Cirrhosis and Liver Cancer Mortality in the United States · 2012. 2. 18. · Confidential: For...
32
Confidential: For Review Only Cirrhosis and Liver Cancer Mortality in the United States 1999-2015: An Observational Study Journal: BMJ Manuscript ID BMJ.2018.043691 Article Type: Research BMJ Journal: BMJ Date Submitted by the Author: 12-Feb-2018 Complete List of Authors: Tapper, Elliot; University of Michigan, Parikh, Neehar; University of Michigan Keywords: liver disease, hepatitis, falls, alcohol, hepatocellular carcinoma https://mc.manuscriptcentral.com/bmj BMJ
Transcript of Cirrhosis and Liver Cancer Mortality in the United States · 2012. 2. 18. · Confidential: For...

Confidential: For Review Only
Cirrhosis and Liver Cancer Mortality in the United States
1999-2015: An Observational Study
Journal: BMJ
Manuscript ID BMJ.2018.043691
Article Type: Research
BMJ Journal: BMJ
Date Submitted by the Author: 12-Feb-2018
Complete List of Authors: Tapper, Elliot; University of Michigan, Parikh, Neehar; University of Michigan
Keywords: liver disease, hepatitis, falls, alcohol, hepatocellular carcinoma
https://mc.manuscriptcentral.com/bmj
BMJ

Confidential: For Review Only
��
�
�
�
�
Cirrhosis and Liver Cancer Mortality in the United States 1999-2015: An
Observational Study
Elliot B. Tapper MD (1,2) and Neehar D Parikh MD MS (1,2)
1. Division of Gastroenterology and Hepatology, University of Michigan
2. Gastroenterology Section, VA Ann Arbor Healthcare System, Ann Arbor
�
Keywords: Liver disease, hepatitis, falls, alcohol, liver cancer
Word count: 2,681
Corresponding author: Elliot B. Tapper, MD 3912 Taubman, SPC 5362
1500 E Medical Center Dr Ann Arbor, MI 48109 T: (734) 647-9252 F: (734) 936-7392 e: [email protected] Disclosure: 1. Elliot Tapper is the guarantor of this article 2. Roles
a. Concept: Tapper, Parikh b. Analysis: Tapper, Parikh c. Data acquisition: Tapper, Parikh d. Writing: Tapper, Parikh
3. Conflicts of interest: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years, no other relationships or activities that could appear to have influenced the submitted work 4. Funding: Elliot Tapper receives funding from the National Institutes of Health through the Michigan Institute for Clinical and Health Research (KL2TR002241). 5. The Corresponding Author has the right to grant on behalf of all authors and does grant on behalf of all authors, a worldwide licence to the Publishers and its licensees in perpetuity, in all forms, formats and media (whether known now or created in the future), to i) publish, reproduce, distribute, display and store the Contribution, ii) translate the Contribution into other languages, create adaptations, reprints, include within collections and create summaries, extracts and/or, abstracts of the Contribution and convert or allow conversion into any format including without limitation audio, iii) create any other derivative work(s) based in whole or part on the on the
Page 1 of 31
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
��
�
Contribution, iv) to exploit all subsidiary rights to exploit all subsidiary rights that currently exist or as may exist in the future in the Contribution, v) the inclusion of electronic links from the Contribution to third party material where-ever it may be located; and, vi) licence any third party to do any or all of the above 6. The lead author affirms that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted.
Page 2 of 31
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
��
�
Abstract
Objectives: Cirrhosis and hepatocellular carcinoma (HCC) are morbid and costly conditions,
each marked by the development of fatal, resource intensive complications. National data
regarding trends in demographics and associated causes of liver disease mortality are lacking.
We aimed to describe mortality by age-group, sex, race, state of residence, and comorbidity.
Design: Observational cohort study
Setting: Death certificate data from the Vital Statistics Cooperative and population data from the
US Census Bureau compiled by the Center for Disease Control and Prevention’s Wide-ranging
Online Data for Epidemiologic Research (1999-2015).
Participants: US residents
Main outcome measures: Mortality. Trends evaluated using Joinpoint Regression.
Results: Age-adjusted mortality due to cirrhosis was stable from 1999-2009 (7.5/100,000 to
7.4/100,000) but then increased each year through 2015 to 9.1/100,000 while HCC mortality
plateaued. The age group with the greatest increase in mortality is 25-34, overall average annual
increase of 10.5% (95%CI 8.9-12.2%), largely driven by death due to alcoholic cirrhosis.
Whites, American Indians and Hispanics have experienced the greatest increase in cirrhosis
mortality. Death due to concomitant peritonitis, sepsis, and falls are among the fastest growing
associated comorbid diagnoses. Western and Southern US have the greatest increase in cirrhosis
mortality while the West has the greatest increase in HCC mortality.
Conclusions: Disparate changes in cirrhosis mortality by age, race, liver disease etiology, and
US region necessitate tailoring of preventative plans to inform rational public health outreach.
The trends related to deaths from infections, falls, and the rapid rise in death-rates among young
persons due to alcohol highlight new challenges for optimal care of patients with liver disease.
Page 3 of 31
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
��
�
What this paper adds?
What is already known on this subject?
- Cirrhosis is a morbid condition that is increasing in prevalence
- Although hepatitis C is being eradicated, the burden of alcoholic liver disease and
Nonalcoholic Fatty Liver Disease is increasing
What this study adds
- Mortality due to cirrhosis is increasing in the US since 2009
- Persons aged 25-34 experienced the greatest increase in mortality with an average annual
increase of 10.5% (95%CI 8.9-12.2%) driven by death due to alcoholic cirrhosis.
- Specific demographic subgroups – namely Whites, American Indians and Hispanics –
have experienced the greatest increase in cirrhosis mortality.
- Cirrhosis mortality is improving in Massachusetts and the District of Columbia but worst
in Kentucky, New Mexico, Wyoming, and Arizona.
- Cirrhosis mortality related to falls, sepsis
- Trends in liver cancer mortality are worst in Idaho, Oregon, and Texas.
