Venous thromboembolism (VTE) in obstetrics Dr.Roaa H. Gadeer MD.
Great state. Great opportunity.
Department of Health
Great state. Great opportunity.
Department of Health
Venous thromboembolism (VTE) prophylaxis in
pregnancy and the puerperium Clinical Guideline Education Presentation v2.0
45 minutes
Towards your CPD Hours
References: The Queensland Clinical Guideline Venous thromboembolism (VTE) prophylaxis in pregnancy and the puerperium is the primary reference for this package. Recommended citation: Queensland Clinical Guidelines. Venous thromboembolism (VTE) prophylaxis in pregnancy and the puerperium. Clinical guideline education presentation I14.54-V2-R19. Queensland Health. 2014. Disclaimer: This presentation is an implementation tool and should be used in conjunction with the published guideline. This information does not supersede or replace the guideline. Consult the guideline for further information and references. Feedback and contact details: M: GPO Box 48 Brisbane QLD 4001 | E: [email protected] | URL: www.health.qld.gov.au/qcg Funding: Queensland Clinical Guidelines is supported by the Clinical Access and Redesign Unit, Queensland Health. Copyright: © State of Queensland (Queensland Health) 2014 This work is licensed under a Creative Commons Attribution Non-Commercial No Derivatives 3.0 Australia licence. In essence, you are free to copy and communicate the work in its current form for non-commercial purposes, as long as you attribute the Queensland Clinical Guidelines , Queensland Health and abide by the licence terms. You may not alter or adapt the work in any way. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/3.0/au/deed.en For further information contact Queensland Clinical Guidelines, RBWH Post Office, Herston Qld 4029, email [email protected], phone (+61) 07 3131 6777. For permissions beyond the scope of this licence contact: Intellectual Property Officer, Queensland Health, GPO Box 48, Brisbane Qld 4001, email [email protected], phone (07) 3234 1479.
Queensland Clinical Guidelines: VTE prophylaxis in pregnancy & the puerperium 2

Abbreviations AOR Adjusted odds ratio IPC Intermittent pneumatic
compression APCR Activated protein C resistance IV Intravenous bd Twice daily LMWH Low molecular weight heparin BMI Body mass index PE Pulmonary embolism CI Confidence interval PPH Postpartum haemorrhage COCP Combined oral contraceptive
pill stat Immediately
CS Caesarean section UFH Unfractionated heparin DVT Deep vein thrombosis Subcut subcutaneous GCS Graduated compression
stockings VTE Venous thromboembolism
GI Gastrointestinal > Greater than HIT Heparin induced
thrombocytopenia ≥ Greater than or equal to
INR International normalised ratio Queensland Clinical Guidelines: VTE prophylaxis in pregnancy & the puerperium 3
Introduction
• PE & DVT – are two components of a single disease called VTE
• Pregnant women are at increased risk due to: ◦ Hypercoagulability ◦ Increased venous stasis ◦ Decreased venous outflow ◦ Compression of the inferior vena cava and
pelvic veins by enlarging uterus
Queensland Clinical Guidelines: VTE prophylaxis in pregnancy & the puerperium 4
Incidence
• A leading cause of maternal death • Risk greater postpartum • 40–60% of antenatal VTE occur 1st trimester • VTE rates estimated at 2/1000 pregnancies
◦ 75–80% events caused by DVT & 20–25% by PE ◦ 43–60% of PE occur 4–6 weeks postpartum
• DVT more likely to occur in left lower extremity
Queensland Clinical Guidelines: VTE prophylaxis in pregnancy & the puerperium 5

Communication
• Share & discuss information to support: ◦ Informed choice & consent ◦ Woman centred care
• Discuss management preferences • Provide culturally appropriate information:
◦ VTE ◦ Risks of VTE prophylaxis ◦ Symptoms suggestive of DVT & PE
Queensland Clinical Guidelines: VTE prophylaxis in pregnancy & the puerperium 6

