Cervical Spine Clearance in Trauma for Moderate Resource Settings
49
Cervical Spine Clearance in Trauma For Moderate Resource Settings Emergency Medicine Resident Conference Georgetown Public Hospital Joseph M Reardon, MD We Care
-
Upload
joseph-reardon -
Category
Health & Medicine
-
view
188 -
download
0
Transcript of Cervical Spine Clearance in Trauma for Moderate Resource Settings

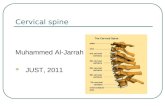
Cervical Spine Clearancein Trauma
For Moderate Resource Settings
Emergency Medicine Resident ConferenceGeorgetown Public Hospital
Joseph M Reardon, MD
We Care

Disclosure Statement
• I have no financial conflicts of interest to disclose.
Special Thanks• Sarah Crosby, MBBS, Hunter New England Health, New South Wales
• Josh Broder, Sam Francis, & Steve Barmach, Duke University Health System

Case

Overview
• When to collar
• How to collar
• When to image
• When to take it off

Overview
• When to collar• American Association of Neurological Surgeons (AANS) Guidelines
• Current Evidence and Decision Rules
• Clinical Practice
• How to collar
• When to image
• When to take it off
• Other spinal trauma

Overview
• When to collar• American Association of Neurological Surgeons Guidelines
• Current Evidence and Decision Rules
• Clinical Practice
• How to collar
• When to image
• When to take it off
• Other spinal trauma

When to collar - AANS
• “all trauma patients with…mechanism of injury having the potential to cause cervical spinal injury should be immobilized”• “A rigid cervical collar and
supportive blocks on a backboard with straps is very effective in limiting motion of the cervical spine and is recommended”
AANS, 2001

When to collar - AANS
• “As many as 20% of spinal column injuries involve multiple non-continuous vertebral levels”•Immobilize whole
spine if truly concerned
AANS, 2001

Overview
• When to collar• American Association of Neurological Surgeons Guidelines
• Current Evidence
• Clinical Practice
• How to collar
• When to image
• When to take it off
• Other spinal trauma

When to collar – Current Evidence
• North America: EMS collars most blunt trauma patients.
• 2010: US Natl Trauma Data Bank Study• Penetrating trauma pts with doubled risk of death if collared
• Mult sources of confounding
University of Michigan, 2010

Overview
• When to collar• American Association of Neurological Surgeons Guidelines
• Current Evidence
• Clinical Practice
• How to collar
• When to image
• When to take it off

When to Collar – Clinical Practice
• Most of our patients arrive to the ER uncollared
• C spine precautions should be maintained from arrival to ER – even during your primary survey!
• Apply imaging decision rules at the bedside and decide if collar is indicated.
Progressive Spine & Orthopedics, 2015

Overview
• When to collar
• How to collar• Miami J
• Philadelphia
• Portable EMS Collar
• Lab!
• When to image
• When to take it off
• Other spinal trauma

Original C-collar
Schreiber, 1943

How to collar – Miami J
Ossur Products, 2016

How to collar: Others
• Ambu: EMS Standard
• Philadelphia:• Not currently evidence-supported.
• Aspen: Most expensive and most effective
• Soft collar:• Use for patients with definite muscular (aka NON-traumatic) neck pain for
whom neck support will reduce pain medication requirements
Surgical Solutions, 2013

How to collar: Plaster of Paris• Long used; no evidence.
• “The cast must extend the entire length of the c-spine. It must have a broad weight-bearing base over the shoulders and support the jaw and occiput.
• ….someone must maintain traction while the plaster is applied and until it sets.
• To apply it, put thick padding over the shoulders, jaw, and occiput. Next apply two broad plaster slabs—one anteriorly and the other posteriorly. Then apply the plaster around the neck to secure these slabs.”
Iserson, 2011

Overview
• When to collar
• How to collar
• When to image• American Association of Neurological Surgeons Guidelines (AANS)
• Eastern Association for Surgery of Trauma Guidelines (EAST)
• Current Evidence
• Clinical Practice
• When to take it off
• Other spinal trauma

When to Image - Guidelines
• AANS:• “Radiographic assessment of the cervical spine is not recommended in
trauma patients who are awake, alert, and not intoxicated, who are without neck pain or tenderness, and who do not have significant associated injuries that detract from their general evaluation.”
• “Plain radiographs contribute no additional information and should not be obtained” (Level II)
• EAST:• Same as AANS

Overview
• When to collar
• How to collar
• When to image• NEXUS
• Canadian C-spine Rule
• NICE Guidelines
• Clinical Practice
• When to take it off

