The influence of surgical margins on local control after breast conserving surgery and postoperative...
21
The influence of surgical margins The influence of surgical margins on local control after breast on local control after breast conserving surgery and conserving surgery and postoperative radiotherapy postoperative radiotherapy Danijela Scepanovic, Martina Lukacovicova, Andrea Hurakova, Marg Danijela Scepanovic, Martina Lukacovicova, Andrea Hurakova, Marg ita Pobijakova ita Pobijakova National Cancer Institute of Slovakia, Bratislava National Cancer Institute of Slovakia, Bratislava ESTRO 29, September 12 – 16 2010, Barcelona, Spain
-
Upload
danijela-scepanovic -
Category
Health & Medicine
-
view
46 -
download
2
Transcript of The influence of surgical margins on local control after breast conserving surgery and postoperative...

The influence of surgical margins The influence of surgical margins on local control after breast on local control after breast
conserving surgery and conserving surgery and postoperative radiotherapypostoperative radiotherapy
Danijela Scepanovic, Martina Lukacovicova, Andrea Hurakova, MargDanijela Scepanovic, Martina Lukacovicova, Andrea Hurakova, Margita Pobijakovaita Pobijakova
National Cancer Institute of Slovakia, BratislavaNational Cancer Institute of Slovakia, Bratislava
ESTRO 29, September 12 – 16 2010, Barcelona, Spain

BackgroundBackgroundRadiotherapy prevents local Radiotherapy prevents local
recurrence of breast cancer after recurrence of breast cancer after breastbreast--conserving surgery. conserving surgery.
ESTRO 29, September 12 – 16 2010, Barcelona, Spain
PurposePurposeTo evaluate the influence of a surgical To evaluate the influence of a surgical
margins on local control, who underwent margins on local control, who underwent lumpectomy and whole breast irradiation lumpectomy and whole breast irradiation
with or without boost as part of their breast with or without boost as part of their breast conserving therapy (BCT) for early stage conserving therapy (BCT) for early stage
breast cancer (I and II stage).breast cancer (I and II stage).

Materials and methods, Materials and methods, from 2000 till 2004from 2000 till 2004
Patient characteristicsPatient characteristics
0.45.3
24.5
30.125.4
11.6
2.7
05
1015
20253035
20-29
30-39
40-49
50-59
60-69
70-79
80-89
NN 449449MeanMean (SD):(SD): 56,5 (11,5) 56,5 (11,5) yearsyearsMediMediaan:n: 56 56 yearsyears95% 95% CICI:: 55,5 55,5 -- 57,6 57,6 yearsyearsMin. Min. –– max.max. 27 27 -- 88 88 yearsyears
34.3%65.7%
Premenopausal
Postmenopausal
Age of pts (years)
%
pts
Age of patients (N = 449) Menostatus (N = 449)
NN %%
PremenopPremenopausalausal154154 34,334,3
PostmenopauPostmenopausalsal295295 65,765,7
ESTRO 29, September 12 – 16 2010, Barcelona, Spain

Materials and methods, Materials and methods, from 2000 till 2004from 2000 till 2004
I.I. Tumor characteristicsTumor characteristics
12.7%12.7%
74.6%
DuctalLobularOther
NN %%
DuDuctalctal 335335 74,674,6LobulLobularar 5757 12,712,7OtherOther 5757 12,712,7
0.7%
66.8%
32.5%T1
T2
T3
ESTRO 29, September 12 – 16 2010, Barcelona, Spain
Pathology (N = 449)
NN %%
T1T1 300300 66,866,8T2T2 146146 32,532,5T3T3 33 0,70,7
T stage (N = 449)
Materials and methods, Materials and methods, from 2000 till 2004from 2000 till 2004
IIII.. Tumor characteristicsTumor characteristics
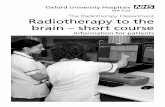
Surgical margins (N = 449)N stage (N = 449)
67.0%
33.0%
N0N+
26.9%
73.1%
<5 mm
>5 mm
NN %%
N0N0 301301 67,067,0N+N+ 148148 33,033,0
NN %%
<5 mm<5 mm 121121 26,926,9>5 mm>5 mm 328328 73,173,1
ESTRO 29, September 12 – 16 2010, Barcelona, Spain

