
Cholesterolbehandeling in 2016 · FH is een autosomaal dominante genetische aandoening HeFH HoFH...
82
Dienst Endocrinologie, UZ Leuven Cholesterolbehandeling in 2016 Ann Mertens, MD, PhD
Transcript of Cholesterolbehandeling in 2016 · FH is een autosomaal dominante genetische aandoening HeFH HoFH...

Dienst Endocrinologie, UZ Leuven
Cholesterolbehandeling in 2016
Ann Mertens, MD, PhD
Programma
1. Belang van cholesterolbehandeling2. Bepalen van het risico bij uw patiënt3. Wat meten ? Tot chol – TG – HDL – LDL – nonHDL – lp(a) –
apoB/A1 – nuchter/niet-nuchter ? 4. Welke targets nastreven ?5. Familiale Hypercholesterolemie6. Welke behandeling ?
• Statines• Ezetimibe• PCSK9-inhibitoren• Fibraten
7. Speciale aandachtspunten• Statines en diabetes• Statine geassocieerde spierpijn (SAMS)
8. Besluit

Programma
1. Belang van cholesterolbehandeling2. Bepalen van het risico bij uw patiënt3. Wat meten ? Tot chol – TG – HDL – LDL – nonHDL – lp(a) –
apoB/A1 – nuchter/niet-nuchter ? 4. Welke targets nastreven ?5. Familiale Hypercholesterolemie6. Welke behandeling ?
• Statines• Ezetimibe• PCSK9-inhibitoren• Fibraten
7. Speciale aandachtspunten• Statines en diabetes• Statine geassocieerde spierpijn (SAMS)
8. Besluit

Adapted from Rosensen RS. Exp Opin Emerg Drugs 2004;9(2):269-279
LaRosa JC et al. N Engl J Med 2005;352:1425-1435
Statines en LDL -Chol Hypothese

Belang van LDL -Cholesterol
Elke verlaging van de LDL-C waarde met 1 mmol/L (40 mg/dL)vermindert het jaarlijkse risico op CV events met o ngeveer 20-24%, onafhankelijk van het werkingsmechanisme 1,2,3,4
1. Cholesterol Treatment Trialists’ (CTT) Collaborators.Lancet. 2010;376:1670-81. 2. Perk J, et al. Eur Heart J. 2012;33(13):1635-701. 3. Cannon CP, et al. N Engl J Med 2015;372:2387–97. 4. CTT Collaboration. Lancet 2005;366:1267–78 LDL-C reduction (mmol/L)
Rel
ativ
e R
isk
Red
uctio
n
SA
BE
.ALI
.16.
09.0
328
0
Lower LDL-C (mg/dL)
Pro
port
iona
l red
uctio
nin
CH
D r
isk
(log
scal
e)
30%
20%
10%
1.0 2.0 3.0 4.0 5.0 6.0 7.0 8.0 9.0 10.0 11.0 12.0 13.0 14.0 15.0 16.0 17.0 18.0 19.0 20.0 21.0
PCSK9 46Lrs11591147
GISSI-PA to Z
SEARCH
ALLHAT-LLT
LDLRrs6511720
NPC1L1 LDL-C scoreHMGCR LDL-C score
Genetically lower LDL-C
Pharmacologically lower LDL-C
IMPROVE-IT
Combined NPC1L1 & HMGCR LDL-C score
HMGCR LDL-C scoreNPC1L1 LDL-C score
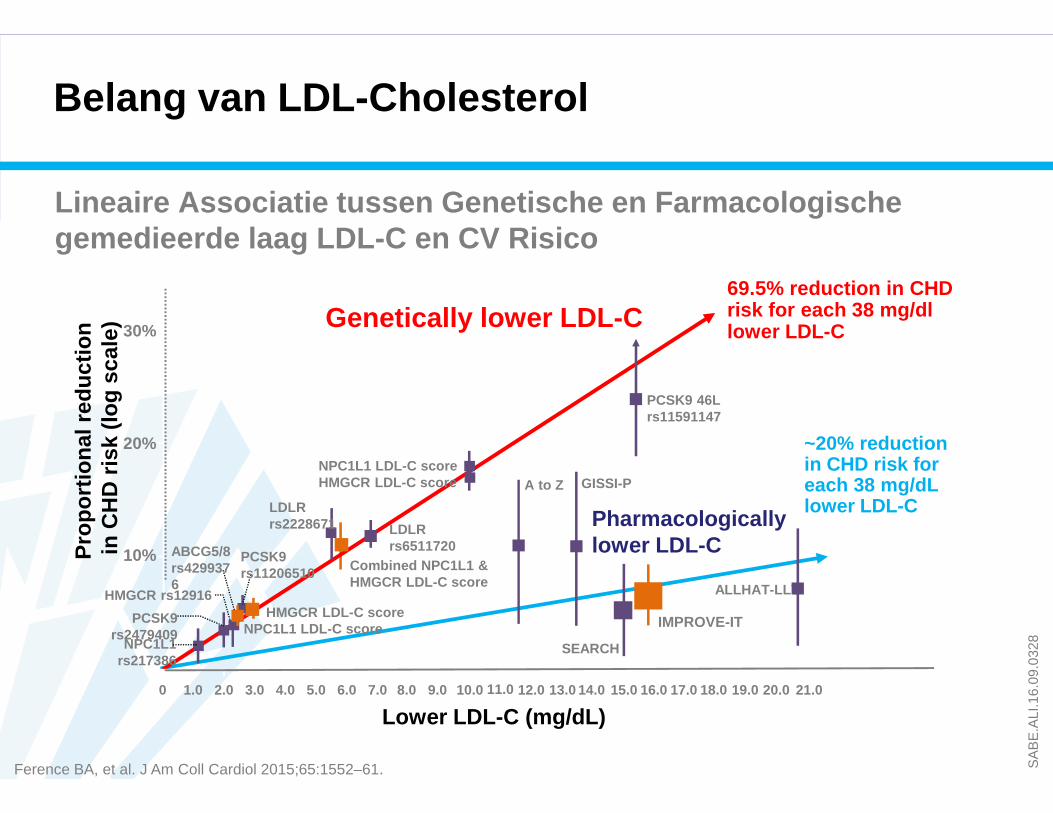
~20% reduction in CHD risk for each 38 mg/dLlower LDL-C
69.5% reduction in CHD risk for each 38 mg/dllower LDL-C
LDLRrs2228671
NPC1L1 rs217386
PCSK9 rs2479409
ABCG5/8rs4299376
HMGCR rs12916
PCSK9rs11206510
Ference BA, et al. J Am Coll Cardiol 2015;65:1552–61.
Lineaire Associatie tussen Genetische en Farmacolog ische gemedieerde laag LDL-C en CV Risico
Belang van LDL -Cholesterol
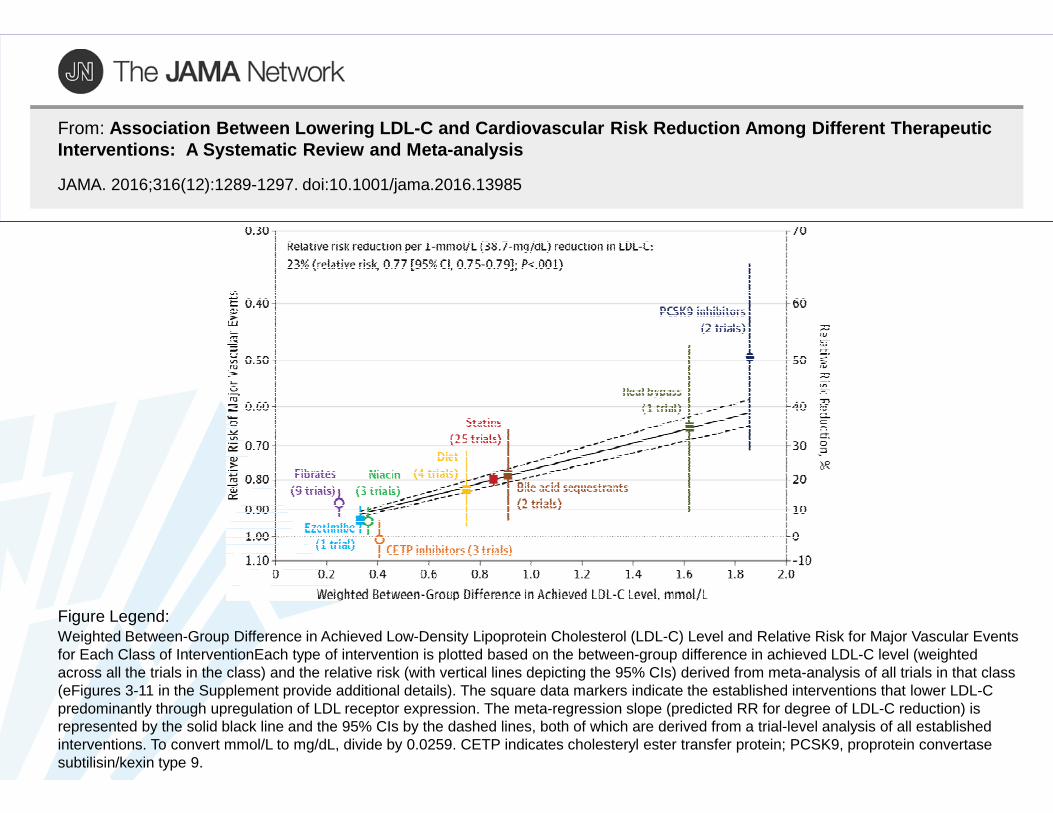
From: Association Between Lowering LDL-C and Cardiovascul ar Risk Reduction Among Different Therapeutic Interventions: A Systematic Review and Meta-analysis
JAMA. 2016;316(12):1289-1297. doi:10.1001/jama.2016.13985
Weighted Between-Group Difference in Achieved Low-Density Lipoprotein Cholesterol (LDL-C) Level and Relative Risk for Major Vascular Events for Each Class of InterventionEach type of intervention is plotted based on the between-group difference in achieved LDL-C level (weighted across all the trials in the class) and the relative risk (with vertical lines depicting the 95% CIs) derived from meta-analysis of all trials in that class (eFigures 3-11 in the Supplement provide additional details). The square data markers indicate the established interventions that lower LDL-C predominantly through upregulation of LDL receptor expression. The meta-regression slope (predicted RR for degree of LDL-C reduction) is represented by the solid black line and the 95% CIs by the dashed lines, both of which are derived from a trial-level analysis of all established interventions. To convert mmol/L to mg/dL, divide by 0.0259. CETP indicates cholesteryl ester transfer protein; PCSK9, proprotein convertase subtilisin/kexin type 9.
Figure Legend:

Programma
1. Belang van cholesterolbehandeling2. Bepalen van het risico bij uw patiënt3. Wat meten ? Tot chol – TG – HDL – LDL – nonHDL – lp(a) –
apoB/A1 – nuchter/niet-nuchter ? 4. Welke targets nastreven ?5. Familiale Hypercholesterolemie6. Welke behandeling ?
• Statines• Ezetimibe• PCSK9-inhibitoren• Fibraten
7. Speciale aandachtspunten• Statines en diabetes• Statine geassocieerde spierpijn (SAMS)
8. Besluit
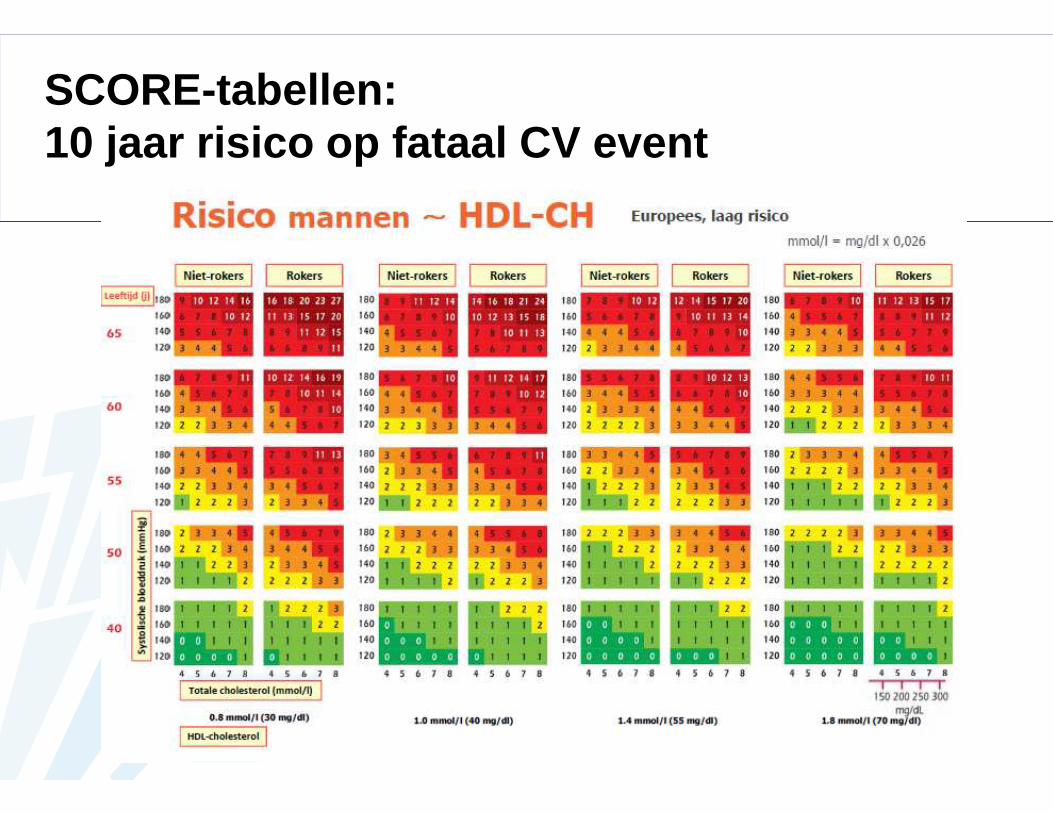
SCORE-tabellen : 10 jaar risico op fataal CV event