When to image - Evidence
• NEXUS


Clinical Clearance of the C-Spine in the Awake Patient
NEXUS
Sensitivity 90.7%
Specificity 36.8%
Radiography Rate 66.6%
Canadian C-Spine Rule
Sensitivity 99.4%
Specificity 45.1%
Radiography Rate 55.9%
Stiell IG, et al. The Canadian c-spine rule versus the nexus low-risk criteria in patients with trauma.
NEJM 2003;349:2510-2518
When to image - Evidence

NICE Guidelines

NICE Guidelines – Risk Factors requiring CT in UK*á la Canadian C spine Rule
**RISK FACTORS FOR C SPINE INJURY:
• GCS less than 13 on initial assessment. See recommendations on GCS.
• The patient has been intubated.
• Plain X-rays are technically inadequate (for example, the desired view is unavailable).
• Plain X-rays are suspicious or definitely abnormal.
• A definitive diagnosis of cervical spine injury is needed urgently (for example, before surgery).
• The patient is having other body areas scanned for head injury or multi-region trauma.
• The patient is alert and stable, there is clinical suspicion of cervical spine injury and any of the following apply:• age 65 years or older• dangerous mechanism of injury (fall from a height of greater than 1 metre or 5 stairs; axial load to the head,
for example, diving; high-speed motor vehicle collision; rollover motor accident; ejection from a motor vehicle; accident involving motorised recreational vehicles; bicycle collision)
• focal peripheral neurological deficit• paraesthesia in the upper or lower limbs.

So do we have to scan everyone???

Cost-effective C-Spine Scanning in GuyanaHigh-risk Factor Fracture Probability (%)
Focal neurologic deficit 31.1
Severe head injury‡ 11.2
High-energy mechanism and age older than 50 years 14.8
* Severe head injury = skull fracture, intracranial hemorrhage, or injury causing unconscious state during emergency department evaluation. High-energy mechanism = high-speed motor vehicle accident (>30 mph) or pedestrian struck by car.
Blackmore, et al., Radiology, 1999

What I would do:
• CT C spine for all high risk patients with potential for recovery:• Focal neuro deficit
• Severe head injury
• High energy mechanism (>60mph, pedestrian, ejection, fall >5ft, axial load) and PEx suggesting neck injury
• Age over 50 years and PEx suggesting neck injury
• X-ray for all other patients based on Canadian rule

Overview
• When to collar
• How to collar
• When to image
• When to take it off• Evidence
• Clinical Practice
• Other spinal trauma

C-collar Removal: Imaging
• The Primary screening modality is axial CT from the occiput to T1 with sagittal and coronal reconstructions (Level II)
• If there is neurological deficit attributable to a c-spine injury an MRI should be obtained

C-Collar Removal: Neck Pain with negative CT in the neurologically intact patient
Options (Level III)
1. Continue collar
2. Remove collar after negative and adequate flexion extension films
• Picks up c-spine instability in 6.75-8% of normal c-spine films
• Incidence of isolated ligamentous injury is rare (0.6% of traumatic c-spine injuries)
*Note: In obtunded pt, keep the collar on!!

C-Collar Removal: SCIWORASignificant Cord Injury without obvious radiological
abnormality
• Higher incidence in pediatric population• The relatively large size of the head
• Inherent skeletal mobility• Cord vulnerable to damage
• Higher incidence above 60 yo• Posterior vertebral spurs, loss of disc height
• Risk of central cord syndrome after hyperextension injury
• If worried: Consider MRI.
• 2011 Meta-analysis (14,327 pts): Sensitivity of CT for unstable C-spine fractures was >99.9%• Limitations: Ignored stable fractures, heterogeneity of alternative modalities
• Conclusions: Imaging for SCIWORA after negative CT, in the absence of compelling extenuating circumstances, is unnecessary
Panczykowski, Tomcyz, J Neurosurg 2011

Overcoming SCIWORA
• Physical Exam (ATLS Secondary Survey©™®)• Check multiple dermatomes, assess progression of GCS
• Strength & reflexes as proxies of upper motor neuron damage
• Consider rectal exam if any suspicion for spinal cord injury (as in ATLS, not mandatory if there is very low suspicion of neurologic injury)

Overview
• When to collar
• How to collar
• When to image
• When to take it off• Evidence
• Clinical Practice
• Other spinal trauma

C-Collar Removal: Clinical Practice
• Persistent pain:• No study has yet validated a method of risk-stratifying patients with
persistent pain and negative CT C-spine
• In setting of negative CT C-spine, we assess severity of pain. For mild pain that could be attributable to positioning and discomfort of the immobilization, we generally clear the c-spine. Moderate or severe pain or consultant concern necessitates keeping the collar on.
• Obtunded patient:• Do not remove collar – Defer to admitting team

