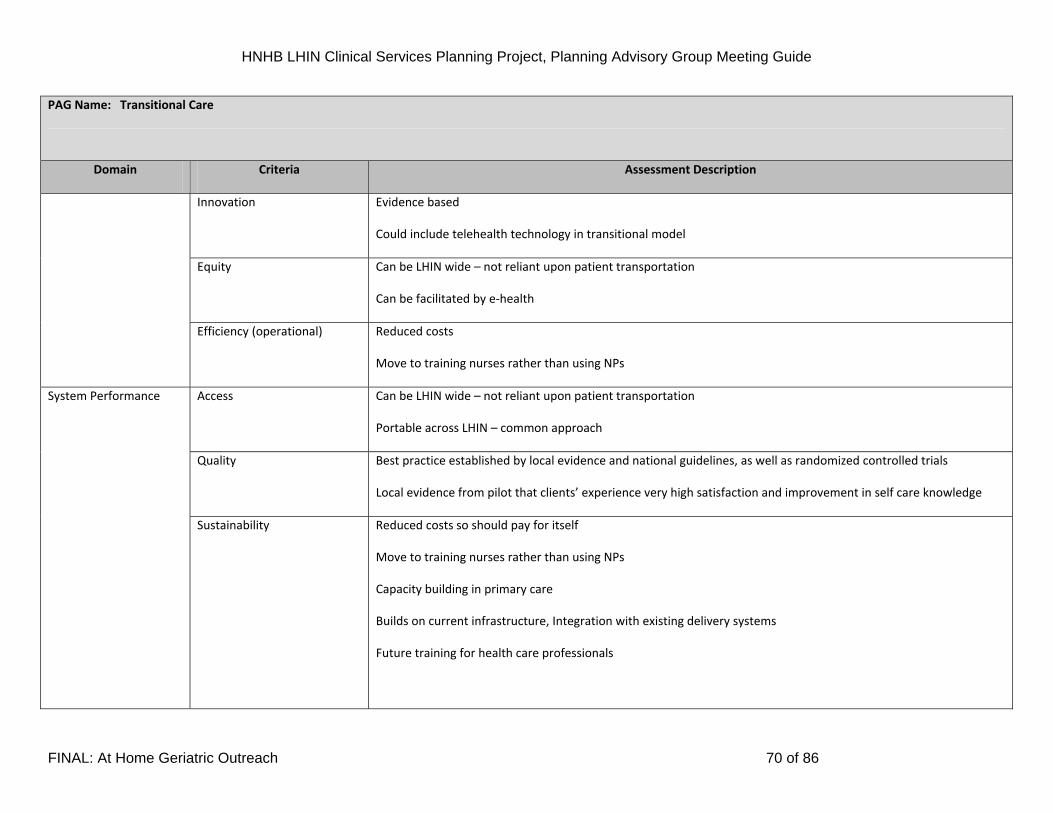
HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name: Transitional Care
Domain Criteria Assessment Description
Innovation Evidence based
Could include telehealth technology in transitional model
Equity Can be LHIN wide – not reliant upon patient transportation
Can be facilitated by e‐health
Efficiency (operational) Reduced costs
Move to training nurses rather than using NPs
Access Can be LHIN wide – not reliant upon patient transportation
Portable across LHIN – common approach
Quality Best practice established by local evidence and national guidelines, as well as randomized controlled trials
Local evidence from pilot that clients’ experience very high satisfaction and improvement in self care knowledge
System Performance
Sustainability
Reduced costs so should pay for itself
Move to training nurses rather than using NPs
Capacity building in primary care
Builds on current infrastructure, Integration with existing delivery systems
Future training for health care professionals
FINAL: At Home Geriatric Outreach 70 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name: Transitional Care
Domain Criteria Assessment Description
Integration
By definition; supports continuity care across the system. Essential core nature of the intervention.
FINAL: At Home Geriatric Outreach 71 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
9. Complete Template #5. Describe the pre‐requisites, enablers and challenges to implementation of the ideal service model.
