Cerebral venous sinus thrombosis in a patient with type 1 ... Hosseini.pdf · Cerebral venous sinus...
3
CASE REPORT 34 Pract Diab Int January/February 2010 Vol. 27 No. 1 Copyright © 2010 John Wiley & Sons Case history A 17-year-old British man of Indian origin presented with a two-day history of severe generalised head- ache followed by blurred vision and vomiting on the day of admission. He was known to have type 1 diabetes mellitus since the age of 11 years. He had been treated with a basal bolus insulin regimen using glargine and NovoRapid. Despite regular input from medical and nursing teams, his glycaemic control had been deterio- rating (HbA1c 12.7%, 11.8%, 9.8%, and 9.6% at 0, -3, -6 and -12 months from admission respectively). He had no known diabetic micro- or macrovascular complications and was normotensive. He was a full-time student living with his parents, with no history of thrombophilia in the family. He denied any history of smok- ing, using any recreational drugs or alcohol consumption. On admission, general physical and systemic examinations were within normal limits and there were no meningism, papilloedema, pyram- idal or cerebellar signs. His blood glucose was 11mmol/L. An initial urinary dipstick showed 2+ ketones although subsequent repeats were all negative and arterial blood gas analy- sis excluded acidosis – serum pH 7.38 (7.35–7.45), calculated osmolality 305mmol/kg, base excess -1.4mEq/L (±2mEq/L) and serum bicarbonate 23mmol/L (21–28mmol/L). The rest of his routine haematological and biochemical profiles were within normal limits. An urgent CT scan of his brain (Figure 1a) raised the suspicion of a dural venous sinus thrombosis. A subsequent magnetic resonant venogram confirmed the diagnosis of sagittal sinus and left transverse sinus thrombosis (Figure 1b). Anticoagulation was initiated with low molecular weight heparin, and maintained with warfarin. While in hospital he developed diplopia secondary to right 6th nerve palsy that was considered to be a false local- ising sign. The symptoms responded well to treatment and his neuro- logical signs improved prior to dis- charge from hospital. Investigations for underlying thrombophilic state, myeloproliferative disorders, auto- immune conditions and haemoglo- binopathy were all negative. Discussion Cerebral venous sinus thrombosis (CVST) is an uncommon disorder with an estimated annual incidence of three to four cases per million. 1 Most patients are young adults or children and clinical presentation is variable but often dramatic. Headache is the presenting symp- tom in 70–90% of cases, while seizures, focal deficits, cranial nerve syndromes involving IX, X, and XI (jugular foramen syndrome) or III, IV and VI cranial nerve palsies, impairment of consciousness, visual disturbances and papilloedema occur in 25–75% of cases. 2,3 Predisposing factors to CVST can only be identified in 65–80% of patients, with more than one factor often found in individual patients. 4 These include local and systemic conditions predisposing to venous thrombosis including pregnancy, puerperium, oral contraceptive pills, intracranial pathologies, malignan- cies, connective tissue and inflam- matory diseases, haematological conditions and drugs. 2 As a general rule, Virchow’s triad, as first formu- lated (venous stasis, vessel wall injury, acquired or genetic changes in composition of blood), is still the primary mechanism for the develop- ment of venous thrombosis. 4 Cerebral venous sinus thrombosis in a patient with type 1 diabetes in the absence of ketoacidosis AA Hosseini, RS Manjunatha, A Jacob, M El-Lahawi, V Baskar* ABSTRACT While the increased risk of thrombosis in the arterial tree among individuals with diabetes has been well studied, little is known about such risk in the venous system outside the settings of hyperosmolarity or ketoacidosis. Cerebral venous sinus thrombosis (CVST) is a recognised but extremely rare complication of diabetic ketoacidosis (DKA). We report a case of CVST in a patient with type 1 diabetes but without DKA, in whom we speculate that chronic poor glycaemic control was a contributory factor. Copyright © 2010 John Wiley & Sons. Practical Diabetes Int 2010; 27(1): 34–35 KEY WORDS cerebral venous sinus thrombosis; diabetes; diabetic ketoacidosis Akram A Hosseini, MD, MRCP Mohammed El-Lahawi, MBBS, MRCP Neurology Department, New Cross Hospital, Wolverhampton, UK Rashmi S Manjunatha, MBBS, MRCP Varadarajan Baskar, MD, MRCP Wolverhampton Diabetes Centre, New Cross Hospital, Wolverhampton, UK Abraham Jacob, FRCP, FRCPath, Haematology Department, New Cross Hospital, Wolverhampton, UK *Correspondence to: Dr Varadarajan Baskar, Wolverhampton Diabetes Centre, New Cross Hospital, Wolverhampton WV10 0QP, UK; e-mail: varadarajan.baskar@ rwh-tr.nhs.uk Received: 28 April 2009 Accepted in revised form: 2 July 2009
Transcript of Cerebral venous sinus thrombosis in a patient with type 1 ... Hosseini.pdf · Cerebral venous sinus...

