Ch46 Spleen
34
CHAPTER 46 CONGENITAL ABNORMALITIES OF THE SPLEEN RUPTURE OF THE SPLEEN ANEURYSM AND INFARCTION ENLARGEMENT OF THE SPLEEN SPLENECTOMY IN THE HAEMOLYFIC ANAEMIAS SPLENOMEGALY SPLENECTOMY The spleen arises by mesenchymal differentiation along the left side of the dorsal mesogastrium in the 8 mm embryo. The weight of the normal adult spleen is between 75 and 154) g, and it is situated posteriorly between the fundus of the stomach and the diaphragm in the line of the tenth rib. The spleen is in contact with the adrenal gland, the upper pole of the kidney, the pancreas and the splenic flexure of colon. The cut surface of the spleen consists of areas of ‘red pulp’ within which can be seen pale, ovoid nodules (about 1 mm diameter) of ‘white pulp’ (Malpighian bodies). The splenic artery divides at the hilus into branches which run along the trabeculae. These trabecular arteries pass into the white pulp (Fig. 46.1) where they give off branches which are almost perpendicular to the central trunk. This
-
Upload
akash-kumar-shah -
Category
Documents
-
view
230 -
download
4
Transcript of Ch46 Spleen

CHAPTER 46
CONGENITAL ABNORMALITIES OF THE SPLEENRUPTURE OF THE SPLEENANEURYSM AND INFARCTIONENLARGEMENT OF THE SPLEENSPLENECTOMY IN THE HAEMOLYFIC ANAEMIASSPLENOMEGALYSPLENECTOMY
The spleen arises by mesenchymal differentiation along the left side of the dorsal mesogastrium in the 8 mm embryo. The weight of the normal adult spleen is between 75 and 154) g, and it is situated posteriorly between the fundus of the stomach and the diaphragm in the line of the tenth rib. The spleen is in contact with the adrenal gland, the upper pole of the kidney, the pancreas and the splenic flexure of colon.
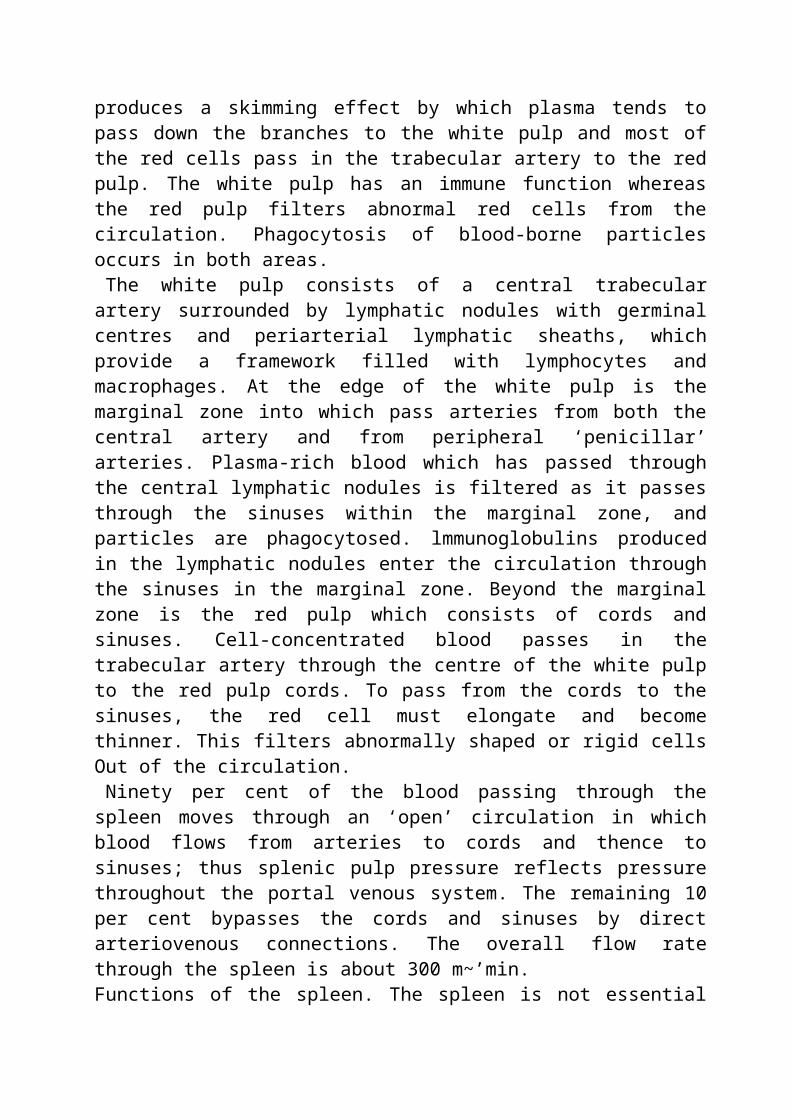
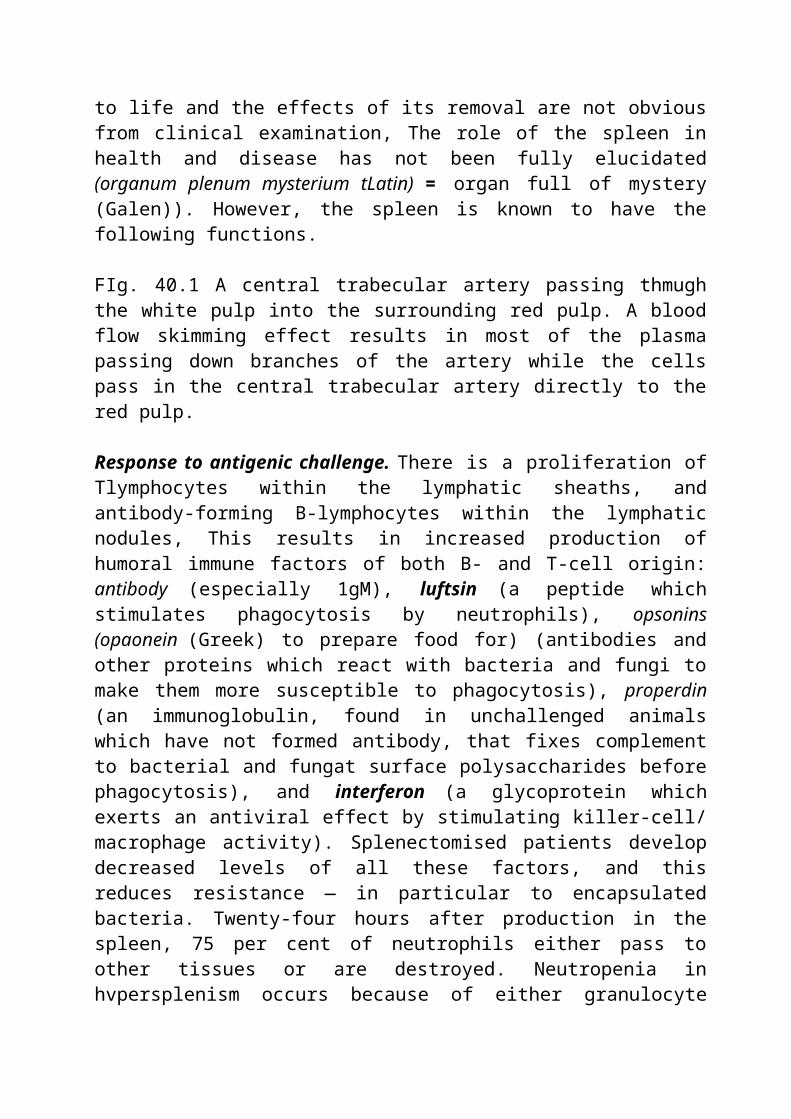
The cut surface of the spleen consists of areas of ‘red pulp’ within which can be seen pale, ovoid nodules (about 1 mm diameter) of ‘white pulp’ (Malpighian bodies). The splenic artery divides at the hilus into branches which run along the trabeculae. These trabecular arteries pass into the white pulp (Fig. 46.1) where they give off branches which are almost perpendicular to the central trunk. This produces a skimming effect by which plasma tends to pass down the branches to the white pulp and most of the red cells pass in the trabecular artery to the red pulp. The white pulp has an immune function whereas the red pulp filters abnormal red cells from the circulation. Phagocytosis of blood-borne particles occurs in both areas.
