“Challenging practice in non-ST segment elevation Acute Coronary Syndromes (ACS)” Professor...
18
“Challenging practice in non-ST segment elevation Acute Coronary Syndromes (ACS)” Professor Jennifer Adgey Royal Victoria Hospital, Belfast 26 th January 2006 Conflicts of interest- Speaker symposia: Eli-Lilly, MSD, Sanofi- Aventis, BMS, GSK
-
Upload
vivien-briggs -
Category
Documents
-
view
214 -
download
0
Transcript of “Challenging practice in non-ST segment elevation Acute Coronary Syndromes (ACS)” Professor...

“Challenging practice in non-ST segment elevation Acute
Coronary Syndromes (ACS)”
Professor Jennifer AdgeyRoyal Victoria Hospital, Belfast
26th January 2006
Conflicts of interest- Speaker symposia: Eli-Lilly, MSD, Sanofi-
Aventis, BMS, GSK

Chest pain in the A&E department
• Approximately 600,000 patients per annum attend A&E in the UK with chest pain
• 25% will have NSTE-ACS
J R Coll Physicians Edinb 2003;33:36-43

Epidemiology of Acute Coronary Syndromes
ST-segment elevation MI
Prevalence: 30%-42%
Non-ST-segment elevation ACS
Prevalence: 51%-63%
Death and non-fatal (re)-infarction at 6 months: 13%

Acute Coronary Syndromes: Mortality at 6 Months
Days from randomization
Savonitto et al. JAMA. 1999;281:707.
Mo
rta
lity
(%)
1800 20 40 60 80 100 1600
6
8
10
2
4
120 140
% Mortality at 6 Months
T-wave inversion3.4% (n=2,723)
ST-segment elevationand depression9.1% (n=1,769)
ST-segment depression8.9% (n=4,263)
ST-segment elevation6.8% (n=3,369)

Risk stratification, Risk of progression to death and MI
Elevated troponin levelsDiabetes Patients with recurrent ischaemiaRecurrent chest painDynamic ST-segment changes(ST-segment depression or transient ST-segment elevation)Haemodynamic instabilityMajor arrhythmias (VF, VT) Early post-infarction unstable angina
No elevation of troponin or otherNo elevation of troponin or other biochemical markersbiochemical markers
Negative troponin test recorded Negative troponin test recorded twicetwice
No recurrence of chest pain No recurrence of chest pain
within observational period within observational period
No ST-segment depressionNo ST-segment depressionNegative T waves, flat T waves, Negative T waves, flat T waves, normal ECGnormal ECG
High-risk patients Low-risk patients
Infusion of GP IIb-IIIa Inhibitor
Invasive strategy
Conservative strategy
Baseline treatment: heparin (LMWH or UFH), ASA, clopidogrel, beta-blockers, nitrates

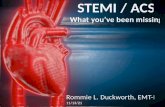
Troponin + is associated with presence of Thrombus on Angioscopy
0
10
20
30
40
50
60
70
80
90
100
• Only 20% to 25% of thrombi seen on angioscopy (gold standard) is seen on angiography (i.e. angiography misses 4 out of 5 thrombi in Tn + pts)
Okamatsu et al, Circulation 2004; 109:465-470.
Tn - Tn -Tn + Tn +
9%18%
86%
34%
Angiogram Angioscope
% T
hro
mb
us
P=0.0001
P=0.41
Only 1 of 5 thrombi
detected

NSTE-ACS
Medical treatmentPCI with provisional
abciximab or eptifibatide
Conservative approach
Early non invasive stress testing
PCI with abciximab
or eptifibatide
PCI with eptifibatide or tirofiban
Silber S. et al. ESC PCI guidelines 2005
ESC PCI Guidelines for NSTE ACS
ASA, Clopidogrel, UFH, Betablockers, Nitrates, Statins (ACE)
Low risk
Without upstream GP IIb/IIIa RA
With upstream GP IIb/III RA
Invasive approach
High risk

Can the results of clinical trials be transferred to the real world? – NRMI 4
In-hospital mortality for patients treated with a glycoprotein (GP) IIb/IIIa inhibitor versus those not treated, by the National Registry of Myocardial Infarction non–ST-elevation myocardial infarction (NRMI-NSTEMI) risk score.
Early use
(N=15, 379)
No early use (N=45, 391)
Overall (N=60,770)
P
3.3% 9.6% 8% <0.0001
In-hospital mortality by early use of GPIIb/IIIa inhibitor
JACC 2003;42:45-53

JACC 2003;42:45-53

CRUSADE: Unadjusted Mortality According to Early* GP IIb-IIIa Inhibitor Use
∆ 41%P < 0.0001†
∆ 41%P < 0.0001†
2.7%
4.6%
0%
2%
4%
6%
8%
% In-hospital Mortality
No Early GP IIb-IIIa Inhibitor (n = 41,896)
Early GP IIb-IIIa Inhibitor (n = 24,168)
*Within 24 hours
†Risk-adjusted odds ratio:
0.96 (0.86, 1.07)
‡‡
Source: Duke Clinical Research Institute.
CRUSADE - Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes with Early Implementation of the ACC/AHA Guidelines; GP = glycoprotein.

