Chapter 22 - Canadian Pharmacists Association chapters/CTMA... · Chapter 22 ChapterAllergic 22...
23
Copyright © Canadian Pharmacists Association. All rights reserved. Compendium of Therapeutics for Minor Ailments Respiratory Conditions Chapter 22 Chapter 22 Allergic Rhinitis Jennifer Kendrick, BScPharm, ACPR, PharmD Pathophysiology Allergic rhinitis affects 10–30% of the population, and the prevalence is increasing. 1,2,3 It is estimated that more than 500 million people worldwide are affected. 3 The prevalence of allergic rhinitis is thought to be highest in school-age children; 80% of people with allergic rhinitis are diagnosed before 20 years of age. 1,4 Allergic rhinitis is associated with a genetic predisposition; children have a 30% chance of developing allergic rhinitis if one parent is affected and a 50% chance if both are affected. 5,6 Allergic rhinitis is characterized by inflammation of the nasal mucosa following inhalation of an allergen. 1,4,6,7 The allergic reaction is mediated by antigen-antibody responses and takes place in 3 phases. The first phase, sensitization, occurs on first contact with the allergen. IgE is produced and binds to receptors on the surface of mast cells and basophils. The second and third phases occur on re- exposure to an allergen in a sensitized individual. The second phase, immediate reaction, occurs within minutes of re-exposure and lasts up to 30–90 minutes. In this phase the allergen binds to allergen- specific IgE and the mast cells release preformed mediators, histamine and tumor necrosis factor alpha (TNF-α), and newly generated mediators, leukotrienes LTC4, LTD4, LTE4, prostaglandin D2 and kinins. The third phase, late reaction, occurs 4–8 hours after exposure. It is characterized by migration of inflammatory cells, eosinophils, monocytes, macrophages and basophils. Allergic rhinitis was previously classified as seasonal or perennial; however, this classification was determined to be inadequate for a number of reasons. For example, outdoor pollens and moulds may be perennial in some regions and symptoms of perennial allergy may not be present year-round. The Allergic Rhinitis and its Impact on Asthma (ARIA) guideline proposed the classifications of intermittent allergic rhinitis (IAR) and persistent allergic rhinitis (PAR) in 2008. 3 IAR is defined as symptoms of allergic rhinitis occurring <4 days/week or for <4 weeks at a time. PAR is defined as symptoms of allergic rhinitis occurring ≥4 days/week and for ≥4 weeks at a time. Allergic rhinitis is further classified based on severity. In mild allergic rhinitis, symptoms are present but not troublesome and there is no impairment in daily activities, school or work and no sleep disturbance. In moderate/ severe allergic rhinitis, one or more is present: troublesome symptoms, impairment in daily activities, school or work, or sleep disturbance. 3,7 The ARIA classification has been validated in both adults and children. Rhinitis may also be nonallergic. Conditions associated with nonallergic rhinitis are listed in Table 1. Drugs associated with rhinitis are listed in Table 2. Goals of Therapy ■ Prevent symptoms by avoiding exposure to allergen(s) ■ Alleviate signs and symptoms produced by the allergic response ■ Improve quality of life 226 Respiratory Conditions
Transcript of Chapter 22 - Canadian Pharmacists Association chapters/CTMA... · Chapter 22 ChapterAllergic 22...

Copyright © Canadian Pharmacists Association. All rights reserved. Compendium of Therapeutics for Minor Ailments
Respiratory Conditions
Chapter 22Chapter 22Allergic RhinitisJennifer Kendrick, BScPharm, ACPR, PharmD
PathophysiologyAllergic rhinitis affects 10–30% of the population, and the prevalence is increasing.1,2,3 It is estimatedthat more than 500 million people worldwide are affected.3 The prevalence of allergic rhinitis isthought to be highest in school-age children; 80% of people with allergic rhinitis are diagnosed before20 years of age.1,4 Allergic rhinitis is associated with a genetic predisposition; children have a 30%chance of developing allergic rhinitis if one parent is affected and a 50% chance if both are affected.5,6
Allergic rhinitis is characterized by inflammation of the nasal mucosa following inhalation of anallergen.1,4,6,7 The allergic reaction is mediated by antigen-antibody responses and takes place in 3phases. The first phase, sensitization, occurs on first contact with the allergen. IgE is produced andbinds to receptors on the surface of mast cells and basophils. The second and third phases occur on re-exposure to an allergen in a sensitized individual. The second phase, immediate reaction, occurs withinminutes of re-exposure and lasts up to 30–90 minutes. In this phase the allergen binds to allergen-specific IgE and the mast cells release preformed mediators, histamine and tumor necrosis factor alpha(TNF-α), and newly generated mediators, leukotrienes LTC4, LTD4, LTE4, prostaglandin D2 andkinins. The third phase, late reaction, occurs 4–8 hours after exposure. It is characterized by migrationof inflammatory cells, eosinophils, monocytes, macrophages and basophils.
Allergic rhinitis was previously classified as seasonal or perennial; however, this classification wasdetermined to be inadequate for a number of reasons. For example, outdoor pollens and moulds maybe perennial in some regions and symptoms of perennial allergy may not be present year-round. TheAllergic Rhinitis and its Impact on Asthma (ARIA) guideline proposed the classifications ofintermittent allergic rhinitis (IAR) and persistent allergic rhinitis (PAR) in 2008.3 IAR is defined assymptoms of allergic rhinitis occurring <4 days/week or for <4 weeks at a time. PAR is defined assymptoms of allergic rhinitis occurring ≥4 days/week and for ≥4 weeks at a time. Allergic rhinitis isfurther classified based on severity. In mild allergic rhinitis, symptoms are present but not troublesomeand there is no impairment in daily activities, school or work and no sleep disturbance. In moderate/severe allergic rhinitis, one or more is present: troublesome symptoms, impairment in daily activities,school or work, or sleep disturbance.3,7 The ARIA classification has been validated in both adults andchildren.
Rhinitis may also be nonallergic. Conditions associated with nonallergic rhinitis are listed in Table 1.Drugs associated with rhinitis are listed in Table 2.
Goals of Therapy■ Prevent symptoms by avoiding exposure to allergen(s)■ Alleviate signs and symptoms produced by the allergic response■ Improve quality of life
226 Respiratory Conditions

Compendium of Therapeutics for Minor Ailments Copyright © Canadian Pharmacists Association. All rights reserved.
Table 1: Possible Nonallergic Causes of Acute and Chronic Rhinitis3,4,6,7
■ Drug-induced (see )■ Hormones
– pregnancy, menstruation, hypothyroidism■ Infection
– viral, bacterial, fungal, other■ Nonallergic rhinitis with eosinophilia syndrome (NARES)■ Other
– emotions, e.g., stress, sexual arousal– vasomotor rhinitis, e.g., exercise, cold air– anatomic abnormalities, e.g., nasal septal deviation, enlarged adenoids and tonsils, nasal tumors, choanal atresiaa
– food and alcohol– nasal polyps– atrophy– foreign body
a A congenital defect where the posterior nares do not communicate with the nasopharynx.
Table 2: Drugs Associated with Rhinitis6,8
■ ACE inhibitors■ ASA and other NSAIDs■ Cocaine■ Diuretics, e.g., amiloride, hydrochlorothiazide■ Gabapentin■ Hydralazine
■ Oral contraceptives■ Phosphodiesterase-5 inhibitors, e.g., sildenafil■ Psychotropics, e.g., chlorpromazine, risperidone■ Sympatholytics, e.g., clonidine, doxazosin, methyldopa,
phentolamine, prazosin■ Topical decongestants (prolonged use)
Patient AssessmentThe sensitization phase of allergic rhinitis is asymptomatic. Symptoms of the second or immediatephase include sneezing, nasal and palatal pruritus, congestion and clear rhinorrhea.9 Symptoms of thedelayed phase are similar but nasal congestion predominates.4 Patients may also have itchy, red,watery eyes (allergic conjunctivitis), itchy throat, ear fullness and popping, and a feeling of pressureover the cheeks and forehead.4 Facial signs of allergic rhinitis are illustrated in Figure 1. The allergicsalute is a sign more commonly seen in children, where the patient wipes the nose with the palm of thehand in an upward motion.
Some patients present primarily with symptoms of sneezing and rhinorrhea, whereas others are mostlybothered by nasal blockage and have little or no itching or sneezing.6 Eye symptoms are morecommonly associated with outdoor allergens.3,7
Allergic rhinitis can have a significant impact on a patient's quality of life. Patients may haveheadache, difficulty concentrating, fatigue or sleep disturbance.6 Malaise or fatigue may be presentingcomplaints in children.9 Complications of allergic rhinitis include sinusitis, otitis media, asthma, andsleep apnea. In children, there may be dental overbite and a high-arched palate due to chronic mouthbreathing.3,6
An assessment plan for patients suffering from allergic rhinitis is illustrated in Figure 2. During theassessment, also identify precipitating factors/allergens and assess occupational exposure and responseto previous therapy.
Chapter 22: Allergic Rhinitis 227