Risk and benefit • Explain risks & benefits of VTE prophylaxis:
◦ Risk of VTE & consequences if no prophylaxis ◦ Relative effectiveness of treatment ◦ Burden of prolonged compliance with
treatment ◦ Cautions & contraindications to prophylactic
options
Queensland Clinical Guidelines: VTE prophylaxis in pregnancy & the puerperium 7

Risks of prophylaxis Patient-related risk factors for bleeding • Active bleeding • At risk of major haemorrhage (e.g. placenta previa) • Acquired or inherited bleeding disorders • Recent central nervous system bleeding • Intracranial or spinal lesion • Abnormal blood coagulation & thrombocytopenia • Severe platelet dysfunction • Active peptic ulcer or active ulcerative disease • Obstructive jaundice or cholestasis • Recent major surgical procedure • Medications that affect clotting process • Regional axial or recent lumbar puncture
Queensland Clinical Guidelines: VTE prophylaxis in pregnancy & the puerperium 8

Risks of prophylaxis Aspect Risk
Pharmacological prophylaxis
• Contraindications ◦ Known hypersensitivity ◦ History of or current HIT ◦ Creatinine clearance < 30 mL/minute
• Cautions ◦ Renal and/or hepatic impairment
Mechanical prophylaxis
• Caution where there is: ◦ Morbid obesity & ill fitting stocking ◦ Inflammatory conditions of lower legs ◦ Severe peripheral/diabetic neuropathy ◦ Severe oedema of legs ◦ Severe lower limb deformity
• IPC can exacerbate ischaemic disease Queensland Clinical Guidelines: VTE prophylaxis in pregnancy & the puerperium 9
Signs and symptoms Type Clinical presentation
PE
• Dyspnoea (most common)
• Palpitations • Chest pain • Haemoptysis
• Hypoxia/cyanosis • Tachycardia • Tachypnoea • Hypotension • Collapse
DVT
• Often proximal & may not present with usual features of distal DVT
• Unilateral leg pain • Swelling in extremity
• Increased calf/thigh circumference
• Increased temperature • Prominent superficial
veins • Pitting oedema
Queensland Clinical Guidelines: VTE prophylaxis in pregnancy & the puerperium 10
Clinical standards
• Educate clinicians about risk assessment • Document risk assessment • Develop written care plan • Measure & document observations
consistent with clinical situation • Use early warning tools/forms to detect
deterioration • Use standard forms for prophylactic &
therapeutic medications Queensland Clinical Guidelines: VTE prophylaxis in pregnancy & the puerperium 11
High risk factors
• Strongest personal risk factor for VTE in pregnancy is a history of thrombosis ◦ 15 – 25% of VTE in pregnancy are recurrent
events ◦ Thrombophilia is present in 20–50% of
women who experience VTE during pregnancy & postpartum
Queensland Clinical Guidelines: VTE prophylaxis in pregnancy & the puerperium 12

High risk factors
• Antenatal ◦ Single prior unprovoked VTE ◦ Single prior VTE pregnancy or COCP related ◦ Single prior VTE & thrombophilia ◦ Single prior VTE & family history of thrombophilia ◦ Prior recurrent VTE (>1) ◦ Family history VTE (but no personal history VTE) &
antithrombin deficiency • Postnatal
◦ Antenatal LMWH ◦ Any personal history of VTE
Queensland Clinical Guidelines: VTE prophylaxis in pregnancy & the puerperium 13

Known risk factors Risk factors
Socio-demographic
• Age (greater than 35 years)
• BMI ≥ 30 kg/m2
• Cigarette smoker (>10/day)
Medical history
• Single previous VTE with no family history VTE or thrombophilia
• Thrombophilia and no previous VTE
• Family history VTE • Antiphospholipid
syndrome • Thrombophilia (inherited
or acquired) • Sickle cell disease
• Ovarian hyperstimulation syndrome
• Gross varicose veins • Inflammatory conditions • Nephrotic syndrome • Cancer • Pre-existing diabetes • Cardiac or lung disease • Systemic lupus
erythematosous
Queensland Clinical Guidelines: VTE prophylaxis in pregnancy & the puerperium 14

