LIVER CIRRHOSIS LIVER CIRRHOSIS. THE ANATOMY OF THE PORTAL VENOUS SYSTEM.
61
LIVER CIRRHOSIS LIVER CIRRHOSIS
-
Upload
magdalen-clarke -
Category
Documents
-
view
307 -
download
19
Transcript of LIVER CIRRHOSIS LIVER CIRRHOSIS. THE ANATOMY OF THE PORTAL VENOUS SYSTEM.
LIVER CIRRHOSIS LIVER CIRRHOSIS
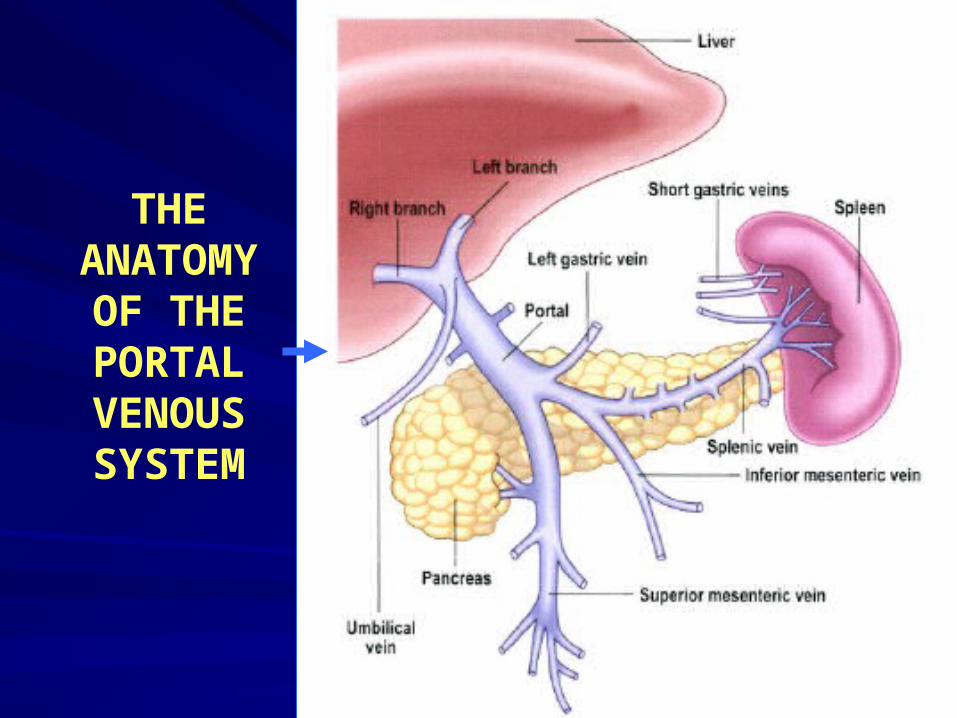
THE ANATOMY
OF THE PORTAL VENOUS SYSTEM
LIVER CIRRHOSISLIVER CIRRHOSIS
Diffuse disorganization of normal Diffuse disorganization of normal hepatic structure by regenerative hepatic structure by regenerative nodules that are surrounded by nodules that are surrounded by fibrotic tissue.fibrotic tissue.
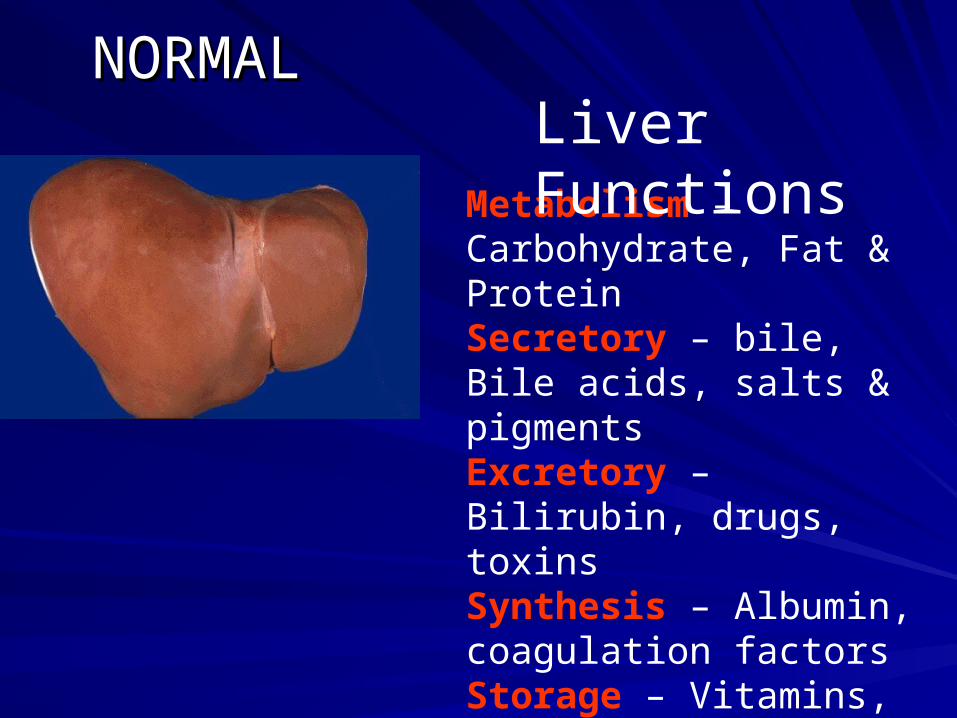
NORMALNORMAL
Metabolism – Carbohydrate, Fat & ProteinSecretory – bile, Bile acids, salts & pigmentsExcretory – Bilirubin, drugs, toxinsSynthesis – Albumin, coagulation factorsStorage – Vitamins, carbohydrates etc.Detoxification – toxins, ammonia, etc.
Liver Functions
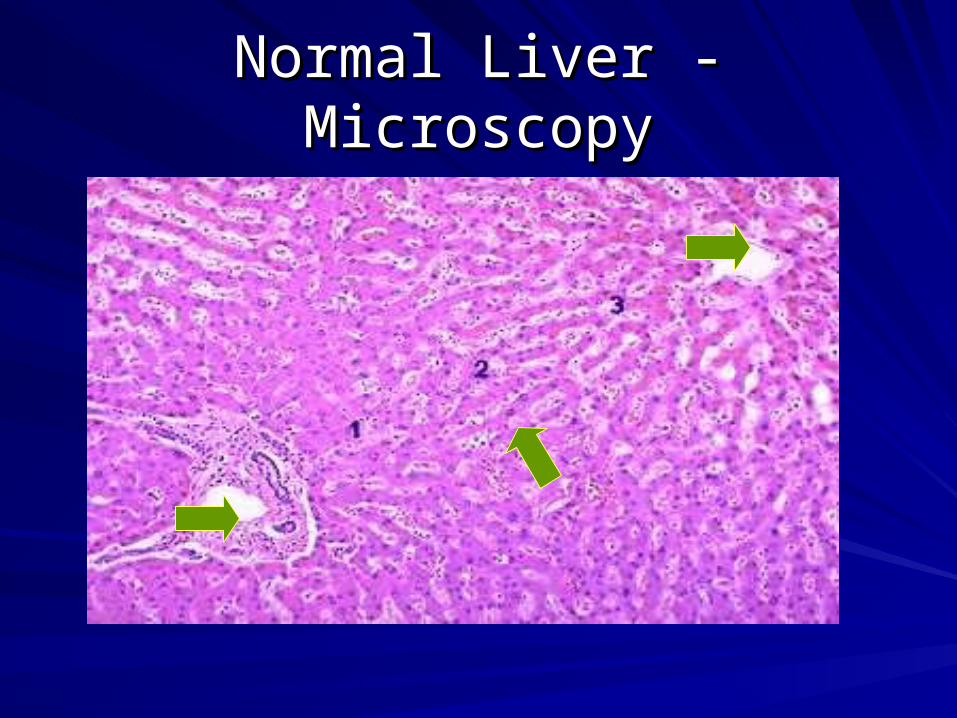
Normal Liver - MicroscopyNormal Liver - Microscopy
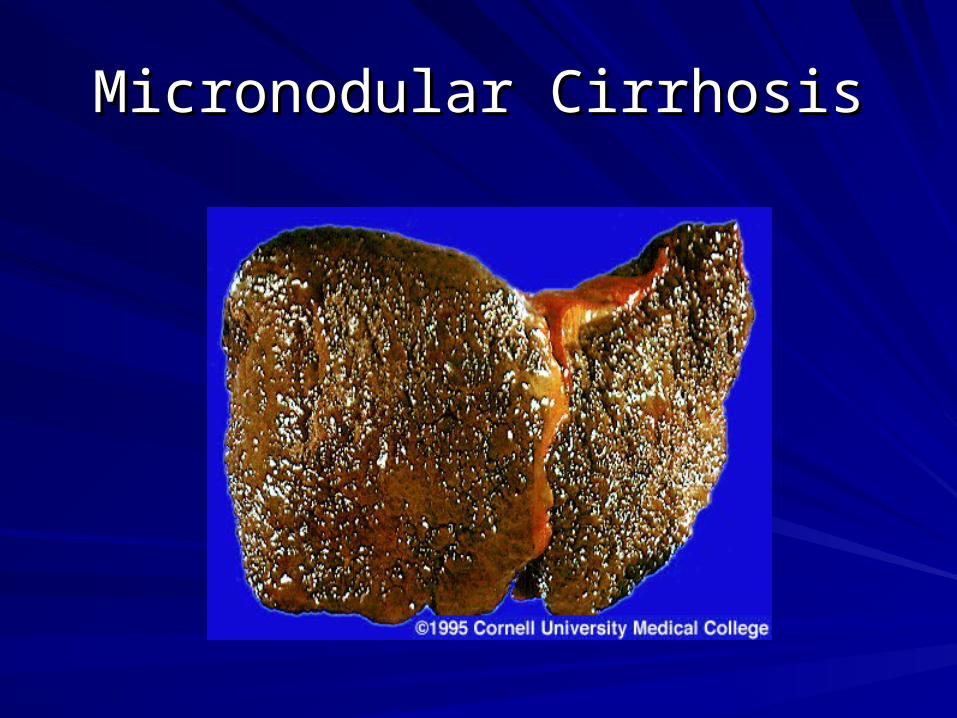
Micronodular CirrhosisMicronodular Cirrhosis
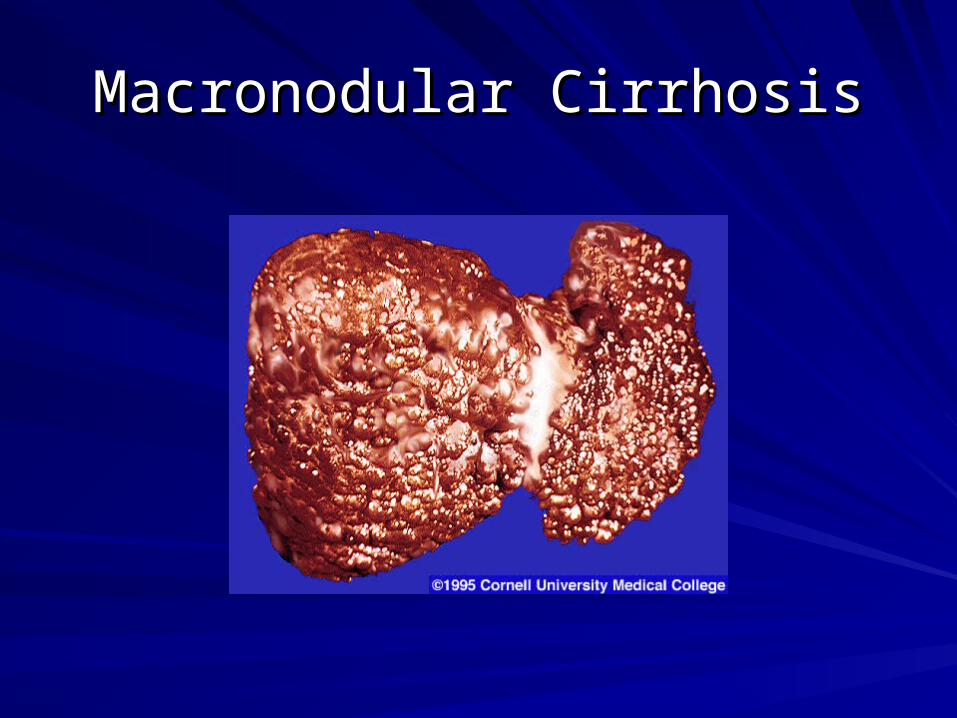
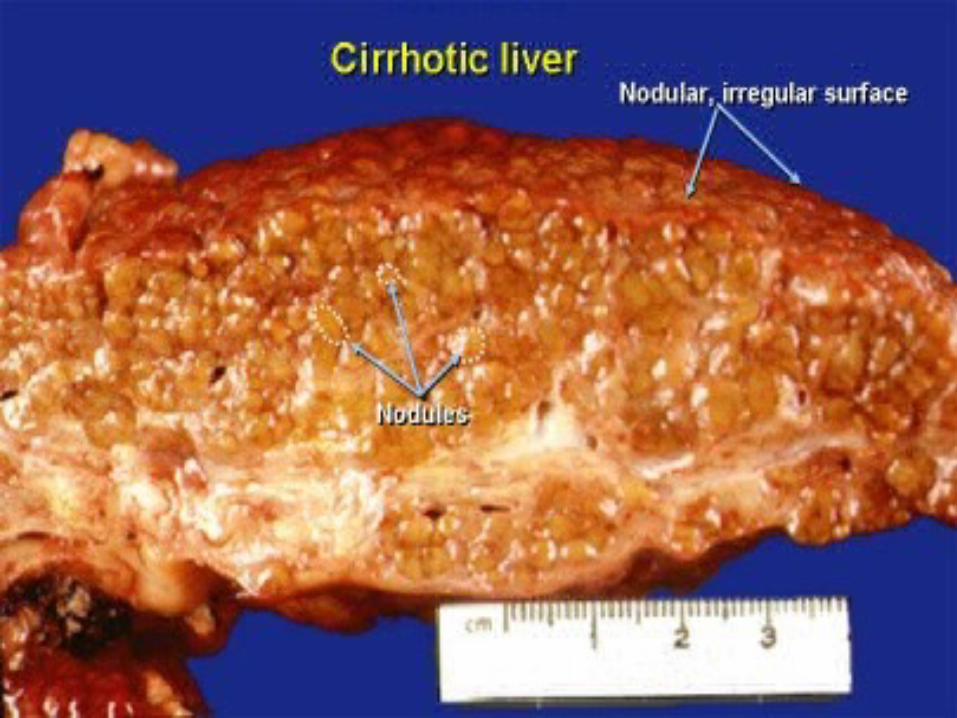
Macronodular CirrhosisMacronodular Cirrhosis
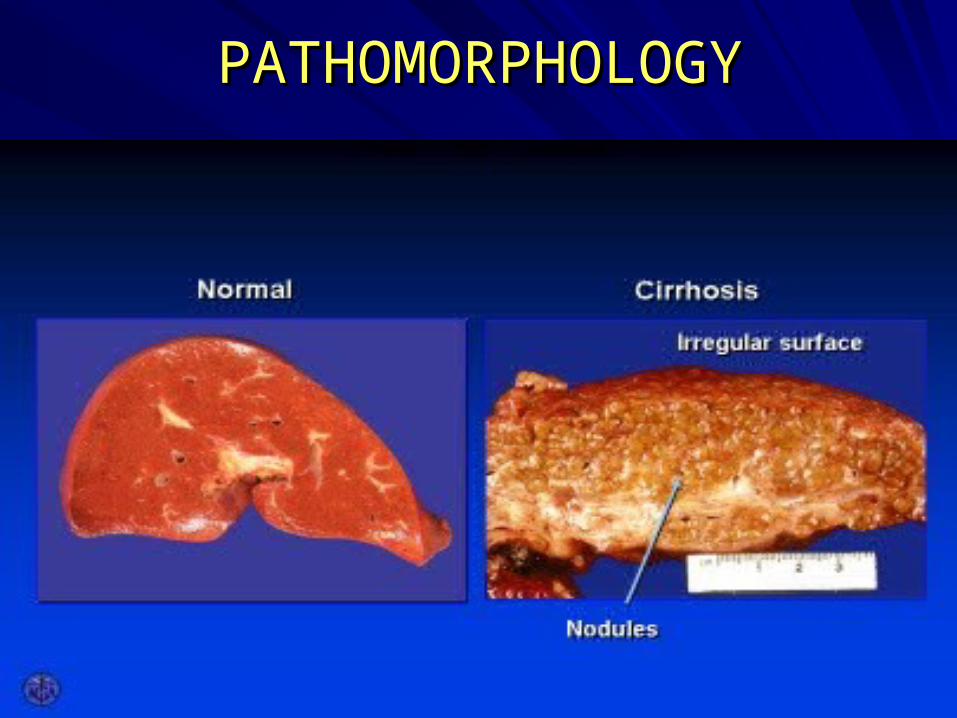
PATHOMORPHOLOGYPATHOMORPHOLOGY
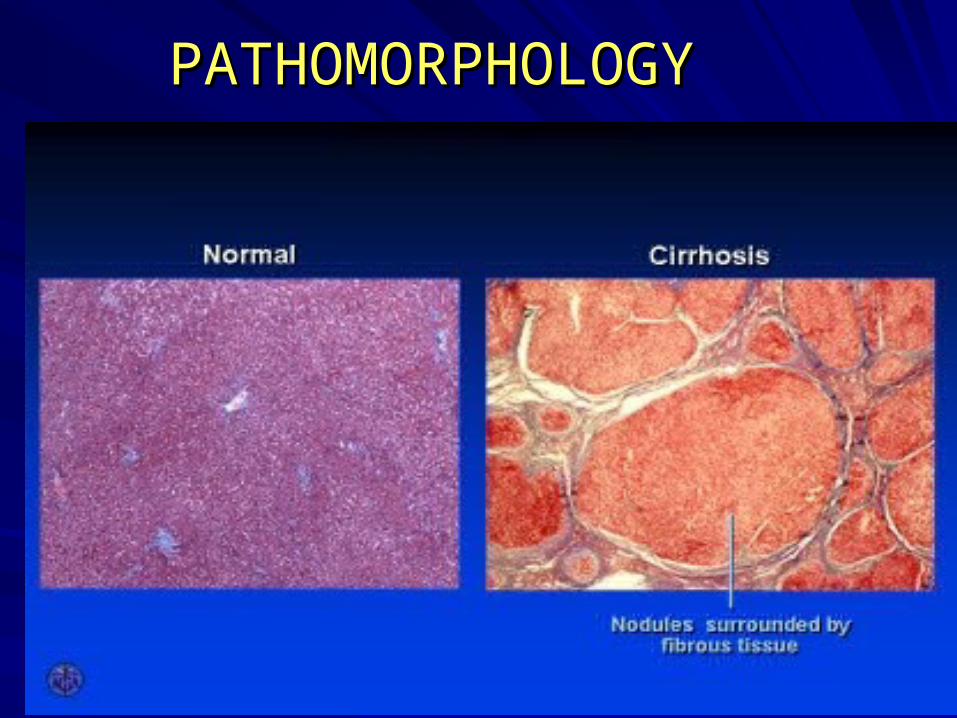
PATHOMORPHOLOGYPATHOMORPHOLOGY
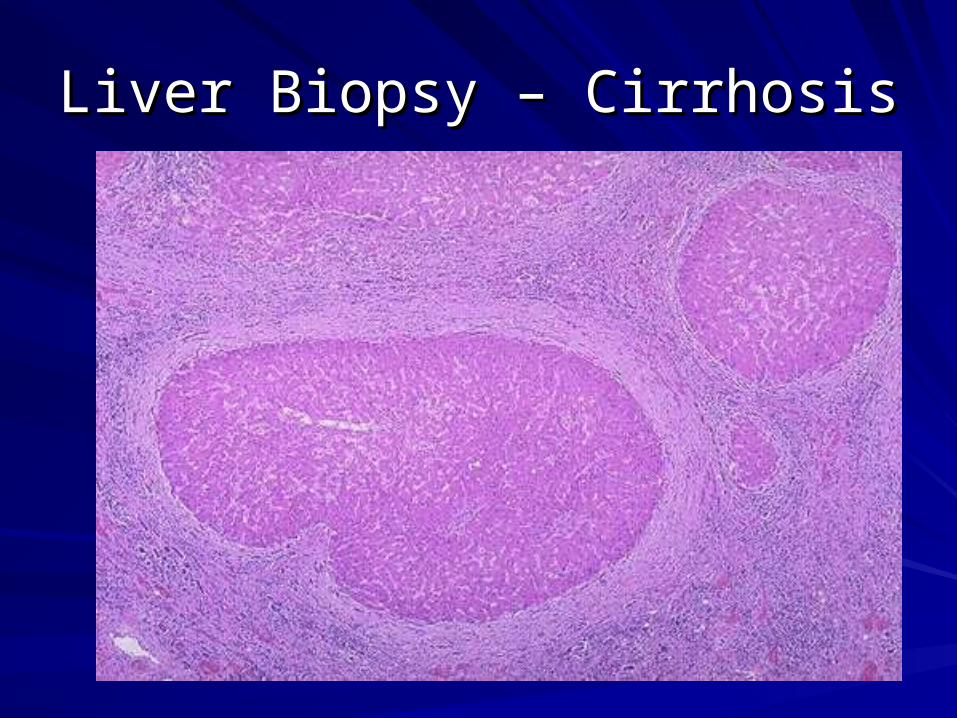
Liver Biopsy – CirrhosisLiver Biopsy – Cirrhosis
