
Oral Ulcerative Lesions -...
33
Oral Ulcerative Lesions Giovanni Lodi, Elena Varoni, Jairo Robledo-Sierra, Alessandro Villa, and Mats Jontell Abstract Ulcers are the most common lesions affecting the oral mucosa, and they can be ascribed to a plethora of local or systemic conditions, making differential diagnosis pivotal and often difficult. As oral ulcers, they can be a manifestation of local or systemic conditions of very different nature and severity, including trauma (mechanical, chemical, thermal), drug reactions, immune-mediated diseases, infec- tions, and neoplasms; a careful differential diagnosis is mandatory. Recurrent aphthous stomatitis (RAS) is the most frequent ulcera- tive disorder of the oral cavity, affecting 10–20% of the general population. RAS lesions typically present as round or oval shallow ulcers of the nonkeratinized mucosa, with a yellow-grayish fibrin pseudomembrane and a characteristic erythematous halo. They usually appear first in childhood or adolescence, in subjects without other systemic signs. RAS may present in four main forms based on its clinical appearance (minor, major, herpetiform, and severe), and its management depends on the frequency and severity of the lesions. RAS episodes are self- limiting and in most cases do not need treat- ment. For severe and painful cases, the aim of therapy is to control pain and to reduce the frequency of episodes. Topical corticosteroids are typically first-line treatment, but they do not affect the rate of recurrence. Less frequently, aphthous stomatitis can be associated with a number of systemic conditions, including gas- trointestinal disorders, in particular inflamma- tory bowel diseases and celiac disease, Behçet syndrome, food allergy, and deficiencies of micronutrients, mainly vitamin B12, folate, fer- ritin, and iron. In all these cases, the detection of oral lesions can lead to an early diagnosis of the underlying condition, which management requires a multi-specialist approach. Keywords Oral ulcer • Oral ulcerative disease • Oral ulcer- ative conditions • Recurrent aphthous ulcera- tion • Recurrent aphthous stomatitis • Aphthous-like ulcers • Crohn’ s disease • Celiac disease • Inflammatory bowel disease • Behçet syndrome • Food allergy • Micronutrient deficiency G. Lodi (*) • E. Varoni Dipartimento di Scienze Biomediche, Chirurgiche e Odontoiatriche, Università degli Studi di Milano, Milan, Italy e-mail: [email protected]; [email protected] J. Robledo-Sierra • M. Jontell Department of Oral Medicine and Pathology, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden e-mail: [email protected]; [email protected]; [email protected] A. Villa Division of Oral Medicine and Dentistry, Brigham and Women’ s Hospital & Dana Farber Cancer Center and Department of Oral Medicine, Infection and Immunity, Harvard School of Dental Medicine, Boston, MA, USA e-mail: [email protected]; [email protected] # Springer International Publishing AG 2017 C.S. Farah et al. (eds.), Contemporary Oral Medicine, https://doi.org/10.1007/978-3-319-28100-1_12-1 1
Transcript of Oral Ulcerative Lesions -...

Oral Ulcerative Lesions
Giovanni Lodi, Elena Varoni, Jairo Robledo-Sierra,Alessandro Villa, and Mats Jontell
AbstractUlcers are the most common lesions affectingthe oral mucosa, and they can be ascribed toa plethora of local or systemic conditions,making differential diagnosis pivotal andoften difficult. As oral ulcers, they can be amanifestation of local or systemic conditionsof very different nature and severity, includingtrauma (mechanical, chemical, thermal), drugreactions, immune-mediated diseases, infec-tions, and neoplasms; a careful differentialdiagnosis is mandatory. Recurrent aphthousstomatitis (RAS) is the most frequent ulcera-tive disorder of the oral cavity, affecting 10–20%of the general population. RAS lesions typicallypresent as round or oval shallow ulcers of thenonkeratinized mucosa, with a yellow-grayish
fibrin pseudomembrane and a characteristicerythematous halo. They usually appear firstin childhood or adolescence, in subjects withoutother systemic signs. RAS may present in fourmain forms based on its clinical appearance(minor, major, herpetiform, and severe), andits management depends on the frequency andseverity of the lesions. RAS episodes are self-limiting and in most cases do not need treat-ment. For severe and painful cases, the aim oftherapy is to control pain and to reduce thefrequency of episodes. Topical corticosteroidsare typically first-line treatment, but they do notaffect the rate of recurrence. Less frequently,aphthous stomatitis can be associated with anumber of systemic conditions, including gas-trointestinal disorders, in particular inflamma-tory bowel diseases and celiac disease, Behçetsyndrome, food allergy, and deficiencies ofmicronutrients, mainly vitamin B12, folate, fer-ritin, and iron. In all these cases, the detectionof oral lesions can lead to an early diagnosis ofthe underlying condition, which managementrequires a multi-specialist approach.
KeywordsOral ulcer •Oral ulcerative disease •Oral ulcer-ative conditions • Recurrent aphthous ulcera-tion • Recurrent aphthous stomatitis •Aphthous-like ulcers •Crohn’s disease •Celiacdisease • Inflammatory bowel disease • Behçetsyndrome • Food allergy • Micronutrientdeficiency
G. Lodi (*) • E. VaroniDipartimento di Scienze Biomediche, Chirurgiche eOdontoiatriche, Università degli Studi di Milano, Milan,Italye-mail: [email protected]; [email protected]
J. Robledo-Sierra • M. JontellDepartment of Oral Medicine and Pathology, SahlgrenskaAcademy, University of Gothenburg, Gothenburg, Swedene-mail: [email protected];[email protected]; [email protected]
A. VillaDivision of Oral Medicine and Dentistry, Brigham andWomen’s Hospital & Dana Farber Cancer Center andDepartment of Oral Medicine, Infection and Immunity,Harvard School of Dental Medicine, Boston, MA, USAe-mail: [email protected]; [email protected]
# Springer International Publishing AG 2017C.S. Farah et al. (eds.), Contemporary Oral Medicine,https://doi.org/10.1007/978-3-319-28100-1_12-1
1

ContentsIntroduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
Ulcerative Lesions of the Mouth . . . . . . . . . . . . . . . . . . . . 3Reactive Ulcerative Conditions . . . . . . . . . . . . . . . . . . . . . . . 3Immunological Ulcerative Conditions . . . . . . . . . . . . . . . . 6Infective Ulcerative Conditions . . . . . . . . . . . . . . . . . . . . . . . 6Neoplastic Ulcerative Conditions . . . . . . . . . . . . . . . . . . . . . 8
Recurrent Aphthous Stomatitis (RAS) . . . . . . . . . . . . . 8Epidemiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Etiopathogenesis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Diagnosis and Clinical Presentation . . . . . . . . . . . . . . . . . . 9Management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Aphthous Stomatitis Associated with SystemicConditions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
Gastrointestinal Disorders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11Behçet Syndrome . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20Food Allergy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
Recurrent Aphthous Stomatitis and MicronutrientDeficiency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
Conclusions and Future Directions . . . . . . . . . . . . . . . . . 27
Cross-References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
Introduction
An ulcer of the mouth results from the completeloss of epithelium which exposes the underlyingconnective tissues. When the loss is limited to theepithelial layers, the term erosion is preferred,although such distinction can be difficult on thebasis of clinical investigation only.
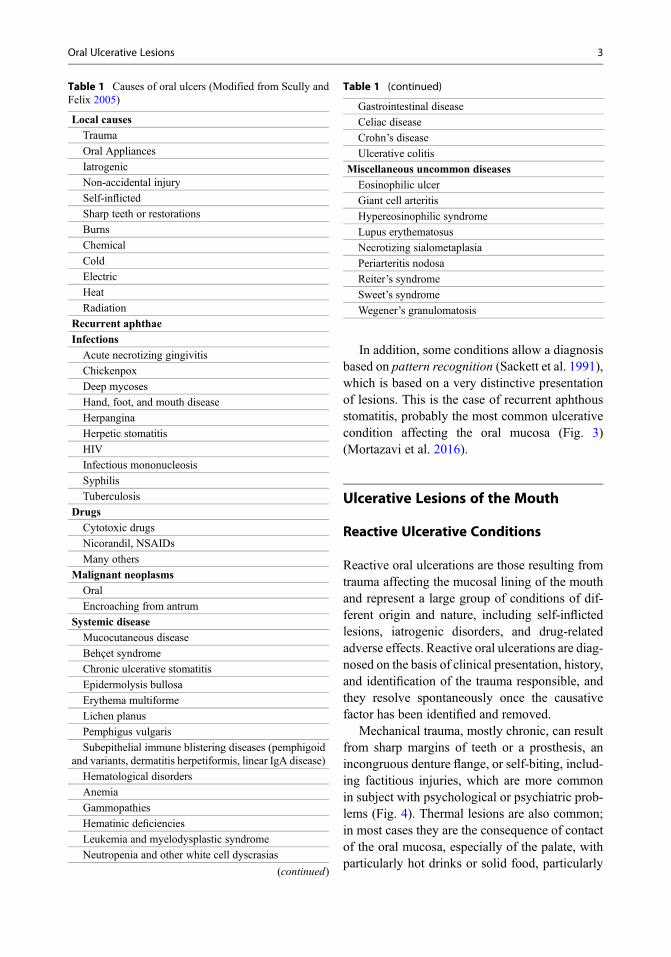
As indicated by a number of epidemiologicalstudies (Axéll 1976; Carrard et al. 2011; García-Pola Vallejo et al. 2002; Pentenero et al. 2008;Shulman et al. 2004), ulcerations are among themost common lesions affecting the oral mucosa.This is probably due to the fact that not only domany of the most common oral conditions presentas ulcerative lesions (see other chapters on“▶Oral Lichen Planus,” “▶Oral Vesicular andBullous Lesions,” and “▶Oral and MaxillofacialViral Infections”) but also that an ulcer can be themanifestation of a large number of local and sys-temic conditions, including viral, bacterial,parasite and fungal infections, immune-mediateddiseases, neoplasms, hematological disorders,trauma (mechanical, chemical, thermal), and
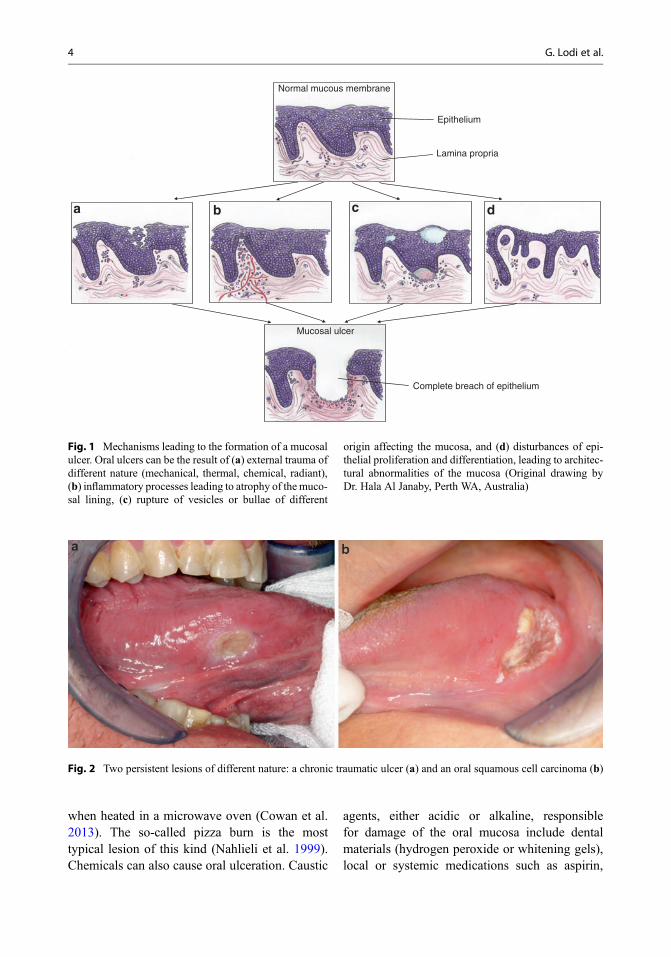
drug reactions (Table 1). In addition, an ulcerativelesion can result from different processes andetiopathogenic mechanisms, such as bullae orvesicle formation and rupture, external forces,host-related factors, or alteration of epithelial pro-liferation and differentiation (Fig. 1). Thus, differ-ential diagnosis of an oral ulcer is a key skill inoral medicine practice, since similar lesions canhave a deeply different impact on the well-beingof patients, and a misdiagnosis can bring veryserious consequences. This is the case with achronic traumatic ulcer of the tongue, a very com-mon lesion that can share a number of featureswith a squamous cell carcinoma of the same site,as they are both long-lasting, pauci-symptomatic,indurated, single lesions (Fig. 2). While thefirst resolves spontaneously once the traumaticcause has been removed, the latter is potentiallylethal (see chapters on “▶White and Red Lesionsof the Oral Mucosa” and “▶Oral MucosalMalignancies”).
Although histological examination and spe-cific laboratory tests are often mandatory, a carefulclinical examination, associated with thoroughhistory taking, can provide insights into the natureof an oral ulcer. Important clinical features ininvestigating a patient affected by ulcer(s) of themouth range from:
• Number of lesions, single as for oral cancer ormultiple as for herpetic infection
• Specific localization, as for aphthae which pre-fer nonkeratinized mucosa or chronic trau-matic ulcer, in relation with a scabrous orrough surface
• Duration, with a recent onset typical of acuteconditions, or extensive length for chroniclesions, including oral cancer
• Presence of a blister preceding the ulcer, afeature of immune-mediated conditions(bulla) or viral infection (vesicle)
• Presence of other mucosal changes, as for orallichen planus, which ulcers are always associ-ated with other manifestations of the disease,and extraoral signs, as for mucocutaneous con-ditions with frequent skin involvement (i.e.,pemphigus, erythema multiforme)
2 G. Lodi et al.
In addition, some conditions allow a diagnosisbased on pattern recognition (Sackett et al. 1991),which is based on a very distinctive presentationof lesions. This is the case of recurrent aphthousstomatitis, probably the most common ulcerativecondition affecting the oral mucosa (Fig. 3)(Mortazavi et al. 2016).
Ulcerative Lesions of the Mouth
Reactive Ulcerative Conditions
Reactive oral ulcerations are those resulting fromtrauma affecting the mucosal lining of the mouthand represent a large group of conditions of dif-ferent origin and nature, including self-inflictedlesions, iatrogenic disorders, and drug-relatedadverse effects. Reactive oral ulcerations are diag-nosed on the basis of clinical presentation, history,and identification of the trauma responsible, andthey resolve spontaneously once the causativefactor has been identified and removed.
Mechanical trauma, mostly chronic, can resultfrom sharp margins of teeth or a prosthesis, anincongruous denture flange, or self-biting, includ-ing factitious injuries, which are more commonin subject with psychological or psychiatric prob-lems (Fig. 4). Thermal lesions are also common;in most cases they are the consequence of contactof the oral mucosa, especially of the palate, withparticularly hot drinks or solid food, particularly
Table 1 Causes of oral ulcers (Modified from Scully andFelix 2005)
Local causes
Trauma
Oral Appliances
Iatrogenic
Non-accidental injury
Self-inflicted
Sharp teeth or restorations
Burns
Chemical
Cold
Electric
Heat
Radiation
Recurrent aphthae
Infections
Acute necrotizing gingivitis
Chickenpox
Deep mycoses
Hand, foot, and mouth disease
Herpangina
Herpetic stomatitis
HIV
Infectious mononucleosis
Syphilis
Tuberculosis
Drugs
Cytotoxic drugs
Nicorandil, NSAIDs
Many others
Malignant neoplasms
Oral
Encroaching from antrum
Systemic disease
Mucocutaneous disease
Behçet syndrome
Chronic ulcerative stomatitis
Epidermolysis bullosa
Erythema multiforme
Lichen planus
Pemphigus vulgaris
Subepithelial immune blistering diseases (pemphigoidand variants, dermatitis herpetiformis, linear IgA disease)
Hematological disorders
Anemia
Gammopathies
Hematinic deficiencies
Leukemia and myelodysplastic syndrome
Neutropenia and other white cell dyscrasias
(continued)
Table 1 (continued)
Gastrointestinal disease
Celiac disease
Crohn’s disease
Ulcerative colitis
Miscellaneous uncommon diseases
Eosinophilic ulcer
Giant cell arteritis
Hypereosinophilic syndrome
Lupus erythematosus
Necrotizing sialometaplasia
Periarteritis nodosa
Reiter’s syndrome
Sweet’s syndrome
Wegener’s granulomatosis
Oral Ulcerative Lesions 3
when heated in a microwave oven (Cowan et al.2013). The so-called pizza burn is the mosttypical lesion of this kind (Nahlieli et al. 1999).Chemicals can also cause oral ulceration. Caustic
agents, either acidic or alkaline, responsiblefor damage of the oral mucosa include dentalmaterials (hydrogen peroxide or whitening gels),local or systemic medications such as aspirin,
Normal mucous membrane
Epithelium
Lamina propria
Complete breach of epithelium
Mucosal ulcer
a b c d
Fig. 1 Mechanisms leading to the formation of a mucosalulcer. Oral ulcers can be the result of (a) external trauma ofdifferent nature (mechanical, thermal, chemical, radiant),(b) inflammatory processes leading to atrophy of themuco-sal lining, (c) rupture of vesicles or bullae of different
origin affecting the mucosa, and (d) disturbances of epi-thelial proliferation and differentiation, leading to architec-tural abnormalities of the mucosa (Original drawing byDr. Hala Al Janaby, Perth WA, Australia)
Fig. 2 Two persistent lesions of different nature: a chronic traumatic ulcer (a) and an oral squamous cell carcinoma (b)
4 G. Lodi et al.