Materials and methods, Materials and methods, from 2000 till 2004from 2000 till 2004
IIIIII.. Tumor characteristicsTumor characteristics
Grade (N = 449)Lymph-angioinvasion (N = 449)
0.2%
80.0%
19.8%Present
Absent
Unknown
14.3%
57.7%
15.6%12,4% G1
G2
G3
Unknown
NN %%
G1G1 6464 14,314,3G2G2 259259 57,757,7G3G3 7070 15,615,6UnknownUnknown 5656 12,412,4
NN %%
PPresentresent 8989 19,819,8AbsentAbsent 359359 80,080,0UnknownUnknown 11 0,20,2
ESTRO 29, September 12 – 16 2010, Barcelona, Spain

Materials and methods, Materials and methods, from 2000 till 2004from 2000 till 2004
IIVV.. Tumor characteristicsTumor characteristics
Boost (N = 449)HER2 status (N = 449)
18.3%18.9%
62.8%
Negative
Positive
Unknown 57.7%
42.3%
Yes
No
NN %%
NegatiNegativeve 282282 62,862,8PoPossitivitivee 8585 18,918,9UnknownUnknown 8282 18,318,3
NN %%
YesYes 259259 57,757,7NNoo 190190 42,342,3
ESTRO 29, September 12 – 16 2010, Barcelona, Spain

Materials and methods, Materials and methods, from 2000 till 2004from 2000 till 2004
RadiotherapyRadiotherapy
ESTRO 29, September 12 – 16 2010, Barcelona, Spain
• All of patients were operated by lumpectomy of a breast tumor and axillary dissection, followed by whole breast irradiation to 50Gy in 5
weeks, with two tangential fields, 6MVX energy.
• They were randomly assigned to receive either no extra irradiation or a boost dose of 10 - 16Gy to the original tumor bed.
• There were 328 pts (73%) with microscopically complete excision (more than 5mm) and 121 pts (27%) with a microscopically incomplete excision (less or equal than 5mm). Patients with
microscopically complete excision who did not receive boost were 159 (48%). However, boost was not applied in 33 pts (27%) with a
microscopically incomplete excision.

Technique of boost (N = 259)Dose of boost (N = 259)
NN %%
<9 <9 GyGy 22 0,80,81010--16 16 GyGy 254254 98,098,0>17 >17 GyGy 33 1,21,2
NN %%
ee-- 172172 66,466,4XX 00 0,00,0BTBT 8787 33,633,6
Materials and methods, Materials and methods, from 2000 till 2004from 2000 till 2004
BoostBoost
ESTRO 29, September 12 – 16 2010, Barcelona, Spain

