
Chizobam N. Idahosa and A. Ross...
35
Clinical Evaluation of Oral Diseases Chizobam N. Idahosa and A. Ross Kerr Abstract Oral medicine is concerned with the diagnosis and non-surgical management of medically related disorders of the oral and maxillofacial region as well as the oral health management of medically compromised patients. Oral diseases have a wide range of clinical presentations and can manifest either as a local oral disease or as a sign of an underlying systemic condition. Therefore, oral health is a vital component of overall systemic health and an oral lesion may in certain situations be the initial presentation of a systemic disorder. Consequently, it is imperative that oral health-care providers and physicians are adequately trained to accurately diagnose and manage diseases affecting the oral and maxillofacial region. This chapter addresses the systematic approach required for the evaluation of patients who present with oral diseases. This includes the process of obtaining a thorough history, performing a comprehensive clinical examination, performing vital signs, and ordering appropri- ate investigations that provide the clinician with key information vital to establishing a final diagnosis. The categories and classifica- tion systems of oral diseases as well as the indications for referrals and consultations with other health-care providers and guidelines for documentation are reviewed. Keywords Medical history • Physical examination • Extraoral examination • Intraoral examination • Differential diagnosis • Definitive diagnosis • Documentation Contents Introduction .......................................... 2 The Medical Record ................................. 2 The Patient History .................................. 2 The Patient Examination ............................ 11 Imaging ............................................... 24 Diagnosis .............................................. 25 Referral/Consultation ............................... 32 Documentation ....................................... 34 Conclusion and Future Directions .................. 34 Cross-References ..................................... 34 References ............................................ 34 C.N. Idahosa Department of Oral and Maxillofacial Pathology, Medicine and Surgery, Temple University Kornberg School of Dentistry, Philadelphia, PA, USA e-mail: [email protected] A.R. Kerr (*) Department of Oral and Maxillofacial Pathology, Radiology & Medicine, New York University College of Dentistry, NY, New York, USA e-mail: [email protected] # Springer International Publishing AG 2017 C.S. Farah et al. (eds.), Contemporary Oral Medicine, DOI 10.1007/978-3-319-28100-1_3-1 1
Transcript of Chizobam N. Idahosa and A. Ross...

Clinical Evaluation of Oral Diseases
Chizobam N. Idahosa and A. Ross Kerr
AbstractOral medicine is concerned with the diagnosisand non-surgical management of medicallyrelated disorders of the oral and maxillofacialregion as well as the oral health management ofmedically compromised patients. Oral diseaseshave a wide range of clinical presentations andcan manifest either as a local oral disease or asa sign of an underlying systemic condition.Therefore, oral health is a vital component ofoverall systemic health and an oral lesion mayin certain situations be the initial presentationof a systemic disorder. Consequently, it isimperative that oral health-care providers andphysicians are adequately trained to accuratelydiagnose and manage diseases affecting theoral and maxillofacial region. This chapteraddresses the systematic approach requiredfor the evaluation of patients who presentwith oral diseases. This includes the processof obtaining a thorough history, performing
a comprehensive clinical examination,performing vital signs, and ordering appropri-ate investigations that provide the clinicianwith key information vital to establishing afinal diagnosis. The categories and classifica-tion systems of oral diseases as well as theindications for referrals and consultationswith other health-care providers and guidelinesfor documentation are reviewed.
KeywordsMedical history • Physical examination •Extraoral examination • Intraoral examination •Differential diagnosis • Definitive diagnosis •Documentation
ContentsIntroduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
The Medical Record . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
The Patient History . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
The Patient Examination . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
Imaging . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
Referral/Consultation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
Documentation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
Conclusion and Future Directions . . . . . . . . . . . . . . . . . . 34
Cross-References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
C.N. IdahosaDepartment of Oral andMaxillofacial Pathology, Medicineand Surgery, Temple University Kornberg School ofDentistry, Philadelphia, PA, USAe-mail: [email protected]
A.R. Kerr (*)Department of Oral and Maxillofacial Pathology,Radiology & Medicine, New York University College ofDentistry, NY, New York, USAe-mail: [email protected]
# Springer International Publishing AG 2017C.S. Farah et al. (eds.), Contemporary Oral Medicine,DOI 10.1007/978-3-319-28100-1_3-1
1

Introduction
Oral medicine is a specialty at the interface ofmedicine and dentistry focused on the diagnosisand nonsurgical management of medically relateddisorders of the oral and maxillofacial region(Scully et al. 2016; Stoopler et al. 2011). Thescope of practice of an oral medicine specialistinvolves the evaluation of patients with a widerange of maxillofacial conditions including “oralmucosal disorders, orofacial pain, temporoman-dibular disorders, salivary gland disorders,chemosensory disorders, sleep disorders, oralmanifestations of systemic disorders, as well asthe dental treatment of medically compromisedpatients” (Sollecito et al. 2013). The oral cavityis the gateway to the body; therefore, oral health isan essential component of overall systemic health.Many systemic disorders have oral manifesta-tions; conversely, the oral management of patientsmay be impacted by the presence of systemicdisorders (Stoopler and Sollecito 2016). There-fore, it is important that oral health-care providersare trained, not only to diagnose and managepatients with odontogenic diseases (i.e., dentalcaries/odontogenic infections, periodontal dis-eases, and malpositioned teeth/jaws) but also toeffectively diagnose other oral diseases within thescope of oral medicine and provide safe dentaltreatment to those patients with underlying sys-temic disorders (Miller et al. 2001). This chapteraddresses the necessary steps involved in the eval-uation of patients who present with such diseases,both soft and hard tissue diseases. This includesthe process of obtaining a thorough history,performing a comprehensive clinical examina-tion, performing vital signs, and ordering appro-priate investigations such as laboratory tests andimaging, that provide the clinician with key infor-mation vital to establishing a final diagnosis. Thecategories and classification systems of oral dis-eases as well as a general overview of the diag-nostic process, the indications for referrals andconsultations with other health-care providers,and guidelines for documentation are reviewed.
The Medical Record
The patient’s medical information obtained from aclinical evaluation is considered confidential andmust be carefully documented and stored forfuture reference in a safe and protected manner.The medical record is collected either as a paper-based health record or as an electronic healthrecord (EHR). Transmission of informationbetween multiple providers caring for the samepatient is often inefficient, prone to errors, andslow with the use of paper-based health records.As clinical management of patients often requiresinput from multiple health-care providers, therehas been a move by many countries to implementthe use of EHR as a means of improving safety,efficiency, and accessibility of records acrossmultiple sites (Ludwick and Doucette 2009).Irrespective of the type of record used, it is theresponsibility of the oral health-care provider toobtain and record all information relevant to thepatient’s treatment including all aspects of thehistory, examination findings, vital signs, andinvestigational reports such as clinical photo-graphs, radiographs/medical imaging studies, lab-oratory tests, and histopathological findings.
The Patient History
The history is the information relevant to thepatient’s health obtained by careful interview ofthe patient or a reliable source. For new patients,the initial goal of the history is to help reach a finaldiagnosis and formulate a treatment plan. For anestablished patient, the goal is to elicit new infor-mation to facilitate ongoing care. The patient’shistory alone often reveals key elements of theinformation needed to reach a definitive diagno-sis, and the importance of a thorough and system-atic approach to collect this information cannot beunderestimated. The history also aids in the riskassessment of patients prior to the provision oforal care as medical conditions that may increasethe risk of adverse events and complications in thedental setting are identified. Likewise, through thehistory, symptoms that may indicate the presenceof undiagnosed health conditions may be
2 C.N. Idahosa and A.R. Kerr

recognized. The process of history-taking pro-vides an opportunity for the clinician to developa rapport with the patient, which is necessary foreffective communication during the interview andsubsequent encounters. It is important for the cli-nician to make the patient comfortable bearing inmind that patients come from diverse social andcultural backgrounds with differing attitudes andbeliefs to health care. The clinician should there-fore encourage the participation of the patient indecision-making and should listen to the patient’sperceptions and concerns regarding their clinicalproblems respectfully and without bias. It is alsoimportant that the clinician greets the patient in aculturally appropriate manner, ensures that theinterview location is private, and pays attentionto the patient during the interview. The use ofopen-ended questions is preferred to directquestioning and clarification of the patient’sunderstanding should be sought when appropri-ate. Language barriers can be a major issue, andinterpreters should be on hand to facilitate com-munication. In addition, parents or legal guardiansmust accompany minors and those with disabil-ities that limit communication. An exhaustivesystematic approach should be followed forevery patient, whether new or established. Thiswill maximize the opportunity to capture all rele-vant information and minimize the risk of missingsomething. The master clinician with years ofexperience can often quickly and efficiently nav-igate the history, whereas the novice may be lessefficient and take longer. The road to mastery isbuilt on a disciplined systematic approach wherethere is no room for shortcuts. Table 1 providesthe elements for taking both a new and establishedpatient history.
Biographical data: The biographical data areimportant for identification and administrativepurposes as well as to ensure that the patient’scontact information is accurate and available foruse when needed. This includes the patient’sname, contact information, date of birth, gender,race/ethnicity, primary language, occupation, andprimary care physician’s name and contact infor-mation (and other pertinent specialists).
Chief concern: The chief concern states whythe patient is in your office. It is a brief description
Table 1 Elements of the new patient encounter
Chief concernHistory of presenting concernOnset of symptomsAnatomic site(s)Description of symptom(s)Precipitating factorsAggravating/relieving factorsSecondary signs or symptomsHistory of past investigations and treatments
Medical historyCurrent medical diagnosesPast medical historyCurrent medicationsAllergiesReview of systemsFamily medical historySexual history
Social historyRelationship statusChildrenOccupationCultural and religious beliefsTobacco useAlcohol useIllicit drug useRecent travel history
Dental historyCurrent dental symptomsLast dental visit and reason for seeking dental careFrequency of dental visitsPrevious dental treatmentsHistory of maxillofacial traumaHome careOral habitsTMJ historyExposure to fluoride and type of fluoridePresence of dental phobia
Nutritional historyExtraoral examinationGeneral inspectionSkin/hairEyesTMJsMuscles of masticationSalivary glandsMidline neck structuresLymph nodes
Intraoral examinationLipsLabial mucosaeBuccal mucosaeGingivaeTongueHard palateOropharynxFloor of mouth
(continued)
Clinical Evaluation of Oral Diseases 3

of the primary reason for the patient’s consultationand evaluation recorded in the patient’s ownwords. Examples of chief concerns include orallesions, pain, altered sensations (e.g., numbness,taste alterations), dry mouth or too much saliva,halitosis, slow healing of a surgical wound, facialor oral/neck swelling, abnormal bleeding, an alter-ation in oral function (e.g., chewing, swallowingetc.), or tooth abnormalities.
History of presenting concern: The history ofpresenting concern is an exhaustive chronologicalaccount of all aspects of the chief concernobtained by carefully interviewing the patient.The following information should be documentedas part of the history of presenting concern, andthe reader is alerted to Table 2 where examples ofspecific questions for selected categories of chiefcomplaints are provided.
(i) Onset of symptoms: Determine when thesymptoms started and if the onset was sud-den or gradual.
(ii) Anatomic site(s): Determine the anatomicsite affected and ascertain whether thesymptoms involve a single anatomic loca-tion or multiple sites.
(iii) Description of symptoms: This includes adescription of the course of symptoms andtheir characteristics considering both quali-tative and quantitative descriptors. Establish
if the symptoms are occurring for the firsttime or recurring. Determine if the symp-toms are constant or episodic. Also, find out
Table 1 (continued)
DentitionSaliva
Cranial nerves (I–XII)Vital signsBlood pressureHeart rate and rhythmRespirationTemperature
ImagingPhotography/videographyPlain filmsComputed tomography (CT)Magnetic resonance imaging (MRI)Sialography
DiagnosisDifferential diagnosis/working diagnosisDefinitive diagnosis
Treatment
Table 2 History of present illness
Questions for patients with ulcerative lesionsWhen did it start?How did it start?Any history of trauma?Is this the first episode or is it recurrent?How many? Single or multiple?Do the old ones heal before new ones come up?Any pain, sensitivity to spicy foods, difficulty eating or
swallowing?Any extraoral sites involved? Skin, genital, scalp,
ocular.Did you start a new medication or oral hygiene
product?Any associated systemic symptoms such as fever and
malaise?Does anyone in your family have similar problems?Do you have any gastrointestinal symptoms such as
diarrhea and bleeding?Any joint pain?
Questions for patients with salivary gland disorders:When did the problem start?Any swelling? Where is the swelling? Is it associated
with meals?Any pain? Where is the pain? Is it associated with
meals?Is your mouth dry?Has the texture of your saliva changed?Any pus draining?Are your eyes dry?Any joint pain?Any associated systemic symptoms such as fever and
malaise?Does anyone in your family have similar problems?
Questions for patients with temporomandibular jointdisorders:When did the symptoms start?Any precipitating factors such as trauma or prolonged
mouth opening?Any joint sounds in the past or currently?Is your mouth opening restricted?Has your jaw ever locked in the past?Do you clench or grind your teeth?Has your occlusion changed?Do you have joint/muscle pain affecting other parts of
your body?Any altered sensation?
4 C.N. Idahosa and A.R. Kerr