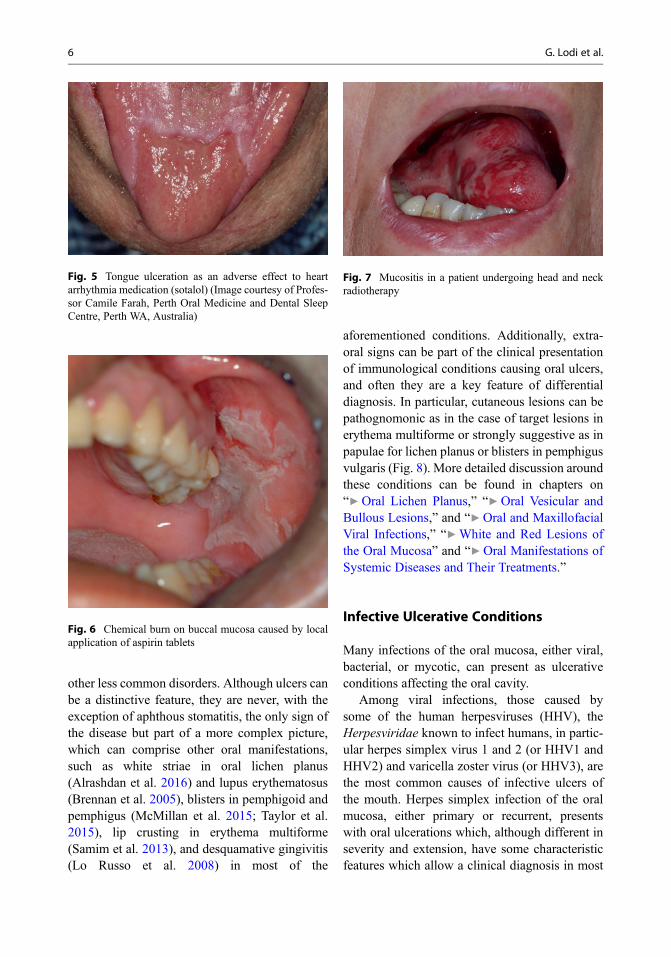
bisphosphonates, antipsychotic drugs, antihyper-tensive medications, mouthwashes, recreationaldrugs, and non-pharmaceutical substances (hairproducts, battery acid) (Figs. 5 and 6) (Gilvetti2010). Exposure to ionizing radiation for the treat-ment of head and neck cancer almost invariablyleads to mucositis, a diffuse and painful ulcerationof the oral mucosa (Fig. 7).
Immunological Ulcerative Conditions
Immunological conditions affecting the oralmucosa are a group of diseases which arecommon causes of oral ulcerations, comprisingaphthous stomatitis, oral lichen planus, mucousmembrane pemphigoid, pemphigus vulgaris,erythema multiforme, lupus erythematosus, and
(i) Traumatic ulcerAcute solitary ulcers (ii) Necrotizing sialometaplasia
Acute ulcers
Acute multiple ulcers (i) Primary herpetic gingivostomatitis(ii) Varicella-Zoster Virus infection(iii) Herpangina
(i) Long-standing traumatic ulcers (iv) Hand-foot-and-mouth disease(ii) Necrotizing sialometaplasia (v) Erythema multiforme(iii) Eosinophilic ulcer (vi) Necrotizing ulcerative gingivitis
Chronic solitary ulcers (iv) Ulcerative squamous cell carcinoma (vii) Oral hypersentivity reactions(v) Cytomegalovirus-associated ulceration (viii) Plasma cell gingivostomatitis(vi) Tuberculous ulcer (ix) Chemotherapy-related ulcers
Oral Ulcers Chronic ulcers (vii) Syphilitic ulceration (chancre)(viii) Deep fungal ulceration
(Histoplasmosis, Blastomycosis, andMucormycosis)
(i) Pemphigus vulgaris(ii) Mucous membrane pemphigoid
Chronic multiple ulcers (iii) Bullous pemphigoid(iv) Lichen planus (v) Linear IgA disease
(i) Recurrent aphthous stomatitisRecurrent ulcers Solitary/multiple ulcers (ii) Recurrent herpes stomatitis
(iii) Herpes-associated erythema multiforme(iv) Cyclic neutropenia(v) Behçet’s disease
Fig. 3 Diagnostic flowchart for oral ulcerative lesions (Mortazavi et al. 2016)
Fig. 4 Self-inflicted ulcer of the tongue in a child (a) and teenager (b) with psychiatric disorders
Oral Ulcerative Lesions 5
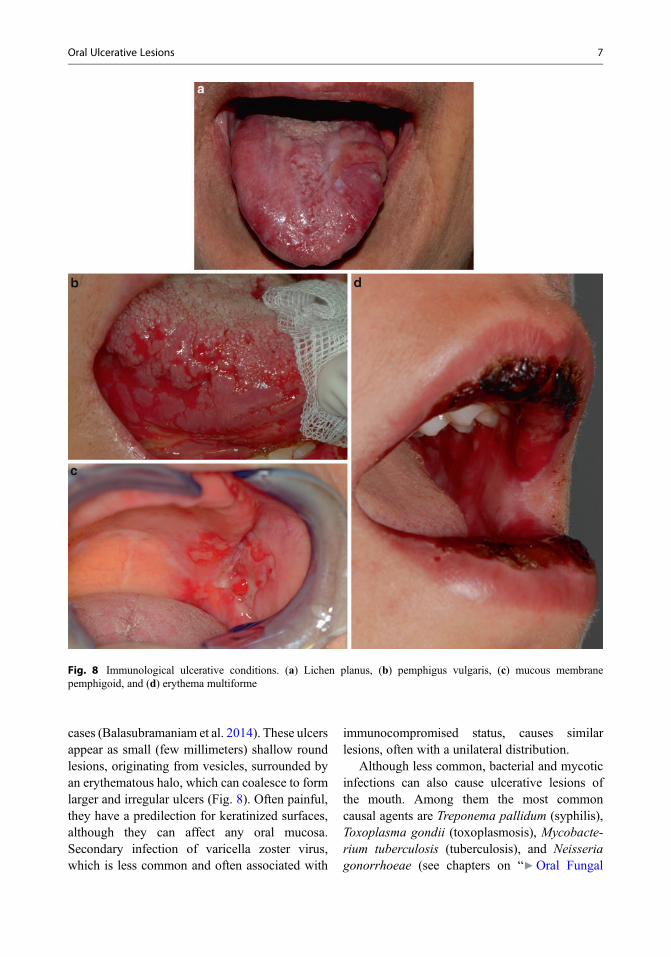
other less common disorders. Although ulcers canbe a distinctive feature, they are never, with theexception of aphthous stomatitis, the only sign ofthe disease but part of a more complex picture,which can comprise other oral manifestations,such as white striae in oral lichen planus(Alrashdan et al. 2016) and lupus erythematosus(Brennan et al. 2005), blisters in pemphigoid andpemphigus (McMillan et al. 2015; Taylor et al.2015), lip crusting in erythema multiforme(Samim et al. 2013), and desquamative gingivitis(Lo Russo et al. 2008) in most of the
aforementioned conditions. Additionally, extra-oral signs can be part of the clinical presentationof immunological conditions causing oral ulcers,and often they are a key feature of differentialdiagnosis. In particular, cutaneous lesions can bepathognomonic as in the case of target lesions inerythema multiforme or strongly suggestive as inpapulae for lichen planus or blisters in pemphigusvulgaris (Fig. 8). More detailed discussion aroundthese conditions can be found in chapters on“▶Oral Lichen Planus,” “▶Oral Vesicular andBullous Lesions,” and “▶Oral and MaxillofacialViral Infections,” “▶White and Red Lesions ofthe Oral Mucosa” and “▶Oral Manifestations ofSystemic Diseases and Their Treatments.”
Infective Ulcerative Conditions
Many infections of the oral mucosa, either viral,bacterial, or mycotic, can present as ulcerativeconditions affecting the oral cavity.
Among viral infections, those caused bysome of the human herpesviruses (HHV), theHerpesviridae known to infect humans, in partic-ular herpes simplex virus 1 and 2 (or HHV1 andHHV2) and varicella zoster virus (or HHV3), arethe most common causes of infective ulcers ofthe mouth. Herpes simplex infection of the oralmucosa, either primary or recurrent, presentswith oral ulcerations which, although different inseverity and extension, have some characteristicfeatures which allow a clinical diagnosis in most
Fig. 5 Tongue ulceration as an adverse effect to heartarrhythmia medication (sotalol) (Image courtesy of Profes-sor Camile Farah, Perth Oral Medicine and Dental SleepCentre, Perth WA, Australia)
Fig. 6 Chemical burn on buccal mucosa caused by localapplication of aspirin tablets
Fig. 7 Mucositis in a patient undergoing head and neckradiotherapy
6 G. Lodi et al.
cases (Balasubramaniam et al. 2014). These ulcersappear as small (few millimeters) shallow roundlesions, originating from vesicles, surrounded byan erythematous halo, which can coalesce to formlarger and irregular ulcers (Fig. 8). Often painful,they have a predilection for keratinized surfaces,although they can affect any oral mucosa.Secondary infection of varicella zoster virus,which is less common and often associated with
immunocompromised status, causes similarlesions, often with a unilateral distribution.
Although less common, bacterial and mycoticinfections can also cause ulcerative lesions ofthe mouth. Among them the most commoncausal agents are Treponema pallidum (syphilis),Toxoplasma gondii (toxoplasmosis), Mycobacte-rium tuberculosis (tuberculosis), and Neisseriagonorrhoeae (see chapters on “▶Oral Fungal
Fig. 8 Immunological ulcerative conditions. (a) Lichen planus, (b) pemphigus vulgaris, (c) mucous membranepemphigoid, and (d) erythema multiforme
Oral Ulcerative Lesions 7

Infections” and “▶Non-Odontogenic BacterialInfections” for more detail).
Neoplastic Ulcerative Conditions
A single, indurated ulcer is a common presen-tation of oral cancer and must be carefully differ-entiated from traumatic or bacterial ulcers. Oralsquamous cell carcinoma represents more than90% of cancer of the mouth (Chi et al. 2015);however a range of other malignancies of theoral cavity may also present as ulcers, includingneoplasms of the salivary glands, hematologicmalignancies, metastatic neoplasms, and Kaposisarcoma (Fig. 9).
Recurrent Aphthous Stomatitis (RAS)
Recurrent aphthous stomatitis (RAS), or “cankersores,” is a common oral mucosal disease affect-ing 10–20% of the general population. It is char-acterized by recurring ulcers of the oral mucosausually manifesting first in childhood or adoles-cence in patients with no other systemic diseases.
RAS may present in four main forms based on itsclinical appearance: minor, major, herpetiform,and severe (Table 2).
Epidemiology
RAS usually initially develops in individualsbetween 10 and 19 years of age and becomesless common with time (Ship et al. 2000). Casesof RAS that become more severe with age may beindicative of an underlying systemic condition(e.g., Behçet disease, connective tissue disorders,hematologic diseases) and merit further investiga-tion. The incidence of RAS ranges between 5%and 50% and is dependent on the socioeconomicstatus and ethnicity of patients (Ship 1962). Theprevalence of RAS in children has been reportedto be as high as 40% (Miller et al. 1980) and isinfluenced by family history; individuals whoseparents have a history of RAS are at higher risk ofdeveloping RAS compared to those who have anegative family history (90% vs. 20%) (Ship1972). In addition, children with a high socioeco-nomic status are five times more likely to developRAS (Crivelli et al. 1988; Gallo et al. 2009).
Fig. 9 Neoplastic ulcerative conditions. (a) Low-grade salivary adenocarcinoma and (b) diffuse large B cell lymphoma
Table 2 Types of recurrent aphthous stomatitis
Type Size Duration
Minor <1.0 cm 7–10 days
Major >1.0 cm Weeks, often with scarring
Herpetiform Few mm (usually >10 ulcers) 7–10 days
Severe <1.0 cm (same as minor) Continuously
8 G. Lodi et al.

Etiopathogenesis
The etiology of RAS is multifactorial and notyet well understood. Theories in the past haveassociated RAS with several bacterial and viralinfections, such as varicella zoster virus (VZV),cytomegalovirus (CMV), and human herpesvirus (HHV) 6 and 7, oral streptococci, andHelicobacter pylori, although none of these havebeen confirmed and data remain inconclusive (Linet al. 2005; Pedersen and Hornsleth 1993; Victoriaet al. 2003).
Common risk and triggering factors associatedwith RAS include local factors (e.g., smokingcessation and trauma), hematologic or immuno-logic defects, and genetics. Heredity may play arole as both twins and children with parentsaffected by RAS are more prone to develop thedisease (Miller et al. 1980). Several specifichuman leukocyte antigens (HLAs) have beenassociated in RAS patients (HLA-A2, HLA-B5,HLA-B12, HLA-B44, HLA-B51, HLA-B52,HLA-DR2, HLA-DR7, and HLA-DQ series)confirming the inherited nature of this disease(Albanidou-Farmaki et al. 2008).
RAS is considered an immuno-mediatedcondition; however specific abnormalities of theimmune system have not yet been identified(Baccaglini et al. 2008). Immunoglobulin serumlevels and natural killer cells are usually withinnormal ranges in patients with RAS. Studies haveshown defects of cell-mediated immunity with analteration in the CD4+:CD8+ T lymphocyte ratio(Preeti et al. 2011). Specifically, CD4+ cells aremore frequent in the pre-ulcer and healing phases,while CD8+ cell levels are higher when the ulceris present (Bachtiar et al. 1998; Sun et al. 2000). Adysfunction of the mucosal cytokine cascade hasbeen associated with RAS with a subsequentincreased cell-mediated immune response andlocal ulceration of the oral mucosa. Increasedlevels of interleukin-2 (IL-2), IL-4, IL-5, inter-feron-γ, and tumor necrosis factor-α in aphthousulcers and raised levels of circulating IL-6 havebeen found in patients with RAS (Boras et al.2006; Buno et al. 1998; Pekiner et al. 2012; Yama-moto et al. 1994). In addition, RAS has beenlinked to genetic factors, specifically those genes
controlling the release of pro-inflammatory cyto-kines IL-1B and IL-6 (Bazrafshani et al. 2002).
Other possible precipitating factors for RASinclude nutritional deficiencies, psychologicalstress, anxiety, hormonal fluctuations, allergyto certain foods, and sodium lauryl sulfate-containing toothpaste (Akintoye and Greenberg2014). Conditions that may present with RASinclude micronutrient deficiencies, Behçet dis-ease, celiac disease, inflammatory bowel disease,and HIV disease (see below).
Diagnosis and Clinical Presentation
The diagnosis of RAS is generally made throughthe patient’s history and clinical presentation.Biopsy is not indicated, although it may be helpfulin atypical cases to rule out other conditions. Oralulcers typically develop in the first two decades oflife, and the frequency of developing recurrentlesions decreases during the third decade. Insome rare cases, the severity and frequency ofRAS can increase in the elderly. RAS typicallypresents as round or oval shallow ulcers ofthe nonkeratinized mucosa with a yellow-grayishfibrin pseudomembrane with a characteristic ery-thematous halo. The labial and buccal mucosaeare the most commonly affected sites. Major RASmay also involve other sites such as the tonguedorsum, hard palate, soft palate, and palatoglossaland palatopharyngeal arches. Sometimes a burn-ing sensation or tingling may precede the devel-opment of oral ulcers with localized erythema.Crunchy, spicy, acidic food and certain beveragesmay make eating, speaking, and swallowing un-comfortable. Four main forms exist: minor,herpetiform, major, and severe (Table 2).
Minor aphthous stomatitis (Fig. 10) representsthe most common form; minor aphthae are lessthan 1 cm in diameter and can be single or multi-ple. The ulcers are round, shallow, and often sym-metric. Once present, they can be painful (mainlyduring the first 3–4 days, exacerbated with oralfunction), usually last 7–10 days, and heal withoutscarring. The majority of patients with RAS reportone to six lesions at a time with few recurringepisodes in 1 year.
Oral Ulcerative Lesions 9

