Surgical interventions for the early management of Bell's palsy
Upload
rose-weaverCategory
view
219download
0
CH 12Surgical Interventions and
Postoperative Management

Indications for Surgery for Musculoskeletal Disorders of the Extremities and Spine
• Incapacitating pain• Marked limitation of active or passive motion• Gross instability• Deformity• Significant structural degeneration• Chronic joint swelling• Failed conservative or previous surgical management• Significant loss of function leading to disability

GUIDELINESFOR PREOPERATIVEMANAGEMENT
• Benefits of Preoperative Contact with a Patient• Examination and evaluation of impairments and
functional status• Opportunity to identify and prioritize a patient’s needs
and understand a patient’s goals and functional expectations after surgery
• A basis for establishing rapport to after surgery• Patient education about the scheduled surgery and the
components of postoperative rehabilitation

Preoperative Examination and Evaluation
• Pain. level of pain with a visual analog scale or a scale• Range of motion and joint integrity. Active and passive range of motion (ROM). Check the
stability and mobility of joints.• Integrity of the skin. Scars from previous injuries or surgeries, particularly those that are adherent
and restrict mobility of skin.• Muscle performance (strength and endurance). Muscle strength of the affected areas,
recognizing that pain adversely affects strength. Assess the functional strength of unaffected body segments in anticipation of postoperative ambulation with assistive devices, transfers, and activities of daily living (ADL).
• Posture. Identify the patient’s preferred positions for comfort and any postural abnormalities that may affect
• ROM and function.• Gait analysis. Analyze the gait characteristics, type of supportive or protective devices currently
used, and degree of weight bearing tolerated during ambulation.• Note any inequality in leg lengths.• Functional status. Identify the patient’s preoperative functional limitations and abilities and his or
her perception of disability using a quantitative, self-report measurement tool.

Preoperative Patient Education—Methods and Rationale
• Overview of the plan of care• Postoperative precautions• Bed mobility and transfers• Initial postoperative exercises:
– Deep-breathing and coughing exercises.– Active ankle exercises (pumping exercises) – Gentle muscle-setting exercises of immobilized joints.
• Gait training. Supportive devices • Wound care

• Considerations for Postoperative Management

Factors That Influence the Components, Progression, and
Outcomes of a Postoperative Rehabilitation Program• Extent of tissue pathology or damage• Size or severity of the lesion• Type and unique characteristics of the surgical procedure• Patient-related factors
– Age, extent of preoperative impairments, and functional limitations– Health history, particularly use of medications and diabetes– Lifestyle history, including use of tobacco– Needs, goals, expectations, and social support– Level of motivation and ability to adhere to an exercise program
• Stage of healing• Characteristics of tissues involved
– Response to immobilization and remobilization
• Integrity of adjacent structures• Philosophy of the surgeon

Phases of Postoperative Rehabilitation
• Maximum protection phase• Moderate protection phase• Minimum protection/return to function
phase

MANAGEMENT GUIDELINES—Postoperative Rehabilitation: Impairments
• pain • Swelling• circulatory and pulmonary complications• Joint stiffness or limitation of motion• Muscle atrophy• Loss of strength for functional activities• Limitation of weight bearing• Potential loss of strength and mobility in
unoperated joints

MANAGEMENT GUIDELINES-Maximum Protection Phase

MANAGEMENT GUIDELINES-Moderate and Minimum Protection Phase

Potential Postoperative Complications
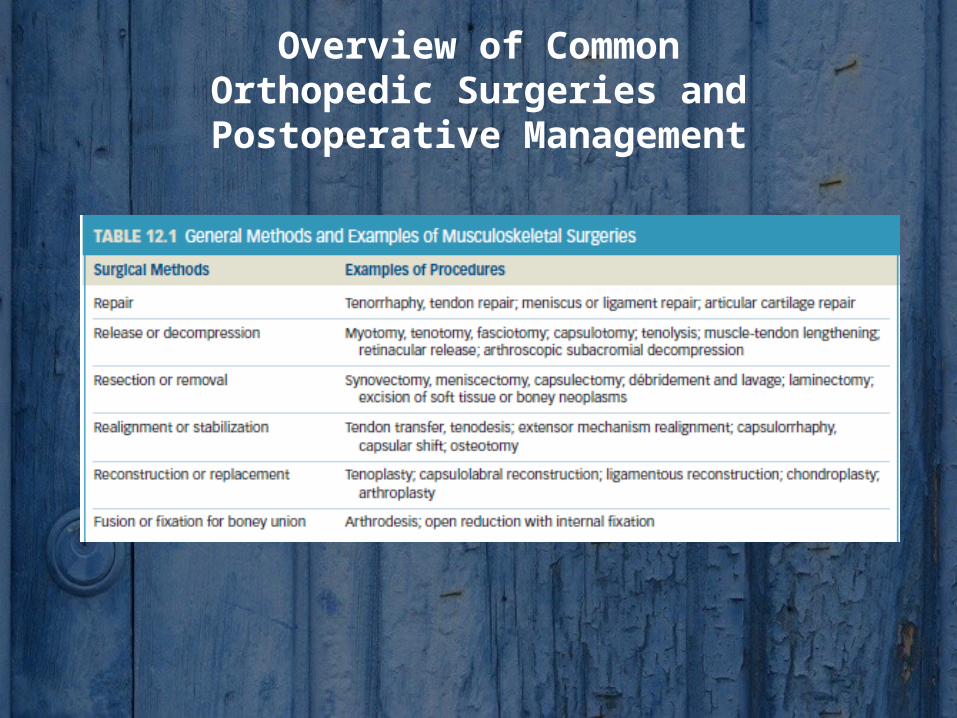
Overview of CommonOrthopedic Surgeries and
Postoperative Management