Programma
1. Belang van cholesterolbehandeling2. Bepalen van het risico bij uw patiënt3. Wat meten ? Tot chol – TG – HDL – LDL – nonHDL – lp(a) –
apoB/A1 – nuchter/niet-nuchter ? 4. Welke targets nastreven ?5. Familiale Hypercholesterolemie6. Welke behandeling ?
• Statines• Ezetimibe• PCSK9-inhibitoren• Fibraten
7. Speciale aandachtspunten• Statines en diabetes• Statine geassocieerde spierpijn (SAMS)
8. Besluit


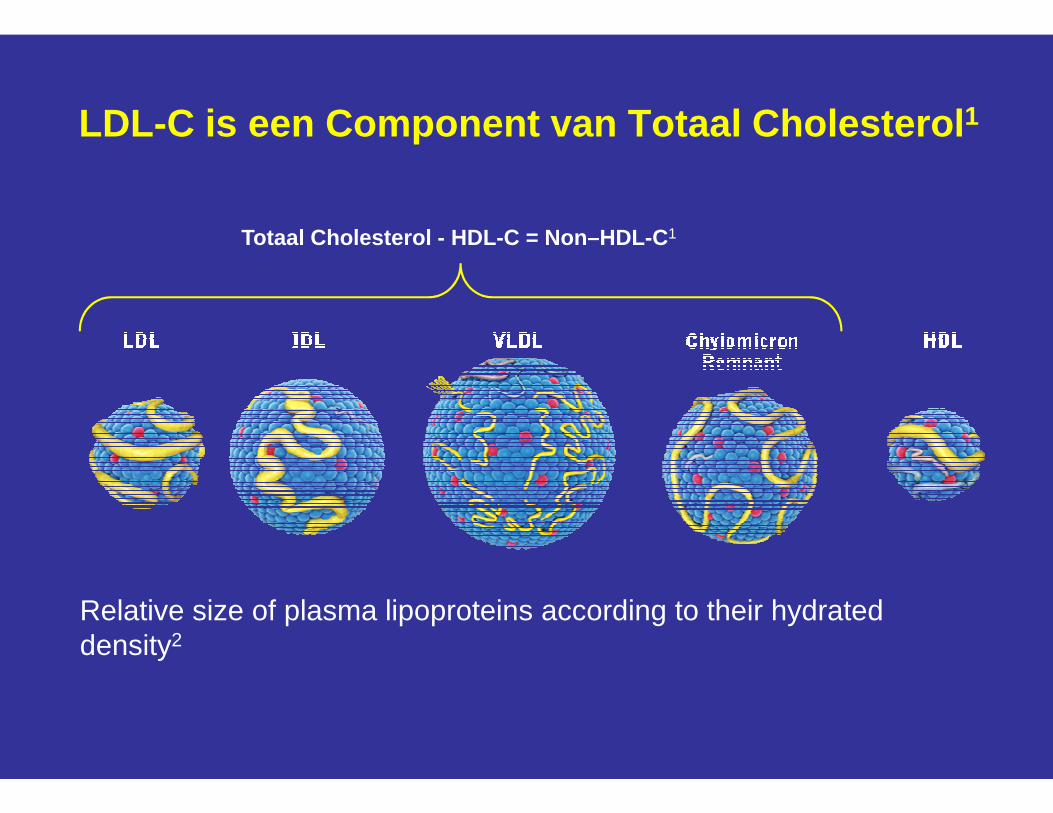
Totaal Cholesterol - HDL-C = Non–HDL-C 1
LDL-C is een Component van Totaal Cholesterol 1
Relative size of plasma lipoproteins according to their hydrated density2

Nuchter ? Niet-nuchter ?
Traditioneel: nuchtere bloedname, na overnacht vasten� Triglyceriden variëren na de maaltijd
Maar: grootste deel van de dag: niet-nuchtere toestand
Onderzoek bij > 300.000 personen: Postprandiale effectenbeïnvloeden de cholesteroltesten minimaal:
- Weinig effect op HDL- Slechts beperkt effect op tot chol – LDL-chol en nonHDL chol (+ 8 mg/dL)- Matige toename van triglyceriden (+ 25 mg/dL)
� deze effecten zijn klinisch niet significant� bevestigd in meta-analyse met > 100.000 patiënten: CV
risicoassociaties zijn vergelijkbaar of zelfs sterker bij gebruik van NN bloedname
Nordestgaard et al. Eur Heart J 2016;37:1944-58(ESC pocket guidelines p 22)
Nuchter ? Niet-nuchter ?
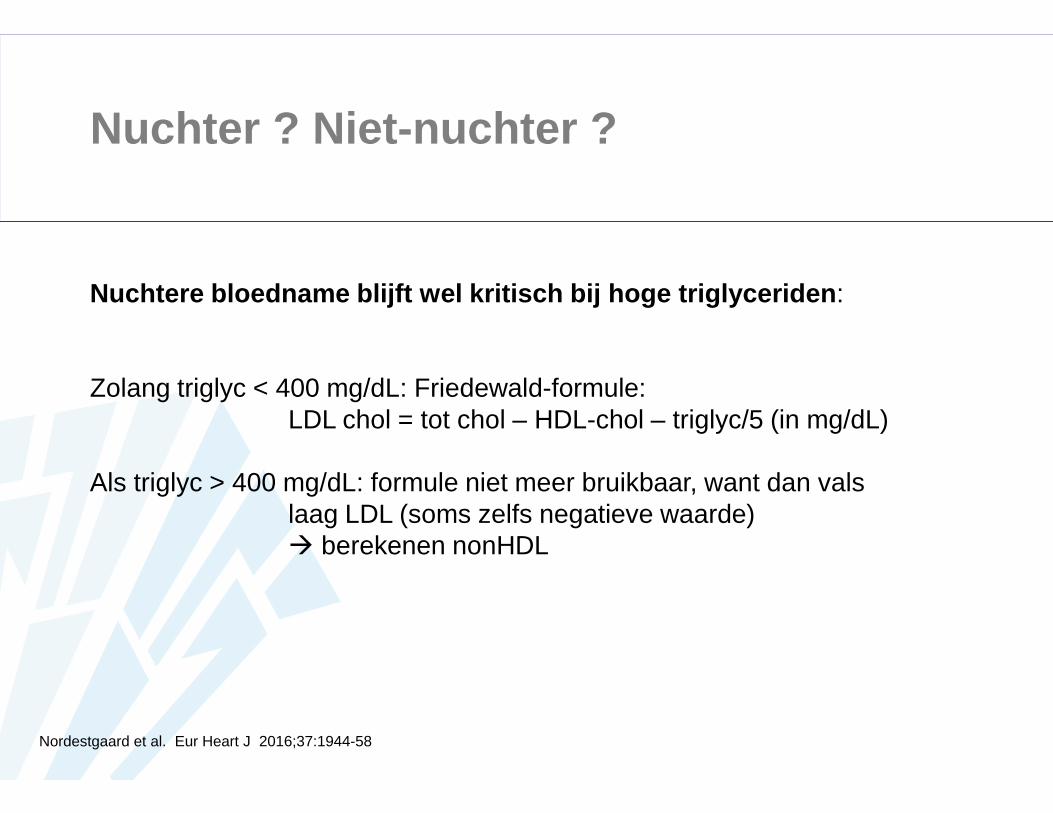
Nuchtere bloedname blijft wel kritisch bij hoge triglyceri den :
Zolang triglyc < 400 mg/dL: Friedewald-formule:LDL chol = tot chol – HDL-chol – triglyc/5 (in mg/dL)
Als triglyc > 400 mg/dL: formule niet meer bruikbaar, want dan vals laag LDL (soms zelfs negatieve waarde)� berekenen nonHDL
Nordestgaard et al. Eur Heart J 2016;37:1944-58
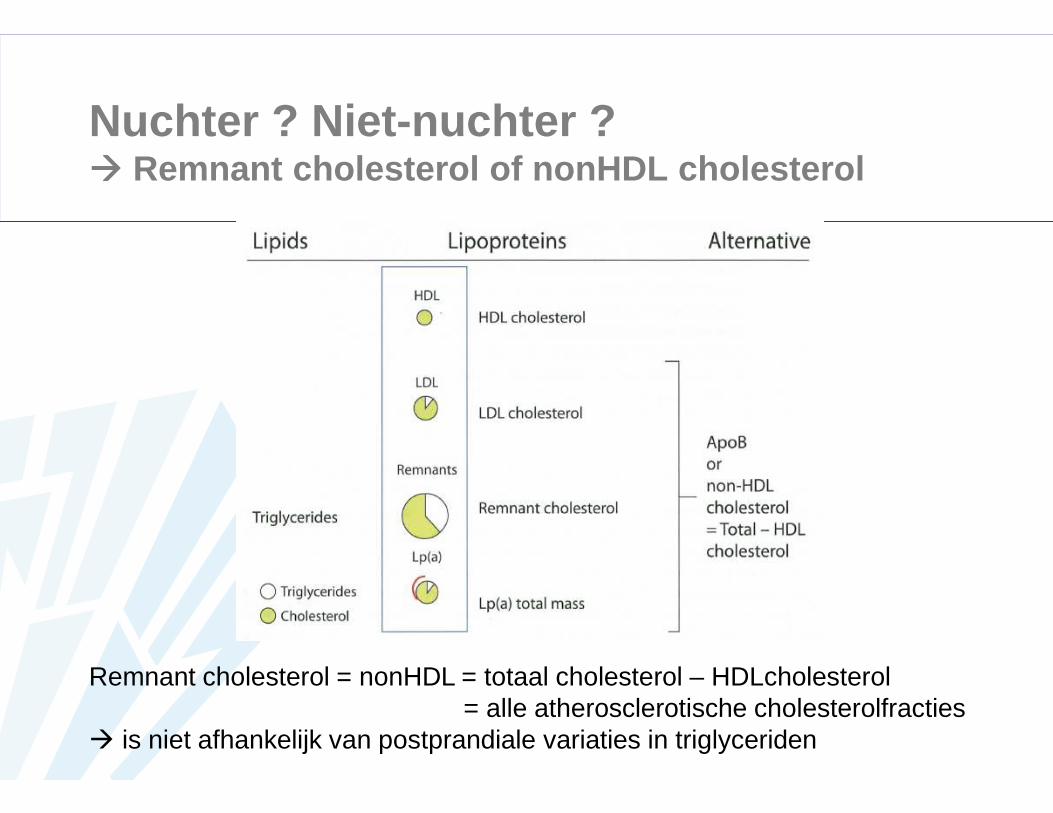
Nuchter ? Niet-nuchter ?���� Remnant cholesterol of nonHDL cholesterol
Remnant cholesterol = nonHDL = totaal cholesterol – HDLcholesterol= alle atherosclerotische cholesterolfracties
� is niet afhankelijk van postprandiale variaties in triglyceriden

Programma
1. Belang van cholesterolbehandeling2. Bepalen van het risico bij uw patiënt3. Wat meten ? Tot chol – TG – HDL – LDL – nonHDL – lp(a) –
apoB/A1 – nuchter/niet-nuchter ? 4. Welke targets nastreven ?5. Familiale Hypercholesterolemie6. Welke behandeling ?
• Statines• Ezetimibe• PCSK9-inhibitoren• Fibraten
7. Speciale aandachtspunten• Statines en diabetes• Statine geassocieerde spierpijn (SAMS)
8. Besluit

!!!

