
CLINICAL PEDIATRIC DENTISTRY I DSV 441 CHAPTER 18 RESTORATIVE DENTISTRY (364-387) STAINLESS STEEL...
16
CLINICAL PEDIATRIC DENTISTRY I DSV 441 CHAPTER 18 RESTORATIVE DENTISTRY (364-387) STAINLESS STEEL CROWNS FOR POSTERIOR TEETH McDonald, Avery, Dean. Dentistry For The Child And Adolescent, 8th Ed. 23 Tuesday 7\42015 1:00 pm-2:00 pm OTHMAN AL-AJLOUNI 1
-
Upload
peregrine-mclaughlin -
Category
Documents
-
view
229 -
download
3
Transcript of CLINICAL PEDIATRIC DENTISTRY I DSV 441 CHAPTER 18 RESTORATIVE DENTISTRY (364-387) STAINLESS STEEL...
CLINICAL PEDIATRIC DENTISTRY I DSV 441CHAPTER 18 RESTORATIVE DENTISTRY
(364-387) STAINLESS STEEL CROWNS FOR POSTERIOR TEETH
McDonald, Avery, Dean. Dentistry For The Child And Adolescent, 8th Ed.
23
Tuesday 7\42015
1:00 pm-2:00 pm
OTHMAN AL-AJLOUNI 1
LECTURE OUTLINE
PREPARATION OF THE TOOTH
SELECTION OF CROWN SIZE
CONTOURING OF THE CROWN (When Necessary)
2
LEARNER OBJECTIVES
At the end of the lecture student should know
How to do preparation for SSC
How to select SSC
How to fit and cement SSC
3
S T A I N L E S S S T E E L C R O W N S F O R P O S T E R I O R T E E T H
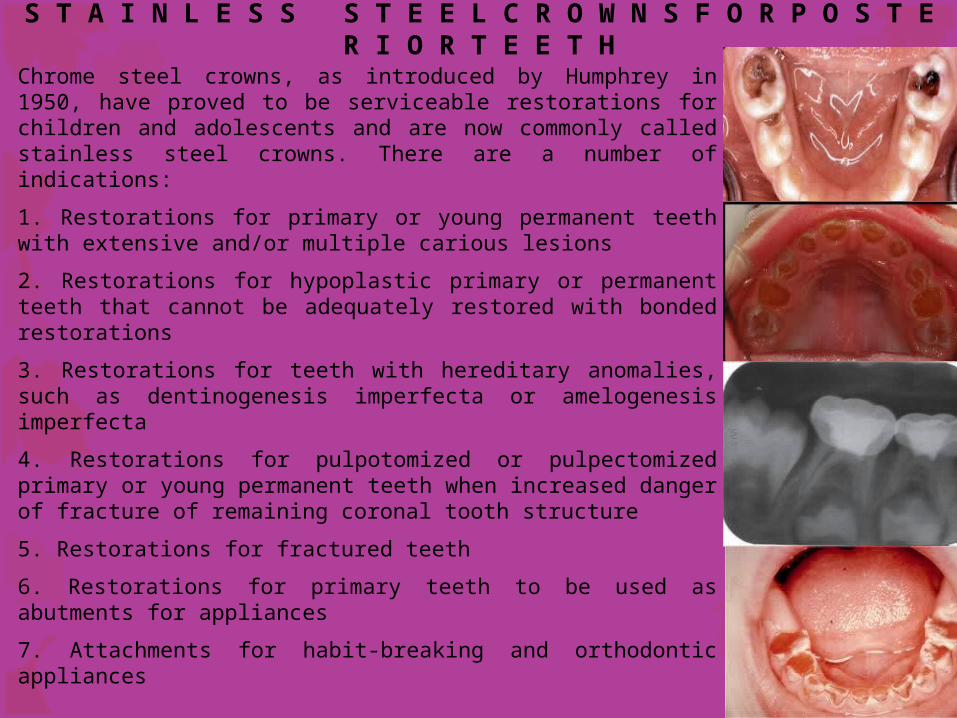
Chrome steel crowns, as introduced by Humphrey in 1950, have proved to be serviceable restorations for children and adolescents and are now commonly called stainless steel crowns. There are a number of indications:
1. Restorations for primary or young permanent teeth with extensive and/or multiple carious lesions
2. Restorations for hypoplastic primary or permanent teeth that cannot be adequately restored with bonded restorations
3. Restorations for teeth with hereditary anomalies, such as dentinogenesis imperfecta or amelogenesis imperfecta
4. Restorations for pulpotomized or pulpectomized primary or young permanent teeth when increased danger of fracture of remaining coronal tooth structure
5. Restorations for fractured teeth
6. Restorations for primary teeth to be used as abutments for appliances
7. Attachments for habit-breaking and orthodontic appliances4