Page 4 of 31
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
��
�
Introduction
� Cirrhosis, the end result for most chronic liver diseases,1 is characterized by fatal,
resource-intensive complications. These include hepatocellular carcinoma (HCC), hepatic
encephalopathy (which also causes falls), gastrointestinal hemorrhage, infections, and renal
failure. Compounding the problem, the prevalence of cirrhosis in the United States (US) has
doubled in the last decade.2 3 Although hepatitis C (HCV), a major cause of cirrhosis, could be
eradicated given recently widely available effective antiviral therapy, this trend is likely to
continue.4 Even in the coming post-HCV era, deaths due to cirrhosis are expected to triple by
2030,5 driven primarily by the increasing prevalence of nonalcoholic fatty liver disease
(NAFLD) in parallel with rising obesity rates.6 7
Cirrhosis and HCC carry personal, social, and financial burdens for patients, their
families, and society. They are disabling,8 stressful for caregivers,9 and resource intensive even
in death where terminal hospitalizations cost in excess of $50,000 per-patient.10 Prevention and
early management of cirrhosis is therefore cost-effective.11-13 However, nationally representative
data to guide the optimal allocation of resources and preventive efforts are limited, particularly
regarding differential mortality by demographic subgroups or regions of the country.14 Herein, to
fill this gap, we analyze the Center for Disease Control and Prevention’s Wide-ranging Online
Data for Epidemiologic Research (CDC WONDER) platform.�� �
Page 5 of 31
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
��
�
Methods
All data were obtained CDC WONDER platform.15 For more details on CDC Wonder
please see the Supplemental Material. Our primary aim was to describe temporal trends in
death-rates attributable to cirrhosis (ICD-10 K70.3, K74.5, and K74.6) and HCC (C22.0) as the
primary/underlying cause. All rates obtained were age-adjusted, standardized to the 2000 US
population using the direct method unless otherwise indicated. Secondarily, we sought to
describe how these trends differed based on demographic subgroups; age, sex, race (Asian
Pacific Islander, American Indian/Alaska Native, black/African American, and
white/Caucasian), Hispanic ethnicity, and place of residence. We also aimed to describe trends in
causes of death related to specific complications associated with cirrhosis. Specifically, we
examined death due to gastrointestinal hemorrhage (ICD-10 K25-K28, K92.0-K92.2, I85.0),
peritonitis (K65), sepsis (A41), hepatorenal syndrome (K76.7), or falls (W00-W19) in patients
with cirrhosis. Given the association between NAFLD and complications of the metabolic
syndrome like cerebrovascular disease and ischemic heart disease (I20-I25, I60-I69),16 we also
assessed trends in death-rates due to these conditions.
To test for unmeasured secular trends, all findings were compared to non-cirrhotic
control populations. Some controls were pre-selected to reflect death-rates for chronic disease,
cancer, and infection. Specifically, we examined the trends in deaths due to cardiovascular
disease (ICD-10 I00-I99), cerebrovascular disease and ischemic heart disease (I20-I25, I60-I69),
colon cancer (C18), and sepsis (A41). Other controls were selected post-hoc based on trends
observed in our study. These included deaths due to alcohol use disorder (F10), peritonitis, falls,
and end-stage renal disease (N18.0, N18.5). Finally, we assessed overall trends in several states
Page 6 of 31
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
��
�
that had the greatest increase or highest death-rates due to cirrhosis and HCC (e.g. Arizona, New
Mexico, and Wyoming).
Data Analysis
Trends in death-rates were then evaluated using the National Cancer Institute’s Joinpoint
program (version 3.5.2; available: http://surveillance.cancer.gov/joinpoint), which uses a
piecewise linear regression approach to determine whether rates over time are best described by
a single line or by multiple linear segments (i.e., none or >1 joinpoints). We allowed a maximum
of 3 joinpoints with a minimum of 3 observations per segment. The best model (in which
additional joinpoints did not improve model fit) was identified using log-transformed data. We
obtained the annual percentage change (APC) in death-rates over each linear segment as well as
the average annual percentage change (AAPC) from 1999-2015 for each model. The APC was
obtained using Monte-Carlo permutation analysis to fit a series of 4,500 randomly permuted
straight lines on a logarithmic scale to observed rates to estimate APC, resulting in trends of
variable length. Trends were only described as increasing or decreasing when the APC was
significantly different from 0 (two-tailed P<0.05). We noted many significant changes in the
APC beginning at 2009. We therefore provided the AAPC for 2009-2015. We created state heat-
maps, highlighting the age-adjusted death-rate in each state for 3 evenly-spaced study years
(1999, 2008, 2015). We also compared trajectories in death-rate by contrasting the AAPC with
each state’s baseline death-rate and the AAPC before and after 2009. Patients were not involved
in the study design. As this is a publically available dataset of de-identified data, no ethics
approval was obtained.
Page 7 of 31
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
�
�
Results
Overall Trends (Table 1)
During the study period, cirrhosis caused a total of 426,575 deaths (20,669 in 1999 and
33,973 in 2015) and 125,869 were attributed to HCC (5,112 in 1999 and 10,059 in 2015). Since
1999 when the death rate from cirrhosis per 100,000 Americans was 7.53 (95%CI7.42-7.63),
there has been a 1.1% (95%CI0.7-1.6) average annual increase in cirrhosis related mortality.
This rate, however, has risen more rapidly since 2009 (AAPC: 3.4% 95%CI3.2-3.8). Deaths
related to HCC have risen by an AAPC 2.0% (95%CI1.6-2.4) yearly since 1999. In contrast to
cirrhosis trends, the rate of HCC related deaths have slowed since 2009 (AAPC: 1.2%
95%CI0.3-2.1). (Supplementary Table 1) Males had a higher burden of age-adjusted cirrhosis
mortality when compared to females by a 2:1 ratio and a higher burden of HCC related deaths by
a nearly 4:1 ratio. The highest burden of age-adjusted cirrhosis mortality was seen in American
Indians (16.5/100,000 people), followed by whites (8.1/100,000 people). Age-adjusted HCC
death-rates were highest in Asian/Pacific Islander patients. Hispanics had relatively high age-
adjusted mortality from both cirrhosis (12.4/100,000) and HCC (3.7/100,000). The Southern and
Western regions of the US had the highest age-adjusted mortality from cirrhosis (8.7/100,000
and 8.5/100,000, respectively) while the Western US alone had the highest age adjusted
mortality related to HCC (2.7/100,000).
Cause-Specific Mortality Trends
Supplementary Table 1 depicts the time trends in comorbid causes of death for patients
who died from cirrhosis. The AAPC for cirrhosis-related deaths due to peritonitis (1.9%
95%CI0.8-3.0), sepsis (3.7% 95%CI3.2-4.1), cerebrovascular and ischemic heart disease (0.4%
Page 8 of 31
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
�
�
95%CI0.1-0.7), and falls (4.5% 95%CI3.5-4.5) have risen since 1999. Conversely, deaths due to
cirrhosis and gastrointestinal bleeding or hepatorenal syndrome have fallen or remained stable
from 1999-2015, with respective AAPC of -0.8%(95%CI-1.3- -0.4) and -0.3%(95%CI-0.9- 0.3).
Similar changes were observed when specific codes for variceal hemorrhage (ICD-10 I85.9) and
comorbid end-stage renal disease (N18.0, N18.5) were examined. However, despite
improvements in death-rates for these conditions, all gains were made from 1999-2008. When
examining the trends from 2009-2015, the death-rate associated with each potential cirrhosis-
related complication we queried, including fatal bleeding and renal failure, have risen. Notably,
from 2009-2015 the magnitude of increased death-rate due to peritonitis and sepsis rose
substantially with respective AAPC of 6.1%(95%CI 4.2-81) and 7.3%(95%CI 6.4-8.1).
Demographic Trends in Death-Rates
Cirrhosis
We evaluated trends in cirrhosis death-rates in demographic subgroups with several
significant findings.(Table 2) First, cirrhosis-related mortality increased significantly from 2009-
2015. Although several subgroups had significant declines in cirrhosis-related mortality from
1999-2008, these trends reversed in nearly every demographic subgroup beginning in 2009.