Known risk factors Risk factors
Pregnancy related
• Immobility • Preeclampsia/eclampsia • Artificial reproductive
therapy (ART) • Gestational diabetes • Multiparity (> 2 or 3) • Multiple pregnancy • Intrauterine growth
restriction
• Hyperemesis/dehydration • Current systemic
infection (requiring antibiotics or hospitalisation)
• Antepartum haemorrhage
• Surgical procedure in pregnancy
Birth/ Postpartum
• Prolonged labour (> 24 hours)
• CS or operative vaginal birth
• Stillbirth • Preterm birth
• PPH (> 1L) • Transfusion • Surgical procedure in
puerperium • Postpartum infection
Queensland Clinical Guidelines: VTE prophylaxis in pregnancy & the puerperium 15

Risk assessment
• Failure to recognise and/or treat risk factors contributes to maternal mortality & morbidity
• Assess for risk factors in early pregnancy or before conception – repeat if change in risk status & following birth ◦ Ask about symptoms ◦ Commence prophylaxis at times of additional risk
• Assess risk of bleeding and/or contraindications to prophylaxis before offering VTE prophylaxis
• Formulate an overall risk assessment
Queensland Clinical Guidelines: VTE prophylaxis in pregnancy & the puerperium 16

Risk assessment
• Evidence correlating risk factors & occurrence of VTE is imprecise with wide & sometimes contradictory risk estimates
• Presence of multiple risk factors may have additive or synergistic effects but the combinations with the greatest risk are unknown
Queensland Clinical Guidelines: VTE prophylaxis in pregnancy & the puerperium 17

Risk assessment criteria
Queensland Clinical Guidelines: VTE prophylaxis in pregnancy & the puerperium 18
Risk assessment Antenatal criteria Postnatal criteria
All risk • All pregnant women • All postnatal women
Therapeutic anticoagulation
• Pre-pregnancy therapeutic anticoagulation
• Antenatal therapeutic anticoagulation
High risk • 1 or more antenatal high risk factors
• 1 or more postnatal high risk factors
Moderate risk • 3 or more risk factors • If hospitalised, 2 or
more risk factors
• Emergency CS in labour
• 3 or more risk factors
Lower risk • 0-2 antenatal risk factors
• 1-2 postnatal risk factors
Additional assessments
Queensland Clinical Guidelines: VTE prophylaxis in pregnancy & the puerperium 19
Aspect Consideration
Previous VTE
• Family history of VTE increases risk two-fold • Refer woman with history of VTE to
practitioner experienced in VTE prophylaxis • All women with previous VTE require full
thrombophilia screen
Pre-existing conditions
• Liaise with experienced team • Multidisciplinary approach • Individualise thromboprophylaxis • Refer to anaesthetics for peripartum plan

Mechanical prophylaxis • Graduate compression stockings (GCS)
◦ Compliance essential ◦ Contraindicated in critical limb ischemia ◦ Individually measure & fit ◦ Check skin integrity regularly
• Intermittent pneumatic compression (IPC) combined with other prophylactic modalities has been shown to decrease the incidence of DVT in high-risk non-pregnant patients
Queensland Clinical Guidelines: VTE prophylaxis in pregnancy & the puerperium 20

Pharmacological prophylaxis • Determine dose (standard, intermediate or
therapeutic) based on individual risk assessment
• Low Molecular Weight Heparin (LMWH) ◦ Agent of choice for antenatal thromboprophylaxis ◦ Does not cross placenta/No evidence of
teratogenicity ◦ Associated with fewer bleeding episodes compared
with Unfractionated Heparin (UFH) ◦ Risk of HIT/ osteoporosis lower with LMWH
Queensland Clinical Guidelines: VTE prophylaxis in pregnancy & the puerperium 21