if symptoms are stable, worsening, orimproving. Ask the patient to describe thecharacteristics of the symptoms, in theirown words, using qualitative descriptorssuch as dull, sharp, throbbing, aching, stab-bing, electric shock-like, burning, dry, itchy,thick, rough, bumpy, swollen. Pain or dis-comfort should be rated quantitatively usinga scale such as visual analog/numerical rat-ing scale from 1 (minimal) to 10 (unbear-able) or a Wong-Baker Faces scale (Fig. 1)(Wong-Baker FACES Foundation 2016).Enquire about the impact of the symptomson the patient’s quality of life.
(iv) Precipitating factors: Enquire about any fac-tors that triggered the onset or that exacer-bated the symptoms.
(v) Aggravating/relieving factors: Determinewhat makes the symptoms better or worse.
(vi) Secondary signs or symptoms: These areseparate from the primary symptom(s) andoften the patient may be unaware they maybe correlated with the underlying problem(e.g., primary herpetic gingivostomatitis canbe associated with fever and malaise, orsleep issues may lead to an increase inorofacial pain).
(vii) History of past investigations and treat-ments: Prior diagnoses, investigations, andtreatment modalities for the chief concernshould be noted including pertinent negativeresults and failed treatments such as medi-cation regimens.
Medical history: Although a self-administered health history form is routinely uti-lized for obtaining medical history informationfrom patients, it is not equivalent to an exhaustivehistory. It is imperative that the oral health-careprovider verbally reviews all entries on the health-history formwith all patients, and supplements thehistory with additional questions as deemednecessary.
(i) Current medical diagnoses: A thoroughmedical history should be elicited toinclude details of the patient’s current med-ical diagnosis as well as treatment
modalities. The oral health-care providershould determine if the patient has beendiagnosed with any of the medical condi-tions listed in Table 3. Information relevantto the onset of diagnosis, course of disease,associated complications, and level of con-trol should be documented. This will facil-itate risk assessment and the identificationof conditions that may necessitate modifi-cations to treatment. In addition, it is impor-tant to include information on routinehealth maintenance, the type of medicalspecialist managing the patient, as well asthe frequency of office visits. For example,the medical history on a 57-year-old dia-betic female patient would include informa-tion on date of diagnosis, frequency ofoffice visits to her endocrinologist and/orprimary care physician, home blood glu-cose test results, HbA1c, and target organdamage. The medical history should alsoinclude all relevant details of treatmentmodalities, which can potentially alter thedelivery of care, such as implanted defibril-lators in patients with cardiovascular disor-ders, chemotherapy scheduling in oncologypatients, dialysis scheduling in patientswith end-stage renal disease, and chronicleof total joint replacements.
(ii) Past medical history: Patients should beasked if they have had any relevant medicalproblems in the past. The history shouldinclude previous major illnesses, consulta-tions and referrals to specialists and theiroutcomes, hospitalizations, surgeries,major trauma, and blood transfusions.
(iii) Current medications: Document all currentmedications and supplements taken by thepatient. These include prescription medica-tions, over-the-counter medications, vita-mins, herbal supplements, and traditionalhome remedies. The name, dosage, route,frequency, start date, and reason why thepatient is taking each medication should benoted. Online medication references haveevolved rapidly and are indispensable toolsthat should be utilized for checking thecategory, mechanism of action, dosing and
Clinical Evaluation of Oral Diseases 5

administration details, adverse reactions,and interactions. When possible, thegeneric medication name should be usedfor the purposes of recording the medica-tions in the patient’s record. When patientsare unsure of the medications they are tak-ing, it is important to seek clarification fromtheir physician or pharmacist. Cliniciansshould be alerted to specific medicationsthat have increased potential for adverseevents and that can influence treatmentdecisions, such as antiresorptive agents(e.g., bisphosphonates), anticoagulants,
immunosuppressants (e.g., corticoste-roids), immunomodulators, and medica-tions for treating cancer (e.g.,chemotherapy and immune therapies).
(iv) Allergies: History of drug, food, and envi-ronmental allergies should be carefullydocumented. The type of allergic reactionexperienced as well as the severity of theepisode should be noted (e.g., contact der-matitis, anaphylactic reaction). It is impor-tant to make a distinction between adversereactions to medications and true allergy.For example, gastrointestinal side effects
Fig. 1 Wong-Baker FACES® Pain Rating Scale. After explaining to the patient that each face represents a person with nopain, some, or a lot of pain, the patient is asked to choose the face that best depicts the pain they are experiencing
Table 3 Pertinent medical history.
Cardiovascular Hypertension, congestive heart failure, angina, myocardial infarction, arrhythmia, infectiveendocarditis, rheumatic heart disease
Pulmonary Asthma, emphysema, tuberculosis, seasonal and environmental allergiesEndocrine Diabetes, thyroid disease, Addison’s disease, Cushing syndromeHematologic Sickle cell anemia, other forms of anemia, leukemia, lymphoma, multiple myeloma, other
hematologic disordersGenitourinary Kidney diseaseGastrointestinal Peptic ulcer, GERD, Crohn’s disease, ulcerative colitis, hepatitis, cirrhosisNeurologic Epilepsy/seizures, CVA, headaches, multiple sclerosisPsychiatric/emotional
Anxiety, depression, eating disorders, drug abuse and dependence, bipolar, schizophrenia
Musculoskeletal Osteoarthritis, osteoporosis, rheumatoid arthritisInfectiousdiseases
HIV/AIDS
Skin Rashes, ulcersMalignancy
GERD gastroesophageal reflux disease, CVA cerebrovascular accident, HIV human immunodeficiency virus, AIDSacquired immunodeficiency syndrome
6 C.N. Idahosa and A.R. Kerr

such as nausea, vomiting, and constipationmay not be related to an allergic reaction.
(v) Review of systems: The review of systemsis a careful and systematic review of rele-vant signs and symptoms related to differ-ent body systems that the patient may beexperiencing or has experienced in therecent past (see Table 4). As an integralpart of the medical history, the review ofsystems is helpful in identifying other med-ical problems that have not yet been diag-nosed (e.g., polydipsia, polyphagia,polyuria in a patient who has not been diag-nosed with diabetes mellitus). Review ofsystems is also helpful in assessing theseverity of diagnosed medical problems.An example would be dyspnea with mildactivity versus strenuous exercise in apatient diagnosed with congestive heartfailure. Finally, the review of systems canuncover pertinent details relevant to thechief concern/history of presenting con-cern, which will aid in reaching a diagnosis(e.g., skin and genital lesions in a patientwith oral ulcers secondary to Behcet’s dis-ease). Both positive and negative responsesshould be documented. All positiveresponses should be followed up withmore in-depth and focused questions andthese patients should be referred to theirphysicians for further evaluation and man-agement as indicated.
(vi) Family medical history: This shouldinclude information on hereditary diseases(e.g., hemophilia), familial illnesses (e.g.,recurrent aphthous stomatitis, hyperten-sion, diabetes mellitus, cancers, psychiatricdisorders, alcohol, and drug addiction),contagious infections (e.g., tuberculosis),and illnesses arising from environmentalexposure to toxins. The relationship of thepatient to the affected relative, current sta-tus of the relative (alive or deceased) andcause of death if deceased should be noted.
(vii) Sexual history: Information related to thepatient’s sexual history (sexual relation-ships, practices, and number of partners)relevant to their chief concern or
examination findings should bedocumented. This is particularly relevantto infectious diseases with the potential tohave oral manifestations including ashuman immunodeficiency virus (HIV)infection, syphilis, gonorrhea, human pap-illoma virus (HPV) infections, herpes sim-plex virus (HSV) infection, infectiousmononucleosis, and hepatitis B or C.
(viii) Psychological history: The psychologicalhistory is an important element of the med-ical history that may be overlooked.Patients suffering from depression, anxiety,or other mental illnesses require carefulevaluation, and a comprehensive historyof their clinical course and treatments,including medications, must be elicited.Patients who appear to have undiagnosedmental illness should be referred to a pri-mary care provider.
Social history: The patient’s social history willreveal information about the following domains:
(i) Relationship status: This will provideinsight on the level of support available tothe patient. Find out whether the patient issingle, married, divorced, in a domesticpartnership, or in a long-term relationship.
(ii) Children: Find out if the patient has chil-dren and their level of dependency. Alter-natively, if they are older, can they provideadditional support as needed by the patient?
(iii) Occupation: It is helpful to know the typeof work the patient does (e.g., outdoorsvs. indoors).
(iv) Cultural and religious beliefs: With thegrowing trend in immigration and popula-tion migration, oral health-care providersshould be cognizant of the fact that patientscome from different backgrounds with var-ious cultural and religious beliefs, whichcan impact provision of care. Patientsfrom certain ethnicities may decline oralmedications and opt for herbal and tradi-tional remedies while others may be unableto comply with instructions during periodsof fasting. Also, based on their religious
Clinical Evaluation of Oral Diseases 7

doctrine that blood is sacred, Jehovah’sWitnesses do not accept transfusion ofwhole blood and its four major derivatives(red cells, white cells, plasma, and platelets)but may accept transfusion of blood prod-ucts such as clotting factors, erythropoietin,and immunoglobulins (Sarteschi 2004).
(v) Tobacco use: Tobacco use is a leadingcause of preventable death. According tothe World Health Organization (WHO),there are 1 billion smokers worldwide andtobacco use is a public health threat leadingto the death of approximately 6million peo-ple a year (WHO 2016). Tobacco productsadversely affect nearly every human organsystem. Exposure leads to the developmentof a wide range of disorders including sys-temic diseases (e.g., cardiovascular dis-eases, respiratory diseases, and cancers)and oral diseases (e.g., periodontal disease,oral potentially malignant disorders, andoral cancer) resulting in reduced quality oflife and life expectancy. Oral health-care
providers can make a significant impactby asking every patient about tobacco useand providing applicable tobacco cessationeducational resources. They should beaware of the different types of tobaccoproducts available, such as smoked tobaccoproducts (cigarettes, cigars, and pipe),clove cigarettes known as kreteks, bidis(coarse tobacco rolled in a tree leaf fromSouth Asia), hookah (the smoking of fla-vored tobacco with a form of water-pipe(Waziry et al. 2016)), and smokelesstobacco formulations including snuff, snus(Swedish-style tobacco), and paan/betelquid (areca nut and tobacco wrapped in abetel leaf and chewed), gutkha (an areca nuttobacco mixture sold in single use sachetsand chewed) (Couch et al. 2016). E-ciga-rettes are relatively new handheld nicotinedelivery systems that produce a vaporizedflavored liquid by pressing a button. Thelong-term oral and systemic health risks ofe-cigarettes are currently unknown (Couch
Table 4 Review of systems
General Recent weight change, fatigue, malaise, fever, chills, night sweatsDermatologic Rashes, lumps, ulcers, dryness, pruritus, finger clubbing, nail changesHead Headaches, dizziness, head traumaEyes Changes in vision and visual fields, spots, floaters, diplopia, blurriness, dryness, tearing, itching,Ears Hearing loss, pain, discharge, tinnitus, vertigoNose, sinuses Stuffiness, sneezing, rhinorrhea, itching, epistaxis, changes in sense of smellMouth, throat,neck
Bleeding or painful gums, lesions, dental pain, halitosis, altered taste, hoarseness, sore throat,dysphagia, neck swelling
Respiratory Dyspnea, chest pain, wheezing, cough, sputum, hemoptysisCardiovascular Chest pain, palpitations, orthopnea, dyspnea on exertion, paroxysmal nocturnal dyspnea,
peripheral edemaGastrointestinal Appetite changes, abdominal pain, nausea, vomiting, diarrhea, constipation, heart burn, belching,
bloating, flatulence, dysphagia, bleeding (hematemesis, hemorrhoids, melena, hematochezia),jaundice, ascites
Genitourinary Frequency, hesitancy, urgency, incontinence, nocturia, dysuria, hematuria, abnormal genitaldischarge, genital lesions, changes in libido
Endocrine Polydipsia, polyuria, polyphagia, heat and cold intolerance, weight gain or loss, excessivesweating, thyroid enlargement or pain
Hematologic Anemia, easy bruising or bleeding, lymphadenopathyMusculoskeletal Arthritis, arthralgia, pain, swelling, redness, limitations in range of motion, muscle weakness,
traumaNeurologic Seizures, memory loss, loss of consciousness, paresthesia, anesthesia, muscle weakness, paralysis,Gynecologic Menopause, menstrual changes, dysmenorrheaPsychiatric/emotional
Mood, anxiety, depression, changes in sleep pattern, decreased ability to concentrate
8 C.N. Idahosa and A.R. Kerr

