
Case Presentation Cont. - Lipid inhibition is 2.5-fold greater than previously reported responses in...
1
Advanced Therapies in the Management of Homozygous Familial Hypercholesterolemia Matthew C. Weiss, MD; Vanessa Hurta, NP; James Underberg, MD, MS New York University School of Medicine, New York, NY Background Discussion References • Gidding. The Agenda for Familial Hypercholesterolemia: A Scientific Statement From the American Heart Association. Circulation. 2015. • Nordestgaard. Familial hypercholesterolaemia is underdiagnosed and undertreated in the general population: guidance for clinicians to prevent coronary heart disease. Eur Heart J. 2013. • Goldberg. Familial Hypercholesterolemia: Screening, diagnosis, and management of pediatric and adult patients. Clinical guidance from the National Lipid Assoc. Expert Panel on FH. Journ Clin Lipidology. 2011. • Raal. Inhibition of PCSK9 with evolocumab in homozygous familial hypercholesterolemia (TESLA Part B): a randomised, double-blind, placebo- controlled trial. Lancet. 2014. • Familial Hypercholesterolemia (FH) is an under- recognized autosomal dominant disease with a prevalence of 1:250 in the general population. • Homozygous FH (HoFH), the more severe subtype, is a rare, 1:160,000-300,000 disease, traditionally felt to be due to the complete absence of the LDL-receptor on the hepatocyte; and now recognized to be secondary to a number of possible biallele or compound mutations across various genes, including LDL-R, ApoB, and PCSK9. • Traditional treatment includes the use of statins, bile acid sequestrants, niacin, and ezetimibe. • More recently anti-sense and monoclonal antibody therapies have been developed, but accounts of their simultaneous use have not yet been reported in the literature. Table 1: Cholesterol Response to Medications *on daily: rosuvastatin 40mg, ezetimibe 10mg; and cholestyramine twice daily § on top of baseline medications ¶ on top of baseline medications and mipomersen • This is the first known case of a HoFH patient simultaneously treated with traditional and recently- approved medications, including the anti-sense drug mipomersen and a PCSK9 inhibitor. • The patient’s dramatic 74% reduction in LDL-C with PCSK9 inhibition is 2.5-fold greater than previously reported responses in HoFH patients (TESLA). • Her response to medical therapy informs the clinician of her genotype; namely, her dramatic response to PCSK9 inhibition excludes the “traditionally” conceived null/null LDL-R genotype of classic HoFH. • In this case, treatment with mipomersen and evolocumab on top of standard therapies, was not only safe and highly efficacious in reducing cholesterol burden, but also avoided the need for additional therapy, including apheresis. • Index admission: TTE with severe aortic stenosis and cardiac catheterization with multi-vessel disease. She underwent CABG and AVR. LDL-C on index admission was 360mg/dL despite compliance with therapies previously mentioned. • In Lipid Clinic follow-up, her diagnosis was specified as HoFH. • She was started on mipomersen, a second-generation oligonucleotide anti-sense therapy, which inhibits translation of ApoB-100 mRNA thereby reducing atherogenic lipoprotein production. Case Presentation Cont. • After three doses of mipomersen her LFTs were unchanged and her LDL-C was 238mg/dL. • At that time the FDA approved a novel injectable PCSK9 inhibitor for treatment of FH and the patient was empirically trialed on evolocumab on top of background therapy. After two doses, LDL-C was 62mg/dL. Objective Case Presentation Cont. • We report the first known case, to our knowledge, of the simultaneous use of the combination of mipomersen and evolocumab in a patient with HoFH. Case Presentation • A 41 year-old Hispanic woman presented to the Bellevue Hospital Lipid Clinic after recent hospitalization for angina. • PMH: HIV (on HAART, CD4 656) and “hyperlipidemia.” • Medications: daily rosuvastatin 40mg, ezetimibe 10mg, aspirin 81mg and twice daily cholestyramine. • Never-smoker. • Fam Hx: +HLD in father, paternal grandmother, and in multiple siblings • As a 7 year-old child in Mexico she had developed sub- cutaneous nodules on her elbows and ankles. Tot Chol (mg/dL) LDL (mg/dL) HDL (mg/dL) TG (mg/dL) Non-HDL (mg/dL) ApoB (mg/dL) % LDL Reduction From immediately prior Index admission* 419 360 30 147 389 288 -- First Lipid Clinic visit* 397 331 31 193 366 -- -- S/p 3 doses mipomersen § 287 238 33 83 254 -- 28 S/p 2 doses evolocumab ¶ 108 62 38 40 70 48 74 Figures 1-3: Physical Exam Findings 1) Right lateral elbow xanthoma 2) Flexor surface Left elbow 3) AP view of Right ankle xanthoma 3. 1. 2.