Major aphthous ulcers (Fig. 11) are larger(usually >1.0 cm in diameter), deep, extremelypainful lesions, which interfere with speech andeating, and last for weeks or months. In somecases, major aphthae may be misdiagnosed as avesiculobullous disorder, squamous cell carci-noma, or granulomatous disease. The lesionsmay heal with scar formation. In the most severecases, hospitalization for intravenous feeding maybe required.
Herpetiform aphthous stomatitis (Fig. 12) is arare variant, with multiple small ulcers, measuringfew millimeters, with a crop-like appearance thatusually coalesce to form a large lesion with irreg-ular margin similar to HSV-related ulcers. Theoverall appearance is identical to the minoraphthous ulcers (although smaller in size), andthese also heal within 7–10 days.
Severe aphthous ulcers (Fig. 13) are a variantin which patients are almost never ulcer-free,and they are often associated with chronic pain,malnutrition, and weight loss. Patients typicallydevelop new ulcers when the previous ones arehealing. Both the keratinized and nonkeratinizedmucosa may be affected. In HIV patients, severerecurrent aphthous ulcers are often larger than1.0 cm in diameter.
In cases of atypical RAS (such as in olderindividuals with new episodes or in patients withother/new systemic symptoms), laboratory testsmay be helpful. A blood workup might be indi-cated if hematologic deficiencies are suspected(e.g., low serum levels of vitamin B12, folate,ferritin, and iron) or in HIV patients with a CD4
Fig. 10 Minor recurrent aphthous stomatitis on the buccalmucosa
Fig. 11 Major recurrent aphthous stomatitis on the softpalate
Fig. 12 Herpetiform recurrent aphthous stomatitis on the soft palate (a) and lower labial mucosa (b)
10 G. Lodi et al.

count below 100/mm3 (Crivelli et al. 1988).Tissue biopsies may be obtained to rule outvesiculobullous disorders (e.g., mucous mem-brane pemphigoid or pemphigus) or granuloma-tous diseases (e.g., sarcoidosis or Crohn’sdisease).
Management
The management of RAS depends on the fre-quency and severity of the lesions. In manycases (especially for the minor form) treatment isnot necessary as the pain is tolerable and doesnot interfere with the daily life activities ofthe patient (Fig. 14). The main therapeutic goalfor severe and painful cases is to reduce thefrequency of the episodes and control the pain.Patients who report one to two outbreaks a year
may be instructed to use over-the-counter localanesthetics (such as 10% benzocaine), viscouslidocaine, or mucoadhesive agents such as poly-vinylpyrrolidone sodium hyaluronate (Gelclair®,Helsinn Healthcare SA, Lugano, Switzerland)and methylcellulose paste (Orabase Paste®
Colgate, Colgate-Palmolive Company, New York).Amlexanox is a prescription medication withanti-inflammatory properties incorporated in amucoadhesive agent that has shown some effec-tiveness (OraDisc A™, Access PharmaceuticalsInc., Addison, TX). Reassurance and patienteducation on the condition are also indicated.Patients with more frequent and severe episodesmay be treated with topical corticosteroids andother immunosuppressive agents to shorten theduration and size of the ulcers (Baccaglini et al.2011; Scully et al. 2003). High-potency topicalsteroids (betamethasone, clobetasol, or fluo-cinonide) are usually applied on the affectedarea two to three times daily after meals. Largerand recalcitrant ulcers (such as the ones observedin the major form) can be treated by intralesionaltherapy such as triamcinolone injections at10 mg per cm2 of ulceration (Table 3). Systemictherapy for severe outbreaks that do not respondto topical measures can be managed with pred-nisone (usually at 1 mg/kg), pentoxifylline, dap-sone, colchicine, azathioprine, or thalidomide.Due to possible side effects with these medica-tions, patients should be carefully monitoredlong term. Thalidomide is indicated for patientswith severe or major RAS cases who failed othertreatments (Hello et al. 2010). Thalidomide
Fig. 14 Spontaneous healing of an aphthous lesion on the buccal mucosa at initial presentation (a) and 10 days later (b)
Fig. 13 Severe recurrent aphthous stomatitis on the uvula,palatoglossal arches, and soft palate
Oral Ulcerative Lesions 11
causes severe birth defects, and as such womenof childbearing age must agree to use two formsof contraception. In the United States, cliniciansprescribing thalidomide must be registered in theREMS (Risk Evaluation and Mitigation Strat-egy) program for thalidomide. Noteworthy, theevidence supporting such treatments are scarce,as showed by a Cochrane review in 2012(Table 4).
Aphthous Stomatitis Associatedwith Systemic Conditions
Gastrointestinal Disorders
Aphthous lesions are often reported as common ininflammatory bowel diseases (IBD) and celiacdisease (CD); thus it is not unusual that a patientwith an established gastrointestinal disorderreports recurring oral ulcers with an aspectrecalling common aphthae. In addition, aphthouslesions can represent early features of these intes-tinal conditions and thus suggestive of these dis-eases (Fasano and Catassi 2012; Kalla et al. 2014).For such reasons, when a patient reports abdom-inal pain, persistent diarrhea, and weight loss,
together with oral aphthous lesions, the clinicalsuspicion of IBD or CD should be considered(Scully 2006). In these patients, aphthous lesionscan be either proper extraintestinal manifestationsof the gastrointestinal disturbance or signs ofnutritional and hematological deficiencies due tothe malabsorption of micronutrients, a typicalcomplication of such conditions (Slebioda et al.2014) (Table 5).
Inflammatory Bowel Disease (IBD)Inflammatory bowel disease (IBD) is a broad termto define chronic or recurring inflammation of thegastrointestinal tract, due to the dysregulation ofmucosa immune cells. IBD include two types ofchronic intestinal disorders, Crohn’s disease andulcerative colitis, two chronic inflammatory dis-eases of the digestive tract likely to originate froman inappropriate inflammatory response to intes-tinal microbes in a genetically susceptible hostwhich can be differentiated by means of the loca-tion of lesions along the gastrointestinal tract, aswell as histological features (Abraham and Cho2009). About one-third of IBD patients also dis-play a wide range of extraintestinal manifesta-tions, which mainly involve the joints, skin, oralmucosa, eyes, and liver. Focusing on oral
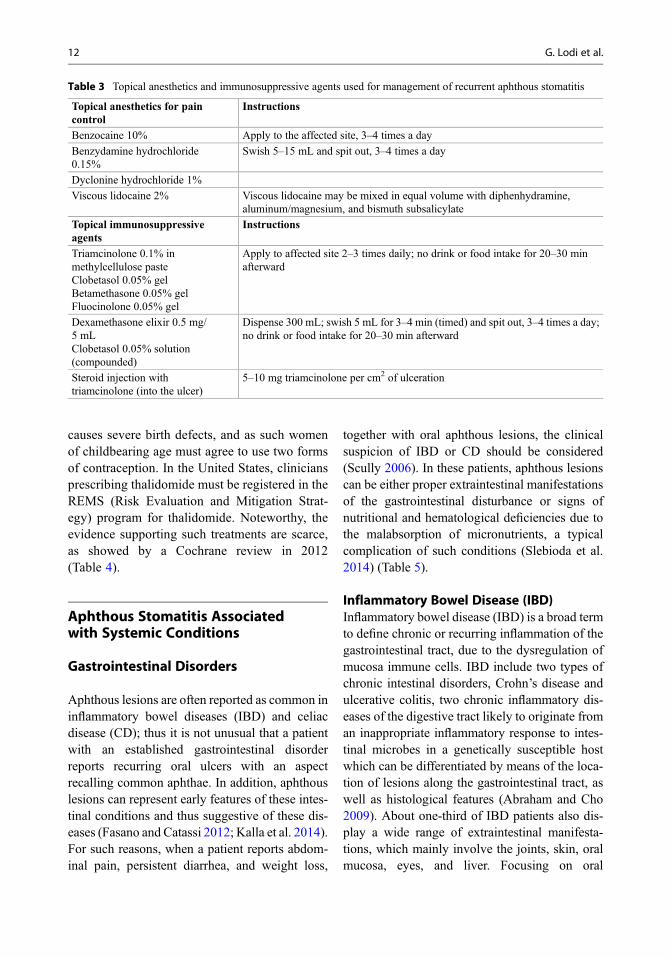
Table 3 Topical anesthetics and immunosuppressive agents used for management of recurrent aphthous stomatitis
Topical anesthetics for paincontrol
Instructions
Benzocaine 10% Apply to the affected site, 3–4 times a day
Benzydamine hydrochloride0.15%
Swish 5–15 mL and spit out, 3–4 times a day
Dyclonine hydrochloride 1%
Viscous lidocaine 2% Viscous lidocaine may be mixed in equal volume with diphenhydramine,aluminum/magnesium, and bismuth subsalicylate
Topical immunosuppressiveagents
Instructions
Triamcinolone 0.1% inmethylcellulose pasteClobetasol 0.05% gelBetamethasone 0.05% gelFluocinolone 0.05% gel
Apply to affected site 2–3 times daily; no drink or food intake for 20–30 minafterward
Dexamethasone elixir 0.5 mg/5 mLClobetasol 0.05% solution(compounded)
Dispense 300 mL; swish 5 mL for 3–4 min (timed) and spit out, 3–4 times a day;no drink or food intake for 20–30 min afterward
Steroid injection withtriamcinolone (into the ulcer)
5–10 mg triamcinolone per cm2 of ulceration
12 G. Lodi et al.
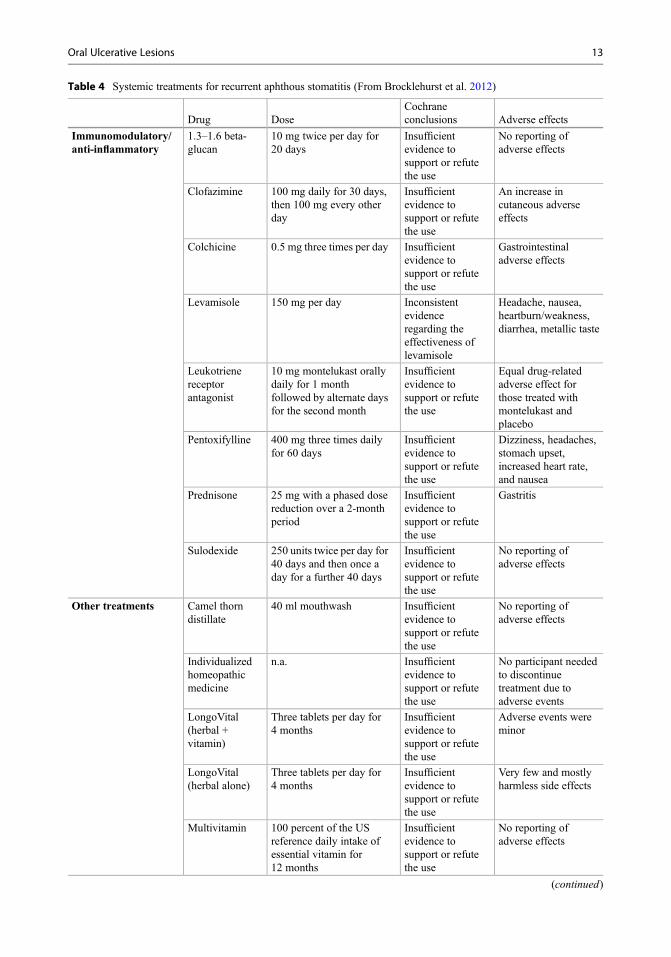
Table 4 Systemic treatments for recurrent aphthous stomatitis (From Brocklehurst et al. 2012)
Drug DoseCochraneconclusions Adverse effects
Immunomodulatory/anti-inflammatory
1.3–1.6 beta-glucan
10 mg twice per day for20 days
Insufficientevidence tosupport or refutethe use
No reporting ofadverse effects
Clofazimine 100 mg daily for 30 days,then 100 mg every otherday
Insufficientevidence tosupport or refutethe use
An increase incutaneous adverseeffects
Colchicine 0.5 mg three times per day Insufficientevidence tosupport or refutethe use
Gastrointestinaladverse effects
Levamisole 150 mg per day Inconsistentevidenceregarding theeffectiveness oflevamisole
Headache, nausea,heartburn/weakness,diarrhea, metallic taste
Leukotrienereceptorantagonist
10 mg montelukast orallydaily for 1 monthfollowed by alternate daysfor the second month
Insufficientevidence tosupport or refutethe use
Equal drug-relatedadverse effect forthose treated withmontelukast andplacebo
Pentoxifylline 400 mg three times dailyfor 60 days
Insufficientevidence tosupport or refutethe use
Dizziness, headaches,stomach upset,increased heart rate,and nausea
Prednisone 25 mg with a phased dosereduction over a 2-monthperiod
Insufficientevidence tosupport or refutethe use
Gastritis
Sulodexide 250 units twice per day for40 days and then once aday for a further 40 days
Insufficientevidence tosupport or refutethe use
No reporting ofadverse effects
Other treatments Camel thorndistillate
40 ml mouthwash Insufficientevidence tosupport or refutethe use
No reporting ofadverse effects
Individualizedhomeopathicmedicine
n.a. Insufficientevidence tosupport or refutethe use
No participant neededto discontinuetreatment due toadverse events
LongoVital(herbal +vitamin)
Three tablets per day for4 months
Insufficientevidence tosupport or refutethe use
Adverse events wereminor
LongoVital(herbal alone)
Three tablets per day for4 months
Insufficientevidence tosupport or refutethe use
Very few and mostlyharmless side effects
Multivitamin 100 percent of the USreference daily intake ofessential vitamin for12 months
Insufficientevidence tosupport or refutethe use
No reporting ofadverse effects
(continued)
Oral Ulcerative Lesions 13

