
Chapter 13 Psychological Disorders Slides prepared by Randall E. Osborne, Texas State University-San...
73
Chapter 13 Psychological Disorders Slides prepared by Randall E. Osborne, Texas State University- San Marcos PSYCHOLOGY Schacter Gilbert Wegner
-
Upload
collin-augustine-jacobs -
Category
Documents
-
view
216 -
download
0
Transcript of Chapter 13 Psychological Disorders Slides prepared by Randall E. Osborne, Texas State University-San...

Chapter 13
Psychological Disorders
Slides prepared by Randall E. Osborne, Texas State University-San Marcos
PSYCHOLOGYSchacter
Gilbert
Wegner

PSYCHOLOGYSchacter
Gilbert
Wegner
13.1
Identifying Psychological Disorders: What Is Abnormal?

3
13.1 Identifying Psychological Disorders
- “Psychological Disorder” is a relatively new invention•possessed by demons•God’s punishment•criminal
- Medical model
- DSM-IV-TR

4
13.1 Defining the Boundaries of Normality
- Deviation from average?
- DSM-IV-TR—three key elements for symptoms to qualify as a potential mental disorder• manifested in symptoms that involve disturbances in
behavior, thoughts, or emotions• symptoms associated with significant personal distress or
impairment• symptoms stem from an internal dysfunction
biological, psychological, or both

5
13.1 Defining the Boundaries of Normality
- Determining the degree to which a person has a mental disorder is difficult
- Global assessment of functioning

6
13.1 Classification
- North American clinicians used to divide disorders into just two categories:•psychosis•neurosis
- 1952—Diagnostic Manual of Mental Disorders (DSM) published• recognized need to have a consensual
diagnostic system

7
13.1 Classification
- DSM-IV-TR- Neurosis —now
anxiety disorders• each of the anxiety
disorders, then, is defined by observable features such as excessive anxiety in general, in a particular setting, etc.

8
13.1 Classification
- Comorbidity—diagnosis is also difficult because some people suffer from more than one disorder
9
13.1 Classification & Causation
- Medical model suggests that a diagnosis is useful because any given category of illness is likely to have a distinctive cause
- Etiology of mental disorders- Common prognosis- In reality, it is too simplistic to think that there is a single cause, internal to the person that has a single cure

10
13.1 Classification & Causation
- Integrated perspective•biological factors•psychological factors•environmental factors
- Diathesis-stress model—predisposed with a trigger•a diathesis can be inherited (heritability)•stressful conditions, though, needed to trigger
11
13.1 Consequences of Labeling
- Stigma may explain why 70% of people with diagnosable mental disorders do not seek treatment
- Erroneous beliefs•mental disorder is a sign of personal weakness•psychiatric patients are dangerous•education about mental disorders dispels the
stigma

PSYCHOLOGYSchacter
Gilbert
Wegner
13.2
Anxiety Disorders: When Fears Take Over

13
13.2 Generalized Anxiety Disorder
- Anxiety disorder
- Generalized anxiety disorder•why generalized?•5% prevalence•SES differences?•benzodiazepines (valium, librium) stimulate
GABA

14
13.2 Phobic Disorders
- Specific phobia
- Social phobia
- Preparedness theory
- Temperament
- Abnormalities in neurotransmitters serotonin and dopamine common

15
13.2 Panic Disorder
- Panic disorder—recurring panic attacks
- Agoraphobia
- 8-12% have an occasional panic attack
- Modest heritability component
- Those with panic disorder acutely sensitive to sodium lactate (reinforces biological view)
16
13.2 Obsessive-Compulsive Disorder
- Anxiety plays a role
- Primary symptom is unwanted, recurrent thoughts (obsession) and actions (compulsion)
- Numbers often take on exaggerated meaning
- 2.5% prevalence rate

17
13.2 Obsessive-Compulsive Disorder
- Most common obsessions involve contamination, aggression, death, sex, disease, orderliness, and disfigurement
- Most common compulsions involve cleaning, checking, repeating, ordering/arranging, and counting
- Obsessions typically derive from concerns that could pose a real threat (e.g., contamination, disease)—preparedness theory• but perceived threat is extreme and becomes
maladaptive