Template #5: Description of Pre-requisites, Enablers and Challenges to Implementation: Category Pre‐requisites Enablers Challenges
Policy/legislation Appropriate funding levels
Supported by national policy re:
Chronic Disease Management for
Heart Disease “Canadian Heart Health
Strategy Action Plan”
Resources (e.g., human, fiscal, capital,
etc.)
Human Resource investment
Funding model for Geriatrician
Consultation e.g. clinic space and
supporting resources
Need family physician
Using rich RAI HC data to risk
stratifying
Care Connectors
Sharing of electronic care passport eg.
Memory sticks
Limited clinic space for Geriatrician
clinics
Long waiting lists for Geriatricians
No family physician
Community readiness
Community champions to promote
uptake of new service
Seniors Education to target the at risk
population
CCAC support already in place for
many of these individuals
Linkages with retirement homes and
supportive housing settings
Fear from some seniors – perception
that it may complicate their care
Support from family medicine
FINAL: At Home Geriatric Outreach 72 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
Services
Community Based Geriatrician
consults e.g. CCAC branches, other
Community Agencies.
Co location agreements
Supporting infrastructure already in
place re; hospital, primary care, CCAC,
geriatric consults
Partnerships/linkages
Hospitals need to invest in what
happens in the community after
patient discharge.
CCAC has established linkages with
FHTs and Hospitals
Hospitals need to invest in what
happens in the community after
patient discharge
FINAL: At Home Geriatric Outreach 73 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
HAMILTON NIAGARA HALDIMAND BRANT
LOCAL HEALTH INTEGRATION NETWORK
CLINICAL SERVICES PLANNING PROJECT
Video Conferencing Geriatrics
PLANNING ADVISORY GROUP MEETING GUIDE
FINAL: At Home Geriatric Outreach 74 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
Complete Template #1. Describe the strengths and challenges within the existing health care system in addressing population health care needs for the
PAG’s patient/client population. Primers for discussion: ‘Summary of Community Values and Preferences’ (Appendix A), ‘Criteria for PAG Service Delivery
Models’ (Appendix B) and ‘Guiding Principles for PAG Service Delivery Models’ (Appendix C).
Template #1: Strengths and Challenges within the Current System in Addressing Population Needs PAG Name Geriatrics ‐
Video conferencing
PAG Facilitator
Dr. D. Cowan
Strengths Challenges
Can be used across multiple sites and for a variety of purposes;
educational and clinical.
Increased access to specialized geriatric services
Cuts out need for transportation in some instances. Links well with
screening and assessment by outreach teams to assess risk. People who
cannot travel may be able to access a video conferencing site and with a
nurse get access to a geriatrician via video link
FINAL: At Home Geriatric Outreach 75 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
10. Complete Template #2: Describe the leading factors that are most likely to increase or decrease the demand for health care by the PAG’s patient/client population by 2013. For each of these factors, indicate whether it will have a modest or significant impact on the future demand for health care. And, list factors that may influence the demand for care beyond 2013
Template #2: Factors Most Likely to Increase or Decrease the Future Demand for Health Care:
Same as template 2 from the previous section
FINAL: At Home Geriatric Outreach 76 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
Complete Template #3. Describe the key components of an ideal service delivery model for the PAG’s target population.
Template #3: Components of an Ideal Service Delivery Model PAG Name
Videoconferencing Geriatric Consultation and Out‐reach Service PAG facilitator: Dr. D. Cowan
Component of service delivery
model
Services associated with this component of the
model
Clinical and non‐clinical interdependencies (e.g.,
DI, lab, other programs/services, other PAGs) Linkages to community services
Health Promotion/Disease
Prevention
Health promotion and disease prevention is an
integral part of comprehensive geriatric
consultation. We focus upon the person as a whole
routinely assessing and screening or many
preventable diseases/problems such as cognitive
impairment, depression,
polypharmacy/inappropriate prescribing,
osteoporosis, falls and fragility fractures,
deconditioning, and malnutrition, amongst others.
These disease prevention interventions can now be
provided to clients in outlying areas who would not
receive such services. There is also an important
“learning by seeing” function whereby general
practitioners/allied healthcare workers adopt these
practices and apply them to others in their practice.
