Clinical Practice Review Issue7 July Aug Sept 09
2
Clinical Practice Review Editorial 1 Hand hygiene compliance 1 Vitamin and mineral supplements taken @ the Women’s 2 Right Patient – Right Care 4 ISBAR is here! 5 Pharmacy news 6 THE ROYAL WOMEN’S HOSPITAL QUALITY AND SAFETY UNIT NEWSLETTER ISSUE 7 JULY, AUGUST, SEPTEMBER 2009 1 Hospital acquired infections, hand hygiene and an age-old problem: The renewed focus on improving hand hygiene in recent years has seen overall compliance rise from 20% at RWH two years ago (you may remember the Herald Sun headline at the time and RWH topping the “Worst Offenders” list) to 75% in the latest audit. • The World Health Organizations’ target is 55% and Victorian hospitals are aiming for 60%. While women’s hospitals have been relatively spared from the multi- resistant organisms (MRO) that are commonplace in general hospitals, RWH has observed an increase in MRO burden. • Meticulous hand hygiene practices are essential to reduce the spread of these MROs as well as other pathogens. Doctors versus Nurses! Multiple studies on hand hygiene compliance across various institutions confirm that doctors perform poorly when compared with nurses. This is despite the fact that nurses have more opportunities for patient contact than doctors. Many theories for this have been proposed but we will let you use your imagination! • Nurses have improved their hand hygiene compliance at RWH • Doctors have failed to make significant gains above 60%. • Doctors have the opportunity to spread more nosocomial pathogens as they potentially move between more patients than do other staff. • Poor compliance amongst medical staff is reducing the overall performance of RWH when we benchmark with other hospitals. Hand hygiene compliance D09-135 design@thewomens October 2009 5 Gestational trophoblastic disease (GTD) covers a spectrum of tumors ranging from premalignant (hydatidiform mole) to malignant (invasive mole or choriocarcinoma). Complete and partial hydatidiform moles are the two most common types of pre-malignant GTD and both can progress to invasive moles. In a complete mole, an ovum devoid of maternal nuclear DNA is fertilised by 2 sperm or a single sperm – it duplicates its chromosomes to give a diploid complement of male DNA. In a partial mole the two sperms fertilise an ovum with maternal nuclear DNA forming a triploid conceptus (Figure 1). These proliferate to form abnormal trophoblasts. The uterus enlarges rapidly despite the absence of a fetus and the placenta contains many cysts to give a typical molar appearance. Maternal blood vessel formation increases and facilitates metastatic spread of the disease. Human chorionic gonadotrophin (hCG) is synthesised in the molar tissues and therefore can be used as a tumour marker to monitor disease progression or response. Invasive moles, choriocarcinomas and placental site trophoblasts are malignant tumours and are collectively known as gestational trophoblastic tumours 1 . GTDs are classified as low risk, high risk and ultrahigh risk and their medical management differs based on the risk and resistance to chemotherapy. Low risk patients are managed with the methotrexate (MTX) and calcium folinate regimen. Actinomycin may be used as an alternative if methotrexate is not tolerated. High risk patients are managed with the EMACO regimen, which consists of Etoposide, Methotrexate and Actinomycin, given on alternate weeks with Cyclophosphamide and vincristine(Oncovin®). Ultra-high risk patients are treated with the EMAPE regimen which includes Etoposide, high dose Methotrexate and Actinomycin, given on alternate weeks with CisPlatin and Etoposide with or without intrathecal methotrexate. All patients diagnosed with molar pregnancy are recorded in the Hydatidiform Mole Registry. Between 2002 and 2008, a total of 649 patients were diagnosed with molar pregnancy. Only forty-eight (7%) patients had persistent elevated hCG and received medical treatment (Figure 2). Thirty eight of those patients received low risk treatment – seven of them developed resistance to Methotrexate and were switched on to the high risk treatment regimen. In total ten patients received high risk treatment and only one patient received the ultrahigh risk regimen. Huda Ismail Treatment options for Gestational Trophoblastic Disease Susan Braybrook, telephone (03) 8345 2025 or email [email protected] For further information http://www.thewomens.org.au For intranet users http://intranet.thewomens.org.au/qualityandsafety Please let the associate editor have your views on the contents of this newsletter, or any other matters involving clinical practice which may be of interest to our readers. For any further enquiries regarding