Materials and methods, Materials and methods, from 2000 till 2004from 2000 till 2004
ESTRO 29, September 12 – 16 2010, Barcelona, Spain
Surgical margins were used to assess risk of local recurrence.
Also, we evaluated influence of• age
• menstrual status • histological type of cancer
• size of tumor • presence of axillar lymph nodes metastases
• presence of lymph–angioinvasion• histological grade
• presence of c-erb-B2/neu • application of boost and
• technique of boost (electrons or iridium 192 implant, high dose rate - HDR) on rate of local recurrence.
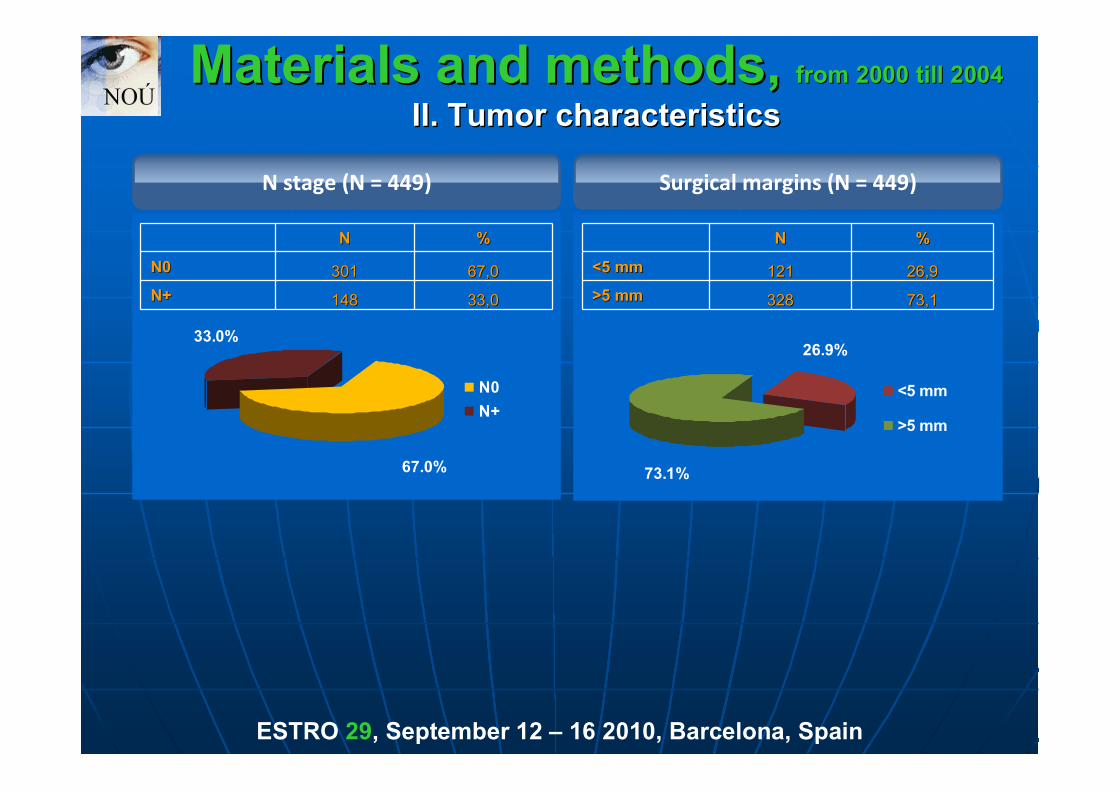
Surgical margins (N = 449)
Negative surgical margins were associated with statistically significant influenceon low risk of local recurrence (p < 0,001). However, there was not statistically
significant influence of boost in patients with microscopically incompleteexcision (p = 0,181).
Boost in patients with microscopicallyincomplete excision (N = 121)
SurgicalSurgicalmarginsmargins
NN 55--yearsyearsDFSDFS
betabeta RR (95% RR (95% CCI)I)
<5 mm<5 mm 121121 0,920,92 1,001,00>5 mm>5 mm 328328 0,990,99 --2,842,84 0,06 (0,01 0,06 (0,01 –– 0,26)0,26)
012
2436
4860
7284
96108
120132
Čas (měsíce)
0,00,10,20,30,40,50,60,70,80,91,0
Kum
ulat
ivní
pod
íl be
z re
cidi
vy(%
)
<5 mm >5 mm
Resekční okraj
BoostBoost NN 55--yearsyearsDFSDFS
betabeta RR (95% RR (95% CCI)I)
YesYes 8888 0,900,90 1,001,00NNoo 3333 0,970,97 --1,401,40 0,25 (0,03 0,25 (0,03 –– 1,92)1,92)
0 12 24 36 48 60 72 84 96 108 120 132
Čas (měsíce)
0,00,10,20,30,40,50,60,70,80,91,0
Kum
ulat
ivní
pod
íl be
z re
cidi
vy (%
)
Ano Ne
Aplikace boostu
p < 0,001p = 0,181
I. I. ResultsResults ESTRO 29, September 12 – 16 2010, Barcelona, Spain