• UFH • Warfarin:
◦ Contraindicated for antenatal thromboprophylaxis ◦ Consider postnatal only for prolonged
thromboprophylaxis or treatment ◦ If warfarin used pre-pregnancy recommence
postpartum
• LMWH, UFH & Warfarin safe for B/Feeding
Queensland Clinical Guidelines: VTE prophylaxis in pregnancy & the puerperium 22
Pharmacological prophylaxis
Newer agents
• Safety info limited about newer agents • The American College of Chest Physicians
recommend: ◦ Limit use of Fondaparinux for severe allergic
reactions to Heparin and cannot receive Danaparoid ◦ Avoid oral direct thrombin (e.g. Dabigatran) & Factor-
Xa inhibitors (e.g. Rivaroxaban, Apixaban) ◦ Breastfeeding women use alternative anticoagulants
rather than Fondaparinux & Factor Xa inhibitors • Not recommended with neuraxial blockade • Discuss newer agents with experienced team
Queensland Clinical Guidelines: VTE prophylaxis in pregnancy & the puerperium 23
Aspirin
• No controlled trials on use of aspirin for thromboprophylaxis in pregnancy
• The American College of Physicians recommend against aspirin for VTE in any patient group
• No adverse fetal outcomes reported in a meta-analysis of large RCTs of low-dose aspirin for prevention of preeclampsia
• Insufficient evidence to recommend routine aspirin for thromboprophylaxis in antenatal & postnatal period
Queensland Clinical Guidelines: VTE prophylaxis in pregnancy & the puerperium 24

Prophylactic management
• Minimise immobilisation & dehydration • Routine laboratory thrombophilia
screening not recommended • If anticoagulation required peripartum use
a multidisciplinary team approach • Develop a plan for the peripartum
management of anticoagulation (prophylactic or therapeutic)
Queensland Clinical Guidelines: VTE prophylaxis in pregnancy & the puerperium 25
Prophylactic management
• If identified risk factor(s) include any of the following, refer to Section 5 of clinical guideline for specific management: ◦ Significant personal history of VTE ◦ Thrombophilia ◦ Antiphospholipid syndrome ◦ Long-term therapeutic coagulation
Queensland Clinical Guidelines: VTE prophylaxis in pregnancy & the puerperium 26
Antenatal prophylaxis
Queensland Clinical Guidelines: VTE prophylaxis in pregnancy & the puerperium 27
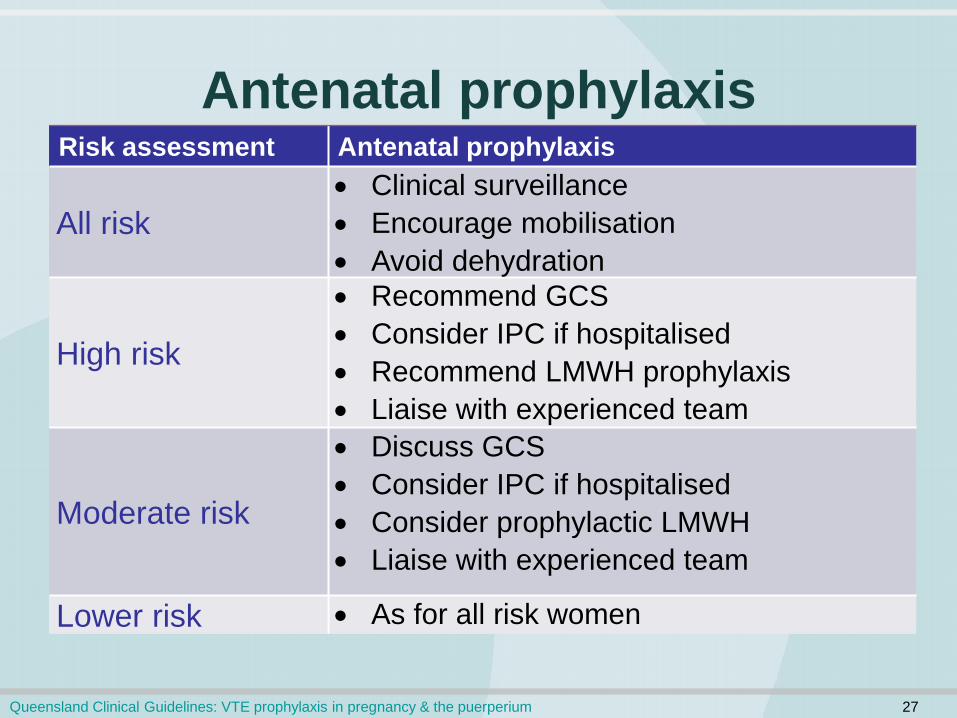
Risk assessment Antenatal prophylaxis
All risk • Clinical surveillance • Encourage mobilisation • Avoid dehydration
High risk
• Recommend GCS • Consider IPC if hospitalised • Recommend LMWH prophylaxis • Liaise with experienced team
Moderate risk
• Discuss GCS • Consider IPC if hospitalised • Consider prophylactic LMWH • Liaise with experienced team
Lower risk • As for all risk women