Pharmacy news please contact [email protected] ISBAR is here! Carol Vance Claire Fitzgerald What is ISBAR? ISBAR is a structured communication tool that improves the quality of information exchange when discussing patients. The tool was initially developed in the Navy to improve communication and has since been adapted for medical use. Inefficient communication can compromise patient care and using a standard approach to communication decreases the chance of forgetting relevant information and helps to decrease assumptions by making the reason for the call obvious at the outset. I Identification S Situation B Background A Assessment R Request or Recommendation Identify Identify yourself, the person you are speaking to, the patient, your location. Situation ‘Spoil’ the story. Stating the purpose of the call at the start of the conversation helps the receiver focus their attention appropriately when listening to the story. If urgent, make this clear from the start. Background Tell the story. Provide relevant information only and remember, less is more, particularly if the receiver already knows the patient. Assessment State what you think is going on. Give your interpretation of the situation. Include your degree of certainty - stating the obvious is helpful. Don’t leave the receiver to guess what you are thinking – tell them. Request / Recommendation State what you want and ask questions. What you say for ‘situation’ may be a concise summary of what you say for ‘assessment’ and ‘request’. This repetition is helpful as it emphasises the key purpose of the referral. Uses for ISBAR • Inpatient or outpatient • Urgent or non-urgent communications • Conversations with other staff, either in person or over the phone - Particularly useful in nurse – doctor communication - Also helpful in doctor-doctor and nurse-nurse communication • Discussions with allied health professionals • Conversations with peers • As a prompt for writing letters to other care providers • Escalating a concern Lanyard cards are available as a reminder about ISBAR, as well as notepads (which are found on the Gynaecology wards) which may help to organise your thoughts before beginning your communication. We encourage you to give ISBAR a try and start using it as a tool to improve all your clinical conversations. Carol Vance Principle Registrar Quality and Safety Fellow Claire Fitzgerald Project Manager Agree project EDITORIAL The backbone of good (best) clinical practice remains patient centred care that is effective and safe. This edition has articles that address the last two of these. Most clinicians consider identifying their patient as a given. So routine that there can be a lapse in concentration. Readers will be astonished to hear that in recent years there have been 105 incidents reported at the Women’s where there has been such a lapse. As Ruth Bergman points out in her article on page 4 the true incidence of misidentifying patients is not known. Another patient safety article concerns the age old issue of washing our hands to reduce nosocomial infection. Andrew Daley reports that the gap between doctors and nurses in handwashing compliance has widened again. In August 2008 it was nurses 73%, doctors 67% whereas in August 2009 it was 79% versus 51%! With regards to effective care, Huda Ismail reviews the management of trophoblastic disease in the Pharmacy section, and Jenny Taylor reviews the use of vitamin supplements in our pregnant patients. Her audit shows that pregnant women with poor diets who could benefit most from multivitamin supplements were the least likely to use them. Sobering stuff. Finally, many around the hospital will now be aware of the ISBAR tool for effective communication. Carol Vance’s and Claire Fitzgerald’s article is a concise reminder of the methodology. Please let us know what you think, both of our content this year and thoughts for future articles. Leslie Reti, editor [email protected] continued next page HeraldSun 25.5.08 continued from back page... Pharmacy news A single sperm with 23 chromosomes fertilises an egg with 23 chromosomes Normal conception Two sperm fertilise an egg. This results in a triploid conceptus with 69 chromosomes. Partial Mole This results in a conceptus with 46 chromosomes but all of them are derived from the father. Monospermic Complete Mole The paternal chromosomes double up The maternal chromosomes double up and This results in a conceptus with 46 chromosomes but again all of them are derived from the father. Fertilisation by two sperm Dispermic Complete Mole The maternal chromosomes are lost Fig 1. Genetic Origin of Hydatiform Mole Adverse reactions to chemotherapy (ADR) were common however few resulted in the delay of treatment. Only two patients required treatment cessation (Figure 3,4). ADR were similar in both main regimen as shown in Figure 5 Chemotherapy is an effective treatment for GTD. Resistance to methotrexate has been low and is effectively managed with other chemotherapy agents. Huda Ismail Senior Pharmacist, Oncology and ADR coordinator References 1. Gestational Trophoblastic disease, SOGC Clinical Practice Guidelines, No. 114, May 2002 continued next page Fig 2. GTD patients who received treatment 1 2 3 4 5 6 1 Low risk managed with MTX. 31 (66%) 2 Low risk resistent to MTX. 7 (1%) 3 Transferred to other hospital. 