Age (N = 449)
There was difference but not statistically significant between 2 categories ofpatients according age (<60 years and >=60 years) (p = 0,047).
AgeAge NN 55--yearsyearsDFSDFS
BetaBeta RR (95% RR (95% CCI)I)
<60<60 271271 0,970,97 1,001,00>=60>=60 178178 0,990,99 --0,840,84 0,43 (0,12 0,43 (0,12 –– 1,54)1,54)
0 12 24 36 48 60 72 84 96 108 120 132
Čas (měsíce)
0,00,10,20,30,40,50,60,70,80,91,0
Kum
ulat
ivní
pod
íl be
z re
cidi
vy (%
)
<60 >=60
Věkp = 0,196
Age (N = 449)
NN BetaBeta RR (95% RR (95% CCI)I) pp--valuevalue
VVěěkk 449449 --0,050,05 0,95 (0,90 0,95 (0,90 –– 1,00)1,00) 0,0470,047
II. II. ResultsResults ESTRO 29, September 12 – 16 2010, Barcelona, Spain
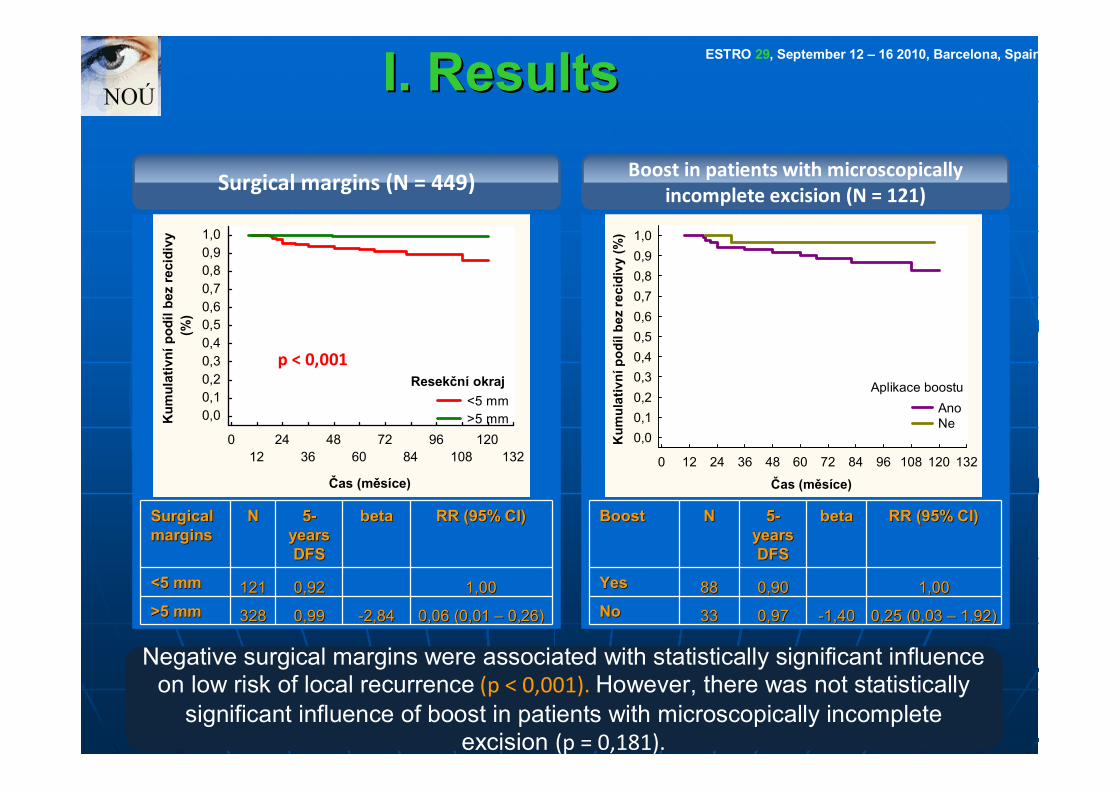
There was low risk of local recurrence in postmenopausal patients. However, there was difference but not statistically significant (p = 0,074).
Histologie
ResekResekččnnííokrajokraj
NN 55--letletéé DFSDFS RR (95% IS)RR (95% IS)
<5 mm<5 mm
>5 mm>5 mm
Menostatus (N = 449)
NN 55--yearsyearsDFSDFS
BetaBeta RR (95% RR (95% CCI)I)
PremenopauPremenopausalsal 154154 0,950,95 1,001,00PostmenopauPostmenopausalsal 295295 0,990,99 --0,970,97 0,38 (0,13 0,38 (0,13 –– 1,10)1,10)
0 12 24 36 48 60 72 84 96 108 120 132
Čas (měsíce)
0,00,10,20,30,40,50,60,70,80,91,0
Kum
ulat
ivní
pod
íl be
z re
cidi
vy (%
)
Premenopauza Postmenopauza
p = 0,074
III. III. ResultsResults ESTRO 29, September 12 – 16 2010, Barcelona, Spain