Intrapartum prophylaxis
• If receiving intermediate or high risk antenatal thromboprophylaxis: ◦ Document and discuss a plan of care that considers
individual risk factors & clinical circumstances • Liaise with multidisciplinary team re:
◦ Timing of anticoagulation cessation prior to established labour/planned birth
◦ Timing for recommencement of thromboprophylaxis following birth
• Consider precautions related to neuraxial blockade
Queensland Clinical Guidelines: VTE prophylaxis in pregnancy & the puerperium 28
Postnatal prophylaxis
• Begin as soon as possible after birth • Risk greater after CS • Vaginal birth with multiple risk factors may
still require specific prophylaxis • UFH may be substituted for LMWH at
obstetrician/physician’s discretion • Consider precautions regarding neuraxial
blockade management
Queensland Clinical Guidelines: VTE prophylaxis in pregnancy & the puerperium 29
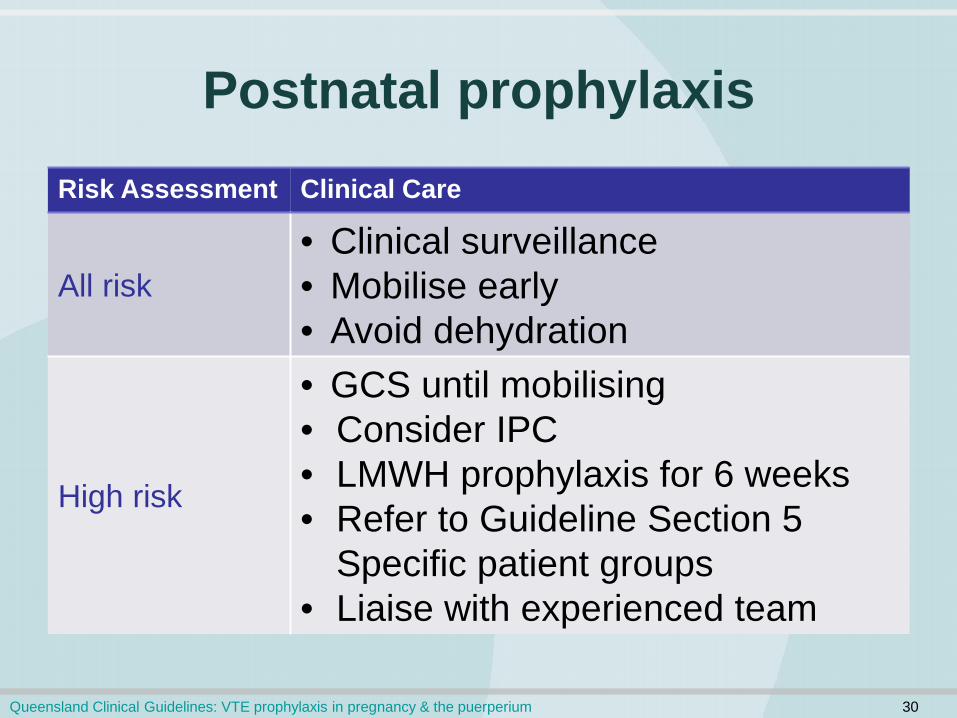