et al. 2016). The risk of oral and pharyngealcancers increases the longer a personsmokes. The use of paan, betel quid andrelated products, which are usually placedin the oral vestibules, increases the risk ofsubmucous fibrosis, a precancerous condi-tion characterized by oral burning and lim-ited mouth opening (Tilakaratne et al.2016). The tobacco history, therefore,should include information on current andpast use, the type of tobacco products, dura-tion and frequency of use, and details aboutcessation attempts, if any. A cumulativecigarette smoking history should bedocumented in pack-years (number of20 cigarette-packs per day multiplied bythe number of years smoked).
(vi) Alcohol use: Alcohol use disorder is com-mon in society and alcohol use can lead tomultiorgan consequences, some of whichcarry significant morbidity and mortality(e.g., liver cirrhosis). Studies have shownan association between the consumption ofalcohol and the risk of oral cancer (Ogden2005). Alcohol potentiates the carcinogeniceffect of tobacco in a synergistic manner,thereby multiplying the risk of oral cancer(Petersen 2009; Reidy et al. 2011). Oralhealth-care providers can and should elicita history of alcohol use, and collect infor-mation about current or past use, types ofalcoholic beverages consumed, currentdrinking patterns (i.e., how many days amonth or week, the time of day when thepatient consumes alcohol), and quantity(number of units of alcohol/week). It isimportant to appreciate the dose equiva-lents for alcoholic beverages [i.e., a 12 oz.beer (5% alcohol) is equivalent to a 5 oz.glass of table wine (12% alcohol) or a1.5 oz. distilled alcoholic drink (40% alco-hol)]. Low risk use is defined as eitherfewer than 3 units of alcohol at a sitting or7 or less units of alcohol/week for women,and either fewer than 4 units at a sitting or14 or less units of alcohol/week for men.Higher rates carry significantly higher ratesfor alcohol use disorder (NIAAA. National
Institute on Alchohol Abuse and Alcohol-ism 2005). It is also important to assess theimpact of alcohol, if any, on the patient’squality of life by finding out if alcohol hasadversely affected their mood, behavior,diet, occupation, and relationships(Table 5), in which case referral to a medi-cal professional may be indicated.
(vii) Illicit drug use: This encompasses the non-medical use of prescription drugs (e.g., opi-oids, barbiturates, and amphetamines) andillicit drugs (such as cocaine and heroin)(Degenhardt and Hall 2012). Marijuana isconsidered an illicit drug in most countries.Enquire about current and past history ofdrug use, the type(s) used, the route ofadministration (i.e., intravenous, inhaled,smoked, or consumed by mouth), and anytreatment for addiction. It is important toconsider prescribing medications withoutincreased potential for addiction to patientswith a history of drug abuse and depen-dence. Also, current use of some illicitdrugs may potentially interact with localanesthesia or medications prescribed byoral physicians (e.g., cocaine).
(viii) Recent travel history: This has becomemore important with respect to recent travelto geographic regions with endemic dis-eases such as tuberculosis, Ebola, leish-maniasis, or Zika virus.
Dental history: The dental history can provideadditional information related to the chief concernthat is valuable in reaching a diagnosis. It is alsoimportant for evaluating the patient’s level of den-tal awareness, motivation, utilization of dentalservices, and risk/susceptibility for dental disease.The following should be documented as part ofthe dental history:
(i) Current dental symptoms: pain, swelling,halitosis, bleeding, mobile, or fracturedteeth
(ii) Last dental visit and reason for seekingdental care: emergency or routine dentalcare
(iii) Frequency of dental visits
Clinical Evaluation of Oral Diseases 9

(iv) Previous dental treatments: recall visits/dental prophylaxis, restorative dentistry,oral surgery, implants, orthodontics, peri-odontics, endodontics, and fixed andremovable prosthodontics
(v) History of maxillofacial trauma(vi) Home care: Brushing and flossing/inter-
proximal habits (i.e., frequency, timing inthe context of meals, and technique). Oralhygiene products such as dentifrices,flosses, and mouthrinses should berecorded as they can sometimes causemucosal reactions
(vii) Oral habits: clenching, bruxism, cheek bit-ing, nail biting
(viii) History of temporomandibular joint (TMJ)pain, clicking or locking, and the use oforthotic devices or night guards
(ix) Exposure to fluoride and type of fluoride(x) Presence of dental phobia and anxiety
Nutritional history: Nutritional factors areassociated with the development and progressionof various oral and systemic diseases. Therefore, itis necessary to evaluate the nutritional and dietaryhabits of patients in relation to their chief concernand presenting symptoms. Oral health-care pro-viders may also play a role in the interception andmanagement of obesity and eating disorders (e.g.,bulimia and anorexia nervosa). The following
points may be considered when taking the nutri-tional history:
(i) Dental caries: There are multiple risk factorsfor dental caries, a number of which aremodifiable, including diet. Therefore, thenutritional history should include informa-tion on frequency of meals and snacks, anda detailed history of the consumption of sug-ared beverages (Marshall 2009)
(ii) Periodontal diseases: Severe vitamin C defi-ciency (i.e., scurvy) is associated with peri-odontal disease.
(iii) Dental erosion: Repeated exposure to acidicbeverages (e.g., carbonated soda and sportsdrinks) can promote the initiation and pro-gression of dental erosion. Patients who suf-fer from eating disorders such as anorexianervosa and bulimia may practice self-induced vomiting leading to dental erosionon the lingual and palatal surfaces of teeth.
(iv) Oral cancer: a diet rich in fruits and vegeta-bles is protective against oral cancer.
(v) Oral mucosal disorders and neuropathies:Vitamin B12 deficiency may occur in strictvegetarians and is associated with glossitisand stomatitis. Chronic undernutrition andother vitamin deficiencies (B2, B6, folicacid) may predispose patients to angular
Table 5 Assessment for alcohol use disorder
In the past year have you?1. Had times when you ended up drinking more, or longer than you intended?2. More than once wanted to cut down or stop drinking, or tried to, but couldn’t?3. Spent a lot of time drinking? Or being sick or getting over the aftereffects?4. Experienced craving, a strong need, or urge, to drink?5. Found that drinking, or being sick from drinking, often interfered with taking care of your home or family? Or causedjob troubles? Or school problems?6. Continued to drink even though it was causing trouble with your family or friends?7. Given up or cut back on activities that were important or interesting to you, or gave you pleasure, in order to drink?8. More than once gotten into situations while or after drinking that increased your chances of getting hurt (such asdriving, swimming, using machinery, walking in a dangerous area, or having unsafe sex)?9. Continued to drink even though it was making you feel depressed or anxious or adding to another health problem? Orafter having had a memory blackout?10. Had to drink much more than you once did to get the effect you want? Or found that your usual number of drinks hadmuch less effect than before?11. Found that when the effects of alcohol were wearing off, you had withdrawal symptoms, such as trouble sleeping,shakiness, irritability, anxiety, depression, restlessness, nausea, or sweating? Or sensed things that were not there?
10 C.N. Idahosa and A.R. Kerr

cheilitis, stomatitis, oral ulcerations, andburning mouth symptoms.
(vi) Major salivary gland enlargement: May beseen in patients with chronic malnutrition.
The Patient Examination
The history is followed by a comprehensivevisual/tactile head and neck examination. Medicalproviders (i.e., primary care physicians) rarelyperform a detailed intraoral examination, whichunderscores the important role of oral health-careproviders in this regard. Yet, the patient examina-tion performed by oral health-care providers goesfar beyond the evaluation of dental and periodon-tal structures. Clinicians should have detailedknowledge of how to evaluate both oral and non-oral structures of the head and neck, and perform acranial nerve examination. An understanding ofnormal anatomy and function facilitates the detec-tion of abnormalities during the examination. Theinterplay between the history and the examinationdeepens as the clinician explores new avenues ofquestioning based upon the detection of suchabnormalities. This section emphasizes the impor-tance of performing a consistent and comprehen-sive examination, a skill that is vastly undervaluedand yet, when performed correctly, can yieldimportant clues to the diagnostic process. Withpractice, this examination should not take longerthan a few minutes on average. Table 1 summa-rizes the steps.
Extraoral examination: This part of theexamination has been broken into eight sections,and requires the patient to loosen/remove anyclothing to allow visualization of the head andneck structures:
(i) General inspection: During the history tak-ing an astute clinician has already begun theexamination process by performing a visualinspection of the patient. Height andweight; dress and personal hygiene; postureand gait; dexterity and body movements;eye movements and facial expression;speech, mood, and cognitive ability; andothers may be gauged over the first few
minutes of the patient encounter. Heightand weight may be combined to assess apatient’s body mass index (BMI), calcu-lated as the weight in kilograms(kg) divided by the height in meters squared(m2).
(ii) Skin/hair: Clinicians should evaluate thehead, face, and neck, or any other visibleareas of skin (i.e., hands, arms, legs, or feet)noting the texture, turgor, color, and obvi-ous asymmetry, growths, or lesions (e.g.,pigmented or ulcerated skin lesions). Fin-gernails and hair distribution should also beevaluated (e.g., hair loss or fingernailpathology such as onychomycosis).
(iii) Eyes: Observe general features such as eyeposition, eyelids, lashes, and structures ofthe eyeball (cornea, sclera, iris, pupils, tearproduction, noting any asymmetry).Assessment of visual acuity and ocularfunction is covered in the cranial nerveassessment.
(iv) Temporomandibular joints (TMJs): TheTMJs may be examined by placing theindex fingers anterior to the tragus of theears and asking the patient to open andclose their jaws (Fig. 2a). This will allowthe clinician to locate the lateral poles of thecondyles, palpate any TMJ swelling orpain, assess the rotation and translation ofthe condyles, and detect joint sounds (i.e.,crepitus, clicks, or pops), or deviations/lim-itations in the normal range of jaw move-ment. Subtle joint sounds may beappreciated more easily by using a stetho-scope. The range of motion is an easilyreproducible measure of jaw movement.The normal range for maximum openingis variable (approximately 40–60 mm) andobtained by precisely measuring theinterincisal distance with a ruler (Fig. 2b)or vernier calipers, or crudely by the num-ber of fingers one is able to insert betweenthe teeth. Three fingers (measuring approx-imately 47 mm) is a reliable surrogate fornormal opening (Zawawi et al. 2003).Observing excursive jaw movements (i.e.,protrusion, or lateral excursions of
Clinical Evaluation of Oral Diseases 11

approximately 7 mm) reveal limitations inrange, allow comparison between sides(i.e., asymmetry), and which movements,if any cause pain or other signs.
(v) Muscles of mastication and other head andneck musculature: There are four mainpairs of masticatory muscles: masseters,temporalis, medial pterygoids, and lateralpterygoids. All are innervated by the man-dibular branch of the trigeminal nerve (V3),and therefore V3 nerve function may beassessed when examining these muscles.The examination of the muscles of masti-cation begins with a visual inspection forany asymmetry or gross enlargement of themasseters and temporalis muscles at rest.Then the patient is asked to clench theirteeth in order to visualize and palpate mus-cle contraction and assess strength, symme-try, and size of the muscles. At a minimum,digital palpation of the masseters andtemporalis muscles should be performed(the predictive value of palpating the pter-ygoids is low) and may reveal muscle ten-derness or pain, or indicate sites of referredpain. It is important to assess each musclein turn using consistent pressure (approxi-mately 1 kg), palpating at multiple points,for approximately 2 s each, along the lengthof the muscles, comparing right to left.Identified painful trigger points may be pal-pated for up to 5 s to appreciate referralpatterns (Schiffman et al. 2014). The use
of an algometer may assist in providingconsistent pressure. The anterior (Fig. 3a)and more posteriorly the middle and poste-rior aspects of the temporalis muscles maybe examined in turn, followed by the mas-seter muscles (Fig. 3b). The tendon of thetemporalis at the coronoid process of themandible may be palpated intraorally. Askpatients to provide a rating of any tender-ness or pain (0 for no tenderness, 1 foruncomfortable tenderness, 2 for definitetenderness or pain, or 3 for significantpain that causes the patient to pull away toavoid further pain). The lateral and medialpterygoids are difficult to reliably palpatebut may be assessed functionally. Painelicited when protruding the jaw with resis-tance from the examiner may indicate theinferior lateral pterygoid muscles as a pos-sible source. The power stroke of bitingdown on an object may result in pain fromthe superior lateral pterygoid muscles.Neck muscles, such as the sternocleido-mastoids, posterior cervical muscles (i.e.,trapezius, longissimus (capitis andcervicis), splenius (capitis and cervicis),and levator scapulae), and strap musclesof the neck may be similarly palpated andalso evaluated for range of motion by turn-ing the head all the way to the left, then tothe right, then lifting the chin up, and thentilting the head left and right.
Fig. 2 (a) Location of lateral pole of right TMJ. (b) Measurement of interincisal opening
12 C.N. Idahosa and A.R. Kerr