Pathology (N = 449)
Histological type and size of tumor had not influence on local control.
Size of tumor (N = 449)
HistologHistologyy NN 55--yearsyearsDFSDFS
BetaBeta RR (95% RR (95% CCI)I)
DuDuctalctal 335335 0,970,97 -- --LobuLobularlar 5757 1,001,00 -- --OOtherther 5757 1,001,00 -- --
SizeSize ofoftumortumor
NN 55--yearsyearsDFSDFS
BetaBeta RR (95% RR (95% CCI)I)
T1T1 300300 0,980,98 -- --T2T2 146146 0,970,97 -- --T3T3 33 1,001,00 -- --
0 12 24 36 48 60 72 84 96 108 120 132
Čas (měsíce)
0,00,10,20,30,40,50,60,70,80,91,0
Kum
ulat
ivní
pod
íl be
z re
cidi
vy (%
)
Duktální Lobulární Ostatní
Histologický typ
0 12 24 36 48 60 72 84 96 108 120 132
Čas (měsíce)
0,00,10,20,30,40,50,60,70,80,91,0
Kum
ulat
ivní
pod
íl be
z re
cidi
vy (%
)
1 2 3
T
IV. IV. ResultsResults ESTRO 29, September 12 – 16 2010, Barcelona, Spain

Axillar lymph nodes (N = 449)
Cox regression model could not be applicated on lymph nodes status. However, there was very statistically significant influence of negative lymph-angioinvasion
on low risk of local recurrence (p < 0,001).
Lymph-angioinvasion (N = 448)
LULU NN 55--yearsyearsDFSDFS
BetaBeta RR (95% RR (95% CCI)I)
N0N0 301301 1,001,00 -- --N+N+ 148148 0,930,93 -- --
LymLymphph//angioinangioinvasionvasion
NN 55--yearsyearsDFSDFS
BetaBeta RR (95% RR (95% CCI)I)
PoPositivesitive 8989 0,930,93 1,001,00NegativNegativee 359359 0,990,99 --1,791,79 0,17 (0,06 0,17 (0,06 –– 0,48)0,48)
0 12 24 36 48 60 72 84 96 108 120 132
Čas (měsíce)
0,00,10,20,30,40,50,60,70,80,91,0
Kum
ulat
ivní
pod
íl be
z re
cidi
vy (%
)
N0 N+
LU
0 12 24 36 48 60 72 84 96 108 120 132
Čas (měsíce)
0,00,10,20,30,40,50,60,70,80,91,0
Kum
ulat
ivní
pod
íl be
z re
cidi
vy (%
)
Pozitivní Negativní
Lymfo/angioinvaze
p < 0,001
V. V. ResultsResults ESTRO 29, September 12 – 16 2010, Barcelona, Spain