Copyright © Canadian Pharmacists Association. All rights reserved. Compendium of Therapeutics for Minor Ailments
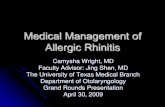
Figure 1: Facial Signs of Allergic Rhinitis
Morgan's Lines or Dennie's sign or folds are extra creases at the lower eyelids due to edema. Allergic shiners describe discoloured infraorbital areas due tovenous stasis resulting from nasal swelling. The transverse nasal crease is a crease seen at the junction of the bulbous portion of the nose and thenosebridge and is caused by recurrent nose rubbing (allergic salute). Conjunctival injection refers to conjunctival redness fading toward the edges.
Consider the need for prescription therapy or referral for allergy testing if the patient has already triedappropriate nonprescription therapy for 2 weeks without an adequate response, or if the allergenresponsible for symptoms cannot be readily identified.3 Also refer patients for further assessment ifthey have signs or symptoms that are unilateral or are not usually associated with allergic rhinitis (e.g.,fever, pain, loss of smell or taste, recurrent epistaxis, purulent nasal or ocular secretions, postnasal dripwith or without rhinorrhea) or symptoms suggesting complications such as asthma.3
PreventionPrevention is the first step in the management of allergic rhinitis. Although consensus is thatimprovement in symptoms should occur with allergen avoidance, little evidence supports individualmeasures.3 While some measures such as washing pets, impermeable covers for bedding, and airfiltration have been shown to reduce the allergen level, a corresponding reduction in allergic symptomshas not been shown.9 The benefits of environmental control may take weeks or months to fullymanifest. Avoidance measures for common allergens are presented below.1,3,6,7
Pollen■ Keep windows and doors closed when at home or in the car.■ If using air conditioning, keep the unit on recirculate or the indoor cycle, if the choice is available.■ Do not use window or attic fans.■ Monitor weather reports on pollen counts, if available. Decrease outdoor exposure during periods
of high pollen counts. Pollen counts tend to be highest on sunny, windy days.■ Do not dry clothing outdoors.■ Shower or bathe and wash hair after outdoor activity to remove pollen from hair and skin and
prevent contamination of bedding.
228 Respiratory Conditions

Compendium of Therapeutics for Minor Ailments Copyright © Canadian Pharmacists Association. All rights reserved.
Outdoor Moulds■ Remain in a closed environment as much as possible.■ If using air conditioning, keep the unit on the indoor cycle, if the choice is available; note, however,
that units can be heavily contaminated with mould.■ Use of face masks for activities such as raking leaves or working with compost or dry soil may
have limited value because air seeps around the edges of the mask and the mask does not protectthe eyes.
Indoor Moulds■ Use fungicide on sinks, shower stalls, nonrefrigerated vegetable storage areas and garbage pails. A
solution of equal parts household bleach and water effectively kills mould.■ Avoid console humidifiers and cool mist vaporizers; if these must be used, keep them scrupulously
clean.■ If the home is built over a crawl space, install a plastic vapor barrier over exposed soil and keep
foundation vents open.■ If the basement is damp or tends to flood, avoid carpeting or furnishing the basement. Use a
dehumidifier at all times and empty the extracted water from the air frequently; remove anystanding water as soon as possible.
■ Remove houseplants, which are a common source of mould. Alternatively, keep soil surface dryand clean of debris to reduce mould.
House Dust Mites■ Avoid carpeting the bedroom and main living areas.■ Plastic, leather or wood furniture is best.■ Some acaricides (e.g., benzyl benzoate, tannic acid) appear to reduce the mite population if used
regularly. However, their clinical effect is not established and they are not routinely recommended.3■ If possible, clean while the allergic individual is not at home.■ Mite-sensitive persons should avoid vacuuming or making beds. Those who must do their own
cleaning should wear a facemask during cleaning and for 10–15 minutes afterward.■ Use a vacuum cleaner with an efficient double filtration system.■ Keep indoor humidity between 40% and 45%.■ Minimize use of humidifiers as excess humidity promotes mite growth.■ Encase all mattresses, box springs and pillows in the allergic individual's bedroom in zippered,
allergen-proof casings.■ Consider replacing old mattresses.■ Wash bedding in hot (>55°C) water at least every 2 weeks. Cooler water temperatures will not kill
dust mites, nor will detergents.■ Avoid stuffed toys that cannot be washed. Alternatively, put stuffed toys or pillows in a hot dryer or
in plastic bags and freeze every 2 weeks to kill dust mites.■ Do not store items under the bed.■ Use window shades instead of venetian blinds.■ Evidence suggests the best strategy is a combination of the above interventions.10
Chapter 22: Allergic Rhinitis 229

Copyright © Canadian Pharmacists Association. All rights reserved. Compendium of Therapeutics for Minor Ailments
Animal Allergens■ Permanent removal of pets from the home is the best way to control animal allergens. This should
be followed by thorough cleaning of the house, including washing carpets. “Trial” removal of petsis not helpful; it can take 20 weeks or longer for cat allergen levels to drop to levels comparable tohomes without cats.
■ If the family is unable to remove the animal from the home then:– remove carpets and replace with hard flooring– keep the animal away from the allergic individual's bedroom and other living areas where the
allergic individual spends time– a high-efficiency particulate air (HEPA) filter or electrostatic air purifier may be helpful– washing cats weekly and dogs once or twice weekly may help but evidence to support this
approach is lacking– eliminate litter boxes if possible; otherwise place them in an area unconnected to the air supply
for the rest of the house.
Occupational Allergens■ For individuals affected by occupational rhinitis, recommend minimizing or eliminating exposure.■ Common causes of occupational rhinitis include animal or vegetable proteins (e.g., mouse, rat,
wheat, grains, latex), enzymes, pharmaceuticals (e.g., antibiotics) and chemicals (e.g., resins).
Nonpharmacologic TherapyIntranasal saline spray and irrigation has been shown to reduce nasal symptoms and the need forpharmacologic therapy in children and nonpregnant adults.11 The effect of intranasal saline irrigationin pregnant women is less clear.12 Isotonic saline is preferred to hypertonic saline, as it improvesmucociliary clearance; however, the optimal dose, frequency and delivery have not been established.11
Tobacco smoke can aggravate symptoms and should be avoided by all patients with allergic rhinitis.3Other irritants that should be avoided include insect sprays, air pollution and fresh tar or paint.3
Pharmacologic TherapyWhen avoidance of allergens is ineffective or impractical, consider pharmacologic options. If it ispossible to predict the onset of symptoms (e.g., intermittent exposure), prophylactic medication shouldbe started before exposure.
For comparative ingredients of nonprescription products, consult the Compendium of Products forMinor Ailments—Cough, Cold and Allergy Products.
Table 3 summarizes the pharmacologic activity of different therapies for the treatment of allergicrhinitis.
Medications for treatment of allergic rhinitis are described in Table 5 and Table 6.
Several guidelines for the treatment of allergic rhinitis are available and each provides similartreatment recommendations.3,6,7,9 For mild symptoms, second-generation antihistamines are thedrugs of choice, although they produce only a modest improvement in nasal congestion. First-generation antihistamines are no longer recommended first-line due to their adverse effect profile.6For moderate to severe allergic rhinitis, regularly administered intranasal corticosteroids arerecommended as first-line therapy.14
230 Respiratory Conditions