(vi) Salivary glands: There are three pairedmajor salivary glands (parotid, submandib-ular, and sublingual glands) along withgreater than 300 minor salivary glands dis-tributed throughout the mouth. Assessmentbegins with a visual inspection of theparotid and submandibular glands forswelling or asymmetry. There are a numberof chronic disease processes (e.g., diabetesor liver disease) that can manifest withbilateral salivary gland enlargement. Inhealth, palpation of the salivary glandswill reveal a soft consistency withouttenderness.
(vii) Midline neck structures (trachea and thy-roid gland): Examination of the trachea iswarranted to rule-out displacement orchange in axial mobility, possibly due tothe encroachment of neck neoplasms. Thetrachea extends inferiorly from the larynx,and half of the trachea is within the neck.Tracheal displacement from its midlineposition may be verified by both inspectionand palpation of the trachea in relation tothe suprasternal notch. By gently graspingthe tracheal rings, the trachea can be movedlaterally and a grating is appreciatedbecause of the movement of the cartilagi-nous rings. Equal movement and grating isa normal finding. The thyroid is a bilobedgland found in the midline of the lowerneck. The lobes are joined by an isthmus,
which crosses in front of the trachea inferiorto the level of the cricoid cartilage. Thelobes extend laterally with the most lateralaspects of the gland found deep to thesternocleidomastoid muscles (Fig. 4a).The first step to examining the thyroid isthe inspection (both from in front and fromthe side of the patient) for any obviousasymmetry or swelling (e.g., a goiter orthyroid neoplasm). Since the thyroid glandmoves with the trachea during swallowing,the patient can be asked to swallow a sip ofwater, facilitating visualization as the thy-roid tissue moves superiorly. This isfollowed by palpation, performed eitherfrom behind (i.e., the posterior approach)or in front of the patient to detect any dis-crete nodules within the gland or its associ-ated lymph nodes. The prominence of thethyroid cartilage (Adam’s apple) is an easyfirst landmark to detect manually. The nextring inferior is the cricoid cartilage, and justinferior to this is the location of the isthmus.Pushing the sternocleidomastoid muscleslaterally and posteriorly, it is possible topalpate the lobes in turn by applying lightpressure, comparing the right and left sidesfor asymmetry (Fig. 4b).
(viii) Lymph nodes: An understanding of thelymphatic drainage of the head and neck isa prerequisite for this step of the extraoralexamination. There is a collar of lymph
Fig. 3 (a) Palpation of right anterior temporalis muscle. (b) Palpation of right masseter muscle
Clinical Evaluation of Oral Diseases 13

nodes of the head that drain into the deeperneck lymph nodes, which ultimately draininto the thorax (Fig. 5a, b). The head andneck lymph node system is divided intolevels (I–VI) from superior to inferior.Superficially located lymph nodes are pal-pable in health, and they are soft, moveable,and nontender. Deeper nodes may becomepalpable when enlarged (lymphadenopa-thy). Most commonly, lymphadenopathyis due to an inflammatory etiology (e.g.,an odontogenic infection) and involvedlymph nodes become enlarged and tender,although they typically remain soft andmoveable. Lymphadenopathy can occur inassociation with cancer metastasis (e.g.,squamous cell carcinoma) and are typicallyenlarged, firm to palpation, nontender and,if there is extracapsular spread, they maybecome nonmovable or fixed. Level I nodesare detected in the submandibular and sub-mental triangles of the neck. Level II, III,and IV lymph nodes may be detectedwithin the anterior triangle of the neck,and level V nodes in the posterior triangleof the neck. Level VI nodes are found
below the hyoid bone in the anterior centralaspect of the neck. Following the examina-tion of the thyroid gland, it makes sense tobegin the lymph node examination in theanterior triangle, then move into the poste-rior triangle, and end with the submandib-ular and submental triangles. Theboundaries of the anterior triangle of theneck are the midline of the neck anteriorly,the sternocleidomastoid muscle posteriorly,and the inferior border of the mandiblesuperiorly (Fig. 6a). The level II, III, andIV deep lateral cervical nodes follow thepath of the internal jugular vein deep tothe sternocleidomastoid muscle. Look forthe outline of the sternocleidomastoid mus-cles, and asking the patient to lift and turntheir head away from the side being exam-ined is often helpful to identify this muscle.With the neck relaxed, it is possible to pal-pate anterior and deep to the muscle fromsuperior to inferior, and compare findingsfrom both sides (Fig. 6b). The boundariesof the posterior triangle are the sternoclei-domastoid muscle anteriorly, the trapeziusmuscle posteriorly, and the clavicle
Fig. 4 (a) Position of the thyroid gland and it’s isthmus i) in relation to thyroid cartilage (tc), cricoid cartilage (cc), andsternocleidomastoid muscle (scm). (b) Palpation of the thyroid gland
14 C.N. Idahosa and A.R. Kerr

inferiorly (Fig. 7a). Palpate along the pos-terior border of the sternocleidomastoidmuscle from the supraclavicular nodes infe-riorly to the postauricular and occipitalnodes superiorly (Fig. 7b). The submandib-ular and submental triangles comprise themost superior aspect of the anterior triangleof the neck and contain level I nodes whichreceive drainage from most oral structures(Fig. 8a). Submandibular nodes are gener-ally superficial and therefore palpable inhealth, allowing the examiner to feel thecharacteristics of healthy nodes. Have thepatient lower their chin and then gently pull
the soft tissues laterally across the inferiorborder of the mandible (Fig. 8b). In thisway, it is possible to “capture” the nodebetween the examiner’s finger and the infe-rior border, and then feel the node “pop”back into place. Similarly, submental nodesmay be palpated by moving the submentalsoft tissues anteriorly (Fig. 8c). Lymphnodes draining facial structures, such asthe preauricular and buccal nodes mayalso be palpated.
Intraoral examination: This part of the exam-ination is rarely performed in a comprehensive
Fig. 5 (a) Collar of lymphnodes draining head andface. (b) Descendingsystem of lymph nodes
Clinical Evaluation of Oral Diseases 15

manner by health-care providers outside of den-tistry, and as such, it is critical to perform it whenthe opportunity arises, certainly for all newpatients, for all recall visits, and during emer-gency/urgent care visits regardless of the type ofemergency/urgency. Patients should be informedthat they are receiving an oral examination todetect not only dental and periodontal problems,but also to detect mucosal and other abnormali-ties, such as the rare instance of oral cancer. Theconcept of self-examination may also be broachedwith the patient, along with instructions of thesteps they can perform at home. This exam isboth visual and tactile (i.e., with palpation), andpatients should be asked to remove removabledental appliances, and to rinse out food particles.Develop a consistent examination sequence, theorder of which is not that important, as long as allelements are completed. An adequate light sourceis critical to the intraoral examination. A standardoverhead halogen dental light or, preferably, a
portable light-emitting diode (LED) white head-light affixed to loupes in order to keep both handsfree. Other adjuncts include an air syringe, mouthmirrors, and gauze.
(i) Lips: The lips’ vermillion border with theskin is normally sharply demarcated andhomogenous in color and texture. Inspectand bimanually palpate the lip for surfacechanges or color irregularities (Fig. 9a).
(ii) Labial mucosae: Reflect the lips to visualizethe labial vestibule, and inspect/palpate forany surface or submucosal abnormalities(Fig. 9b–d).
(iii) Gingivae: Inspect and palpate all gingivalstructures. Healthy gingivae should bepink, stippled, nonedematous, and haveknife-edged interdental papillae (Fig. 9e).
(iv) Buccal mucosae: Retract this tissue digi-tally or with a mouth mirror to inspect/pal-pate all aspects of the buccal mucosae,
Fig. 6 (a) Boundaries ofthe anterior triangle of theneck. (b) Palpation of thedeep cervical nodes
16 C.N. Idahosa and A.R. Kerr

including the posterior aspects of the buccalvestibules. Palpate the parotid extraorallyto evaluate salivary flow through theStenson’s duct orifice (Fig. 9f).
(v) Tongue: The tongue is divided into the“oral tongue” (the anterior 2/3rd) and thebase of tongue (the posterior 1/3rd). Theoral tongue is comprised of the dorsal, lat-eral, and ventral surfaces, which are ame-nable to inspection and palpation. A pieceof gauze may be wrapped around thetongue to allow access to the posterioraspects of the dorsum and posterolateralborder of the tongue where the foliate papil-lae and lymphoid tissues may be inspected/palpated and compared bilaterally(Fig. 9g–i). The dorsal tongue harbors a
number of specialized papillae, namely arow of round pink mildly elevated circum-vallate papillae dotted in a V-distribution atthe posterior border of the oral tongue;small red fungiform papillae distributedthroughout the dorsal surface (and oftenconcentrated at the tip of the tongue); andmost commonly the tiny fingerlikekeratinized filiform papillae. The foliate,circumvallate and fungiform papillaehouse taste buds. The ventral tongue has athin mucosal lining contiguous with thefloor of mouth, contains a midline frenum,plica frimbriata lateral to the frenum, andone may observe the deep lingual veins(Fig. 9j). The posterior 1/3rd of the tongueis more difficult to visualize directly;
Fig. 7 (a) Boundaries ofthe posterior triangle of theneck. (b) Palpation of theposterior triangle
Clinical Evaluation of Oral Diseases 17

however, it should be palpated and/or visu-alized indirectly by mirror or endoscopygag reflex permitting (Fig. 9n, o).
(vi) Floor of mouth: Since abnormal surfacechanges may be subtle, air-drying thisregion facilitates examination. The sublin-gual caruncles or sublingual papillae aretwo small round structures found eitherside of the frenum, and these houseWharton’s duct openings. Fanning out lat-erally from these papillae are elevated sub-lingual folds containing the openings fromthe sublingual glands (Fig. 9k). Bimanualpalpation of the floor of mouth should beperformed by gently moving two opposingfingers, one extraorally and the otherintraorally, from posterior to anterior, softlypalpating the interposing soft tissue(Fig. 9p).
(vii) Hard palate: Inspection and palpation of thehard palate is important. Small mucosalswellings are easy to miss when the exam-iner relies on inspection alone (Fig. 9l).
(viii) Oropharynx: The oropharynx comprisesthe soft palate, the uvula, anterior and pos-terior pillars (or fauces), the posterior pha-ryngeal wall, the palatine tonsils, and baseof tongue (Fig. 9m). These structures, alongwith the nasopharyngeal and lingual tonsilscomprise Waldeyer’s ring, part of themucosal immune system. A tongue bladeor mouth mirror may be used to depress thetongue. This is the opportunity to assesscranial nerves IX and X by provoking agag reflex and having the patient say“aahh” and watch the even elevation ofthe soft palate. The retromolar trigone isthe area distal to the mandibular retromolarpad and this should be part of the examina-tion. The palatine tonsils sit in the tonsillarfossae between the pillars. It is important torecord their presence (many patients havehad them surgically removed), color, andsymmetry. The base of tongue contains thelingual tonsils.
Fig. 8 (a) Boundaries of submandibular/submental triangles. (b) Palpation of the superficial submandibular lymphnodes. (c) Palpation of the submental nodes
18 C.N. Idahosa and A.R. Kerr

Fig. 9 Soft Tissue Examination: (a) Lips, (b) Lower labialmucosa/vestibule, (c) Palpation of lower lip, (d) Upperlabial mucosa/vestibule, (e) Gingivae, (f) Buccal mucosa,(g) Dorsal tongue, (h) Lateral border of tongue, (i) Pos-terolateral tongue showing foliate papillae/lymphoid
tissue, (j) Ventral surface of tongue, (k) Floor of mouth,(l) Palpation of hard palate, (m) Oropharynx, (n) Indirectinspection of base of tongue, (o) Palpation of base oftongue, (p) Bimanual palpation of the floor of mouth
Clinical Evaluation of Oral Diseases 19