4 (8%) 4 Currently receiving treatment. 1 (2%) 5 Ultra-high risk. 1 (2%) 6 High risk treatment required. 1 (2%) Fig 5. Common ADR experienced by MTX and EMACO 9 8 7 6 5 4 3 2 1 0 infection dry eye mouth ulcer SOB pain nausea anaemia fatigue constipation headache drop in NPS rash EMACO group MTX group Fig 3. Tolerance to MTX treatment Fig 4. ADR experienced from EMACO treatment 5.0 4.5 4.0 3.5 3.0 2.5 2.0 1.5 1.0 0.5 0.0 1 Nil ADR. 28 (74%) 2 ADR result in hospital admission. 3 (8%) 3 ADR result in treatment cessation. 2 (5%) 4 ADR managed with medications. 5 (13%) Nil ADR ADR managed with medication ADR result in dose change or treatment delay ADR result in hospital admission 2 3 4 1
-
Upload
dannylewis7 -
Category
Documents
-
view
221 -
download
2
Transcript of Clinical Practice Review Issue7 July Aug Sept 09

Clinical Practice ReviewEditorial 1
Hand hygiene compliance 1
Vitamin and mineral supplements taken @ the Women’s 2
Right Patient – Right Care 4
ISBAR is here! 5
Pharmacy news 6
the Royal women’s hosPital quAlIty And SAfEty unIt nEWSlEttERissue 7 july, AuguSt,
SEPtEmBER 2009
1
hospital acquired infections, hand hygiene and an age-old problem: the renewed focus on improving
hand hygiene in recent years has
seen overall compliance rise from
20% at RWH two years ago (you
may remember the Herald Sun
headline at the time and RWH topping
the “Worst Offenders” list) to 75%
in the latest audit.
• TheWorldHealthOrganizations’
target is 55% and Victorian
hospitals are aiming for 60%.
While women’s hospitals have been
relatively spared from the multi-
resistant organisms (mRO) that are
commonplace in general hospitals,
RWH has observed an increase
in mRO burden.
• Meticuloushandhygiene
practices are essential to reduce
the spread of these mROs
as well as other pathogens.
Doctors versus nurses!multiple studies on hand hygiene
compliance across various institutions
confirm that doctors perform poorly
when compared with nurses. this is
despite the fact that nurses have more
opportunities for patient contact than
doctors. many theories for this have
been proposed but we will let you use
your imagination!
• Nurseshaveimprovedtheirhand
hygiene compliance at RWH
• Doctorshavefailedtomake
significant gains above 60%.
• Doctorshavetheopportunity
to spread more nosocomial
pathogens as they potentially
move between more patients
than do other staff.
• Poorcomplianceamongst
medical staff is reducing the
overall performance of RWH
when we benchmark with
other hospitals.
hand hygiene compliance
D09
-135
des
ign@
thew
omen
s O
ctob
er 2
009
5
gestational trophoblastic disease
(gtd) covers a spectrum of tumors
ranging from premalignant
(hydatidiform mole) to malignant
(invasive mole or choriocarcinoma).
Complete and partial hydatidiform
moles are the two most common
types of pre-malignant gtd and
both can progress to invasive moles.
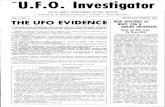
In a complete mole, an ovum devoid
of maternal nuclear dnA is fertilised
by 2 sperm or a single sperm –
it duplicates its chromosomes
to give a diploid complement
of male dnA. In a partial mole
the two sperms fertilise an ovum
with maternal nuclear dnA forming
a triploid conceptus (figure 1).
these proliferate to form abnormal
trophoblasts. the uterus enlarges
rapidly despite the absence of a fetus
and the placenta contains many cysts
to give a typical molar appearance.
maternal blood vessel formation
increases and facilitates metastatic
spread of the disease. Human
chorionic gonadotrophin (hCg)
is synthesised in the molar tissues
and therefore can be used
as a tumour marker to monitor
disease progression or response.
Invasive moles, choriocarcinomas
and placental site trophoblasts
are malignant tumours and are
collectively known as gestational
trophoblastic tumours1.
gtds are classified as low risk,
high risk and ultrahigh risk and
their medical management differs
based on the risk and resistance
to chemotherapy.
low risk patients are managed
with the methotrexate (mtX) and
calcium folinate regimen. Actinomycin
may be used as an alternative
if methotrexate is not tolerated.