Compendium of Therapeutics for Minor Ailments Copyright © Canadian Pharmacists Association. All rights reserved.
Table 3: Comparative Symptom Relief of Allergic Rhinitis Therapies7,13
Medication Rhinorrhea Congestion Sneezing Nasal ItchEye
Symptomsa
Oral antihistamines + +/- + + +/-
Intranasal mast cell stabilizers +/- +/- +/- +/- -
Decongestants (oral and topical) - + - - -
Intranasal corticosteroids ++ ++ ++ ++ +/-
Leukotriene receptor antagonists + + +/- +/- +/-
Intranasal anticholinergics ++ - - - -
Intranasal antihistamines ++ ++ ++ ++ +/-
a See Chapter 13: Conjunctivitis.Abbreviations: (+/-) = modest or variable effect
AntihistaminesIntroduced in the 1940s, antihistamines were the first medications used for the treatment of allergicrhinitis. They act as competitive antagonists for the histamine-1 (H1) receptor found on the surface oftarget cells in the nose, lung, conjunctiva and skin.15 They also act as a reverse agonist, meaning thatthey change the three-dimensional configuration of the receptor, decreasing its affinity for histamineand down-regulating histamine-driven symptoms.15 Antihistamines decrease nasal itching, sneezing,rhinorrhea, conjunctival itching and lacrimation but generally do not relieve nasal congestion.Desloratadine, fexofenadine and cetirizine have modest effects on nasal congestion.16Antihistamines are first-line treatment in mild cases of allergic rhinitis.3,6,9
Antihistamines are divided into 2 major classes: first- and second-generation. All are similarlyeffective; however, adverse effect profiles and pharmacology differ.15,17,18,19,20,21
First-generation antihistamines have a rapid onset but relatively short duration of action due to theirshort half-life.22,23 They are poorly selective for the H1 receptor and also exert effects on cholinergicreceptors. The anticholinergic effect manifests as dry mouth and nasal passages, difficulty voidingurine, constipation and tachycardia. They are also highly lipophilic and therefore cross the blood-brainbarrier and interact with central H1 receptors. This results in CNS effects such as sedation andpsychomotor and cognitive impairment. In children, paradoxical excitation may occur.24 Performanceimpairment has been documented using various measures (e.g., reaction time, visual-motorcoordination, arithmetical exercises and memory, learning and driving tests) although more recent datasuggest that the magnitude of these effects has been overstated.25,26 CNS depression and impairmentcan be independent of any subjective complaints by the patient.27 First-generation antihistamines alsoimpair learning and academic performance in children.27 Workers taking first-generationantihistamines have lower work performance and are more likely to be involved in workplaceaccidents. Daytime performance effects are noted even when the antihistamine is taken only atbedtime.6,27
First-generation antihistamines can decrease rhinorrhea, but mucus secretion may be thickened and canbe more bothersome for some patients.15
The first-generation antihistamines should be used with caution in patients with narrow-angleglaucoma, stenosing peptic ulcer, pyloroduodenal obstruction, symptomatic prostatic hypertrophy orbladder-neck obstruction, cardiovascular disease and chronic lung disease.
Chapter 22: Allergic Rhinitis 231

Copyright © Canadian Pharmacists Association. All rights reserved. Compendium of Therapeutics for Minor Ailments
Second-generation antihistamines are more selective for H1 receptors and less lipophilic.Consequently, they do not have significant anticholinergic adverse effects and do not cross the blood-brain barrier.20 Use of cetirizine in standard doses is associated with more sedation compared withplacebo, but less than first-generation antihistamines.6 Administration of standard doses of loratadineand desloratadine results in an incidence of sedation equivalent to placebo; however, drowsiness hasbeen reported at higher than recommended doses, or rarely in susceptible individuals at recommendeddoses.6 Fexofenadine appears to be nonsedating, even at increased doses. Due to their improvedadverse effect profile, especially with regard to sedation and psychomotor performance, second-generation antihistamines represent a better choice than first-generation agents for the treatment ofallergic rhinitis.6,14 Clinical trials comparing various second-generation antihistamines demonstratesimilar reduction of symptoms.2,19,21,28 They are less effective than intranasal corticosteroids for mostsymptoms of allergic rhinitis.6 Two meta-analyses demonstrated intranasal corticosteroids were moreeffective than antihistamines for relieving congestion and sneezing; for ocular symptoms, nodifference was found.29,30
The intranasal antihistamine levocabastine is effective for sneezing, nasal pruritus and rhinorrhea. Ithas a rapid onset of action (<15 minutes), but must be used 2–4 times daily.22 The intranasalantihistamine azelastine (available only in combination with fluticasone in Canada) is clinicallysimilar to oral second-generation antihistamines for the relief of nasal symptoms.30
Antihistamines are more effective when taken before allergen exposure. The best results are obtainedwith chronic dosing compared with intermittent dosing; therefore, patients should take theantihistamine for as long as they are in contact with the allergen.14 If one antihistamine is not effective,switching to another antihistamine may be beneficial.31
Mast Cell StabilizersSodium cromoglycate (also called cromolyn sodium) modestly reduces itching, sneezing andrhinorrhea but is not effective for nasal congestion.3 Treatment should begin before exposure to theallergen and continue for the entire allergen season.22 If treatment begins after allergen exposure, reliefmay be delayed up to 4 weeks. Sodium cromoglycate is less effective than corticosteroids for allergicrhinitis and has not been adequately compared with leukotriene receptor antagonists andantihistamines.6,30
DecongestantsDecongestants are available in oral and topical formulations. Oral decongestants generally have aweaker effect on nasal obstruction than the topical formulations.22 When given orally, decongestantscan cause systemic adverse effects (see Table 5). Most available agents do not cause blood pressureelevations in normotensive persons unless the recommended dose is significantly exceeded.32Elevation of blood pressure may occur at standard doses in hypertensive patients.33
Systemic absorption from topical formulations is low, resulting in mainly local adverse effects (seeTable 6). Rhinitis medicamentosa (rebound vasodilation) can occur if topical decongestants are usedfor more than 3–5 days.34 In one study, 49% of patients reported using an intranasal decongestant dailyfor at least one year, even though 80% reported having received education about limiting the durationof use. Intranasal decongestant overuse was less common in patients who were using intranasalcorticosteroid or oral antihistamine.35 Overuse can lead to nasal congestion when the topical agent isstopped, and to permanent overgrowth of nasal tissue with chronic overuse. This condition is morelikely to occur with shorter-acting agents (phenylephrine) than with longer-acting agents(oxymetazoline and xylometazoline). Many solutions to this problem have been proposed, includingslow tapering of the decongestant, adding or switching to intranasal corticosteroids, or abruptdiscontinuation of the topical decongestant. Abrupt cessation is effective but may be uncomfortable forthe patient as nasal congestion may persist for several days or weeks.34
232 Respiratory Conditions