(ix) Dentition: A detailed description of theexamination of the teeth and supportingstructures to detect common dental diseases(i.e., caries and periodontal disease) isbeyond the scope of this book. However,the state of the dentition can provideinsights about the overall health of thepatient, and a careful examination of thedentition to detect dental abnormalitiesbeyond caries, periodontitis, odontogenicinfections, and occlusal/jaw discrepancies(i.e., that might typically be managed ortho-dontically) is warranted. Examples are den-tal erosion, disorders of enamel or dentinformation, intrinsic or extrinsic discolor-ation (e.g., secondary to tetracycline use).Deviations from the normal tooth number,shape, color, eruption patterns, and occlu-sion offer the initial clues. The involvementmay be restricted to a single tooth, multipleteeth, or be generalized to the entire denti-tion. These clues provide the basis for fur-ther probing of the patient’s history,including family history (e.g., where ahereditary disease, such as amelogenesisimperfecta, might be suspected). The clini-cal examination may need to besupplemented with radiographs (or otherdiagnostic testing) to further characterizethe abnormalities. Clinicians should alsoassess the relationship of teeth to the sur-rounding mucosae. Broken and sharp teeth,restorations, or dentures can lead to fric-tional keratosis or traumatic ulcers. Largeamalgam restorations can cause locallichenoid reactions of the adjacent mucosa.
(x) Saliva: Salivary gland function may becrudely assessed by identifying the glandopenings intraorally (Stenson’s ducts fromthe parotid glands open on the buccalmucosae near the maxillary 2nd molar,and Wharton’s ducts emanate from the sub-lingual caruncles in the floor of mouth), andthen “milking” each gland and observingsaliva secretion. The presence, consistency/viscosity (normal viscosity versus thick/stringy, or bubbly), and color of the saliva(clear versus turbid) may be recorded,
although a reduction or absence of salivamay not necessarily be associated with truesalivary gland hypofunction (e.g., dehydra-tion). Other signs of normal salivary flowmay include a glistening of mucosal sur-faces commensurate with adequate salivaand the presence of salivary pooling in thefloor of the mouth. Clinicians should alsolook for signs of salivary dysfunction (seechapter on Salivary Gland Disorders andDiseases).
The gold standard for the assessment ofnormal salivary gland function is bysialometry, measuring the quantity andquality of saliva generated by the glandsin both the basal (unstimulated) state andduring stimulation, either by measuring thecollective secretions from all the glands(i.e., whole saliva) or by measuring salivafrom each gland individually. Ideally,sialometry should be performed during amorning appointment with the patientinstructed not to eat or drink (except wateras needed) for 90 min before the appoint-ment. With the patient in a relaxed state andin a quiet environment, the procedures ofsaliva collection should be clearlyexplained to the patient. Sitting in anupright position, the patient should beinstructed to swallow their saliva, tilt theirhead forward, and place a preweighedcollecting tube next to their mouth(Navazesh et al. 2008). Setting the timerfor 5 min or more, they should allow salivato drool out of their mouth into the tube. Atthe end of the time, they should expectorateall residual saliva into the tube. The tubeshould be weighed to calculate the weightof saliva and the value divided by the num-ber of minutes collected to generate a flowrate. One gram is equivalent to 1 mL ofsaliva and mean normal unstimulated flowrates are 0.3–0.4 mL/min. Stimulated sali-vary flow rates are performed if a patienthas an abnormally low unstimulated flowrate (i.e., <0.2 mL/min) and may be mea-sured by a number of techniques includingasking the patient to chew a flavorless gum
20 C.N. Idahosa and A.R. Kerr

base, paraffin wax, or a sugarless lemondrop for 5 min, expectorating every 30 sduring collection. The mean normal stimu-lated flow rate is 1–2 ml/min. In patientssuspected to have dental erosion, salivarypH and buffering capacity can also beundertaken using commercially availablekits (e.g., GC Saliva Check, GC Corpora-tion, Japan).
Sialometry to measure individual glandsecretions, to detect salivary pH, bufferingcapacity, and composition is also possible,although not routinely performed outside ofa research setting.
(xi) Screening adjunctive techniques: These aredefined as techniques that are applied topatients during an examination to provideadditional information about the patient ora specific abnormality detected (e.g., theuse of light-based visualization techniquessuch as tissue autofluorescence devices toscreen for malignant and potentially malig-nant disorders). This is covered in moredetail in the chapter on Oral MucosalMalignancies.
Cranial nerve examination: There are 12 cra-nial nerves (CN), although routine assessment ofevery cranial nerve is not typically indicated. Oralhealth-care providers will routinely test cranialnerves V, VII, IX, X, and XII during a routineexamination. The others may be tested when thereis an indication.
(i) Olfactory nerve (CN I): The sense of smellmay be tested using familiar inoffensiveodors, such as soap. First assess the patencyof each nasal passage by asking the patientto occlude one side and then breath throughthe open passage of the other side. If bothare patent, ask the patient to close theireyes, occlude one nostril at a time andsniff the smell of the selected substance.Ask them to name the substance and testboth sides.
(ii) Optic nerve (CN II): Visual acuity may betested using a Snellen chart. Patients arepositioned 20 feet from the chart
(alternatively, a miniature hand chart maybe used) and asked to cover one eye andthen read the smallest line of print possible.Visual acuity is expressed as two numbers(e.g., 20/40). The first is the distance fromthe patient to the chart, and the second is thedistance at which the patient’s eye can readthe line of the smallest numbers. Visualfields may also be assessed via confronta-tion testing, usually by the static fingerwiggle test and the kinetic red target test.Pupillary reactions are mediated by CNs IIand III (see below).
(iii) Oculomotor nerve (CN III): The pupillaryreflex (also mediated by CN II) may beassessed through two reactions: the lightreaction and the near reaction. The lightreaction is assessed by shining a light intoone eye which should lead to pupillary con-striction in both eyes (the light is sensed bythe retina, which stimulates the optic nerve,and then impulses are sent from the brainback via CN III to cause the pupil to con-strict (i.e., iris muscle dilation). The nearreaction is when the patient is asked tofocus their gaze on an object, such as afinger placed equidistant from both eyes,that is brought closer and leads to pupillaryconstriction (i.e., accommodation). CN IIIalso provides motor innervation to most ofthe extraocular muscles (i.e., all except thelateral rectus and superior oblique mus-cles), along with the levator palpebraesuperioris muscles (to elevate the uppereyelid).
(iv) Trochlear nerve (CN IV): This nerve pro-vides motor innervation to the superioroblique muscle and is assessed along withCNs III and VI by instructing the patient tofollow the six extraocular movements (i.e.,an “H” shape made by a finger or pencil):all the way to one side, then up and down,then all the way to the other side, then upand down.
(v) Trigeminal nerve (CN V): This nerve hasthree divisions, two of which are sensory(V1: ophthalmic and V2: maxillary) andone which is both sensory and motor (V3:
Clinical Evaluation of Oral Diseases 21

mandibular). The sensory nerves may beassessed by having the patient close theireyes and then lightly touching the facialskin distribution, on both sides, of thethree sensory branches. Then, perform thesame steps with a pin or sharp object. Askthe patient to tell you where they feel thesensation, and the type of sensation (softtouch or sharp prick), comparing sides.The corneal reflex (V1) may be assessedby touching the cornea with a wisp of cot-ton and observing a blink. Motor branchesto the muscles of mastication may beassessed by asking the patient to clenchtheir jaws and observing bilateral contrac-tion of the masseters and temporalis mus-cles. The patient’s ability to performsymmetric jaw movements (opening, clos-ing, lateral, and protrusive jaw movements)may be assessed too.
(vi) Abducens nerve (CN VI): This nerve pro-vides motor innervation to the lateral rectusocular muscle, and assessment is similar tothat of CNs II and IV.
(vii) Facial nerve (CN VII): This nerve providesmotor innervation to the muscles of facialexpression and also carries taste and othersensory neurons. The motor portion may beassessed by asking patients to perform anumber of facial grimaces, such as wrin-kling their forehead (contracting thefrontalis muscles), tightly contracting theeyelids (orbicularis oculi), or smiling andshowing the teeth (orbicularis oris). Lookfor symmetry.
(viii) Vestibulocochlear nerve (CN VIII): Audi-tory acuity may be simply assessed by thewhispered voice test. Standing behind thepatient so they cannot see the lips of theexaminer, simultaneously occlude the non-test ear and gently rub its external meatus,then exhale completely and then whisperthree random numbers from 6 inchesaway. Ask the patient to repeat the numbersand repeat on the other ear. For patientswho fail this test, a tuning fork may beused to assess neurosensory and conductivehearing loss (i.e., the Rinne test for air and
bone conduction, and the Weber test forlateralization). Assessment of the vestibularsystem is rarely performed as part of theroutine cranial nerve examination.
(ix) Glossopharyngeal nerve (CN IX): Visceralfunctions aside, this nerve provides motorinnervation to the stylopharyngeus musclewhich helps elevate the pharynx and lar-ynx, and provides sensation to the posteriororal cavity including taste sensation fromthe posterior third of the tongue. It is usu-ally assessed by testing the gag reflex, byplacing a tongue depressor onto the poste-rior aspect of the tongue; however, absenceof a gag reflex does not assure aglossopharyngeal nerve palsy.
(x) Vagus nerve (CN X): The vagus providesmotor innervation to other pharyngeal andlaryngeal muscles, along with fibers to theheart, thoracic, and abdominal viscera. Itmay be assessed in conjunction with CNIX by asking the patient to say “ah” andwatching the symmetric elevation of thesoft palate and uvula.
(xi) Spinal accessory nerve (CN XI): This is amotor nerve to the sternocleidomastoid(SCM) and trapezius muscles. The SCMsmay be assessed asking the patient to turntheir head against the force of your hand,and the trapezius muscles may be assessedby the shrugging the shoulders againstforce. Look for symmetrical strength.
(xii) Hypoglossal nerve (CN XII): This nerveprovides motor innervation to the intrinsicand extrinsic tongue muscles. Look forsymmetry at rest and then ask the patientto protrude their tongue. Fasciculation ofthe tongue or deviation may indicate anipsilateral CN XII palsy.
Vital signs: Oral health-care providers shouldbe able to perform vital signs on all patients; thisincludes blood pressure, heart rate and rhythm,respiration, temperature, and others.
(i) Blood pressure: Blood pressure is typicallymeasured chairside using a sphygmoma-nometer and stethoscope and is technique
22 C.N. Idahosa and A.R. Kerr

sensitive. Either arm may be selected (unlessone arm has an A-V shunt for dialysis, or haslymphedema secondary to a breast mastec-tomy), but the arm should be free of anyclothing. The brachial artery should be pal-pated for a pulse (Fig. 10a) and the arm liftedso that the antecubital crease is at heartheight, then the inflatable cuff is centeredover the artery, positioned above the crease.Inflate the cuff until the radial pulse is elim-inated and check the blood pressure reading.Deflate the cuff, place the bell-side of thestethoscope over the brachial artery, andreinflate to a pressure 30 mg Hg above theprevious inflation value, and slowly deflatethe cuff listening for two sets of sounds(Fig. 10b): the pressure at which the soundsare initially heard is the systolic pressure,and the pressure when the sounds arecompletely lost is the diastolic pressure.Blood pressure is calculated from the aver-age of two readings (one on each arm).A threshold blood pressure reading of!90 mg Hg diastolic in an adult aged30–59 years or readings of either !150 mgHg systolic or!90 mg Hg diastolic in adults>60 years is indicative of hypertension and astrong recommendation for initiation of
pharmacotherapy (Grade A evidence)(James et al. 2014). There are a number ofscenarios leading to false positive (e.g.,white coat hypertension, or recent coffeeintake) or false negative (e.g., orthostatichypotension) blood pressures in a clinicalsetting. Serial ambulatory or home bloodpressure testing will provide more predict-able readings. Blood pressure readings inexcess of !180 mg Hg systolic or!110 mg Hg diastolic are suggestive of ahypertensive urgency, regardless of the pres-ence of associated signs and symptoms suchas headache, nosebleeds, severe anxiety, orshortness of breath. Such patients require amore detailed examination to rule out under-lying systemic diseases (e.g., renal disease).
(ii) Heart rate and rhythm: The radial artery istypically chosen to assess this, and the clini-cian should place the pads of both the middleand index fingers just proximal to the wristwith sufficient pressure to detect the pulse(Fig. 10c). Assess the rhythm first, and ifregular, count the pulse for 30 s thenmultiplythe value by 2. The normal range is 50–90beats/min and if the rate is abnormally high(tachycardia) or low (bradycardia), measureagain for a full 60 s. If the rhythm is irregular,
Fig. 10 (a) Palpation to identify brachial artery. (b) Placement of cuff and bell of stethoscope. (c) Palpation to identifyradial artery
Clinical Evaluation of Oral Diseases 23
attempt to detect a pattern. Irregular rhythm,tachycardia, or bradycardia typically willindicate further cardiac testing (e.g., electro-cardiography) to identify the underlyingetiology.
(iii) Respiration: The rate, rhythm, and depth ofbreathing may be observed over a 60-speriod. A regular rhythm of approximately20 breaths is normal.
(iv) Temperature: An average normal oral tem-perature is 37 "C (98.6 "F), yet it can fluctu-ate to as low as 35.8 "C (96.4 "F) in the earlymorning or to as high as 37.3 "C (99.1 "F) inthe evening. The oral temperature isperformed preferably by an electronic ther-mometer with the tip placed under the tongueand with the lips closed.
(v) Other vital signs: Pain assessment is consid-ered a vital sign in most medical settings.There are a number of validated pain assess-ment tools available (see the chapter on clin-ical evaluation of orofacial pain). Pulseoximetry is also considered a vital sign. It isa surrogate measure for arterial blood oxy-gen saturation and normal values are >90%.
Imaging
Imaging studies, discussed in greater detail in thechapter on Diagnostic Imaging Principles andApplications in Head and Neck Pathology, areimportant diagnostic tools. In addition to radio-graphic and other imaging modalities (i.e., mag-netic resonance imaging (MRI)), this section willinclude digital photography and videography.Because most radiographs utilized by oralhealth-care providers carry the risk of radiationexposure, they should be carefully selected (Far-man 2005). The choice of an imaging modalityshould therefore be based upon its ability to con-tribute to diagnosis and management and not onits availability. In addition to dental disease, radio-graphs should be ordered to visualize the boneunderlying soft tissue lesions, for intraosseouspathology, trauma and suspected fractures, sali-vary gland disorders, TMJ pain, and dysfunctionand to rule out intracranial lesions in specific
patients. It is important for radiographs to showthe full extent of all lesions captured. Key findingsthat should be put into consideration wheninterpreting jaw lesions include: location, numberof lesions, shape, border characteristics, dimen-sion, internal structure, cortical expansion, andeffect on adjacent structures/teeth. Imagingmodalities utilized in the head and neck regioninclude the following:
Photography and videography in oral medi-cine: The documentation of examination abnor-malities, typically by digital photography, serves anumber of important functions. Firstly, imagesserve as a baseline record of the initial presenta-tion of an abnormality that may be used for diag-nosis, to communicate with colleagues who arepart of the patient’s care, as part of a scientificpublication, or for the purpose of comparison overa number of follow-up visits (e.g., to gaugeresponse to treatment). Secondly, images can beused for patient education and may be sent topatients for their own records. Thirdly, imagesserve as part of the patient’s record. They “speaka thousand words” and can be useful from a med-icolegal standpoint. Videography may also beuseful to convey abnormal examination findings,such as a cranial nerve palsy or recording a pro-cedure. There is a dizzying array of digital camerasystems available to clinicians that range in costand image output. Smart phones have becomepopular in medical photography for their simplic-ity, good image resolution, and ease of sharingimages. Sophisticated digital cameras with macro-lenses and ring flash systems are expensive,although they produce images suitable for publi-cation quality, with excellent resolution and theability to capture focused images of intraoralabnormalities with variable depth of field. Beforetaking images, the patient should provide writtenconsent that covers all issues related to patientprivacy, although these requirements may varydepending on local regulations. Patient positioningand the use of oral retractors will greatly facilitatethe capture of quality images. The storage ofimages is also an important issue. If an electronichealth record is being used, images should beuploaded as part of the patient’s record. If this isnot feasible, images should be labeled with the
24 C.N. Idahosa and A.R. Kerr