PSYCHOLOGYSchacter
Gilbert
Wegner
13.3
Dissociative Disorders: Going to Pieces
19
13.3 Dissociative Disorders
- Dissociative disorder
- Dissociative identity disorder
- 0.5 to 1% prevalence
- Female to male ratio = 9 to 1
- Most report history of severe childhood abuse and trauma
20
13.3 Dissociative Disorders
- Cannot result from normal forgetting or brain injury, drugs, or another mental disorder
- Dissociative amnesia• loss is usually for a traumatic specific event or
period of time
- Dissociative fugue• loss of former identity and assumption of a new
identity

PSYCHOLOGYSchacter
Gilbert
Wegner
13.4
Mood Disorders: At the Mercy of Emotions

22
13.4 Mood Disorders
- Depressive disorders- Much more than sadness•dysfunctional•chronic•outside socially or culturally accepted norms
- Not the same as sorrow and grief•normal, possibly adaptive, response to a tragic
situation

23
13.4 Depressive Disorders
- Major depressive disorder• twice as common in women as men
hormones as postpartum depression
response style
- Dysthymia•same symptoms, less severe but longer
- Double depression- Seasonal affective disorder (SAD)

24
13.4 Depressive Disorders—Biological Factors
- Heritability estimates range from 33-45%
- Drugs that affect norepinephrine and serotonin can reduce depression
- Diminished activity in left prefrontal cortex and increased activity in right•areas associated with the processing of
emotions

25
13.4 Depressive Disorders—Psychological Factors
- Negative cognitive style
- Helplessness theory
- May construct social world in ways that contribute to and confirm their negative beliefs
- Depressed low self-esteem individuals seek confirming negative feedback

26
13.4 Bipolar Disorder
- Bipolar disorder—defined- Lifetime risk of 1.3% for both genders•10% have rapid cycling bipolar disorder•4 or more mood episodes per year
- Persistent illness•24% relapsed within 6 months•77% have at least one new episode within 4
years
27
13.4 Bipolar Disorder
- Biological factors•high rate of heritability (80% for identical twins)•close relatives also at heightened risk for
unipolar depression•bipolar disorder may be polygenic
- Psychological factors•stressful life experiences•stress + personality

PSYCHOLOGYSchacter
Gilbert
Wegner
13.5
Schizophrenia: Losing the Grasp on Reality