LIVER CIRRHOSISLIVER CIRRHOSIS CLASSIFICATIONCLASSIFICATION (etiologic) (etiologic)
VViraliral
AlcoholicAlcoholic
ToxicToxic
AutoimmuneAutoimmune
MetabolicMetabolic
ССongestiveongestive
BiliaryBiliary
CCryptogenic ryptogenic
LIVER CIRRHOSISLIVER CIRRHOSIS CLASSIFICATIONCLASSIFICATION
CLASSIFICATION CLASSIFICATION ((HistopathologicHistopathologic ))
MicronodularMicronodular (nodules(nodules < 3 < 3 mm mm
in diameter)in diameter)
MacronodularMacronodular(nodules(nodules >> 3 3 mm mm
in diameter)in diameter)
MixedMixed
LIVER CIRRHOSISLIVER CIRRHOSIS CLASSIFICATIONCLASSIFICATION
DEGREE OF PROGRESSDEGREE OF PROGRESS AND PROCESSAND PROCESS
ACTIVITYACTIVITY
ACTIVEACTIVE NONACTIVE
QuicklyQuickly progressiveprogressive
SlowlySlowly progressiveprogressive
Latent
LIVER CIRRHOSISLIVER CIRRHOSIS CLASSIFICATIONCLASSIFICATION
SEVERITY OF DISEASE
Compensation stage
Subcompensation stage
Decompensation stage
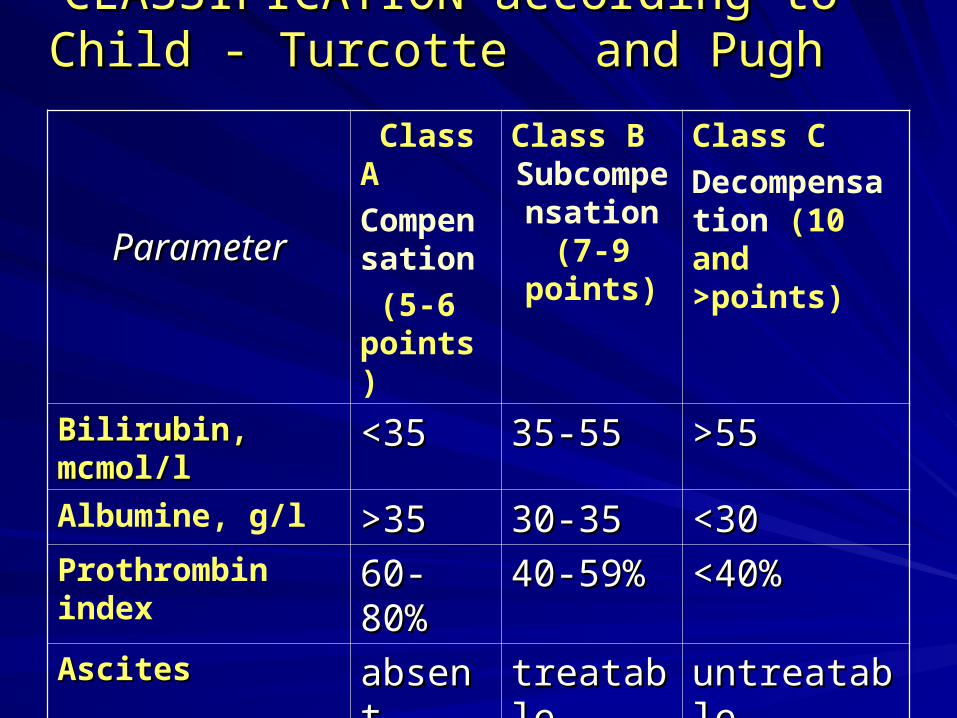
CLASSIFICATION according toCLASSIFICATION according to Child - Turcotte and Pugh Child - Turcotte and Pugh
ParameterParameter
Class A
Compensation
(5-6 points)
Class BSubcompensation
(7-9 points)
Class C
Decompensation (10 and >points)
Bilirubin, mcmol/lBilirubin, mcmol/l <35<35 35-5535-55 >55>55Albumine, g/l >35>35 30-3530-35 <30<30Prothrombin index 60-80%60-80% 40-59%40-59% <40%<40%AscitesAscites absentabsent treatabletreatable untreatableuntreatableEncephalopathy Encephalopathy absentabsent 1-2 st.1-2 st. 3-4 st.3-4 st.