Second, both sexes experienced similar increases in mortality. Third, whites and American
Indians had more rapid increase in cirrhosis mortality after 2009 with AAPC of 3.9%(95%CI
3.4-4.5) and 3.8%(95%CI 1.5-6.3) compared to African Americans. Fourth, non-Hispanic
patients experienced a slower rise in cirrhosis related mortality than Hispanic patients. Fifth, in
Page 9 of 31
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
���
�
recent years, the Northeast US had the slowest rise (AAPC 1.5% 95%CI 0.9-2.2) while the south
had the fastest (3.9% 95%CI3.2-4.6).
Though the incidence of cirrhosis-related mortality was lower in young people, persons
aged 25-34 experienced the highest AAPC in cirrhosis mortality; 3.7% (95%CI2.4-5.1) over the
whole period and 10.5% (95%CI8.9-12.2) from 2009-2015.(Figure 1) Whites and American
Indians had the most rapid increase in this age group. Increased death-rates in the 25-34 age
group were driven by alcoholic cirrhosis, where the average AAPC from 2009-2015 was 15.3%
(95%CI 13.0-17.7) compared to 6.3% 95%CI3.6-9.0 for other causes of cirrhosis. These finding
is reinforced by Supplementary Figure 1 which demonstrates parallel changes in mortality due
to both alcohol use disorder and alcoholic liver disease.�
Hepatocellular Carcinoma
The demographic trends in mortality from HCC are markedly different from cirrhosis.
First, overall, from 1999-2011 there was a 2.4% (95%CI:2.1-2.8) increase in HCC mortality
nationally. Since 2011, the death-rate has plateaued. Females experienced a consistent increase
in HCC mortality through 1999-2015 while HCC death-rates for males plateaued beginning in
2011. Second, American Indians experienced continuous increases in HCC mortality while
Whites experienced increased HCC mortality only in recent years (since 2011). By contrast,
Asian/Pacific Islanders had consistent decrease in HCC mortality since 1999 while African
Americans had a plateau in HCC mortality since 2011. Third, all US regions except for the
Northeast experienced increased HCC mortality since 1999. Fourth, as seen in Figure 1, while
Page 10 of 31
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
���
�
HCC related mortality has decreased in younger patients (<55 years) since 2009, mortality
among those >55 years-old increased during the same timeframe.
State-Level Variation in Mortality
The fastest rise in cirrhosis and HCC related mortality occurred in the Western and
Southern US. In Figure 2, we show that the highest mortality and greatest increases in mortality
were observed in Southern, Western and Mid-Western states from 1999-2015. Figure 3A
contrasts changes in mortality for cirrhosis and HCC with the baseline mortality rate for
individual states. The states with the greatest AAPC in cirrhosis related mortality include
Wyoming 3.7% (95%CI1.9-5.6), Oregon 2.9% (95%CI1.6-4.2), Arkansas 2.8% (95%CI1.4-4.3),
and Iowa 2.8% (95% CI1.6-3.9). Five states experienced decreases in cirrhosis related deaths,
with the largest decrease observed in the District of Columbia -2.1 (95%CI-4.1- -0.1).
We also evaluated state-level trends in HCC-related death-rates. No state experienced a
decreasing mortality due to HCC (Figure 3B). Many of the same states with worsening cirrhosis
mortality also experienced worsening HCC mortality (e.g. Oregon, Iowa). However, some states
experienced increased HCC-related deaths out-of-sync with cirrhosis trends. These include
Arizona (5.1% 95%CI3.7-6.5), Kansas (4.3% 95%CI2.8-5.8), Kentucky (4.0% 95%CI3.1-5.0),
and Washington (3.9% 95%CI3.1-4.6).
Page 11 of 31
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
���
�
In Figure 3C-D, we compare the AAPC for mortality in the first half of the study period
(1999-2008) to the AAPC in the last half of the study period (2009-2015). In the lower left
quadrant of Fig.3C are the only 2 states (Washington DC and Massachusetts) that experienced
consistent improvements in cirrhosis-mortality. In contrast, the upper right quadrant has all states
with consistently worsening death-rates (e.g. Oregon, Idaho, Alabama). In the left upper
quadrant are those states with reversals from improvements to worsening (e.g. New York,
Connecticut, Kentucky, Utah). The contribution to these trends from alcohol use disorder is
explored by demonstrating death-rates by state in Supplementary Figure 2. In some cases, they
are consistent with cirrhosis trends (e.g. Oregon), and not in others (e.g. Massachusetts). With
respect to HCC,(Fig.3D) no state observed an improvement from 2009-2015 while Western and
Southern states experience the worst trends.
Page 12 of 31
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
���
�
Secular Trends (1999-2015)
In Supplementary Table 2, we compare the cirrhosis-specific trends to other conditions
to assess for the presence of unmeasured secular trends. First, death trends for broader definitions
of liver disease (including all liver-related ICD-10 codes) were not different than a definition that
focused on cirrhosis codes. Second, death-rates due to heart disease and colon cancer fell while it
rose for cirrhosis. Third, whereas death due to gastrointestinal hemorrhage and peritonitis
increased for patients with cirrhosis since 2009, they did not rise in patients without coding for
cirrhosis. Sepsis death-rates increased minimally in the non-cirrhotic population from 2009-2015
(AAPC 1.2%(95%CI0.1-2.3), but increased by 7.3%(95%CI6.4-8.1) per year in cirrhosis
patients. Fourth, while death-rates fell for non-cirrhotic patients in Arizona, New Mexico, and
Wyoming, death-rates due to cirrhosis in each state rose substantially.
�
� �
Page 13 of 31
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
���
�
Discussion
Cirrhosis and HCC are deadly conditions, each with increasing footprints in American
public health. Understanding the factors associated with mortality due to these conditions will
inform how best to allocate resources. In this study of national data from 1999-2015, we find 6
major trends in cirrhosis and HCC mortality in the US.
First, we show mortality due to cirrhosis has been rising since 2008. Whereas Asrani et al
previously demonstrated unchanged age-and-sex-adjusted death-rates due to liver disease from
1979 (25.8/100,000) to 2008 (25.7/100,000) in Olmstead county,17 our analysis shows increased
mortality in the context of declining mortality due to other causes such as heart disease and colon
cancer. Second, increased cirrhosis mortality disproportionately affects young persons aged 25-
34, White, American Indian, and Hispanic Americans, and those living in the Southern or
Western US. Third, increases in cirrhosis mortality among young people appears to be driven by
alcohol use disorder. Fourth, while mortality due to HCC continues to increase in older
Americans, it is decreasing in younger people and Asians. This could be due to increasing the
early detection of HCC, application of curative/locoregional therapies, and, because hepatitis B
is the principal cause of HCC worldwide and among Asian-Americans, effective vaccines and
antiviral therapy for hepatitis B.18-21 These trends also parallel those observed for the incidence
of HCC.22 Fifth, the causes of death associated with cirrhosis that had the most consistent and
substantial increases over the study period were infections and falls. Common complications of
cirrhosis such as hepatic encephalopathy and sarcopenia (both prevalent in up to 40% of patients
Page 14 of 31
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
���
�
with cirrhosis23), while not directly fatal themselves, both increase the risk of mortality due to
falls, frailty, and infection.8 24-26 Finally, specific states in the South and West experienced the
worst trends for cirrhosis and HCC mortality. Only Massachusetts and the District of Columbia
claimed consistent reductions in cirrhosis mortality. Adverse trends in Kentucky, New Mexico,
Wyoming, and Arizona in particular require further study for explanation. The areas of greatest
need for attention to HCC mortality appear to be Idaho, Oregon, and Texas.