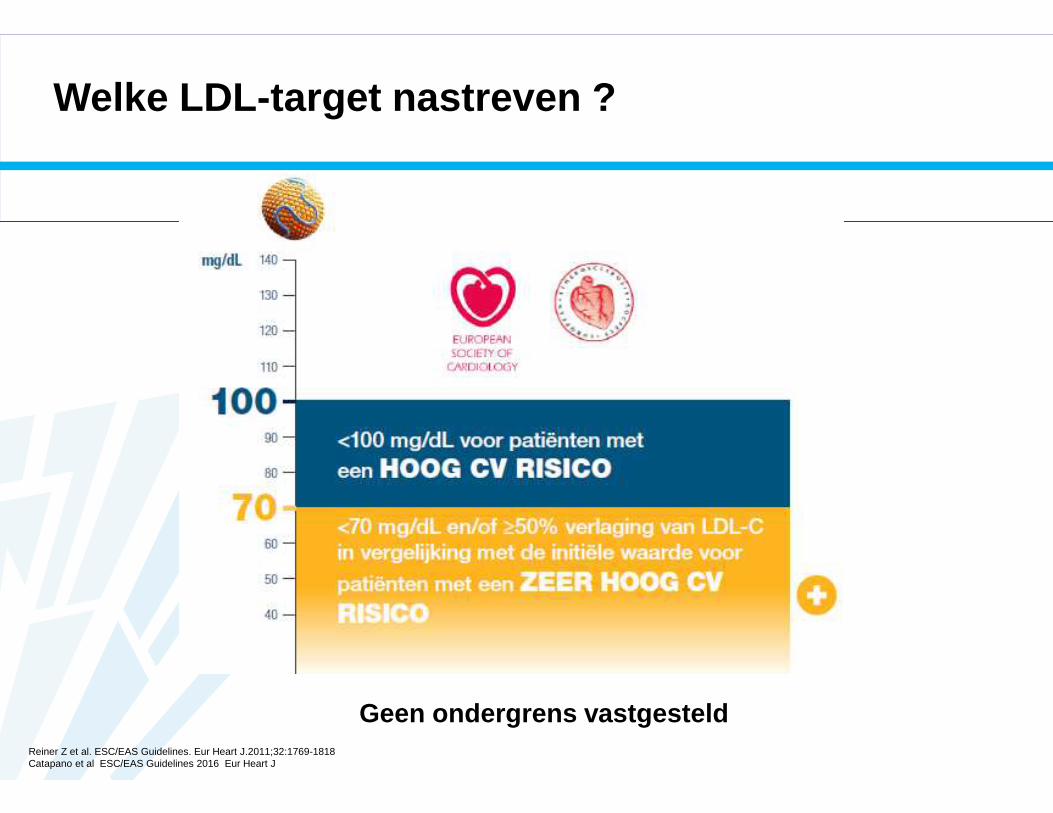
Welke LDL-target nastreven ?
Reiner Z et al. ESC/EAS Guidelines. Eur Heart J.2011;32:1769-1818Catapano et al ESC/EAS Guidelines 2016 Eur Heart J
Geen ondergrens vastgesteld
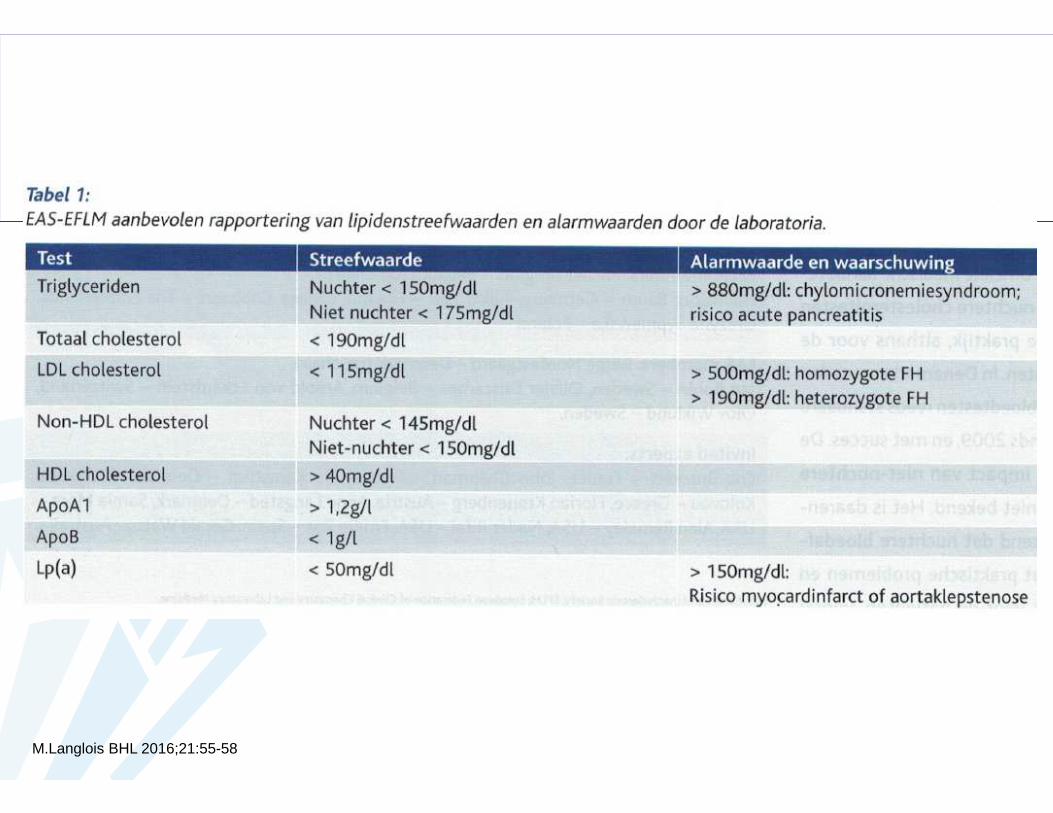
M.Langlois BHL 2016;21:55-58

Programma
1. Belang van cholesterolbehandeling2. Bepalen van het risico bij uw patiënt3. Wat meten ? Tot chol – TG – HDL – LDL – nonHDL – lp(a) –
apoB/A1 – nuchter/niet-nuchter ? 4. Welke targets nastreven ?5. Familiale Hypercholesterolemie6. Welke behandeling ?
• Statines• Ezetimibe• PCSK9-inhibitoren• Fibraten
7. Speciale aandachtspunten• Statines en diabetes• Statine geassocieerde spierpijn (SAMS)
8. Besluit

0,0
0,5
1,0
1,5
2,0
2,5
Fre
quen
cy p
er 1
000
birt
hs
• Prevalentie van HeFH is ~1:5001-3
• Prevalentie van HoFH is ~1:1,000,0002,3
Figure adapted from Genetic Alliance UK. Available at http://www.geneticalliance.org.uk/education3.htm.
1. Citkowitz E. Familial Hypercholesterolemia. http://emedicine.medscape.com/article/121298-overview#a0199.2. Vella A, et al. Mayo Clin Proc. 2001;76(10):1039-1046.3. Austin MA, et al. Am J Epidemiol. 2004;160(5):407-420.
Dominant otosclerosis
Adult PCKD
Sickle cell disease
Multiple exostoses
Huntington's disease
Fragile X syndrome
Neuro-fibromatosis
Cystic fibrosis
Duchenne muscular dystrophy
FH
2.0 per 1000
1.00.8
0.5 0.5 0.5 0.5 0.4 0.4 0.3
PCKD, polycystic kidney disease.
Familiale Hypercholesterolemie

HeFH versus HoFH���� FH is een autosomaal dominante genetische aandoenin g
HeFH HoFH
• Veroorzaakt door 2 defecte genen• LDL-C waarden: 500 – 800 mg/dl• Verspreid atherosclerotisch CVD• Eerste CVD vaak tijdens kinderjaren• CV sterfte < 20 jaar
• Zeer zelden
– Geschatte prevalentie 1:1.000.000 (oude schatting) tot 1:300.000
• Veroorzaakt door 1 defect gen• LDL-C waarden: 190– 400 mg/dl• Risico op vroegtijdig CVD 20x
verhoogd• Vroegtijdig atherosclerotisch CVD
– 30 – 40 jaar bij mannen– 40 – 50 jaar bij vrouwen
• Geschatte prevalentie 1:500 (oude schatting) tot 1:200
• België: > 25.000 patiënten• Europa: 4,5 M patiënten
www.belchol.be
één copy (allel) van het gen is defect beide copies (allelen) van het gen zijn defect
SA
BE
.ALI
.16.
09.0
328
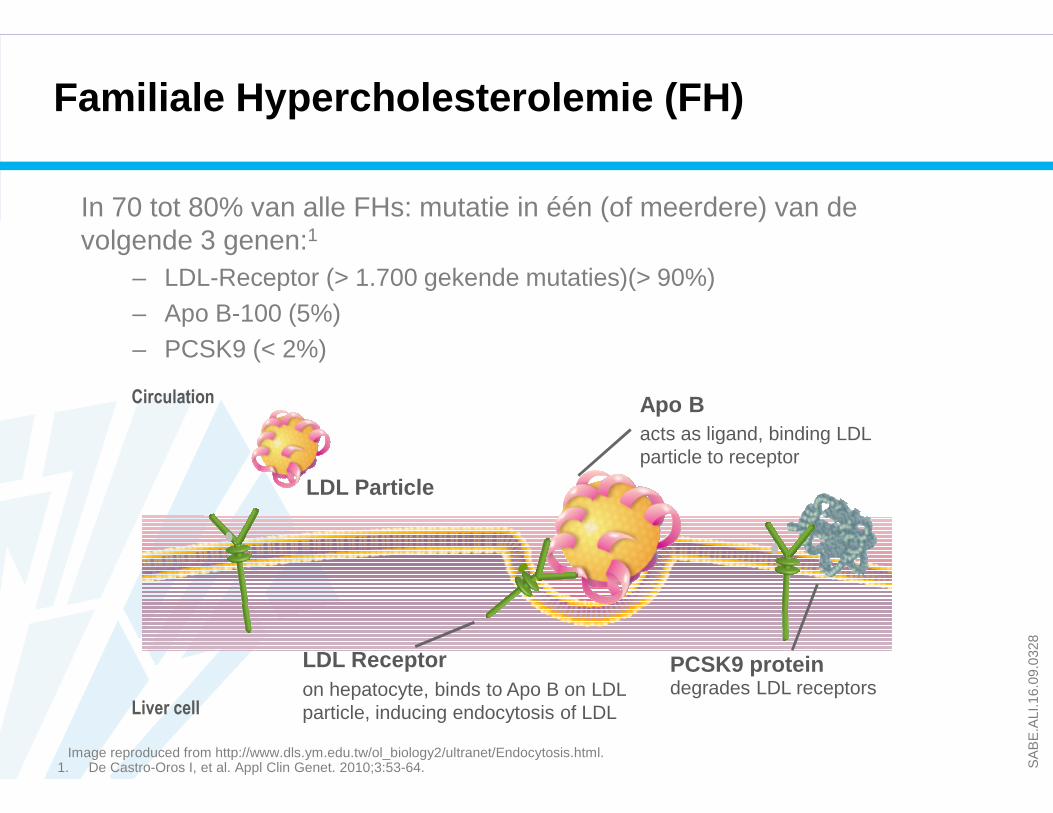
In 70 tot 80% van alle FHs: mutatie in één (of meerdere) van de volgende 3 genen:1
– LDL-Receptor (> 1.700 gekende mutaties)(> 90%)– Apo B-100 (5%)– PCSK9 (< 2%)
acts as ligand, binding LDL particle to receptor
PCSK9 protein
Liver cell
Circulation
LDL Particle
Apo B
LDL Receptoron hepatocyte, binds to Apo B on LDL particle, inducing endocytosis of LDL
degrades LDL receptors
Image reproduced from http://www.dls.ym.edu.tw/ol_biology2/ultranet/Endocytosis.html.1. De Castro-Oros I, et al. Appl Clin Genet. 2010;3:53-64.
Familiale Hypercholesterolemie (FH)

SA
BE
.ALI
.16.
09.0
328
FH: Klinische tekens
A. XanthelasmaB. Corneal arcusa
C. Achilles tendon xanthomasD. Tendon xanthomasb,1-3
E. Tuberous xanthomasc
F. Planar xanthomasc
A Common in older individuals (even non-FH); definitive of FH in younger individuals.
B 30%-50% of the HeFH population have tendon xanthomas.C Seen mostly in HoFH, and not as often in HeFH
1. Ferrières J, et al. Circulation. 1995;92(3):290-295.2. Bertolini S, et al. Arterioscler Thromb Vasc Biol. 2000;20(9):E41-E52.3. Descamps OS, et al. Atherosclerosis. 2001;157(2):514-518.
Figure adapted from Mahley RW, et al. In: Kronenberg HM. Williams Textbook of Endocrinology. 11th ed. Philadelphia: Saunders; 2008.
Afwezigheid van deze klinische kenmerken sluit FH niet uit !
A B
C D
E F