Videoconferencing can also serve as an important
direct educational tool for rural health care teams
which can take of case conferences surrounding
their individual patients, or educational sessions
with health care teams.
The major partner in this initiative
is the Ontario Telemedicine
Network whose mandate is to
provide equitable and timely access
to health care services, and medical
education, to those in outlying
areas using videoconferencing
technology. Underutilized
videoconferencing technology is
already available to all hospitals in
Ontario, as well as Family Health
Teams. The Ontario telemedicine
network has a goal to increase
direct patient services using
videoconferencing by 30% annually
and is committed to partnering
with geriatricians in LHIN’s 4.
Our service will be closely aligned
with other community partners
such as the Alzheimer's Society and
the Community Care Access
Centers. This will provide local
FINAL: At Home Geriatric Outreach 77 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name
Videoconferencing Geriatric Consultation and Out‐reach Service PAG facilitator: Dr. D. Cowan
Component of service delivery
model
Services associated with this component of the
model
Clinical and non‐clinical interdependencies (e.g.,
DI, lab, other programs/services, other PAGs) Linkages to community services
support to the frail elderly as well
as a means to follow up with
specific recommendations and care
plans for each patient.
Other linkages would include Meals
on Wheels, Lifeline, DVA, There is
excellent evidence suggesting that
community education and support
prevents/delays
institutionalization.
FINAL: At Home Geriatric Outreach 78 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name
Videoconferencing Geriatric Consultation and Out‐reach Service PAG facilitator: Dr. D. Cowan
Component of service delivery
model
Services associated with this component of the
model
Clinical and non‐clinical interdependencies (e.g.,
DI, lab, other programs/services, other PAGs) Linkages to community services
Primary Care
This is likely the most important aspect of
telemedicine consultations services. While we are a
consultation model, it is also blended with primary
care in so far as a consultation process directly
involves the primary care team as they will be with
the patient during the clinical encounter. This
serves the referring team will benefit from direct
communication with the geriatrician, moreover,
the patient can receive specialized services within
their primary care setting which is a much more
patient centered approach (i.e. preventing travel
over long distances and allowing them to the
setting and a setting which is more familiar and
comfortable.) . This model also provides a more
equitable distribution of services to rural
communities, as well as increasing efficiencies in so
far as physicians do not have to travel long
distances to see patients. Wasted travel time can
be directed toward seeing multiple patients in
multiple communities on the same day.
As above.
FINAL: At Home Geriatric Outreach 79 of 86
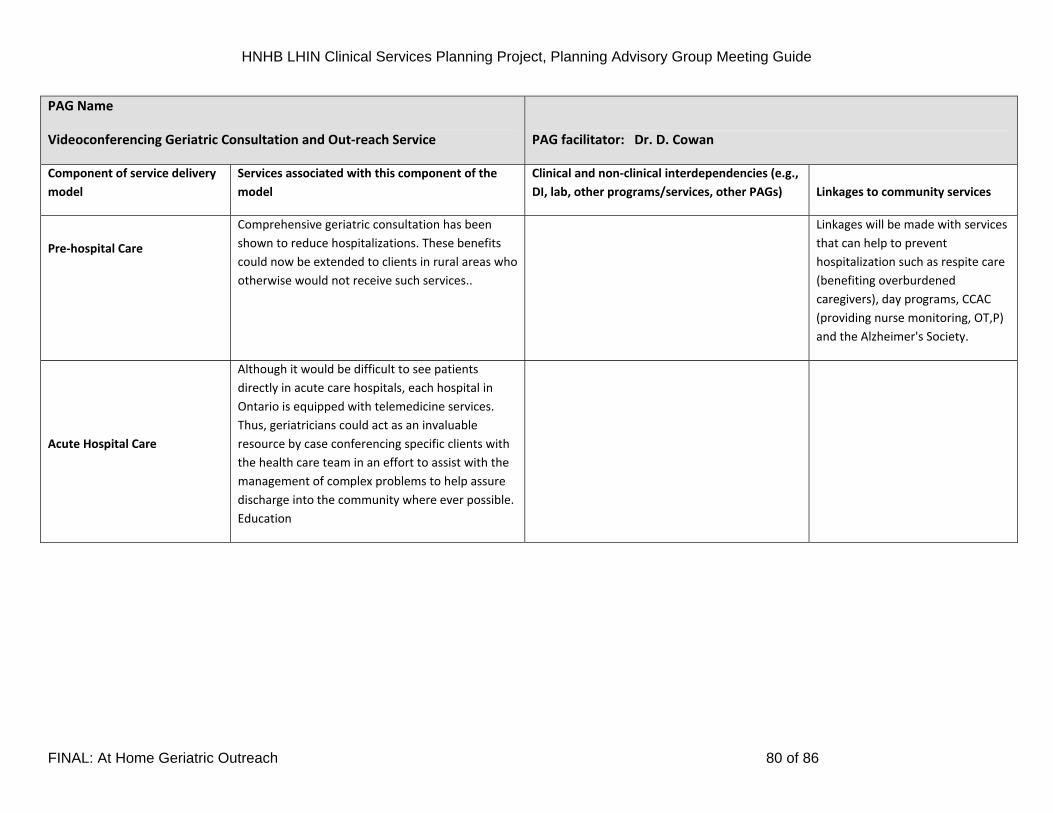
HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name
Videoconferencing Geriatric Consultation and Out‐reach Service PAG facilitator: Dr. D. Cowan
Component of service delivery
model
Services associated with this component of the
model
Clinical and non‐clinical interdependencies (e.g.,