29
13.5 Schizophrenia
- Schizophrenia—defined
- Symptoms—2 or more of the following during a continuous period of 1 month with signs of the disorder persisting for at least 6 months• delusion• hallucination• disorganized speech• grossly disorganized or catatonic behavior• negative symptoms (e.g., blunted affect)
30
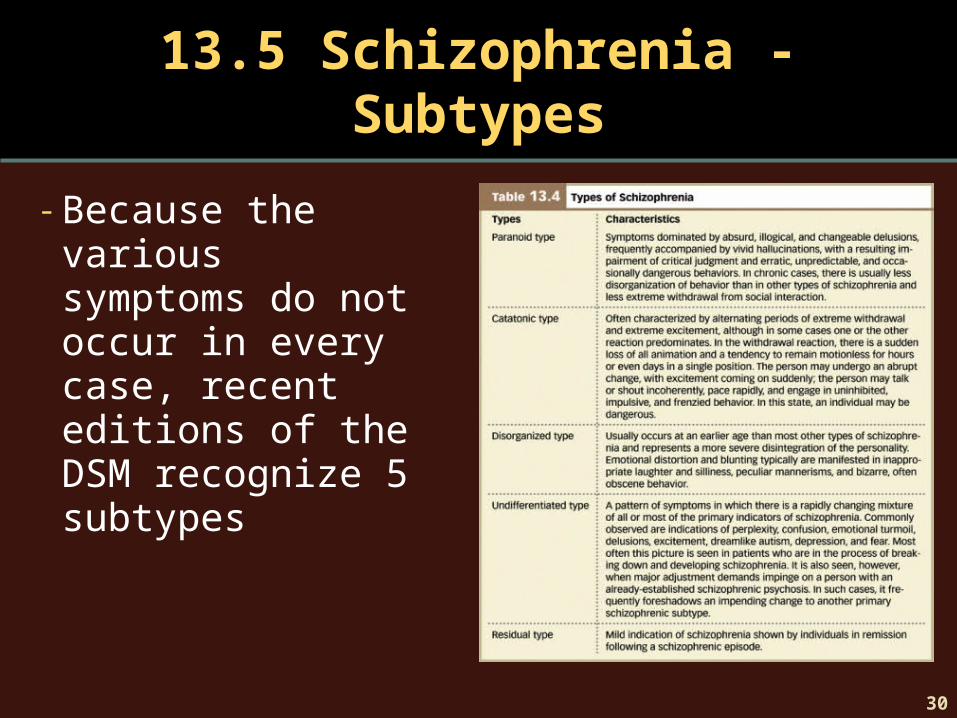
13.5 Schizophrenia - Subtypes
- Because the various symptoms do not occur in every case, recent editions of the DSM recognize 5 subtypes
31
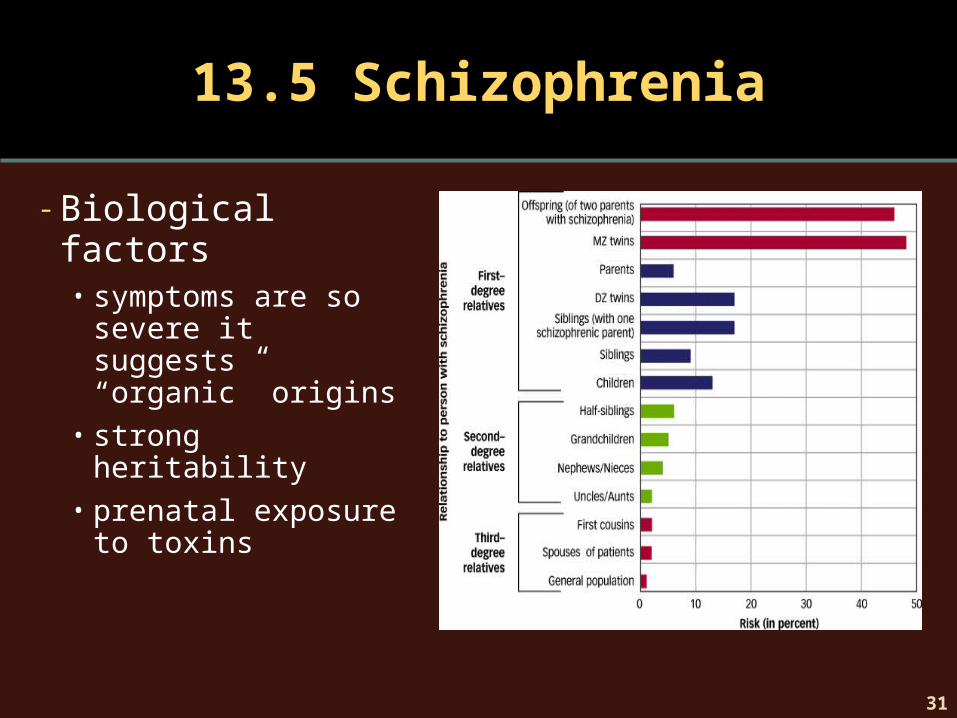
13.5 Schizophrenia
- Biological factors• symptoms are so
severe it suggests “organic” origins
• strong heritability• prenatal exposure to
toxins

32
13.5 Schizophrenia
- Prenatal exposure to toxins
- Dopamine hypothesis
- Neuroanatomy• enlarged ventricles
(left photo)• tissue loss in parietal
lobe progressing to much of brain

33
13.5 Schizophrenia
- Psychological factors- Family environment•extreme conflict• lack of communication•chaotic relationships
- Expressed emotion • intrusiveness•excessive criticism
PSYCHOLOGYSchacter
Gilbert
Wegner
13.6
Personality Disorders: Going to Extremes

35
13.6 Personality Disorders
- Personality disorders—defined
- Fall into three clusters:• odd/eccentric• dramatic/erratic• anxious/inhibited