Familiale hypercholesterolemie en CV risico
CHD, coronary heart disease; CV, cardiovascular; FH, familial hypercholesterolemia; HDL-C, high-densitylipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol.Nordestgaard BG, et al. Eur Heart J 2013;34:3478–90.
Cumulatieve LDL-C blootstelling bij individuen met of zo nder FH in functie van hun leeftijd bij begin van statine therap ie
Cum
ulat
eive
LDL-
C (
mg/
dL)
Leeftijd (jaren)
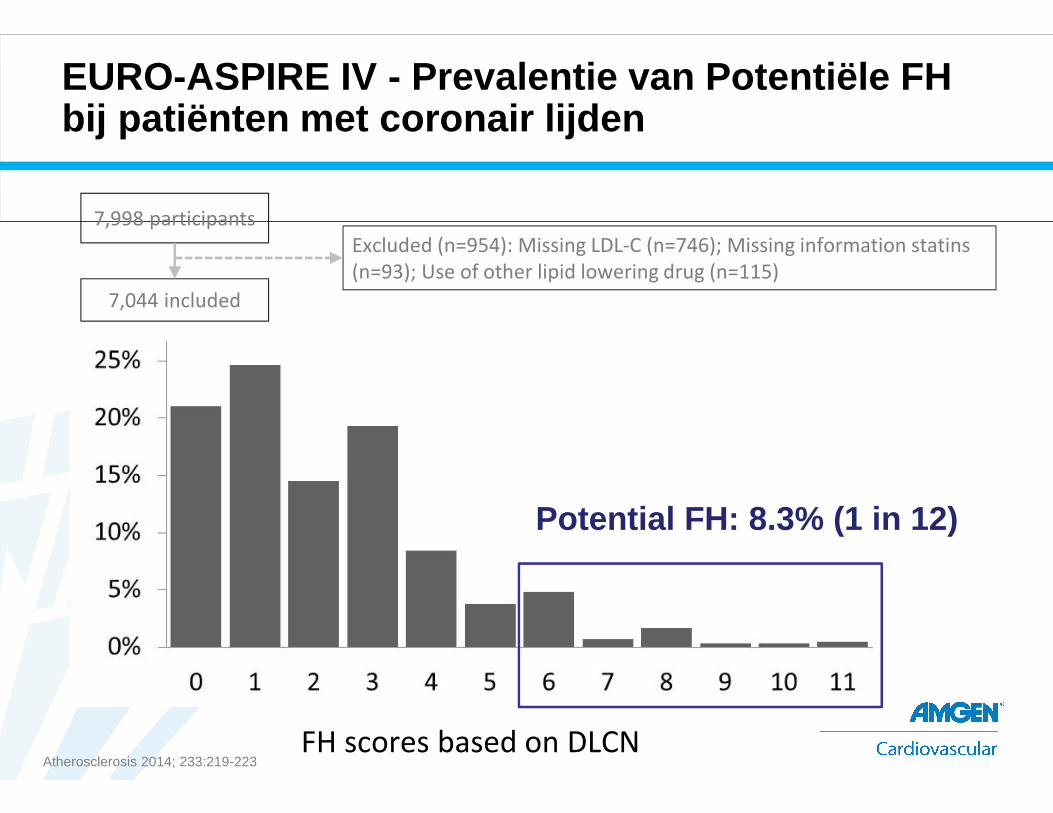
EURO-ASPIRE IV - Prevalentie van Potentiële FH bij patiënten met coronair lijden
7,998 participants
7,044 included
FH scores based on DLCN
Excluded (n=954): Missing LDL-C (n=746); Missing information statins
(n=93); Use of other lipid lowering drug (n=115)
Potential FH: 8.3% (1 in 12)
Atherosclerosis 2014; 233:219-223
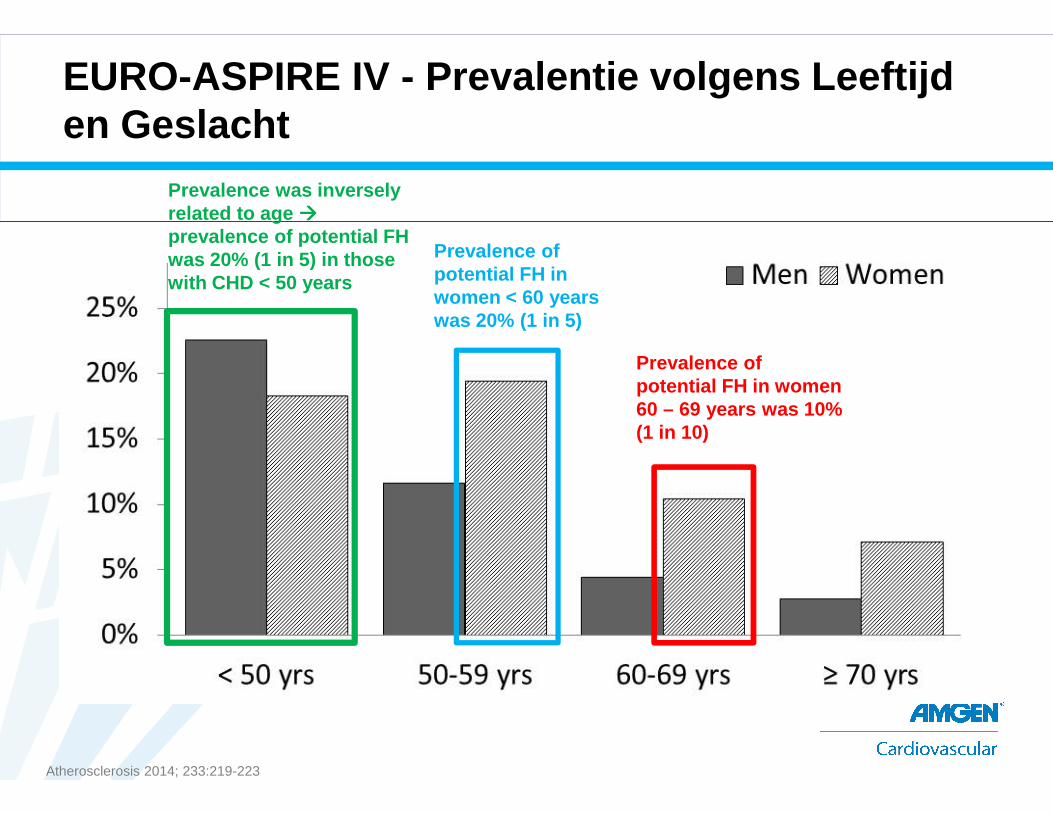
Prevalence was inversely related to age ����prevalence of potential FH was 20% (1 in 5) in those with CHD < 50 years
Prevalence of potential FH in women < 60 years was 20% (1 in 5)
Prevalence of potential FH in women 60 – 69 years was 10% (1 in 10)
EURO-ASPIRE IV - Prevalentie volgens Leeftijden Geslacht
Atherosclerosis 2014; 233:219-223

Geschatte percentage van individuen met diagnose van HeFH in verschillende landen
HeFH, heterozygous familial hypercholesterolemia.Nordestgaard BG, et al. Eur Heart J 2013;34:3478–90.
0 25 50 75 100
NetherlandsNorwayIceland
SwitzerlandUK
SpainBelgiumSlovakia
DenmarkSouth Africa
AustraliaHong Kong
FranceTaiwan
ItalyOman
USACanada
JapanChileBrazil
Mexico
Number of HeFH (estimated based on 1/500)
33,3009900600
15,600123,60092,20022,20011,10011,100
100,00045,00014,100
130,90046,300
121,0005700
621,20068,600
254,80034,300
381,500214,900
71%43%19%13%12%6%4%4%4%3%1%1%1%
<1%<1%<1%<1%<1%<1%<1%<1%<1%
HeFH is ondergediagnosticeerdin vele landen
Wanneer denken aan FH ?
Iedere patiënt met prematuur ACS (< 55 j man; < 60 j vrouw)
en LDL-C > 190 mg/dl zonder statine therapie
of LDL-C > 130 mg/dl met matige/hoge intensiteit statine
moet beschouwd worden als “mogelijk” FH” (Michel Farnier)

HeFH Diagnose
• Genetische diagnose : mutatie testing op LDL-R, ApoB en PCSK9
genen
– UCL St. Luc
– UZ Leuven
– CHU Liège
• Klinische diagnose
– Dutch Lipid Clinic Network (DLCN) score
• Cascade screening
– MEDPED score (verwanten)
SA
BE
.ALI
.16.
09.0
328
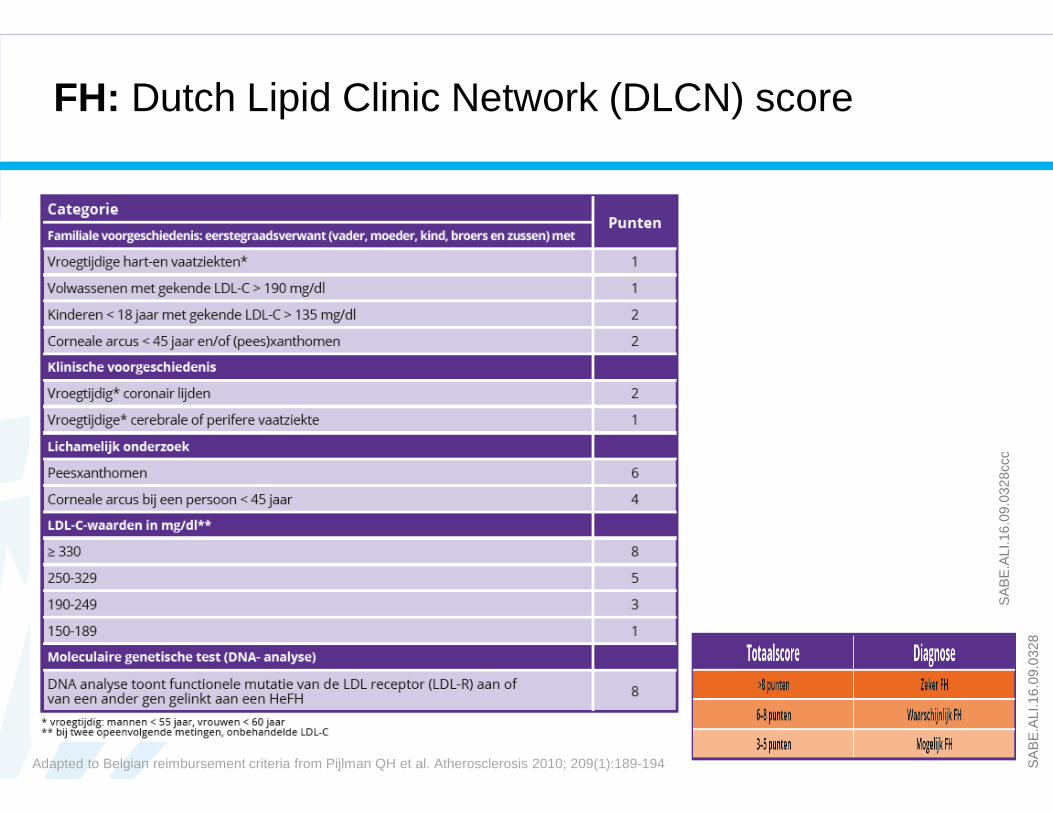
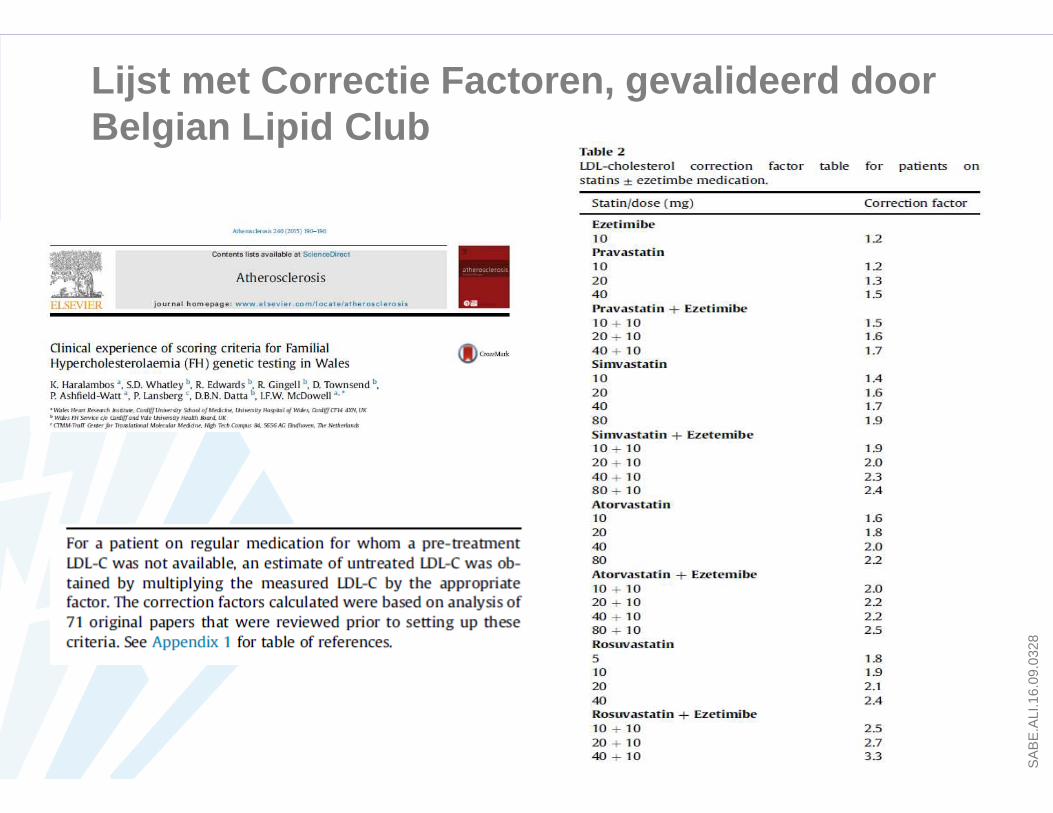
Adapted to Belgian reimbursement criteria from Pijlman QH et al. Atherosclerosis 2010; 209(1):189-194
SA
BE
.ALI
.16.
09.0
328c
cc
FH: Dutch Lipid Clinic Network (DLCN) score
SA
BE
.ALI
.16.
09.0
328
Lijst met Correctie Factoren, gevalideerd door Belgian Lipid Club