involvement of IBD, pediatricians and dentistsplay a critical role in the diagnosis of oral mani-festations as an early sign of IBD. The prevalenceof IBD is increasing worldwide, and it is higher inindustrialized countries. In particular, the
prevalence of Crohn’s disease has been estimatedto be around 30–50 cases in 100,000 inhabitantsin Western countries (Laranjeira et al. 2015). InEurope, the prevalence has been attested around6.3 in 100,000 individuals (Burisch et al. 2013),
Table 4 (continued)
Drug DoseCochraneconclusions Adverse effects
Propolis 500 mg per day Insufficientevidence tosupport or refutethe use
Low rates of minimalside effects
Sub-antimicrobialdoxycycline
20 mg twice daily for90 days
Insufficientevidence tosupport or refutethe use
No differences inadverse eventscompared withplacebo
Tetracyclinesuspension
25 mg four times per dayfor 5 days
Insufficientevidence tosupport or refutethe use
No differences inadverse eventscompared withplacebo
Vitamin B12 1000 mcg daily for6 months
Insufficientevidence tosupport or refutethe use
No reporting ofadverse effects
Table 5 Clinical manifestations of inflammatory bowel diseases (IBD), i.e., Crohn’s disease and ulcerative colitis.Extraintestinal manifestations occur more frequently in patients affected by Crohn’s disease than ulcerative colitis
Gastrointestinalmanifestations
Extraintestinalmanifestations
Abdominal pain – alteredbowel habits
Joint (arthritis, spondylitis,back pain)
Bloody diarrhea, weightloss
Liver (hepatobiliarydisorders, fatty liver)
Fever, occasionally Eye (uveitis)
Skin (pyodermagangrenosum)Oral mucosa
Specific Indurated tag-like lesions
Cobblestoning
Orofacial Crohn’s disease (granulomatosis)
Granular cheilitis
Lip swelling with vertical fissures
Pyostomatitis vegetans
Non specific Aphthous stomatitis
Angular cheilitis
Persistent submandibular lymphadenopathy
Recurrent buccal abscesses
Perioral erythema
Malabsorption-related oral changes (glossitis, oralcandidosis, angular cheilitis)
14 G. Lodi et al.
while in the United States is 201 per 100,000adults (National Center for Chronic Disease Pre-vention and Health Promotion 2015). For ulcera-tive colitis, in Europe, the prevalence is 11.4 per100,000 individuals (Burisch et al. 2013), while inthe United States is 238 per 100,000 adults, with-out significant difference between sexes (NationalCenter for Chronic Disease Prevention and HealthPromotion 2015).
Etiology of IBD, most likely multifactorial, isstill unknown, where several factors such assmoking habit, diet, and geographic and socialenvironment play a pivotal, triggering role(Lankarani et al. 2013). Though not clearly eluci-dated yet, the pathogenesis appears related tooverly aggressive acquired immune responses toa subset of commensal enteric bacteria developedin genetically susceptible hosts and environmen-tal factors which precipitate the onset orreactivation of disease (Lankarani et al. 2013).
• Genetics – Four genes (CARD15, SLC22A4and SLC22A5, DLG5, PPARG) have beenassociated with Crohn’s disease and one withulcerative colitis (MDR1), which regulateinnate immune responses, bacterial killing,and immune responses to microbial antigensand epithelial function (Sartor 2006).
• Immune response – Crohn’s disease and ulcer-ative colitis show enhanced local recruitmentand retention of effector macrophages, neutro-phils, and T cells and then activated and ableto release pro-inflammatory cytokines (Sartor2006). Crohn’s disease is mainly a TH1- andTH17-mediated process, while ulcerative coli-tis is an atypical TH2 disorder: although directevidence of defective regulatory T-cell func-tion is lacking in either disease, a plethora ofstudies support deficiency in innate immuneresponses in Crohn’s disease (Sartor 2006).
• Commensal microbial stimulants – Entericmicroflora can stimulate immune responseseither by functioning as adjuvants, activatinginnate immune responses (such as dendriticcells) or antigens, or stimulating the clonalexpansion of T cells that selectively recog-nize the antigen through their T-cell receptor(Sartor 2006).
• Environmental triggers – These factors includesmoking, which is protective in ulcerative coli-tis but detrimental in Crohn’s disease, diet,the use of antibiotics and nonsteroidal anti-inflammatory drugs (NSAIDs), stress, andinfection (Sartor 2006).
Even if mechanisms which initiate the onset ofdisease or reactivate quiescent IBD are not wellunderstood, from a broad perspective, these trig-gering factors alter mucosal barrier integrity,immune responses, or the luminal microenviron-ment, each of which has an impact on susceptibil-ity to inflammation (Sartor 2006).
The basis of an accurate diagnosis of IBDis focused on clinical presentation, colonoscopy,and biopsy of ulcer tissue (Scully 2006), in com-bination, because there is no unique manifestationof IBD. Colonoscopy reveals inflammatory lesionssurrounded by normal mucosa, which initiallyappear as spherical aphthoid erosions, then per-sisting invariant or progressing to form ulcers(Jung 2012). If mucosal inflammation and edemaincrease in correlation to activity of IBD, theintestinal mucosa shows a nodular surface witha cobblestone appearance (Jung 2012). Crohn’sdisease can affect any part of the digestive tract,while ulcerative colitis is limited to the colon andrectum (Baumgart and Sandborn 2007). Biopsy isusually performed on areas beyond erosions orulcers, which has the highest potential for detectinggranuloma, in turn difficult to find in the cob-blestone mucosa (Jung 2012). Histologically,ulcerative colitis displays chronic inflammatorylesions restricted to the mucosal epithelium,while Crohn’s disease affects the full thicknessof the bowel wall (Baumgart and Sandborn 2007).
EpidemiologyThe global prevalence of the oral manifestation ofIBD in adults varies from 5% to 50% (Katsanoset al. 2015; Lankarani et al. 2013); this wide rangeresults from several reports that also include non-specific oral manifestations of IBD, which mightbe related to medical treatment or derived fromother etiologies. IBD prevalence is higher in chil-dren than in adults and in Crohn’s disease than in
Oral Ulcerative Lesions 15
ulcerative colitis (Katsanos et al. 2015; Lankaraniet al. 2013; Pittock et al. 2001).
Aphthae may occur in 10–30% of adultpatients with Crohn’s disease and in a signifi-cantly smaller proportion of subjects with ulcera-tive colitis (Akintoye and Greenberg 2014;Katsanos et al. 2015; Lankarani et al. 2013; Singhet al. 2015). This frequency is not significantlydifferent than in the unaffected population(Bradley et al. 2004). However, in a recentTurkish study, aphthous stomatitis (40.2%) wasthe most common mucocutaneous manifestationreported in both ulcerative colitis (44.6%) andCrohn’s disease (33.3%), and no relationshipwas found between mucocutaneous manifesta-tions and age, duration of disease, activity indices,or location of IBD (Topaloğlu Demir et al. 2014).
EtiopathogenesisThe pathogenesis of the IBD oral manifestationsis still unclear. In Crohn’s disease, pathologicalfeatures of aphthae include, as highlighted by oralmucosa biopsies: (i) granuloma formation, simi-larly to that observed in intestinal lesions, (ii) thepresence of lymphocytes around vessels in thesubepithelial tissue and of plasma cells con-taining IgM, and (iii) a decreased heat shock
protein 27 (HSP27) expression compared to con-trols (Katsanos et al. 2015).
Only weak evidence supports a genetic pre-disposition for oral manifestations, though studiesshow altered patterns of T-cell cytokine pro-duction leading to loss of tolerance to oral anti-gens, association between HLA-B27 and IBDextraintestinal symptoms, and DRB1*0103 alleleincrease in patients with ulcerative colitis com-plaining of oral ulcers (Katsanos et al. 2015).
Increased frequency of oral manifestationsamong IBD patients has been recently correlatedwith aberrations in the oral salivary microbiota,where Bacteroidetes was significantly increasedwith a concurrent decrease in Proteobacteria(Katsanos et al. 2015).
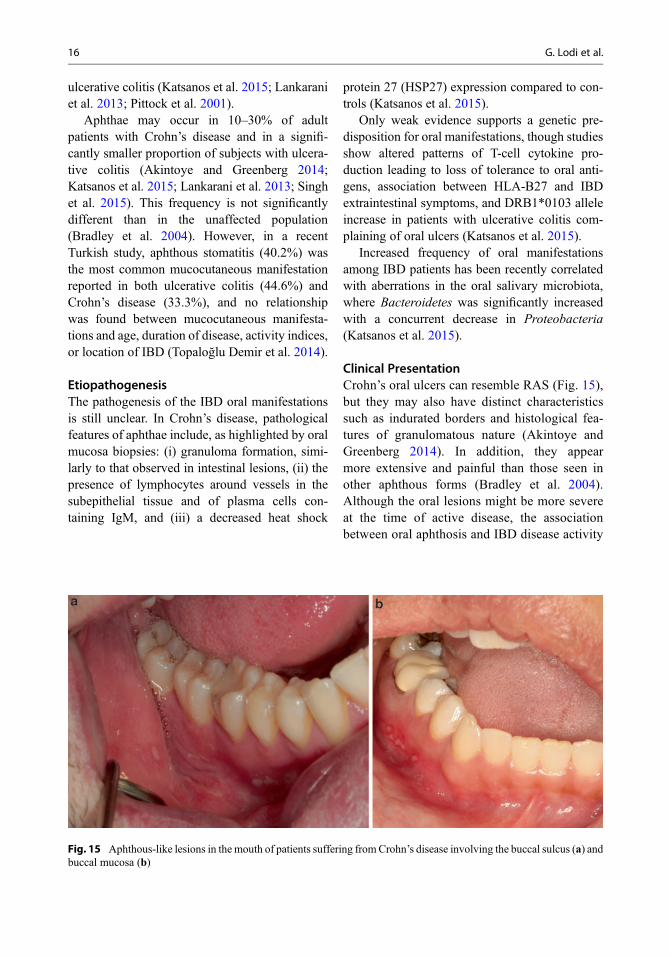
Clinical PresentationCrohn’s oral ulcers can resemble RAS (Fig. 15),but they may also have distinct characteristicssuch as indurated borders and histological fea-tures of granulomatous nature (Akintoye andGreenberg 2014). In addition, they appearmore extensive and painful than those seen inother aphthous forms (Bradley et al. 2004).Although the oral lesions might be more severeat the time of active disease, the associationbetween oral aphthosis and IBD disease activity
Fig. 15 Aphthous-like lesions in the mouth of patients suffering fromCrohn’s disease involving the buccal sulcus (a) andbuccal mucosa (b)
16 G. Lodi et al.
is not clear, and data are still controversial(Akintoye and Greenberg 2014; Katsanos et al.2015).
IBD can display other oral lesions differentfrom aphthous ulcers (Katsanos et al. 2015;Lankarani et al. 2013), which are more commonin patients suffering from Crohn’s disease thanin subjects with ulcerative colitis, particularlyin Crohn’s disease patients with proximalgastrointestinal tract and/or perianal involve-ment (Lankarani et al. 2013) These include cob-blestoned buccal mucosa, granular cheilitis,and granular gingival swelling, similar to oro-facial granulomatosis (Katsanos et al. 2015).Pyostomatitis vegetans is another specific finding,which can be typically associated with bothCrohn’s disease and ulcerative colitis (Katsanoset al. 2015).
Subjects with extraintestinal manifestationsof IBD seem to be more likely to suffer froma combination of these; thus IBD patients withaphthae may have concomitantly extraintestinalmanifestations including peripheral and axialarthropathies, erythema nodosum, uveitis, and pri-mary sclerosing cholangitis (Veloso et al. 1996).In addition, aphthous ulcers, as extraintestinalmanifestations of IBD, usually parallel the diseaseactivity of IBD, occurring during active intestinaldisease and responding favorably to its treatment(Veloso et al. 1996).
Oral Lesions in the Diagnosis of IBDNormally, intestinal involvement precedes oralmanifestations; however in 5–10% of IBD casesand in up to 60% in patients with Crohn’s disease(Lankarani et al. 2013), the specific oral mani-festations may precede gastrointestinal symp-toms by many years. It has been estimated that10–37% of children who receive a diagnosisof orofacial granulomatosis may start sufferingfrom Crohn’s disease in the following years(Katsanos et al. 2015). In the presence oforal manifestations, histological examination isonly recommended for lesions suggestive ofgranulomatosis. Although it is not possible todistinguish orofacial granulomatosis and oralCrohn’s disease just on the basis of histolo-gical features, referral to a gastroenterologist is
recommended when the presence of granulomatosisis confirmed in a patient with bowel features sug-gestive of IBD (such as persistent diarrhea).
To date, it is not possible to distinguish patientswith RAS from those with aphthous-like ulcers ofthe mouth who are likely to develop IBD. Sincethe buccal epithelium of children with Crohn’sdisease appears immunologically more reactivewhen compared to that of adult patients, showingoverproduction of certain chemokines (CXCL-8,CXCL-9, and CXCL-10), it has been hypothe-sized that these could be used as a screening toolfor children with IBD and RAS (Katsanos et al.2015). Similarly, levels of tumor necrosis factor-α(TNF-α), found to be higher in the mucosa ofpatients with Crohn’s disease and oral aphthae,could also contribute to recognize immune-mediated oral ulcers associated with this condition(Bradley et al. 2004).
Patient ManagementManagement of Crohn’s disease is based mainlyon anti-inflammatory and immunosuppressivetopical and systemic therapies as well as dietaryadvice, including elimination of cinnamon, ben-zoate, glutaminate, cocoa, and with micronu-trient supplementation. The medical therapies forCrohn’s disease are usually sufficient also forthe control of oral manifestations of the disease(Veloso et al. 1996). Oral aphthosis usuallyresolves in most treated children, despite that upto 30% of affected patients, especially pediatricones, may continue to manifest oral lesions afterdisease control (Lankarani et al. 2013). In suchcases where specific oral manifestations, suchas cobblestoned mucosa, granulomatosis, andlip and facial swelling, are refractory and uncom-fortable, as well as in those cases where oralaphthae are recurrent and severe, local treatmentfor pain and discomfort relief is indicated. It canbe easily achieved by topical applicationof anesthetic drugs (lidocaine gel) and anti-inflammatory drugs, mainly steroids, such as tri-amcinolone or dexamethasone ointments, up tothree times/day for about 10 days (Akintoye andGreenberg 2014). Systemic or intralesional ste-roids and other immunomodulators are alsorecommended for severe refractory and/or
Oral Ulcerative Lesions 17

persistent cases not responding to topical thera-pies (Akintoye and Greenberg 2014).
Celiac Disease (CD)CD is a chronic, multisystem, immune-mediateddisease of the small intestine triggered in geneti-cally predisposed individuals by exposure todietary gluten, particularly to gliadin, a specificgluten protein which belongs to the group of pro-lamins (Gujral et al. 2012). The latter are plantstorage proline-rich proteins present in wheat, rye,and barley. Originally thought to affect whiteEuropeans solely, CD is nowadays widely distrib-uted globally, becoming a frequent food intoler-ance. The worldwide mean prevalence of CDhas been reported to range from 0.5% to 1%,depending on the population under investigation.The prevalence of 1% reflects figures in Europeand North America (Gujral et al. 2012). In thegeneral population, high-risk groups for CDare those with familial history of biopsy-provenCD or affected by type 1 diabetes or systemicautoimmune disorders such as thyroiditis (Gujralet al. 2012).
The pathogenesis of CD is dependent on both astrong genetic predisposition and environmentaltriggers. The primary environmental factor is theingestion of food containing gluten, while themain genetic factor is the class II major histo-compatibility complex HLA- DQ2 or DQ8genes, also shared in patients with type 1 diabetesand other systemic autoimmune disorders (Gujralet al. 2012; Lionetti et al. 2014). A recent random-ized clinical trial on infants at high risk of CDindicated that a high-risk HLA genotype was apivotal predictor of disease, while the delayedintroduction of gluten in the diet did not modifyrisk of developing the disease, although it wasassociated with a delayed onset of disease(Lionetti et al. 2014).
Several pathways have been involved in CDpathogenesis. Besides the direct toxicity of gliadinagainst the enterocytes, gliadin peptides appearedto upregulate stress molecules in intraepitheliallymphocytes, promoting a lymphocyte-mediatedcytotoxic response against enterocytes (Barkerand Liu 2008). Moreover, the structure of gliadinitself, unusually rich in proline residues, results
in an intrinsic resistance to gastrointestinal diges-tion, along with a preference for binding toDQ2 molecules, further mediating autoimmuneinflammation (Barker and Liu 2008). An additio-nal, pivotal pathway for CD development involvestransglutaminase (tTG), a calcium-dependentenzyme. tTG has the main molecular role ofcross-linking and deamidation of gliadin, pro-ducing an epitope that binds efficiently to DQ2and is recognized by gut-derived gliadin-reactiveCD-4+ T cells (Barker and Liu 2008). tTG auto-antibodies, as immunoglobulin A (IgA), occurbecause antigen-presenting cells “inadvertently”target tTG-gliadin complexes, resulting in animmune reaction against both gliadin and tTG(Barker and Liu 2008). tTG IgA, detectable inthe serum of almost all CD individuals is alsoassociated to extraintestinal symptoms of CD,which can deposit in the liver, kidney, lymphnodes, and muscles (Gujral et al. 2012). tTG IgAdisappears slowly from the bloodstream, when thepatient is under a gluten-free diet.
EpidemiologyWeight loss or other signs of malabsorption maybe suggestive of the presence of CD in a patientwith oral aphthae, even though this disease hasbeen detected in less than 5 percent of patientswith RAS referred to a hospital clinic for exami-nation (Scully 2006).
Dental enamel defects and oral aphthae repre-sent the two most common oral manifestationsassociated with CD. The prevalence of dentalenamel defects in CD patients with mixed or per-manent dentition ranges widely, from 9.5% to95.9%, while in patients with deciduous teeth, itdecreases to 5.8–13.3% (Rashid et al. 2011). Suchdifference is due to the difference in time of erup-tion, and the fact that crowns of permanent teethdevelop within the seventh year of age after theintroduction of dietary gluten in the child, and thedevelopment of deciduous teeth occurs primarilyin utero, in the absence of gluten gastrointestinalexposure of the fetus. Regarding oral aphthae,figures are difficult to extrapolate, since severalreports fail to specify the exact diagnostic criteriaused. Some controlled studies, however,suggested a higher frequency of recurrent oral
18 G. Lodi et al.