Postnatal prophylaxis Risk Assessment Clinical Care
All risk • Clinical surveillance • Mobilise early • Avoid dehydration
High risk
• GCS until mobilising • Consider IPC • LMWH prophylaxis for 6 weeks • Refer to Guideline Section 5
Specific patient groups • Liaise with experienced team
Queensland Clinical Guidelines: VTE prophylaxis in pregnancy & the puerperium 30
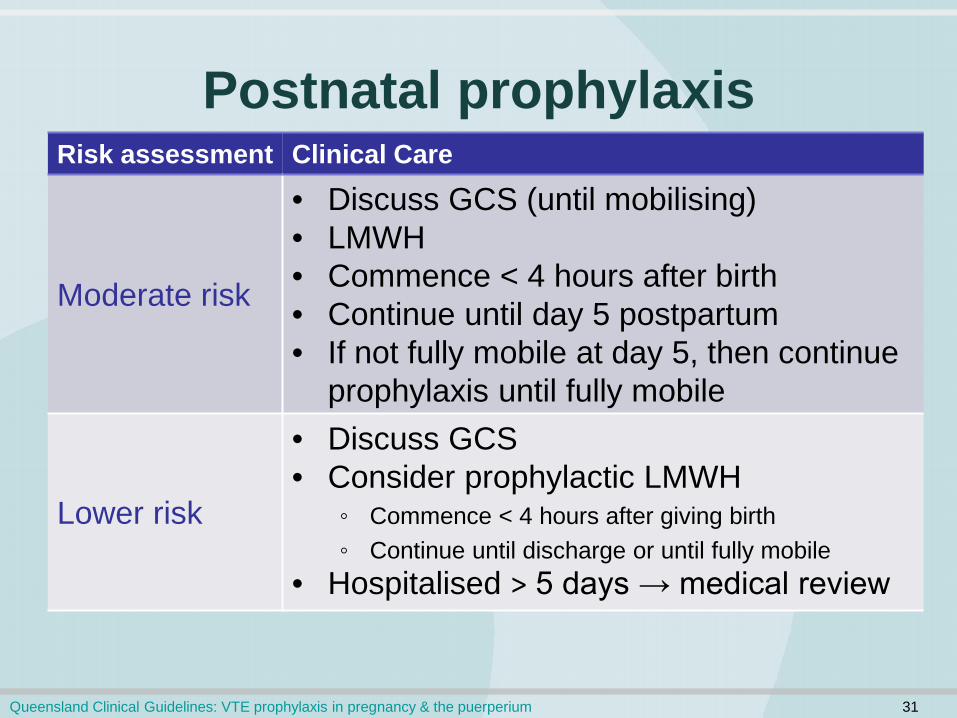
Postnatal prophylaxis Risk assessment Clinical Care
Moderate risk
• Discuss GCS (until mobilising) • LMWH • Commence < 4 hours after birth • Continue until day 5 postpartum • If not fully mobile at day 5, then continue
prophylaxis until fully mobile
Lower risk
• Discuss GCS • Consider prophylactic LMWH
◦ Commence < 4 hours after giving birth ◦ Continue until discharge or until fully mobile
• Hospitalised > 5 days → medical review
Queensland Clinical Guidelines: VTE prophylaxis in pregnancy & the puerperium 31