36
13.6 Personality Disorders
- Antisocial personality disorder•history of conduct disorder•sociopath and psychopath•one study of 22,790 prisoners—47% of men and
21% of women were diagnosed with APD• less activity in amygdala and hippocampus to
words that elicit fear in non-APD

37

Chapter 14
Treatment of Psychological
Disorders
Slides prepared by Randall E. Osborne, Texas State University-San Marcos
PSYCHOLOGYSchacter
Gilbert
Wegner

PSYCHOLOGYSchacter
Gilbert
Wegner
14.1
Treatment: Getting Help to Those Who Need It
40
14.1 Getting Help to Those Who Need It
- Why people need treatment- Personal costs• interfere with life•symptoms worsen
- Social and financial burdens•affects family life, work, relationships•estimated financial burden of 42.3 million
annually

41
14.1 Getting Help to Those Who Need It
- Why people cannot or will not seek treatment:•may not believe disorder needs treated•barriers present access to treatment•don’t know enough about treatment to be able to
get it
- Beliefs may keep someone from seeking treatment
42
14.1 Approaches to Treatment
- Psychotherapy• interact with psychotherapist
- Medical/Biological•disorder is treated with drugs or surgery

PSYCHOLOGYSchacter
Gilbert
Wegner
14.2
Psychological Therapies: Healing the Mind through Interaction

44
14.2 Approaches to Treatment
- Psychotherapy• psychological
therapy
- Eclectic psychotherapy

45
14.2 Psychodynamic Therapy
- Psychodynamic therapy—defined- Psychoanalysis•conversion disorder
- How can therapist develop insight?• free association•dream analysis• interpretation•analysis of resistance

46
14.2 Psychodynamic Therapy
- Free association• client reports what enters
mind without censorship or filtering
- Resistance• fear of confronting
unconscious

47
14.2 Psychodynamic Therapy
- Dream analysis• disguised clues to unconscious
- Interpretation• decipher meaning underlying what client says or does
- Analysis of resistance• present interpretations to client and assess resistance• resistance might mean the interpretation “hits close to
home”

48
14.2 Psychodynamic Therapy
- Transference•client and analyst develop a close relationship•understanding this relationship may give clues to
client’s past and future relationships
- Beyond psychoanalysis•Freud’s students generated new approaches•social themes• interpersonal psychotherapy

49
14.2 Behavioral and Cognitive Therapies
- Approaches now usually integrated—cognitive behavioral therapy (CBT)
- Behavior therapy•applying principles of learning to change
problems
- Aversion therapy•eliminating unwanted behaviors— positive
punishment

50
14.2 Behavioral and Cognitive Therapies
- Promoting desired behaviors• token economy
- Eliminating unwanted emotional responses• exposure therapy• systematic
desensitizationvirtual reality therapy

51
14.2 Behavioral and Cognitive Therapies
- Cognitive therapy• emphasize the
“meaning” of an event
- Albert Ellis—rational emotive behavior therapy• therapist points out
errors in client’s thinking
- Cognitive restructuring
- Mindfulness meditation

52
14.2 Behavioral and Cognitive Therapies
- Cognitive behavioral therapy• acknowledges that there are behaviors that people
cannot control through rational thought• focuses on dysfunctional thoughts and maladaptive
behaviors
- Aspects of CBT• problem focus• structured• transparent• flexible

53
14.2 Humanistic and Existential Therapies
- Assume human nature is generally positive- Emphasize natural tendency of each individual to
strive for personal improvement- Person-centered therapy (Rogers)
• client can determine therapy goals• empathy• unconditional positive regard
- Gestalt therapy—“own” thoughts, behaviors, and feelings• focusing• empty chair technique
54
14.2 Groups in Therapy
- Individuals do not suffer alone—nor are they the only ones who suffer
- Couples therapy
- Family therapy
- Self-defeating interaction cycle
- Think of family, couple, as a system

55
14.2 Group Therapy
- If individual can benefit from interacting with therapist, might benefit more interacting with other clients interacting with the therapist•built-in set of peers•not alone in one’s suffering• role models for appropriate behavior