The white pulp consists of a central trabecular artery surrounded by lymphatic nodules with germinal centres and periarterial lymphatic sheaths, which provide a framework filled with lymphocytes and macrophages. At the edge of the white pulp is the marginal zone into which pass arteries from both the central artery and from peripheral ‘penicillar’ arteries. Plasma-rich blood which has passed through the central lymphatic nodules is filtered as it passes through the sinuses within the marginal zone, and particles are phagocytosed. lmmunoglobulins produced in the
lymphatic nodules enter the circulation through the sinuses in the marginal zone. Beyond the marginal zone is the red pulp which consists of cords and sinuses. Cell-concentrated blood passes in the trabecular artery through the centre of the white pulp to the red pulp cords. To pass from the cords to the sinuses, the red cell must elongate and become thinner. This filters abnormally shaped or rigid cells Out of the circulation.
Ninety per cent of the blood passing through the spleen moves through an ‘open’ circulation in which blood flows from arteries to cords and thence to sinuses; thus splenic pulp pressure reflects pressure throughout the portal venous system. The remaining 10 per cent bypasses the cords and sinuses by direct arteriovenous connections. The overall flow rate through the spleen is about 300 m~’min.Functions of the spleen. The spleen is not essential to life and the effects of its removal are not obvious from clinical examination, The role of the spleen in health and disease has not been fully elucidated (organum plenum mysterium tLatin) = organ full of mystery (Galen)). However, the spleen is known to have the following functions.
FIg. 40.1 A central trabecular artery passing thmugh the white pulp into the surrounding red pulp. A blood flow skimming effect results in most of the plasma passing down branches of the artery while the cells pass in the central trabecular artery directly to the red pulp.
Response to antigenic challenge. There is a proliferation of Tlymphocytes within the lymphatic sheaths, and antibody-forming B-lymphocytes within the lymphatic nodules, This results in increased production of humoral immune factors of both B- and T-cell origin: antibody (especially 1gM), luftsin (a peptide which stimulates phagocytosis by neutrophils), opsonins (opaonein (Greek) to prepare food for) (antibodies and other proteins which react with bacteria and fungi to make them more susceptible to phagocytosis), properdin (an immunoglobulin, found in unchallenged animals which have not formed antibody, that fixes complement to bacterial and fungat surface polysaccharides before phagocytosis), and interferon (a glycoprotein which exerts an antiviral effect by stimulating killer-cell/ macrophage activity). Splenectomised patients develop decreased levels of all these factors, and this reduces resistance — in particular to encapsulated bacteria. Twenty-four hours after production in the spleen, 75 per cent of neutrophils either pass to other tissues or are destroyed. Neutropenia in hvpersplenism occurs because of either granulocyte sequestration in the spleen, e.g. in hyperspleniSm~ or splenic destruction of altered granulocytes as in autoimmune neutropeniaS.Destruction of ubnonnafly shaped or rigid red cells by calling and pitting which take place in the red pulp. Culling refers to the filtering and phagocytosis of old red blood cells which have either been damaged or contain inclusions such as
nuclei, nuclear remnants (Howell—Jolly bodies), target cells, siderocytes and spherocytes. Pitting is the removal of certain inclusions, e.g. red blood cell nuclei or malarial parasites from red blood cells, without destroying the cells. The normal red cell lifespan of approximately 120 days is not prolonged after splenectomy because there are other sites of red cell destruction.Phagoctttosis of foreign substances by reticuloendothelial macrophages in the spleen. This is exemplified by the uptake of radio-o a ue thorium into the spleen following administration of the contrast agent thorotrast which was once used in arteriography and cerebral ventriculography. Thorium can be seen in the spleen on plain radiograph 20 years after administration of the thorotrast. Radioactive decay of the thorium over this period can produce splenic fibrosis and hyposplenism. Particulate matter, and bacteria, fungi and protozoa are also removed from the circulation by these macrophages. A similar process of phagocytosiS of abnormal lipoids is the cause of splemc enlargement in the lipoid dystrophies.
Platelet reservoir. The spleen normally sequesters 30—40 per cent of blood platelets. The lifespan of platelets in the circulation is about 10 days. in splenomegaly. up to 80 per cent of the platelet pool can be sequestered in the spleen and this, together with accelerated platelet destruction, can result in thrombocytopenia. Platelet phagoqtosis is a normal function of the spleen but in conditions such as idiopathic thrombocytopenic purpura it is accelerated. In some animals, but not in humans, the spleen also contains a reserve of red cells which can be released into the circulation following a hypoxic stimulus.Erythrocyte production. Red blood cells are normally produced inthe fetal spleen from the fourth month of development until birth. Erythropoiesis does not take place in the spleen after birth unless marrow production of red cells is detective, e.g. in myelotibrosis.
