Clinical anatomy of elbow
42
CLINICAL ANATOMY OF ELBOW JOINT DR. RAJESH ARORA PROFESSOR ANATOMY
-
Upload
mrinal-joshi -
Category
Healthcare
-
view
565 -
download
2
Transcript of Clinical anatomy of elbow

CLINICAL ANATOMY OF ELBOW JOINT
DR. RAJESH ARORAPROFESSOR ANATOMY

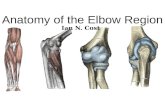
ELBOW JOINT Compound joint Hindge joint Cubital Articulation humero-ulnar humero-radial superior radio-ulnar joint

BONY STRUCTURE OF ELBOW

HUMERUS LOWER END

HUMERO-ULNAR PART It is articulation between trochlea of humerus and
trochlear notch of ulna The medial edge of trochlea is 6mm beyond the lateral
edge Plane of the joint is 2cms distal to intercondylar line
slopes downwards and medially Two nonarticular depressions coronoid fossa and
olecrenon fossa are present in relation to this articulation
Trochlear notch of ulna is reciprocally saddle shape and formed by the articular surfaces of olecrenon and coronoid processes

HUMERO-RADIAL PART Structurally it is a ball and socket type
of joint. The ball is represented by capitulum of
humerus and socket is by articular surface of disc like head of the radius
In full flexion head of the radius lodges radial fossa above the capitulum.

the annular ligament binds the head of the radius to the radial notch of the ulna forming the proximal radioulnar joint – this is a pivot joint allowing for pronation and supination

RELATIONS

LIGAMENTS OF ELBOW JOINT
Capsular ligament Ulnar collateral ligament or Medial
ligament Radial collateral ligament or Lateral
ligament

FIBROUS CAPSULE Fibrous capsule completely envelop the
joint. It is attached to the lower end of
humerus in a continuous line, which excludes the two epicondyles but include three fossae.
Cushions of extra-synovial fat fill up the three fossae.

ULNAR COLLATERAL LIGAMENT UCL is triangular in shape and extends
from medial epicondyle to medial margin of trochlear notch. The ligament consists of three bands, Anterior Posterior and Inferior
UCL is overlapped by Triceps ,FCU , FDS and Ulnar nerve.

ULNAR COLLATERAL LIGAMENT

RADIAL COLLATERAL LIGAMENT RCL is triangular and extends from
lateral epicondyle to annular ligament. It is related to supinator and ECRB

RADIAL COLLATERAL LIGAMENT

SYNOVIAL MEMBRANE

CARRYING ANGLE
The angle between the long axes of the humerus and the long axes of ulna when the forearm is supinated
This is called carrying angle because it allows the forearm to angle away from the body when a load is carried in the hand
Carrying angle is generally greater in females than in males

Carry Angle of the Elbow The angle between the long axes of
the humerus and the ulna when the arm is in an anatomical position
This is called this because it allows the forearm to angle away from the body when a load is carried in the hand
Carrying angle is generally greater in females than in males

RELATIONS OF ELBOW JOINT In front-Brachialis, tendon of biceps, median
nerve and brachial artery. Behind- Triceps and anconeus. Medially-common origin of superficial
flexors, Flexor carpi ulnaris and ulnar nerve. Laterally- common origin of superficial
extensors, supinator, extensor carpi radialis brevis, radial nerve with its superficial and deep branches

ANTERIOR RELATIONS

ARTERIAL SUPPLY Peri-articular branches of anastomosis
around elbow joint. NERVE SUPPLY Musculo-cutaneous nerve through
branch to Brachialis Radial nerve through nerve to
anconeous Ulnar nerve

MOVEMENTS Flexion- (C5 and C6) range is about 150
degree when flexor surface of arm and forearm approximate
Chief flexor is brachialis, biceps when forearm is supinated act as spurt muscle, brachioradialis in midprone position act as shunt muscle.

MOVEMENTS AT ELBOW JOINT

EXTENSION Extension-(C7 and C8) reached when
arm and forearm assume straight line. It makes the joint close-packed
It is performed by triceps, anconeus and assisted by gravity

BURSAE AROUND ELBOW JOINT Above the olecrenon, between the
triceps tendon and capsule of the joint. A subcutaneous bursa on the dorsal
triangular surface of olecrenon process. Between the biceps tendon and the
smooth anterior part of radial tuberosity.

BURSAE AROUND ELBOW JOINT

OLECRANON BURSITIS the olecranon bursa
is the largest bursa in the elbow and sits just over the olecranon process
injury results due to a direct fall, constant irritation, or infection

an acutely inflamed bursa will rapidly swell, show signs of redness and increased heat
often termed golf ball swelling the bursa may become infected – it
will be swollen and hot to touch along with a possible fever , pain , tenderness and restricted range of motion.


ELBOW DISLOCATION / SUBLUXATION Ulnar dislocation- It occurs in hyperextension ( Fall on
hand elbow extended) with violent twisting action of the ulna .This needs a tremendous amount of force
More common displacement is of radial head especially in children , swinging of children by their arms , may cause radial head to snap out of the annular ligament

severe pain with loss of functions , cracking or snapping sensation , rapid swelling , obvious deformity and inability to move elbow
90 % posterior , management is important to avoid long term disabilities


ELBOW STRAIN Elbow strains usually the result of
attempting to overcome large force with muscles
inadequate warm-up , excessive training (past point of fatigue)
common with biceps brachii, brachiallis, triceps
pain and point tenderness over the injury site, reduced strength and ROM

ELBOW SPRAIN usually the result of fall on extended
arm, producing a hyperextension of elbow
or through a valgus/varus force may be due to a repetitive force that
irritate or tear the ligaments pain , local tenderness . pain and or
laxity with stressing of the ligament, decreased ROM

MEDIAL EPICONDYLITIS
little league elbow or golfer’s elbow
repetitive motions with poor technique, muscular weakness or anatomical weakness
often seen in the acceleration phase of throwing

valgus force is placed on the elbow, which strains the flexor muscle , the ulnar collateral ligament and possibly the ulnar nerve.
swelling at the medial epicondyle, point tenderness, pain on resisted wrist flexion and pronation
tingling and numbness may be felt if the ulnar nerve is involved

MEDIAL EPICONDYLITIS

LATERAL EPICONDYLITIS tennis elbow most common overuse injury in the
elbow this condition is typically due to
eccentric overloading of the extensor muscles as seen in the deceleration phase of throwing or the tennis stroke
pain will be located on the lateral epicondyle , it may be swollen and the pain will increase with resisted wrist extension

Contributing factors to tennis elbow
lack of experience poor technique on backhand heavy stiff racquet ( 12 - 12.5 seem
to be best) grip size racquet strings to tight( 2-3 lbs. best) playing surface ( ball bounces more
off cement)

CUBITAL TUNNEL SYNDROME
impingement of ulnar nerve in cubital tunnel of the elbow ( through ulnar groove and under the ulnar collateral ligament)
here the nerve is vulnerable to compression and tensile stress caused by trauma

sharp pain along medial aspect forearm, tingling and numbness into ring and little finger of hand
signs and symptoms reproduced by tapping over ulnar groove

SUPRACONDYLAR FRACTURE OF HUMERUS

THANKS