Clinical and Health-Policy Implications
Cirrhosis is morbid and costly to treat and therefore efforts to prevent progression of all
liver diseases are cost-effective.12 13 27 28 Our data highlight several modifiable sources of
mortality. First, young American Indians and Whites with benefit from intensified resources for
alcohol use disorders. Second, falls in patients with cirrhosis are associated with hepatic
encephalopathy, frailty, and psychoactive medications such as benzodiazepines.24 29 30 Falls could
be prevented through early identification and treatment of mild hepatic encephalopathy, ensuring
adequate nutrition, enrollment in physical activity programs, and targeted campaigns for
psychoactive medication deprescribing. Third, patients with a history of spontaneous bacterial
peritonitis experience improved survival from secondary (antibiotic) prophylaxis, yet many do
not receive it.31 Quality improvement efforts are needed optimize care delivery in these cases.31
Fourth, research and outreach are required to understand and contextualize the factors associated
with the adverse trends identified in many states.
Page 15 of 31
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
���
�
Contextual Factors
Several considerations must be made in the interpretation of these findings. First, these
findings are based on data abstracted from death certificates. Death certificates may be
inaccurate (in up to 15% of cases32) and this study does not explicitly validate disease coding
with chart review. For this reason, we chose the diagnostic codes most specific to cirrhotic
complication. Still, sensitivity analyses using a variety of coding algorithms for liver disease
confirm consistency of results and comparisons of our results to other conditions imply
independence from secular trends. Second, given variance in coding for hepatitis C (substantial
changes after 2004), we cannot provide mortality estimates specific to viral hepatitis. Third,
though we have detected worsening mortality since 2009, the precise explanations for this trend
require further study. For example, we identify the most at-risk states, but granular data is needed
to determine root-causes, be they trends in healthcare access, policy (e.g. alcohol tax-rates),
alcohol abuse, or the differential changes in the comorbidities of a given state’s population.
Fourth, it is unclear how these trends are – or will be – affected direct-active antivirals for
HCV. Screening for HCV is recommended given the availability of highly efficacious therapy,
however hundreds of thousands of individuals in the US have undetected HCV or do not have
access to antiviral therapy.13 33 At the same time, HCV eradication will prevent the development
of cirrhosis and its complications, potentially changing these trends if re-assessed in the next 5-
10 years. However, HCV therapy cannot modify the significant trends observed related to
alcohol or the expected increase in the burden of NAFLD.5
Page 16 of 31
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
���
�
Conclusion
Specific demographic subgroups and states are disproportionately affected by adverse
trends in cirrhosis and HCC-related mortality. Additionally, patients with cirrhosis are more
likely to die due to specific secondary causes including falls and infections. These data
underscore gaps in care and opportunities for prevention.
Page 17 of 31
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
��
�
� ����������� ��������� �������������
�
�
�
�
�
�
�
�
�
��� ��� !�� ���� ����"�"� ����� !���#���������� ����������!�������$%&�'�� ��#������ !��$�� �
(����������� ���� � )�� ������"� ��( ��� �� ��� ����
Deaths Crude rate
(per 100,000) Age-adjusted (per 100,000) Deaths
Crude rate (per 100,000)
Age-adjusted (per 100,000)
Overall 426,575 8.34 (8.32-9.37) 7.80 (7.78-7.83) 125,869 2.46 (2.45-2.48) 2.27 (2.26-2.29)
Female Male
150,232 276,343
5.78 (5.75-5.81) 11.0(10.9-11.0)
5.13 (5.11-5.16) 10.8 (10.8-10.8)
29,187 96,682
1.12 (1.11-1.14) 3.85 (3.82-3.87)
0.97 (0.95-0.98) 3.82 (3.79-3.84)
American Indian Asian/PI
African American White
8,354 6,117
37,825 374,279
12.9 (12.7-13.2) 2.31 (2.26-2.37)
5.5 (5.4-5.6) 9.14 (9.11-9.17)
16.5 (16.1-16.9) 2.87 (2.80-2.95)
6.3 (6.2-6.4) 8.14 (8.11-8.17)
1,254 10,460 19,468 94,687
1.94 (1.83-2.05) 3.96 (3.88-4.03) 2.83 (2.79-2.87) 2.31 (2.30-2.33)
3.00 (2.82-3.18) 4.89 (4.79-4.98) 3.32 (3.27-3.37)
2.01 (2.00 – 2.02)
Hispanic Non-Hispanic
58,622 366,472
7.52 (7.46-7.59) 8.46 (8.43-8.48)
12.4(12.3 – 12.5) 7.38(7.35-7.40)
15,695 109,819
2.01 (1.98-2.05) 2.53 (2.52-2.55)
3.69 (3.63-3.75) 2.16 (2.15-2.17)
Northeast Midwest
South West
66,721 84,264
173,547 102,043
7.15 (7.10-7.21) 7.49 (7.44-7.54) 9.26 (9.21-9.30) 8.64 (8.59-8.70)
6.34 (6.29-6.39) 6.91 (6.86-6.96) 8.66 (8.62-8.70) 8.54 (8.49-8.59)
23,996 24,172 45,105 32,596
2.57 (2.54-2.61) 2.15 (2.12 – 2.18)
2.41 (2.38-2.43) 2.76 (2.73 – 2.79)