ulcers in CD patients compared with controlgroups (Baccaglini et al. 2011; de Carvalho et al.2015). Excluding case reports, studies investigat-ing the prevalence of CD in patients with RASprovide a broad range of estimates, ranging from4% to 40% (Baccaglini et al. 2011). Conversely,studies on the prevalence of RAS in patients withCD show that the number of subjects who haveRAS ranges from 3% to 61% (Baccaglini et al.2011), while in a large survey of a Canadianpopulation with biopsy-proven CD, 16% of chil-dren and 26% of adults reported suffering fromrecurrent oral ulcers (Rashid et al. 2011).
EtiopathogenesisThe exact cause of aphthous ulcers in CD isunknown, although they have been related mainlywith hematinic deficiencies, including low serumiron, folic acid, and vitamin B12 due to malab-sorption in patients with untreated CD (see recur-rent aphthous stomatitis and deficiencies ofmicronutrients). Similarly, the exact mechanismleading to dental defects is largely unclear.Immune-mediated damage has been proposedto be the primary cause, though nutritional dis-turbances, putatively producing hypocalcemiaand vitamin insufficiencies, as well as gluten-dependent stimulation of oral naïve lymphocytescannot be completely ruled out (Rashid et al. 2011).
Clinical PresentationAphthous ulcers and dental enamel defects belongto a group of well-documented dental and oralmucosa manifestations of CD (Table 6). The pres-ence of recurrent aphthous lesions, especially inindividuals with dental enamel defects, is nowconsidered a significant condition for suspecting
CD. Interestingly, in around one-fifth of cases,oral ulcers can represent the first sign of CD;several authors have reported cases of patientspresenting with recurrent oral ulceration who sub-sequently received a diagnosis of CD (Baccagliniet al. 2011). Clinically, the features of oralaphthous lesions in CD are not far from theclassical picture of idiopathic oral aphthae; theyhave been mostly described as minor RASalthough, as mentioned above, most studies havenot reported well-defined criteria for diagnosis ofRAS (Baccaglini et al. 2011).
If CD appears in children, when permanentteeth are developing, abnormalities in the struc-ture of the dental enamel can arise, usuallysymmetrically and chronologically in all fourquadrants. Typical aspects include enamel hypo-plasia and hypomineralization, with pitting,grooving, and sometimes complete loss of enamel(Rashid et al. 2011). A classification of these CDdental defects has been developed (Table 6) (Aineet al. 1990), which are less frequent in adults withCD, due to the fact that CD onset may haveoccurred after dentition development or mayhave had affected restored or extracted teeth(Rashid et al. 2011).
Oral Lesions in the Diagnosis of CeliacDiseaseThe clinician should always consider CD amongdifferential diagnosis in any patient presentingwith dental enamel defects and recurrent aphthouslesions, since their association is considered spe-cific to CD. The presence of a hereditary case ofCD or concomitant autoimmune diseases, espe-cially type 1 diabetes, will further increase theprobability of CD.
Table 6 Oral and dental lesions associated with celiac disease
Oral mucosa lesions Dental lesions
Recurrent aphthous ulcersCheilosisAtrophic glossitis
Delayed dental eruptionEnamel defects (classification according to Aine (de Carvalho et al. 2015):Grade I: defects in color of enamel – single or multiple cream, yellow or brown
opacitiesGrade II: slight structural defects – rough enamel surface, horizontal grooves, shallow
pitsGrade III: evident structural defects – deep horizontal grooves and vertical pitsGrade III: severe structural defects – shape changes
Oral Ulcerative Lesions 19

Children with a documented history of RASand signs of malabsorption should undergo a den-tal examination and, if presenting with enameldefects, should be referred to a gastroenterologistwho may confirm the diagnosis of CD by per-forming laboratory and instrumental evaluations(Marty et al. 2016). While awaiting diagnosticconfirmation of CD, the clinician should not rec-ommend a gluten-free diet for the patient (Rashidet al. 2011).
Oral health-care providers play an importantrole in detecting both classical and atypical casesof CD, contributing to decreasing diagnosticdelay, which is still high. Delay in CD diagnosiscan lead to a plethora of complications, fromanemia to osteoporosis and, in worse cases, repro-ductive disorders and increased risk of developingintestinal malignancies such as small intestineadenocarcinoma and lymphoma (Green andCellier 2007; Rashid et al. 2011).
Patient ManagementCurrently, the main therapeutic intervention forCD is a gluten-free diet. Adherence to a gluten-free diet improves gastrointestinal symptomsand may also reduce frequency and severity ofaphthous ulcers, although this has not been con-firmed in all reports (de Carvalho et al. 2015). Theresponse to therapy is poor in up 30% of patients(refractory form of CD), mainly due to lack ofcompliance with diet (Green and Cellier 2007).
Severe and persistent aphthae can oftenbe managed as idiopathic forms of RAS, usingtopical antiseptic and steroid medicamentsand reserving systemic therapies for severe,non-respondent cases.
Behçet Syndrome
Behçet syndrome or Behçet disease (BD) is aninflammatory multisystemic disorder with vascu-lar, articular, gastrointestinal, neurologic, urogen-ital, pulmonary, and cardiac involvement. Thedisease was first described in 1937 by the Turkishdermatologist, Hulusi Behçet, as a triad of symp-toms, namely, recurrent oral ulcers, genital ulcers,and uveitis (Behçet 1937).
EpidemiologyThe onset of BD usually occurs in the third orfourth decade of life. BD is seen worldwide,although it is a rare condition. It has a typicalgeographic distribution, with an increased preva-lence in people with ancestors who lived in theSilk Route, which extended from Japan to theMiddle East and Mediterranean countries. Turkeyhas the highest prevalence, with a prevalence inthe population aged 12 years or older of420/100,000 (Azizlerli et al. 2003). The diseaseis rarely observed in Western countries: the prev-alence of BD is approximately 0.64/100,000 inthe United Kingdom and 0.12–0.33/100,000 inthe United States (Sakane et al. 1999). The overallgender distribution has been reported to beroughly equal, but some regional variability alsoexists. BD shows a male predominance in certainMiddle East and Mediterranean countries and afemale predominance in Japan and South Korea(Bang et al. 2003).
There is a strong association between thegeographic distribution of human leukocyteantigen HLA-B51 and the prevalence of BD.The frequency of HLA-B51 along the Silk Routeranges between 20% and 25% among the gen-eral population and 50–80% among patientswith BD (Alpsoy 2016). In contrast, the fre-quency of HLA-B51 in Northern Europe and theUnited States is around 2–8% in the general pop-ulation and 15% among patients with BD (Dalviet al. 2012).
EtiopathogenesisThe etiology of BD is unknown. The most widelyaccepted theory behind its pathogenesis is thatan environmental stimulus elicits an abnormalimmune response in a genetically susceptiblehost. The presence of HLA-B51 is still consideredthe strongest susceptibility factor for BD, assubjects carrying this gene have a signifi-cantly increased risk of developing this condition(de Menthon et al. 2009). The presence ofHLA-B51 alone is not sufficient to explain theetiology of the disease in all cases; only 60% ofpatients with BD express HLA-B51, and thisHLA allele is seen frequently in the absence ofthe disease (Keogan 2009). These data suggest
20 G. Lodi et al.
that other susceptibility genes or genetic varia-tions may also be involved.
It has also been suggested that environmentalfactors may play a pivotal role in the pathogenesisof BD. The presence of HSV-1-infected cells andthe load of Streptococcus species, particularlyS. sanguinis, have been found to be higher inpatients with BD compared to controls. However,their role in the etiology of the disease remains tobe determined. A clinical hypothesis is that infec-tious agents and associated stress proteins foundin the oral cavity of patients with BD induce cross-reactivity with host cells and stimulate the prolif-eration of autoreactive T-cell clones. Heat shockproteins can be recognized by pattern recognitionreceptors as an endogenous “danger” signal, lead-ing to activation of innate and adaptive immuneresponses. They also increase the expression ofadhesion molecules on endothelial cells. Over-expression of pro-inflammatory cytokines (mainlyIL-17, IL-23, and interferon-γ) appears to beresponsible for the enhanced inflammatory reac-tion. Increased neutrophil activity and neutrophilinfiltration in affected organs may be caused byincreased IL-17 response. This inflammatory pro-cess eventually results in tissue damage and vas-culitis (Keogan 2009).
Clinical PresentationBD is characterized by unpredictable exacerba-tions and remissions and presents with a widespectrum of clinical manifestations. It is associ-ated with increased mortality due to involvementof the central nervous system, lungs and largevessels, bowel perforation, and gastrointestinalhemorrhage (Keogan 2009). Mucocutaneouslesions constitute the hallmark of BD. Oral ulcersare the most common feature, affecting 92–100%of the patients, followed by genital ulcers(57–93%) and cutaneous lesions (38–99%)(Alpsoy et al. 2007). Ocular and articular involve-ments are also frequent traits of the disease.
No specific histopathological features havebeen described in BD. Large vessel involvementis generally characterized by vasculitis withthrombosis or aneurysm, while the mucocutane-ous lesions often display leukocytoclastic vascu-litis or a neutrophilic vascular reaction.
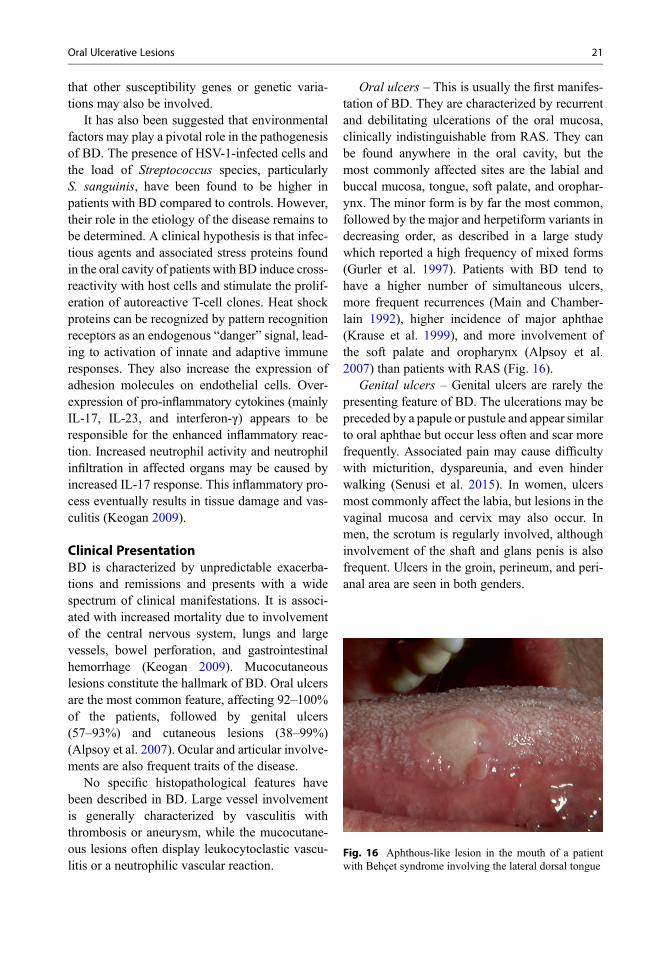
Oral ulcers – This is usually the first manifes-tation of BD. They are characterized by recurrentand debilitating ulcerations of the oral mucosa,clinically indistinguishable from RAS. They canbe found anywhere in the oral cavity, but themost commonly affected sites are the labial andbuccal mucosa, tongue, soft palate, and orophar-ynx. The minor form is by far the most common,followed by the major and herpetiform variants indecreasing order, as described in a large studywhich reported a high frequency of mixed forms(Gurler et al. 1997). Patients with BD tend tohave a higher number of simultaneous ulcers,more frequent recurrences (Main and Chamber-lain 1992), higher incidence of major aphthae(Krause et al. 1999), and more involvement ofthe soft palate and oropharynx (Alpsoy et al.2007) than patients with RAS (Fig. 16).
Genital ulcers – Genital ulcers are rarely thepresenting feature of BD. The ulcerations may bepreceded by a papule or pustule and appear similarto oral aphthae but occur less often and scar morefrequently. Associated pain may cause difficultywith micturition, dyspareunia, and even hinderwalking (Senusi et al. 2015). In women, ulcersmost commonly affect the labia, but lesions in thevaginal mucosa and cervix may also occur. Inmen, the scrotum is regularly involved, althoughinvolvement of the shaft and glans penis is alsofrequent. Ulcers in the groin, perineum, and peri-anal area are seen in both genders.
Fig. 16 Aphthous-like lesion in the mouth of a patientwith Behçet syndrome involving the lateral dorsal tongue
Oral Ulcerative Lesions 21

Ocular lesions – Ocular disease is seen in30–70% of patients and is more frequent andsevere in men. Typically, ocular symptoms beginafter the onset of oral ulceration. However, intra-ocular inflammation is the presenting feature inapproximately 20% of cases. Ocular disease isbilateral in 85% of patients and runs a relapsingcourse in 95% of cases (Kitaichi et al. 2007).Severity may differ between the eyes. Panuveitis,posterior uveitis, anterior uveitis, retinal vasculi-tis, optic neuritis, and retinal vein occlusion arethe most common features and cause significantmorbidity. Formation of a hypopyon, a visiblelayer of pus in the anterior chamber, is seen in
12% of patients and rarely in other conditions(Tugal-Tutkun et al. 2004) (Fig. 17).
Cutaneous lesions – Skin lesions are describedin approximately 80% of patients withBD. Erythema nodosum-like lesions are seen in30% of patients, mainly on the lower extremitiesbut also on the face, neck, and buttocks. Lesionsrarely ulcerate, resolve within 2–3 weeks, andcan cause post-inflammatory hyperpigmentation.While clinically similar to classical erythemanodosum, lesions of BD differ histologically, withevidence of vasculitis (Kim and LeBoit 2000).Other common skin lesions include papulopustularlesions, superficial thrombophlebitis, and pathergy.
Fig. 17 Ocular lesions of Behçet syndrome. (a) Mildconjunctival injection and hypopyon, (b) retinal hemor-rhage associated with retinal vasculitis, and (c) retinal
vasculitis (demonstrated by fluorescein angiography)(Images courtesy of Dr. Hiroshi Goto, Tokyo MedicalUniversity)
22 G. Lodi et al.