Compendium of Therapeutics for Minor Ailments Copyright © Canadian Pharmacists Association. All rights reserved.
CorticosteroidsIntranasal corticosteroids are more effective against the nasal symptoms of allergic rhinitis than oraland intranasal antihistamines, nasal cromoglycate and leukotriene receptor antagonists.29,30 Intranasalcorticosteroids are the drugs of choice for moderate to severe or persistent allergic rhinitis, and formild allergic rhinitis that does not respond to antihistamines.3,6,9 Some intranasal corticosteroids(mometasone furoate and fluticasone furoate) have a modest benefit on allergic conjunctivitissymptoms.6,10,36,37,38 A meta-analysis suggests that intranasal corticosteroids as a class are effective forocular symptoms of allergic rhinitis; however the magnitude of effect has not been quantified.39 Onsetof action of intranasal corticosteroids is within 6–8 hours of first dose, although maximum effect maytake a few weeks. Short courses of oral corticosteroids may be required for severe cases of allergicrhinitis that is unresponsive to other treatment.6 Patients may prefer intranasal corticosteroids inaerosol form compared with spray form; therefore, switching to another intranasal corticosteroidformulation may be recommended if patient tolerability is affecting therapy.40 Regular use ofintranasal steroids is more effective than intermittent use.14
Leukotriene Receptor Antagonists (LTRA)Montelukast is superior to placebo but less effective than intranasal corticosteroids for nasalsymptoms of allergic rhinitis.30 Montelukast is similar in efficacy to loratadine, but patient response ismore variable than with antihistamines.30 There may be additive effects when it is used concomitantlywith antihistamines. Montelukast is more effective than oral antihistamines and comparable tointranasal corticosteroids for reduction of asthma symptoms and use of rescue asthma medication.30 Asa result, montelukast may be a reasonable option for allergic rhinitis coexisting with asthma.6,7,9Otherwise, montelukast is not recommended as first-line therapy for allergic rhinitis.9
ImmunotherapyAccording to clinical practice guidelines, allergen immunotherapy should be considered for patientswho continue to have moderate to severe symptoms despite treatment or those who require systemiccorticosteroids.2,9 Immunotherapy may be indicated when the exposure to allergens is significant andunavoidable (e.g., grass pollen), and when the symptom complex is severe enough to warrant the time,expense and small risk of anaphylaxis.6 Allergen immunotherapy is the only treatment that can modifythe natural history of allergic rhinitis and potentially induce long-term disease remission after cessationof treatment. It may also prevent the development of new allergies and reduce the risk of developmentof asthma in children. Therefore, allergen immunotherapy may be considered even in milder cases ofallergic rhinitis. Immunotherapy is administered by subcutaneous injection, although sublingualimmunotherapy seems to be somewhat effective as well.6,41,42
AnticholinergicsIntranasal ipratropium bromide is effective for rhinorrhea secondary to allergic rhinitis but not forother symptoms.22
Combination TherapiesCombination therapy is recommended by some guidelines when patients have inadequate response tomonotherapy.9 Some combinations have been shown to be more effective than monotherapy whileothers have not.
First- and Second-generation AntihistaminesSome experts suggest a second-generation antihistamine during the day and a first-generationantihistamine at bedtime to promote sleep. Evidence to support this practice is lacking and next-day
Chapter 22: Allergic Rhinitis 233

Copyright © Canadian Pharmacists Association. All rights reserved. Compendium of Therapeutics for Minor Ailments
sedation is possible.2 If sleep is disturbed due to allergies, symptom relief itself can be expected toimprove sleep.
Antihistamine plus DecongestantBecause antihistamines may have only a modest effect on nasal congestion, antihistamines anddecongestants are often combined. Some patients may respond to this combination whencorticosteroids have failed or when either medication alone does not provide adequate relief of nasalsymptoms.2,30
Antihistamine plus CorticosteroidIntranasal corticosteroids are often combined with oral antihistamines to treat severe or resistant casesof allergic rhinitis.6 This strategy seems logical because the 2 drugs have different mechanisms ofaction. Evidence is insufficient to support the combination of intranasal corticosteroids and oralantihistamines, as it has not been consistently shown to be superior to either medication alone.2,30However, intranasal corticosteroid in combination with intranasal antihistamine (fluticasone/azelastine) is more effective for the nasal symptoms of allergic rhinitis than either medication alone.30
Antihistamine or Intranasal Corticosteroid plus LTRAAn additive effect has been shown when LTRAs and either oral antihistamines or intranasalcorticosteroids are used concomitantly.30 The efficacy of oral antihistamines in combination with aLTRA is less than that of intranasal corticosteroids alone.6 However, antihistamine-LTRA combinationtherapy may provide an alternative for patients who are unresponsive or nonadherent to intranasalcorticosteroid therapy.
Special PopulationsChildrenThe guidelines for treatment of allergic rhinitis in children are similar to those for adults.6 Healthcarepractitioners must ensure they select the correct dosage, ensure proper administration and minimizeadverse effects.3,7,24 Most second-generation antihistamines are now available in pediatricformulations for children >6 months and are generally preferred over first-generation agents due toimproved adverse effect profiles. Table 5 and Table 6 provide dosage guidelines and age limits for oraland intranasal agents. Intranasal corticosteroids are also effective and are considered safe in children>2 years of age, depending on the formulation.24 Intranasal budesonide and mometasone furoatehave not shown growth suppression with prolonged use at recommended doses.6,43,44 Intranasalbeclomethasone dipropionate, fluticasone propionate and triamcinolone acetonide have beenshown to reduce growth velocity by 0.2–0.9 cm per year within the first year of treatment.45,46,47Longer term studies have not been conducted. If intranasal corticosteroids are used, use the lowestpossible dose, monitor growth and use other therapies (e.g., antihistamines) to minimize the dose ofcorticosteroid required for symptom control.6 Decongestants are not recommended for use in childrenunder 6 years.48,49 In those children, intranasal saline drops or spray may be used to clear nasalpassages before eating or sleeping.
PregnancyIntranasal cromoglycate and intranasal corticosteroids are both considered safe during pregnancyalthough beclomethasone, budesonide and fluticasone propionate have accumulated more safetydata than other intranasal corticosteroids.6 Neither first- nor second-generation antihistamines havebeen associated with teratogenic effects in pregnancy.50,51 First-generation antihistamines werepreviously favoured because of substantially greater experience; however, safety data for cetirizineand loratadine now indicate these are acceptable options. Chlorpheniramine has a good safety
234 Respiratory Conditions

Compendium of Therapeutics for Minor Ailments Copyright © Canadian Pharmacists Association. All rights reserved.
record in pregnancy. Although diphenhydramine has good safety data and is still recommended andfrequently used in pregnancy, there have been isolated reports of cleft palate.51 Sedation and impairedperformance may limit the use of first-generation antihistamines. Oral decongestants should beavoided in the first trimester.51 A topical decongestant may be used; at usual doses, they do notpresent a risk to the fetus. Immunotherapy generally should not be started during pregnancy. Coursesof immunotherapy started prior to conception may be continued if beneficial and not causing systemicreactions; doses should not be increased during pregnancy.52 See Appendix V: Pregnancy andBreastfeeding: Self-care Therapy for Common Conditions.
BreastfeedingRecommendations for breastfeeding are similar to those during pregnancy. Both first- and second-generation antihistamines are considered safe while breastfeeding.53 First-generation antihistaminesmay in theory diminish milk production via their anticholinergic effect; however, this has not beenreported in practice. Infant somnolence should be monitored when a first-generation antihistamine orcetirizine is used.
The systemic absorption of topical decongestants is low and transfer into breast milk is unknown.Consequently, these agents are expected to be reasonably safe during breastfeeding.
The American Academy of Pediatrics considers pseudoephedrine to be compatible withbreastfeeding.51 Information on the use of other oral decongestants during breastfeeding is limited.
Information on the use of topical sodium cromoglycate during breastfeeding is not available, althoughthe manufacturer recommends caution.
Monitoring of TherapyTable 4 provides a monitoring plan framework that should be individualized.
Table 4: Monitoring of Therapy for Allergic Rhinitis
Symptoms Monitoring Endpoint of Therapy Actions
Allergic symptoms(sneezing, runny nose,itchy and watery eyes,congestion, rhinorrhea)
Patients: DailyHealthcare practitioner:Next visit or by telephone 1wk later
Patient able to performdaily activities.Patient able to sleep.
If nonprescription therapy is ineffectiveafter 1 wk, optimize allergen avoidanceand medication dose (if applicable). Ifsymptoms not controlled after a furtherwk of therapy, consider another agent.Refer as necessary.3
Drowsiness(antihistamine)
Patient: DailyHealthcare practitioner:Next visit or by telephonewhen checking for efficacy
Patient not drowsy duringthe day.
Switch to a less sedating antihistamine.If using cetirizine, could give dose atbedtime.
Insomnia(oral decongestant)
Patient: DailyHealthcare practitioner: 1wk
No insomnia. Change medication schedule so lastdose taken 4–6 h before bedtime ordiscontinue medication.
Elevated blood pressurein hypertensive patients(oral decongestant)
Patient: DailyHealthcare practitioner:Monitor blood pressure ofhypertensive patients twicein the first wk
No elevation in bloodpressure above baseline.
Stop decongestant if blood pressureelevated above baseline.
Chapter 22: Allergic Rhinitis 235