2.24 (2.21 – 2.27) 1.94 (1.92- 1.97)
2.22 (2.20 – 2.24) 2.73 (2.70 – 2.76)
Page 18 of 31
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
��
�
� �������* " ��%���� � ���(� ���� �(��������� !�)�� ������"� ��( ��� �� ��� ���� ��������������� �����+ ���!�,� ����� �,������
������ �����,"����"���
�
�������� !��� �(����������� ���� � �������� !��� �)�� ������"� ��( ��� �� ��� ����
Joinpoint segment APC (95%CI) P-value
Joinpoint segment APC (95%CI) P-value
Overall
1999-2003 2003-2006 2006-2009 2009-2015
0.2 (-0.6-0.9) -1.5 (-3.6-0.7) 0.6 (-1.5-2.8) 3.4 (3.1-3.8)
0.6 0.1 0.5
<0.001 Overall 1999-2011 2011-2015
2.4 (2.1-2.8) 0.5 (-0.9-2.0)
<0.001 0.4
Female Female Female
Male Male
1999-2002 2002-2008 2008-2015 1999-2009 2009-2015
1.4 (-1.0-3.8) -0.8 (-1.8-0.1)
4.0 (3.5-4.5) -0.6(-0.8- -0.3)
3.2 (2.7-3.7)
0.2 0.1
<0.001 <0.001 <0.001
Female Male Male
1999-2015 1999-2011 2012-2015
1.2 (0.9-1.4) 2.6 (2.3-2.9)
0.3 (-1.0-1.6)
0.02 <0.001
0.6
American Indian American Indian
Asian/Pacific Islander African American African American
White White
1999-2010 2010-2015 1999-2015 1999-2008 2008-2015 1999-2009 2009-2015
-0.3(-1.2-0.6) 3.8(1.5-6.3)
0.2 (-0.3-0.7) -3.7 (-4.3- -3.1)
1.9 (1.9-2.8) 0.1 (-0.2-0.4) 3.9 (3.4-4.5)
0.5 0.004
0.3 <0.001 <0.001
0.4 <0.001
American Indian Asian/Pacific Islander
African American African American
White White
1999-2015 1999-2015 1999-2011 2011-2015 1999-2011 2011-2015
2.3 (0.9-3.7) -2.8 (-3.5- -2.1)
3.1 (2.4-3.8) -1.4 (-4.2 -1.4)
2.6(2.5-2.8) 1.0 (0.2-1.8)
0.003 <0.001 <0.001
0.3 <0.001
0.01
Hispanic Hispanic
Non-Hispanic Non-Hispanic
1999-2009 2009-2015 1999-2007 2007-2015
-0.3 (-0.6 - -0.1) 3.7 (3.2-4.2)
-1.7 (-2.4 - -1.0) 1.3 (0.7-1.8)
0.01 <0.001 <0.001 <0.001
Hispanic Non-Hispanic Non-Hispanic Non-Hispanic
1999-2015 1999-2007 2007-2010 2010-2015
0.5 (-0.01-1.0) 2.0 (1.5-2.4) 4.0 (0.3-7.8)
0.5 (-0.2 – 1.3)
0.1 <0.001
0.04 0.15
Northeast Northeast Midwest Midwest
South South West West
1999-2007 2007-2015 1999-2008 2008-2015 1999-2009 2009-2015 1999-2008 2008-2015
-2.2 (-2.9- -1.5) 1.5 (0.9-2.2)
-0.4 (-0.7- -0.1) 3.1 (2.7-3.5)
-0.2(-0.6-0.1) 3.9 (3.2-4.6)
-0.2(-0.7-0.3) 3.3 (2.6-3.9)
<0.001 <0.001
0.01 <0.001
0.2 <0.001
0.4 <0.001
Northeast Northeast
Midwest South West
1999-2010 2010-2015 1999-2015 1999-2015 1999-2015
2.3(1.7-2.9) -0.2 (-1.9-1.6)
2.4(2.2-2.6) 2.2(1.7-2.6) 1.9(1.5-2.2)
<0.001 0.8
0.001 <0.001 <0.001
���������� ���������!�!�������� ������-� ��!"�� ��.���������� ��!� ���� �������!"�� ��.�����" �#������ ����� �����!� ���� ���.�����������!$�
& �� -�� �� ���/������� ���� ����������0�� ��� ��/�������� ��� #����.����� ��"������� ��#������� ��� ������� � �����1�!��-��"��� �� ��-�
!�##��� ��!� ���� ���$�*&�'�*����� �& !� /�*2%&�'�*�� 2% ��#���&�� !��/�**�'�*#��� �*����� /�34�'�3����� ��/�56�'�5�!.���/�,�'�,�"��/�6�'�
6���
Page 19 of 31
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
���
�
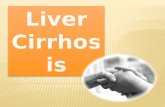
Figure 1: Death-rate Trends by Age-Group
Each bar represents the average annual percentage change in the death-rate due to cirrhosis and
hepatocellular carcinoma (HCC). Panels A and C show changes over 1999-2008; B and D show
changes 2009-2015. Panels A and B: Key trends include increasing cirrhosis mortality for
Americans aged 25-34 and contrasting HCC mortality trends for groups younger (decreasing)
and older (increasing) than 55-65. The magnitude of these trends rises in recent years. Panels C
and D: Trends for both cirrhosis and HCC mortality worsen for patients of white race over all,
American Indian race in the young (age 25-34 from 2009-2015) and appear to improve early in
the study period for young African Americans while they worsen for older African Americans
(age 65-74) in the latter half of the study period.
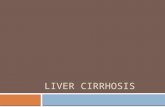
Figure 2: Age Adjusted Death-rates Attributable to Cirrhosis and Hepatocellular
Carcinoma over Time
The age-adjusted mortality for each condition in each state is presented in quartiles for the first,
middle and last year of the study. Quartiles for each time period are denoted by yellow (first),
light orange (second), dark orange (third), and red (fourth). Striped or shaded states imply data
that is either unreliable or suppressed to protect patient identity.
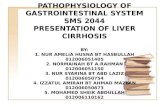
Figure 3: States with Significant changes in Death-rates Attributable to Cirrhosis and
Hepatocellular Carcinoma
A-B: The average annual percentage change (AAPC) in mortality for each individual state is
plotted against the baseline age-adjusted death-rate for cirrhosis (A) and hepatocellular
carcinoma (HCC, B)
C-D: In order to characterize the trajectory of mortality due to cirrhosis (C) and HCC (D), the
AAPC since 2009 is plotted against the AAPC in the first half of the study (1999-2008) for
individual states.
Note: States without significant trends were excluded from this figure for simplicity.