Investigation of the spleenConditions that cause splenomegaly can often be diagnosed by history, and physical and laboratory examination, e.g. a haemolytic anaemia is detectable by full blood count, reticulocyte count and tests for haemolysis. Similarly, splenomegaly associated with portal hypertension caused by hepatic cirrhosis is diagnosed by the physical signs of liver dysfunction, abnormal liver function tests and evidence of oesophageal varices. Many conditions that cause splenomegaly also cause lymphadenopathY. The cause of the splenomegsly should then be determined from investigations for diseases known to cause splenomegaly and lymphadenopathy — possibly including a lymph node biopsy. There are also more direct methods of investigating the spleen:
Plain radiograph. The spleen may be visible as a soft tissue shadow in plain films of the upper abdomen. This finding, repeated at intervals, is evidence that the spleen is not ruptured. Calcification in the spleen may suggest an old infarct or a hydatid cyst. Multiple areas of calcification suggest splenic tuberculosiS

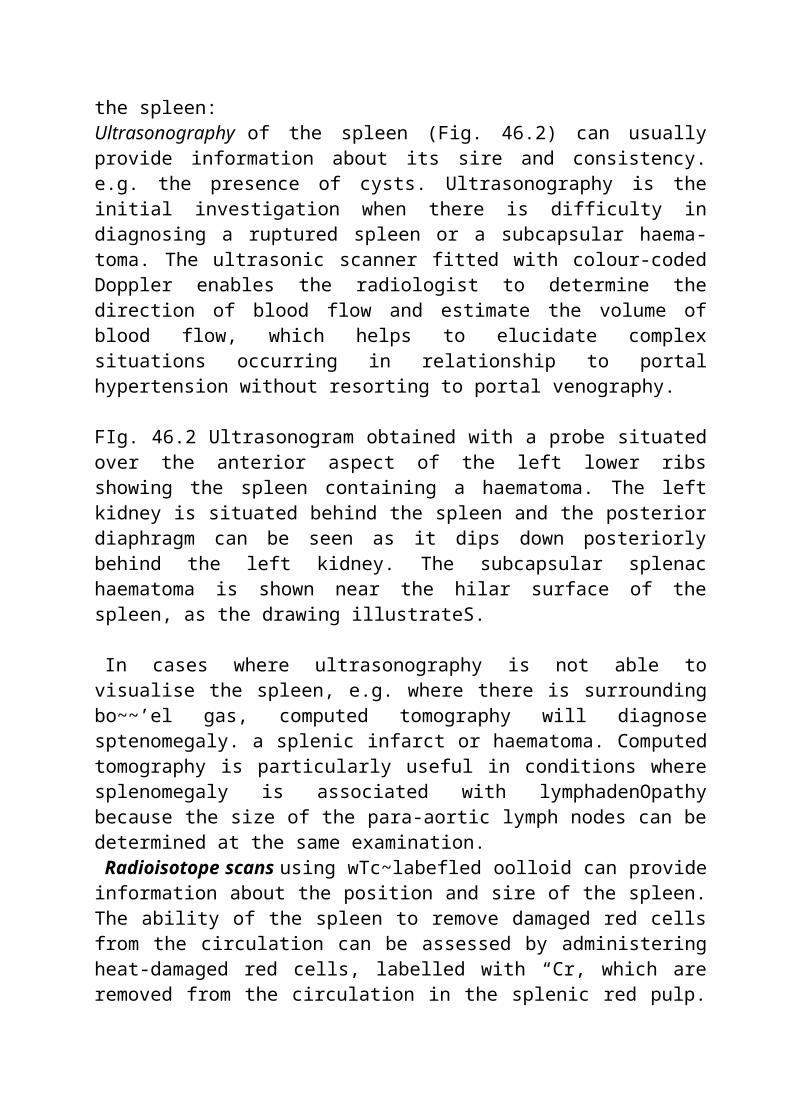
Scanning. There are various techniques for scanning the spleen:Ultrasonography of the spleen (Fig. 46.2) can usually provide information about its sire and consistency. e.g. the presence of cysts. Ultrasonography is the initial investigation when there is difficulty in diagnosing a ruptured spleen or a subcapsular haematoma. The ultrasonic scanner fitted with colour-coded Doppler enables the radiologist to determine the direction of blood flow and estimate the volume of blood flow, which helps to elucidate complex situations occurring in relationship to portal hypertension without resorting to portal venography.
FIg. 46.2 Ultrasonogram obtained with a probe situated over the anterior aspect of the left lower ribs showing the spleen containing a haematoma. The left kidney is situated behind the spleen and the posterior diaphragm can be seen as it dips down posteriorly behind the left kidney. The subcapsular splenac haematoma is shown near the hilar surface of the spleen, as the drawing illustrateS.
In cases where ultrasonography is not able to visualise the spleen, e.g. where there is surrounding bo~~’el gas, computed tomography will diagnose sptenomegaly. a splenic infarct or haematoma. Computed tomography is particularly useful in conditions where splenomegaly is associated with lymphadenOpathy because the size of the para-aortic lymph nodes can be determined at the same examination.
Radioisotope scans using wTc~labefled oolloid can provide information about the position and sire of the spleen. The ability of the spleen to remove damaged red cells from the circulation can be assessed by administering heat-damaged red cells, labelled with “Cr, which are removed from the circulation in the splenic red pulp. Administration of platelets labelled with 1131n provides similar information about the sequestration of platelets in the spleen.
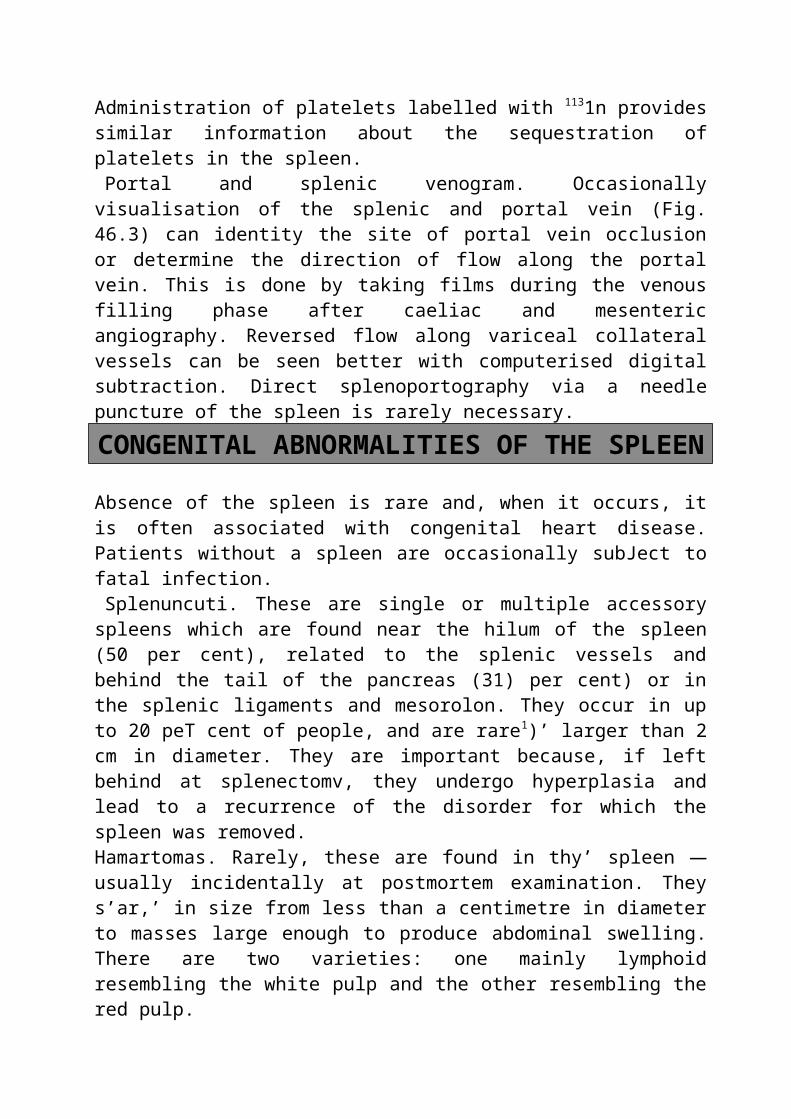
Portal and splenic venogram. Occasionally visualisation of the splenic and portal vein (Fig. 46.3) can identity the site of portal vein occlusion or determine the direction of flow along the portal vein. This is done by taking films during the venous filling phase after caeliac and mesenteric angiography. Reversed flow along variceal collateral vessels can be seen better with computerised digital subtraction. Direct splenoportography via a needle puncture of the spleen is rarely necessary.
CONGENITAL ABNORMALITIES OF THE SPLEEN
Absence of the spleen is rare and, when it occurs, it is often associated with congenital heart disease. Patients without a spleen are occasionally subJect to fatal infection.
Splenuncuti. These are single or multiple accessory spleens which are found near the hilum of the spleen (50 per cent), related to the splenic vessels and

behind the tail of the pancreas (31) per cent) or in the splenic ligaments and mesorolon. They occur in up to 20 peT cent of people, and are rare1)’ larger than 2 cm in diameter. They are important because, if left behind at splenectomv, they undergo hyperplasia and lead to a recurrence of the disorder for which the spleen was removed.Hamartomas. Rarely, these are found in thy’ spleen — usually incidentally at postmortem examination. They s’ar,’ in size from less than a centimetre in diameter to masses large enough to produce abdominal swelling. There are two varieties: one mainly lymphoid resembling the white pulp and the other resembling the red pulp.
