
CHAPTER 20 HEART FAILURE AND CIRCULATORY SHOCK Essentials of Pathophysiology.
49
CHAPTER 20 HEART FAILURE AND CIRCULATORY SHOCK Essentials of Pathophysiology
-
Upload
greyson-simon -
Category
Documents
-
view
237 -
download
6
Transcript of CHAPTER 20 HEART FAILURE AND CIRCULATORY SHOCK Essentials of Pathophysiology.
CHAPTER 20
HEART FAILURE AND CIRCULATORY SHOCK
CHAPTER 20
HEART FAILURE AND CIRCULATORY SHOCK
Essentials of Pathophysiology

PRE LECTURE QUIZTrue/False Decreased cardiac output will lead to an increase in
renal blood flow and glomerular filtration rate. The endothelins are potent vasodilators that are
released from the endothelial cells throughout the circulation.
Myocardial hypertrophy is a long-term mechanism by which the heart compensates for increased workload.
Afterload represents the force that the contracting heart must generate to eject blood from the filled heart.
Five major complications of severe shock are acute respiratory distress syndrome, acute renal failure, gastrointestinal ulceration, disseminated intravascular coagulation, and multiple organ dysfunction syndrome.
F
F
T
T
T
PRE LECTURE QUIZ In __________ heart failure, blood backs up in the
systemic circulation, causing peripheral edema and congestion of the abdominal organs.
The most common cause of ____________ shock is myocardial infarction.
Examples of conditions that cause __________ shock include loss of whole blood (e.g., hemorrhage), plasma loss (e.g., severe burns), or extracellular fluid (e.g., gastrointestinal fluids lost in vomiting or diarrhea).
An increase in __________ rate is an early sign of shock.
A life-threatening condition, acute __________ edema is the most dramatic symptom of left heart failure and is characterized by capillary fluid moving into the alveoli.
cardiogenic
heart
hypovolemic
pulmonary
right

STANDARD ECG WAVEFORM
Atrial Contraction initiated
Ventricular Contraction initiated Ventricular
RelaxationPapillary Muscle
Relaxation
ST segment can indicate ischemia or infarction

ST SEGMENT ELEVATION
ST Depression
With a 12 lead ECG certain leads can be connected to each other to reverse the R wave and accentuate the ST Elevation

CORORNARY OCCLUSION
total occlusion of the proximal segment of left
anterior descending artery, and
severe disease involving the proximal segment of
the obtuse marginal branch
Angiogram

TYPES OF HEART FAILURE
High-output versus low-output failure Is cardiac output high or low?
Systolic or diastolic failure Is the heart failing to pump out enough
blood, or failing to accept enough blood from the body and lungs?
Right-sided or left-sided failure Is the right or left side of the heart
failing?

MANIFESTATIONS OF HEART FAILURE
Effects of impaired pumping
Effects of decreased renal blood flow RAA pathway
Effects of the sympathetic nervous system
Angioplasty CABG

MANIFESTATIONS OF HEART FAILURE
Orthopnea: Straight Breathing, ie. Must be
straight upright, or difficult breathing occurs

CONTROL OF HEART FUNCTION

SCENARIO:
Mr. M has heart failure and he complains of severe shortness of breath, and has fluid in his lungs. He has tachycardia, increased diastolic blood pressure, pale moist skin, and says he feels weak, dizzy, and anxious all the time.
Question:Which of these signs and symptoms are due to decreased renal blood flow?
Which are due to the sympathetic nervous system? Which side of his heart do you think is failing?