56
14.2 Self-Help and Support Groups
- Some of the same benefits of group therapy but lower cost
- Can do more harm than good—no trained professional present
- Alcoholics Anonymous•chronic disease•discourage self-blame• look beyond self for strength

PSYCHOLOGYSchacter
Gilbert
Wegner
14.3
Medical and Biological Treatments: Healing the Mind
through the Brain

58
14.3 Medical and Biological Treatments
- Trepanning
- Antipsychotic medications•completely changed the way schizophrenia was
managed•work well for positive symptoms but not negative

59
14.3 Medical and Biological Treatments
- Psychopharmacology•antipsychotic medications may block dopamine
receptors in mesolimbic areas—associated with positive symptoms such as delusions and hallucinations
- Atypical antipsychotics•appear to affect both dopamine and serotonin
receptors•work well on both positive and negative
symptoms

60
14.3 Medical and Biological Treatments
- Antianxiety medications
- Facilitate action of GABA
- Benzodiazepines•potential for abuse•dangerous when mixed with alcohol•withdrawal symptoms•side effects
61
14.3 Medical and Biological Treatments
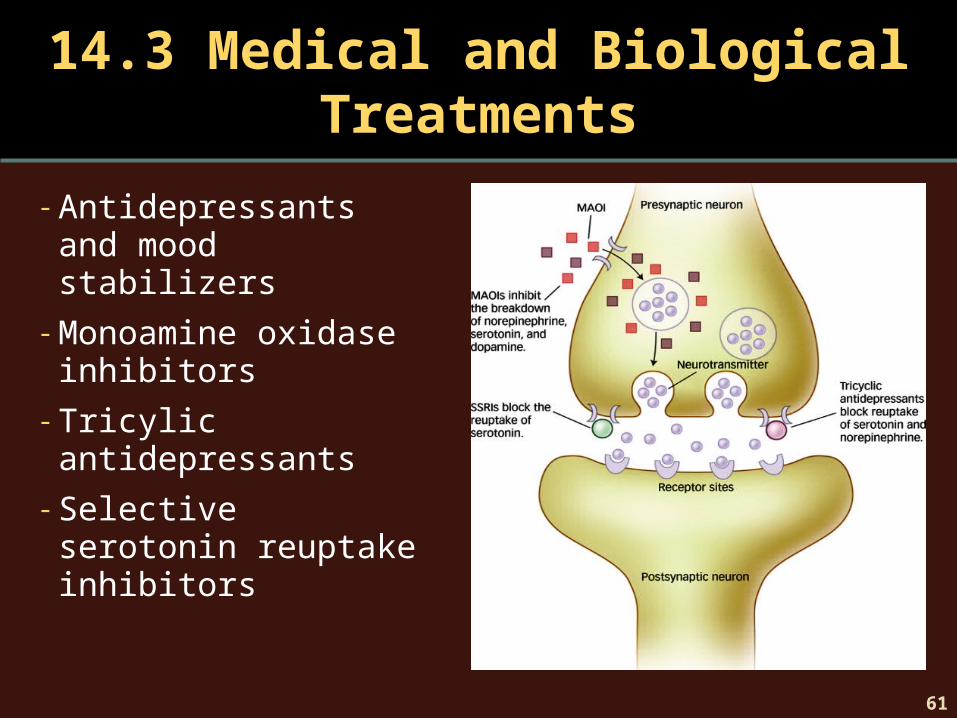
- Antidepressants and mood stabilizers
- Monoamine oxidase inhibitors
- Tricylic antidepressants
- Selective serotonin reuptake inhibitors
62
14.3 Medical and Biological Treatments
- Herbal and natural products•St. John’s Wort
- Not considered medications so not closely scrutinized or regulated
- Some evidence that some of these work but not overwhelming
- Worthy of more research
63
14.3 Medications in Perspective
- Medications can be life changing
- Can relieve negative symptoms but leave specific problems untreated
- For severe disorders, medication is usually a critical first step
- For other disorders (such as depression) issue is deciding whether medication or psychotherapy should be used
64
14.3 Medications in Perspective
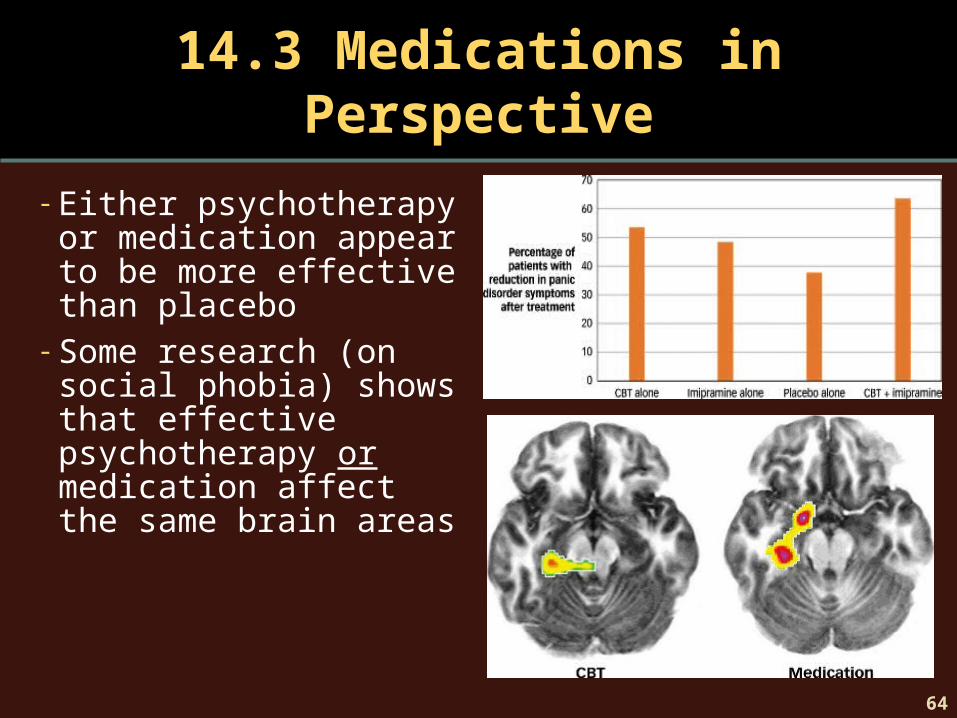
- Either psychotherapy or medication appear to be more effective than placebo
- Some research (on social phobia) shows that effective psychotherapy or medication affect the same brain areas