Fig. ~.3 Venous phase of a selective mesenteric angiogram. The superior mesenteric vein (SM’.’) and portal vein (P’~O are filled with contrast. Due to portal hypertension abnorma~ retrograde flow has occurred with flow from the portal vein via the coronary vein (LCV) adjacent to the stomach into oesophageal varices (DV) running up the lower part of the oesophagus.
Splenic cysts. Non-parasitic cysts are rare. They consist of true cysts formed from embryonal rests and include dermoids and mesenchymal inclusion cysts, or false cysts resulting from trauma which contain seroua or haemorrhagic fluid.
RUPTURE OF THE SPLEEN
Splenic rupture should be suspected after any trauma, but particularly if there had been direct injury to the left upper quadrant of the abdomen from any angle. Occasionally, a fall without direct trauma to the trunk can rupture the spleen, especially if it is diseased or enlarged, e.g. in infectious mononucleosis or malaria. Advantage was once taken of the fragility of the enlarged spleen in Far Eastern countries where malaria is endemic. Murderers could achieve their purpose by digging a victim beneath the left ribs with a weapon known as a larang; the enlarged malarial spleen would rupture easily. A splenic injury should be suspected if there are fractures of the overlying ribs. Iatrogenic rupture remains common, and is a reminder of the need for care when dissecting in the left upper quadrant of the abdomen, especially if adhesions are present.
Cases of ruptured spleen may be divided into three groups.The patient succumbs rapidly, never rallying from the initial shock. This type is
comparatively rare in temperate climates. Tearing of the splenic vessels and complete avulsion of the spleen from its pedicle give rise to rapid blood loss which can be fatal within minutes.
Initial shock; recovery from shock; signs of a ruptured spleen: these are the usual signs seen in surgical practice. After the initial shock has passed off, there
are signs which point to intra-abdominal bleeding.General signs of internal haemorrhage are variable. Perhaps the most helpful
are increasing pallor, a rising pulse rate, sighing respiration and restlessness. -Local signs.I. Abdominal guarding is present in more than 50 per cent of cases; it is most
pronounced in the left upper quadrant.2. Local bruising and tenderness in the left upper abdominal quadrant.3. Abdominal distension commences about 3 hours after the accident, and is due
to the irritative effect of the intraperitoneal blood which produces peritonism and ileus.
4. Kehr’s sign is pain referred to the left shoulder. There may be hyperaesthesia in this area. This sign can often be demonstrated a quarter of an hour after elevation of the foot of the bed. It is due to blood itt contact with the undersurface of the diaphragm, the pain being mediated through afferent fibres in the phrenic nerve.
5. Shifting dullness itt the flanks is often present.6. Rectal examination frequently reveals tenderness and sometimes a soft
swelling, due to blood or dot in the rectovesical pouch.
Ballance’s sign is positive in about 25 per cent of cases. There is a dull note in both flanks, but on the right side it can be made to shift, whereas on the left it is constant. The interpretation is that there is blood in the peritoneal cavity, but the blood in the neighbourhood of the lacerated spleen has coagulated.
Despite these traditional signs, continued blood loss from bleeding vessels on the surface of the torn spleen is hard to diagnose. Continued observation, noting a fullness in the upper abdomen and minimal tenderness arouse suspicion, especially in the presence of a decrease in urine output despite adequate fluid replacement.
The delayed type of case. After the initial signs have passed off, the symptoms of a serious intra-abdominal catastrophe are postponed for a variable period up to 15 days. or even more. As a rule it is only a matter of minutes to an hour or so, during which time the patient often appears to have recovered from the blow. Thus a rugby footballer may continue to play after a short rest, only to collapse later from internal haemorrhage. The cause of the delayed haemorrhage is local vasoconstriction with or without the formation of blood clot which seals the tear. The causes of the haemorrhage are those of reactionary or secondary haemorrhage.
Investigation. tjltrasonography of the spleen is the investigation of choice where there is difficulty in making a diagnosis of splenic rupture. The spleen can usually be visualised and a surrounding haematoma may suggest rupture (Fig. 4s.2). Serial examinations, by showing a change in splenic size, can identify an
enlarging subcapsular haematoma.A normal, well-outlined spleen on plain radiograph of the upper abdomen is a
reliable sign of an intact spleen. The radiological signs of splenic rupture are:1. Obliteration of the splenic outline.2. Obliteration of the psoas shadow.3. Indentation of the left side of the gastric air bubble.4. Fracture of one of more lower ribs on the left side (present in 27 per cent of
cases).5. Elevation of the left side of thc diaphragm.6. Free fluid between gas-filled intestinal coils.
If doubt persists computed tomography taking 5 mm cuts through the spleen will enable an accurate diagnosis to he made.
Treatment of rupture’ of the’ spleenImmediate laparotomy and splenectomv is the only reliable course. Blood is evacuated and, after injury to other viscera has been excluded, the abdomen is closed. When the organ is damaged by a stab wound or missile penetrating the left pleural cavity, access to the spleen is best obtained by excising the thoracic and diaphragmatic wounds, and enlarging the opening in the diaphragm. Blood transfused should be as required. In the management of splenic trauma, lifesaving control of haemorrhage is the prime concern but with experience control of the haemorrhage can be achieved in conjunction with splenic preservation. This is now almost mandatory in children.
After splenectomy long-term antibiotic protection should be given (see also under Splenectomy).
Rupture of a malarial spleen. As has been mentioned, in tropical countries this is a frequent catastrophe. The delayed type of rupture (following a trivial injury) is also very common, and the patient is admitted with a perisplenic haemat,ma. 11 splenectomy can be performed before the haematoma bursts into the general peritoneal cavity, the prognosis is less grave. Enlarged spleens from any cause can rupture spontaneously or with mild trauma.
The operation is considerably’ more difficult than in the case of a ruptured normal spleen. Surgeons with tropical experience have surmounted these difficulties by ligating the splenic vessels as they run along the superior border of the body of the pancreas (Fig. 46.4), before disturbing the haematoma (Andreasen) (and see below).
Fig. 46.4 Usual position of a splenic aneurysm.
ANEURYSM AND INFARCTION
Aneurysm of the splenic artery. This is an uncommon condition; estimates of its incidence at postmortem examination vary between 0.04 per cent and 1 percent. Whereas aneurysms of other arteries are more common in men, in the splenic artery they are about twice as common in women. They are usually single and situated on the main trunk of the splenic artery (Fig. 46.4), but more than one is found in a quarter of cases.
The aneurysm is symptomless unless it ruptures. Occasionally it is palpable in the epigastrium or associated with a bruit over the left hypochondriuns. It may be discovered accidental], on plain radiograph of the upper abdomen, as a calcified ring situated to the left of the first lumbar vertebra. Rupture of the aneurysm is unsuspected in about half of all cases; it bursts into the peritoneal cavity and the symptoms resemble those of splenic rupture. Nearly half of alt cases of rupture occur in patients less than 45 years of age, and a quarter of all cases are in pregnant women (usually’ in the last trimester of pregnanc-v or actually in labour).