Are GPIIb/IIIa inhibitors really necessary when clopidogrel is available?
Eptifibatide provides additional platelet inhibition in Non-ST-Elevation MI patients already treated with aspirin and clopidogrel - PEACE
T1 – before clopidogrel administration
T2 – >2 hours after clopidogrel
T3 – during eptifibatide infusion following clopidogrel
JACC 2004;43:162-168

Months
Cum
ula
tive
eve
nt r
ate
(%)
14
12
10
8
6
4
2
0 2 4 6 8 10 12
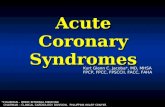
placebo
INTEGRILIN 35% RRR p=0.001 (at 12 months)
12.4%
8.0% 3.9%
4.4%
NNT=23 (at 12 months)
ESPRIT: 1-Year Death or MI
(adapted from The ESPRIT Investigators study, 2000)

DEACON Study: Bivalirudin and Clopidogrel Alone Do Not Adequately Prevent
Platelet Aggregation
Am J Cardiol 2005;95:1453–1456
Bivalirudin + Clopidogrel
% Platelet Inhibition of TRAP-induced Aggregation
% Platelet Inhibition of ADP-induced Aggregation
- 20%
0%
20%
40%
60%
80%
Baseline 10 min 30 min 1 hr
100%
- 20%
0%
20%
40%
60%
80%
100%
Baseline 10 min 30 min 1 hr
Bivalirudin + Clopidogrel
INTEGRILIN + Heparin + Clopidogrel
INTEGRILIN + Heparin + Clopidogrel
Heparin + Clopidogrel Heparin +
Clopidogrel
When to start GPIIb/IIIa inhibitor therapy (upstream or downstream)?

Six month mortality in patients with and without new or recurrent MI during the first 72 hours after randomisation in the Platelet Glycoprotein
IIb/IIIa in Unstable Angina: Receptor Suppression Using Integrelin Therapy (PURSUIT) trial.
0
2
4
6
8
10
12
14
16
18
20
1 2 3 4 5 6
MI within 72 h
No MI within 72h
Cu
mu
lati
ve m
ort
alit
y ra
te
Time in months
18.3%
5.5%
12.8% ↓ (p=0.001)
Clin Cardiol 2000;23 (suppV):V1-V12
Placebo and eptifibatide 180/2.0 combined

PURSUIT
• Patients receiving eptifibatide had significantly reduced incidence of MI at 72 hours (5.6% vs 6.9% with placebo p=0.009) as well as prior to PCI within 72 hours (1.8% vs 5.5% with placebo p=0.001)
Clin Cardiol 2000;23 (suppV):V1-V12

Incidence of death or MI at 30 days according to management strategy during the first 72 hours
Placebo (%)
Eptifibatide
(%)
P
Diagnostic CC<72 hours
North America
Worldwide
15.8
16.2
12.1
12.8
0.008
0.005
PCI <72 hours
North America
Worldwide
16.6
16.8
11.4
11.8
0.024
0.012
CABG <72 hours
North America
Worldwide
32.7
33.5
19.3
18.4
0.009
0.001
No PCI <72 hours
North America
Worldwide
14.5
15.6
11.8
14.6
0.035
0.226

PURSUIT
• The benefit of GpIIb/IIIa inhibitor (eptifibatide) is most marked if commenced within 6 hours of symptom onset
• Largest absolute reduction in death or MI at 30 days in those in whom eptifibatide was started within 6 hours of symptom onset (2.8%) compared to 2.3% AR reduction in patients treated between 6 and 12 hours and 1.4% AR reduction >12 hours
Clin Cardiol 2000;23 (suppV):V1-V12

Challenging practice in non-ST segment elevation Acute Coronary Syndromes (ACS)
• Identification of high risk patients admitted via the A&E department
• Early upstream administration of small molecule GPIIb/IIIa inhibitors (eptifibatide, tirofiban) are of benefit in patients receiving aspirin, clopidogrel, heparin and intervention (PCI)
• Long term follow up