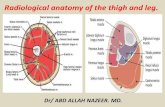
Anatomy of the Front Limb Small Animal. Anatomy of the Front Leg Scapula.
Upload
aunum-iqbalCategory
view
310download
0
Clinical Anatomy
Dr. Aunum IqbalDemonstrator
Sialkot Medical College

Tibial Fractures

Types:1.Compound/Open fractures
2.Transverse march/stress fractures
3.Diagonal fractures

Compound/open fracturesCommonest site: junction of upper 2/3rds and lower 1/3rd of shaft of Tibia
Cause: Direct trauma to leg
Poor blood supply in this area leads to non-union of fractured ends
This area is subcutaneous, thus fracture is of open/ compound type, i.e where skin is damaged as well

Transverse march/stress fracturesCommonest site is lower 1/3rd of shaft of Tibia
Cause: long hikes without training

Diagonal fracturesCommonest site: Junction of upper 2/3rds and lower 1/3rd of shaft of Tibia
Cause: Torsion (twisting) of leg during skiing
Associated fracture of Fibula
Shortening of limb due to overriding of fractured ends

Important bursae
and Bursitis

Bursae around knee joint
1. Deep suprapatellar bursa (b/w Femur and Quadriceps tendon; communicates with synovial membrane of knee joint)
2. Subcutaneous prepatellar bursa (b/w Patella and skin)
3. Deep infrapatellar bursa (b/w Tibia and ligamentum patellae)
4. Subcutaneous infrapatellar bursa (b/w lower half of Tibial tuberosity and skin)
5. Popliteal bursa (b/w tendon of Popliteus and capsule of knee joint; communicates with synovial membrane of knee joint)
6. Semimembranosus bursa (beneath the Semimembranosus tendon)
7. Pes anserinus/subsartorial bursa (beneath the Sartorius, Gracilis and Semitendinosus tendons)
Quadriceps femoris tendon
Ligamentum patellae
Patella
67
Pes anserinus
Popliteus
Semimembranosus

Pes anserinusa.k.a. Goose foot
Conjoined tendons of 3 muscles that insert onto the medial surface of upper part of shaft of Tibia: Sartorius, Gracilis and Semitendinosus
The name, "goose foot", arises from the 3 pronged manner in which the conjoined tendon inserts onto the tibia.
Behind this common insertion, Pes anserinus bursa is present.

1. Subcutaneous calcaneal bursa (b/w skin and Calcaneum)
2. Retrocalcaneal bursa (b/w Achilles tendon and Calcaneum) – Inflammation is called Calcaneal Bursitis
3. Subcutaneous bursa of medial malleolus of Tibia
Bursae around ankle
joint

Calcaneal Tendinitis
and Ruptured Achilles tendon

• Inflammation of Achilles tendon
• Cause: Running injuries lead to tearing of Collagen fibers in the tendon
• Symptoms: Pain during walking
• If untreated, it may lead to rupture of Achilles tendon

Calcaneal tendon reflex / Ankle reflex

• Achilles tendon is struck with a hammer, just above Calcaneum, while the foot is dorsiflexed
• Normal result: Plantar flexion at ankle joint – showing intact spinal nerves
• Spinal nerves tested: S1 and S2
• If S1 or S2 spinal nerves are damaged, this reflex would be absent i.e. no plantar flexion

Fabella and
Fabellar syndrom
e

Fabella: (little bean-Latin)
A small sesamoid bone found in the tendon of lateral head of the Gastrocnemius muscle behind the lateral condyle of the femur
Present in 3-5% of people
Fabellar Syndrome:
Tenderness over the posterior aspect of the lateral Femoral condyle due to repetitive friction of Fabella over it
Fabella

Musculocutaneous/ venous
pump

• a.k.a second heart/ peripheral heart
• Contraction and relaxation of deep muscles of posterior compartment of leg, causes pumping of blood
• Blood from superficial veins goes towards deep veins and then towards the heart
• This direction of blood flow is due to the presence of one-way valves in the veins
• This mechanism increases venous return to the heart: hence prevents pooling of blood in the peripheries

Compartment
Syndrome

• Posterior compartment of leg has two groups of muscles; superficial and deep.
• Deep group of muscles lie in a tightly packed space; the deep compartment
• Nerves and vessels of posterior compartment of leg pass through the deep compartment
• When swelling occurs, it causes compression of these nerves and vessels, leading to Compartment Syndrome
• It leads to: • Necrosis (death) of muscles – due to damaged arterial supply
• Paralysis of muscles – due to compression of nerves

Handy points
• Triceps surae/Calf: Medial and lateral bellies of Gastrocnemius and Soleus
• Muscles of posterior compartment mainly produce plantar flexion at ankle joint
• Damage to Tibial nerve will cause loss of plantar flexion
• Plantar flexion is stronger than dorsiflexion
• Muscles involved in standing on tiptoes: Triceps surae (93% force)
• Nerve involved in standing on tiptoes: Tibial nerve
• Damage to Tibial nerve: Patient can not stand on tiptoes

Handy points
Tibia - Shin bonePatella - Knee cap
Calcaneum - Heel bone
Plantaris - Freshman's nerveTriceps surae/Calf: Medial and lateral bellies of Gastrocnemius and SoleusPes anserinus: Common insertion of
Sartorius, Gracilis and Semitendinosus on Tibia
Anti-gravity muscle in posterior leg: Soleus
Popliteus – unlocking of knee joint by 5 degree lateral rotation of Femur on Tibia
Achilles tendon – largest tendon in bodyPatella – largest sesamoid bone in body

DIFFERENCE BETWEEN ACTIONS OF GASTROCNEMIUS AND SOLEUS:• Gastrocnemius: Plantar flexion at
ankle joint and flexion at knee joint
Soleus: Plantar flexion at ankle joint only
• Muscle for walking and running: Soleus
Muscle for long jump: Gastrocnemius
• Gastrocnemius can plantar flex with the extended knee. When knee is flexed, Soleus causes plantar flexion
• Soleus: anti gravity muscle; helps in standing
• Line of gravity passes anterior to Tibia in leg
• Therefore gravity tends to pull the body forward over the feet
• It is prevented by contraction of Soleus
• During standing on both the legs, Soleus is continuously active


Thank you!