S T A I N L E S S S T E E L C R O W N S F O R P O S T E R I O R T E E T H
Randall compared performance of crown restorations with that of multisurface amalgam restorations. Crown restorations were superior to amalgam restorations in treatment of multisurface cavities in primary molars.
Especially in children at high risk for caries.
Stainless steel crown (SSC) is an extremely durable restoration.... Children with extensive decay, large lesions or multiple surface lesions in primary molars should be treated with SSC.
Because of protection from future decay provided by their feature of full coverage and their increased durability and longevity, strong consideration should be given to use of SSCs in children who require general anesthesia.
Finally, a strong argument for use of SSC restoration is its cost effectiveness based on its durability and longevity.
5
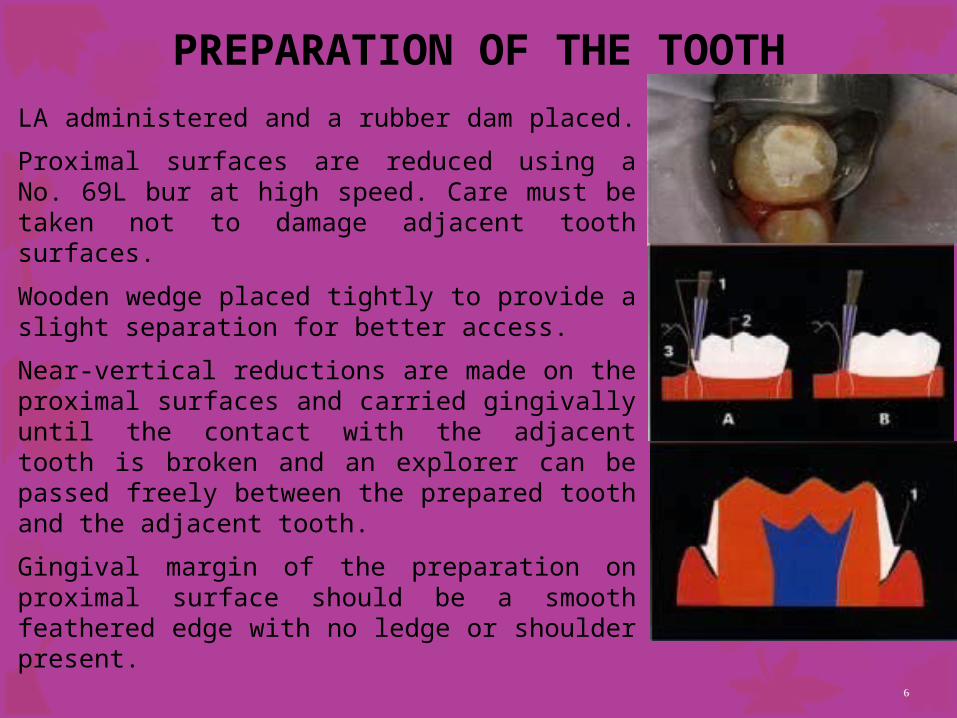
PREPARATION OF THE TOOTHLA administered and a rubber dam placed.
Proximal surfaces are reduced using a No. 69L bur at high speed. Care must be taken not to damage adjacent tooth surfaces.
Wooden wedge placed tightly to provide a slight separation for better access.
Near-vertical reductions are made on the proximal surfaces and carried gingivally until the contact with the adjacent tooth is broken and an explorer can be passed freely between the prepared tooth and the adjacent tooth.
Gingival margin of the preparation on proximal surface should be a smooth feathered edge with no ledge or shoulder present.
6