Overview
• When to collar
• How to collar
• When to image
• When to take it off
• Other spinal trauma• Evidence
• EAST Guidelines
• Clinical Practice

Thoracolumbar Spine Trauma
• 4.4% of trauma patients have TLS fracture• 19-50% of these fractures are associated with spinal cord damage
• Higher incidence of neurologic deficit when fracture identification was delayed (10.5% vs 1.4%)
• Standard hospital stretcher IS sufficient to immobilize the TLS spine

Overview
• When to collar
• How to collar
• When to image
• When to take it off
• Other spinal trauma• Evidence
• EAST Guidelines
• Clinical Practice

EAST Recommendations (2007)
• Level II Guidelines• Trauma patients who are awake, without any evidence of intoxication, with
normal mental status, neurologic and physical examinations may be cleared clinically

Mode of Imaging of TLS
• Plain films are adequate for the examination of the TLS if the patient does not require CT scan for any other reason (III)
• CT with axial reconstruction is superior to plain films for screening of TLS for bony injury (II)
• CT scout films can be used for spine assessment (II)
• CT scan may be associated with less overall radiation exposure than plain films (III)
• MRI is indicated for patients with neurologic deficits, abnormal CT scans or clinical suspicion despite normal radiographic evaluation suggesting an unstable injury (III)• Early decompression of traumatic lesions improves outcome

Plain Film vs CT of TLS
• Ballock et al. (1992)• plain radiography of the thoracolumbar spine would have missed
25% of fractures
• Gestring et al. (2002)- CT protocol for examining TLS• Anterior, posterior and lateral scout films and axial images
• 100% sensitivity and specificity

Plain Film vs CT of TLS, contd
• Hauser et al. (2003)-prospective study 222 patients• Plain radiography of the TL spine vs Helical CT (5mm images)
• CT scan accuracy 99% vs plain radiographs 87%
• CT could also differentiate acute vs old #
• Sheridan et al. (2003)• Reformatted helical T (2.5mm images) vs plain x-ray
• Sensitivity for Thoracic #- CT 97% vs x-ray 62%
• Sensitivity for Lumbar #- CT 95% vs x-ray 86%


Overview
• When to collar
• How to collar
• When to image
• When to take it off
• Other spinal trauma
• QUESTIONS

Review Questions
• Which of the following injuries is considered unstable?
• A.) Unilateral facet dislocation
• B.) Bursting fracture of the vertebral body
• C.) Transverse process fracture
• D.) Clay shoveler’s fracture
• E.) Flexion teardrop fracture

Review Questions
• Which of the following injuries is considered unstable?
• A.) Unilateral facet dislocation
• B.) Bursting fracture of the vertebral body
• C.) Transverse process fracture
• D.) Clay shoveler’s fracture
• E.) Flexion teardrop fracture

Review Questions• Which of the following patients is most in need of cervical spine
imaging?
• A.) 64-yo male who fell down 3 steps after drinking
• B.) 26-yo female who awoke with severe neck pain radiating down left shoulder
• C.) 30-yo helmeted motorcyclist who has tingling in right 4th and 5th
digits
• D.) 45-yo man with pain radiating up and down back after lifting a table
• E.) 50-yo restrained driver who crashed at 60mph and has left radius fracture

Review Questions• Which of the following patients is most in need of cervical spine
imaging?
• A.) 64-yo male who fell down 3 steps after drinking
• B.) 26-yo female who awoke with severe neck pain radiating down left shoulder and can’t turn head to the right
• C.) 30-yo helmeted motorcyclist who has tingling in right 4th and 5th
digits
• D.) 45-yo man with pain radiating up and down back after lifting a table
• E.) 50-yo restrained driver who crashed at 60mph and has left radius fracture

NICE Guidelines – Risk Factors mandating CT*á la Canadian C spine Rule
**RISK FACTORS FOR C SPINE INJURY:
• GCS less than 13 on initial assessment. See recommendations on GCS.
• The patient has been intubated.
• Plain X-rays are technically inadequate (for example, the desired view is unavailable).
• Plain X-rays are suspicious or definitely abnormal.
• A definitive diagnosis of cervical spine injury is needed urgently (for example, before surgery).
• The patient is having other body areas scanned for head injury or multi-region trauma.
• The patient is alert and stable, there is clinical suspicion of cervical spine injury and any of the following apply:• age 65 years or older• dangerous mechanism of injury (fall from a height of greater than 1 metre or 5 stairs; axial load to the head,
for example, diving; high-speed motor vehicle collision; rollover motor accident; ejection from a motor vehicle; accident involving motorised recreational vehicles; bicycle collision)
• focal peripheral neurological deficit• paraesthesia in the upper or lower limbs.