The treatment of choice is splenectomv and removal of the length of artery bearing the aneurysm. If the aneurysm has eroded into the pancreas or is close to the origin of the splenic artery, then proximal and distal ligation of the sac is usually followed by thrombosis in the aneurysm. In younger patients, particularly women, with an asymptomatic splenic artery aneurysm, surgical treatment is indi-cated after the diagnosis has been confirmed by selective coeliac arteriography. The maternal mortality rate for surgery at the time of rupture, in late pregnancy, is over 70 per cent. In elderly patients, particularly men, where an asymptomatic calcified aneurysm is detected on plain radiograph, there is less risk of rupture and surgery is not indicated.
Infarction of the spleen (Fig. 46.5). This occurs in patients with massive spleens resulting from a myeloproliferative syndrome, or with vascular occlusion produced by sickle-cell disease or an embolus from an infected heart valve in bacterial endocarditis. The infarct may be asymptomatic or may cause left upper quadrant abdominal pain radiating to the left shoulder with splinting of the left hemidiaphragrn, guarding, and at times a friction rub heard over the splenic area. Sedation and bed rest are sufficient, except rarely’ when a septic infarct causes an abscess necessitating splenectomy.
Fig. 4&5 Infarct of the spleen.
ENLARGEMENT OF THE SPLEEN
The spleen is a meeting place of medicine and surgery. Table 46.1 summarises
the many causes of enlargement of the organ.
In connection with Table 46.1, the following points should be noted. In idiopathic thrombocytopenic purpura the spleen, although somewhat enlarged, is seldom palpable. In psittacosis the enlarged spleen can be palpated regularly’ after the first few days of the illness; this enlargement is helpful to differentiate the condition from other varieties of pneumonia. In portal hypertension the spleen is enisrged secondars to hepatic cirrhosis or portal vein thrombosis
Table 48.1 Causes of enlargement of the spleen
‘ Typhoid and paratyphoidTyphusAnthraxTuberculosistSepticaemiaAbscess of the spleen*Wail’s diseaseInfectious mononucleosis
I Psittacosis alariahistosomiasis (Egyptiansplenomegaly)tTrypanosomiasisla-azardatid Cyst’
Tropical splenomegalytBacterial
Spirochaetal1. Infective Viral2. Blood
diseasesRicketsAmyloid
3. MetabolIcPorphyriaGaucher’s diseas4 (Chapter 45)lfrt 4 infective endocarditis*nac Mitral stenosis
4. Circulatory Portal hypertension (Chapter 45)
Occlusion of Thrombophlebitistthe portal vein Neoplastic, e.g.
carcinoma of tall of pancrea4
I Still’s disease (Chapter 19)Felty’s syndromet (Chapter 46)
{ CangenitalAquired’Angioma
7. Neorlastic Hodgkin’s lymphoma* (Chapter 13) Primary fibrosarcomaOther lymphomas~
* Benefited by splenectomy. t Often benefited by splenectomy.* Splenectomy sometimes indicated.
(Chapter 45). As emphasised in Table 46.1, not all causes of splenomegaly will require splenectomy as part of their treatment. Elective splenectomy is required to treat haematological disease with medically uncontrolled hypersplenism; occasionally to stage and diagnose lymphoma; to treat splenic cysts, tumours and abscesses; and for the relief of discomfort associated with giant splenomegaly.
Myelofibrosis*Acute IeukaemiaChronic leukaemia (Iymphocytic or granulocytic)1:Pernicious anaemiaPolycythaemia veraErythroblastosis fetalisHereditary spherocytosis’Autoimmune haemolytic anaemiatIdiopathic thrombocytopenic purpuraMediterranean anaemia (thalassaemia)*Sickle-cell disease*Idiopathic thrombocytopenic* purpura (ITP)Purpura. Not all cases of purpura (purpura = porphyra (Greek) = purple) benefit from splenectomy’. Purpura is defined as a focal haemorrhage into the skin. A history of purpura and evidence of it on examination should be sought before any surgical procedure is undertaken. Purpuca may result from:
1. Increased capillary fragility, as in steroid-induced or Henoch— SchOnlein purpura.
2. Defective platelets (thrombocytopathies), for example, after taking aspirin which inhibits thromboxane and prostaglandin and reduces their property’ of making the platelet adhesive.
3. A reduced number of normal platelets (thrombocytopenia). This can be a consequence of;
(a) decreased platelet production by marrow megakaryocytes, for example. because of marrow suppression by cytotoxic chemotherapy. or in aplastic anaemia;
(b) increased platelet consumption, as is seen in disseminated intravascular coagulation where the clotting cascade is triggered by septicaemia and platelets adhere to vascular endothelium. or in a large haemangioma in which platelets adhere to the abnormal endothelium;(c) increased platelet destruction by the spleen. This may be assodated with autoimmune disease, e.g. systemic lupus erythematosus; with drug reactions, for example, to quinine; and with certain infections. e.g. mononucleosis. Alternatively, as in idiopathic thrombocvtopenic purpura, the platelet destruction may not be associated with any other condition;
(d) increased splenic sequestration of platelets. This can be assodated with any condition that produces gross splenic enlargement, e.g. portal hypertension.
Splenectomy may sometimes be helpful in purpura associated with splenic destruction or sequestration (3c and 3d, above). It is most reliably of use in idiopathic thrombocytopenic purpura.
Aetiology of lIP. In most cases the low platelet count in lIP is due to the development of antibodies which damage the patient’s own platelets (the normal blood-platelet count is 250 000-400 000 per mm’ (250—400 x 10’!l)). Transfused platelets have a short surs’ival time after transfusion into patients with ff1’, and the children born to mothers with IT? may have a temporary, maternal antibody-induced thrombocytopenia after birth.
Clinical features. Purpuric patches (ecchymoses) occur in the skin and mucous membranes which tend to be more prominent in dependent areas because of a higher, gravity aided, intravascular pressure. A tendency to spontaneous bleeding from mucous membranes, e.g. epistaxis, and in women to menorrhagia, and prolonged bleeding from minor wounds is common. Urinary and gastrointestinal haemorrhage, and haemarthrosis are rare. Intracranial haemorrhage is also rare, but is the most frequent cause of death. Cutaneous ecchymoses may be found on examination and the tourniquet test is positive. The spleen is palpable in only 25 per cent of cases, and gross splenic enlargement suggests that the diagnosis is not ITP.
Investigations. The bleeding time is increased but the clotting and prothrombin times are normal. The platelet count in the peripheralblood film is reduced (usually less than BOX 10~/l). Examination of a bone marrow biopsy reveals a plentiful supply of platelet-producing megakaryocytes (the giant cells of bone marrow give origin to blood platelets).
Treatment. The behaviour of the disease is different in children and adults. In children, the disease regresses spontaneously in 75 per cent of cases after one attack.., Short courses of corticosteroids or occasionally azathioprine are usually
followed by recovery. Splenectomy is reserved for severe cases who have relapsed or girls approaching menarche. In adults, the initial attack is less severe than in children, but the disease relapses and becomes more severe. Splenectomy is indicated where the ITP has persisted for more than 6—9 months.
Sixty per cent of patients can be regarded as cured, 20 per cent will be improved and 15 per cent or more will derive no benefit from the splenectomy. It is often, though not invariable, that a response to steroids predicts a good response to splenectomy. If severe bleeding has not been controlled by steroids, fresh blood transfusion or transfusion with platelet concentrates before operation is necessary. Splenectomy is contraindicated during the acute phase of ITP; the disease should first be controlled by medical treatment. Occasionally, in resistant cases, the antiplatelet immune response can temporarily be blocked by IgG transfusion to saturate the spleruc Fc binding sites and reduce platelet destruction to allow the platelet count to rise at the time of surgery.