Page 20 of 31
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
���
�
�����������
�$�,��"�� ��/�*#!� ��3)$�7��������������$�����������8���9���:�����$�!����,���������9�:������
;���<�
��$����2,���������9�:������;�"������!�� �� ��=���������2��2��<�
�$�>�����7*/�7������1�,7/�?��� �%@/���� �$���� !��� ��"�!� ��#����������� !���� ������"� ��� ��� �� ��-�
" !���-� ��������!��� ���� �+,������ �/����������$����������� �����8��9�:����������8�
A"�1�����$�!������$����20$� ����$����$��$����
�$��B*�����?/�? ��� ��� ��?/�% ��� ���7$�3 �"� ��������-� !����� ������� !�� ������#��"���� ��� ������������
��-���� ���������.��#������"!���$��������������8���������$�!������$����20$0���$����$��$����
;�"������!�� �� ��=����������2��2��<�
�$�5�� �*/�?��� �%/�>���-�@/���� �$��� �#��� ��� ��#���� ������(� ����� ����� ��� ��� � � ��� ��
�� ���� ����-�����#����.� ������� ���!"���� ��#�!������ ����� �� �� ��$��������� �
�������� �������������������8��9:��������$�
�$�4�����(/�C 1 ���)/�7���� �C/���� �$�5�!��� ���������!������#� � ���������# ��-�������!��� ���
!��� ��� ���� ��D�� � �� ��� ��� ���� ��"�!� ��#�!��� ��$�������� ��
�$�% ��E��3�/�5 ������6F/�6 ��F/���� �$�%��0����!�� ��� ���� �������-� !� � � ������������ ����� ������
��� ��!��������� ��� � ��� �. ������� !!���� ��� �����+ ���!�,� ���$�������� ������
�$�G�" �����H5/�,��� �� �5/�*#� !-�5/���� �$�(� ����� ��������� �� ����#��������������� �� "����
�#����� ���������!��� ����� �����+ ���!�,� ����#������������$�������������������� �����
������� �����89�:�������$���$�
$�� �����4>/�=� E������ ��/�5������ �5*/���� �$�,� ! �!� ������� ����#�#� ���-� ���� ��! ��!����!�������
�#����� ���-�� ������� ��1�!�� ��� ���.�������������$�������� �����8��9�:�����$�
$�> 0 0�F,/�6 !��F>/�?���� ��%/���� �$������"����!��� ��� ���"�!� ��#����������� !���� ����
� ���� ��� ��-�� �� ��� ��� !�� ��������$������������������������������� �
����8���9:��������$�
��$�% ����**/�6 ��� ��*5/�5 -�=%/���� �$�% ��� �����( ��� !�)� ����( ���+����1 ��� �#���% ��� ���6����4 !�
,� ���7��������� ��� ������4 !��#�7�#�$�������������������� ������������ ������
��$�� �����4>/�( � �*5/�,�����3/���� �$���������������#�� ���#������ ������"� ��� ��� �� �� �� ��� ���
.������� ������(����������$�����������8���9�:�����$�
��$�� �����4>/�,� �"�� �3/�)" � E�55/���� �$�(�����##��������� �" ��� ��#� � ���������# ��-�������
!��� ���.����3*=7��#�������������� !����� ��� ��� ������!��� ��� ���� ����� ��-$�������������
������������������ �����8���9:���$�
��$�C�� ��>/�,�����>�/�6���� ��� �F,/���� �$�����������##������ �����#������������������� � ��#������ ������
(� ����!-�� �+,����� �-�� �������� ��$�������������������������������8���9�:�������$�
��$�6������7/�����#��*%/�@ . ��=/���� �$�& ��!� ����#�)�� ������"� ��( ��� �� �� �*������+ ���!�,� ���/�
=�������������"�������$����������� �����8���9�:���������$�!����
��$����20$� ����$����$��$����
��$�(�(�6�3�4C���(� �����#������� ���(� ����� !�%���� ��� ������;*� �� ����#�����
�����22.� !��$�!�$���2� ������!���������������$�
��$�*��� �*5/�����-��5/�7 ��� �FF/���� �$�3� ���������= ��-�7��������� ���& ��!� ��� !�&�� ���� �
5�� ������>"�!� � !��� ���� ����G� ��(���" ��-�,�"!-$�������� ������
��$�*�� ��,@/�7 ��� �FF/�G . �>/���� �$�+ !������� ��� ��#���������� ��!����� ���-�� �����+ ���!�,� ���$�
���������� �����8���9�:������$���$�
�$�(�� �(�F/�G ��)�&/�,"�F/���� �$�C��E��#���� ������"� ��� ��� �� � ������ ��������� ���� !�� ���#����"��
��� ������>����"���3*������$����������8��9�:������$�
�$�*���E�"���,=/�5�?�- �@*/�C����� �54$�)�� ������"� ��� ��� �� �� ��!� ��/����� ���-/� !��"���� ��
��� !��� �����+ ���!�,� ����#���������������$���������������������� ����8��9:������$�
Page 21 of 31
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
���
�
��$�*���E�"���,=/�)� ��-�,F/�("�� �����F4/���� �$�(� �� ����� ������"� ��� ��� �� �� ��!� ��� !�������
� �������� ���-�� ����� �����+ ���!�,� ���$��������������������8��9�:�������$�!����
��$���2 0�$����$���
��$�+� � �,I/��"##-�*?/�5�3�����,/���� �$�4 ����������� � ��� � !� ����� ��� ��#��"� �����
��� ��� ���� ���� ������"� ��� ��� �� $�������� �����8��9�:��������$�!����
��$����2���$����
��$�6������7/�����#��*%/�@ . ��=/���� �$�& ��!� ����#���� ������"� ��� ��� �� �� � ������+ ���!�,� ���/�
#�������������"�������$����������� �����8���9�:������$���$�
��$�C�#� � ������ ��� � ��-���������� ���-������-�!���� � ���� ������������� ��� ���#���� ����
� ���� ��� ��-$�5 -��(�� ���%�����!� ��8�����$�4�������$�
��$�� �����4>/�C������3�-� �G/�,� �"�� �3$�%�-��� ��������!�� ��� ��� ��� ����������E��#�# ���� !�# ���
��� ��!�� 0"������ ������� ��1�!�� ��� ���.�������������$�������������������� ������������ �
����8��9:��������$�
��$�7 ��F(/�=� ��,/����� "���3*/���� �$�=� ���-����!�����. ����������� ���-�� ��������� ��� ��� !�! ���$�
����������������������������������8��9:������$�
��$�> 0 0�F,/��J7� �-�F?/�� !� �%/���� �$�)�� ����4 ���� ��� ��-�&��*����� ��!�6����5��� ���-�� �% ��� ���
6����(���������& !��� !� ���#�������4D�� ��� ������� �= ��"���$�������������������� �����
������� �����8��9�:�������$���$�
��$�7��! ���*F/�(����� �)6/�,�� !�� ��%C/���� �$�*������ �������##�����#����� �� ����!"���� ��� � � �
��� �������� ���-�� ���������� ��!�������##������ �����#���� ������(���� ��� ��� �� ��-��� �����#�
������!��� ��$��������������������������������������� �����8��9�:������$�
�$�I��!�"�01� �&@/���-�5/�) � K�,F/���� �$�,���� � �� !�� ��-���� ��� ���#����� ���#������� ���
��� ������>����"��� #����� ����������##������$����������� �����8��9�:�������$�
�$�C��L �4/����� !���5�/�3 ! ��5F/���� �$�C !���1�!���������"!-���##������#� ��D������������ ����
!���"�� ���"������ � ��� �� �� ��� ���.�������������$���������������������������������
����8�9:�������$�
��$�C��L �4/�(M�!�� �F/������ ��5/���� �$�5� �� ����� ����� ���� ��� ��-���� ����� ��!�.����# ���$�����
�������������������������� �����8���9�:����$�
��$�� �����4>$�>"��!� ���##�������A" ���-���������� ������� ���#���������!��� ���� ��-���� ���������.��#�
A" ���-���������� ��� ��� �����$�������������������� ������������ �����8��9:��������$�
��$�
��$�?��� �CC/�=� E�*@/�)��� �5/���� �$����� ��"� �-��#�� �������� ���-��� ��������� ��!�� �!� ���
�����#�� ����� �����+ ���!�,� ���$���������������� �����8��9�:�������$�
��$�(�� �. ��F/�6 ��N/�*-����/���� �$�)�� ������(����� ���>"�!� �� �����+ ���!�,� ����� ������� ��#��� ��
!������ ��� �� ����� ��$�������� �����8��9�:��������$�!������$����2���$�����
�
Page 22 of 31
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
Figure 1: Death-rate Trends by Age-Group Each bar represents the average annual percentage change in the death-rate due to cirrhosis and
hepatocellular carcinoma (HCC). Panels A and C show changes over 1999-2008; B and D show changes 2009-2015. Panels A and B: Key trends include increasing cirrhosis mortality for Americans aged 25-34 and contrasting HCC mortality trends for groups younger (decreasing) and older (increasing) than 55-65. The
magnitude of these trends rises in recent years. Panels C and D: Trends for both cirrhosis and HCC mortality worsen for patients of white race over all, American Indian race in the young (age 25-34 from 2009-2015) and appear to improve early in the study period for young African Americans while they worsen for older
African Americans (age 65-74) in the latter half of the study period.