Transcript of Case Presentation Cont. - Lipid inhibition is 2.5-fold greater than previously reported responses in...
Advanced Therapies in the Management of Homozygous Familial Hypercholesterolemia Matthew C. Weiss, MD; Vanessa Hurta, NP; James Underberg, MD, MS
New York University School of Medicine, New York, NY
Background
Discussion
References • Gidding. The Agenda for Familial Hypercholesterolemia: A Scientific Statement
From the American Heart Association. Circulation. 2015. • Nordestgaard. Familial hypercholesterolaemia is underdiagnosed and
undertreated in the general population: guidance for clinicians to prevent coronary heart disease. Eur Heart J. 2013.
• Goldberg. Familial Hypercholesterolemia: Screening, diagnosis, and management of pediatric and adult patients. Clinical guidance from the National Lipid Assoc. Expert Panel on FH. Journ Clin Lipidology. 2011.
• Raal. Inhibition of PCSK9 with evolocumab in homozygous familial hypercholesterolemia (TESLA Part B): a randomised, double-blind, placebo-controlled trial. Lancet. 2014.
• Familial Hypercholesterolemia (FH) is an under-recognized autosomal dominant disease with a prevalence of 1:250 in the general population.
• Homozygous FH (HoFH), the more severe subtype, is a rare, 1:160,000-300,000 disease, traditionally felt to be due to the complete absence of the LDL-receptor on the hepatocyte; and now recognized to be secondary to a number of possible biallele or compound mutations across various genes, including LDL-R, ApoB, and PCSK9.
• Traditional treatment includes the use of statins, bile acid sequestrants, niacin, and ezetimibe.
• More recently anti-sense and monoclonal antibody therapies have been developed, but accounts of their simultaneous use have not yet been reported in the literature.
Table 1: Cholesterol Response to Medications *on daily: rosuvastatin 40mg, ezetimibe 10mg; and cholestyramine twice daily §on top of baseline medications ¶on top of baseline medications and mipomersen
• This is the first known case of a HoFH patient simultaneously treated with traditional and recently-approved medications, including the anti-sense drug mipomersen and a PCSK9 inhibitor.
• The patient’s dramatic 74% reduction in LDL-C with PCSK9 inhibition is 2.5-fold greater than previously reported responses in HoFH patients (TESLA).
• Her response to medical therapy informs the clinician of her genotype; namely, her dramatic response to PCSK9 inhibition excludes the “traditionally” conceived null/null LDL-R genotype of classic HoFH.
• In this case, treatment with mipomersen and evolocumab on top of standard therapies, was not only safe and highly efficacious in reducing cholesterol burden, but also avoided the need for additional therapy, including apheresis.
• Index admission: TTE with severe aortic stenosis and cardiac catheterization with multi-vessel disease. She underwent CABG and AVR. LDL-C on index admission was 360mg/dL despite compliance with therapies previously mentioned.
• In Lipid Clinic follow-up, her diagnosis was specified as HoFH. • She was started on mipomersen, a second-generation oligonucleotide anti-sense therapy,
which inhibits translation of ApoB-100 mRNA thereby reducing atherogenic lipoprotein production.
Case Presentation Cont. • After three doses of mipomersen her LFTs were
unchanged and her LDL-C was 238mg/dL. • At that time the FDA approved a novel injectable
PCSK9 inhibitor for treatment of FH and the patient was empirically trialed on evolocumab on top of background therapy. After two doses, LDL-C was 62mg/dL.
Objective
Case Presentation Cont.
• We report the first known case, to our knowledge, of the simultaneous use of the combination of mipomersen and evolocumab in a patient with HoFH.
Case Presentation • A 41 year-old Hispanic woman presented to the
Bellevue Hospital Lipid Clinic after recent hospitalization for angina.
• PMH: HIV (on HAART, CD4 656) and “hyperlipidemia.” • Medications: daily rosuvastatin 40mg, ezetimibe 10mg,
aspirin 81mg and twice daily cholestyramine. • Never-smoker. • Fam Hx: +HLD in father, paternal grandmother, and in
multiple siblings • As a 7 year-old child in Mexico she had developed sub-
cutaneous nodules on her elbows and ankles.