PointsPoints:: 11 22 33
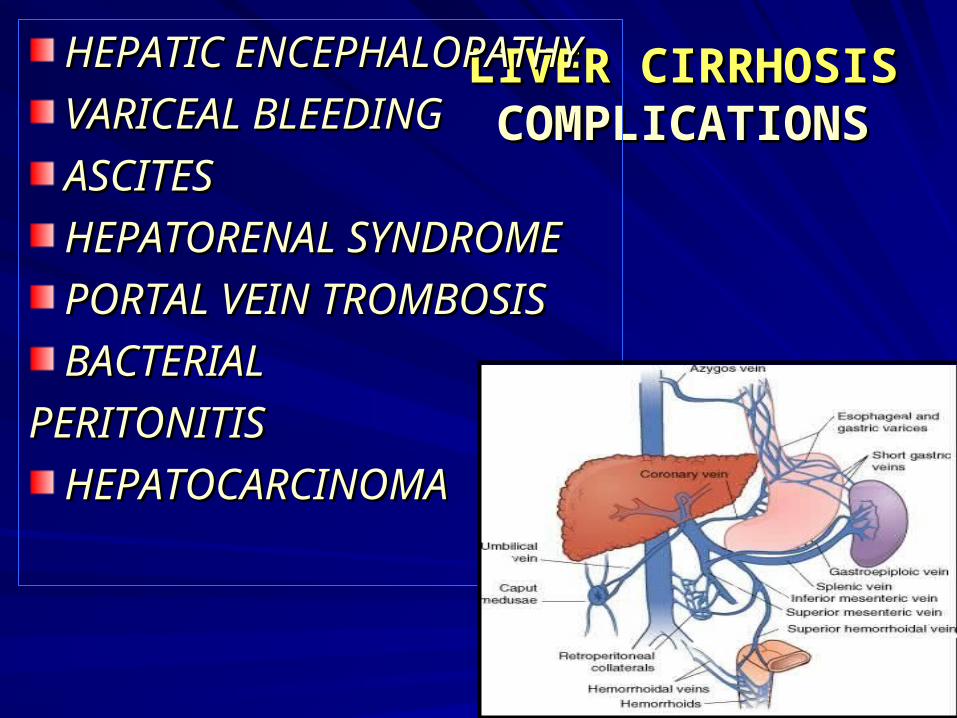
LIVER CIRRHOSISLIVER CIRRHOSISССOMPLICATIONSOMPLICATIONS
HEPATIC HEPATIC ENCEPHALOPATHY ENCEPHALOPATHY
VVARICEAL BLEEDINGARICEAL BLEEDING
ASCITESASCITES
HEPATORENAL SYNDROMEHEPATORENAL SYNDROME
PORTAL VEIN TROMBOSISPORTAL VEIN TROMBOSIS
BACTERIAL BACTERIAL
PERITONITISPERITONITIS
HEPATOCARCINOMAHEPATOCARCINOMA
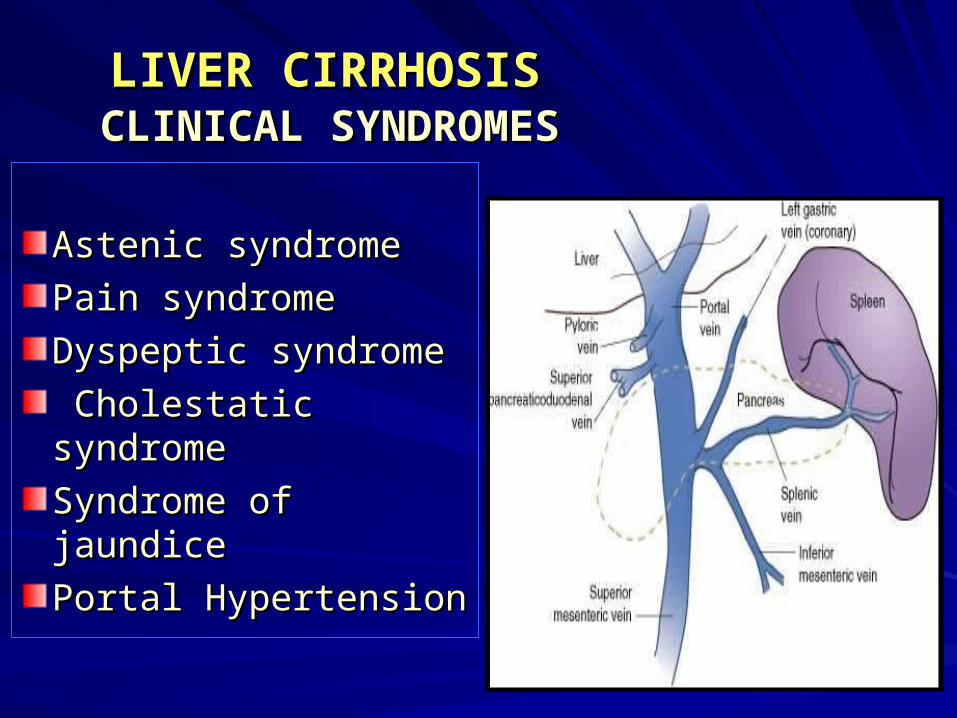
LIVER CIRRHOSISLIVER CIRRHOSIS CLINICAL SYNDROMES CLINICAL SYNDROMES
Astenic syndrome Astenic syndrome
Pain syndromePain syndrome
Dyspeptic syndromeDyspeptic syndrome
Cholestatic Cholestatic syndromesyndrome
Syndrome of jaundiceSyndrome of jaundice
Portal HypertensionPortal Hypertension
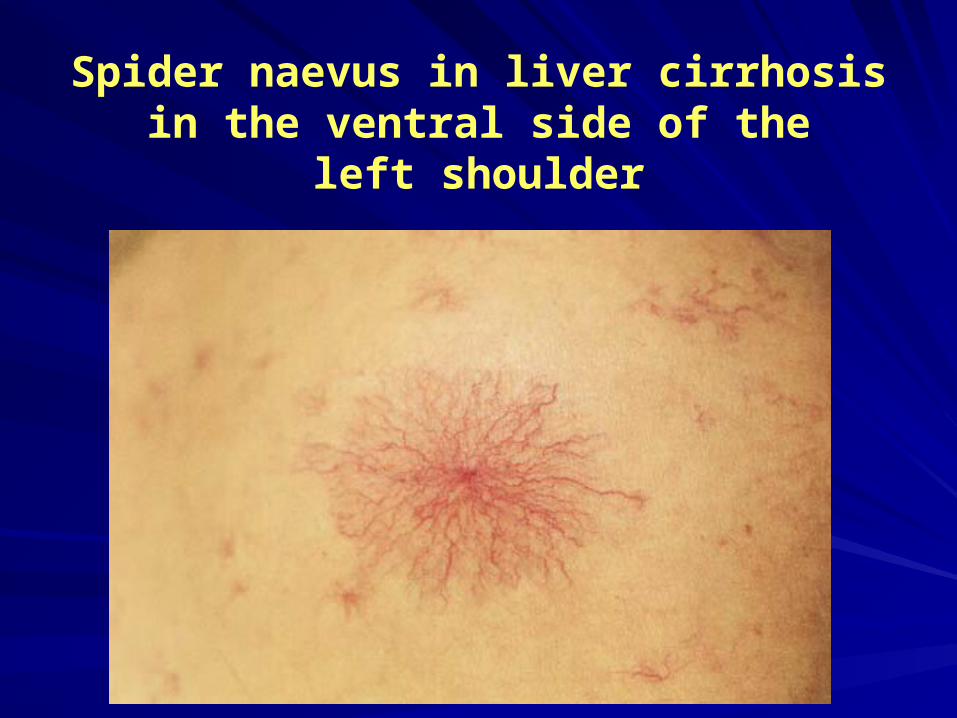