DiagnosisSince there are no pathognomonic signs nor anyspecific laboratory, radiologic, or histologic find-ings for BD, the diagnosis is purely based onthe recognition of clinical findings together withthe exclusion of other conditions. Despite largeresearch efforts over the past few decades, nouniversally accepted diagnostic criteria exist forBD, as documented by the existence of 17 sets ofdiagnosis/classification criteria (Davatchi et al.2015). The criteria proposed in 1990 by the Inter-national Study Group (ISG) for Behçet Disease(International Study Group for Behçet Disease1990) remain the most widely used among experts(Table 7). Recently, the International Team for theRevision of the International Criteria for BehçetDisease (ICBD) published new criteria (Interna-tional Team for the Revision of the InternationalCriteria for Behçet Disease 2014), where oralulcers, genital ulcers, and ocular lesions receivetwo points each and other manifestations (cutane-ous lesions, neurologic and vascular involvement,and positive skin pathergy test) receive one pointeach. If a patient receives four points or more, thepatient is diagnosed with BD. It has been shownthat the ICBD criteria are more sensitive but lessspecific than the ISG criteria, which may causeoverdiagnosis.
Patient ManagementNo curative therapy is currently available forBD. The ultimate goals of treatment are to prevent
irreversible organ damage, which occurs espe-cially in the early stage and active phases of thedisease, and to alleviate symptoms. As for RAS,the treatment of oral ulcers and other mucocuta-neous lesions in patients with BD consists mainlyin the use of topical agents, particularly steroids.However, the number of randomized controlledtrials for targeted therapy is scarce. A recent sys-tematic review on the management of oral ulcersin BD concluded that there was insufficient evi-dence to support or refute the use of any topical orsystemic intervention with regard to pain, episodeduration, or episode frequency associated withlesions (Taylor et al. 2014).
Systemic therapy with colchicine, pentoxifylline,and dapsone is often useful when mucocutaneouslesions are frequent or severe. In refractory casesthalidomide, azathioprine, or biological agents,such as tumor necrosis factor-α antagonists(infliximab, etanercept) and interferon-α, may benecessary.
Food Allergy
Food allergy has been investigated as a putativecause of aphthous-like lesions, though scientificevidence to support this association is still sparse.Since the oral cavity is subjected to a wide spec-trum of antigenic agents, including food, allergicreactions to such antigens might manifest as ulcer-ative lesions.
Table 7 Diagnostic criteria for Behçet disease by the International Study Group for Behçet Disease
Diagnostic criteria forBehçet disease
Recurrent oral ulceration Minor aphthous, major aphthous, or herpetiform ulceration observed by the physician/dentist or patient that recurred at least three times in one 12-month period
Plus, two of the following:
Recurrent genitalulceration
Aphthous ulceration or scarring observed by the physician or patient
Eye lesions Anterior uveitis, posterior uveitis, cells in the vitreous on slit lamp examination, orretinal vasculitis observed by an ophthalmologist
Cutaneous lesions Erythema nodosum observed by physician or patient, pseudofolliculitis orpapulopustular lesions, or acneiform nodules observed by physician in postadolescentpatients not receiving corticosteroids
Positive pathergy test Read by the physician at 24–48 h
Findings applicable only in the absence of other clinical explanation
Oral Ulcerative Lesions 23
EpidemiologyA recent epidemiological study, “National Healthand Nutrition Examination Survey (NHANES),”investigated food allergy prevalence in US chil-dren in 1988–1994 and in 2005–2006, stratifiedby race and/or ethnicity (McGowan et al. 2016).Nearly 8,000 subjects were included, and theprevalence of food sensitization was 24.3%, withno significant differences between the two-timeperiods for milk, egg, or peanut sensitization,while shrimp sensitization decreased markedly(McGowan et al. 2016). One of the first studiessuggesting a putative role of food allergy or intol-erance in RAS was a small case series publishedin 1986, showing a significant improvement in6 out 15 patients following dietary withdrawal(Wright et al. 1986). Subsequent reports thatexplored sensitivity to foods, preservatives, orother agents in patients with a diagnosis of RASreported a prevalence of 35–50% (Wardhana andDatau 2010).
EtiopathogenesisAlthough causality between a certain food andaphthous-like lesions cannot be definitely stated,the association between allergy and RAS can behypothesized on the basis of RAS pathogenesis.The latter includes immediate type I reactions ordelayed type IV reactions, similar to IgE-mediatedand cell-mediated food hypersensitivity, as isalso supported by histological findings of lesions(Wardhana and Datau 2010).
Among possible etiological factors, the associ-ation between immunity to cow’s milk proteins(CMP) and RAS has been investigated. A strongassociation between high levels of serum anti-CMP IgA, IgG, and IgE antibodies and clinicalmanifestations of RAS has been reported (Besuet al. 2009). In one study, 50 subjects with RAS(36 with proven increased immunity to CMPand 14 without this increased immunity) wereenrolled, and data showed that levels of serumanti-fresh cow’s milk IgA, IgG, and IgE anti-bodies were significantly higher than levels ofserum anti-fresh goat’s milk in subjects withRAS with proven increased immunoreactivity toCMP (Besu et al. 2009). These results indicatethat patients with RAS with increased immunity
to CMP could consider the use of goat’s milk asthe alternative protein source. The same groupof authors further provided evidence of an etio-logical role for cow’s milk proteins in RAS deter-mining the prevalence of increased levels ofserum antibodies to specific cow’s milk proteins(SCMP), constituents of cheese or whey in sub-jects with RAS. Results indicated a strong associ-ation between high levels of serum anti-SCMPIgA, IgG, and IgE antibodies, especially tocaseins: α-, β-, and κ-casein from cow’s milk andclinical manifestations of RAS (Besu et al. 2013).
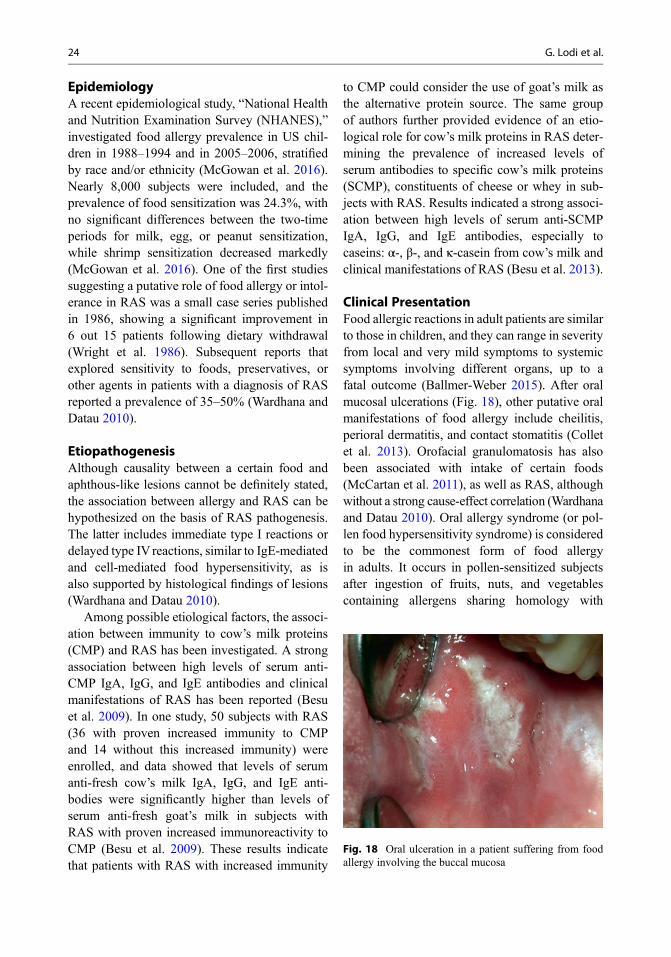
Clinical PresentationFood allergic reactions in adult patients are similarto those in children, and they can range in severityfrom local and very mild symptoms to systemicsymptoms involving different organs, up to afatal outcome (Ballmer-Weber 2015). After oralmucosal ulcerations (Fig. 18), other putative oralmanifestations of food allergy include cheilitis,perioral dermatitis, and contact stomatitis (Colletet al. 2013). Orofacial granulomatosis has alsobeen associated with intake of certain foods(McCartan et al. 2011), as well as RAS, althoughwithout a strong cause-effect correlation (Wardhanaand Datau 2010). Oral allergy syndrome (or pol-len food hypersensitivity syndrome) is consideredto be the commonest form of food allergyin adults. It occurs in pollen-sensitized subjectsafter ingestion of fruits, nuts, and vegetablescontaining allergens sharing homology with
Fig. 18 Oral ulceration in a patient suffering from foodallergy involving the buccal mucosa
24 G. Lodi et al.

pollen allergens. It is limited to the oropharynx inpruritus, and clinical presentation may includetingling, erythema, and swelling of the lip, oralmucosa, palate, and throat (Ho et al. 2014).
Clinical history and physical examination arethe foundation for the diagnosis of RAS caused byfood allergy. Aphthous lesions, however, do notdiffer from the clinical presentation of idiopathicRAS; thus further elements are required to achievea diagnosis of food allergy.
DiagnosisIn a patient with a clinical history suggesting foodallergy, first-line diagnostic testing consists ofskin testing or measurement of serum food-specific IgE levels or both. However, sensitizationoften does not equate to clinical allergy, and amedically supervised oral food challenge is thediagnostic gold standard (Abrams and Sicherer2016). Once the suspected food has been identi-fied, the best way to demonstrate the associationbetween food allergy and RAS in a single patientis probably to verify the resolution or a significantimprovement of aphthous lesions following thewithdrawal of the suspected food from the diet(elimination diet) and the relapse of the oral ulcersfollowing rechallenge with the same food. Dietelimination is not always successful regardlessof whether leukocytes released histamine afterexposure to food antigens is noted or not (Wrayet al. 1982).
Patient ManagementReduction in frequency and severity of recur-rences and maintenance of remission are amongthe goals of therapies to treat RAS. Eliminationdiets are frequently utilized in both diagnosis andmanagement of RAS caused by food allergy, i.e.,once certain foods are suspected of triggering theallergic reactions, they are completely omittedfrom the diet. Strict exclusion diets result inimprovement and/or resolution of ulcers in awide range of cases, from 25% to 75% of patients(Wardhana and Datau 2010). The success of suchdietary intervention depends on the correct iden-tification of the food allergens and on the abilityof the patient to avoid them during daily life(Wardhana and Datau 2010).
Besides dietary approaches, treatment of RASassociated with food allergy involves, once more,the use of topical and/or systemic treatments,mainly based on steroid agents, following thesame posology used for idiopathic RAS(Wardhana and Datau 2010).
Recurrent Aphthous Stomatitisand Micronutrient Deficiency
The WHO definition of micronutrients states that“these substances are the magic wands that enablethe body to produce enzymes, hormones and othersubstances essential for proper growth and devel-opment. As tiny as the amounts are, however, theconsequences of their absence are severe” (WorldHealth Organization 2016). The association ofRAS with deficiencies of different micronutrients(i.e., vitamin B12, iron, folate, and, more recently,zinc), as well as the putative role of these sub-stances in its pathogenesis, has been the subject ofa number of studies since the 1960s (Ship 1962).At the time, early reports of RAS patients whoimproved or even healed following vitamin sup-plementation led to the idea that RAS could be adeficiency syndrome, at least in some cases. Sincethen, many studies have investigated the fre-quency of different micronutrient deficienciesamong RAS patients. Nevertheless, a definitiveconclusion has not been reached yet. In fact, dif-ferences in terms of diagnostic criteria, patient andcontrol selection, laboratory technique, and nor-mal value range make data hardly comparableand to certain extent explain conflicting results(Table 7).
The deficiency of vitamin B12, a coenzyme forfat and carbohydrate metabolism, protein synthe-sis, and hematopoiesis, is responsible for megalo-blastic anemia, neurological symptoms, chronictiredness, and mood disturbance (Vidal-Alaballet al. 2005). The association of RAS and defi-ciency of vitamin B12 has been investigated in anumber of controlled and noncontrolled studiesthat found a frequency of vitamin B12 deficiencyamong RAS patients to range between 0% and45% (Fig. 19). Another micronutrient of the vita-min B group often investigated among RAS
Oral Ulcerative Lesions 25

patients is folic acid, a vitamin necessary forpurine and pyrimidine synthesis, erythropoiesis,and methionine regeneration, the deficiency ofwhich causes effects similar to that of vitaminB12 (Fairfield and Fletcher 2002). Patients withfolic acid deficiency can represent up to 51%of patients suffering from RAS (Table 7). In arecent meta-analysis including data of over 1100subjects from 8 case-control studies publishedbetween 1975 and 2014, the rate of vitamin B12and folic acid deficiencies was significantlyhigher in RAS patients, compared with controls(vitamin B12: odds ratio = 3.75, 95% confidenceinterval, 2.38–5.94; folic acid, odds ratio = 7.55,95% confidence interval, 3.91–14.60) (Chenet al. 2015).
Similar data are available for iron deficiencyand anemia. Although sideremia, transferrin, andtotal iron binding capacity have been the subjectof investigation, ferritin (a protein that stores iron)is the indicator more commonly used in studiesexploring the association of RAS and irondeficiency, which has been found below normalvalues in a proportion of patients ranging between7% and 40% (Table 8). In the aforementionedmeta-analysis, ferritin below normal values wasmore common in 687 patients with RAS than inthe 583 controls (odds ratio 2.62, 95%; confidenceinterval 1.69–4.06) (Chen et al. 2015). Similarly,although diagnostic criteria for anemia varied
among studies, up to 60% of patients with RASmay have hemoglobin values below normalrange, and pooled data from controlled studiesshows a significant association (odds ratio 1.77,95%; confidence interval 1.12–2.80).
When vitamin B12, folic acid, and iron aretaken together, the proportion of patients sufferingfrom aphthae, with one or more micronutrientdeficiency, can be as high as 50% (Compilatoet al. 2010) and the difference with control sub-jects statistically significant (Lopez-Jornet et al.2014). Notably, anemia and deficiencies of serumferritin and folate may be more common in femalepatients with RAS, but the same is not true forvitamin B12 (Burgan et al. 2006).
Little is known about the prevalence of oralmucosal lesions among subjects with hematinicdeficiencies, although a recent study reported a22% prevalence of aphthous lesions in patientsdeficient in vitamin B12 and vitamin B9 (Andrèset al. 2016).
Clinical form (minor, major, herpetic, severe),localization, and severity of lesions do not seemto be useful in identifying RAS patients withhematinic deficiencies. In fact, as stated in oneof the first studies investigating this association,“it was not possible by clinical examination ofthe ulcers to separate patients with an underlyingdeficiency or disease from those with no suchabnormality” (Wray et al. 1975). In fact, clinicalfeatures are similarly distributed in deficient andnon-deficient subjects (Lopez-Jornet et al. 2014;Rogers and Hutton 1986; Sun et al. 2015; Wrayet al. 1978).
The role played by diet in RAS onset has beeninvestigated by comparing nutritional habitsamong RAS patients and controls, with reportedsignificant differences in vitamin B12 and folateintakes (Kozlak et al. 2010), but not in specificfood categories (Ogura et al. 2001; Ship 1962).Noteworthy, single or multiple deficiencies ofsuch micronutrients can be a consequence ofinsufficient absorption in the gastrointestinaltract, a common consequence of chronic inflam-matory conditions of the bowel, includingCrohn’s disease and celiac disease, disordersoften associated with RAS.
Fig. 19 Oral ulcers involving the lateral and dorsal sur-faces of the tongue in a patient suffering from vitamin B12deficiency
26 G. Lodi et al.

Table 8 Frequency of micronutrient deficiencies among patients affected by recurrent aphthous stomatitis
Study ID RAS patients Controls Lower reference value
Vitamin B12
Burgan et al. 2006 38/143 (27%) 18/143 (13%) 180 pg/mL
Challacombe et al. 1977 1/40 (2%) 0/26 (0%) 200 ng/L
Compilato et al. 2010 5/32 (15%) 0/29 (0%) 226 pg ⁄mL
Khan et al. 2013 27/60 (45%) 9/60 (15%) 220 pg/mL
Koybasi et al. 2006 12/34 (35%) 0/32 (0%) Not reported
Lopez-Jornet et al. 2014 5/92 (5%) 1/94 (1%) 200 pg/mL
Olson et al. 1982 0/90 (0%) 0/23 (0%) 160 pg/mL
Piskin et al. 2002 8/35 (23%) 0/26 (0%) 200 pg/mL
Porter et al. 1988 2/69 (3%) 2/75 (3%) Not reported
Rogers and Hutton 1986 0/102 (0%) – Not reported
Sun et al. 2015 13/273 (5%) 0/273 (0%) 200 pg/mL
Thongprasom et al. 2002 0/23 (0%) 0/19 (0%) 150 pg/mL
Wray et al. 1975 5/130 (4%) 1/130 (1%) 120 ng/L
Folic acid
Burgan et al. 2006 7/143 (5%) 0/143 (0%) 2.5 ng/mL
Challacombe et al. 1977 7/40 (17%) 4/26 (15%) 5 μg/LCompilato et al. 2010 6/32 (19%) 0/29 (0%) 2.3 ng ⁄mL
Khan et al. 2013 31/60 (51%) 6/60 (10%) 1.5 ng/mL
Lopez-Jornet et al. 2014 4/92 (4%) 1/94 (1%) 2.7 ng/mL
Piskin et al. 2002 4/35 (11%) 0/26 (0%) 3 μg/LRogers and Hutton 1986 22/102 (21%) – Not reported
Sun et al. 2015 7/273 (3%) 0/273 (0%) 4 ng/mL
Wray et al. 1975 7/130 (5%) 3/130 (2%) 2.5 μg/LFerritin
Burgan et al. 2006 24/143 (17%) 14/143 (10%) 12 (female) and 14 (male) ng/mL
Compilato et al. 2010 13/32 (40%) 0/29 (0%) 10 (female) and 22 (male) ng⁄mL
Lopez-Jornet et al. 2014 6/92 (7%) 5/94 (5%) 12 ng/mL
Piskin et al. 2002 6/35 (17%) 3/26 (11%) 9 (female) and 18 (male) ng⁄mL
Porter et al. 1988 8/69 (12%) 4/75 (5%) Not reported
Hemoglobin
Babaee et al. 2016 17/28 (60%) 9/28 (32%) 14 (female) and 17 (male) g/dL
Burgan et al. 2006 20/143 (14%) 15/143 (10%)
Challacombe et al. 1977 14/193 (7%) 2/100 (2%) 11.5 (female) and 13 (male) g/dL
Compilato et al. 2010 11/32 (34%) 2/29 (7%) 12.0 (female) and 12.5 (male) g⁄dL
Khan et al. 2013 35/60 (58%) 26/60 (43%) 12 (female) and 14 (male) g/dL
Olson et al. 1982 6/90 (7%) 2/23 (9%) 11 (female) and 13 (male) g/dL
Porter et al. 1988 0/69 (0%) 0/75 (0%) Not reported
Rogers and Hutton 1986 6/102 (6%) – Not reported
Sun et al. 2015 57/273 (21%) 0/273 (0%) 12 (female) and 13 (male) g/dL
Zinc
Bao et al. 2016 33/156 (21.2%) – 70 μg/dL (10.7 μmol/L)
Orbak et al. 2003 17/40 (42.5%) – 95 μg/dLOzler 2014 7/25 (28%) 1/25 (4%) 95 μg/dLWray 1982 0/20 (0%) – 55 μg/dL
Oral Ulcerative Lesions 27