High risk patients are managed
with the EmACO regimen, which
consists of Etoposide, methotrexate
and Actinomycin, given on alternate
weeks with Cyclophosphamide
and vincristine(Oncovin®).
ultra-high risk patients are
treated with the EmAPE regimen
which includes Etoposide,
high dose methotrexate and
Actinomycin, given on alternate
weeks with CisPlatin and
Etoposide with or without
intrathecal methotrexate.
All patients diagnosed with
molar pregnancy are recorded
in the Hydatidiform mole Registry.
Between 2002 and 2008,
a total of 649 patients were
diagnosed with molar pregnancy.
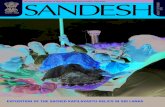
Only forty-eight (7%) patients
had persistent elevated hCg
and received medical treatment
(figure 2). thirty eight of those
patients received low risk
treatment – seven of them
developed resistance to methotrexate
and were switched on to the high
risk treatment regimen. In total ten
patients received high risk treatment
and only one patient received the
ultrahigh risk regimen.
Please let the associate editors have your views on the contents of this newsletter, or any other matters involving clinical practice which may be of interest to our readers.
huda ismail
treatment options for gestational trophoblastic disease
Susan Braybrook, telephone (03) 8345 2025 or email [email protected] further information http://www.thewomens.org.au for intranet users http://intranet.thewomens.org.au/qualityandsafety
Please let the associate editor have your views on the contents of this newsletter, or any other matters involving clinical practice which may be of interest to our readers.
for any further enquiries regarding Pharmacy news please contact [email protected]
ISBAR is here!
Carol Vance
Claire Fitzgerald
what is isBaR?ISBAR is a structured communication
tool that improves the quality
of information exchange when
discussing patients. the tool was
initially developed in the navy
to improve communication and
has since been adapted for medical
use. Inefficient communication
can compromise patient care
and using a standard approach
to communication decreases the
chance of forgetting relevant
information and helps to decrease
assumptions by making the reason
for the call obvious at the outset.
i identification
s situation
B Background
a assessment
R Request or
Recommendation
identify Identify yourself, the person
you are speaking to, the patient,
your location.
situation‘Spoil’ the story. Stating the
purpose of the call at the start
of the conversation helps the receiver
focus their attention appropriately
when listening to the story. If urgent,
make this clear from the start.
Background tell the story. Provide relevant
information only and remember,
less is more, particularly if the
receiver already knows the patient.
assessmentState what you think is going
on. give your interpretation
of the situation. Include your degree
of certainty - stating the obvious
is helpful. don’t leave the receiver
to guess what you are thinking
– tell them.
Request / RecommendationState what you want and
ask questions.
What you say for ‘situation’
may be a concise summary
of what you say for ‘assessment’
and ‘request’. this repetition
is helpful as it emphasises the
key purpose of the referral.
uses for isBaR• Inpatientoroutpatient
• Urgentornon-urgent
communications
• Conversationswithother
staff, either in person
or over the phone
- Particularly useful
in nurse – doctor
communication
- Also helpful in
doctor-doctor and
nurse-nurse
communication
• Discussionswithallied
health professionals
• Conversationswithpeers
• Asapromptfor
writing letters to other
care providers
• Escalatingaconcern
lanyard cards are available
as a reminder about ISBAR,
as well as notepads (which
are found on the gynaecology
wards) which may help
to organise your thoughts
before beginning your
communication. We encourage
you to give ISBAR a try and start
using it as a tool to improve
all your clinical conversations.
Carol Vance Principle Registrar quality and Safety fellow
Claire Fitzgerald Project manager Agree project
eDitoRial
The backbone of good (best) clinical practice remains patient centred care that is effective and safe. This edition has articles that address the last two of these. Most clinicians consider identifying their patient as a given. So routine that there can be a lapse in concentration. Readers will be astonished to hear that in recent years there have been 105 incidents reported at the Women’s where there has been such a lapse. As Ruth Bergman points out in her article on page 4 the true incidence of misidentifying patients is not known. Another patient safety article concerns the age old issue of washing our hands to reduce nosocomial infection. Andrew Daley reports that the gap between doctors and nurses in handwashing compliance has widened again. In August 2008 it was nurses 73%, doctors 67% whereas in August 2009 it was 79% versus 51%! With regards to effective care, Huda Ismail reviews the management of trophoblastic disease in the Pharmacy section, and Jenny Taylor reviews the use of vitamin supplements in our pregnant patients. Her audit shows that pregnant women with poor diets who could benefit most from multivitamin supplements were the least likely to use them. Sobering stuff. Finally, many around the hospital will now be aware of the ISBAR tool for effective communication. Carol Vance’s and Claire Fitzgerald’s article is a concise reminder of the methodology.