LEFT-SIDED HEART FAILURE
Systolic: LV does not pump enough blood to body
Diastolic: LV does not accept enough blood from lungs
Body lacks blood
Lungs fill with fluid
right heart
lungs
left heart
body
Blood Flow

RIGHT-SIDED HEART FAILURE
Systolic: RV does not pump enough blood to lungs
Diastolic: RV does not accept enough blood from body
Body fills with blood
Lungs do not oxygenate enough blood
right heart
lungs
left heart
body
Blood Flow

PULMONARY EDEMA
Capillary fluid moves into alveoli Lung becomes stiffer Harder to inhale Less gas exchange in alveoli Crackles Frothy pink sputum
Hemoglobin not completely oxygenated

QUESTION
Tell whether the following statement is true or false:
The characteristic pink sputum produced is pulmonary edema is tinged with blood.

ANSWER
True
In pulmonary edema, the alveolar capillary membrane is damaged, and blood from the capillaries moves into the alveoli. The blood from the capillaries causes the sputum (produced from the lower respiratory tract) to appear pink or light red.
CARDIOGENIC SHOCK
Heart fails to pump blood adequately
Decreased cardiac output lowers BP
Sympathetic system responds
Vasoconstriction increases resistance to blood flow
Increased workload on heart worsens heart failure

TYPES OF SHOCK
Cardiogenic
Hypovolemic
Obstructive
Distributive
Septic

BLOOD PRESSURE
BP = CO x PR
Which of the following affect CO, and which affect PR? Why? Blood volume Heart rate Vasoconstriction Angiotensin II Aldosterone Epinephrine Histamine

SCENARIO:
Mr. M was injured in a motorcycle accident.
On his arrival at the hospital he presented with bleeding from the right leg, restlessness, pallor, sweating, elevated heart rate, weak pulse, rapid breathing, and lack of bowel sounds; his blood pressure was slightly elevated
Question: What has happened to this patient’s:
Stroke volume Cardiac output Sympathetic nervous system

SCENARIO (CONT.)
Although he was given 6 units of blood, Mr. M got worse
He became lethargic and his blood pressure began to fall; he still had no bowel sounds or urine production
Question: The intern ordered epinephrine, and
Mr. M’s blood pressure increased. Why?
Later, you overhear the resident telling the intern that was not the best treatment. Why not, if it raised Mr. M’s blood pressure?

SCENARIO (CONT.)
Mr. M’s blood pressure went up a bit
He has been moved out of the ICU
Question:
His chart says you should do a 24-hour urine collection. Why?

SCENARIO (CONT.)
Mr. M appears to be improving
He sleeps quite a lot, but his blood pressure has remained stable; he had a little urine production; and he did not eat his supper
Checking on him in the evening, you notice that he is slightly flushed, his respiration rate is a little high, and his temperature is elevated
Question:
What is happening to his peripheral resistance?
What do you expect his heart rate to be like? Why?
DISTRIBUTIVE OR VASODILATORY SHOCK
Blood vessels dilate
There is not enough blood to fill the circulatory system
Blood flow decreases
Less blood is returned to the heart
Less blood is circulated to the body

QUESTION
Which type of shock is caused by low blood volume?
a. Cardiogenic
b. Hypovolemic
c. Distributive
d. Septic
ANSWER
b. Hypovolemic
Hypo (low) volemia (blood volume) occurs when a patient has lost blood due to trauma, surgery, or third space fluid loss.
CAUSES OF DISTRIBUTIVE SHOCK
Decreased sympathetic activity: neurogenic Brain or spine injury; anesthetics;
insulin shock; emotion Vasodilator substances in blood
Type I hypersensitivity (anaphylactic shock)
Inflammatory response to infection (sepsis)
Vessel damage from severe hypovolemia

MECHANISM OF TYPE I HYPERSENSITIVITY
Mast cell
Mast cell degranulates
IgE attaches to mast cell
Allergen attaches to IgE
Allergen
Granules released: Histamine,
acetylcholine, kinins, leukotrienes, and prostaglandins all cause vasodilation

ANAPHYLAXIS
Systemic response to the inflammatory mediators released in type I hypersensitivity
Histamine, acetylcholine, kinins, leukotrienes, and prostaglandins all cause vasodilation
º What will happen when arterioles vasodilate throughout the body?
Acetylcholine, kinins, leukotrienes, and prostaglandins all can cause bronchoconstriction
º What will happen when the bronchioles constrict?