Grade (N = 393)
There was not local recurrence in patients with grade 1 of tumor. Influence ofHER2 status was not statistically significant to risk of local recurrence (p = 0,304).
GradGradee NN 55--yearsyearsDFSDFS
BetaBeta RR (95% RR (95% CCI)I)
11 6464 1,001,00 -- --22 259259 0,960,96 -- --33 7070 0,970,97 -- --
0 12 24 36 48 60 72 84 96 108 120 132
Čas (měsíce)
0,00,10,20,30,40,50,60,70,80,91,0
Kum
ulat
ivní
pod
íl be
z re
cidi
vy (%
)
1 2 3
Grading
HER2 status (N = 367)
HER2HER2 NN 55--years years DFSDFS
BetaBeta RR (95% RR (95% CCI)I)
NegatNegativeive 282282 0,990,99 1,001,00PoPossitivitivee 8585 0,940,94 0,320,32 1,38 (0,75 1,38 (0,75 –– 2,54)2,54)
0 12 24 36 48 60 72 84 96 108 120 132
Čas (měsíce)
0,00,10,20,30,40,50,60,70,80,91,0
Kum
ulat
ivní
pod
íl be
z re
cidi
vy (%
)
Negativní Pozitivní
HER2 status
p = 0,304
ESTRO 29, September 12 – 16 2010, Barcelona, Spain VI. ResultsVI. Results