Spider naevus in liver cirrhosis in the ventral side of the
left shoulder
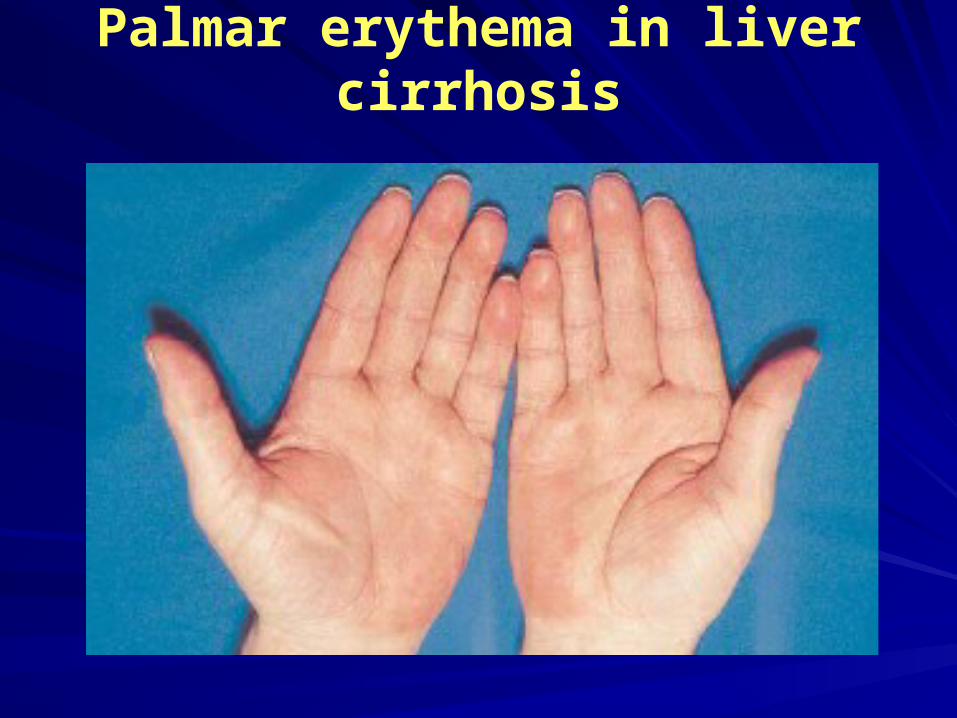
Palmar erythema in liver cirrhosis
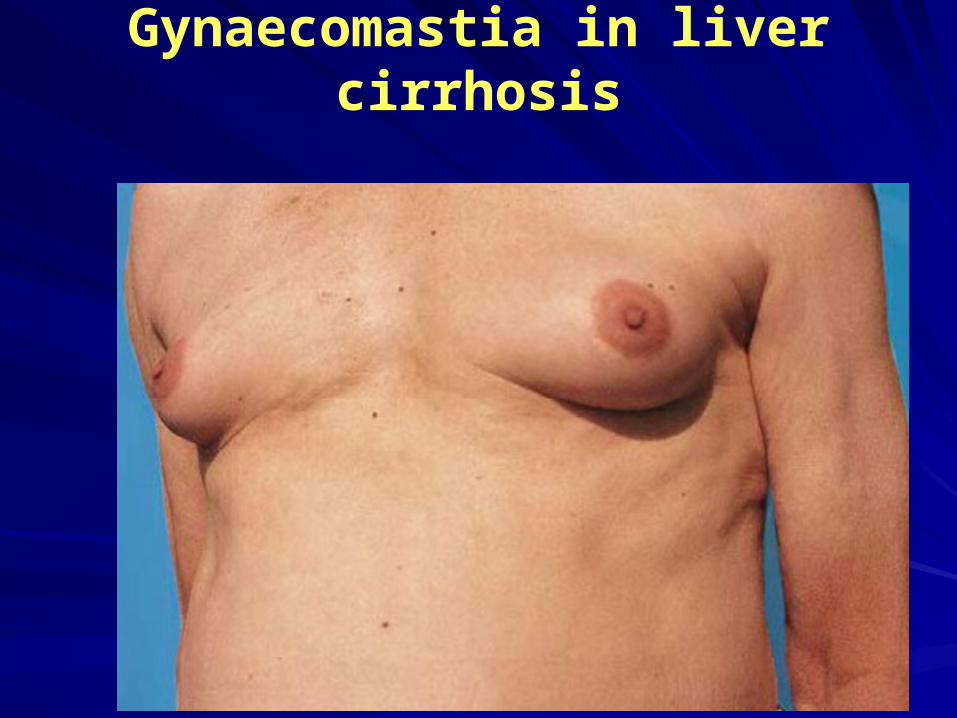
Gynaecomastia in liver cirrhosis

Xanthelasmas in biliary cirrhosis as a result of primary
biliary cholangitis
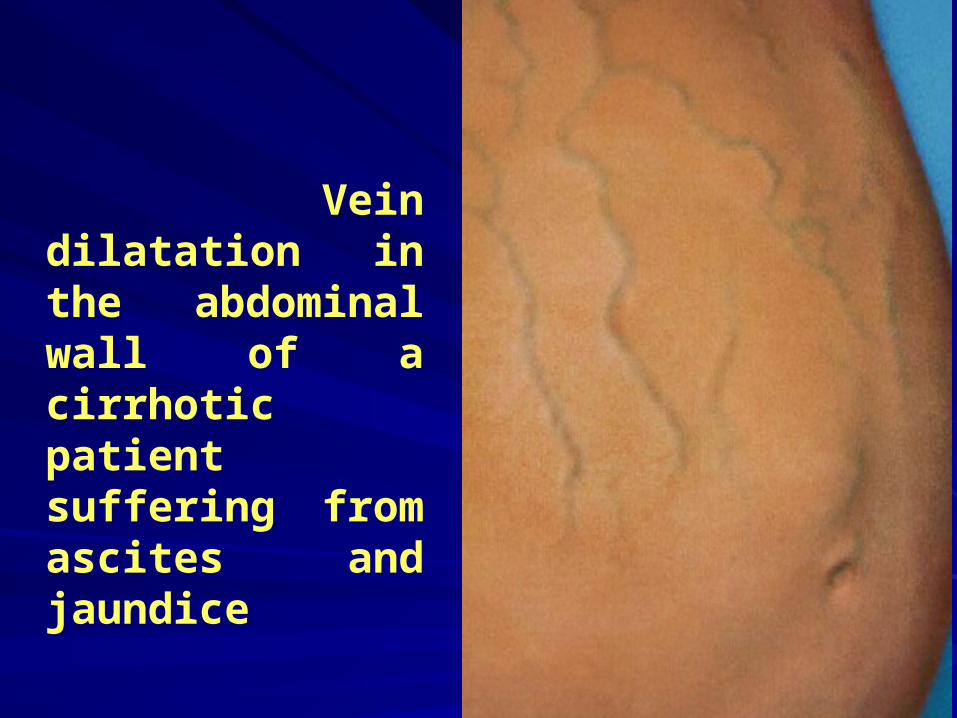
Vein dilatation in the abdominal wall of a cirrhotic patient suffering from ascites and jaundice
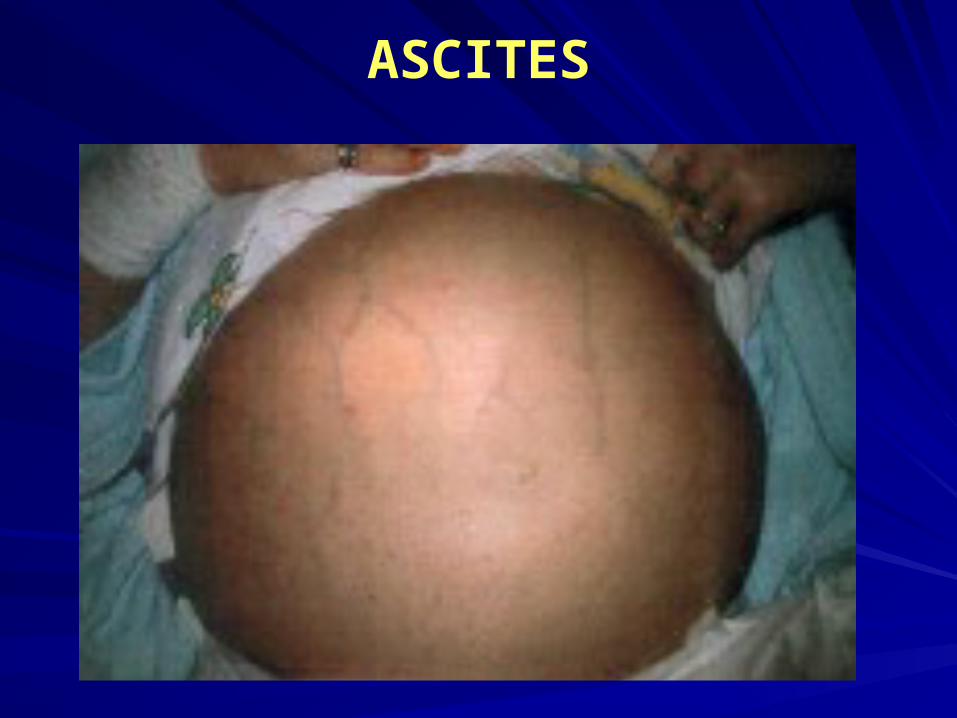
ASCITES
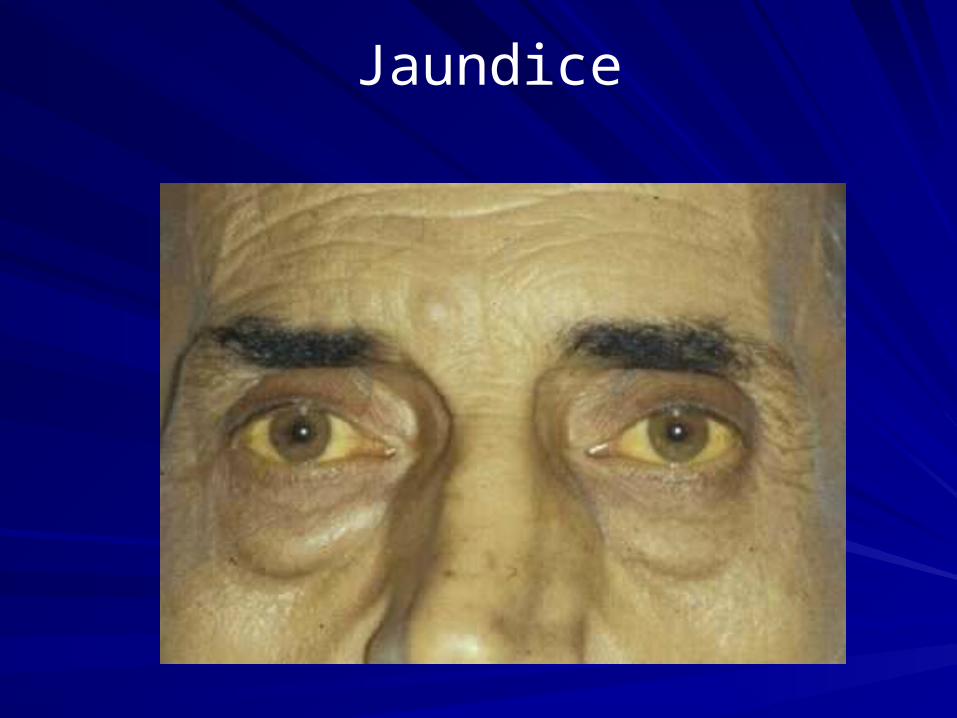
Jaundice
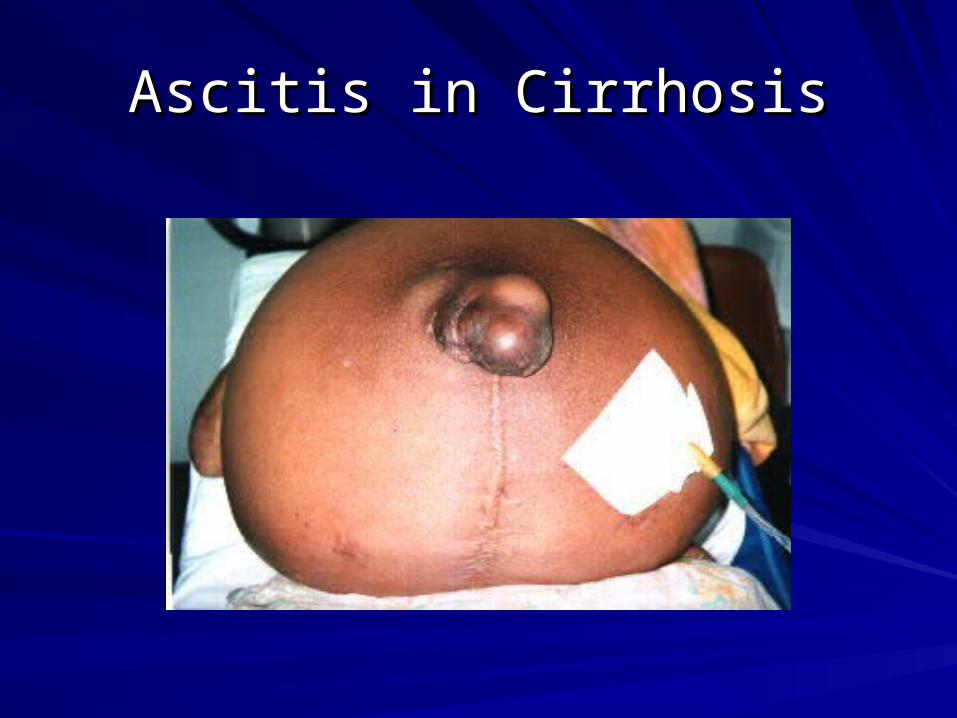
Ascitis in CirrhosisAscitis in Cirrhosis
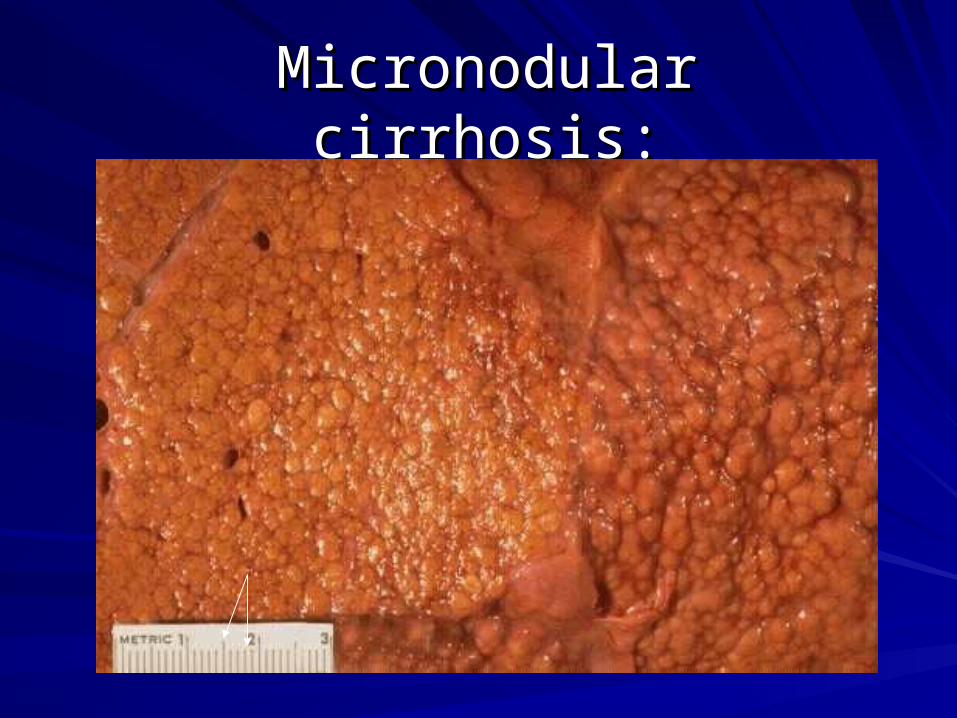
Micronodular cirrhosis:Micronodular cirrhosis:
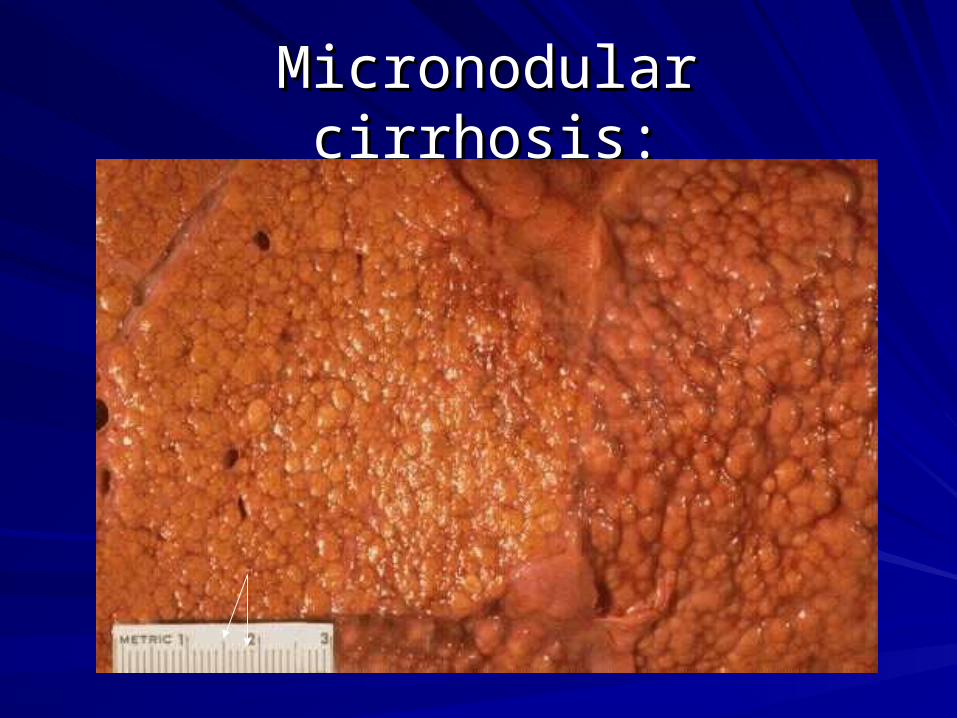