Programma
1. Belang van cholesterolbehandeling2. Bepalen van het risico bij uw patiënt3. Wat meten ? Tot chol – TG – HDL – LDL – nonHDL – lp(a) –
apoB/A1 – nuchter/niet-nuchter ? 4. Welke targets nastreven ?5. Familiale Hypercholesterolemie6. Welke behandeling ?
• Statines• Ezetimibe• PCSK9-inhibitoren• Fibraten
7. Speciale aandachtspunten• Statines en diabetes• Statine geassocieerde spierpijn (SAMS)
8. Besluit

Huidige behandelingsmogelijkheden
1. Statines
Standaardbehandeling
GEMIDDELDE LDL-C DALING
2. Ezetimibe
Als bijkomende LDL-daling nodig isof bij statine-intolerantie
15% tot 22%
Laag
Intensiteit:
Reiner Z et al. Eur Heart J. 2011;32:1769-818.Stone N et al. JACC 2014;25(63) :2889–93.
<30%
Matig
30% tot <50%
Hoog
≥ 50%
fluva 40 prava 10-20 simva 10
atorva 10-20 fluva 80 prava 40-80rosu 5-10 simva 20-40
atorva 40-80 rosu 20-40

Huidige onvervulde medische noden
Langslet G et al. Expert Review of Cardiovascular Therapy 2015;13(5) :477-488. Reiner Z, et al. Eur Heart J. 2011;32 :1769-818.
Familiale Hypercholesterolemie
Secundaire Preventie Statine Intolerantie
Een aantal (zeer) hoog risicopatiënten heeft additionele t herapie nodig:

SA
BE
.ALI
.16.
09.0
328
Evolutie van mAbs
Monoclonal antibodies against PCSK9:
• Alirocumab – Praluent® – Sanofi
• Evolocumab – Repatha® – Amgen
• Bococizumab – Pfizer
1st generation100% mouseHighly immunogenic
2nd generation30 % mouseStill immunogenic
3rd generation5- 10% mouseReduced immunogenicity but time consuming to make
4th generation100% humanLeast immunogenicProduced by “transgenic” mice or genetically engineered bacteria
fully human
humanized
-ximab -zumab -umab-omab

Lambert G, et al. J Lipid Res. 2012;53:2515-24
PCSK9: Proproteineconvertase subtilisine/kexine type 9
PCSK9 regelt de expressie van LDL -receptor via targeting van de lysosomale degradatie
PCSK9 = Proprotein Convertase Subtilisin Kexin 9

ODYSSEY Long TERM: Alirocumab behoudt eenConsistente LDL-C Reductie gedurende 78 Weken
1 Robinson JG et al. NEJM 2015; 372:1489-99.
SA
BE
.ALI
.16.
09.0
328
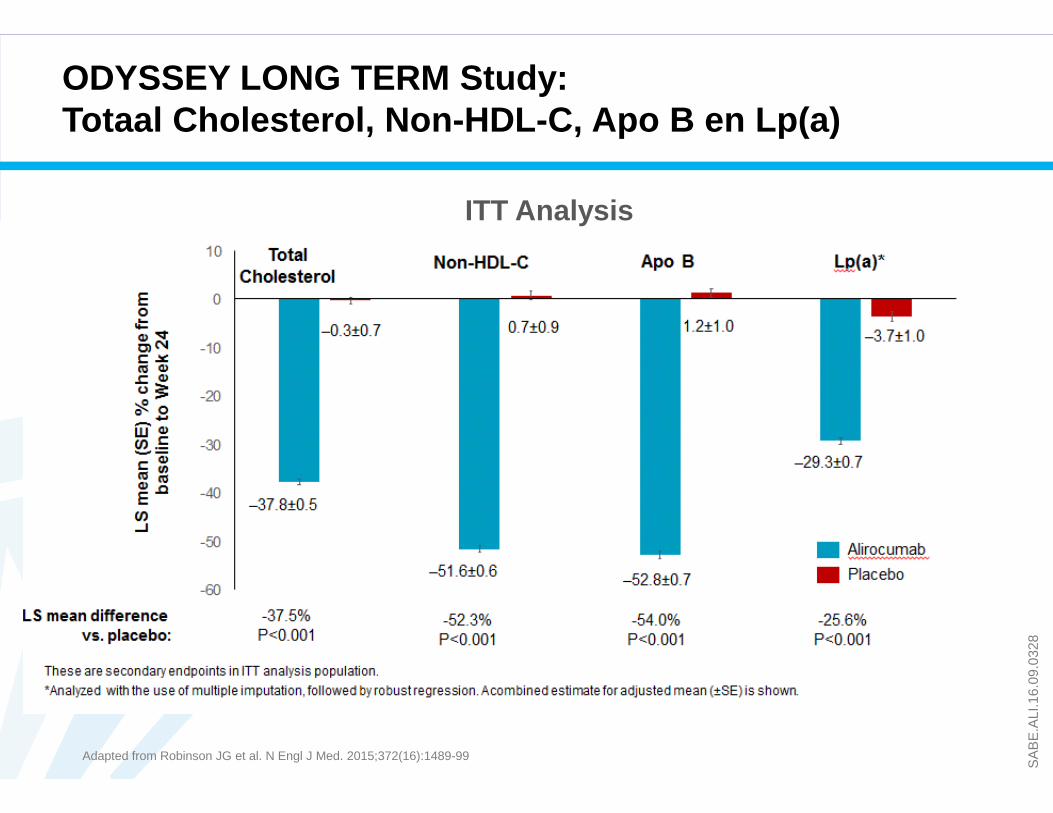
Adapted from Robinson JG et al. N Engl J Med. 2015;372(16):1489-99
ODYSSEY LONG TERM Study: Totaal Cholesterol, Non-HDL-C, Apo B en Lp(a)
ITT Analysis

SA
BE
.ALI
.16.
09.0
328
ODYSSEY LONG TERM: Overzicht van Nevenwerkingen
AE=adverse event; d/c=discontinuation; LDL-C= low-density lipoprotein cholesterol; URTI=upper respiratory tract infection.Adapted from Robinson JG, et al. N Engl J Med. 2015;372(16):1489-1499 (supplementary appendix).
PRALUENT ®
(alirocumab) Injection(N=1550)
PRALUENT 2 Consecutive
LDL-C <25 mg/dL (N=575)
Placebo(N=788)
AE leading to study d/c 7.2% 4.5% 5.8%AE leading to death 0.5% 0.7% 1.3%
AEs Occurring in ≥5% of Any GroupNasopharyngitis 13.5% 11.0% 13.1%URTI 7.4% 6.1% 8.6%Injection site reaction 5.9% 3.8% 4.2%Urinary tract infection 5.8% 6.1% 6.9%Diarrhea 5.8% 4.9% 5.7%Influenza 5.7% 4.5% 5.7%Back pain 5.5% 6.1% 6.7%Myalgia 5.4% 3.1% 2.9%Bronchitis 5.4% 5.4% 5.2%Arthralgia 5.3% 3.8% 6.6%Headache 5.0% 1.9% 5.7%

Robinson JG et al. NEJM 2015; 372:1489-99.
ODYSSEY Long TERM: Post hoc Analyse van Geadjudiceerde Majeure Cardiovasculaire Events

2018
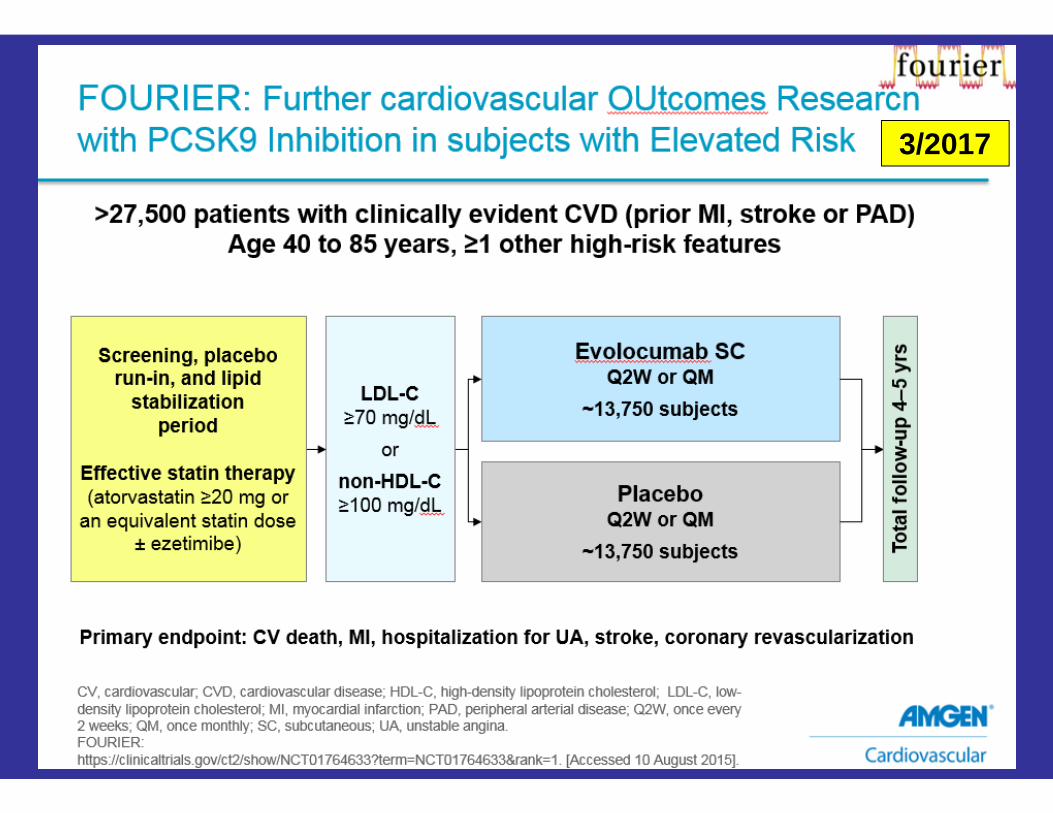
3/2017
- Resultaat van cardiovasculaire outcome
- Vragen ivm veiligheid:- Neurocognitieve aspecten- Incidentie van nieuwe diabetes
???