Tot Chol
(mg/dL)
LDL
(mg/dL)
HDL
(mg/dL)
TG
(mg/dL)
Non-HDL
(mg/dL)
ApoB
(mg/dL)
% LDL
Reduction From immediately
prior
Index
admission* 419 360 30 147 389 288 --
First Lipid
Clinic visit* 397 331 31 193 366 -- --
S/p 3 doses
mipomersen§ 287 238 33 83 254 -- 28
S/p 2 doses
evolocumab¶ 108 62 38 40 70 48 74
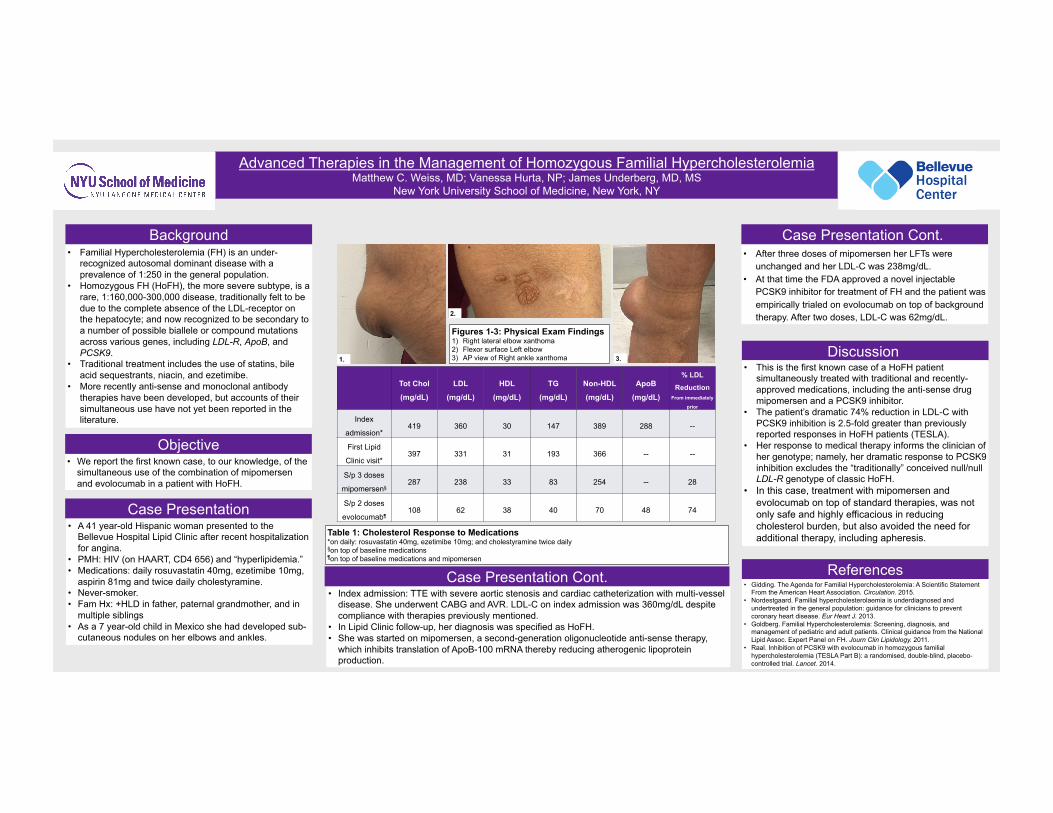
Figures 1-3: Physical Exam Findings 1) Right lateral elbow xanthoma 2) Flexor surface Left elbow 3) AP view of Right ankle xanthoma 3. 1.
2.
![BOYMOR.QLE QL.REP] - Stacksxk898wv6983/xk898wv6983.pdf · 15 jun 1978 6:55 boymor.qle ql,rep] page 1-1 (cont.) (cont.) (cont.) (cont.) (cont.) (cont.) prover prover (cont.) 5 comment](https://static.fdocuments.net/doc/165x107/6057337242a55f07515b3baa/qlrep-stacks-xk898wv6983xk898wv6983pdf-15-jun-1978-655-boymorqle-qlrep.jpg)




![Mipomersen, an apolipoprotein B synthesis inhibitorlnu.diva-portal.org/smash/get/diva2:1308142/FULLTEXT01.pdf · Lipoprotein(a) (Lp[a]) is known to be a factor in increasing the risk](https://static.fdocuments.net/doc/165x107/5e55e7f6dcf0151cc70848f0/mipomersen-an-apolipoprotein-b-synthesis-1308142fulltext01pdf-lipoproteina.jpg)