Micronodular cirrhosis:Micronodular cirrhosis:
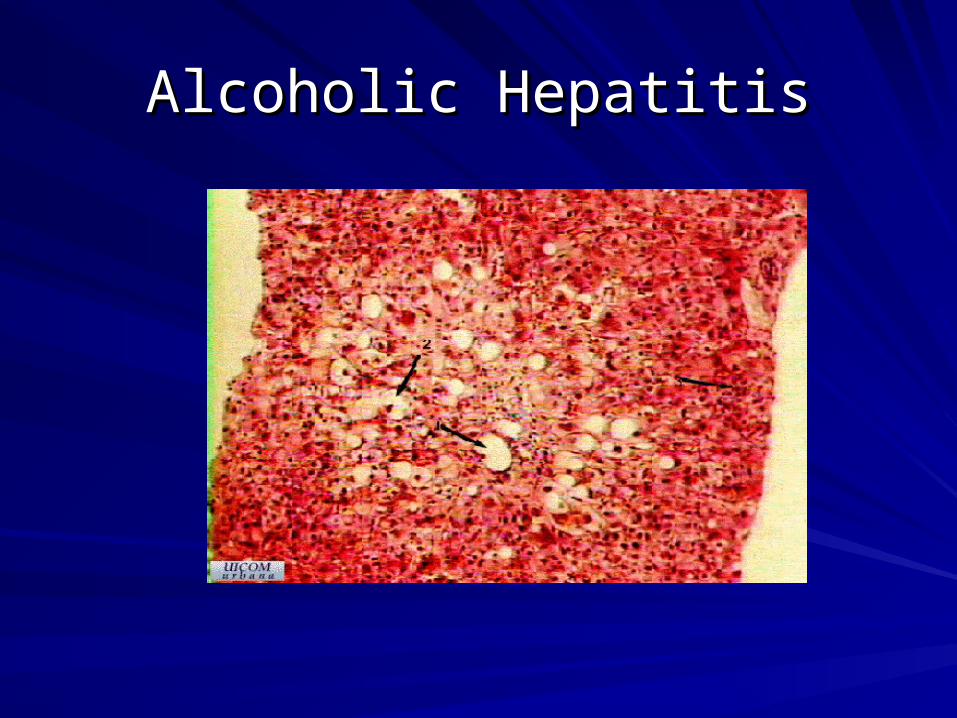
Alcoholic HepatitisAlcoholic Hepatitis

Macronodular CirrhosisMacronodular Cirrhosis
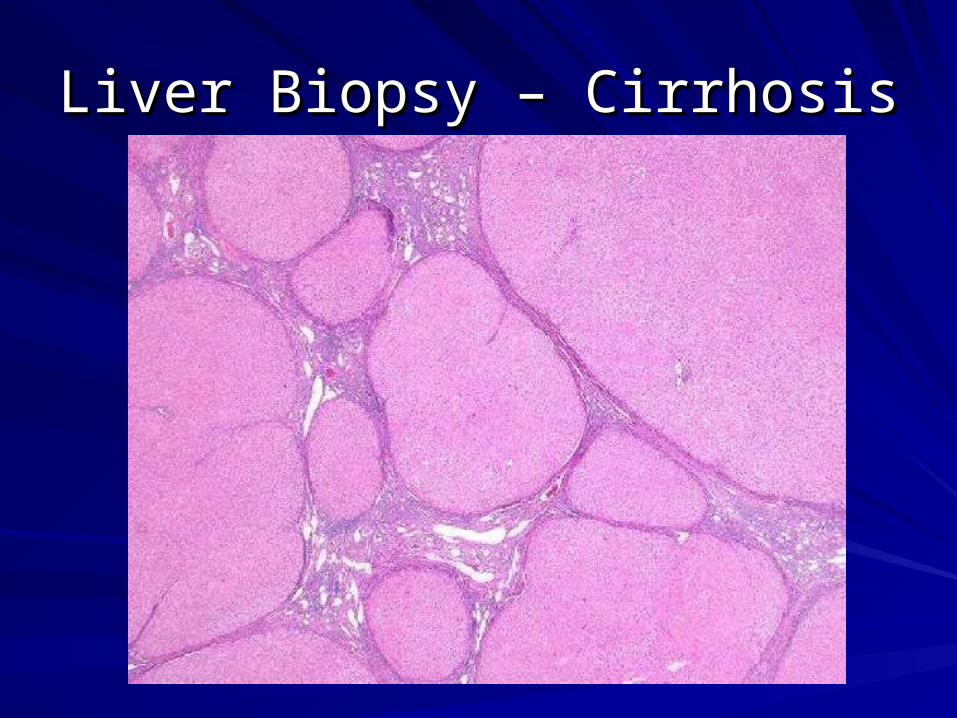
Liver Biopsy – CirrhosisLiver Biopsy – Cirrhosis
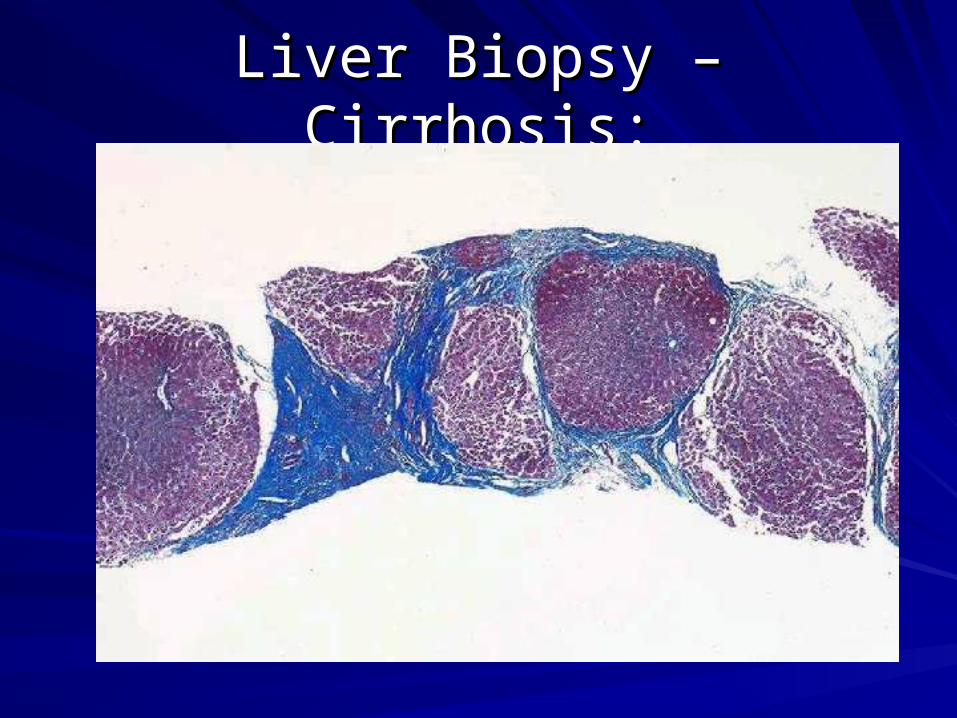
Liver Biopsy – Cirrhosis:Liver Biopsy – Cirrhosis:
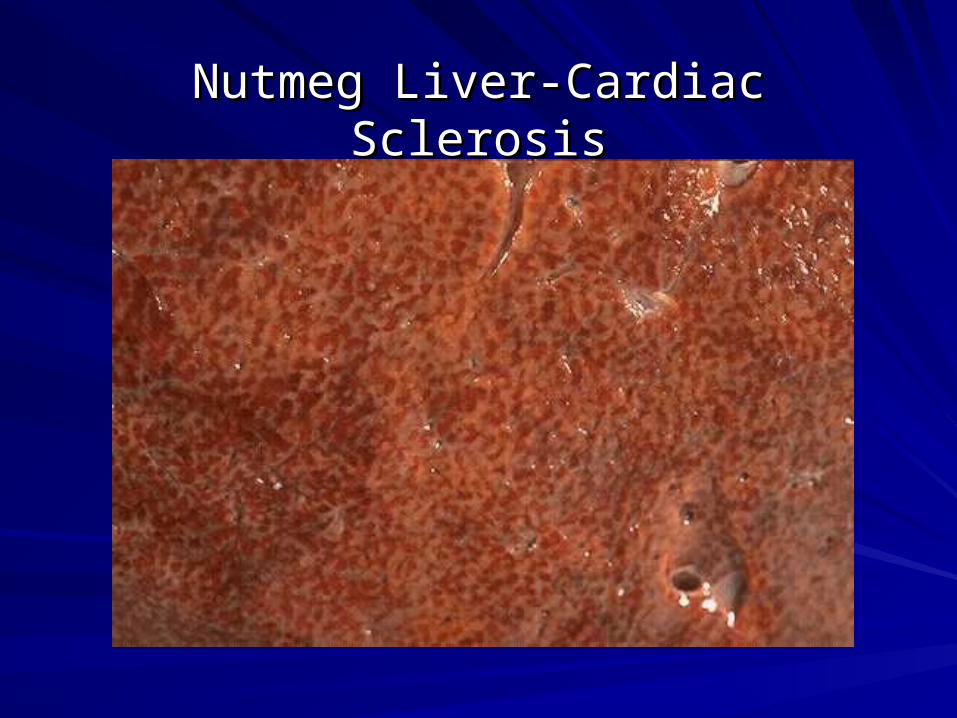
Nutmeg Liver-Cardiac SclerosisNutmeg Liver-Cardiac Sclerosis
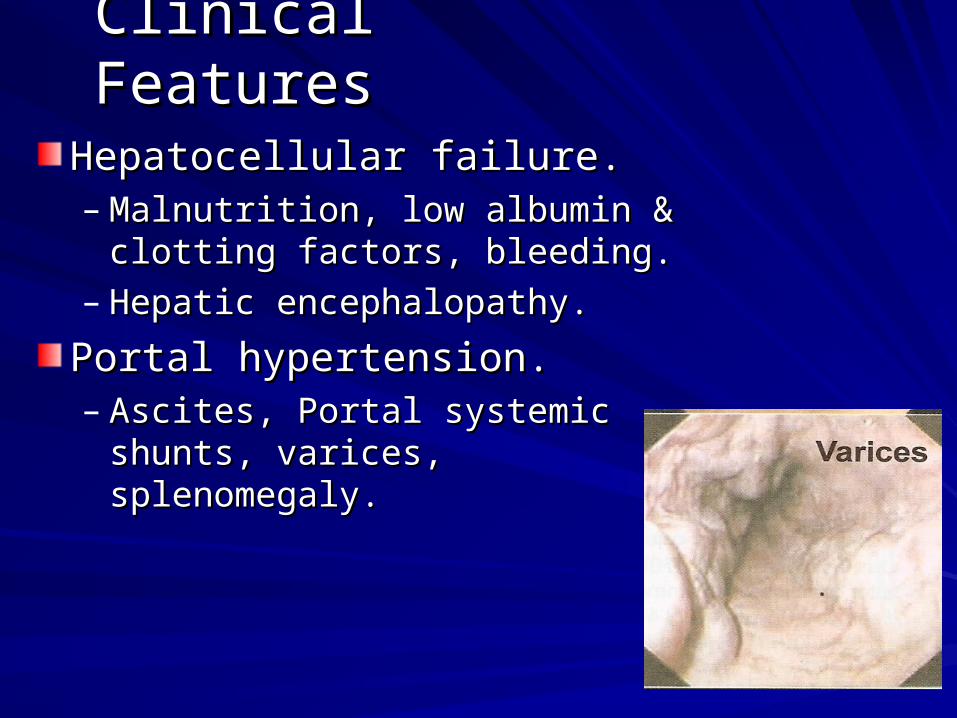
Clinical FeaturesClinical Features
Hepatocellular failure.Hepatocellular failure.– Malnutrition, low albumin & clotting Malnutrition, low albumin & clotting
factors, bleeding.factors, bleeding.– Hepatic encephalopathy.Hepatic encephalopathy.