Application of boost (N = 449)
Application of boost had higher risk of local recurrence because the boost was applied in patients with positive surgical margins more often (p = 0,031).
Technique of boost had not influence on risk of local recurrence (p = 0,112).
Technique of boost (N = 259)
BoostBoost NN 55--years years DFSDFS
BetaBeta RR (95% RR (95% CCI)I)
YesYes 259259 0,960,96 1,001,00NNoo
190190 1,001,00 --2,242,240,11 (0,01 0,11 (0,01 ––
0,82)0,82)
Technique Technique of of boostboost
NN 55--years years DFSDFS
BetaBeta RR (95% RR (95% CCI)I)
ee-- 172172 0,940,94 1,001,00BTBT 8787 0,990,99 --1,231,23 0,29 (0,06 0,29 (0,06 –– 1,34)1,34)
0 12 24 36 48 60 72 84 96 108 120 132
Čas (měsíce)
0,00,10,20,30,40,50,60,70,80,91,0
Kum
ulat
ivní
pod
íl be
z re
cidi
vy (%
)
Ano Ne
Boost
0 12 24 36 48 60 72 84 96 108 120 132
Čas (měsíce)
0,00,10,20,30,40,50,60,70,80,91,0
Kum
ulat
ivní
pod
íl be
z re
cidi
vy (%
)
e- BT
p = 0,031
p = 0,112
VII. ResultsVII. Results ESTRO 29, September 12 – 16 2010, Barcelona, Spain
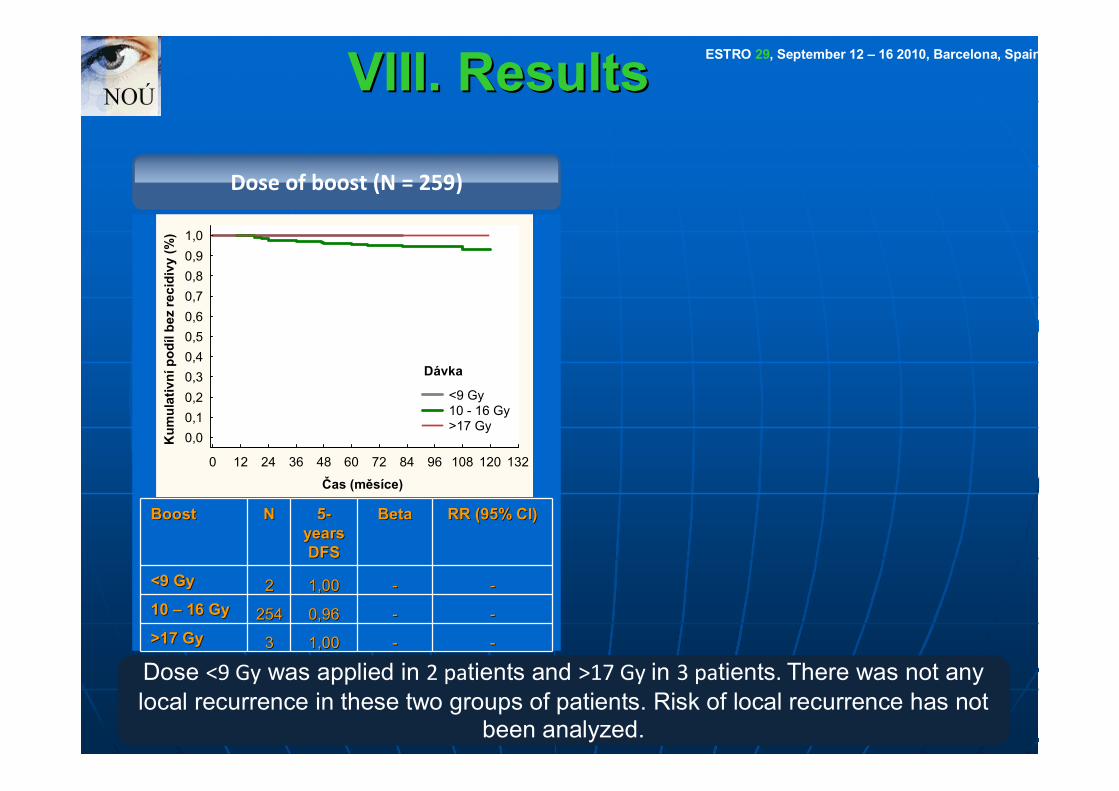
Dose of boost (N = 259)
Dose <9 Gy was applied in 2 patients and >17 Gy in 3 patients. There was not any local recurrence in these two groups of patients. Risk of local recurrence has not
been analyzed.
BoostBoost NN 55--years years DFSDFS
BetaBeta RR (95% RR (95% CCI)I)
<9 Gy<9 Gy 22 1,001,00 -- --10 10 –– 16 Gy16 Gy 254254 0,960,96 -- -->17 Gy>17 Gy 33 1,001,00 -- --
0 12 24 36 48 60 72 84 96 108 120 132
Čas (měsíce)
0,00,10,20,30,40,50,60,70,80,91,0
Kum
ulat
ivní
pod
íl be
z re
cidi
vy (%
)
<9 Gy 10 - 16 Gy >17 Gy
Dávka
VIII. ResultsVIII. Results ESTRO 29, September 12 – 16 2010, Barcelona, Spain
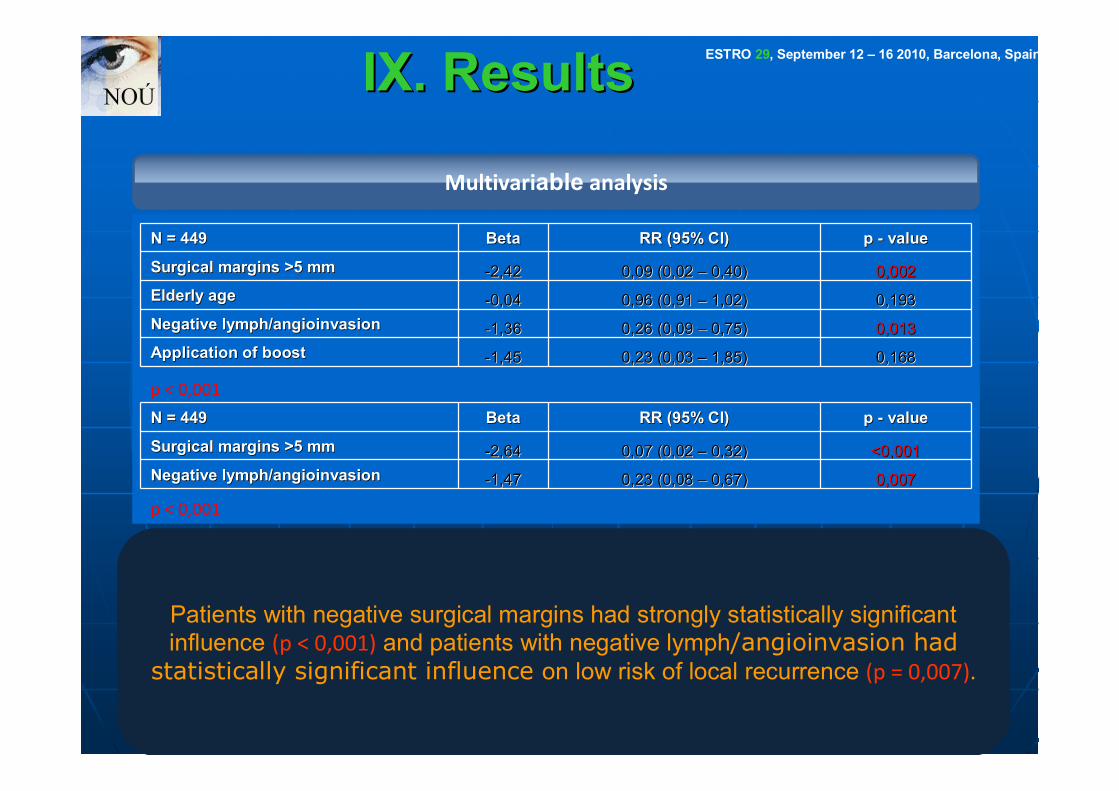
Multivariable analysis
Patients with negative surgical margins had strongly statistically significant influence (p < 0,001) and patients with negative lymph/angioinvasion had
statistically significant influence on low risk of local recurrence (p = 0,007).