DI, lab, other programs/services, other PAGs) Linkages to community services
Pre‐hospital Care
Comprehensive geriatric consultation has been
shown to reduce hospitalizations. These benefits
could now be extended to clients in rural areas who
otherwise would not receive such services..
Linkages will be made with services
that can help to prevent
hospitalization such as respite care
(benefiting overburdened
caregivers), day programs, CCAC
(providing nurse monitoring, OT,P)
and the Alzheimer's Society.
Acute Hospital Care
Although it would be difficult to see patients
directly in acute care hospitals, each hospital in
Ontario is equipped with telemedicine services.
Thus, geriatricians could act as an invaluable
resource by case conferencing specific clients with
the health care team in an effort to assist with the
management of complex problems to help assure
discharge into the community where ever possible.
Education
FINAL: At Home Geriatric Outreach 80 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name
Videoconferencing Geriatric Consultation and Out‐reach Service PAG facilitator: Dr. D. Cowan
Component of service delivery
model
Services associated with this component of the
model
Clinical and non‐clinical interdependencies (e.g.,
DI, lab, other programs/services, other PAGs) Linkages to community services
Non‐acute Hospital Care
A backlog of ALC patients is one of the greatest
challenges facing acute care hospitals. As in the
case with Acute care Hospital, individual clients
could be case conferenced to ensure care is
optimized thereby increasing the probability
patients can be discharged to the community. For
patients who cannot reliably be discharged, this
often neglected group with multiple co‐morbidities
will receive care that otherwise would not have.
Post‐Hospital Care
Early follow‐up following discharge has been shown
to reduce hospitalizations in the elderly. It would
not be practical to have these patients assessed by
geriatricians were not in the immediate geographic
area. Telemedicine services would provide a means
for geriatric input following hospitalization in a
timely manner to hopefully maintain patients in the
community and prevent re‐admission.
Community‐based Acute Care
Community‐based Non‐Acute
Care
FINAL: At Home Geriatric Outreach 81 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
Diagram of Ideal Service Delivery Model:
+++++ Please refer to overall Specialized Geriatric Services Model diagram
FINAL: At Home Geriatric Outreach 82 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
Template #4. Assess and Describe the PAG service delivery model using the HNHB LHIN Criteria PAG Name: Videoconferencing PAG facilitator – Dr. D. Cowan
Domain Criteria Assessment Description
Strategic Fit Alignment with LHIN priorities
for health improvement
Geriatric consultation and outreach service via video teleconferencing supports many LHIN priorities including
focusing on geriatric services, mental health and e‐health. Successful geriatric interventions can reduce
hospitalizations, reduce lengths of stay (for example HELP programmes),
Alignment with trends in
health care needs and system
transformation
This intervention helps to address the impending crisis in health care involving the aging population. It is also an
innovative model utilizing videoconferencing technology to provide these services in an efficient and equitable
manner to patients and healthcare providers alike.