Portal hypertension.Portal hypertension.– Ascites, Portal systemic shunts, Ascites, Portal systemic shunts,
varices, splenomegaly.varices, splenomegaly.
Bleeding in Liver disease:Bleeding in Liver disease:
vitamin K – in liver vitamin K – in liver gamma-gamma-carboxyglutamic acid – for coagulation carboxyglutamic acid – for coagulation factors II, VII, IX, and X. factors II, VII, IX, and X.
Liver disease Liver disease factor VII is the first to go factor VII is the first to go so the defect will appear initially in the so the defect will appear initially in the extrinsic pathway, i.e., abnormal PT. extrinsic pathway, i.e., abnormal PT. When severe it affects both pathways.When severe it affects both pathways.
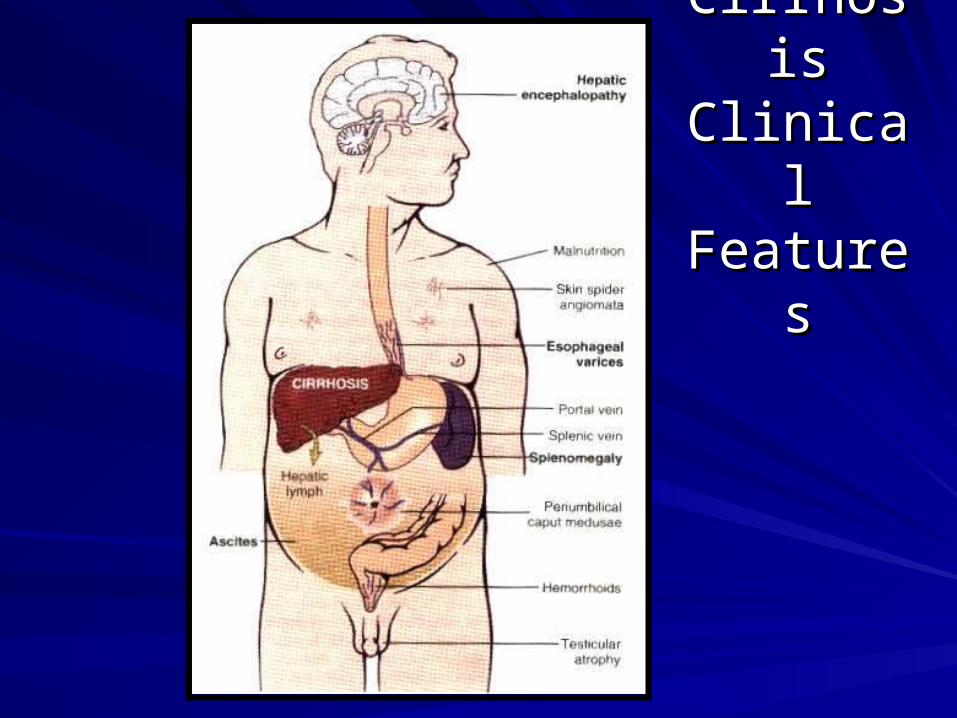
CirrhosisCirrhosisClinical Clinical
FeaturesFeatures
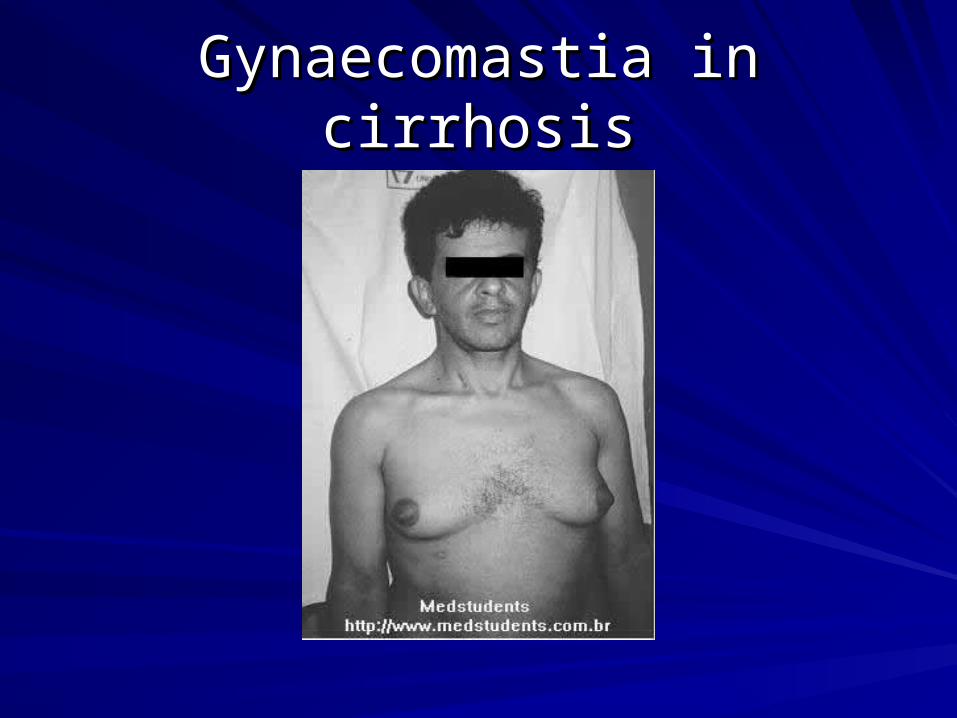
Gynaecomastia in cirrhosisGynaecomastia in cirrhosis
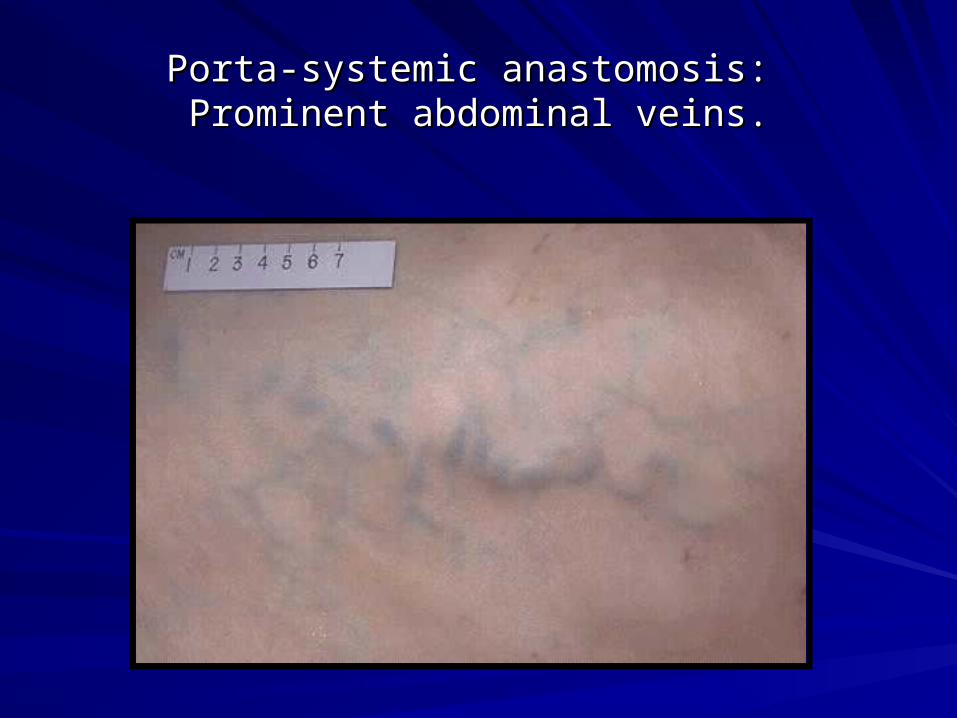
Porta-systemic anastomosis: Porta-systemic anastomosis: Prominent abdominal veins.Prominent abdominal veins.
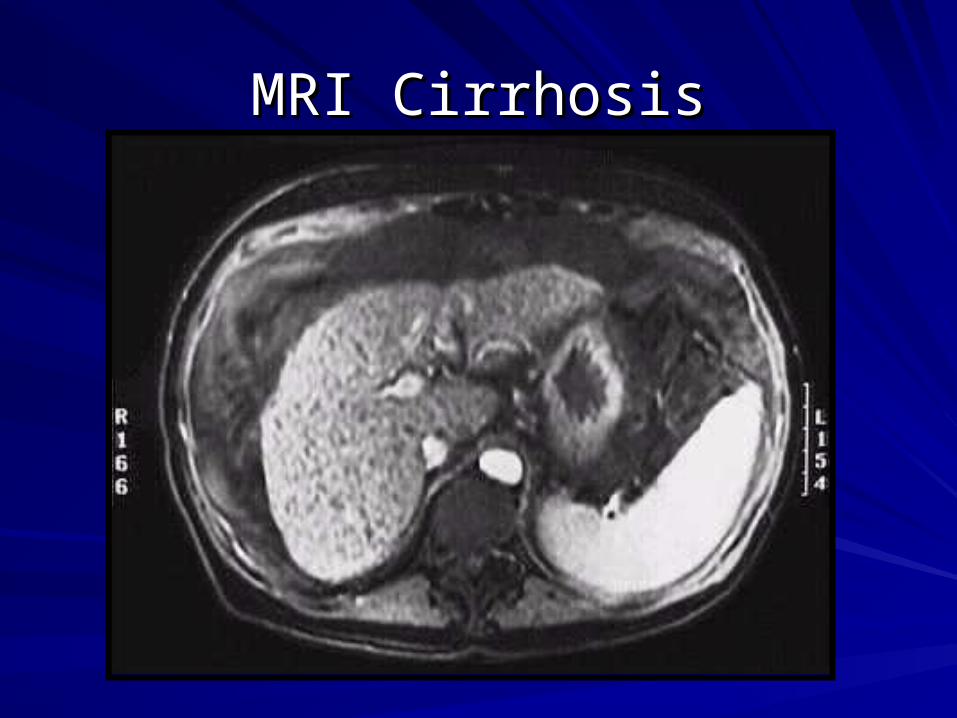
MRI CirrhosisMRI Cirrhosis

Complications:Complications:Congestive splenomegaly.Congestive splenomegaly.Bleeding varices.Bleeding varices.Hepatocellular failure.Hepatocellular failure.– Hepatic encephalitis / hepatic coma.Hepatic encephalitis / hepatic coma.Hepatocellular carcinoma.Hepatocellular carcinoma.