More recently, zinc has been the subject ofinvestigation in groups of patients affected byRAS. Zinc is an essential micronutrient forhumans. It is a constituent of a large number ofenzymes, fundamental for cell growth, collagensynthesis, wound healing, and normal function ofreproductive, neurologic, immune, dermatologic,and gastrointestinal systems. The features of mildzinc deficiency are frequently nonspecific andinclude diarrhea, cognitive and behavioral prob-lems, hair loss, eye problems, growth retardation,and recurrent infections (Bao et al. 2016; Shahet al. 2016). Patients with RAS may have lowermean levels of zinc in serum compared with con-trols (Ozturk et al. 2013), as well as higher rateof zinc deficiency (Table 8). In addition, studieson animal models, specifically in rats, haveshown that a zinc-deficient diet is associatedwith aphthous ulcers and other alterations ofthe oral mucosa (Orbak et al. 2007; Seyedmajidiet al. 2014).
On the basis of anecdotal reports of RASpatients with documented clinical improvementsfollowing replacement therapy, few randomizedcontrolled trials have been conducted. One studytreated RAS patients who had experienced atleast three episodes in the previous 12 months,irrespective of their vitamin serum level, and com-pared a multivitamin supplement containing theUS reference daily intake of vitamins A, B1, B2,B3, B5, B6, B9, B12, C, D, and E with placebo(Lalla et al. 2012). Noteworthy, the multivitaminsupplement showed no benefit either in the sub-group of participants with low baseline levels ofB12 or in those with a highly frequent form. Thetrial was judged at low risk of bias by a Cochranereview and showed no differences in number orduration of RAS episodes between the two groups(Brocklehurst et al. 2012). A separate placebo-controlled randomized trial tested the effects of a6-month monotherapy with vitamin B12 (1000mcg sublingual daily) in patients with RAS.Again, patients were selected on the basis of thefrequency of aphthous episodes (at least one out-break every 2 months in the last year), and morethan 80% had normal levels of serum vitamin B12.
At completion of the trial, the treatment groupreported less pain, a shorter duration of RASepisodes, and lower frequency of episodes, andduring the last 2 months of treatment, moreparticipants in the same group were free fromulcers (Volkov et al. 2009). However, theCochrane review assessed the study as unclearrisk of bias and concluded that the evidence pro-vided was insufficient to support or refute theuse of vitamin B12 for the treatment of RAS(Brocklehurst et al. 2012).
In conclusion, although a number of patientswith RAS can be affected by micronutrient defi-ciencies, the evidence presently available does notoffer strong support for routine testing of RASpatients or treatment with supplements in theabsence of a demonstrated deficiency (in whichcase improvement of the oral condition is notguaranteed).
Conclusions and Future Directions
An ulcer of the mouth can represent a mani-festation of a number of local and systemicconditions ranging from self-limiting lesions tolife-threatening diseases. Histological examina-tion and specific laboratory tests are often essen-tial elements in the differential diagnosis;however, clinical features, such as number, local-ization, duration, and aspect, are fundamental inthe distinguishing of oral ulcerative lesions, and inmany cases they can be sufficient to establish adefinitive diagnosis and start treatment. A propermanagement of a patient with oral ulceration needsan appropriate knowledge of the different mecha-nisms able to lead to the onset of such mucosallesion and, ideally, of the etiopathogenesis of theunderlining diseases. Unfortunately, for many ofthem, including common disorders as recurrentaphthous stomatitis and immunological condi-tions, very little is known, and for this reason,treatment is essentially palliative, while a betterunderstanding of the causes and pathologicalmechanisms responsible for them would warranta far better management of affected subjects.
28 G. Lodi et al.

Cross-References
▶Clinical Evaluation of Oral Disease▶Clinical Immunology in Diagnoses of Maxillo-facial Disease
▶Gingival Pathology▶ Interface Between Oral and Systemic Disease▶LaboratoryMedicine and Diagnostic Pathology▶Non-Odontogenic Bacterial Infections▶Oral and Maxillofacial Fungal Infections▶Oral and Maxillofacial Viral Infections▶Oral Lichen Planus▶Oral Manifestations of Systemic Diseases andTheir Treatments
▶Oral Mucosal Malignancies▶Oral Vesicular and Bullous Lesions▶ Pediatric Oral Medicine▶ Pharmacotherapeutic Approaches in OralMedicine
▶ Soft and Hard Tissue Operative Investigationsin the Diagnosis of Oral Disease
References
Abraham C, Cho JH. Inflammatory bowel disease. N EnglJ Med. 2009;361(21):2066–78.
Abrams EM, Sicherer SH. Diagnosis and management offood allergy. CMAJ. 2016;188(15):1087–93.
Aine L, Mäki M, Collin P, Keyriläinen O. Dentalenamel defects in celiac disease. J Oral Pathol Med.1990;19(6):241–5.
Akintoye SO, Greenberg MS. Recurrent aphthous stoma-titis. Dent Clin N Am. 2014;58(2):281–97.
Albanidou-Farmaki E, Deligiannidis A, Markopoulos AK,Katsares V, Farmakis K, Parapanissiou E. HLA haplo-types in recurrent aphthous stomatitis: a mode of inher-itance? Int J Immunogenet. 2008;35(6):427–32.
Alpsoy E, Zouboulis CC, Ehrlich GE. Mucocutaneouslesions of Behcet’s disease. Yonsei Med J. 2007;48(4):573–85.
Alpsoy E. Behcet’s disease: a comprehensive reviewwith afocus on epidemiology, etiology and clinical features,and management of mucocutaneous lesions.J Dermatol. 2016; 43(6):620–32.
Alrashdan MS, Cirillo N, McCullough M. Oral lichenplanus: a literature review and update. Arch DermatolRes. 2016;308(8):539–51.
Andrès E, Nachit M, Guillet-Thibault J. Oral manifesta-tions of vitamin B12 and B9 deficiencies: a prospectivestudy. J Oral Pathol Med. 2016;45(2):154.
Axéll T. A prevalence study of oral mucosal lesions inan adult Swedish population. Odontol Revy Suppl.1976;36:1–103.
Azizlerli G, Kose AA, Sarica R. Prevalence of Behcet’sdisease in Istanbul, Turkey. Int J Dermatol. 2003;42(10):803–6.
Babaee N, Hosseinkazemi H, Pouramir M, KhakbazBaboli O, Salehi M, Khadir F, Bijani A, Mehryari M.Salivary oxidant/antioxidant status and haematologicalparameters in patients with recurrent aphthous stomati-tis. Caspian J Int Med. 2016;7(1):13–8.
Baccaglini L, Lalla RV, Bruce AJ, Sartori-Valinotti JC,Latortue MC, Carrozzo M, Rogers RS 3rd. Urbanlegends: recurrent aphthous stomatitis. Oral Dis.2011;17(8):755–70.
Bachtiar EW, Cornain S, Siregar B, Raharjo TW.Decreased CD4+/CD8+ ratio in major type ofrecurrent aphthous ulcers: comparing major to minortypes of ulcers. Asian Pac J Allergy Immunol.1998;16(2–3):75–9.
Balasubramaniam R, Kuperstein AS, Stoopler ET.Update on oral herpes virus infections. Dent Clin NAm. 2014;58(2):265–80.
Ballmer-Weber BK. Food allergy in adolescence and adult-hood. Chem Immunol Allergy. 2015;101:51–8.
Bang DS, Oh SH, Lee KH. Influence of sex on patientswith Behcet’s disease in Korea. J Korean Med Sci.2003;18(2):231–5.
Bao ZX, Yang XW, Shi J, Liu LX. Serum zinc levelsin 368 patients with oral mucosal diseases: a prelimi-nary study. Med Oral Patol Oral Cir Bucal. 2016;21(3):e335–40.
Barker JM, Liu E. Celiac disease: pathophysiology, clinicalmanifestations, and associated autoimmune conditions.Adv Pediatr Infect Dis. 2008;55:349–65.
Baumgart DC, SandbornWJ. Inflammatory bowel disease:clinical aspects and established and evolving therapies.Lancet. 2007;369(9573):1641–57.
Bazrafshani MR, Hajeer AH, Ollier WE, Thornhill MH.IL-1B and IL-6 gene polymorphisms encode significantrisk for the development of recurrent aphthous stoma-titis (RAS). Genes Immun. 2002;3(5):302–5.
Behçet H. Uber rezidivierende aphthöse, durch ein Virusverursachte Geschwure, am Mund, am Auge, und anden Genitalien. Dermatol Wochenschr. 1937;36:1152–7.
Besu I, Jankovic L, Magdu IU, Konic-Ristic A,Raskovic S, Juranic Z. Humoral immunity to cow’smilk proteins and gliadin within the etiology of recur-rent aphthous ulcers? Oral Dis. 2009;15(8):560–4.
Besu I, Jankovic L, Konic-Ristic A, Raskovic S, Besu V,Djuric M, Cakic S, Magdu IU, Juranic Z. The role ofspecific cow’s milk proteins in the etiology of recurrentaphthous ulcers. J Oral Pathol Med. 2013;42(1):82–8.
Boras VV, Lukac J, Brailo V, Picek P, Kordic D, Zilic IA.Salivary interleukin-6 and tumor necrosis factor-alphain patients with recurrent aphthous ulceration. J OralPathol Med. 2006;35(4):241–3.
Oral Ulcerative Lesions 29