Splenectomy for other causes of thrombocytopenic purpura. Occasionally, splenectomy is of benefit in thrombocytopema due to systemic lupus erythematosus and in hypersplenism; also in purpura associated with 3c and 3d above.
SPLENECTOMY IN THE HAEMOLYTIC ANAEMIAS
There are five causes of haemolytic anaemia which are amenable to splenectomy:1. Hereditary spherocytosis.2. Hereditary elliptocytosis.3. Pyruvate kinase deficiency.4. Thalassaemia.5. Acquired autoimmune haemolytic anaemia.
Hereditary spherocytosisThe essential lesion is an increase in permeability of the red cell membrane to sodium. As the sodium leaks into the red cell its osmotic pressure rises, it swells and becomes more spherical and in consequence more fragile. The mechanism by which the cell rids itself of sodium — the sodium pump -. has to work harder. This has two consequences: (1) there is greater loss of membrane phospholipid and so a weakening of the membrane which thus becomes more fragile, and (2)the energy and the oxygen requirements increase. These requirements are particularly difficult to satisfy in the spleen where there is a deficiency of both glucose and oxygen. Thus a large number of red cells are destroyed in the spleen, and splenectomy reduces this cell destruction. Splenectomy does not, of course, cure the congenital red cell membrane defect but it lessens the anaemia and
makes the red cell survival time normal. The defect is transmitted by either parent as a Mendelian autosomal dominant (in 1866 Mendel described ‘dominant’ and ‘recessive’ traits in hybrids; his work passed unnoticed for 35 years). Males and females are equally affected.
The circulating bilirubin is not conjugated with glycuronic acid. It is attached to albumin and is not excreted in the urine (acholuric jaundice). (Although there is excessive breakdown of red cells with transformation of liberated haemoglobin to bilirubin, the bilirubin compound so produced is excreted by the liver and not by the kidneys, thus favouring the formation of pigment gallstones.)
Clinical features. Once the disease manifests itself, spontaneous remissions are almost unknown. As a rule the patient is pale and has jaundice. In established cases lassitude and undue fatigue are present, but they vary with the amount of haemolysis.
Sometimes the patient is born jaundiced or becomes so early in life. In certain families the disease is characterised by severe crises of red blood cell destruction; thus, with the onset of a crisis, an erythrocyte count may fall from 4½ millions to 1½ millions in less than a week. Such crises are characterised by the sudden onset of pyrexia, abdominal pain, nausea, vomiting and extreme pallor, followed by increased jaundice. These crises may be precipitated by acute infection, and can be so severe as to cause death in infancy or childhood. More usually the jaundice, although variable, is very mild, and may not appear until adolescence or even adult life. In adult cases there is often a history of attacks of gallstone colic; indeed, 68 per cent of untreated patients over the age of 10 years have pigment stones in the gallbladder. Every child with gallstones should be investigated for evidence of hereditary spherocytosis and enquiry should be made among relatives of patients with spherocytosis for evidence of similar disease.
On examination the spleen is large, and in thin subjects it can be palpated easily. Sometimes the liver is also palpable. Chronic ulcers of the legs can occur in adults with the disease.
Haematological investigations. The fragility fesf. Increased fragility of erythrocytes characterises this disease. Normally, erythrocytes begin to haemolyse in 0.47 per cent saline solution. In this condition haemolysis occurs in 0.6 per cent or even in stronger solutions.The reticulocyte count. To compensate for the loss of erythrocytes by haemolysis, the bone marrow discharges into the circulation immature red cells, which differ from the adult cells by possessing a reticulum,Faecal urobiliaogen is increased, as most of the urobilinogen is excreted by this route.
Use of radioactive chromium. Labelling of the patient’s own red cells with 51Cr will demonstrate the severity of red cell destruction and if this is accompanied by daily scanning over the spleen it will show the degree of red cell sequestration by the spleen. If splenic radioactivity is high, splenectomy will be of value.Treatment. All patients who have hereditary spherocytosis should be treated by
splenectomy. In juvenile cases the age at which operation is recommended has been decreasing. If it is not imperative before, the optimum time seems to be about 7 years, i.e. before gallstones have had time to form, but subsequent vulnerability to infection is reduced. Ultrasonography should be performed preoperatively to determine the presence or absence of gallstones.
Acquired autoimmune haemolytic anaemiaThis may be due to a drug reaction, e.g. to a-methyldopa, to another disease, e.g. systemic Iupus erythematosus, or its cause may be unknown. Red cell survival is reduced because of an immune reaction triggered by immunoglobulins or complement on the red cell surface. The red cell surface is damaged as a result of the binding of the Sc portion of the red cell antibody to a macrophage Fc receptor in the spleen. The red cell is thus rendered vulnerable to ‘culling’ within the splenic red pulp.
Clinical features. Autoimmune haemolytic anaemias are more common after the age of 50, and in women. The spleen is enlarged in 50 per cent, and pigment gallstones are present in 20 per cent of cases.
Investigations. Anaemia is invariably present and may be associated with spherocytosis because of red cell membrane damage. The Coombe’ test is usually but not invariably positive.
Treatment. Usually the disease has an acute, self-limiting course and no treatment is necessary. Splenedomy should be considered if:
I. Corticosteroids are not effective.2. The patient is developing complications from long-term steroid treatment.3. Corticosteroids are contraindicated, e.g. because of a history of peptic
ulcer. Eighty per cent of patients respond to splenectomy.
Thalassaemia~ (syn. Cooley’s anaemia; Mediterranean anaemia)Thalassacrnia is the result of a defect in haemoglohin peptide chain synthesis which is transmitted as a dominant trait. The disease is really a group of related diseases — a, ~ and y — depending on the haemoglobin peptide chain whose rate of synthesis is reduced. Most patients suffer from ~-thalassaemia in which a reduction in the rate of ~ chain synthesis results in a decrease in haemoglobin A. In addition to a decrease in haemoglobin, intracellular precipitates (Heinz bodies) contribute to premature red cell destruction. The disease is no longer thought to be confined to the descendants of those living around the Mediterranean. Thalassaemia = Greek Lhulassa. sea. (Because it was originally thought to he restricted to people of Mediterranean origin.)
Clinical features. Gradations of disease range from heterozyg~us thalassaemia minor to homozygous thalassaemia major which is associated with chronic anaemia, jaundice and splenomegaly. Patients with homozygous thalassaemia major frequently develop clinical signs within the first year of life: retarded growth, enlarged head with slanting eyes and depressed nose, leg ulcers, jaundice
and abdominal distension (due to splenomegaly).Investigations. Red cells are small, thin and misshapen, and have a characteristic
resistance to osmotic Iysis. In the more severe forms, nucleated red cells and other immature blood cells are seen. The final diagnosis is by haemoglohin electrophoresis.
Treatment. Blood transfusion may be necessary to correct profound anaemia. Splenectomy is occasionally of benefit in patients who require frequent blood transfusion — particularly if they have developed haemolytic antibodies from repeated transfusion — and where the bulky spleen is uncomfortable or painful.