200x148mm (300 x 300 DPI)
Page 23 of 31
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
Figure 2: Age Adjusted Death-rates Attributable to Cirrhosis and Hepatocellular Carcinoma over Time The age-adjusted mortality for each condition in each state is presented in quartiles for the first, middle and last year of the study. Quartiles for each time period are denoted by yellow (first), light orange (second),
dark orange (third), and red (fourth). Striped or shaded states imply data that is either unreliable or suppressed to protect patient identity.
190x126mm (300 x 300 DPI)
Page 24 of 31
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
Figure 3: States with Significant changes in Death-rates Attributable to Cirrhosis and Hepatocellular
Carcinoma
A-B: The average annual percentage change (AAPC) in mortality for each individual state is plotted against the baseline age-adjusted death-rate for cirrhosis (A) and hepatocellular carcinoma (HCC, B)
C-D: In order to characterize the trajectory of mortality due to cirrhosis (C) and HCC (D), the AAPC since 2009 is plotted against the AAPC in the first half of the study (1999-2008) for individual states.
Note: States without significant trends were excluded from this figure for simplicity.
206x180mm (300 x 300 DPI)
Page 25 of 31
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
��
�
�������������� � ������������������������������������������������
������������ �����
�
�����!"�#������$��%�&�'�����(��������)���*��$��$��%�&�'�
�"� ��+� �����,� �����������������������&����+�� ������$��������
�"� ,� �����������������&�-.�.���.�/��������������� ��&�.���.�/��
�
�
#�/����������� �
��������$���� ���#��������� ���������
���������������������#�/������.���.�0� ����������1��� ��������&����.������ �
���������������������#�/���������������������� � �
��������������������2���������#���� ����.�������������$��������
���������������������2���������.+������.������)�����������������%..)�'����$������������
��.������ ���� �����
�
�
�
� �
Page 26 of 31
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
��
�
�����������������������������
����/� ��
����34(� 1���+��� ������������������+�������������������������� &��������
����������+�����/�������5�+����� ���� ��� �0��� ������ ������������-���������� ��� ��������+�"�
#�� ������������� ���� &������������ �%)�����1��&��"�"�-������6 ���� &�,��&�.����������&�
��������(�������$�������6 ���� '&������� �����������/��&�����(�7�8�*�����"� ����
0��� ������������ ��������(����������������������������� ��� ������� �������������9���+�����
����������� ���������+���:&���������+��������� ���� ������7���"�
#�������34(� 1��������� � �������/������� � �� ���������������������
���� ���������������� �9��/� ����������� � �!������������ ��������������7����������
���� �������������������&������� � "� ����� ������� �� �������7������ �������������������;�
���������������+���%�6'&�/���/� ����������������������������������������������������
��+�����/����������34(� 1�������"�3����������������&�7��� ����7� ������������� �� "�
2�� �&�7��� ����������������$��������2����%�$2'&�����������+�����������������������
���������������������������+�����������"�"������ �������� �%����������������� '� �������:<"�
���� ��������� �������������/��/�������/������������ ������&����&�����&�������&�����&�����
�������������� ���������"������&�7��� �������$����������� ����������%$��'������ ���7�����
������ ����� ���������������������������� �� ��� ��$2"�6��� ������+����/�����������
����"�$�������������� ��� �������������������� ���������&�����������7��������������������
��� � ����������������7������������������"�#�� ����7���� ���� � ������ ���� ��������
��� � ������������*���������� � "�!����������������������������&�����������+����/���7� ������
���������������6��������������� ������������� �� � �%6��'���� � ��"�3�����������
�� ����������������� � ������ ��������"�
Page 27 of 31
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
��
�
�
�������������#�/������.���.�0� ����������1��� ��������&����.������ �
� � ����� ������/���/���������� � �
����� �������
��������������
��������
%+�����'�
8����
4+������
��� � ��� ���������������������� � �
������
,� ������ ������
!��������
)�������� � ��� � � �����������
������
����/��
+� ����������
� ������
�������� �� ��
2��� �
����� 5"�=�%5">��5":='� �"5��%�"5>��"<>'� �"�5�%�"����"��'� �"�<�%�"����"��'� �"5:�%�"5=��"<�'� �">>�%�">����">�'� �"���%�"�<��"��'� �"<:%�"<���"��'�
����� 5"�:�%5">��5"::'� �"5:�%�"5���"<�'� �"=��%�"�<��"=�'� �"���%�"����"�='� �"5��%�":���"5�'� �">>�%�">����">�'� �"�:�%�"����"�5'� �"�:%�"����"��'�
����� 5"���%5">��5":='� �":��%�":>��"5='� �"���%�"�5��"=�'� �"�5�%�"�=��"��'� �"5��%�":<��"5>'� �"=��%�"=����">>'� �"���%�"�<��"��'� �"��%�"<:��"�:'�
����� 5"���%5">��5":�'� �":��%�"�5��"::'� �"�<�%�"�:��"=�'� �"���%�"�<��"�:'� �"5��%�":5��"5>'� �">��%�"=5���">:'� �"���%�"�<��"��'� �"�<%�"�=��"�='�
���=� 5":��%5"���5"5�'� �"���%�"�>��":='� �"�<�%�"�:��"=�'� �"�>�%�"����"�<'� �":5�%�":>��"5�'� �">��%�"=5���">:'� �"���%�"�<��"��'� �"�5%�"����"�='�
���>� 5"=5�%5"�<�5">5'� �"���%�"><��"�5'� �"�<�%�"�:��"��'� �"���%�"����"�='� �":5�%�":>��"5�'� �"=5�%�"==���">�'� �"���%�"�<��"��'� �"��%�"�>��"�>'�
����� 5">��%5"=��5"��'� �">��%�"=5��">:'� �"���%�"�5��"=�'� �"�>�%�"����"�<'� �":>�%�":���":5'� �"=>�%�"=����"=�'� �"���%�"����"��'� �"��%�"�:��"�:'�
���:� 5"���%5"���5"=�'� �"���%�"����"=='� �"�<�%�"�5��"=�'� �"��%�"�:��"�>'� �"�<�%�"�:��":�'� �"=>�%�"=����"=<'� �"���%�"����"��'� �"�:%�"����"��'�
���5� 5"���%5"���5"=<'� �"=��%�"�5��"=�'� �"�=�%�"����"�>'� �"���%�"�5��"��'� �":��%�"�5��":='� �"���%�"�����"=='� �"���%�"����"��'� �"�:%�"����"��'�
���<� 5"=:�%5"�:�5">�'� �"=:�%�"=���">�'� �"�:�%�"�>��"�<'� �"�>�%�"����"�<'� �":��%�"�<��":='� �"=��%�"�<���"=�'� �"���%�"����"�='� �"=�%�"����"=:'�
����� 5"=��%5"�:�5">�'� �"=>�%�"=���"=<'� �"�<�%�"�:��"=�'� �"�>�%�"����"�<'� �"�5�%�"����":�'� �"�<�%�"�>���"=�'� �"���%�"����"�='� �"=5%�"=���">�'�
����� 5":>�%5"�>�5"5='� �"=��%�"=���">='� �"=��%�"����"=�'� �"=5�%�"==��">�'� �":��%�"�<��":='� �"==�%�"=����"=5'� �"�=�%�"����"�>'� �">=%�"=<��">�'�
����� 5"�>�%5"<>�<"�='� �">=�%�"=���">5'� �"=��%�"����"=�'� �">=�%�"=���">5'� �":=�%�":���"::'� �"=��%�"=����"=�'� �"�>�%�"�=��"��'� �"��%�">���"�:'�
����� <"���%<"�:�<"��'� �">��%�">���"�='� �"=��%�"=���"=>'� �"�=�%�"><��"�5'� �":=�%�":���":�'� �">>�%�">����"><'� �"���%�"����"��'� �">�%�">>��"�>'�
���=� <"=:�%<"�5�<>:'� �"�=�%�">���"�5'� �"=>�%�"=���"=�'� �":>�%�":���":<'� �":>�%�":���":5'� �">:�%�">����"��'� �"���%�"�=��"�:'� �"��%�">5��"�5'�
���>� <"5��%<":��<"<�'� �"�=�%�">���"�5'� �"=<�%�"=:��">�'� �"5<�%�"5>��"<�'� �":<�%�":���"5�'� �">5�%�">=���"��'� �"�:�%�"����"�5'��� �"><%�">=��"�='�
����� �"���%<"����"��'� �":��%�"�5��"::'� �">��%�"=<��">�'� �"�>�%�"<���"�<'� �"5=�%�"5���"5�'� �"�>�%�"�����"�<'� �"�:�%�"�>��"�5'� �"�>%�">���"��'�
..)�� �"��%�"5��":'� ��"<�%��"=����">'� �"��%�"<�="�'� ="5�%="��>"�'� ��"=�%��"��?��"='� �">�%�"��?��"5'� >"��%="���"�'� �"��%�":��">'�
..)��
������
����� =">�%="��="<'� �"5�%�"��=">'� :"��%>"��<"�'� 5"=�%:">�<"�'� ="<�%�":�?��"�'� ="��%�"��="5'� >"��%="��?��"�'� �"��%�"=��"�'�
..)��@�.+������������������������������"��.�������������������� �������� ������7������;�����������6����+�� "�..)��6����+�� �����������
�� �9�����+����+���� �A��"��"�,� ������ ������/��������� ���������/��������� ���������������������������������� � ������ �+���������������� &��
�����&������� � �����/��������+����� "�)�������� ���������������� ����������/�����������/���������� �������6��������� "��2��� �����
��������/��������� �������������������"
Page 28 of 31
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
��
�
�������������#�/���������������������� � �
�
� (���������������� � ����� � ���4+������
�� �� ��,����..)������������
%��;�6'�
..)������������
�%��;�6'��
..)������������
%��;�6'�
..)������������
�%��;�6'��
.�����+����� �� � �
%B5��B5:'� �"��%�":��"�'� �"��%�"��?��"�'�
�"��%�"5��":'� =">�%="��="<'������������+����� �� �C� �">%�"��?��"�'� �"��%�":��"5'�
.������ ���� ����� �"��%�">��"<'� >"5�%>"���"�'�
.����������� �� �� ��"<�%�=">�����"='� ��"��%��"=�����"5'�
����������� �="=�%�=">����="�'� �="=�%�=">����="�'�
� ����� � ��������� ���������� �� �������
)�������� � ��"��%��"5�����">'� ��"��%��"5�?��"�'� �"��%�"<�="�'� :"��%>"��<"�'�
��� � � �"=�%��"���"5'� �"��%�"���"='� ="5�%="��>"�'� 5"=�%:">�<"�'�
����/�+� ����������
6 �������������� �� �� �="=�%�=":�����"�'� ��"=�%��"������"<'� �">�%�"��?��"5'� ="��%�"��="5'�
,6�/���������
%���+�������'� ��"��%��"<�����":'� �"��%��":�?��"�'� ��"<�%��"=����">'� �"5�%�"��=">'�
.��9���?������� � � ��"=�%��"5�����"<'� ��"5�%��"=�����"�'� �"�%�"���"<'� ="<%�"=��"�'�
(�7�$�D���?��
������� � � ��"��%��"�����"5'� ��"��%��"�����"5'� �"��%�"��>"�'� �"5�%=">�<"�'�
3�����?��
������� � � ��"��%��">�����"�'� ��"��%��">�����"�'� ="5�%�"���":'� ="5�%�"���":'�
�..)��@�.+������������������������������"��.�������������������� �������� ������7������;�
����������6����+�� "�..)��6����+�� ������������� �9�����+����+���� �A��"��"�C�B5��%.���������+���
�� �� �'&�B5��%#D���E�+����� �� �'&�B5��%���������������&������ �7�������� �����&�B5>�%2�/� � �����
����� � ���������+��'&�B5�">�%.��������������� '&�B5:":�%)������������� ��'&�B5:"5�%�����������
�����'"��������� �� �����������������7������/��������� ��������/���� �������������&����F�������
�������������� ���������������������������� *������ ������+����� �� �"�#��� ���� �7���� ��������������
/� � �������������� � ����������������� "�
�
� �
Page 29 of 31
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
��
�
�������������2���������#���� ����.�������������$�������
�
E�����2�� �����D��� �+����������������+����� �� ��%6�������B5�'&���������� ������� ����+���������
���������� �/������ ������ ����������=>�������������"�3���������������������������� �
�� ������&������+�������������������������������%..)�'�� ������� �������� ����=>"�
1������#���� �����������������/�������������� ���� �����%6������2��'�������������"�3��������������
�������������� ��� ������&������������� ��������������������� "��7�+��&���� �� �/���� ��������������
�����������<�%��� �7�'������� ���+�� ���������������"�$������������� ������������ ������������
��+����� �� �"�
�
�
� �
Page 30 of 31
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
��
�
�������������2���������.+������.������)�����������������%..)�'����$��������������.������ ��
�� �����
�
(����$���� ���� �7�����D�������������������� ���� ���������/���� ������������� �7������� �����������
%�������� �+������� ���������������� '"�
#���#���..)�������������/�� ��������������� ���� ������ � �7��������������"�������������
������ � �7����/ ��+������ �+����� ���� G����� &� �����/��������� �����������/��"�6����� � �7����
/ ��+����� �7����&����/���1����6 ����"�
!���������������� �����/ ��+���7��������������� ��� �������������������"��7�+��&� �+����� ���� �
��+����+���������������+�� ������� ����������� ���� ������������&�������67�&�$����&�����������&�
(�7�$�D��&�$� ���� ��� &�6�����������4����"�
Page 31 of 31
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960