Health status (clinical
outcomes & QOL)
A videoconferencing model of geriatric consultation will provide a proven means of intervention to elderly
populations who would not otherwise enjoy the benefits of these services. Outcomes that geriatric consultation
have been shown to achieve include reduced hospitalizations, delay to institutionalization with compression of
morbidity, prevention of outcomes such as falls, and reduced caregiver burden.
Prevalence Prevent measures employed in geriatric consultation have been shown to prevent many negative outcomes
including falls, fractures, frailty and institutionalization, thus reducing the prevalence of these conditions in the
community. Videoconferencing also provides an effective and efficient means of spreading best practices to primary
care physicians and allied healthcare professionals.
Population Health
Health promotion & disease
prevention
As above
System Values Client‐focus Videoconferencing consultation services are extremely client focused in so far as they allow the individual to be
seen closer to their home in a more familiar setting. Client satisfaction data collected by the Ontario Telemedicine
Network indicates that individuals would rather receive teleconference services as opposed to traveling longer
distances to meet with a specialist if they are given the choice.
FINAL: At Home Geriatric Outreach 83 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name: Videoconferencing PAG facilitator – Dr. D. Cowan
Domain Criteria Assessment Description
Partnerships The application videoconferencing Geriatric Consultation takes advantage of a multimillion dollar infrastructure that
is already in place via OTN. Thus there would be little additional cost to take advantage of this valuable resource.
Moreover, OTN is a dedicated partner searching to promote clinical opportunities with an intention of delivering an
additional 30% per year of direct patient services. Geriatricians already have close partnerships with existing
services such as the Alzheimer Society.
Community Engagement Seek local sites to host technology
Innovation This is an innovative approach in so far as videoconferencing consultation is in its infancy and underutilized in this
geographic area. There is only one other person in Ontario providing geriatric consultation by this means. There is
tremendous potential for growth.
Equity The shortage of geriatricians in Ontario is a problem that is not going to be solved quickly. (There are only 45
geriatricians in all of Ontario compared to much larger specialty groups such as cardiology. In fact, demographic
data suggests that the number of geriatricians may even decline given that new graduates are fewer than those
nearing retirement. It is self evident that videoconferencing will greatly improve equity of access to the scarce
resource, particulate particularly for patients in rural and urban under serviced areas.
Efficiency (operational) This PAG model is extremely efficient insofar as it utilizes existing resources that are being some optimally employed
such as the OTN network and other community service providers such as the Alzheimer's Society, CCAC etc
Access Not only will this provide timely access and a more efficient use of geriatrician time by eliminating the need for
travel, this will provide access to geriatric services for clients who would have had none at all.
Quality
System Performance
Sustainability
This is a highly sustainable intervention. The MOHLTC and OTN both have a substantial commitment to providing
videoconferencing consultation services. The infrastructure is in place already. The model is simple, and could be
implemented within a matter of two or three months at any given site. We are presently piloting the feasibility at
one community site already.
FINAL: At Home Geriatric Outreach 84 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name: Videoconferencing PAG facilitator – Dr. D. Cowan
Domain Criteria Assessment Description
Integration
Videoconferencing technology can be used to deliver geriatric services both in terms of education and patient care
in primary care settings, acute care hospitals. The infrastructure is now available in all hospitals in Ontario and 70
Family Health Teams with the goal being to grow further In the primary care setting.
FINAL: At Home Geriatric Outreach 85 of 86

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
11. Complete Template #5. Describe the pre‐requisites, enablers and challenges to implementation of the ideal service model.
FINAL: At Home Geriatric Outreach 86 of 86
Template #5: Description of Pre-requisites, Enablers and Challenges to Implementation: Category Pre‐requisites Enablers Challenges
Policy/legislation Funding for geriatricians Funding for geriatricians
Resources (e.g., human, fiscal, capital,
etc.)
Equipment
Community readiness
Host sites
Services
Partnerships/linkages
Host sites


