SEPSIS OR SYSTEMIC INFLAMMATORY RESPONSE SYNDROME (SIRS)
Inflammatory mediators released into the circulation Tumor necrosis factor Interleukins Prostaglandins
Cause systemic signs of inflammation Fever and increased respiration,
respiratory alkalosis, vasodilation, warm flushed skin
Activate inflammatory pathways Coagulation, complement

SEPSIS OR SYSTEMIC INFLAMMATORY RESPONSE SYNDROME (SIRS) (CONT.)
Discussion:
Why is septic shock called distributive?
In the later phases of septic shock, blood volume decreases. What part of the inflammatory process explains this?

TYPES OF SHOCK
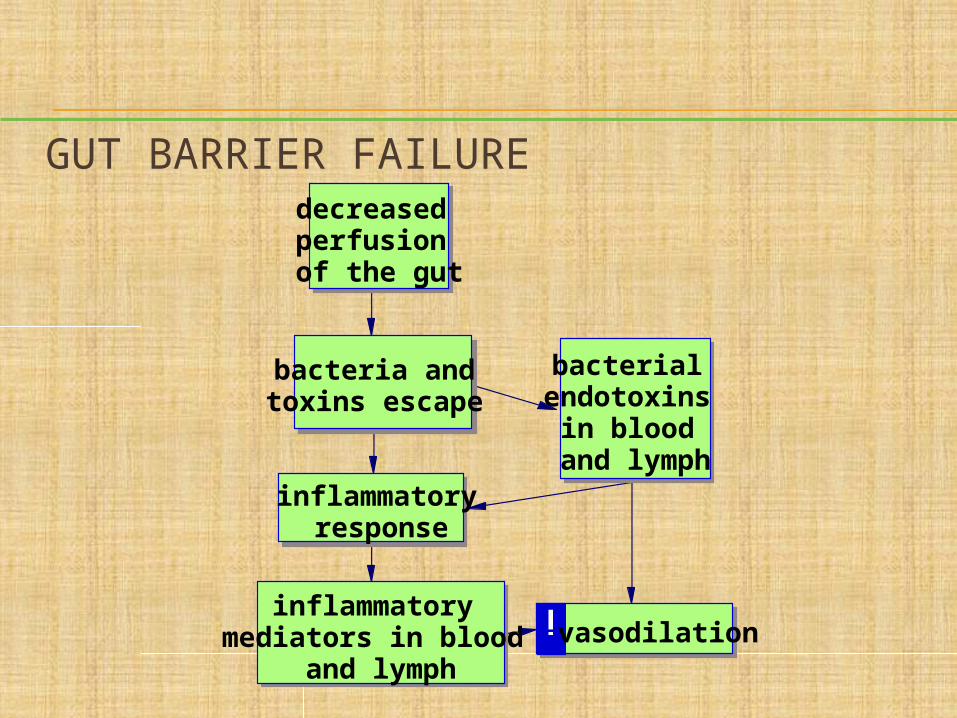
GUT BARRIER FAILUREdecreased perfusion of the gut
bacteria and toxins escape
inflammatory response
bacterial endotoxins
in blood and lymph
inflammatory mediators in blood
and lymphvasodilation

SEPTIC SHOCK
vasodilation
decreased peripheral resistance
decreased blood pressure
SEPTIC SHOCK40% mortality