Copyright © Canadian Pharmacists Association. All rights reserved. Compendium of Therapeutics for Minor Ailments
Advice for the PatientAdvise all patients about allergen avoidance. In addition, patients who require drug therapy shouldreceive counselling regarding proper use of the medication, expected results and management ofadverse effects (see Table 4).
Figure 2: Assessment and Initial Treatment of Patients with Allergic Rhinitis3,4,6,7
236 Respiratory Conditions

Compendium
ofTherapeuticsforMinorAilm
entsCopyright©
Canadian
PharmacistsAssociation.Allrightsreserved.
Table 5: Oral Agents for Allergic RhinitisClass Drug Dosage Adverse Effects Drug Interactions Comments Costa
Antihistamines,First-generation
chlorpheniramineChlor-Tripolon,generics
Adults: 4 mg Q4–6H po;maximum 24 mg/dayChildren: 0.35 mg/kg/daydivided Q4–6H poor2–5 y: 1 mg Q4–6H po;maximum 6 mg/day6–11 y: 2 mg Q4–6H po;maximum 12 mg/day
CNS: Sedation, fatigue,dizziness, impairmentof cognition andperformance.Anticholinergic: Drymouth and eyes,constipation, urinaryretention.
Increased CNS depressionwhen combined: Alcohol,sedatives, tranquilizers,barbiturates.Increased anticholinergicside effects when combinedwith: TCAs, scopolamine.Increase chlorpheniraminelevels resulting in increasedadverse effects whencombined with moderateCYP2D6 inhibitors, e.g.,amiodarone, celecoxib.Avoid combination withstrong CYP2D6 inhibitors,e.g., bupropion, paroxetine.
$
diphenhydramineBenadrylPreparations,generics
Adults: 25–50 mg Q6–8Hpo; maximum 300 mg/dayChildren: 5 mg/kg/day givenin 3 or 4 divided doses po2–5 y: Maximum 37.5 mg/day6–11 y: Maximum150 mg/day
See chlorpheniramine. Increased CNS depression:Alcohol, sedatives,tranquilizers, barbiturates.Increased anticholinergicside effects when combinedwith: TCAs, scopolamine.May increase levels ofCYP2D6 substrates, e.g.,metoprolol, venlafaxine.
Available in pediatric liquidformulation.
$
Antihistamines,Second-generation
cetirizineReactine, generics
Adults: 5–10 mg Q24H po;maximum 20 mg Q24H poChildren:6–12 months: 2.5 mg Q24Hpo12–23 months: 2.5 mg Q24Hpo; maximum 2.5 mg Q12H2–5 y: 2.5 mg Q24H po;maximum 5 mg/day in 1 or 2doses≥6 y: Adult dosage
Minimal to noanticholinergic effects.May cause drowsinessin some individualsespecially at higherdoses.Headache.
Increased CNS depression:Alcohol, sedatives,tranquilizers, barbiturates.Increased anticholinergicside effects: TCAs,scopolamine.
Active metabolite ofhydroxyzine.Available in pediatric 5 mgrapid-dissolve tablet.Available as 5 mg/5 mLsyrup.
$ Chapter22:A
llergicRhinitis
237

Copyright©
Canadian
PharmacistsAssociation.Allrightsreserved.
Compendium
ofTherapeuticsforMinorAilm
ents
Class Drug Dosage Adverse Effects Drug Interactions Comments Costa
desloratadineAerius, generics
Adults: 5 mg Q24H poChildren:6–11 months: 1 mg Q24H po1–5 y: 1.25 mg Q24H po6–11 y: 2.5 mg Q24H po
Minimal to noanticholinergic effects.Headache.
P-gp inhibitors (e.g.,erythromycin, ketoconazole)may increase loratadinelevels while P-gp inducers(e.g., carbamazepine,dexamethasone) maydecrease loratadine levels;clinical effect probablyminimal.
Active metabolite ofloratadine.Available in pediatric liquidformulation.
$
fexofenadineAllegra
Adults: 60 mg Q12H poSustained-release: 120 mgQ24H poChildren:2–11 y: 30 mg Q12H po
See desloratadine. Decreased fexofenadinelevel: Aluminum- andmagnesium-containingantacids.Ingestion of fruit juices suchas apple, grapefruit ororange may decreasebioavailability.
Active metabolite ofterfenadine. Only 5% of adose is metabolized.
$
loratadineClaritin, ClaritinLiquid Capsules,generics
Adults: 10 mg Q24H poChildren:2–5 y: 5 mg Q24H po≥5 y: 10 mg Q24H po
See desloratadine. QTc prolongation reportedwith concomitant use ofloratadine and amiodarone.Caution is advised.P-gp inhibitors (e.g.,erythromycin, ketoconazole)may increase loratadinelevels while P-gp inducers(e.g., carbamazepine,dexamethasone) maydecrease loratadine levels;clinical effect probablyminimal.
Available in pediatric liquidformulation and rapid-dissolve tablets.
$
(cont'd)
Table 5: Oral Agents for Allergic Rhinitis (cont'd) 238Respiratory
Conditions

Compendium
ofTherapeuticsforMinorAilm
entsCopyright©
Canadian
PharmacistsAssociation.Allrightsreserved.
Class Drug Dosage Adverse Effects Drug Interactions Comments Costa
Decongestants pseudoephedrine
Eltor 120,Sudafed, generics
Adults: 60 mg Q4–6H po;maximum 240 mg/daySustained-release: 120 mgQ12H po; maximum 240 mg/dayChildren:6–11 y: 30 mg Q4–6H poMaximum 120 mg/day≥12 y: adult dose
Mild CNS stimulation(nervousness,excitability,restlessness, dizziness,weakness, insomnia).Peripheralvasoconstriction.Tachycardia orpalpitation may occur.Blood pressure may beincreased inhypertensive subjects.May adversely affectblood sugar control indiabetics.
Beta-blockers:Antihypertensive effects maybe reduced.Contraindicated with MAOIsand ergot derivatives.Avoid use withphenothiazines and selectiveserotonin reuptake inhibitors.
Caution in patients withheart disease, high bloodpressure, hyperthyroidism,diabetes, angle closureglaucoma and prostaticenlargement.Concurrent use with or usewithin 2 weeks of MAOIsmay cause hypertensivecrisis.
$$
Antihistamine,Second-generation/DecongestantCombinations
cetirizine/pseudoephedrine
ReactineComplete
Adults: 1 tab (5 mg/120 mg)Q12H poChildren:≥12 y: Give adult dose
See cetirizine.See pseudoephedrine.
See cetirizine.See pseudoephedrine.
See cetirizine.See pseudoephedrine.
$$
desloratadine/pseudoephedrine
Aerius Dual Action12 Hour
Adults: 1 tab (2.5mg/120 mg) Q12H poChildren:≥12 y: Give adult dose
See desloratadine.See pseudoephedrine.
See desloratadine.See pseudoephedrine.
See desloratadine.See pseudoephedrine.
$$
fexofenadine/pseudoephedrine
Allegra-D
Adults: 1 tab (60 mg/120 mg) Q12H poChildren:≥12 y: Give adult dose
See desloratadine.See pseudoephedrine.
See fexofenadine.See pseudoephedrine.
See fexofenadine.See pseudoephedrine.
$$
loratadine/pseudoephedrine
Claritin Allergy +Sinus, ClaritinAllergy + SinusExtra Strength
Adults: 1 tab (5 mg/120 mg)Q12H poor1 tab (10 mg/240 mg) Q24HpoChildren:≥12 y: Give adult dose
See desloratadine.See pseudoephedrine.
See loratadine.See pseudoephedrine.
See loratadine.See pseudoephedrine.
$$
(cont'd)
Chapter22:A
llergicRhinitis
239