Sickle-cell diseaseSickle-cell disease is a hereditary haemolytic anaemia, occurring mainly among those of African origin, in which the normal haemoglobin A is replaced by haemoglobin S (HbS). The HbS molecule crystallises when the blood oxygen tension is reduced and this distorts and elongates the red cell. This increases blood viscosity and obstructs the flow of blood through both the ‘open’ and ‘closed’ circulations in the spleen, and through other blood vessels. Splenic microinfarcts, splenomegaly and, later, autosplenectomy develop. <Ibis is associated with reduced antibody production and a reduced ~j]jty to filter bacteria — especially Streptococcus pneumoniae — in the spleen.
Clinical features. The sickle-cell trait can be detected in 9 per cent of those of African origin but most are asymptomatic; sickle-cell disease occurs in about I per cent of Africans. Depending on the vessels affected by the vascular occlusion, patients may have bone or joint pain. priapiam. neurological abnormalities, skin ulcers or abdominal pain due to visceral blood stasis.
Investigations. Characteristic sickle-shaped cells can be seen in a blood film, but this has now been replaced by haemoglobin electrophoresis.
Treatment, Hypoxia, which provokes a sickling crisis, should be avoided, and particular care should be taken in patients with sickle-cell anaemia undergoing anaesthesia. Adequate hydration and partial exchange transfusion may help in a crisis. Splenectomy is of benefit in a few patients where excessive splenic sequestration of red cells aggravates the anaemia. This hypersplenism may be chronic, which usually occurs in late childhood or adolescence, or acute, which occurs in the first 5 years of tile and may be precipitated by Streptococcus pneumoniae infection. Acute attacks of hypersplenism can usually be treated with packed red cell transfusion, but occasionally splenectomy is of benefit.
HypersplenismThis is an indefinite term which includes splenic enlargement, any combination of anaemia, leukopenia or thrombocytopenia, compensatory bone marrow hyperplasia and improvement after splenectomy. The vagueness of the definition implies careful clinical judgement between surgeon and haematologist to determine when the long- and short-term risks of splenectomy are less than
continued conservative management.
SPLENOMEGALY
SchistosomiasisThis is prevalent in Africa (particularly around the Nile delta), Asia and South America. It is caused by infection with Schistosoma matzsoni in nearly 75 per cent of cases and by Schistosonta hae,natobiurn in nearly 25 per cent of cases. Splenic enlargement is produced by hyperplasia which is induced by phagocytosis of disintegrated worms, ova and toxins, and by portal hypertension which is the result of hepatic fibrosis.Clinical features. Splenomegaly resulting from schistosomiasis can occur at any age and is more prevalent in males. The degree of splenic enlargement reflects the extent of hepatic fibrosis and may be massive.
Investigations. The urine and the faeces are examined for ox’s, Liver function tests reveal a varying degree of hepatic impairment. A hypochromic anaemia is always present.
Treatment. Successful medical treatment of established cases does not result in regression of the splenomegaly. Removal of the painful and bulky spleen is indicated where there is no evidence of hepatic or renal insufficiency. If ascites is present, a portasystemic shunt should be combined with splenectomy.
Tropical splenomegalyMassive enlargement of the spleen occurs frequently in the tropics, e.g. in malaria (especially in children), kala-azar and schistosomiasis (see above). In parts of Africa and New Guinea splenomegaly cannot be fully attributed to these diseases, because tropical splenomegaly is restricted to only a few adults in areas where malaria is endemic. The most likely explanation is an abnormal immune response to malaria or to unusual species of plasmodia. Malnutrition may also be a factor (there is a high incidence in lactating women).
The spleen is grossly enlarged (2000—4000 g). This is associated with anaemia (due to shortened red cell life) and thrombocytopenia (due to splenic sequestration of platelets) which respond to splenectomy. Splenectomy is indicated for those disabled by anaemia or by the weight of an enormous spleen. Splenectomy reduces immunity to malaria and therefore anti-malarial chemotherapy, e.g. 100 mg proguanil daily for life, should follow splenectomy in malaria endemic areas.
Hypersplenism due to portal hypertension
Splenomegaly invariably accompanies portal hypertension. This splenic enlargement results in thrombocytopenia (due to splenic sequestration of platelets) and granulocytopenia. These are permanently relieved when splenectomy accompanies the operation for relief of the portal hypertension. Shunt surgery alone does not have a similar effect.
Felty’s syndromeA moderate number of patients with chronic rheumatoid arthritis develop mild leukopenia; in a few of these, neutropenia becomes extreme and is usually associated with enlargement of the spleen. This combination is referred to as Felt~s syndrome. A remarkable characteristic of this syndrome is that the leukopenia and splenic enlargement are apparently unrelated to the severity of the arthritic changes; indeed, in some instances the arthritis has commenced to improve or has become quiescent by the time the low white cell count and the splenomegalv become unmistakable. In those cases in which the arthritis is slight but the splenic enlargement and the blood changes are much in evidence, a diagnosis of primary splenic neutropenia is sometimes made. The results of splenectomy are variable. Usually there is an improvement in the blood picture with increased neutrophils, but this improvement is not maintained. However, the liability to infections seems to be decreased in many cases and rheumatoid arthritis that has become resistant to steroid therapy may react favourablx to steroid therapy once more.
Tuberculosis of the spleenTuberculosis of the spleen is not so unc.’mmon as is SOmQtime~ believed. It occurs chiefly in adults between 20 and 40 years of age. When a patient has splenonxegaly with asthenia, toss of weight and an evening temperature, it is well to bear in mind the possibility of the enlargement of the spleen being due to tuberculosis. Too often these signs lead to the erroneous diagnosis of leukaemia or some other disorder for which splenectomy is not indicated. Occasionally tuberculosis of the spleen produces portal hypertension. Another form is cold abscess, which is very rare. Splenic puncture, followed by culture, or guinea-pig inoculation, will yield positive results. A therapeutic test with antituberculous drugs (Chapter 7) brings about some improvement, and there is less danger of dissemination of tuhercle bacilli if splenectomy is undertaken. The operation, which usually is rendered difficult because of adhesions, is contraindicated only if other active tuberculous lesions are present. Otherwise the results of splenectomy in tuberculosis of the spleen are excellent.
NeoplasmsThe most common benign tumour of the spleen is the haemangioma which may occasionally develop into a haemangiosarcoma. Splenectom~’ max’ be necessary. The commonest cause of neoplastic enlargement of the spleen is lymphoma.
Splenectomv mae play a part in the management of these conditions (Chapter 13).
PorphyriaPorphyria is a hereditary error of catabolism of haemoglobin in which porphyrinunia occurs. The abdominal crises, which are charactenised by violent intestinal colic with constipation, are liable to be precipitated by the administration of barbiturates, for which these patients have an idiosyncrasy. The patient is anaemic, frequently suffers from photosensitivity, and in advanced stages of the disease neurological or mental symptoms (from damage to the brain) are often present. On examination the spleen will be found to be enlarged. On a number of occasions the splenic enlargement, which is usually well marked, has been overlooked and the abdomen has been opened on the diagnosis of intestinal or appendicular colic, with negative findings. Another manifestation of acute porphyria is spasmodic abdominal pain followed by jaundice.
Two methods of establishing the diagnosis are ax’ailable.The urine is sometimes normal in colour, Usually it is orange (which is often
dismissed as ‘concentrated). If the specimen is left exposed to daylight for a few hours it develops a port-wine colour, particularly near the surface, where it is exposed to the air. There arc several conclusive laboratory tests for porphvrinunia.
Radiography of the abdomen. Serial radiographs show areas of intestinal spasm causing short segments of gaseous dilatation of the small and large intestine, especially of the caecum.