SA
BE
.ALI
.16.
09.0
328
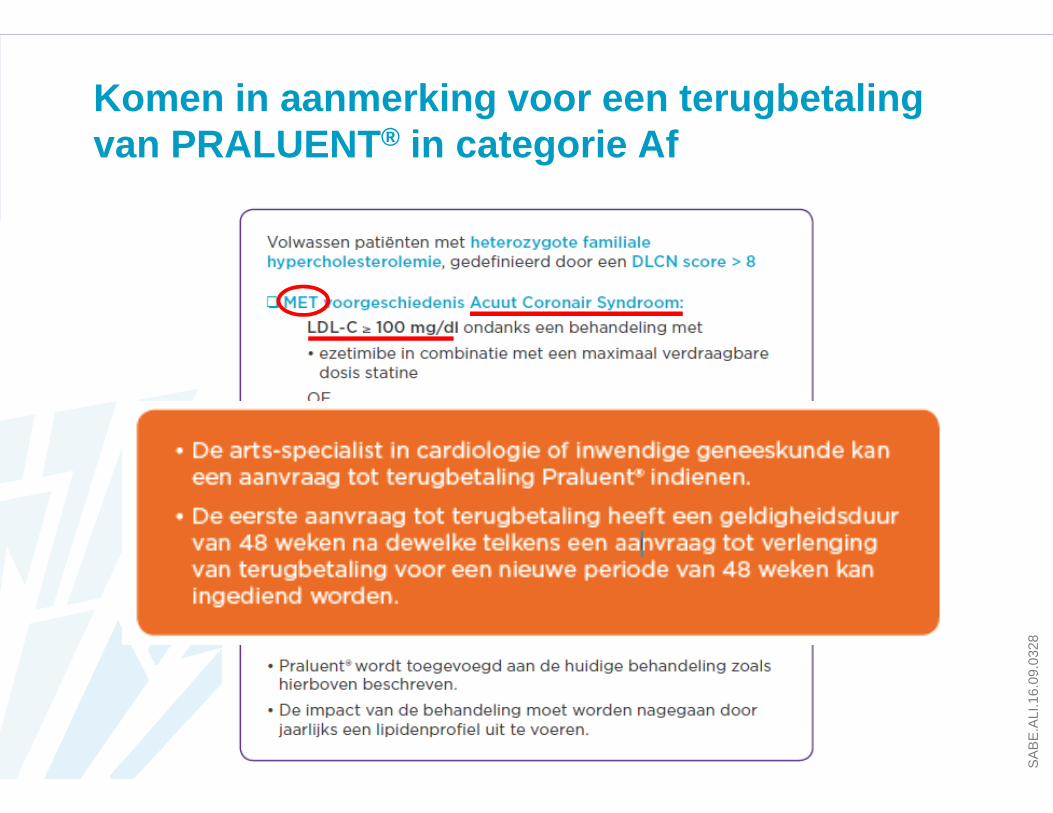
Komen in aanmerking voor een terugbetaling van PRALUENT ® in categorie Af
SA
BE
.ALI
.16.
09.0
328
Komen in aanmerking voor een terugbetaling van PRALUENT ® in categorie Af
SA
BE
.ALI
.16.
09.0
328
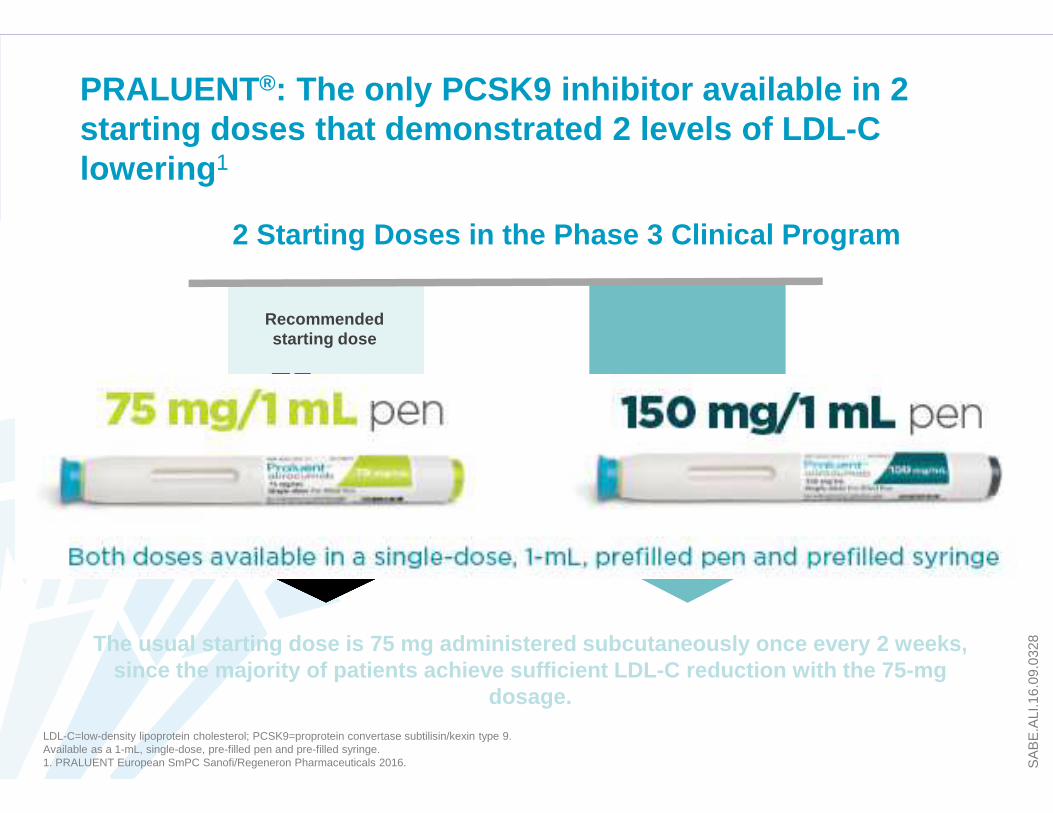
PRALUENT®: The only PCSK9 inhibitor available in 2 starting doses that demonstrated 2 levels of LDL-C lowering 1
LDL-C=low-density lipoprotein cholesterol; PCSK9=proprotein convertase subtilisin/kexin type 9.Available as a 1-mL, single-dose, pre-filled pen and pre-filled syringe.1. PRALUENT European SmPC Sanofi/Regeneron Pharmaceuticals 2016.
Recommendedstarting dose
If needed
OR75 mg
150 mg
150 mg
The usual starting dose is 75 mg administered subcu taneously once every 2 weeks, since the majority of patients achieve sufficient L DL-C reduction with the 75-mg
dosage.
2 Starting Doses in the Phase 3 Clinical Program

Stalenprogramma:Per arts mogelijkheid om 2 patiënten gedurende 1 jaar t e behandelen met Repatha
Amgen: Repatha ®

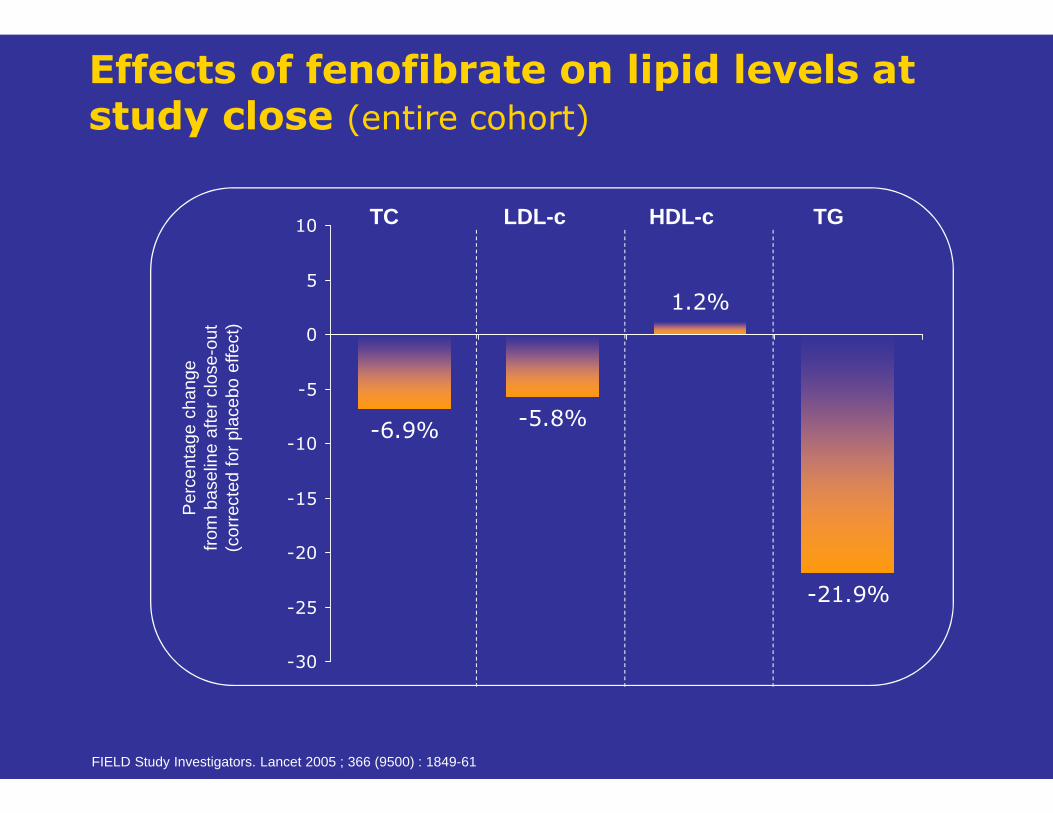
Effects of fenofibrate on lipid levels at study close (entire cohort)
FIELD Study Investigators. Lancet 2005 ; 366 (9500) : 1849-61
-21.9%
1.2%
-5.8%-6.9%
-30
-25
-20
-15
-10
-5
0
5
10 TC LDL-c HDL-c TGP
erce
ntag
e ch
ange
from
bas
elin
e af
ter
clos
e-ou
t(c
orre
cted
for
pla
cebo
effe
ct)

Cum
ulat
ive
risk
(%)
Years from randomization
4,900
4,895
4,835
4,837
4,741
4,745
4,646
4,664
4,547
4,555
2,541
2,553
Placebo
Fenofibrate837
850
10
8
6
4
2
0
0 1 2 3 4 5
Fenofibrate
Placebo
6
Primary endpointCHD events (nonfatal MI, CHD death)
HR = 0.8995% CI = 0.75–1.05p = 0.16
Number of patients still followed-up at the given year
FIELD Study Investigators. Lancet 2005 ; 366 (9500) : 1849-61
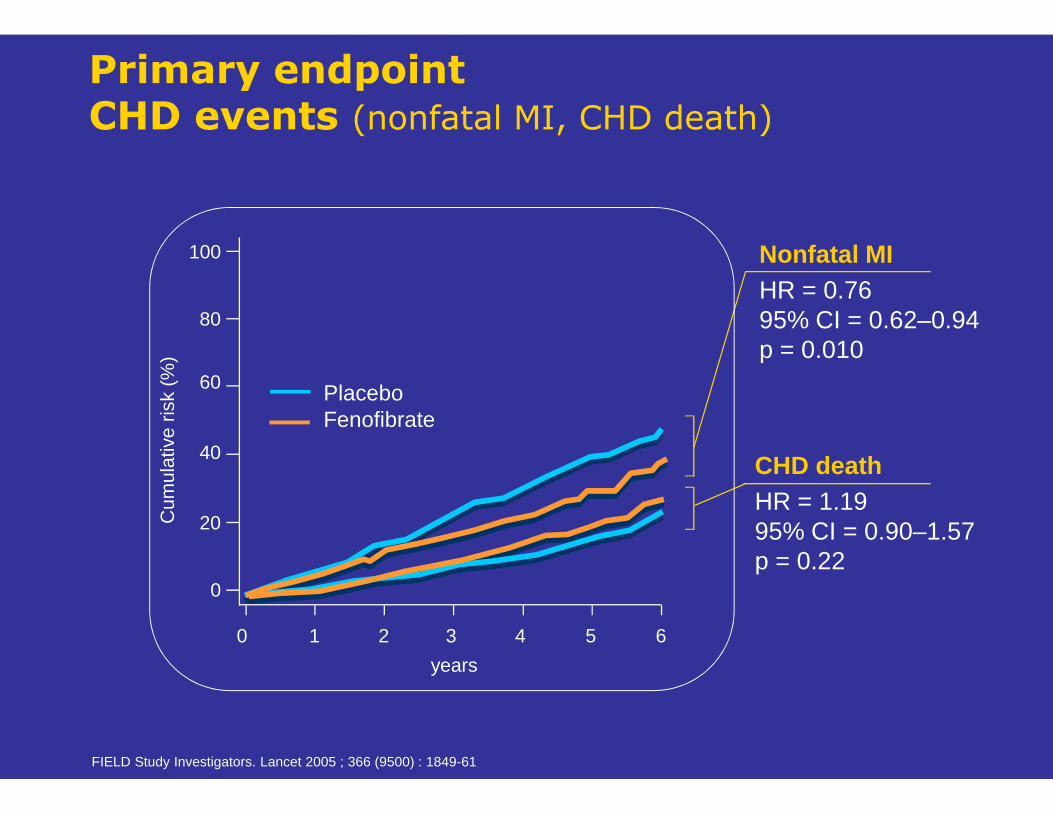
Nonfatal MIHR = 0.7695% CI = 0.62–0.94p = 0.010
CHD deathHR = 1.1995% CI = 0.90–1.57p = 0.22
PlaceboFenofibrate
100
80
60
40
20
0
0 1 2 3 4 5 6
years
Cum
ulat
ive
risk
(%)
Primary endpointCHD events (nonfatal MI, CHD death)
FIELD Study Investigators. Lancet 2005 ; 366 (9500) : 1849-61
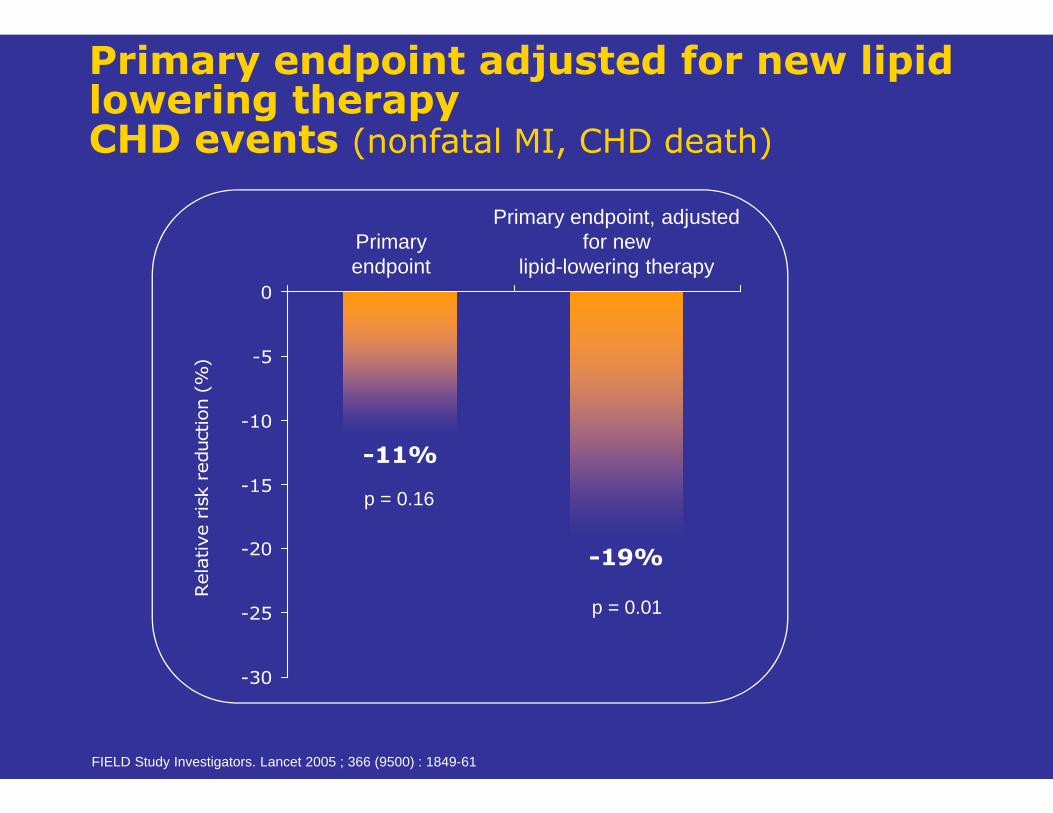
-11%
-19%
-30
-25
-20
-15
-10
-5
0
Rela
tive r
isk r
eduction (
%)
p = 0.16
Primaryendpoint
Primary endpoint, adjusted for new
lipid-lowering therapy
p = 0.01
Primary endpoint adjusted for new lipid lowering therapyCHD events (nonfatal MI, CHD death)
FIELD Study Investigators. Lancet 2005 ; 366 (9500) : 1849-61