date, and patient’s name and chart number on anencrypted computer or other storage device.
Plain films: Traditional dental radiographsinclude bitewings, periapicals, occlusal, and pan-oramic radiographs. Bitewing radiographs areparticularly useful for visualizing interproximalcaries. Intraoral periapical radiographs are usefulfor imaging the dentition and supporting struc-tures while occlusal radiographs of the maxillaandmandible are utilized for visualizing the palateand floor of the mouth, respectively. Panoramicradiographs are useful for gross evaluation ofintraosseous lesions of the maxilla and mandibleand the TMJ. Other maxillofacial radiographsmay also be prescribed depending on the specificneeds of the patient such as the occipitomental(Waters) skull projection used for visualizationof the maxillary sinuses.
Computed tomography (CT): CTs are asso-ciated with a higher radiation dose compared withplain films but provide better anatomic details ofthe hard tissues. With the utilization of contrastmedia, soft tissue structures can also be visual-ized. In the maxillofacial region, they are usefulfor evaluating the extent of maxillary and man-dibular cysts and tumors, salivary gland pathol-ogy, fascial space infections of the head and neck,and cervical lymph node involvement in head andneck cancer patients. Cone beam CT (CBCT) pro-vides reduced radiation exposure compared withCT and is the imaging modality of choice forvisualizing hard tissue structures when a limitedfield of the head and neck is to be evaluated.
Magnetic resonance imaging (MRI):Although expensive, MRIs have no associatedradiation exposure and are excellent for visualiza-tion of soft tissues. In the maxillofacial region,they are indicated for evaluation of the articulardisc and other soft tissue components of the TMJ,neoplasms, and salivary glands and to rule-outintracranial lesions in specific subsets of orofacialpain patients such as those presenting with cranialnerve abnormalities or trigeminal neuralgia.
Other imaging modalities utilized in the max-illofacial region include ultrasonography andsialography for evaluation of salivary glands as
well as positron emission tomography (PET) uti-lized for detection and monitoring ofmalignancies.
Diagnosis
Abnormal findings: Abnormal clinical features(i.e., symptoms and signs) should be accuratelydescribed and recorded. This disciplined processof accurately describing clinical features willgreatly facilitate the diagnostic process andallow effective communication of findings withcolleagues. It is helpful to develop a vocabulary ofdescriptors for the myriad of signs and symptomspatients may present with. As an example, orallesions may be described by symptoms such as thesensation of a surface change or a growth, pain,fever, malaise, burning, sensitivity to acidic orspicy foods or beverages, taste changes, numb-ness, oral dryness, inability to chew, tooth mobil-ity, bleeding, and others. Signs such as color,shape, number, location/distribution, symmetry,surface topographical features, margin definition,size, and tactile consistency of oral soft tissuelesions as well as the presence or absence ofregional lymph nodes should be recorded.Table 6 provides a list of physical descriptorscommonly applied to oral mucosal lesions. Simi-larly, for bone diseases/jaw lesions, the followingnonradiographic features should be described andnoted: asymmetry/bony expansion, palpation ofcortex (bony hard, soft, egg shell), presence ofbruit, tooth mobility, and displacement. Radio-graphic features include: size; number, both singleversus multifocal and localized versus general-ized; position in the jaws; characteristics of lesionborder/periphery such as well-defined versuspoorly defined, punched-out, corticated, sclerotic;shape (e.g., circular, scalloped); internal structuressuch as radiolucent, radio-opaque, mixedradiolucent/radio-opaque, multilocular with orwithout septae; and changes in trabecular patternsor the presence of dystrophic calcifications andtooth-like structures.
Clinical Evaluation of Oral Diseases 25

Categories/classification systems of oral dis-eases: Oral and maxillofacial diseases encompassa wide variety of disorders with different etiolo-gies and pathogenesis. It is always a challenge toadequately fit diseases into classification systems,and overlap is inevitable. Oral and maxillofacialdiseases are initially grouped by their primaryclinical features, such as soft tissue versus hardtissue/bone diseases, orofacial pain, temporoman-dibular disorders, salivary gland dysfunction(hypofunction versus sialorrhea), neurosensorydisorders (halitosis, taste changes, dysesthesias),movement disorders, dental anomalies, and sub-sequently each group branches into classificationtrees based on a myriad of different features.
As an example, the group of soft tissue dis-eases may be classified based on underlying dis-ease process (Table 7), clinical appearance
(Table 8), location (Table 9), or clinical behavior(Table 10). These classification systems can facil-itate the process of narrowing down a list of pos-sible diseases while formulating a differentialdiagnosis. Hard tissue diseases/jaw lesions aretypically classified by their radiographic features,such as radiolucent (Table 11) versus radio-opaque or mixed lesions (Table 12).
Differential diagnosis: Effective managementof patients with oral and maxillofacial diseaseshinges on the ability of the oral health-care pro-vider to arrive at an accurate diagnosis. For somediseases, a clinical diagnosis that can be madebased on the pathognomonic appearance of alesion (e.g., fluid-filled vesicles of recurrent her-pes labialis) is equivalent to the definitive diagno-sis. However, other diagnoses are more elusive,and the clinician may not be able to single out a
Table 6 Descriptive terminology for oral lesions
Term Definition
Abscess Localized collection of purulent exudateAtrophy Loss of tissue resulting in thinning of the epithelium and usually associated with erythemaBulla Fluid filled elevated lesion >5 mm in diameterEcchymosis Red/purple macular area of submucosal hemorrhage/extravasated bloodEndophytic A lesion that is growing inwards into the underlying tissueErosion Partial loss of the surface epithelium not extending through the full thicknessErythema Redness of the mucosa usually caused by inflammation, atrophy of capillary dilatationExophytic A lesion that grows outwards from the surface epitheliumFissure Linear slit or groove in the skin or mucosaFistula Abnormal tract connecting two body cavitiesFixed A lesion that is firmly attached to the overlying or underlying structuresHematoma A localized swelling filled with bloodIndurated Hardening of soft tissue usually due to chronic inflammation or malignancyMacule Circumscribed discolored flat lesion not raised above level of surrounding mucosaMobile A lesion that is freely movable and not attached to the overlying or underlying structuresNodule Circumscribed elevated solid lesion >5 mm in diameterPapillary A lesion that has numerous surface projectionsPapule Circumscribed elevated solid lesion <5 mm in diameterPedunculated Exophytic lesion attached to the underlying tissue by a stalkPetechiae Pin-point red or purple spots caused by submucosal hemorrhagePlaque Slightly elevated area of mucosa with a flat surfacePustule Circumscribed raised lesion containing pusReticular Resembling a netSessile Exophytic lesion attached to the underlying tissue by a broad baseUlcer Break in continuity of the oral mucosa due to loss of full thickness of oral epithelium resulting in
exposure of underlying connective tissue which is usually coated by a white or yellow membraneVerrucous An exophytic lesion with rough wartlike projectionsVesicle Fluid filled elevated lesion <5 mm in diameter
26 C.N. Idahosa and A.R. Kerr

diagnosis, but is able to generate a “shortlist” ofpossible diagnoses, known as the differentialdiagnosis. This list of possible diagnoses isbased on the patient’s history and physical exam-ination findings and is ranked in order from mostlikely to least likely. The diagnosis placed at thetop of a differential list is known as the workingdiagnosis. For novices, the initial differentialdiagnosis may be fairly broad in scope
incorporating many different entities. In contrast,the experienced master clinician may have onlytwo or three entities listed. Thorough knowledgeof human anatomy, pathophysiology, and clinicalbehavior of oral and maxillofacial diseases is crit-ical to ascertaining the correct diagnosis whileavoiding dangerous medical errors. Figures 11,12, 13, 14, and 15 outline differential diagnosis
Table 7 Differential diagnosis of oral mucosal diseases based on etiology
Infectious diseases Candidosis, herpes simplex virus infection, varicella zoster virus infection,coxsackie virus infections measles, oral hairy leukoplakia, tuberculosis,syphilis, human papillomavirus associated oral lesions, infectiousmononucleosis
Allergic, immune-mediated, andautoimmune diseases
Pemphigus vulgaris, mucous membrane pemphigoid, linear IgA disease,aphthous stomatitis, Behçet syndrome, erythema multiforme, oral lichenplanus, lupus erythematosus, graft-versus-host disease, orofacialgranulomatosis
Malignant and potentially malignantdisorders
Actinic cheilitis, leukoplakia, erythroplakia, erythroleukoplakia, oralsubmucous fibrosis, salivary gland malignancies, oral melanoma, verrucouscarcinoma and oral squamous cell carcinoma
Reactive lesions Traumatic ulcerations, frictional keratosis, linear alba, nicotinic stomatitis, focalfibrous hyperplasia, chemical and thermal burns
Hereditary conditions White sponge nevus, epidermolysis bullosa
Table 8 Differential diagnosis of oral mucosal diseases based on clinical appearance
White lesions that can bewiped off
Pseudomembranous candidosis, chemical and thermal burns
White lesions that cannot bewiped off
Linear alba, morsicatio buccarum, leukoedema, white sponge nevus, oral hairyleukoplakia, leukoplakia, leukoedema oral lichen planus, lupus erythematosus,hyperplastic candidosis, frictional keratosis, smoker’s keratosis, and submucous fibrosis
Red lesions Erythematous candidosis, denture associated erythematous stomatitis, irritationalerythema from trauma and burns, submucosal hemorrhage, erythroplakia, lineargingivitis, plasma cell gingivitis, Kaposi sarcoma
Mixed white/red lesions Candidosis, erosive lichen planus, geographic tongue/erythema migrans, systemiclupus erythematosus, contact and systemic allergic reactions, erythroleukoplakia
Vesicular and ulceratedlesions
Aphthous stomatitis, ulcerative lichen planus, mucous membrane pemphigoid,pemphigus vulgaris, erythema multiforme, linear IgA disease, epidermolysis bullosa,traumatic ulcers, herpes simplex virus infections, varicella zoster virus infections,coxsackie virus infections, tuberculosis, deep fungal infections, necrotizingsialometaplasia, syphilis, squamous cell carcinoma
Submucosal bumps andlumps
Focal fibrous hyperplasia, mucocele, lipoma, angiogranuloma, peripheral ossifyingfibroma, peripheral giant cell granuloma, epulis fissuratum, parulis, sialolith, granularcell tumor, hemangioma, neurofibroma, other mesenchymal tumors, salivary glandneoplasms, squamous cell carcinoma
Papillary and verrucouslesions
Squamous papilloma, verruca vulgaris, condyloma acuminatum, focal epithelialhyperplasia, proliferative verrucous leukoplakia, verrucous carcinoma, verruciformxanthoma, verrucous leukoplakia, verrucous hyperplasia
Pigmented lesions Physiologic pigmentation, amalgam tattoo, smoker’s melanosis, melanotic macule,melanocytic nevus, melanoacanthoma, Peutz Jeghers syndrome, Addison’s disease,oral melanoma
Clinical Evaluation of Oral Diseases 27