Treatment. Often there is a striking decrease in the serum sodium level and the patient is improved considerably by infusion of isotonic saline solution with careful control of electrolytic balance. To relieve the abdominal pain methadone is the best drug. If a sedative is required, one’ uf the phcnothiazines, e.g. ch!orpromazine. should he given. Splenectomv is not of value e\cept in the uncommon ervthrcpoietic type with splenomegaly.
Gaudier’s diseaseAs mentioned, the spleen may take an active part in the storage of abnormal lipoids, as does the remainder of the reticuloendothelial system. In the case of Gaucher’s disease the Iipoid in question is glucocerebroside. Gaucher’s disease, which is rare, is characterised by enormous enlargement of the spleen, which may weigh S or 9 lb (3.6 to 4.1 kg). In most cases the splenic enlargement begins in early childhood, often before the age of 12, although the patient rarely seeks advice before adult life, Until the splenic enlargement becomes massive the symptoms are few. There is anaemia, a yellowish— brown discoloration of the skin of the hands and face, and a curious conjunctival thickening (pinguecula) that helps to clinch the clinical diagnosis. Slavonic and ]ess’ish races appear to be more prone to the disease than the rest of humanity. The diagnosis is confirmed
by finding Gauchers cells in the bone marrow.Treatment. Splenectomy rids the patient of a large abdominal swelling. but the operation is difficult because of perisplenitis and friability of the splenic pulp. It does not greatly influence the course of the disease hut because it reduces the hypcrsplcnism (anaemia, leukopenia and thromhocytopenia) and makes the patient more comfortable it may he indicated.
LeukaemiaLeukaemia is one of the conditions to be considered in the differential diagnosis of splenomegaly. The diagnosis can be made by examination of a blood or marrow film. The main treatment is chemotherapy or radiotherapy; occasionally marrow transplantation is necessary. Sptenectomv during the chronic phase of chronic granulocytic leukaemia will not reduce the incidence of blastic transformation or improve survival, The procedure should be reserved for hypersplenism occurring during the chronic phase, or for when bone marrow transplantation might be necessary. In rare instances the removal of a symptomatic enlarged spleen during the blastic phase produces relief but the period of relief is brief and the operation is hazardous,Splenectonay is occasionally indicated for palliation of a painful bulky spleen in chronic lymphocytic leukaemia, but only after consultation with an experienced haematologist
Abscess of the spleenIf a splenic embolus is infected, and the primary condition does not prove fatal, a splenic abscess mae be expected to follow. Other sources of metastatic abscesses of the spleen are typhoid and paratvphoid fever, osteomvelitis, otitis media and puerperal sepsis. An abscess in the upper pole of the spleen may rupture and form a left subdiaphragmatic abscess, If the abscess is in the lower pole, rupture results in diffuse peritonitis.Treatment. As a rule, owing to dense adhesions, drainage of the abscess is the only course. Very rarely, splenectomy may be possible with the abscess in sits. The drainage may be performed percutaneously under ultrasonographic or computed tomographic guidance, so avoiding operative intervention.
SPLENECTOMY
The usual indications for splenectomy are:1. Trauma — either following an accident or during a surgical operation, e.g.
when mobilising the splenic flexure of the colon,2. Removal en bloc with the stomach as part of radical gastrectomy.3. Removal as part of the staging laparotomy undertaken before treatment of
Hodgkin’s Ivmphoma, a very rare indication with the improvement of staging by imaging.
4. To reduce the anaemia or thrombocytopenia in spherocytosis, idiopathic thrombocytopenic purpura or hypersplenism.
5. In association with shunt or variceal surgery for portal hypertension.
Other indications for splenectomy are given in Table 46.1.Technique of splenectomy. Most surgeons use a left paramedian or transverse
left subcostal incision. For large spleens adherent to the diaphragm a thoracoabdominal incision may be necessary. Before operation, the passage of a nasogastric tube enables the stomach to be emptied. This eases the identification of the abdominal oesophagus and decompresses the stomach during the procedure; however, it should be removed at the end of the operation.
If the operation is for traumatic rupture, a quick mobilisation is necessary. The hand is passed round the Outer surface of the spleen, the posterior layer of lienorenal ligament (Fig. 46.6) divided largely by blunt dissection, and the spleen rotated medially into the incision. A large pack is inserted and the short gastric vessels and those in the pedicle are ligated and divided, It is important to separate tho tail of the pancreas from the vessels in the hilum before ligation (see helo ‘ and Malarial spleen, above).
Fig. 406 From the surgical standpoint, the spleen may be said to have two pedrcles the gastrosplenic ligament and the lienorenal ligament The splenrc artery and vein lie in the latter.
For othe conditions requiring splenectomv, the first step is to open th~ gastrosplenic ligament and divide the short gastric vessels (Fig. 45 6) lb1. splenic vessels at the superior border of the pancreas are underrc.n with \ rcnl arid ligated. The posterior surface of the splee-t is exposed the posterior leaf of the lienorenal ligament divided by long curved scissors, and the spleen rotated medially, together with the tail and body of the pancreas. The pancreas is separated from the hium and the vessels dissected Out, ligated and divided. A careful search must be made for accessory spleens. The wound should not be drained, as haemostasis must be perfect before closure of the abdomen.
Postoperative complications.1. Haemorrhage, if a ligature slips off the splenic artery.2. Canine dilatation following partial mobiisation of the stomach when ligating
the short gastric vessels.3. Haematemesis may rarely occur — possibly due to mucosal damage to the
stomach when ligating the short gastric vessels.4. Left basal atelectasis, sometimes with a pleural effusion, is common. This
may be due to damage to or irritation of the left hemidiaphragm or subphrenic abscess, and may be accompanied by persistent hiccough.
5. Damage to the tail of the pancreas during mobilisation of the splenic pedicle. This may produce a localised abscess or, if the area has been well drained, a pancreatic fistula, This may be associated with a left pleural effusion, a peritoneal effusion or abdominal wound dehiscence,
6. Splenectomy is frequently followed by a rise in the white cell and platelet count a few days after the operation. There ma1y be a risk of thrombosis if the platelet count rises to above 1000 x 10 /1 and it is essential to anticoagulate the patient.
7. Canine fistula due to damage of the greater curvature when ligating the short gastric vessels,S.
Postsplenectomy septicaemia. The spleen phagocytoses bacteria, particularly encapsulated bacteria. Splenectomised patients show reduced antibody production when challenged with particulate antigens, are deficient in tuftsin and may have reduced 1gM and properdin levels (see Functions, above). Splenectomised patients are at increased risk of septicaemia due to Strepfocstccus pneunicrni4e, t4eissefia mernngitidis, Hae,nophilus inflzsenzae, and Babesia microti. The risk becomes ever-bigger in splenectomised patients treated with cytotoxic chemotherapy or radiation, and in patients who have undergone splenectomy for thalassaemia, sickle-cell disease, and autoimmune anaemia or thrombocytopenta.Opportunist postsplenectomy infection (OPSI) is now of major concern.
Antibiotic prophylaxis (e.g. amoxidllin) is recommended in the first 2 years after spleriectomy. and in children until the age otiS years. l’neumococcal antitoxin (Pneumovax) should be given 2 weeks preoperatively. It is important to ads’ise the patient of the dangers of OPSI, and to prescribe antibiotics with all infections. Splenectomised patients who live in malaria endemic areas should receive antimalaria prophylaxis.