65
14.3 Biological Treatments beyond Medication
- Electroconvulsive therapy• treat severe depression•memory and concentration loss•usually now used as a “last resort”
- Transcranial magnetic stimulation•magnet placed above right or left eyebrow to
stimulate right or left prefrontal cortex• treat severe depression without memory loss or
concentration loss of ECT

66
14.3 Biological Treatments beyond Medication
- Phototherapy•seasonal affective disorder
- Psychosurgery•OCD unresponsive to other treatments•not like lobotomies of 1930s•cingulotomy—destroy part of cingulate gyrus and
corpus callosum•anterior capsulotomy—create small lesions to
disrupt pathway between caudate nucleus and putamen

PSYCHOLOGYSchacter
Gilbert
Wegner
14.4
Treatment Effectiveness: For Better or for Worse

68
14.4 Treatment Effectiveness
- If you take a pill and soon feel better, did the pill cure you?
- Treatment illusions•natural improvement•nonspecific treatment effects
placebo effects
• reconstructive memorymisremembering symptom severity

69
14.4 Treatment Studies
- Outcome studies•evaluate whether a particular treatment works• treatment and control conditions
- Process studies•answer questions why treatment works or under
what circumstances the treatment will work
- Double-blind experiment

70
14.4 Which Treatments Work

71
14.4 Which Treatments Work

72
14.4 Dangers of Treatment
- Some treatments cause unintended harm
- Side effects, potential drug interactions, dependence, complications
- Iatrogenic illness
- Client in therapy is vulnerable
73
14.4 Dangers of Treatment
- Set of ethical standards•strive to benefit client and do no harm•establish relationship of trust•promote accuracy, honesty, & truthfulness•seek fairness in treatment and take precaution to
avoid bias• respect dignity and worth of all people


