Table 9 Differential diagnosis of oral mucosal diseases based on location
Lip Fordyce granules, recurrent herpes labialis, actinic cheilitis, angular cheilitis, squamous cellcarcinoma
Labial mucosa Mucocele, epulis fissuratum, focal fibrous hyperplasia, salivary gland neoplasms, aphthousulcers, other mesenchymal tumors
Buccal mucosa Linear alba, leukoedema, pseudomembranous candidosis, Fordyce granules, aphthous ulcers,focal fibrous hyperplasia, lipoma, morsicatio buccarum, oral lichen planus, mucousmembrane pemphigoid, pemphigus vulgaris, leukoplakia
Hard palate Denture associated erythematous stomatitis, nicotinic stomatitis, thermal burn, inflammatorypapillary hyperplasia, palatal abscess, recurrent intraoral herpes simplex infection,melanocytic nevus, necrotizing sialometaplasia, salivary gland neoplasms, lymphoma,Kaposi sarcoma, melanoma
Soft palate Petechiae, viral papilloma, pseudomembranous candidosisTonsils/oropharynx Tonsillitis, tonsiloliths, bifid uvula, viral papilloma, lymphoepithelial cyst, squamous cell
carcinomaTongue Hairy tongue, fissured tongue, hairy leukoplakia, erythema migrans, oral lichen planus,
mucous membrane pemphigoid, pemphigus vulgaris, granular cell tumor, focal fibroushyperplasia, neurofibroma, neurilemmoma, median rhomboid glossitis, atrophic glossitis,angiogranuloma, hemangioma, lymphangioma, proliferative, verrucous leukoplakia,squamous cell carcinoma
Floor of mouth Ranula, sialolith, dermoid cyst, lymphoepithelial cyst, salivary gland neoplasms, squamouscell carcinoma
Gingiva and alveolarprocess
Gingivitis, oral lichen planus, recurrent intraoral herpes simplex infection, herpes zoster,mucous membrane pemphigoid, pemphigus vulgaris, gingival overgrowth, parulis, acutenecrotizing ulcerative gingivitis, primary herpetic gingivostomatitis, angiogranuloma,peripheral giant cell granuloma, peripheral ossifying fibroma, pericoronitis, epulis fissuratum,leukemic infiltrates, Kaposi sarcoma, metastatic tumors
Table 10 Differential diagnosis of ulcerative mucosal diseases based on clinical behavior
Localized acute vesicular and/orulcerative lesions
Aphthous ulcer, traumatic ulcer, necrotizing sialometaplasia, recurrent herpeslabialis, recurrent intraoral herpes, syphilitic chancre, anesthetic necrosis
Localized chronic vesicular and/orulcerative lesions
Traumatic ulcerative granuloma with stromal eosinophilia, squamous cellcarcinoma, deep fungal infections, tuberculous ulcers
Multiple acute vesicular and/orulcerative lesions
Erythema multiforme, primary herpetic gingivostomatitis, allergic reactions,varicella zoster infections (chicken pox and shingles), coxsackie virus infections
Multiple chronic vesicular and/orulcerative lesions
Oral lichen planus, mucous membrane pemphigoid, pemphigus vulgaris, linearIgA disease, Behçet syndrome, lupus erythematosus, epidermolysis bullosa,graft-versus-host disease, Wegener’s granulomatosis
Table 11 Differential diagnosis of radiolucent jaw lesions
Single unilocularperiapical
Apical abscess, periapical granuloma, periapical cyst, periapical scar, focal cemento-osseousdysplasia (early stage), cementoblastoma (early stage)
Single unilocularpericoronal
Hyperplastic follicle, eruption cyst, dentigerous cyst, unicystic ameloblastoma, odontogenickeratocyst, ameloblastic fibroma, adenomatoid odontogenic tumor, calcifying odontogeniccyst
Multilocular Odontogenic myxoma, ameloblastoma, central giant cell granuloma, hemangioma,odontogenic keratocysyt, cherubism, brown tumor of hyperparathyroidism, ameloblasticfibroma
Irregular or ill-defined Rarefying osteitis, osteomyelitis, MRONJ, osteoradionecrosis, osteosarcoma,chondrosarcoma, other primary malignancies, metastasis
Multifocal Florid cement-osseous dysplasia (early stage), multiple myeloma, Gorlin syndrome,Langerhans cell disease, cherubism, hyperparathyroidism
MRONJ Medication-related osteonecrosis of the jaw
28 C.N. Idahosa and A.R. Kerr

Table 12 Differential diagnosis of radiopaque and mixed jaw lesions
Well-defined apical lesions Retained roots, condensing osteitis, idiopathic osteosclerosis, cementoblastoma, focalcemento-osseous dysplasia, periapical cemento-osseous dysplasia
Well-defined lesions: Otherlocations
Torus, exostosis, idiopathic osteosclerosis, odontoma, osteoma, central ossifyingfibroma, calcifying odontogenic cyst, calcifying epithelial odontogenic tumor,adenomatoid odontogenic tumor, ameloblastic fibro-odontoma
Irregular or ill-defined Osteomyelitis, MRONJ, osteoradionecrosis, cemento-osseous dysplasia, fibrousdysplasia, osteosarcoma, chondrosarcoma, squamous cell carcinoma, metastaticcarcinoma
Multifocal Craniofacial fibrous dysplasia, florid cemento-osseous dysplasia, MRONJ, Paget’sdisease, Gardner’s syndrome, osteopetrosis
MRONJ Medication-related osteonecrosis of the jaw
Ulcerative lesions
HSV: Herpes Simplex VirusVZV: Varicella Zoster VirusCMV: CytomegalovirusSCC: Squamous cell carcinomaPFAPA: Periodic fever, aphthous stomatitis, pharyngitis, adenitis syndromeTUGSE: Traumatic ulcerative granuloma with stromal eosinophilia
Acute traumatic• mechanical• thermal• chemical
Viral etiologyHSVVZVCMVCoxsackie
Persistent (> 2 weeks)
No
Ulcerative lesion(s)
Yes
Bacterial orfungal etiology
Aphthous ulcer(s)• •
•••
recurrent aphthous stomatitis (minor/herpetiform)• hematinic deficiencies• celiac disease• Behcet’s• PFAPA
Chronic traumatic• TUG/TUGSE
Erythema multiforme
Vesiculobullous disorders• pemphigus• pemphigoid• linear IgA disease• epidermolysis bullosa
Aphthous ulcer(s)• major
Lichen planusor allergic reaction
Aphthous-like ulcer(s)• Crohn’s disease• ulcerative colitis• orofacial granulomatosis• neutropenia
Neoplastic• SCC• lymphoma• salivary gland
Fig. 11 Algorithm for ulcerative lesions
Clinical Evaluation of Oral Diseases 29

algorithms for ulcerative, pigmented, white, red,and exophytic soft tissue lesions.
Definitive diagnosis: The definitive diagnosisis based on the result of a gold standard test fordiagnosing a particular disease such as histopa-thology to diagnose a squamous cell carcinoma.In many situations, arriving at an accurate defini-tive diagnosis from the differential diagnosis willnecessitate an analytic process involving gather-ing additional clinical information from tests andinvestigations. The choice of diagnostic tests isbased on the items in the differential diagnosis andthe most appropriate tests should be chosen basedon test accuracy. Types of investigations neces-sary to determine a diagnosis may be in the formof imaging studies, chairside diagnostic adjuncts,laboratory studies, and biopsy/histopathologicalstudies. Data from the investigations are then cor-related with the clinical findings before the finaldiagnosis is rendered. The management of thepatient is based on the definitive diagnosis; there-fore, it is imperative that the correct diagnosis ismade.
(i) Diagnostic adjuncts: Diagnostic adjuncts areapplied to an identified lesion or lesions to
provide additional information about thenature of the lesion. A number of diagnosticadjuncts may have utility in the characteriza-tion of potentially malignant disorders (e.g.,light-based adjuncts, vital staining with tolu-idine blue, cytopathogical platforms, and sal-ivary techniques) and a more detaileddescription about these adjuncts, their indi-cations and accuracy will be covered in thechapter on Oral Mucosal Malignancies. Theprocess of procuring cells from a lesion,typically from the lesion surface, is knownas exfoliative cytology. Conditions amena-ble to exfoliative cytology are candidosisand possibly herpes simplex infections.Identified lesions may be sampled by scrap-ing the surface with a metal spatula or cottonswab (i.e., a mucosal smear), plated on aglass slide, immediately fixed, and sent to apathology laboratory for staining and micro-scopic analysis. Lesions that are suspected tobe caused by or associated with candidiasis,yet not overtly obvious based on clinicalfeatures alone (e.g., erythematouscandidosis), are indicated for a mucosalsmear and candidal hyphae may be
Pigmented lesions
Generalized
Yes
Pigmented lesions
No
Syndromes/Systemic Diseases:
Peutz-JeghersLaugier-Hunziker Addison Disease
Reactive:tobacco (smoking)post-inflammatorydrugshormonal
Amalgam tattoo
Racial
Intraoral nevus
Melanoacanthoma Malignantmelanoma
Melanotic macule
••••
•••
•
Fig. 12 Algorithm for pigmented lesions
30 C.N. Idahosa and A.R. Kerr

confirmed by periodic acid-Schiff staining,or in the office by a potassium hydroxidefloat.
(ii) Laboratory investigations: These includemicrobiological testing (i.e., standard culturetechniques, or by detecting microbial anti-gens, antibodies and other immune reac-tions, or by newer molecular techniques(e.g., 15 s ribosomal RNA)), and bloodwork(e.g., complete blood counts, metabolicpanels, serological analyses). These investi-gations are covered in the chapters on Labo-ratory Medicine and Diagnostic Pathology,and Clinical Immunology in Diagnoses ofMaxillofacial Disease.
(iii) Biopsy and histopathological investigation:The definitive diagnosis of many oral andmaxillofacial diseases is based on a
histopathologic diagnosis. Performing abiopsy of soft tissue lesions requires minimalsurgical expertise; however, selecting thebiopsy site that will optimally provide repre-sentative tissue requires careful consider-ation because different diseases dictatedifferent sampling techniques. Excisionalbiopsy is performed when the intent is toremove an entire lesion, while incisionalbiopsy is indicated when a representativepart of a lesion is taken. The tissue sampleshould be immediately placed into a bottlecontaining formalin or other appropriatesolutions depending on the investigationrequired and transported to the pathologylaboratory along with a requisition formthat describes the patient demographics, his-tory, and physical findings including the site
White Lesions or lesions with predominant white component
Infections etiology• pseudomembranous
candidosis
Reactive etiology• thermal or chemical• allergy• mechanical trauma
Does lesion rub away
Yes
White lesions
No
StriaeNo apparent cause
Classic reticular striaelichen planuslichenoid mucositis
Atypical striaeLupus erythematosus GVHD
Infectious etiology• hairy leukoplakia•
••
••
HPV-related• hyperplastic candidosis
Keratosis• hereditary
eg white sponge nevus• frictional• tobacco
Leukoplakia: rule out dysplasia or carcinoma • hyperkeratosis or
hyperplasia• dysplasia• carcinoma in situ• squamous cell carcinoma
Fig. 13 Algorithm for white lesions or lesions with a predominant white component
Clinical Evaluation of Oral Diseases 31
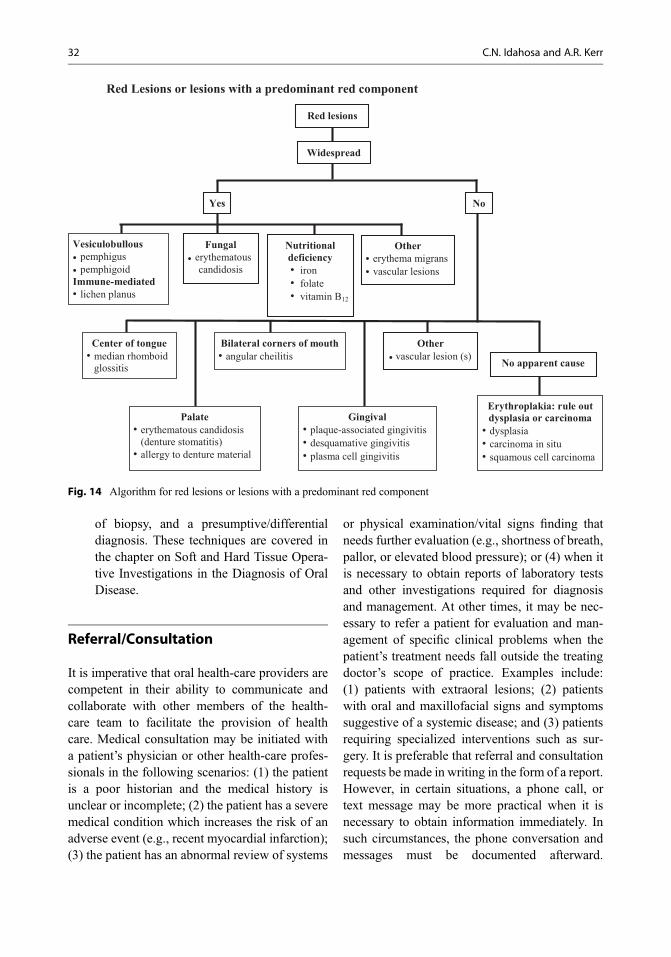
of biopsy, and a presumptive/differentialdiagnosis. These techniques are covered inthe chapter on Soft and Hard Tissue Opera-tive Investigations in the Diagnosis of OralDisease.
Referral/Consultation
It is imperative that oral health-care providers arecompetent in their ability to communicate andcollaborate with other members of the health-care team to facilitate the provision of healthcare. Medical consultation may be initiated witha patient’s physician or other health-care profes-sionals in the following scenarios: (1) the patientis a poor historian and the medical history isunclear or incomplete; (2) the patient has a severemedical condition which increases the risk of anadverse event (e.g., recent myocardial infarction);(3) the patient has an abnormal review of systems
or physical examination/vital signs finding thatneeds further evaluation (e.g., shortness of breath,pallor, or elevated blood pressure); or (4) when itis necessary to obtain reports of laboratory testsand other investigations required for diagnosisand management. At other times, it may be nec-essary to refer a patient for evaluation and man-agement of specific clinical problems when thepatient’s treatment needs fall outside the treatingdoctor’s scope of practice. Examples include:(1) patients with extraoral lesions; (2) patientswith oral and maxillofacial signs and symptomssuggestive of a systemic disease; and (3) patientsrequiring specialized interventions such as sur-gery. It is preferable that referral and consultationrequests be made in writing in the form of a report.However, in certain situations, a phone call, ortext message may be more practical when it isnecessary to obtain information immediately. Insuch circumstances, the phone conversation andmessages must be documented afterward.
Red Lesions or lesions with a predominant red component
Vesiculobullouspemphiguspemphigoid
Immune-mediatedlichen planus
Fungalerythematouscandidosis
Widespread
Yes
Red lesions
No
Center of tongue• median rhomboid
glossitis
Bilateral corners of mouth• •
•••
•
angular cheilitis
Othererythema migransvascular lesions
Erythroplakia: rule out dysplasia or carcinoma • dysplasia• carcinoma in situ• squamous cell carcinoma
No apparent cause
Othervascular lesion (s)
Palate• erythematous candidosis
(denture stomatitis)• allergy to denture material
Gingival• plaque-associated gingivitis• desquamative gingivitis• plasma cell gingivitis
Nutritional deficiency•
••iron
• folate• vitamin B12
Fig. 14 Algorithm for red lesions or lesions with a predominant red component
32 C.N. Idahosa and A.R. Kerr

