VENOUS THROMBOEMBOLISM( VTE ) DEEP VENOUS THROMBOSIS ( DVT ) PULMONARY THROMBOEMBOLISM( PTE )
Upload
arabella-terryCategory
view
218download
0
Chapter EightVenous Disease Coalition
Safe Use of Oral Anticoagulants
VTE Toolk i t

Action of Vitamin K Antagonists(Warafin)
VTE Toolk i t
• Inhibit the production of functional vitamin K dependent clotting factors II, VII, IX, X
• Also inhibit the anti-clotting factors Protein C & S
• Initial changes in INR reflect inhibition of Factor VII (shortest half-life); other factors take nearly a week to decrease to thrombosis-preventing levels
• 20-fold or greater range in maintenance dose among groups of patients (<1 mg/day to >20 mg/day)
• Contraindicated in pregnancy

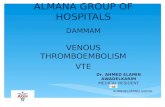
Mechanism of Action of Warafin
VTE Toolk i t
Hypofunctional clotting factors (II, VII, IX, X)
Functional clotting factors(II, VII, IX, X)
FoodGIB
GIB = gastrointestinal bacteria

Vitamin K Dependent Clotting Factors
VTE Toolk i t
XII
XI
IX
X
V
II (Thrombin)
I (Fibrinogen)
Fibrin clot
Tissue factor
aPTT PT/INR
VIII
VII

Factors Contributing to Patient Variability in Warafin Dose
VTE Toolk i t
• Age • Weight• Race• Liver disease• Heart failure• Genetics:
- cytochrome P450 2C9 polymorphisms (CYP 2C9) - vitamin K epoxide reductase (VKOR) polymorphisms
• Alcohol intake • Nutritional status • Diet• Activity level• Drug interactions
• Patient compliance• Who’s supervising anticoagulation

Factors Increasing Bleeding Risk on Oral Anticoagulants
VTE Toolk i t
1. Age > 752. Also receiving antiplatelet drugs3. Uncontrolled hypertension4. History of bleeding (GI, intracranial)5. Cancer6. Chronic renal failure7. Poorly controlled / poorly supervised
anticoagulant therapy

Long-Term Treatment of VTE with a Vitamin K Antagonist (Warafin)
VTE Toolk i t
• Target INR = 2.0 - 3.0
• Lower INR (1.5-1.9) is associated with increased VTE recurrence, but NOT decreased risk of bleeding

Warafin Therapy - Principles
VTE Toolk i t
• Patient and physician must be obsessive
• Do not order daily INR – use long-term trends
• Use a warfarin dosing sheet (for both MD and patient) = a longitudinal record of doses, INR results, next INR date
• Don’t over-react to just out-of-range INR values
• Stop ASA/clopidogrel unless indicated
• Manage hypertension aggressively
• Encourage vitamin K intake

Diet and Warafin Use
VTE Toolk i t
• Do NOT advise restriction of vitamin K-containing food – this is associated with less stable INR values
• Encourage foods high in vitamin K (broccoli, spinach, brussel sprouts)
• “Let me know if you plan a major change in your usual diet”

Warafin and Alcohol
VTE Toolk i t
• Binge drinking increases INR
may reduce compliance
increases UGI bleed risk
reduces the stability of anticoagulation
• Recommend moderation NOT abstinence

New Drugs and Warafin
VTE Toolk i t
• Assume new drugs might affect the INR
• For a known interaction (or uncertain):
- get INR 4-5 days after starting
• If INR was increased previously with the same antibiotic, reduce warfarin dose for a few days

ASA and Warafin Use
VTE Toolk i t
• Generally AVOID
• No additional benefit for most patients
• Definite increase in bleeding risk
• There must be a good reason for the ASA, e.g. coronary artery stent, high-risk mechanical heart valve, acute coronary syndrome, TIA/stroke on warfarin
• Therefore, the combination of an antiplatelet agent and warfarin must be an ACTIVE decision

NSAIDs and Warafin Use
VTE Toolk i t
• Not anticoagulants; minimal platelet inhibition
• Effect on INR unpredictable (may it)
• Like all meds, there should be a good reason for the NSAID
• If starting regular NSAID use, check INR 4-5 days later (if using PRN, don’t bother)
• If high-risk of GI bleeding avoid or add PPI (age >60, previous PUD, GERD, steroids)

What to do if INR is not whatwas expected
VTE Toolk i t
If the INR value is not what you expected, ask the question,
“Why did this happen?”

INR Higher than Expected
VTE Toolk i t
• Miscommunication about dosing by the doctor or patient
“Tell me what doses you’ve taken since the last INR”
• New medication – antibiotics, high dose acetaminophen, amiodarone, NSAIDs, statins, omeprazole, over-the counter drugs, herbals
• Substantial alcohol excess
• Inter-current illness
• Nutrition change – decrease vitamin K intake

INR Lower than Expected
VTE Toolk i t
• Compliance
• Compliance
• Compliance
• Miscommunication about dosing by the doctor or patient
“Tell me what doses you’ve taken since the last INR”
• Nutrition change – increase vitamin K intake
• New medication – ginseng, green tea

Reducing Warafin-RelatedBleeding in Practice
VTE Toolk i t
1. Things you CANNOT change• age• comorbid conditions
2. Things you CAN influence• careful management of hypertension• avoid combined ASA, other antiplatelets if
possible• excellent patient education• obsessive supervision and tracking• appropriate management of elevated INR

Venous Disease Coalition
www.vasculardisease.org/venousdiseasecoalition/
VTE Toolk i t