Copyright©
Canadian
PharmacistsAssociation.Allrightsreserved.
Compendium
ofTherapeuticsforMinorAilm
ents
Class Drug Dosage Adverse Effects Drug Interactions Comments Costa
LeukotrieneReceptorAntagonists
montelukastSingulair,Montelukast, othergenerics
Adults and children ≥15 y:10 mg QHSChildren:6–14 y: 5 mg QHS2–5 y: 4 mg QHS
Headache, abdominalpain, flu-like symptoms.
Strong CYP2C9 and 3A4inducers (e.g.,carbamazepine,phenobarbital, phenytoin,rifampin) may decreasemontelukast levels whereas,strong CYP2C9 inhibitors(e.g., sulfadiazine) mayincrease montelukast levels;clinical significance isuncertain; however, monitorfor reduced efficacy oradverse effects.
Strong CYP2C9 and 3A4inducers (e.g.,carbamazepine,phenobarbital, phenytoin,rifampin) may decreasemontelukast levelswhereas, strong CYP2C9inhibitors (e.g., fluconazole)may increase montelukastlevels; clinical significanceis uncertain; however,monitor for reducedefficacy or adverse effects
$$
a Cost of 10 day supply; includes drug cost only
Dosage adjustment may be required in renal impairment.Abbreviations: CNS = central nervous system; MAOI = monoamine oxidase inhibitor; SR = sustained releaseLegend: $ < $10 $$ $10–20
Table 5: Oral Agents for Allergic Rhinitis (cont'd) 240Respiratory
Conditions

Compendium
ofTherapeuticsforMinorAilm
entsCopyright©
Canadian
PharmacistsAssociation.Allrightsreserved.
Table 6: Intranasal Agents for Allergic RhinitisClass Drug Dosage Adverse Effects Comments Costa
Antihistamines levocabastineLivostin Nasal Spray
Adults and Children (≥12–65 y): 2sprays (50 µg/spray) per nostril BID;may increase to 2 sprays TID–QID
Nasal irritation. Shake well before use.Initial priming required.Discontinue if no improvement seenwithin 3 days.
$$$
Antihistamine/CorticosteroidCombinations
azelastine/fluticasoneDymista
Adults and children ≥12 y: 1 spray(137 µg/50 µg) in each nostril BID
Burning or stinging,nosebleeds.Dysgeusia may occur ifpatient tilts head back toofar during administration.
Avoid use with ritonavir due topotential for systemic corticosteroideffects.Rarely causes drowsiness.
$100
Corticosteroids beclomethasonegenerics
Adults and children ≥6 y: 2 sprays(50 µg/spray) in each nostril BIDAdults: Maximum 12 sprays/dayChildren: Maximum 8 sprays/dayUse lowest effective dose formaintenance therapy
Burning or stinging,nosebleed.May cause mild growthsuppression with prolongeduse.45,46,47
Use at regular intervals. Slow onset(7–14 days for maximal effect).Drug may fail to reach the site ofaction if excessive nasal mucussecretion or edema of the nasalmucosa is present. May use avasoconstrictor (intranasaldecongestant) 2–3 days prior to thesuspension.Aim spray up towards turbinates andaway from septum. Liquid forms maybe more effective than metered-doseinhalers.
$$
budesonideRhinocort Aqua,Rhinocort Turbuhaler
Nasal suspension:Adults and children ≥6 y (64 µg/metered dose): Initial dose 2 spraysin each nostril dailyor1 spray in each nostril BID; maydecrease maintenance dose to 1spray in each nostril dailyNasal powder:Adults and children ≥6 y ( 100 µg/dose):Initial dose 2 applications in eachnostril in the morningor1 application in each nostril BID; maydecrease maintenance dose to 1spray in each nostril dailyMaximum 400 µg/day
See beclomethasone. See beclomethasone.For the nasal suspension, initialpriming needed. Re-prime if not used≥4 days.
$$-$$$
Chapter22:A
llergicRhinitis
241

Copyright©
Canadian
PharmacistsAssociation.Allrightsreserved.
Compendium
ofTherapeuticsforMinorAilm
ents
Class Drug Dosage Adverse Effects Comments Costa
ciclesonideOmnaris
Adults and children ≥12 y: 2 sprays(50 µg/spray) in each nostril daily;maximum 200 µg/day
Burning or stinging,nosebleeds.
See beclomethasone.Initial priming needed.
$$$
flunisolidegenerics
Adults: 2 sprays (25 µg/meteredspray) in each nostril BID, mayincrease to TID if needed; maximum300 µg/dayChildren 6–14 y: 1 spray in eachnostril TID; maximum 150 µg/day
See ciclesonide. See beclomethasone. $$
fluticasone propionateFlonase, generics
Adults and children ≥12 y: 2 sprays(50 µg/spray) in each nostril daily,may increase to BID in severesituations; maximum 400 µg/dayChildren 4–11 y: 1–2 sprays in eachnostril daily; maximum 200 µg/day
See beclomethasone. See beclomethasone. $$$
fluticasone furoateAvamys
Adults and children ≥12 y: 2 sprays(27.5 µg/spray) in each nostril oncedaily; maximum 110 µg/dayChildren ≥2 y to <12 y: 1 spray ineach nostril once daily, may increaseto 2 sprays in each nostril once dailyif needed. Decrease to 1 spray ineach nostril daily for maintenance;maximum 110 µg/day
See ciclesonide. See beclomethasone.Initial priming needed. Re-prime if notused ≥30 days or if cap let off for ≥5days.
$$$
mometasoneNasonex
Adults and children ≥12 y: 2 sprays(50 μg/spray) in each nostril daily,may decrease to 1 spray in eachnostril daily for maintenance; mayincrease to BID in severe situations.Children 3–11 y: 1 spray in eachnostril daily
See ciclesonide. See beclomethasone. $$$
Table 6: Intranasal Agents for Allergic Rhinitis (cont'd) 242Respiratory
Conditions

Compendium
ofTherapeuticsforMinorAilm
entsCopyright©
Canadian
PharmacistsAssociation.Allrightsreserved.
Class Drug Dosage Adverse Effects Comments Costa
triamcinoloneNasacort AQ
Adults and children ≥12 y: 2 sprays(55 µg/spray) in each nostril oncedaily, may decrease to 1 spray ineach nostril once dailyChildren 4–11 y: 1 spray (55 µg/spray) in each nostril once daily, mayincrease to 2 sprays in each nostrilonce daily if needed. Decrease to 1spray in each nostril daily formaintenance; maximum 110 µg/day
See ciclesonide. See beclomethasone. $$$
Decongestants oxymetazolineClaritin AllergyDecongestant, DristanLong Lasting NasalMist, Dristan LongLasting MentholatedNasal Spray
Adults and children ≥6 y: 0.05%solution 2–3 drops or sprays/nostrilQ12H
Burning, stinging, sneezing,dryness of the nasalmucosa.Bradycardia, tachycardia,hypotension andhypertension have beenreported.
Onset of action: 5–10 min.Long duration of action lasting up to12 h.Do not use longer than 3–5 days.
$
phenylephrineDristan Nasal Mist
Adults and children ≥6 y: 0.25% or0.5% solution 2–3 drops or sprays/nostril Q4H
See oxymetazoline. See oxymetazoline. $
xylometazolineOtrivin, Balminil NasalDecongestant
Adults and children ≥6 y: 0.05% or0.1% solution 2–3 drops or 1–2sprays/nostril Q8-10H
See oxymetazoline. See oxymetazoline. $
Mast CellStabilizers
sodium cromoglycateRhinaris CS Anti-allergic
Adults and children >2 y: 1 spray/nostril 3–6 times daily
Local: Sneezing, nasalstinging or irritation, badtaste in the mouth,epistaxis.
Less effective than other agents.Onset of action delayed up to 4 wk.
$$
a Cost of 1 unit (spray pump); includes drug cost only.Legend: $ < $10 $$ $10–20 $$-$$$ $10–30 $$$ $20–30
Chapter22:A
llergicRhinitis
243