Please let us know what you think, both of our content this year and thoughts for future articles.
leslie Reti, editor [email protected] continued next page
HeraldSun 25.5.08
continued from back page...
Pharmacy news
A single sperm with 23 chromosomes fertilises an egg with 23 chromosomes
Normal conception
Two sperm fertilise an egg. This results in a triploid conceptus with 69 chromosomes.
Partial Mole
This results in a conceptus with 46 chromosomes but all of them are derived from the father.
Monospermic Complete Mole
The paternal chromosomes double up
The maternal chromosomes double up
and
This results in a conceptus with 46 chromosomes but again all of them are derived from the father.
Fertilisation by two sperm
Dispermic Complete Mole
The maternal chromosomes are lost
Fig 1. Genetic origin of hydatiform mole
Adverse reactions to chemotherapy
(AdR) were common however
few resulted in the delay
of treatment. Only two patients
required treatment cessation
(figure 3,4).
AdR were similar in both main regimen
as shown in figure 5 Chemotherapy
is an effective treatment for gtd.
Resistance to methotrexate has been
low and is effectively managed with
other chemotherapy agents.
huda ismail Senior Pharmacist, Oncology and AdR coordinator
References1. gestational trophoblastic disease,
SOgC Clinical Practice guidelines,
no. 114, may 2002
continued next page
Fig 2. GtD patients who received treatment
1234
5
6
1 Low risk managed with MTX. 31 (66%)
2 Low risk resistent to MTX. 7 (1%)
3 Transferred to other hospital. 4 (8%)
4 Currently receiving treatment. 1 (2%)
5 Ultra-high risk. 1 (2%)
6 High risk treatment required. 1 (2%)
Fig 5. Common aDR experienced by mtX and emaCo
9876543210
infec
tion
dry e
yem
outh
ulce
r
SOB
pain
naus
eaan
aem
iafa
tigue
cons
tipat
ionhe
adac
hedr
op in
NPS
rash
EMACO group MTX group
Fig 3. tolerance to mtX treatment
Fig 4. aDR experienced from emaCo treatment
5.04.54.03.53.02.52.01.51.00.50.0
1 Nil ADR. 28 (74%)
2 ADR result in hospital admission. 3 (8%)
3 ADR result in treatment cessation. 2 (5%)
4 ADR managed with medications. 5 (13%)
Nil ADR ADR managed with medication
ADR result in dose change or treatment delay
ADR result in hospital admission
2
3
4
1

2 3 4
Ruth Bergman
continued from front page... continued from page 2...
An audit of suitability of vitamin
and mineral supplements taken
by pregnant women.
Vitamin and mineral use is common
in pregnant women but are women
taking supplements that correlate
with their nutritional deficiencies?
the aim of this audit was
to check how supplement use
related to woman’s individual
needs as well as to nutrients
that are at risk in pregnant
women in general such as iron,
folic acid and iodine.
218 pregnant outpatients
routinely seen by dieticians
at RWH had assessment of
• usualdietaryintake
• nutritionalsupplementuse–
both self prescribed and
prescribed by health professionals
• biochemistrythatcouldindicate
nutritional deficiency such
as iron deficiency indicators,
Vitamin B12 and folate levels,
using Clara or laboratory results
filed in patients records.
this was not a random sample
as the women had been referred
to dieticians for reasons such
as weight control or diabetes
or were screened because they were
attending higher risk antenatal clinics
such as multiple Pregnancy, WAds
or young Women’s Clinic.
from 2005 the quality and Safety
unit at the Women’s has received
105 reports of patient safety
incidents associated with the wrong
identification of a woman or baby.1
So far we have been lucky as none
have resulted in a major outcome,
but the potential is there. the true
incidence and probability of wrongly
identifying a patient is unknown but
it is of enough concern for the
Australian Commission on Safety
and quality to highlight it as a national
‘stand-out opportunity to improve
patient safety’2.