Neuraxial blockade
Queensland Clinical Guidelines: VTE prophylaxis in pregnancy & the puerperium 32
Aspect Clinical care
Context
• Safety of a neuraxial blockade depends on anticoagulant used, timing of insertion; whether catheter is left in situ, timing of removal
• Spinal haematoma is a clinical emergency • Consider risk & benefit relative to clinical
situation
Plan care
• Formulate written care plan • Refer to & discuss with anaesthetic team • Monitor for neuraxial haematoma for 24
hours after insertion or removal

Neuraxial blockade
Queensland Clinical Guidelines: VTE prophylaxis in pregnancy & the puerperium 33
Aspect Clinical care
LMWH prophylactic dose
• Wait at least 12 hours after LMWH dose before performance of neuraxial block or removal of catheter
• Wait at least 4 hours following neuraxial blockade or neuraxial catheter removal before giving subsequent LMWH dose
LMWH therapeutic dose
• Avoid therapeutic dosing with catheter in situ • Wait at least 24 hours after last therapeutic
dose LMWH before performing neuraxial blockade or removing catheter
• Wait at least 4 hours after performing neuraxial blockade or removing catheter before giving subsequent LMWH dose
Neuraxial blockade
Queensland Clinical Guidelines: VTE prophylaxis in pregnancy & the puerperium 34
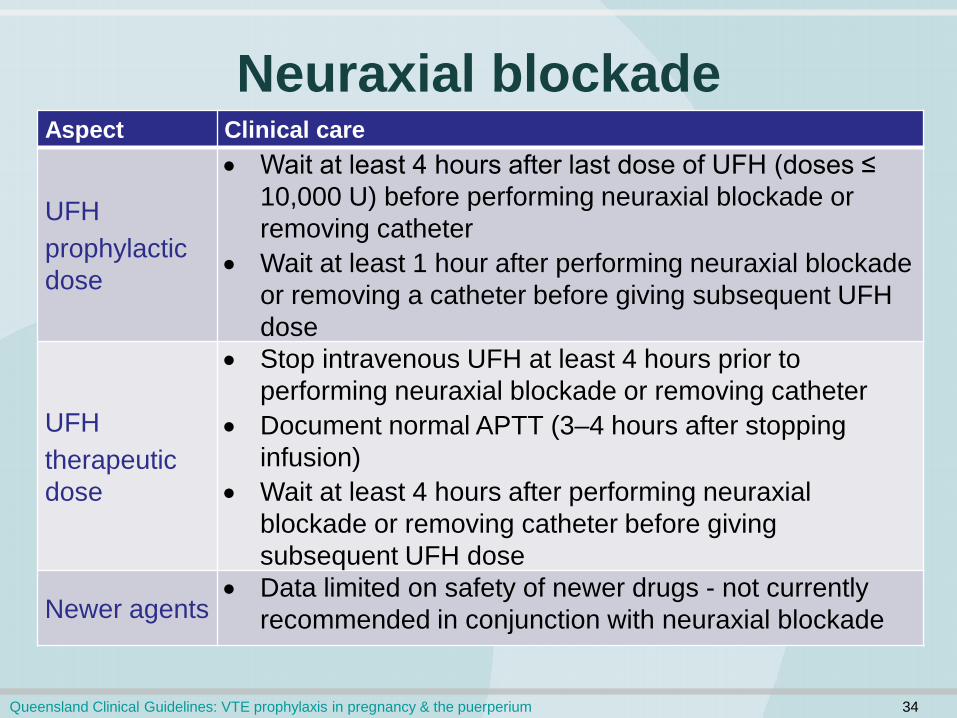
Aspect Clinical care
UFH prophylactic dose
• Wait at least 4 hours after last dose of UFH (doses ≤ 10,000 U) before performing neuraxial blockade or removing catheter
• Wait at least 1 hour after performing neuraxial blockade or removing a catheter before giving subsequent UFH dose
UFH therapeutic dose
• Stop intravenous UFH at least 4 hours prior to performing neuraxial blockade or removing catheter
• Document normal APTT (3–4 hours after stopping infusion)
• Wait at least 4 hours after performing neuraxial blockade or removing catheter before giving subsequent UFH dose
Newer agents • Data limited on safety of newer drugs - not currently
recommended in conjunction with neuraxial blockade
Specific patient groups • Limited evidence to determine best practice • Assess each woman individually • Refer to experienced physician • Where pharmacological prophylaxis
indicated, also consider mechanical methods
(Refer to Clinical Guideline Table 12. Antenatal and postnatal management of specific patient groups)
Queensland Clinical Guidelines: VTE prophylaxis in pregnancy & the puerperium 35
Discharge information
• Provide information on: ◦ Signs & symptoms of VTE ◦ Importance of prophylaxis ◦ Reducing risk ◦ Correct use/application & duration of treatment ◦ Importance of seeking help & who to contact ◦ Anti-coagulation for subsequent pregnancies
• Complete a discharge summary/referral
Queensland Clinical Guidelines: VTE prophylaxis in pregnancy & the puerperium 36

Appendices
Appendix A Drug information
Appendix B Adjusted odds ratio (AOR) for risk of VTE
Appendix C Risk of VTE with Thrombophilia
Queensland Clinical Guidelines: VTE prophylaxis in pregnancy & the puerperium 37