Table 13 lists the information for referral andconsultation requests.
When medical consultation with a patient’sphysician is required prior to dental treatment orsurgery, it is important to communicate the detailsof the planned procedure, anticipated amount ofblood loss if applicable and level of stress to thepatient. These medical consultations are made torequest additional information concerning thepatient that will aid in risk assessment and poten-tial modifications to treatment. Therefore, the finalresponsibility regarding the risk of treatment lieswith the oral health-care provider who must
Exophytic Lesions
MEN 2b: Multiple endocrine neoplasia 2bSCC: Squamous cell carcinomaAML: Acute myelogenous leukemia
Reactive Gingival• angiogranuloma• peripheral giant cell fibroma• peripheral ossifying fibroma
Malignant• salivary• lymphoma• SCC• sarcoma
Multiple
Exophytic soft tissue lesion (s)
Neurogenic• neurofibromatosis
• MEN 2b
Developmental• lymphoepithelial cyst
No
Benign Neoplasm• neurogenic• lipoma• muscle-derived• vascular• minor salivary gland
HPV-related• viral papilloma• condyloma• verruca vulgaris
Others• gingival overgrowth• AML• Cowden’s syndrome• Tuberous sclerosis
HPV-related• HIV-associated• Hecks disease
Yes
Traumatic • traumatic fibroma• fibrous hyperplasia• mucocele• neuroma
Fig. 15 Algorithm for exophytic soft tissue lesions
Table 13 Information for referral and consultationrequests
Patient’s full name, date of birth, address, phone number,and emailReferring doctor’s full name, title, address, phonenumber, fax, and emailDescription of the problemRelevant history and physical examination findingsDifferential diagnosis/definitive diagnosis if availableRadiographs, laboratory tests, and investigations alreadyperformedAll treatment modalities that have been initiated or areanticipated
Clinical Evaluation of Oral Diseases 33

carefully make the final treatment decisions andnot the physician (Gary and Glick 2012).
Documentation
Medical records provide information regardingthe history of patients’ evaluation and treatmentand can serve as useful evidence during lawsuits.Therefore, it is important to maintain accuratewell-organized and complete records in a chrono-logical order. In settings where paper-based healthrecords are utilized, it is important to ensure thatall pages of the health record contain the patient’sname and identification number. All entriesshould be legible, dated, and contain the author’sname and identification. Although there is nogenerally accepted format for documentation ofclinical data, it is imperative to carefully record allaspects of the clinical history, physical examina-tion, diagnosis, and treatment plan at every patientencounter (Table 1). Other important componentsof the medical record, which should be filed in thechart, include laboratory and imaging reports,referral and consultation requests, informed con-sent, operative notes, postoperative orders, email,text messages, and telephone conversations.
Patients with chronic oral diseases will returnfor follow-up evaluation and care. An abbreviatedhistory is sufficient and the SOAP format is help-ful to update the patient’s history and examinationfindings since the last visit (subjective, objective,assessment, and plan). “Subjective” refers to thehistory, “objective” refers to examination find-ings, “assessment” is the diagnosis along withthe disposition of the patient relative to the diag-nosis (e.g., lichen planus, significant improve-ment on topical steroids), and “plan” is the newmanagement plan.
Conclusion and Future Directions
The goal of clinically evaluating oral diseases is toarrive at a definitive diagnosis and provide effec-tive and safe treatment to patients. A careful andsystematic approach must be applied to gatheringand interpreting the information collected during
the medical history and physical examination.Thorough knowledge of the anatomy, physiology,and clinical behavior of oral diseases is essentialto make the correct diagnosis. It is extremelyimportant that oral health-care providers areappropriately trained in the diagnosis and man-agement of diseases affecting the maxillofacialregion.
Cross-References
▶Clinical Evaluation of Orofacial pain▶Clinical Immunology in Diagnoses of Maxillo-facial Disease
▶Diagnostic Imaging Principles and Applica-tions in Head and Neck Pathology
▶Head and Neck Malignancies▶ Interface Between Oral and Systemic Health toInterface Between Oral and Systemic Disease
▶LaboratoryMedicine and Diagnostic Pathology▶Odontogenic Pathology▶Oral Mucosal Malignancies▶Oral Ulcerative Lesions▶Oral Vesicular and Bullous Lesions▶ Salivary Gland Disorders and Diseases▶ Soft and Hard Tissue Operative Techniques inthe Diagnosis of Oral Disease
▶White and Red Lesions of the Oral Mucosa
References
Couch ET, Chaffee BW, Gansky SA, Walsh MM. Thechanging tobacco landscape: What dental professionalsneed to know. J Am Dent Assoc. 2016;147(7):561–9.
Degenhardt L, Hall W. Extent of illicit drug use and depen-dence, and their contribution to the global burden ofdisease. Lancet. 2012;379(9810):55–70.
Farman AG. ALARA still applies. Oral Surg Oral MedOral Pathol Oral Radiol Endod. 2005;100(4):395–7.
Gary CJ, Glick M. Medical clearance: an issue of profes-sional autonomy, not a crutch. J Am Dent Assoc.2012;143(11):1180–1.
James PA, Oparil S, Carter BL, Cushman WC, Dennison-Himmelfarb C, Handler J, et al. 2014 evidence-basedguideline for the management of high blood pressure inadults: report from the panel members appointed to theeighth joint National Committee (JNC 8). JAMA.2014;311(5):507–20.
34 C.N. Idahosa and A.R. Kerr

Ludwick DA, Doucette J. Adopting electronic medicalrecords in primary care: lessons learned from healthinformation systems implementation experience inseven countries. Int J Med Inform. 2009;78(1):22–31.
Marshall TA. Chairside diet assessment of caries risk. J AmDent Assoc. 2009;140(6):670–4.
Miller CS, Epstein JB, Hall EH, Sirois D. Changing oralcare needs in the United States: the continuing need fororal medicine. Oral Surg Oral Med Oral Pathol OralRadiol Endod. 2001;91(1):34–44.
Navazesh M, Kumar SK, University of Southern Califor-nia School of Dentistry. Measuring salivary flow: chal-lenges and opportunities. J Am Dent Assoc. 2008;139(Suppl):35S–40S.
NIAAA. National Institute on Alchohol Abuse and Alco-holism. Helping patients who drink too much: a clini-cian’s guide. 2005.; Available at: http://pubs.niaaa.nih.gov/publications/Practitioner/CliniciansGuide2005/clinicians_guide.htm. Accessed 20 Aug 2016.
Ogden GR. Alcohol and oral cancer. Alcohol. 2005;35(3):169–73.
Petersen PE. Oral cancer prevention and control – theapproach of the World Health Organization. OralOncol. 2009;45(4–5):454–60.
Reidy J, McHugh E, Stassen LF. A review of the relation-ship between alcohol and oral cancer. Surgeon. 2011;9(5):278–83.
Sarteschi LM. Jehovah’s witnesses, blood transfusions andtransplantations. Transplant Proc. 2004;36(3):499–501.
Schiffman E, Ohrbach R, Truelove E, Look J, Anderson G,Goulet JP, et al. Diagnostic criteria for temporomandib-ular disorders (DC/TMD) for clinical and researchapplications: recommendations of the internationalRDC/TMD consortium network* and orofacial pain
special interest Groupdagger. J Oral Facial Pain Head-ache. 2014;28(1):6–27.
Scully C, Miller CS, Aguirre Urizar JM, Alajbeg I,Almeida OP, Bagan JV, et al. Oral medicine(stomatology) across the globe: birth, growth, andfuture. Oral Surg Oral Med Oral Pathol Oral Radiol.2016;121(2):149–157.e5.
Sollecito TP, Rogers H, Prescott-Clements L, Felix DH,Kerr AR, Wray D, et al. Oral medicine: defining anemerging specialty in the United States. J Dent Educ.2013;77(4):392–4.
Stoopler ET, Sollecito TP. Focusing on the medicine indental medicine. Spec Care Dentist. 2016;36(2):59.
Stoopler ET, Shirlaw P, Arvind M, Lo Russo L, Bez C, DeRossi S, et al. An international survey of oral medicinepractice: proceedings from the 5th world workshop inoral medicine. Oral Dis. 2011;17(Suppl 1):99–104.
Tilakaratne WM, Ekanayaka RP, Warnakulasuriya S. Oralsubmucous fibrosis: a historical perspective and areview on etiology and pathogenesis. Oral Surg OralMed Oral Pathol Oral Radiol. 2016;122(2):178–91.
Waziry R, Jawad M, Ballout RA, Al Akel M, Akl EA. Theeffects of waterpipe tobacco smoking on health out-comes: an updated systematic review and meta-analysis. Int J Epidemiol. 2016; doi:10.1093/ije/dyw021.
WHO. World Health Organization tobacco fact sheet.2016.; Available at: http://www.who.int/mediacentre/factsheets/fs339/en/. Accessed 01 Jul 2016.
Wong-Baker FACES Foundation. Wong-Baker FACES®
Pain Rating Scale. 2016.; Available at: http://www.wongbakerfaces.org/. Accessed 04 2017.
Zawawi KH, Al-Badawi EA, Lobo SL, Melis M,Mehta NR. An index for the measurement of normalmaximum mouth opening. J Can Dent Assoc. 2003;69(11):737–41.
Clinical Evaluation of Oral Diseases 35












![Academic Leadership ppt - Benson Idahosa Universityoer.biu.edu.ng/wp-content/uploads/2018/11/... · Microsoft PowerPoint - Academic Leadership ppt [Compatibility Mode] Author: HP](https://static.fdocuments.net/doc/165x107/5f82014dc0ce5a4bec281aaa/academic-leadership-ppt-benson-idahosa-microsoft-powerpoint-academic-leadership.jpg)