Surgical Approaches: Open,Arthroscopic, and Arthroscopically
Assisted Procedures• Open ProcedureAn open surgical procedure involves an incision of adequate length and depth
through superficial and deep layers of skin. The term arthrotomy is used to describe an open procedure in which the joint capsule is incised and joint structures are exposed. Open approaches are necessary for surgeries, such as joint replacement, arthrodesis, internal fixation of fractures, and for some soft tissue repairs and reconstruction, such as tendon or ligament tears.
• Arthroscopic ProcedureArthroscopy is used as a diagnostic tool and as a means of treating a variety of
intra-articular disorders. Arthroscopic procedures are typically performed on an outpatient basis and often under local anesthesia. Arthroscopy involves several very small incisions (portals) in the skin, muscle, and joint capsule for insertion of an endoscope to visualize the interior of the joint by means of a camera.

• Miniature, motorized surgical tools are inserted through the portals and are used to repair tissues in or around the joint, remove loose bodies, or débride the join surfaces. Arthroscopic techniques most often are used for surgical procedures at the shoulder and knee. Procedures include ligament, tendon, and capsule repairs or reconstruction, débridement of joints, meniscectomy, articular cartilage repair, and synovectomy
• Arthroscopically Assisted ProcedureAn arthroscopically assisted procedure uses arthroscopy for a portion of the procedure
but also requires an open surgical field for selected aspects of the operative procedure. This sometimes is referred to as a “mini-open” procedure.

Use of Tissue Grafts
• Autograft. An autograft, also referred to as an autogenous or autologous graft, uses a patient’s own tissue harvested from a donor site in the body. Patellar tendon grafts, for example, have been used for more than four decades for intra-articular anterior or posterior cruciate ligament reconstruction
• Allograft. An allograft uses fresh or cryopreserved tissue that comes from a source other than the patient, typically from a cadaveric donor. This type of graft is used when an autograft in a previous surgery has failed.
• Synthetic grafts. Materials such as Gore-Tex® and Dacron offer an alternative to human tissue and have been used for ligament reconstruction in the knee. Implantation of synthetic ligaments has also been associated with chronic synovitis of the knee.

Repair, Reattachment, Reconstruction, Stabilization, or Transfer of Soft Tissues
• Muscle RepairProcedure
A patient can achieve a more satisfactory outcome with a late repair (approximately 48 to 72 hours after injury) after acute symptoms have decreased. The muscle is reopposed, sutured, and immobilized so it is initially held in a shortened position as it begins to heal.
Postoperative Management• Muscle-setting exercise of the sutured muscle may be initiated immediately after
surgery.• When the immobilization is removed, active ROM, emphasizing controlled motion
within a protected range, may be started to regain joint mobility and prevent contractures.
• Weight bearing is partially restricted until the patient achieves a functional level of strength and flexibility in the repaired muscle.
• Low-load, high-repetition resistance exercises are progressed very gradually to protect the healing muscle and should not elicit pain.
• Vigorous stretching or return to a full level of activity are contraindicated until soft tissue healing is complete—as long as 6 to 8 weeks postoperatively.

• Tendon RepairProcedure
After the tendon is sutured, the repaired muscle-tendon unit is maintained in a shortened position, as with a complete tear of a muscle
Postoperative Management• Muscle setting is begun immediately after surgery to prevent adhesions of the tendon
to the sheath or surrounding tissues and to promote alignment of healing tissue. If it is possible to remove the immobilization for brief periods of exercise, passive motion or active contraction of a muscle group may be permissible within a few days after surgery.
• Controlled antigravity motions are initiated after the repaired tendon has had several weeks to heal.
• Weight bearing may be restricted after an upper or lower extremity tendon repair, and heavy lifting activities are often contraindicated for as long as 6 to 8 weeks after an upper extremity repair.
• Because the muscle-tendon unit must be held in a shortened position for several weeks, regaining full range may be difficult. However, vigorous stretching and high-intensity resistance exercise should not be initiated until at least 8 weeks, when healing of the tendon has occurred

• Post operative management after ligament repair or reconstruction
Rehabilitation after ligament surgery emphasizes early but protected motion and progressive strengthening and weight bearing activities to load the healing tissues consistently but safely.
• Capsule stabilization and reconstructionPostoperative exercise focuses on the following.• To restore ROM, initially active motions are emphasized within a protected
range during early rehabilitation. Movements that place stress on the portion of the capsule that was tightened or repaired are progressed cautiously.
• When strengthening exercises are permissible, emphasis is placed on strengthening the dynamic stabilizers of the joint.
• Tendon Transfer or RealignmentPostoperative Management• As with a tendon repair, early muscle setting and protected motion are
important to maintain tendon gliding. Resisted movements are progressed cautiously and gradually to protect the reattached tendon.
• If the purpose of the transfer was to change the function of the muscle, biofeedback and electrical muscle stimulation often are used to help a patient learn to control the new action of the transferred muscle-tendon unit

Release, Lengthening, or Decompression of Soft Tissues
Procedures
During release or lengthening of a shortened muscle group, a portion of the muscle-tendon unit is surgically sectioned and fibrotic tissues are incised. A tendon also can be partially incised, as in a Z-lengthening to allow greater extensibility
Postoperative Management• CPM and/or active-assistive ROM typically is initiated within a day
or two after surgery. As soft tissue healing progresses, this is followed by active ROM through the gained ranges.
• Strengthening of the antagonists of the lengthened muscle and use of the gained ROM during functional activities also are started