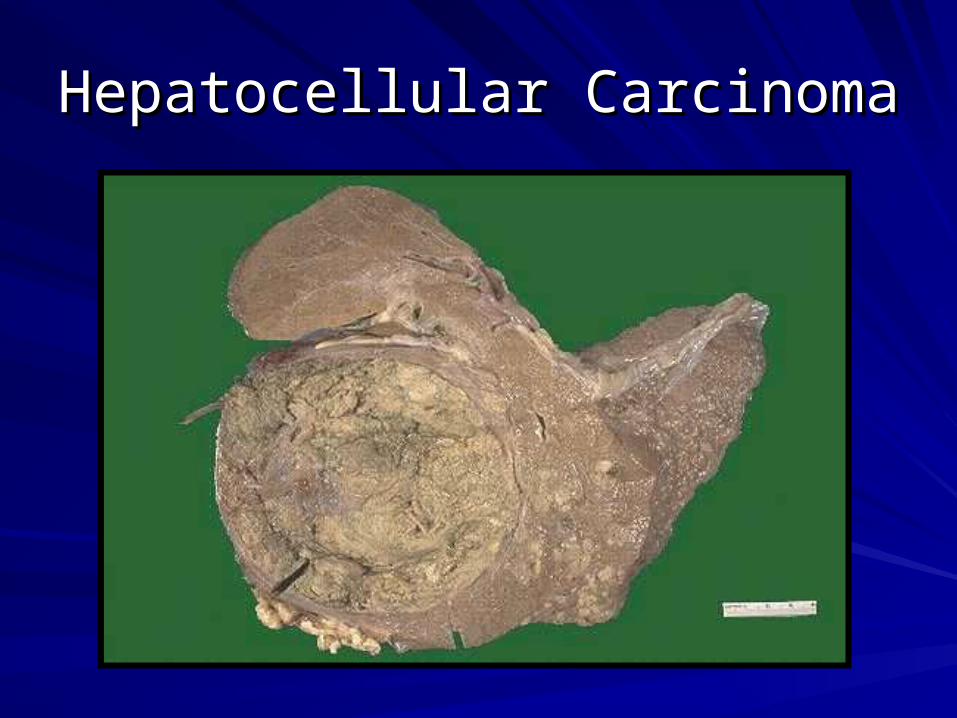
Hepatocellular CarcinomaHepatocellular Carcinoma
LIVER CIRRHOSISLIVER CIRRHOSIS PLAN of INVESTIGATIONSPLAN of INVESTIGATIONS
Total blood count, Blood group and Rhesus factorBiochemical analysis (Glucose, Bilirubin, ALT, AST, GGT, Alkaline phosphatase, Albumin, الال-globulins, -globulins, Cholesterol, Cholesterol, Liver tests, Sodium, Potassium, Urea, Creatinine)Urinanalysis, Diastase of urineCoagulogramMarkers of VViral iral HHepatitisepatitis (chain polimerase reaction, (chain polimerase reaction, immunoenzyme analysis)immunoenzyme analysis)ImmunogramImmunogramECG, Endoscopy, USD, CT, EEGDiagnostic paracentesisNeedle liver biopsy
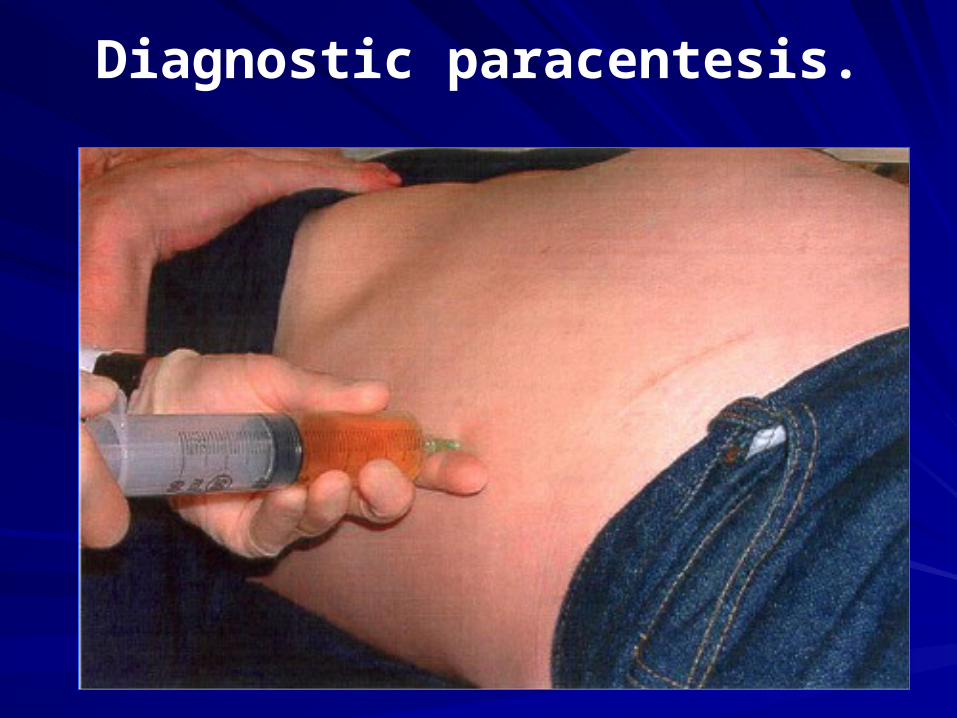
Diagnostic paracentesis.
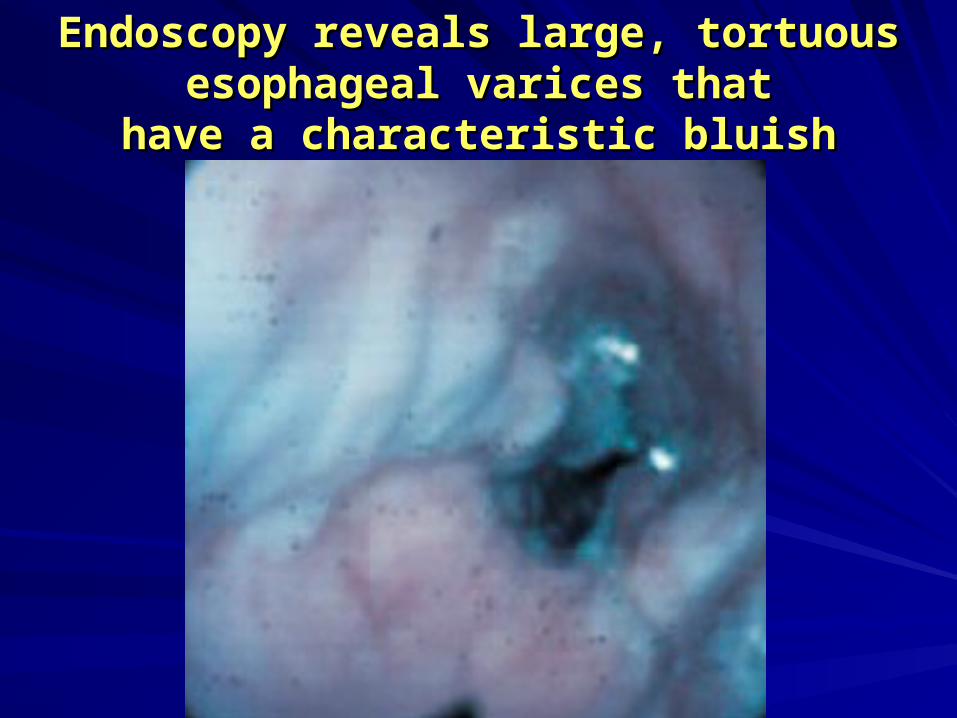
Endoscopy reveals large, tortuous Endoscopy reveals large, tortuous esophageal varices thatesophageal varices that
have a characteristic bluish colorhave a characteristic bluish color
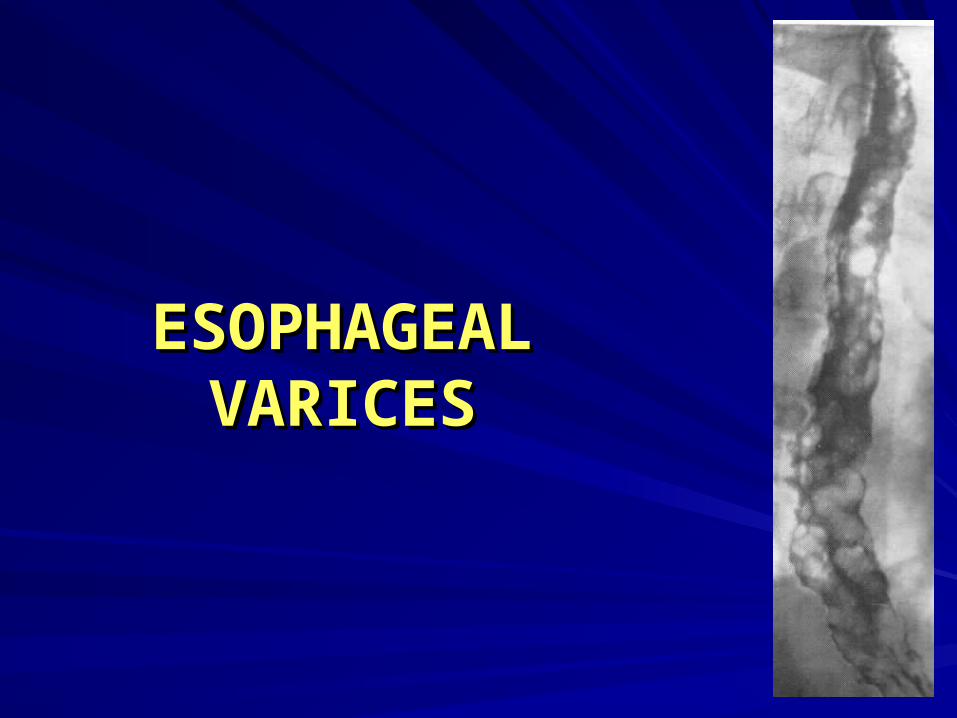
ESOPHAGEAL ESOPHAGEAL VARICESVARICES
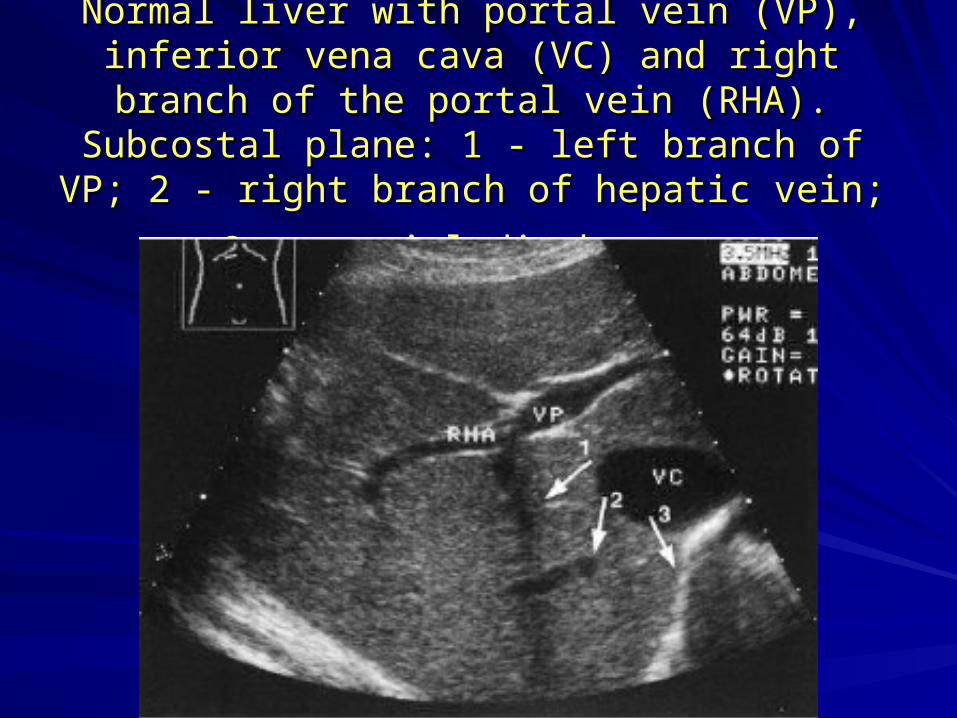
Normal liver with portal vein (VP), inferior vena Normal liver with portal vein (VP), inferior vena cava (VC) and right branch of the portal vein (RHA). cava (VC) and right branch of the portal vein (RHA).