Bradley PJ, Ferlito A, Devaney KO, Rinaldo A. Crohn’sdisease manifesting in the head and neck. ActaOtolaryngol. 2004;124(3):237–41.
Brennan MT, Valerin MA, Napeñas JJ, Lockhart PB. Oralmanifestations of patients with lupus erythematosus.Dent Clin N Am. 2005;49(1):127–41.
Brocklehurst P, Tickle M, Glenny AM, Lewis MA,Pemberton MN, Taylor J, Walsh T, Riley P, Yates JM.Systemic interventions for recurrent aphthous stomati-tis (mouth ulcers). Cochrane Database Syst Rev.2012;9:CD005411.
Buno IJ, Huff JC, Weston WL, Cook DT, Brice SL.Elevated levels of interferon gamma, tumor necrosisfactor alpha, interleukins 2, 4, and 5, but not interleukin10, are present in recurrent aphthous stomatitis. ArchDermatol. 1998;134(7):827–31.
Burgan SZ, Sawair FA, Amarin ZO. Hematologic status inpatients with recurrent aphthous stomatitis in Jordan.Saudi Med J. 2006;27(3):381–4.
Burisch J, Jess T, Martinato M, Lakatos PL, ECCO-EpiCom. The burden of inflammatory bowel diseasein Europe. J Crohns Colitis. 2013;7(4):322–37.
Carrard V, Haas A, Rados P, Filho M, Oppermann R,Albandar J, Susin C. Prevalence and risk indicators oforal mucosal lesions in an urban population from SouthBrazil. Oral Dis. 2011;17(2):171–9.
de Carvalho FK, de Queiroz AM, Bezerra da Silva RA,Sawamura R, Bachmann L, Bezerra da Silva LA,Nelson-Filho P. Oral aspects in celiac disease children:clinical and dental enamel chemical evaluation.Oral Surg Oral Med Oral Pathol Oral Radiol.2015;119(6):636–43.
Challacombe SJ, Barkhan P, Lehner T. Haematologicalfeatures and differentiation of recurrent oral ulceration.Br J Oral Surg. 1977;15(1):37–48.
Chen H, Sui Q, Chen Y, Ge L, Lin M. Impact ofhaematologic deficiencies on recurrent aphthous ulcer-ation: a meta-analysis. Br Dent J. 2015;218(4):E8.
Chi AC, Day TA, Neville BW. Oral cavity and oropharyn-geal squamous cell carcinoma–an update. CA Cancer JClin. 2015;65(5):401–21.
Collet E, Jeudy G, Dalac S. Cheilitis, perioral dermatitisand contact allergy. Eur J Dermatol. 2013;23(3):303–7.
Compilato D, Carroccio A, Calvino F, Di Fede G,Campisi G. Haematological deficiencies in patientswith recurrent aphthosis. J Eur Acad DermatolVenereol. 2010;24(6):667–73.
Cowan D, Ho B, Sykes KJ, Wei JL. Pediatric oral burns: aten-year review of patient characteristics, etiologies andtreatment outcomes. Int J Pediatr Otorhinolaryngol.2013;77(8):1325–8.
Crivelli MR, Aguas S, Adler I, Quarracino C, Bazerque P.Influence of socioeconomic status on oral mucosalesion prevalence in schoolchildren. Community DentOral Epidemiol. 1988;16(1):58–60.
Dalvi SR, Yildirim R, Yazici Y. Behcet’s syndrome. Drugs.2012;72(17):2223–41.
Davatchi F, Sadeghi Abdollahi B, Chams-Davatchi C,Shahram F, Shams H, Nadji A, Faezi T, Akhlaghi M,
Ghodsi Z, Mohtasham N, Ashofteh F. The saga ofdiagnostic/classification criteria in Behcet’s disease.Int J Rheum Dis. 2015;18(6):594–605.
Fairfield KM, Fletcher RH. Vitamins for chronic diseaseprevention in adults: scientific review. JAMA.2002;287(23):3116–26.
Fasano A, Catassi C. Clinical practice. Celiac disease.N Engl J Med. 2012;367(25):2419–26.
Gallo C d B, Mimura MA, Sugaya NN. Psychologicalstress and recurrent aphthous stomatitis. Clinics (SaoPaulo). 2009;64(7):645–8.
García-Pola Vallejo MJ, Martínez Díaz-Canel AI, GarcíaMartín JM, González García M. Risk factors for oralsoft tissue lesions in an adult Spanish population. Com-munity Dent Oral Epidemiol. 2002;30(4):277–85.
Gilvetti C, Porter SR, Fedele S. Traumatic chemical oralulceration: a case report and review of the literature. BrDent J. 2010;208(7):297–300.
Green PHR, Cellier C. Celiac disease. N Engl J Med.2007;357(17):1731–43.
Gurler A, Boyvat A, Tursen U. Clinical manifestations ofBehcet’s disease: an analysis of 2147 patients. YonseiMed J. 1997;38(6):423–7.
Gujral N, Freeman HJ, Thomson AB. Celiac disease: prev-alence, diagnosis, pathogenesis and treatment. World JGastroenterol. 2012;18(42):6036–59.
HelloM, Barbarot S, Bastuji-Garin S, Revuz J, ChosidowO.Use of thalidomide for severe recurrent aphthousstomatitis: a multicenter cohort analysis. Medicine(Baltimore). 2010;89(3):176–82.
Ho MH, Wong WH, Chang C. Clinical spectrum of foodallergies: a comprehensive review. Clin Rev AllergyImmunol. 2014;46(3):225–40.
International Study Group for Behçet Disease. Criteriafor diagnosis of Behçet disease. Lancet.1990;335(8697):1078–80.
International Team for the Revision of the InternationalCriteria for Behçet Disease (ITR-ICBD). The interna-tional criteria for Behçet disease (ICBD): a collabora-tive study of 27 countries on the sensitivity andspecificity of the new criteria. J Eur Acad DermatolVenereol. 2014;28(3):338–47.
Jung SA. Differential diagnosis of inflammatory boweldisease: what is the role of colonoscopy? Clin Endosc.2012;45(3):254–62.
Kalla R, Ventham NT, Satsangi J, Arnott ID. Crohn’s dis-ease. BMJ. 2014;349:g6670.
Katsanos KH, Torres J, Roda G, Brygo A, Delaporte E,Colombel JF. Review article: non-malignant oral man-ifestations in inflammatory bowel diseases. AlimentPharmacol Ther. 2015;42(1):40–60.
Khan NF, Saeed M, Chaudhary S, Khan NF.Haematological parameters and recurrent aphthous sto-matitis. J Coll Physicians Surg Pak. 2013;23(2):124–7.
Keogan MT. Clinical Immunology Review Series: anapproach to the patient with recurrent orogenital ulcer-ation, including Behcet’s syndrome. Clin ExpImmunol. 2009;156(1):1–11.
30 G. Lodi et al.
Kim B, LeBoit PE. Histopathologic features of erythemanodosum – like lesions in Behcet disease: a comparisonwith erythema nodosum focusing on the role of vascu-litis. Am J Dermatopathol. 2000;22(5):379–90.
Kitaichi N, Miyazaki A, Iwata D, et al. Ocular features ofBehcet’s disease: an international collaborative study.Br J Ophthalmol. 2007;91(12):1579–82.
Krause I, Rosen Y, Kaplan I, et al. Recurrent aphthousstomatitis in Behcet’s disease: clinical features andcorrelation with systemic disease expression and sever-ity. J Oral Pathol Med. 1999;28(5):193–6.
Koybasi S, Parlak AH, Serin E, Yilmaz F, Serin D. Recur-rent aphthous stomatitis: investigation of possible etio-logic factors. Am J Otolaryngol. 2006;27(4):229–32.
Kozlak ST, Walsh SJ, Lalla RV. Reduced dietary intakeof vitamin B12 and folate in patients withrecurrent aphthous stomatitis. J Oral Pathol Med.2010;39(5):420–3.
Lalla RV, Choquette LE, Feinn RS, Zawistowski H,Latortue MC, Kelly ET, Baccaglini L. Multivitamintherapy for recurrent aphthous stomatitis: a random-ized, double-masked, placebo-controlled trial. J AmDent Assoc. 2012;143(4):370–6.
Lankarani KB, Sivandzadeh GR, Hassanpour S. Oral man-ifestation in inflammatory bowel disease: a review.World J Gastroenterol. 2013;19:8571–9.
Laranjeira N, Fonseca J, Meira T, Freitas J, Valido S, Leitão J.Oral mucosa lesions and oral symptoms in inflam-matory bowel disease patients. Arq Gastroenterol.2015;52(2):105–10.
Lin SS, Chou MY, Ho CC, Kao CT, Tsai CH, Wang L,Yang CC. Study of the viral infections and cytokinesassociated with recurrent aphthous ulceration.Microbes Infect. 2005;7(4):635–44.
Lionetti E, Castellaneta S, Francavilla R, Pulvirenti A,Tonutti E, Amarri S, Barbato M, Barbera C, Barera G,Bellantoni A, Castellano E, Guariso G, LimongelliMG, Pellegrino S, Polloni C, Ughi C, Zuin G,Fasano A, Catassi C, SIGENP (Italian Society of Pedi-atric Gastroenterology, Hepatology, and Nutrition)Working Group onWeaning and CDRisk. Introductionof gluten, HLA status, and the risk of celiac disease inchildren. N Engl J Med. 2014;371(14):1295–303.
Lo Russo L, Fedele S, Guiglia R, Ciavarella D, LoMuzio L, Gallo P, Di Liberto C, Campisi G. Diagnosticpathways and clinical significance of desquamativegingivitis. J Periodontol. 2008;79(1):4–24.
Lopez-Jornet P, Camacho-Alonso F, Martos N. Hemato-logical study of patients with aphthous stomatitis. Int JDermatol. 2014;53(2):159–63.
Main DM, Chamberlain MA. Clinical differentiation oforal ulceration in Behcet’s disease. Br J Rheumatol.1992;31(11):767–70.
Marty M, Bailleul-Forestier I, Vaysse F. RecurrentAphthous stomatitis as a marker of celiac disease inchildren. Pediatr Dermatol. 2016;33(2):241.
McCartan BE, Healy CM, McCreary CE, Flint SR,Rogers S, Toner ME. Characteristics of patients
with orofacial granulomatosis. Oral Dis.2011;17(7):696–704.
McGowan EC, Peng RD, Salo PM, Zeldin DC, Keet CA.Changes in food-specific IgE over time in the NationalHealth and nutrition examination survey (NHANES).J Allergy Clin Immunol Pract. 2016;4(4):713–20.
McMillan R, Taylor J, Shephard M, Ahmed R,Carrozzo M, Setterfield J, Grando S, Mignogna M,Kuten-Shorrer M, Musbah T, Elia A, McGowan R,Kerr AR, Greenberg MS, Hodgson T, Sirois D.World workshop on oral medicine VI: a systematicreview of the treatment of mucocutaneous pemphigusvulgaris. Oral Surg Oral Med Oral Pathol Oral Radiol.2015;120(2):132–42.
de Menthon M, Lavalley MP, Maldini C, et al. HLA-B51/B5 and the risk of Behcet’s disease: a systematic reviewand meta-analysis of case–control genetic associationstudies. Arthritis Rheum. 2009;61(10):1287–96.
Miller MF, Garfunkel AA, Ram CA, Ship II. The inheri-tance of recurrent aphthous stomatitis. Observationson susceptibility. Oral Surg Oral Med Oral Pathol.1980;49(5):409–12.
Mortazavi H, SafiY, BaharvandM, Rahmani S. Diagnosticfeatures of common oral ulcerative lesions: an updateddecision tree. Int J Dent. 2016;2016:7278925.
Nahlieli O, Eliav E, Shapira Y, Baruchin AM. Centralpalatal burns associated with the eating of microwavedpizzas. Burns. 1999;25(5):465–6.
National Center for Chronic Disease Prevention and HealthPromotion, Centers for Disease Control and Prevention– Epidemiology of the IBD – Inflammatory BowelDisease. [Internet] 2015 [page last updated: March31, 2015]. Available from: www.cdc.gov/ibd/ibd-epidemiology.htm. Accessed 19 Aug 2016.
Ogura M, Yamamoto T, Morita M, Watanabe T. A case-control study on food intake of patients with recurrentaphthous stomatitis. Oral Surg Oral Med Oral PatholOral Radiol Endod. 2001;91(1):45–9.
Olson JA, Feinberg I, Silverman S Jr, Abrams D, Green-span JS. Serum vitamin B12, folate, and iron levels inrecurrent aphthous ulceration. Oral Surg Oral Med OralPathol. 1982;54(5):517–20.
Orbak R, Cicek Y, Tezel A, Dogru Y. Effects of zinctreatment in patients with recurrent aphthous stomatitis.Dent Mater J. 2003;22(1):21–9.
Orbak R, Kara C, Ozbek E, Tezel A, Demir T. Effects ofzinc deficiency on oral and periodontal diseases in rats.J Periodontal Res. 2007;42(2):138–43.
Ozler GS. Zinc deficiency in patients with recurrentaphthous stomatitis: a pilot study. J Laryngol Otol.2014;128(6):531–3.
Ozturk P, Belge Kurutas E, Ataseven A. Copper/zinc andcopper/selenium ratios, and oxidative stress as bio-chemical markers in recurrent aphthous stomatitis. JTrace Elem Med Biol. 2013;27(4):312–6.
Pedersen A, Hornsleth A. Recurrent aphthous ulceration: apossible clinical manifestation of reactivation of vari-cella zoster or cytomegalovirus infection. J Oral PatholMed. 1993;22(2):64–8.
Oral Ulcerative Lesions 31

Pekiner FN, Aytugar E, Demirel GY, Borahan MO. Inter-leukin-2, interleukin-6 and T regulatory cells in periph-eral blood of patients with Behçet’s disease andrecurrent aphthous ulcerations. J Oral Pathol Med.2012;41(1):73–9.
Pentenero M, Broccoletti R, Carbone M, Conrotto D,Gandolfo S. The prevalence of oral mucosallesions in adults from the Turin area. Oral Dis.2008;14(4):356–66.
Piskin S, Sayan C, Durukan N, Senol M. Serum iron,ferritin, folic acid, and vitamin B12 levels in recurrentaphthous stomatitis. J Eur Acad Dermatol Venereol.2002;16(1):66–7.
Pittock S, Drumm B, Fleming P, McDermott M, Imrie C,Flint S, Bourke B. The oral cavity in Crohn’s disease.J Pediatr. 2001;138:767–71.
Porter SR, Scully C, Flint S. Hematologic status inrecurrent aphthous stomatitis compared with otheroral disease. Oral Surg Oral Med Oral Pathol.1988;66(1):41–4.
Preeti L, Magesh KT, Rajkumar K, Karthik R.Recurrent aphthous stomatitis. J Oral MaxillofacPathol. 2011;15(3):252–6.
Rashid M, Zarkadas M, Anca A, Limeback H. Oral man-ifestations of celiac disease: a clinical guide for den-tists. J Can Dent Assoc. 2011;77:b39.
Rogers RS 3rd, Hutton KP. Screening for haematinic defi-ciencies in patients with recurrent aphthous stomatitis.Australas J Dermatol. 1986;27(3):98–103.
Sackett DL, Haynes RB, Guyatt GH, Tugwell P. Clinicalepidemiology: a basic science for clinical medicine.2nd ed. Boston: Little, Brown; 1991.
Sakane T, Takeno M, Suzuki N, et al. Behcet’s disease. NEngl J Med. 1999;341(17):1284–91.
Samim F, Auluck A, Zed C, Williams PM. Erythemamultiforme: a review of epidemiology, pathogenesis,clinical features, and treatment. Dent Clin North Am.2013;57(4):583–96.
Sartor RB. Mechanisms of disease: pathogenesis ofCrohn’s disease and ulcerative colitis. Nat Clin PractGastroenterol Hepatol. 2006;3(7):390–407.
Scully C. Clinical practice. Aphthous ulceration. N Engl JMed. 2006;355(2):165–72.
Scully C, Felix DH. Oral medicine–update for the dentalpractitioner. Aphthous and other common ulcers.Br Dent J. 2005;199(5):259–64.
Scully C, Gorsky M, Lozada-Nur F. The diagnosisand management of recurrent aphthous stomatitis:a consensus approach. J Am Dent Assoc.2003;134(2):200–7.
Senusi A, Seoudi N, Bergmeier LA, et al. Genital ulcerseverity score and genital health quality of life inBehcet’s disease. Orphanet J Rare Dis. 2015;10:117.
Seyedmajidi SA, Seyedmajidi M, Moghadamnia A,Khani Z, Zahedpasha S, Jenabian N, Jorsaraei G,Halalkhor S, Motallebnejad M. Effect of zinc-deficientdiet on oral tissues and periodontal indices in rats. Int JMol Cell Med. 2014;3(2):81–7.
Shah D, Sachdev HS, Gera T, De-Regil LM, Peña-Rosas JP. Fortification of staple foods with zinc forimproving zinc status and other health outcomes inthe general population. Cochrane Database Syst Rev.2016;6:CD010697.
Ship II. Nutrition and food intake in aphthous ulcerations.Arch Environ Health. 1962;5:158–66.
Ship II. Epidemiologic aspects of recurrent aphthousulcerations. Oral Surg Oral Med Oral Pathol.1972;33(3):400–6.
Ship JA, Chavez EM, Doerr PA, Henson BS, Sarmadi M.Recurrent aphthous stomatitis. Quintessence Int.2000;31(2):95–112.
Shulman JD, Beach MM, Rivera-Hidalgo F. The preva-lence of oral mucosal lesions in U.S. adults: datafrom the third National Health and nutritionexamination survey, 1988–1994. J Am Dent Assoc.2004;135(9):1279–86.
Singh B, Kedia S, Konijeti G, Mouli VP, Dhingra R,Kurrey L, Srivastava S, Pradhan R, Makharia G,Ahuja V. Extra-intestinal manifestations of inflamma-tory bowel disease and intestinal tuberculosis: fre-quency and relation with disease phenotype. Indian JGastroenterol. 2015;34:43–50.
Slebioda Z, Szponar E, Kowalska A. Etiopathogenesis ofrecurrent aphthous stomatitis and the role of immuno-logic aspects: literature review. Arch Immunol TherExp. 2014;62(3):205–15.
Sun A, Chu CT, Liu BY, Wang JT, Leu JS, Chiang CP.Expression of interleukin-2 receptor by activatedperipheral blood lymphocytes upregulated by theplasma level of interleukin-2 in patients with recurrentaphthous ulcers. Proc Natl Sci Counc Repub China B.2000;24(3):116–22.
Sun A, Chen HM, Cheng SJ, Wang YP, Chang JY, YC W,Chiang CP. Significant association of deficiencies ofhemoglobin, iron, vitamin B12, and folic acid and highhomocysteine level with recurrent aphthous stomatitis.J Oral Pathol Med. 2015;44(4):300–5.
Taylor J, Glenny AM, Walsh T, et al. Interventions for themanagement of oral ulcers in Behcet’s disease.Cochrane Database Syst Rev. 2014;9:CD011018.
Taylor J, McMillan R, Shephard M, Setterfield J,Ahmed R, Carrozzo M, Grando S, Mignogna M,Kuten-Shorrer M, Musbah T, Elia A, McGowan R,Kerr AR, Greenberg MS, Hodgson T, Sirois D.World workshop on oral medicine VI: a systematicreview of the treatment of mucous membranepemphigoid. Oral Surg Oral Med Oral Pathol OralRadiol. 2015;120(2):161–71.
Thongprasom K, Youngnak P, Aneksuk V. Hematologicabnormalities in recurrent oral ulceration. SoutheastAsian J Trop Med Public Health. 2002;33(4):872–7.
Topaloğlu Demir F, Kocatürk E, Yorulmaz E, Adalı G,Kavala M. Mucocutaneous manifestations of inflam-matory bowel disease in Turkey. J Cutan Med Surg.2014;18(6):397–404.
32 G. Lodi et al.

Tugal-Tutkun I, Onal S, Altan-Yaycioglu R, et al. Uveitisin Behcet disease: an analysis of 880 patients. Am JOphthalmol. 2004;138(3):373–80.
Veloso FT, Carvalho J, Magro F. Immune-related systemicmanifestations of inflammatory bowel disease. A pro-spective study of 792 patients. J Clin Gastroenterol.1996;23(1):29–34.
Victoria JM, Kalapothakis E, Silva Jde F, Gomez RS.Helicobacter pylori DNA in recurrent aphthous stoma-titis. J Oral Pathol Med. 2003;32(4):219–23.
Vidal-Alaball J, Butler CC, Cannings-John R, Goringe A,Hood K, McCaddon A, McDowell I, Papaioannou A.Oral vitamin B12 versus intramuscular vitamin B12 forvitamin B12 deficiency. Cochrane Database Syst Rev.2005;3:CD004655.
Volkov I, Rudoy I, Freud T, Sardal G, Naimer S, Peleg R,Press Y. Effectiveness of vitamin B12 in treating recur-rent aphthous stomatitis: a randomized, double-blind,placebo-controlled trial. J Am Board Fam Med.2009;22(1):9–16.
Wardhana, Datau EA. Recurrent aphthous stomatitiscaused by food allergy. Acta Med Indones.2010;42(4):236–40.
World Health Organization. Nutrition. Micronutrients.[Internet] 2016. Available from: www.who.int/
nutrition/topics/micronutrients/en/#. Accessed 19 Aug2016.
Wray D. A double-blind trial of systemic zinc sulfate inrecurrent aphthous stomatitis. Oral Surg Oral Med OralPathol. 1982;53(5):469–72.
Wray D, Ferguson MM, Mason DK, Hutcheon AW,Dagg JH. Recurrent aphthae: treatment withvitamin B12, folic acid, and iron. Br MedJ. 1975;2(5969):490–3.
Wray D, Ferguson MM, Hutcheon AW, Dagg JH. Nutri-tional deficiencies in recurrent aphthae. J Oral PatholMed. 1978;7(6):418–23.
Wray D, Vlagopoulos TP, Siraganian RP. Food allergensand basophil histamine release in recurrent aphthousstomatitis. Oral Surg Oral Med Oral Pathol.1982;54(4):388–95.
Wright A, Ryan FP, Willingham SE, Holt S, Page AC,Hindle MO, Franklin CD. Food allergy or intolerancein severe recurrent aphthous ulceration of the mouth. BrMed J (Clin Res Ed). 1986;292(6530):1237–8.
Yamamoto T, Yoneda K, Ueta E, Osaki T. Serum cyto-kines, interleukin-2 receptor, and soluble intercellularadhesion molecule-1 in oral disorders. Oral Surg OralMed Oral Pathol. 1994;78(6):727–35.
Oral Ulcerative Lesions 33


