At the Women’s, the occurrence
of mislabelled specimens, duplicate
medical records, unlabelled
medicines charts, incorrect In Patient
management (IPm) registration details
coupled with the wrong person’s Id
stickers in a medical record, indicate
the need for a hospital wide focus on
correct positive patient identification.
Case studies
• Awomaninthebirthcentrehad
a post partum haemorrhage.
In preparation for theatre, one
person collected a cross match
blood specimen and wrote
up a request form, whilst another
labelled the specimen with Id
stickers from the wrong medical
record. the wrong blood type
was detected by pathology.
• Awoman’snamewascalled;
she came in to the outpatient
procedure room accompanied by
her husband who explained he will
interpret for her. the procedure
was explained and a cystoscopy
performed. A short while later
another woman came to the desk
complaining she had been waiting
a long time for a cystoscopy.
Staff realised a procedure was
performed on the wrong person.
• Awomanarrivedintheatre.During
the team time-out checking
process the operating room team
were alerted of a potential problem
as her medical record contained
details of births and procedures
that were not hers. With the
assistance of the woman it was
realised that two medical records
were merged, hers and her sister-
in-law who share the same
surname and date of birth, but one
was meghan and the other megan.
“from 2005 the Quality and Safety unit at The Women’s has received 105 reports of patient safety incidents associated with the wrong identification
of a woman or baby”
Vitamin and mineral supplements taken @ the Women’s
Jenny taylor
Right Patient – Right Care
What can you do?1. learn the WHO “five moments for
hand hygiene” and incorporate these
into your daily routine.
2. Review Hand Hygiene Australia’s
recommendations for medical Staff:
http://www.hha.org.au/userfiles/
file/HHAjulymanual 2009(1).pdf
Section 5.3 (page 45)
3. Perform the “Hand Hygiene
competencyquiz”(takes5minutes)
at http://intranet.thewomens.
org.au/ClinicalEducation
Competency Assessment
4. Play the “Wi 5” game: http://
www.rch.org.au/washup/prof.cfm?
doc_id=12968
5. model appropriate practices
for more junior staff and
medical students.
6. Work with senior nursing staff to
assist with enforcing HH compliance.
7. Review the Washup website
at www.washup.org.au
hand hygiene: your example matters
Colleagues, trainees, and other
staff watch what you do:
• Researchhasshownthatthe
actions of clinicians influence
the behavior of others.
• Showyourcolleaguesthat
hand hygiene is an important
part of quality care.
your patients and their families
watch you too:
• Youractionssendapowerful
message.
• Showyourpatientsthatyou
are serious about their health.
from Centers for disease Control
and Prevention (uSA)
Dr andrew Daley departments of microbiology & Infectious diseases and Infection Control
this was a snapshot of what the
women were doing at the time they
were seen. they may have been
at any stage in the pregnancy but
second trimester was the most
common time.
Resultssupplement use was common with
55% of the women taking multivitamin
preparations. Elevit was the most
popular, used by 47% of those taking
a multivitamin supplement, followed
by Blackmores Pregnancy and
Breastfeeding gold at 33%. the
remaining 20% were taking a variety
of at least 9 other brands.
“Supplement use was common with 55% of the women taking multivitamin preparations”
Supplements vary in content of
significant nutrients such as iron,
vitamin d, omega 3 and vitamin B12.
One of the reasons Elevit is popular is
because it contains a substantial iron
dose, however in contrast to other
pregnancy multivitamins, it contains
no iodine (at this stage). Iodine is one
of the nutrients most needed from a
supplement as there is mild deficiency
in most parts of Australia. Even bread
fortification (commencing September
2009) will not meet the iodine needs
of many pregnant women. 33%
of the women surveyed were getting
supplemental iodine either from
multivitaminsoriodizedsalt
77% of the women took folic acid
supplements at some stage during
the pregnancy (alone or in multivitamin
or iron preparations), however only
29% started it before conception.
most of the remaining 48%
commenced after they knew
they were pregnant and thought
this was appropriate.
43% had indicators of iron deficiency
sometime during the pregnancy
to date. At the time of the audit only
46% of iron deficient women were
taking iron supplements in doses
large enough to be likely to correct
deficiency i.e. 60mg or more per day.
69% of the women had test results
available for vitamin d. 48% of this
sample were deficient when first
tested, with 69% of deficient women
on supplements of 1000 Iu or more.
Iron, iodine, calcium and folic acid
were common dietary deficiencies.