PREPARATION OF THE TOOTHCusps and occlusal portion be reduced with a No. 69L bur revolving at high speed. The general contour of occlusal surface is followed, and approximately 1 mm of clearance with the opposing teeth is required.
The No. 69L bur at high speed used to remove all sharp line and point angles.
It is usually not necessary to reduce buccal or lingual surfaces; in fact, it is desirable to have an undercut on these surfaces to aid in retention of contoured crown. In some cases, however, it may be necessary to reduce distinct buccal bulge, particularly on first primary molar.
If any carious dentin remains after these steps in crown preparation are completed, it is excavated next. 7

SELECTION OF CROWN SIZEThe smallest crown that completely covers preparation should be chosen. Spedding has advocated adhering to two important principles that will help consistently to produce well-adapted stainless steel crowns. First, operator must establish correct occlusogingival crown length; and second, crown margins should be shaped circumferentially to follow natural contours of tooth's marginal gingivae. The crown should be reduced in height, if necessary, until it clears occlusion and is approximately 0.5 to 1 mm beneath free margin of gingival tissue..
8
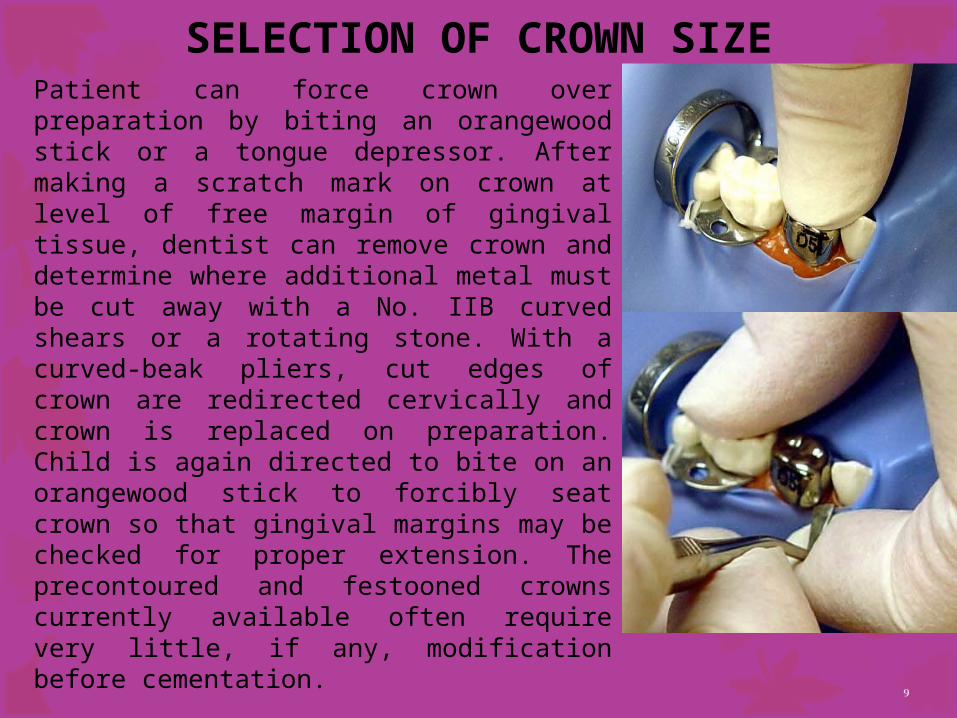
SELECTION OF CROWN SIZEPatient can force crown over preparation by biting an orangewood stick or a tongue depressor. After making a scratch mark on crown at level of free margin of gingival tissue, dentist can remove crown and determine where additional metal must be cut away with a No. IIB curved shears or a rotating stone. With a curved-beak pliers, cut edges of crown are redirected cervically and crown is replaced on preparation. Child is again directed to bite on an orangewood stick to forcibly seat crown so that gingival margins may be checked for proper extension. The precontoured and festooned crowns currently available often require very little, if any, modification before cementation. 9