Copyright © Canadian Pharmacists Association. All rights reserved. Compendium of Therapeutics for Minor Ailments
Suggested Readings
Brozek JL, Bousquet J, Baena-Cagnani CE et al. Allergic Rhinitis and its Impact on Asthma (ARIA)guidelines: 2010 revision. J Allergy Clin Immunol 2010;126:466-76.
Seidman MD, Gurgel RK, Lin SYet al. Clinical practice guideline: Allergic rhinitis. Otolaryngol HeadNeck Surg 2015;152:S1-43.
Wallace DV, Dykewicz MS, Bernstein DI et al. The diagnosis and management of rhinitis: an updatedpractice parameter. J Allergy Clin Immunol 2008;122:S1-84.
Wheatley LM, Togias A. Clinical practice. Allergic rhinitis. N Engl J Med 2015;372:456-63.
References1. Mucci T, Govindaraj S, Tversky J. Allergic rhinitis.Mt Sinai J Med 2011;78:634-44.2. Plaut M, Valentine MD. Clinical practice. Allergic rhinitis. N Engl J Med 2005;353:1934-44.3. Brozek JL, Bousquet J, Baena-Cagnani CE et al. Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines: 2010 revision. J Allergy ClinImmunol 2010;126:466-76.
4. Greiner A, Hellings PW, Rotiroti G et al. Allergic rhinitis. Lancet 2011;378:2112-22.5. Kay AB. Allergy and allergic diseases. First of two parts. N Engl J Med 2001;344:30-7.6. Wallace DV, Dykewicz MS, Bernstein DI et al. The diagnosis and management of rhinitis: an updated practice parameter.J Allergy Clin Immunol 2008;122:S1-84.
7. Scadding GK, Durham SR, Mirakian R et al. BSACI guidelines for the management of allergic and non-allergic rhinitis. Clin Exp Allergy2008;38:19-42.
8. Varghese M, Glaum MC, Lockey RF. Drug-induced rhinitis. Clin Exp Allergy 2010;40:381-4.9. Seidman MD, Gurgel RK, Lin SY et al. Clinical practice guideline: Allergic rhinitis. Otolaryngol Head Neck Surg 2015;152:S1-43.10. Nurmatov U, van Schayck CP, Hurwitz B et al. House dust mite avoidance measures for perennial allergic rhinitis: an updated Cochrane
systematic review. Allergy 2012;67:158-65.11. Hermelingmeier KE, Weber RK, Hellmich M et al. Nasal irrigation as an adjunctive treatment in allergic rhinitis: a systematic review and
meta-analysis. Am J Rhinol Allergy 2012;26:e119-25.12. Garavello W, Somigliana E, Acaia B et al. Nasal lavage in pregnant women with seasonal allergic rhinitis: a randomized study. Int Arch
Allergy Immunol 2010;151:137-41.13. Wilson AM, O'Byrne PM, Parameswaran K. Leukotriene receptor antagonists for allergic rhinitis: a systematic review and meta-analysis. Am
J Med 2004;116:338-44.14. Laekeman G, Simoens S, Buffels J et al. Continuous versus on-demand pharmacotherapy of allergic rhinitis: evidence and practice. Respir
Med 2010;104:615-25.15. Krouse JH. Allergic rhinitis–current pharmacotherapy. Otolaryngol Clin North Am 2008;41:347-58.16. Bachert C. A review of the efficacy of desloratadine, fexofenadine, and levocetirizine in the treatment of nasal congestion in patients with
allergic rhinitis. Clin Ther 2009;31:921-44.17. Lehman JM, Blaiss MS. Selecting the optimal oral antihistamine for patients with allergic rhinitis. Drugs 2006;66:2309-19.18. Simons FE. Advances in H1-antihistamines N Engl J Med 2004;351:2203-17.19. Slater JW, Zechnich AD, Haxby DG. Second-generation antihistamines: a comparative review. Drugs 1999;57:31-47.20. Horak F, Stubner UP. Comparative tolerability of second generation antihistamines. Drug Saf 1999;20:385-401.21. Simons FE. H1-receptor antagonists. Comparative tolerability and safety. Drug Saf 1994;10:350-80.22. Melvin TA, Patel AA. Pharmacotherapy for allergic rhinitis. Otolaryngol Clin North Am 2011;44:727-39.23. Sur DK, Scandale S. Treatment of allergic rhinitis. Am Fam Physician 2010;81:1440-6.24. Turner PJ, Kemp AS. Allergic rhinitis in children. J Paediatr Child Health 2012;48:302-10.25. Bender BG, Berning S, Dudden R et al. Sedation and performance impairment of diphenhydramine and second-generation antihistamines: a
meta-analysis. J Allergy Clin Immunol 2003;111:770-6.26. Weiler JM, Bloomfield JR, Woodworth GG et al. Effects of fexofenadine, diphenhydramine and alcohol on driving performance. A
randomized, placebo-controlled trial in the Iowa driving simulator. Ann Intern Med 2000;132:354-63.27. Church MK, Maurer M, Simons FE et al. Risk of first-generation H(1)-antihistamines: a GA(2)LEN position paper. Allergy 2010;65:459-66.28. Walsh GM, Annunziato L, Frossard N et al. New insights into the second generation antihistamines. Drugs 2001;61:207-36.29. Weiner JM, Abramson MJ, Puy RM. Intranasal corticosteroids versus oral H1 receptor antagonists in allergic rhinitis: systematic review of
randomised controlled trials. BMJ 1998;317:1624-9.30. Glacy J, Putnam K, Godfrey S et al. Treatments for seasonal allergic rhinitis. Rockville: Agency for Healthcare Research and Quality; 2013.
(Comparative Effectiveness Reviews, No. 120.) Available from: www.ncbi.nlm.nih.gov/books/NBK153714.31. Golightly LK, Greos LS. Second-generation antihistamines: actions and efficacy in the management of allergic disorders. Drugs 2005;65:341-
84.32. Johnson DA, Hricik JG. The pharmacology of alpha-adrenergic decongestants. Pharmacotherapy 1993;13:110S-15S.33. Chua SS, Benrimoj SI, Gordon RD et al. A controlled clinical trial on the cardiovascular effects of single doses of pseudoephedrine in
hypertensive patients. Br J Clin Pharmacol 1989;28:369-72.34. Graf P. Rhinitis medicamentosa: aspects of pathophysiology and treatment. Allergy 1997;52:28-34.35. Mehuys E, Gevaert P, Brusselle G et al. Self-medication in persistent rhinitis: overuse of decongestants in half of the patients. J Allergy Clin
Immunol Pract 2014;2:313-9.36. Ratner P, Van Bavel JV, Mohar D et al. Efficacy of daily intranasal fluticasone propionate on ocular symptoms associated with seasonal
allergic rhinitis. Ann Allergy Asthma Immunol 2015;114:141-7.37. van Drunen C, Meltzer EO, Bachert C et al. Nasal allergies and beyond: a clinical review of the pharmacology, efficacy, and safety of
mometasone furoate. Allergy 2005;60:5-19.
244 Respiratory Conditions