Women with biochemistry indicating
iron or Vitamin B12 deficiency were
twice as likely to have inadequate
diets (by dietary recall) and were also
less likely to be taking multivitamins.
In contrast women with adequate
diets were twice as likely to use
multivitamin supplements as those
with inadequate diets.
“pregnant women with
poor diets who could benefit
most from multivitamin
supplements were the least
likely to use them”
In conclusion
• pregnantwomenwithpoordiets
who could benefit most from
multivitamin supplements were
the least likely to use them.
• multivitaminsupplementusers
may still miss out on at risk
nutrients. there is no single
supplement that contains iron
(in significant amounts) as well
as folic acid and iodine.
• mostwomenwereunawarethat
folic acid needs to be started
before pregnancy
• manyiron-orVitaminDdeficient
women were not taking
supplements. Whether this was
due to non-prescription or non
compliance was not assessed.
Jenny taylor department of nutrition and dietetics, the Royal Women’s Hospital [email protected]
RWH nov 2007 mar 2008 Aug 2008 nov 2008 mar 2009 Aug 2009
Overall compliance 20% 44% 73% 77% 73% 75%
nurses 19% 48% 73% 80% 78% 79%
Doctors 24% 67% 61% 50% 51% 21%
Comparison of levels of ‘at risk’ nutrients in a sample of multivitamins suitable for pregnancy
number of tablets or capsules per daily dose
Cost per day
nutrient content per daily dose
Folic acid 600µg*
iodine 220 µg* 250 µg (who)
iron 27mg*
Vitamin D 500iu*
B12 2.6µg*
omega 3 115-430 mg
Blackmores Pregnancy and Breasfeeding gold 2 $0.92 500 250 10 500 3 300
Blackmores I-folic 1 $0.13 500 250
Cenovis Pregnancy and Breastfeeding formula 2 $0.53 500 150 10 - 4 340
Elevit 1 $0.69 800 - 60 500 4 -
fabfol Plus 1 $0.44 500 150 12 200 4 -
fefol multipreg 1 $0.58 500 200 12 200 4 252
myadec multivitamins and minerals 1 $0.13 - 150 5 440 6.3 -
natal Plus 2 $0.83 500 270 10 500 500 -
nature’s Own Pregnancy Platinum 1 $0.45 500 250 5 200 100 150
nature’s Way Pregnancy Smart 2 $0.50 500 150 10 - 3 340
Swisse Pregcel 1 $0.63 500 250 5 200 2.6 -
*Recommended dietary intake for healthy women. Recommendations may be different if deficiency is present
steps for positive identification
Positive identification involves asking
the woman in front of you to state her
first name, surname and date of birth.
this information is checked against the
patient identification wristband(s).
In the outpatient areas, and in
situations where there is no wristband,
(e.g. Pauline gandel Women’s Imaging
Centre, pathology or women phoning
for test results), remember to check
this information against documented
patient identification details such
as the medical record, request form
or databases such as ClARA and
IPM.Asimpleprocess;notdissimilar
to the questions a bank asks prior
to providing any information over
the telephone.
steps for right person, right care,
right site and side
In the outpatient and inpatient
setting the verification of the correct
person, procedure and site includes
clerical staff registering and making
a booking in IPm, admitting staff,
clinicians and the person in charge
of the procedure asking the woman
to state her first name, surname,
date of birth and type of procedure
(if relevant, what site and side
is involved).
this information is checked for accuracy
against the consent or procedural
request form and appropriate diagnostic
images (when available). In theatre this
process is called ‘team time Out’ where
a standard formal process is followed
bythewholeteam;theanaesthetist,
surgeon and theatre nurses.
the matching of the correct person,
procedure, site and side occurs
at all stages of outpatient and inpatient
contact. that is, when a procedure
isbooked;atthetimeofadmission;
duringpreparationforaprocedure;
upon admission to a department where
the procedure is to be conducted
(e.g. Pauline gandel Women’s Imaging
Centre, day Chemotherapy, Pregnancy
day Care Centre) and again on entry
to the procedural room and indeed
anytime a woman or baby moves within
the hospital or is transferred to another
hospital location.
Ruth Bergman
Clinical Incident Co-Ordinator
References1. RISKmAn incident database, report
by patient identification classification2. Australian Commission on Safety and quality
inHealthCare2009IdentificationofAdults;Identification of Babies Women’s Hospital Procedure located on the Intranet.
andrew Daley