N = 44N = 4499 BetaBeta RR (95% RR (95% CCI)I) p p -- valuevalue
Surgical marginsSurgical margins >5 mm>5 mm --2,422,42 0,09 (0,02 0,09 (0,02 –– 0,40)0,40) 0,0020,002Elderly ageElderly age --0,040,04 0,96 (0,91 0,96 (0,91 –– 1,02)1,02) 0,1930,193NegativNegativee lymlymphph/angioinva/angioinvasionsion --1,361,36 0,26 (0,09 0,26 (0,09 –– 0,75)0,75) 0,0130,013Application of boostApplication of boost --1,451,45 0,23 (0,03 0,23 (0,03 –– 1,85)1,85) 0,1680,168
p < 0,001
N = 44N = 4499 BetaBeta RR (95% RR (95% CCI)I) p p -- valuevalue
Surgical marginsSurgical margins >5 mm>5 mm --2,642,64 0,07 (0,02 0,07 (0,02 –– 0,32)0,32) <0,001<0,001NegativNegativee lymphlymph/angioinva/angioinvasionsion --1,471,47 0,23 (0,08 0,23 (0,08 –– 0,67)0,67) 0,0070,007
p < 0,001
ESTRO 29, September 12 – 16 2010, Barcelona, Spain IX. ResultsIX. Results
X. ResultsX. Results
ESTRO 29, September 12 – 16 2010, Barcelona, Spain
• At median follow up of 79 months (minimum=20; maximum=120) the incidence of local recurrence rate was 3% for all group of patients (449pts).
• The cumulative incidence of local recurrence was 1% in group of pts with negative surgical margins versus 8% in group of pts with positive margins
{95% CI, 6% (1%-26%)}, (p<0.001).

ConclusionConclusion
ESTRO 29, September 12 – 16 2010, Barcelona, Spain
The criteria which helped to identify low-risk group of pts for local recurrence were - elderly patients (≥60yrs),
- postmenopausal pts, - negative surgical margins and
- absence of lymph-angioinvasion.
However, negative surgical margins and absence of lymph-angioinvasion were independent factors associated
with local control in our patients.









![Effect of radiotherapy after breast-conserving surgery on ... · Radiotherapy reduced the annual breast cancer mortality rate by one‐sixth (RR=0.82 [0.75, 0.90]). The timing of](https://static.fdocuments.net/doc/165x107/5f025ab17e708231d403db86/effect-of-radiotherapy-after-breast-conserving-surgery-on-radiotherapy-reduced.jpg)