Subcostal plane: 1 - left branch of VP; 2 - right Subcostal plane: 1 - left branch of VP; 2 - right
branch of hepatic vein; 3 - cranial diaphragmbranch of hepatic vein; 3 - cranial diaphragm

Liver cirrhosis with ascites Liver cirrhosis with ascites (longitudinal section): the (longitudinal section): the left lobe of liver is rounded left lobe of liver is rounded and plump; intrahepatic and plump; intrahepatic vessels are reduced. vessels are reduced. Irregular and Irregular and inhomogeneous structure. inhomogeneous structure. Clear undulatory limitation Clear undulatory limitation (arrow) on the underside (arrow) on the underside due to nodular due to nodular transformation.transformation.Wide hypoechoic fringe Wide hypoechoic fringe due to ascitesdue to ascites
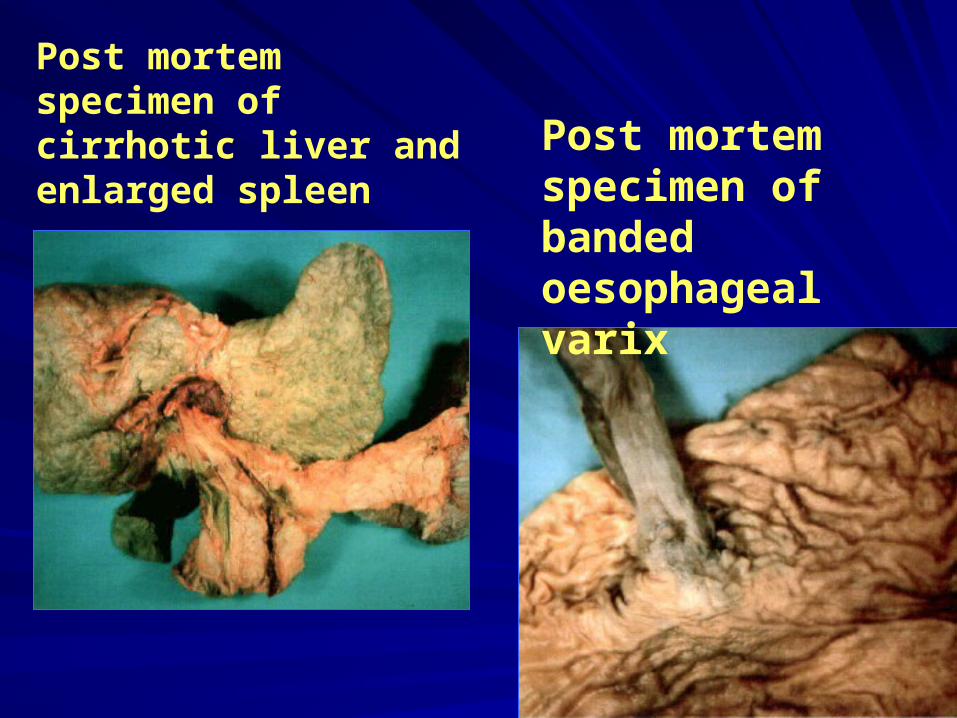
Post mortem specimen of cirrhotic liver and enlarged spleen Post mortem
specimen of banded oesophageal varix
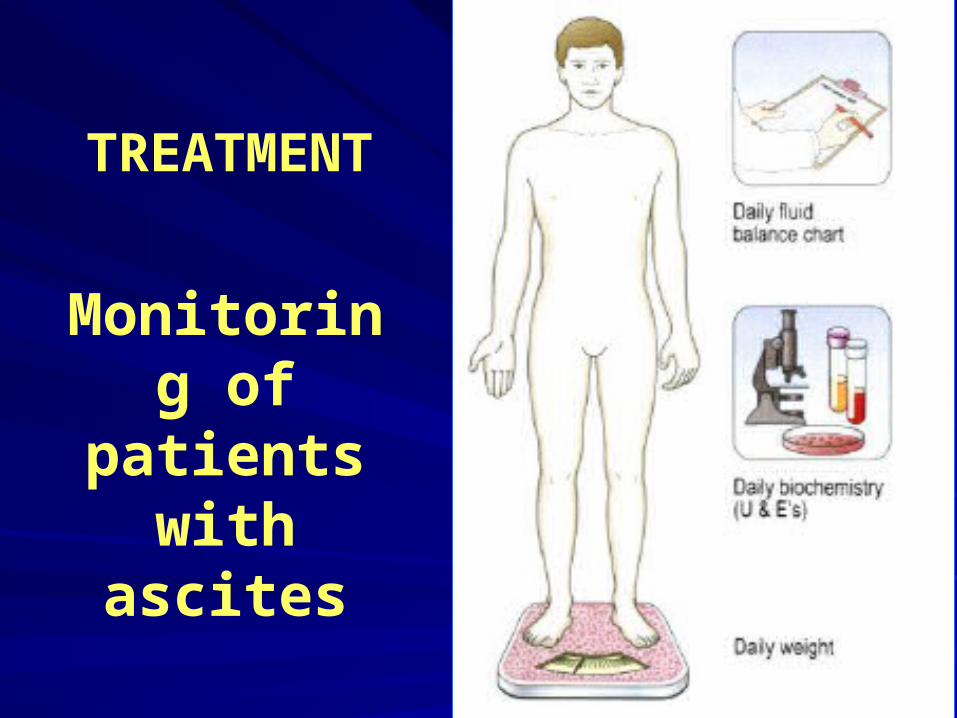
Monitoring of patients
with ascites
TREATMENT
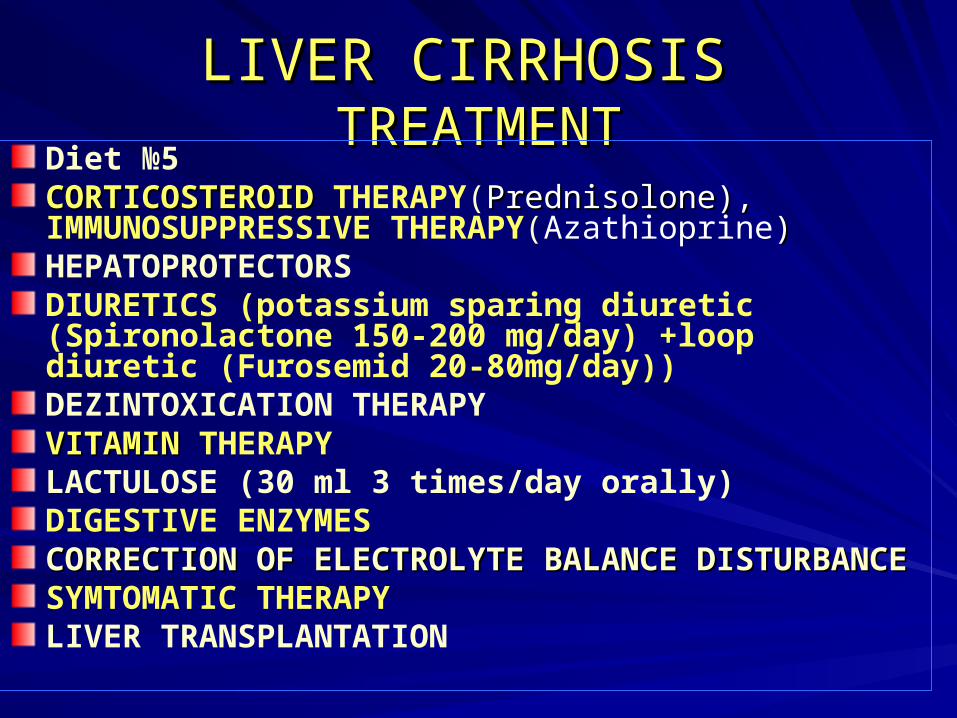
LIVER CIRRHOSISLIVER CIRRHOSIS TREATMENTTREATMENT
Diet №5CCORTICOSTEROIDORTICOSTEROID THERAPY(Prednisolone), Prednisolone), IMMUNOSUPPRESSIVE THERAPY(Azathioprine))HEPATOPROTECTORSDIURETICS (potassium sparing diuretic (Spironolactone 150-200 mg/day) +loop diuretic (Furosemid 20-80mg/day))DEZINTOXICATION THERAPYVITAMIN VITAMIN THERAPYLACTULOSE (30 ml 3 times/day orally)DIGESTIVE ENZYMESCORRECTION OF CORRECTION OF ELECTROLYTE BALANCEELECTROLYTE BALANCE DISTURBANCEDISTURBANCESYMTOMATIC THERAPYLIVER TRANSPLANTATION
Liver transplantation
Liver transplantation should be considered for most patients with end-stage liver disease or acute fulminant hepatic failure, and transplant units should be contacted early regarding referral.
LIVER CIRRHOSISLIVER CIRRHOSISССOMPLICATIONSOMPLICATIONS
HEPATIC ENCEPHALOPATHYHEPATIC ENCEPHALOPATHY
VVARICEAL BLEEDINGARICEAL BLEEDING
ASCITESASCITES
HEPATORENAL SYNDROMEHEPATORENAL SYNDROME
PORTAL VEIN TROMBOSISPORTAL VEIN TROMBOSIS
BACTERIAL PERITONITISBACTERIAL PERITONITIS
HEPATOCARCINOMAHEPATOCARCINOMA
Events precipitating hepatic Events precipitating hepatic encephalopathy inencephalopathy incirrhotic patientscirrhotic patients
Electrolyte imbalanceElectrolyte imbalance
DiureticsDiuretics
VomitingVomiting
DiarrhoeaDiarrhoea
Gastrointestinal bleedingGastrointestinal bleeding
DrugsDrugs
AlcoholAlcohol
InfectionInfection
SpontaneousSpontaneous
bacterial peritonitisbacterial peritonitis
UrinaryUrinary
ChestChest
ConstipationConstipation
Dietary protein Dietary protein overload overload
Drugs that can cause hepaticDrugs that can cause hepaticencephalopathyencephalopathy
BarbituratesBarbiturates
AnalgesicsAnalgesics
Other sedativesOther sedatives
Treatment of hepatic Treatment of hepatic encephalopathyencephalopathy
Identify the precipitating factorsIdentify the precipitating factorsStop diureticsStop diureticsCheck serum Na+, K+, and urea concentrationCheck serum Na+, K+, and urea concentrationEmpty bowels of nitrogen containing contentEmpty bowels of nitrogen containing contentControl bleedingControl bleedingProtein free dietProtein free dietLactuloseLactuloseNeomycin (1 g four times a day by mouth for 1 Neomycin (1 g four times a day by mouth for 1 week)week)Maintain energy, fluid, and electrolyte balanceMaintain energy, fluid, and electrolyte balanceIncrease dietary protein slowly with recoveryIncrease dietary protein slowly with recovery
LIVER CIRRHOSISLIVER CIRRHOSISССOMPLICATIONSOMPLICATIONS
HEPATIC ENCEPHALOPATHY HEPATIC ENCEPHALOPATHY
VVARICEAL BLEEDINGARICEAL BLEEDING
ASCITESASCITES
HEPATORENAL SYNDROMEHEPATORENAL SYNDROME
PORTAL VEIN TROMBOSISPORTAL VEIN TROMBOSIS
BACTERIAL PERITONITISBACTERIAL PERITONITIS
HEPATOCARCINOMAHEPATOCARCINOMA
Characteristic findings associated with Characteristic findings associated with hepatorenalhepatorenal syndromesyndrome
Ascites (but not necessarily jaundice) is usually Ascites (but not necessarily jaundice) is usually presentpresent
Hyponatraemia is usualHyponatraemia is usual
Hepatic encephalopathy is commonly presentHepatic encephalopathy is commonly present
Blood pressure is reduced compared with Blood pressure is reduced compared with previous pressuresprevious pressures recorded in patientrecorded in patient
Pronounced oliguriaPronounced oliguria
Low renal sodium concentrationLow renal sodium concentration
Urinary protein and casts are minimal or absentUrinary protein and casts are minimal or absent
Summary pointsSummary points
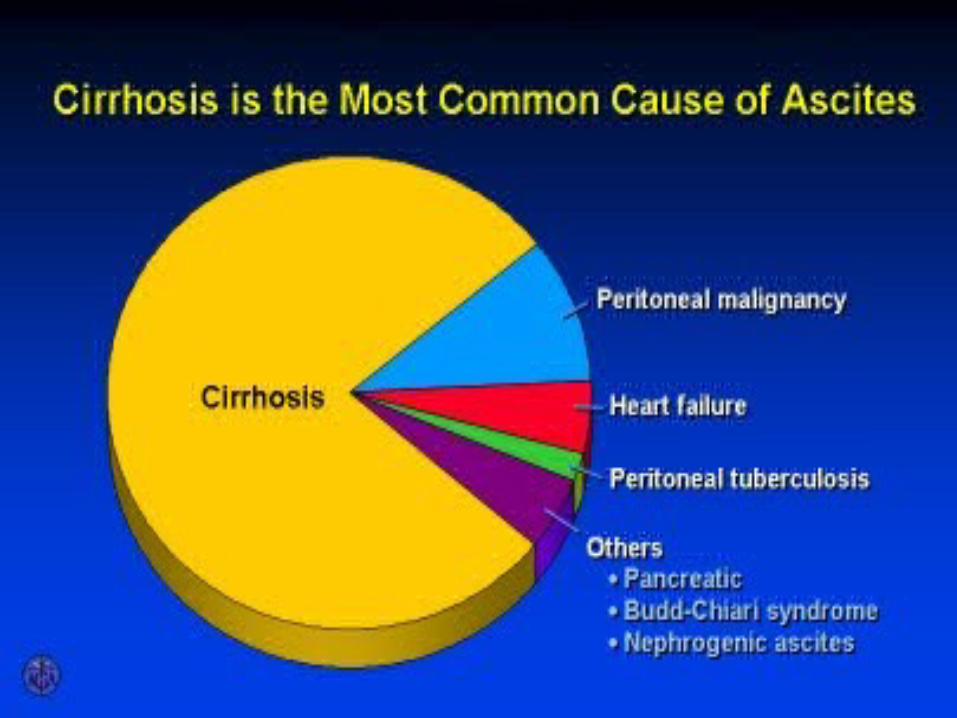
Cirrhosis is the commonest cause of ascites Cirrhosis is the commonest cause of ascites (90%)(90%)Ninety per cent of cases can be managed by Ninety per cent of cases can be managed by sodium restriction andsodium restriction and diureticsdiureticsHepatic encephalopathy is most commonly Hepatic encephalopathy is most commonly precipitated by drugsprecipitated by drugs or gastrointestinal or gastrointestinal haemorrhagehaemorrhageNon steroidal anti inflammatory drugs should be Non steroidal anti inflammatory drugs should be avoided inavoided in cirrhotic patients as they can cause cirrhotic patients as they can cause renal failurerenal failure
Summary pointsSummary pointsPORTAL HYPERTENSION
Normal portal vein pressure is 7 mmHg and pressure is usually above 12 mmHg when oesophageal varices develop.The majority of the oxygen supply of the liver comes from the portal vein, owing to its high flow compared to that in the hepatic artery.Portal hypertension has prehepatic, intrahepatic and post-hepatic causes.Patients with stable portal hypertension should be given beta-blockers.Treatment of ascites requires both dietary salt restriction and diuretics.Fluid restriction is only necessary if hyponatraemia develops.