Programma
1. Belang van cholesterolbehandeling2. Bepalen van het risico bij uw patiënt3. Wat meten ? Tot chol – TG – HDL – LDL – nonHDL – lp(a) –
apoB/A1 – nuchter/niet-nuchter ? 4. Welke targets nastreven ?5. Familiale Hypercholesterolemie6. Welke behandeling ?
• Statines• Ezetimibe• PCSK9-inhibitoren• Fibraten
7. Speciale aandachtspunten• Statines en diabetes• Statine geassocieerde spierpijn (SAMS)
8. Besluit

Statines en Nevenwerkingen
Nevenwerkingen van statines:- Diabetes mellitus- Minder CVAs, maar meer hemorrhagische CVAs- Geen effect op cognitieve functies- Tendinopathie en interstitieel longlijden, slechts klein aantal casussen
� Frequentie is zeer laag en weegt niet op tegen de vasculaire voordelen
JAMA 2016;316(19):1969-70
PREISS META-ANALYSIS 1 SATTAR META-ANALYSIS 2
N = 91,140
1,449(8.8%) 1,300
(8.0%)
2,226(4.9%) 2,052
(4.5%)
Meta-analysis of five randomized controlled endpoint trials comparing intensive-dose statin with moderate-dose statin therapy and including > 1,000 participants
who were followed up for > 1 year
Meta-analysis of 13 randomized controlled endpoint trials of statins with > 1,000 patients
with identical follow-up in both groups and duration > 1 year
IntensiveDose
N = 16,408
ModerateDose
N = 16,344
StatinN = 45,521
PlaceboN = 45,619
LDL-C concentration was not associated with the risk of diabetes
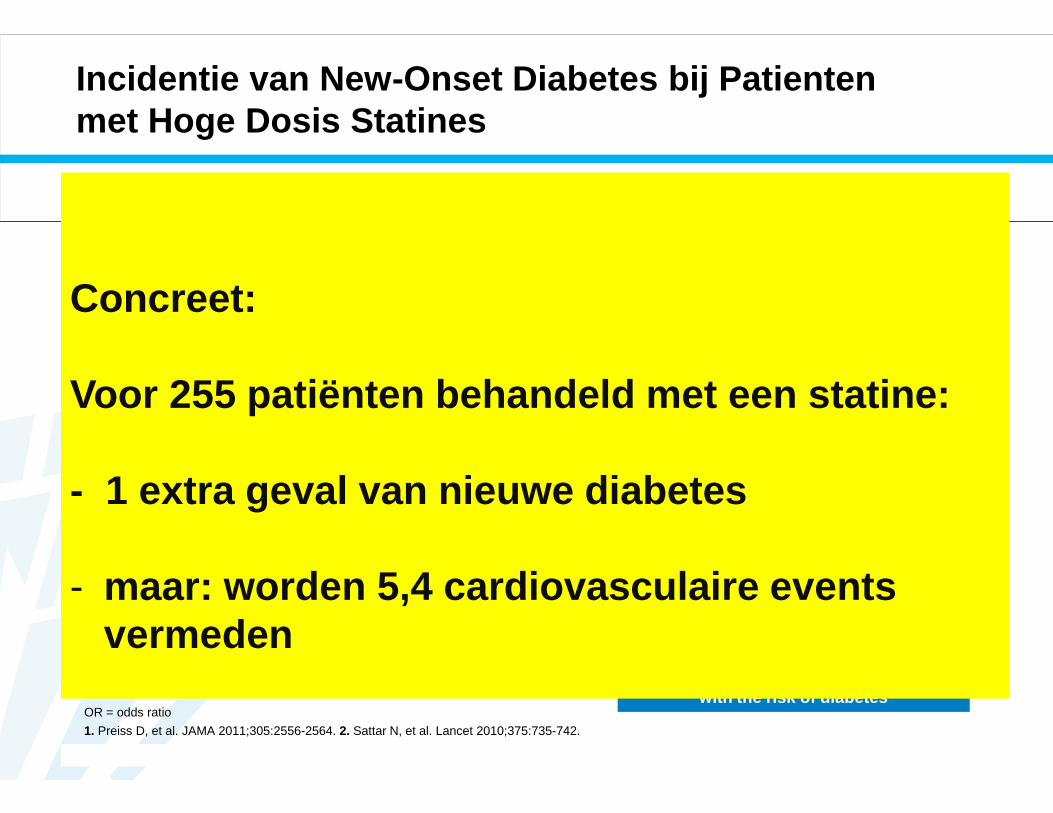
Incidentie van New -Onset Diabetes bij Patientenmet Hoge Dosis Statines
OR = odds ratio
1. Preiss D, et al. JAMA 2011;305:2556-2564. 2. Sattar N, et al. Lancet 2010;375:735-742.
OR (95% CI): 1.12 (1.04–1.22) OR (95% CI): 1.09 (1.0–1.2)
0
500
1000
1500
2000
2500
Per
cent
of P
atie
nts
With
New
O
nset
Dia
bete
s
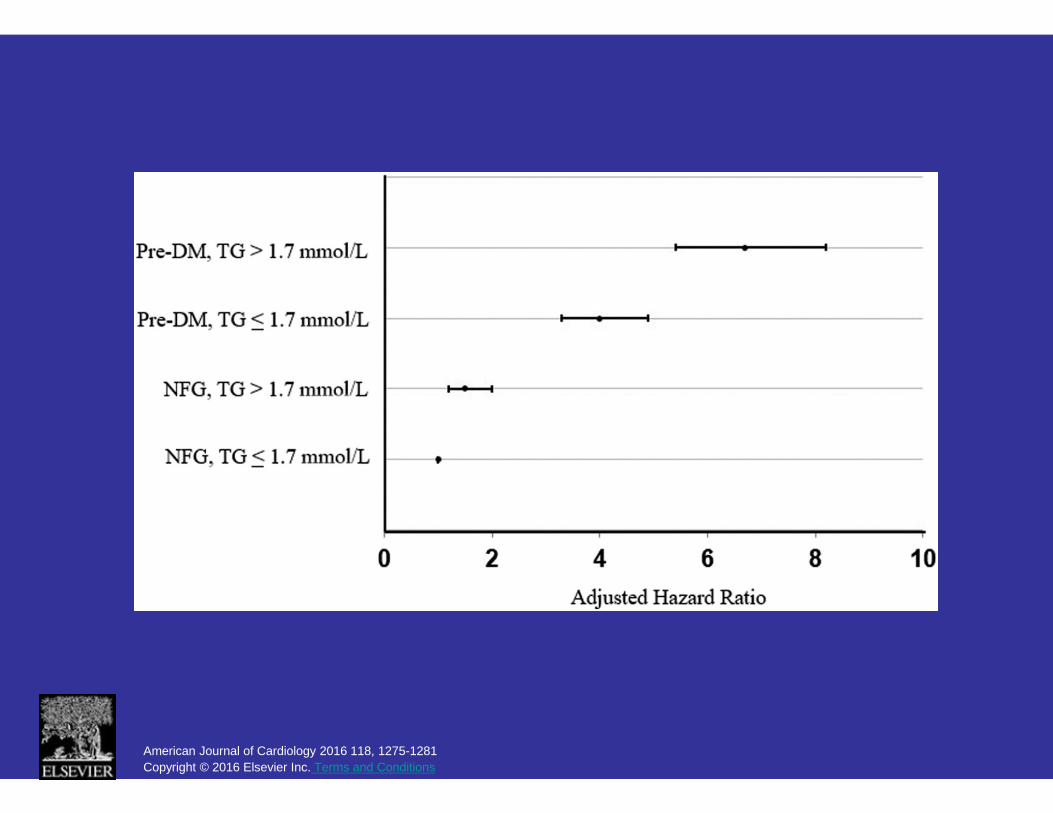
Concreet:
Voor 255 patiënten behandeld met een statine:
- 1 extra geval van nieuwe diabetes
- maar: worden 5,4 cardiovasculaire events vermeden
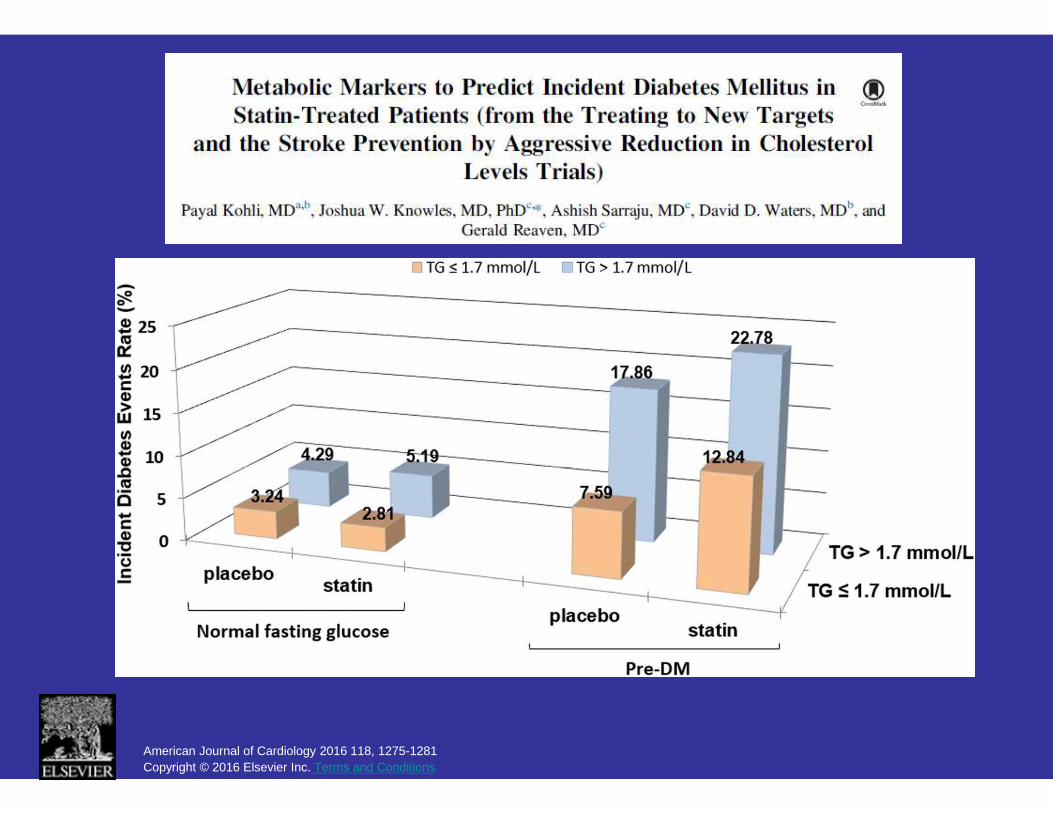
American Journal of Cardiology 2016 118, 1275-1281Copyright © 2016 Elsevier Inc. Terms and Conditions
American Journal of Cardiology 2016 118, 1275-1281 Copyright © 2016 Elsevier Inc. Terms and Conditions