SEPTIC SHOCK Also called systemic
inflammatory response syndrome (SIRS)
Inflammatory mediators also increase the metabolic rate of tissues, so they need more oxygen
The role of the endothelium in severe sepsis and multiple organ
dysfunction syndrome
(Aird, W. C. [2003.] The role of the endothelium in severe sepsis and multiple organ dysfunction syndrome. Blood 101[10],3765-3777. Retrieved February 10, 2004, from http://www.blood journal.org/cgi/content/full/101/10/3765.0)
inflammatory mediators
vascular endothelial cells respond and:
promote clot
formation
create adhesive molecules
more WBCs move out into the tissues and release more
inflammatory mediators
produce more vasodilation
substances (NO)
more vasodilation
The role of the endothelium in severe sepsis and multiple organ dysfunction syndrome

SEPTIC SHOCK (CONT.)
“Despite the prompt implementation of appropriate antibiotic therapy, sepsis mortality remains high, in the range of 28% to 50%.”
(Aird, W. C. [2003.] The role of the endothelium in severe sepsis and multiple organ dysfunction syndrome. Blood 101[10],3765-3777. Retrieved February 10, 2004, from http://www.blood journal.org/cgi/content/full/101/10/3765.0)
“Second, patients with culture-positive and culture-negative sepsis or septic shock have comparable mortality rates.”
SEPTIC SHOCK (CONT.)
“Third, administration of anti-endotoxin antibodies in large, clinical trials did not improve survival.”
(Aird, W. C. [2003.] The role of the endothelium in severe sepsis and multiple organ dysfunction syndrome. Blood 101[10],3765-3777. Retrieved February 10, 2004, from http://www.blood journal.org/cgi/content/full/101/10/3765.0)

QUESTION
Which type of shock is the result of a severe allergic reaction?
a. Cardiogenic
b. Obstructive
c. Anaphylactic
d. Septic
ANSWER
c. Anaphylactic
Anaphylactic shock is caused when inflammatory mediators are released (type I hypersensitivity reaction). The mediators include histamine, acetylcholine, kinins, leukotrienes, and prostaglandins, all of which cause vasodilation.
ACTIVATED PROTEIN C
Drotrecogin alpha - a recombinant form of human activated protein C that has anti-thrombotic, anti-inflammatory, and profibrinolytic properties - a treatment for severe sepsis
Blocks clotting
Blocks inflammation
Increases survival of the most seriously ill sepsis patients
May cause bleeding!
The main function of protein C is its anticoagulant property as an inhibitor
of coagulation factors V and VIII
COMPLICATIONS OF SHOCK
Scenario: A doctor has been called in to treat Mr. M
and has started him on fluid and antibiotics
You are warned to watch him carefully for any signs of respiratory distress
Question: Why would blood pressure
imbalances cause respiratory distress?

COMPLICATIONS OF SHOCK (CONT.)
Acute respiratory distress syndrome
Acute renal failure
Gastrointestinal complications
Disseminated intravascular coagulation
Multiple organ dysfunction syndrome
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS)
Exudate enters alveoli Blocks gas exchange Makes inhaling more difficult
Neutrophils enter alveoli Release inflammatory
mediators Release proteolytic enzymes

ACUTE RENAL FAILURE (ARF)
Renal vasoconstriction cuts off urine production Acute renal failure
Continued vasoconstriction cuts off renal oxygen supply
Renal tubular cells die Acute tubular necrosis

DISSEMINATED INTRAVASCULAR COAGULATION (DIC) coagulation
pathways activated
clots in many small blood vessels
microinfarcts, ischemia
platelets and
clotting proteins used up
bleeding problems

MULTIPLE ORGAN DYSFUNCTION SYNDROME (MODS)
The most frequent cause of death in the noncoronary intensive care unit
Mortality rates vary from 30% to 100%
Mechanism not known

QUESTION
Tell whether the following statement is true or false:
Treatment for ARDS often includes breathing assistance using mechanical ventilation.

ANSWER
TrueBecause alveoli are filled with exudate
and blood that has leaked from the capillary, the surface area available for gas exchange is greatly reduced. Most patients will require ventilatory support until the process reverses. ARDS has a high mortality rate because it is difficult to ventilate these patients.


