Compendium of Therapeutics for Minor Ailments Copyright © Canadian Pharmacists Association. All rights reserved.
38. Kaiser HB, Naclerio RM, Given J et al. Fluticasone furoate nasal spray: a single treatment option for the symptoms of seasonal allergicrhinitis. J Allergy Clin Immunol 2007;119:1430-7.
39. Hong J, Bielory B, Rosenberg JL. Efficacy of intranasal corticosteroids for the ocular symptoms of allergic rhinitis: a systematic review.Allergy Asthma Proc 2011;32:22-35.
40. Berger WE, Prenner B, Turner R et al. A patient preference and satisfaction study of ciclesonide nasal aerosol and mometasone furoateaqueous nasal spray in patients with perennial allergic rhinitis. Allergy Asthma Proc 2013;34:542-50.
41. Kowalski ML. Systemic and specific treatment for a global disease: allergen immunotherapy revisited. Allergy 2006;61:791-5.42. Jacobsen L, Niggemann B, Dreborg S et al. Specific immunotherapy has long term preventive effect of seasonal and perennial asthma: 10-year
follow-up on the PAT study. Allergy 2007;62:943-8.43. Allen DB. Systemic effects of intranasal steroids: an endocrinologist's perspective. J Allergy Clin Immunol 2000;106:S179-90.44. Skoner DP, Gentile DA, Doyle WJ. Effect on growth of long-term treatment with intranasal triamcinolone acetonide aqueous in children with
allergic rhinitis. Ann Allergy Asthma Immunol 2008;101:431-6.45. Skoner DP, Rachelefsky GS, Meltzer EO et al. Detection of growth suppression in children during treatment with intranasal beclomethasone
dipropionate. Pediatrics 2000;105:E23.46. Lee LA, Sterling R, Maspero J et al. Growth velocity reduced with once-daily fluticasone furoate nasal spray in prepubescent children with
perennial allergic rhinitits. J Allergy Clin Immunol Pract 2014;2:421-7.47. Skoner DP, Berger WE, Gawchik SM et al. Intranasal triamcinolone and growth velocity. Pediatrics 2015;135:e348-56.48. Healthy Canadians. Health Canada releases decision on the labelling of cough and cold products for children. Available from:
www.healthycanadians.gc.ca/recall-alert-rappel-avis/hc-sc/2008/13267a-eng.php. Accessed November 30, 2009.49. Peterson RG, Cran B, Knoppert D et al. Scientific Advisory Panel on Nonprescription Paediatric Cough and Cold Medications (SAP-
NPCCM). Record of proceedings. Ottawa: Health Canada; March 20, 2008.50. Mazzotta P, Loebstein R, Koren G. Treating allergic rhinitis in pregnancy. Safety considerations. Drug Saf 1999;20:361-75.51. Briggs GG, Freeman RK. Drugs in pregnancy and lactation: a reference guide to fetal and neonatal risk. 10th ed. Baltimore: Lippincott
Williams & Wilkins; 2015.52. Oykhman P, Kim HL, Ellis AK. Allergen immunotherapy in pregnancy. Allergy Asthma Clin Immunol 2015;11:31.53. Hale TW. Medications and mothers' milk: a manual of lactational pharmacology. 15th ed. Amarillo: Hale Publishing; 2012.
Chapter 22: Allergic Rhinitis 245

Copyright © Canadian Pharmacists Association. All rights reserved. Compendium of Therapeutics for Minor Ailments
Allergic Rhinitis—What You Need to Know
Allergic rhinitis is a condition caused by allergens in the air. Allergens are things that cause allergies.Some of the symptoms of allergic rhinitis are sneezing, coughing, runny nose, and itchy or wateryeyes. The most important thing you can do to feel better is to avoid the things that cause your allergies.Also avoid exposure to cigarette smoke and strong smells. If you do not know what causes yourallergies, see your doctor.
Helpful Hints for People Who Have AllergiesIf you are allergic to pollen:■ Keep the windows and doors of your house closed.■ If you need to use air conditioning, set the unit to the indoor cycle.■ Do not use window or attic fans.■ Check the weather report to find out about the pollen count. The pollen count tells you what kind of
pollen is in the air and how much. Avoid spending time outdoors when the pollen count is high. Thepollen count is highest on sunny, windy days and in the morning.
■ Do not dry your clothing outdoors.■ Shower or take a bath and wash your hair after outdoor activity. This will remove pollen from your
hair and skin. You want to avoid getting pollen into your bedding.
If you are allergic to outdoor moulds:■ Stay indoors as much as possible.■ If you need to use air conditioning, set the unit to the indoor cycle. Have your air conditioner
cleaned regularly. Air conditioners can be heavily contaminated with mould.■ Use a facemask if you rake leaves or work with compost or dry soil.
If you are allergic to indoor moulds:■ Kill mould with a solution of equal parts household bleach and water. Wash sinks, shower stalls,
nonrefrigerated vegetable storage areas and garbage pails with this solution.■ Avoid using a humidifier or cool mist vaporizer. Moulds grow easily where it is damp. If you must
use a humidifier or vaporizer, clean it often with a solution of equal parts bleach and water.■ If your home is built over a crawl space, install a plastic vapor barrier over exposed soil and keep
the foundation vents open.■ If your basement is damp or tends to flood, do not put carpet or furniture there. For a damp
basement, run a dehumidifier at all times. Empty water from the machine often and clean itregularly. For a flooded basement, drain the water as quickly as possible.
■ Fix any leaky faucets or pipes promptly.■ Do not keep houseplants.
If you are allergic to dust mites:■ Do not put carpet in your bedroom or main living areas.■ Plastic, leather or wood furniture is best.■ If possible, have someone else clean the house while you are not at home.■ If you must do your own cleaning, wear a facemask while you clean and for 10–15 minutes
afterward.
246 Respiratory Conditions

Compendium of Therapeutics for Minor Ailments Copyright © Canadian Pharmacists Association. All rights reserved.
■ Use a vacuum cleaner with an efficient double-filtration system.■ Keep indoor humidity between 40% and 45%. You can buy a hygrometer to measure the humidity
in your house at a hardware store or home centre.■ Avoid using a humidifier or cool mist vaporizer.■ Use zippered, allergen-proof casings on all mattresses, box springs and pillows.■ Consider replacing old mattresses.■ Wash your bedding in hot (>55°C) water at least every 2 weeks. Cooler water will not kill dust
mites.■ Do not keep stuffed toys that cannot be washed.■ Do not store items under your bed.■ Use window shades instead of venetian blinds.
If you are allergic to a pet:■ The best choice is to find another home for the animal. It can take several months before the
allergen levels return to normal.■ If you are not able to give up your pet, then:
– You may find it helps to install a HEPA or electrostatic air purifier in your home.– Keep animals out of your bedroom at all times.– Keep animals out of rooms that have carpets.– Try to keep animals off furniture.– Washing cats weekly and dogs twice weekly may help, though this has not been proven.– Get rid of litter boxes if possible. If not, put them in an area that is not connected to the air
supply for the rest of your home.– If the animal lives in a cage, keep it in a room without carpet, far away from your bedroom.
Medication to Help with Allergy SymptomsYou may want to try medication if:■ You don't feel better even when you avoid the things that cause your allergies.■ Your allergies are interfering with your sleep or your daily activities.
Your pharmacist can help you pick the best medication for you and show you how to use it. SeeTable 1. You can choose between pills or a nasal spray.
Table 1: How to Use a Nasal Spray or Drops
Nasal Spray (Adults only)
1. Gently blow your nose.2. Gently shake bottle and remove cap or lid.3. With your head upright but not tilted backward, press your finger against one side of your nose to close the nostril. Spray the
medication into the open nostril, with the tip directed away from the middle of the nose and back towards the nasal cavity.Squeeze the bottle quickly and breathe in slowly through the nose.
4. Remove tip of nasal spray from your nostril and breathe out through your mouth.5. Do the same thing on the other side.6. Blow your nose in 3–5 minutes.
(cont'd)
Chapter 22: Allergic Rhinitis 247

Copyright © Canadian Pharmacists Association. All rights reserved. Compendium of Therapeutics for Minor Ailments
Table 1: How to Use a Nasal Spray or Drops (cont'd)
7. Rinse the tip of the spray bottle with hot water, but try not to get water in the bottle. Replace lid.8. Do not use more nose spray than the recommended amount.
Nose Drops (Adult or child)
1. Gently blow your nose.2. Lie on your back on a bed with your head hanging slightly over the side.3. Gently shake bottle. Fill the dropper with the recommended amount of medication. Put the dropper just inside one nostril
(about 0.8 cm or one-third inch). If possible, don't let the dropper touch the skin.4. Apply the recommended number of drops. Apply the medication to the other nostril in the same way.5. Stay in the same position for about 5 minutes. Tilt head from side to side.6. Blow the nose 3–5 minutes later.7. You can also take nose drops by tilting your head back (instead of lying down). Use the recommended number of drops for
each nostril. Then bend over at the waist and hold that position for a few seconds before coming up straight again.8. Rinse the dropper with hot water and return it to the bottle.9. Do not use nose drops more than is recommended on the package.
248 Respiratory Conditions




![Diagnosis and Management of Rhinitis: Complete Guidelines ... · different forms of rhinitis (allergic, non-allergic, occupational rhinitis, hormonal rhinitis [pregnancy and hypothyroidism],](https://static.fdocuments.net/doc/165x107/5d61f07588c993197b8b51b8/diagnosis-and-management-of-rhinitis-complete-guidelines-different-forms.jpg)