American Journal of Cardiology 2016 118, 1275-1281Copyright © 2016 Elsevier Inc. Terms and Conditions

American Journal of Cardiology 2016 118, 1275-1281 Copyright © 2016 Elsevier Inc. Terms and Conditions

Lotta et al. JAMA. 2016;316(13):1383-1391. doi:10.1001/jama.2016.14568

Ference et al. NEJM 2016;375:22:2144-53
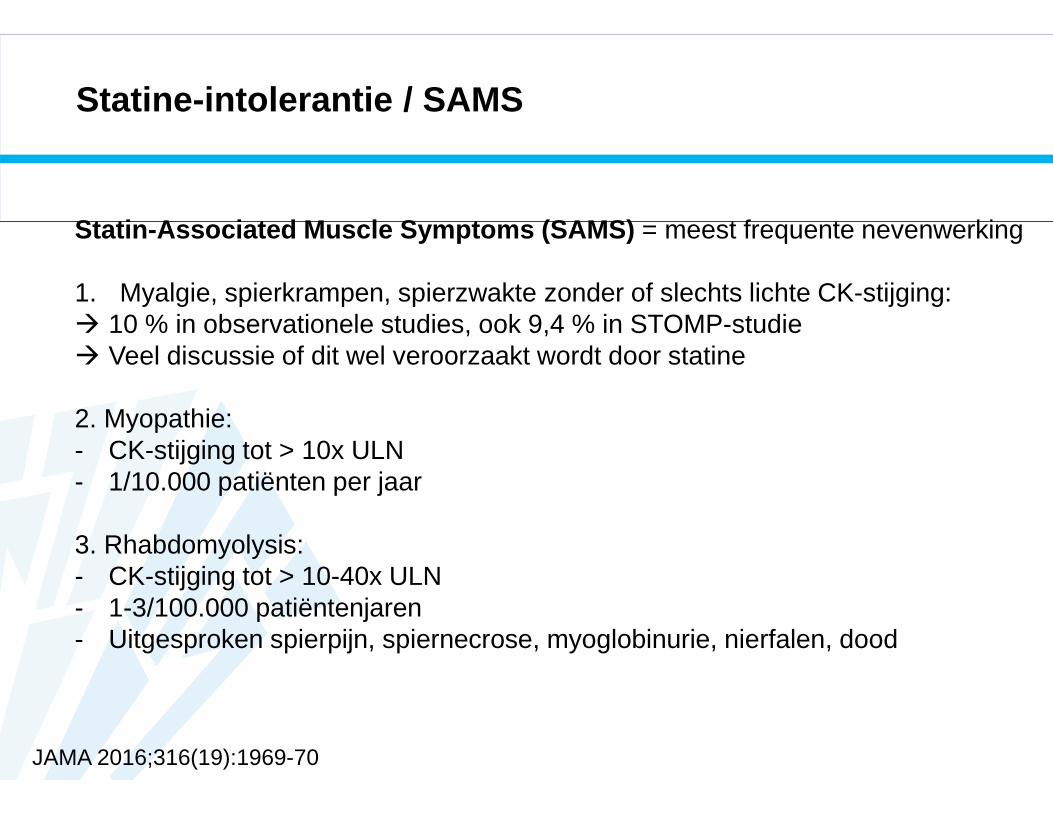
Statine-intolerantie / SAMS
Statin-Associated Muscle Symptoms (SAMS) = meest frequente nevenwerking
1. Myalgie, spierkrampen, spierzwakte zonder of slechts lichte CK-stijging: � 10 % in observationele studies, ook 9,4 % in STOMP-studie� Veel discussie of dit wel veroorzaakt wordt door statine
2. Myopathie:- CK-stijging tot > 10x ULN- 1/10.000 patiënten per jaar
3. Rhabdomyolysis:- CK-stijging tot > 10-40x ULN- 1-3/100.000 patiëntenjaren- Uitgesproken spierpijn, spiernecrose, myoglobinurie, nierfalen, dood
JAMA 2016;316(19):1969-70

Statine-intolerantie / SAMS
4. Necrotiserende myopathie met antistoffen tegen HMG-CoA-Reductase:� leidt tot persisterende myopathie: triade ‘spierpijn + spierzwakte + CK-stijging’,
die niet verdwijnt na stopzetting statine� zeer zelden� Commerciële kit beschikbaar voor bepaling antistoffen
JAMA 2016;316(19):1969-70
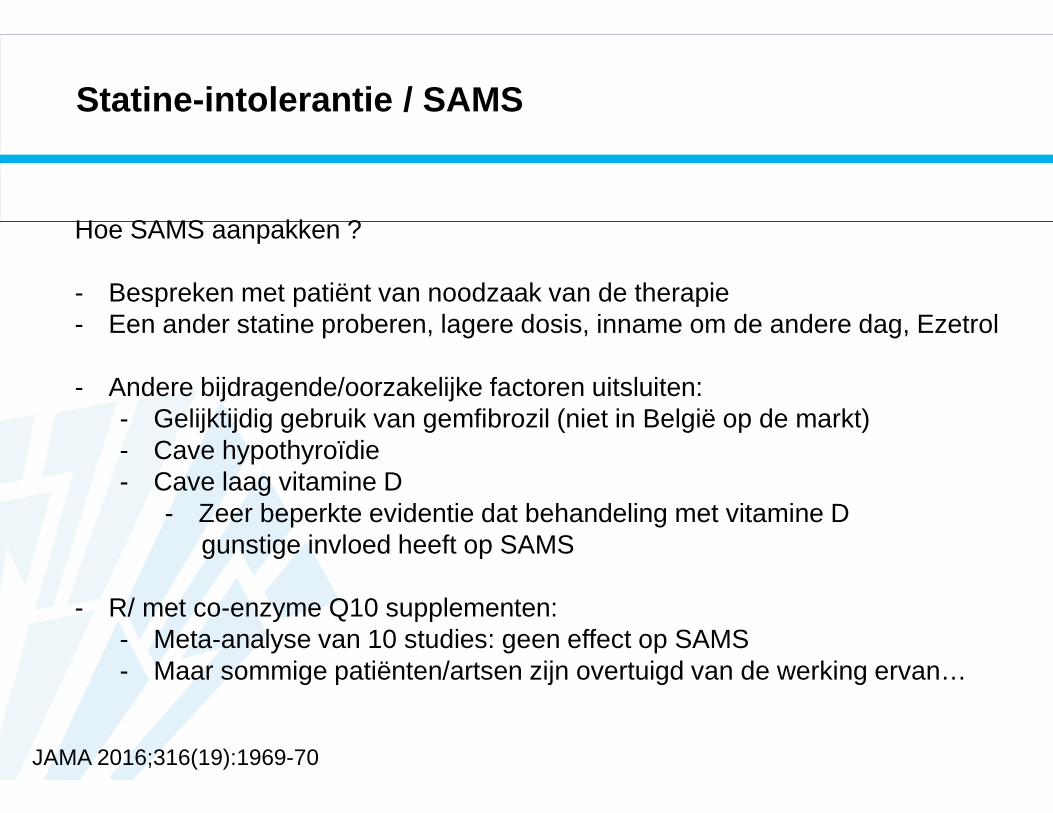
Statine-intolerantie / SAMS
Hoe SAMS aanpakken ?
- Bespreken met patiënt van noodzaak van de therapie- Een ander statine proberen, lagere dosis, inname om de andere dag, Ezetrol
- Andere bijdragende/oorzakelijke factoren uitsluiten:- Gelijktijdig gebruik van gemfibrozil (niet in België op de markt)- Cave hypothyroïdie- Cave laag vitamine D
- Zeer beperkte evidentie dat behandeling met vitamine D gunstige invloed heeft op SAMS
- R/ met co-enzyme Q10 supplementen:- Meta-analyse van 10 studies: geen effect op SAMS- Maar sommige patiënten/artsen zijn overtuigd van de werking ervan…
JAMA 2016;316(19):1969-70
Besluit
Belang van LDL-waarde = overduidelijk
Levensstijlaanpassing steeds benadrukken
Statine = absolute voorkeursbehandeling bij hypercholesterolemie
Niet zomaar ‘fire and forget’, maar dosis van statine aanpassen en monitoren om LDL-target te bereiken
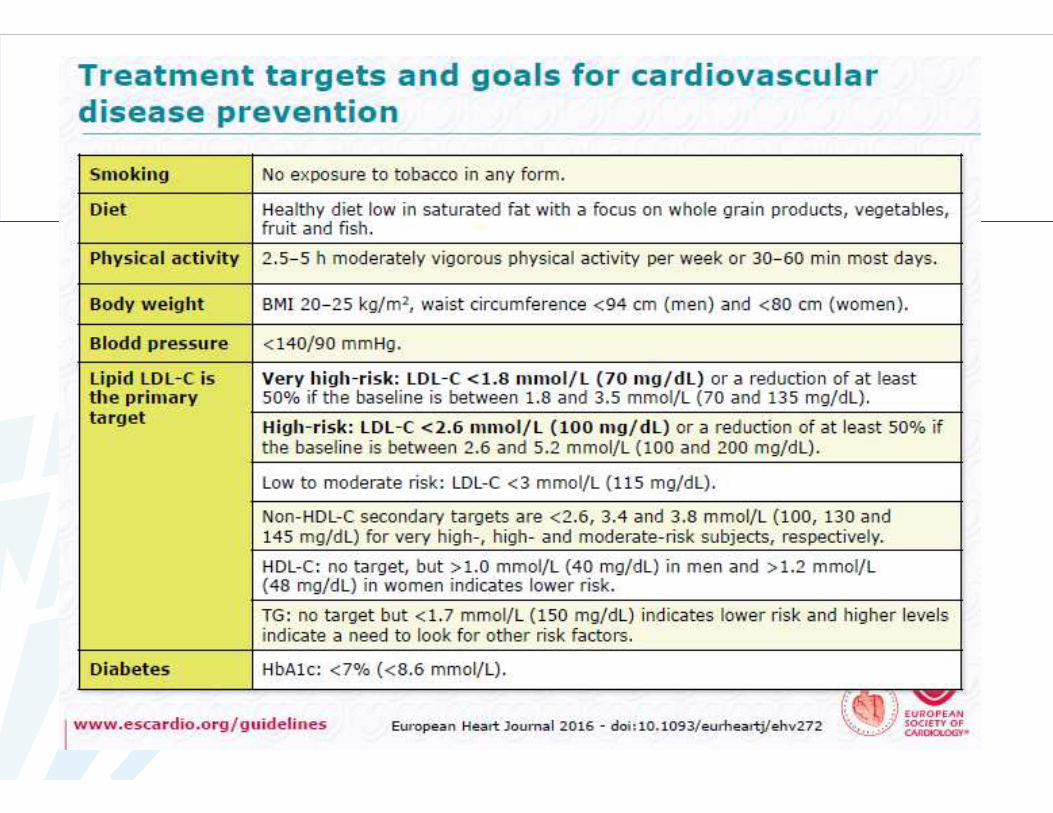
Very high risk LDL < 70 mg/dL of 50 % reductie tov startwaardeHigh risk LDL < 100 mg/dLModerate risk LDL < 115 mg/dL
PCSK9-inhibitoren: voorlopig alleen bij FH patiënten� 2 CVO-studies afwachten ivm eindpunten & veiligheid










![T aTjXg m ?baWlah 05.2019/Norda 24.05.pdf'(Jo]eZd_a Jh `c_Wije a AbeWT F_?j[a" (*$&+$(&'/ HepcemW M 8W`haWX` Fml`\^bjf^\` \a\V]TgbeX` ^ba^hefh Vmb a ^\X` ^b`\f]\ bVXa\T];VX] ceT VX](https://static.fdocuments.net/doc/165x107/5e1f11d5bc713a72ff30abdc/t-atjxg-m-bawlah-052019norda-2405pdfjoezda-jh-cwije-a-abewt-fja.jpg)






![Assessment report · lipoprotein (a) [Lp(a)] in patients with homozygous familial hypercholesterolaemia (HoFH) and in patients with severe heterozygous familial hypercholesterolaemia](https://static.fdocuments.net/doc/165x107/5e32b9f8d3afcb53c94a2775/assessment-report-lipoprotein-a-lpa-in-patients-with-homozygous-familial-hypercholesterolaemia.jpg)