CONTOURING OF THE CROWN (WHEN NECESSARY)
A crown-contouring pliers with a ball-and-socket design is used at cervical third (if loosely fitting, start at middle third) of buccal and lingual surfaces to help adapt margins of crown to cervical portion of tooth. The handles of pliers are tipped toward center of crown, so that metal is stretched and curled inward as crown is moved toward pliers from opposite side. A curved-beak pliers is used to further improve contour on buccal and lingual surfaces.
10
CONTOURING OF THE CROWN (WHEN NECESSARY)
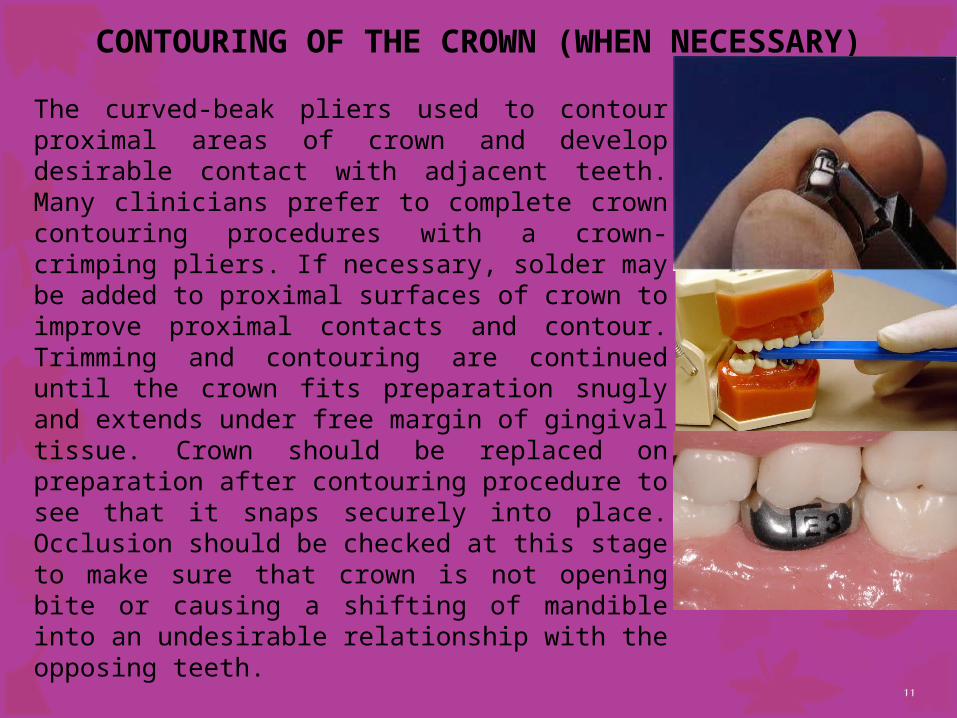
The curved-beak pliers used to contour proximal areas of crown and develop desirable contact with adjacent teeth. Many clinicians prefer to complete crown contouring procedures with a crown-crimping pliers. If necessary, solder may be added to proximal surfaces of crown to improve proximal contacts and contour. Trimming and contouring are continued until the crown fits preparation snugly and extends under free margin of gingival tissue. Crown should be replaced on preparation after contouring procedure to see that it snaps securely into place. Occlusion should be checked at this stage to make sure that crown is not opening bite or causing a shifting of mandible into an undesirable relationship with the opposing teeth.
11

CONTOURING OF THE CROWN (WHEN NECESSARY)
The final step before cementation is to produce a beveled gingival margin that may be polished and that will be well tolerated by gingival tissue. A rubber abrasive wheel can be used to produce smooth margin. On occasion best-fitting crown may need to be modified to produce a more desirable adaptation to prepared cervical margin. The oversized crown may be cut and the cut edges overlapped.
12
CONTOURING OF THE CROWN (WHEN NECESSARY)
The crown is removed from tooth and overlapped material repositioned and welded. A small amount of solder is flowed over outside margin. Crown is finished in previously recommended manner and cemented to prepared tooth.
If tooth is too large for largest crown, a similar technique may be helpful. Crown cut on buccal or lingual surface. After crown has been adapted to prepared tooth, an additional piece of 0.004-inch stainless steel band material may be welded into place. A small amount of solder should be added to outer surface of margins. Crown may then be contoured in usual manner, polished, and cemented into place.
13
Tuesday, April 18, 2023Professor Othman Al-Ajlouni14

Pre- Operative: Post- Operative:
Tuesday, April 18, 2023 Professor Othman Al-Ajlouni 15

THANK YOU


