CASE REPORT
34 Pract Diab Int January/February 2010 Vol. 27 No. 1 Copyright © 2010 John Wiley & Sons
Case historyA 17-year-old British man of Indianorigin presented with a two-day history of severe generalised head -ache followed by blurred vision andvomiting on the day of admission. Hewas known to have type 1 diabetesmellitus since the age of 11 years. Hehad been treated with a basal bolusinsulin regimen using glargine andNovoRapid. Despite regular inputfrom medical and nursing teams, hisglycaemic control had been deterio-rating (HbA1c 12.7%, 11.8%, 9.8%,and 9.6% at 0, -3, -6 and -12 monthsfrom admission respectively). He had no known diabetic micro- ormacrovascular complications and wasnormotensive. He was a full-time student living with his parents, withno history of thrombophilia in thefamily. He denied any history of smok-ing, using any recreational drugs oralcohol consumption.
On admission, general physicaland systemic examinations werewithin normal limits and there wereno meningism, papilloedema, pyram-idal or cerebellar signs. His blood glucose was 11mmol/L. An initial urinary dipstick showed 2+ ketonesalthough subsequent repeats were allnegative and arterial blood gas analy-sis excluded acidosis – serum pH 7.38(7.35–7.45), calculated osmolality305mmol/kg, base excess -1.4mEq/L(±2mEq/L) and serum bicarbonate23mmol/L (21–28mmol/L). Therest of his routine haematologicaland biochemical profiles were withinnormal limits. An urgent CT scan of
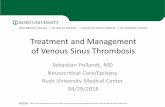
his brain (Figure 1a) raised the suspicion of a dural venous sinusthrombosis. A subsequent magneticresonant venogram confirmed thediagnosis of sagittal sinus and lefttransverse sinus thrombosis (Figure1b). Anticoagulation was initiatedwith low molecular weight heparin,and maintained with warfarin. Whilein hospital he developed diplopia secondary to right 6th nerve palsythat was considered to be a false local-ising sign. The symptoms respondedwell to treatment and his neuro -logical signs improved prior to dis-charge from hospital. Investigationsfor underlying thrombophilic state,myeloproliferative disorders, auto -immune conditions and haemoglo-binopathy were all negative.
DiscussionCerebral venous sinus thrombosis(CVST) is an uncommon disorderwith an estimated annual incidenceof three to four cases per million.1Most patients are young adults orchildren and clinical presentation
is variable but often dramatic.Headache is the presenting symp-tom in 70–90% of cases, whileseizures, focal deficits, cranial nervesyndromes involving IX, X, and XI(jugular foramen syndrome) or III,IV and VI cranial nerve palsies,impairment of consciousness, visualdisturbances and papilloedemaoccur in 25–75% of cases.2,3Predisposing factors to CVST canonly be identified in 65–80% ofpatients, with more than one factoroften found in individual patients.4These include local and systemicconditions predisposing to venousthrombosis including pregnancy,puerperium, oral contraceptive pills,intracranial pathologies, malignan-cies, connective tissue and inflam-matory diseases, haematologicalconditions and drugs.2 As a generalrule, Virchow’s triad, as first formu-lated (venous stasis, vessel wallinjury, acquired or genetic changesin composition of blood), is still theprimary mechanism for the develop-ment of venous thrombosis.4
Cerebral venous sinus thrombosis in a patient with type 1 diabetes in theabsence of ketoacidosisAA Hosseini, RS Manjunatha, A Jacob, M El- Lahaw i, V Baskar*
ABSTRACTWhile the increased risk of thrombosis in the arterial tree among individuals with diabeteshas been well studied, little is known about such risk in the venous system outside thesettings of hyperosmolarity or ketoacidosis. Cerebral venous sinus thrombosis (CVST) isa recognised but extremely rare complication of diabetic ketoacidosis (DKA). We report acase of CVST in a patient with type 1 diabetes but without DKA, in whom we speculatethat chronic poor glycaemic control was a contributory factor. Copyright © 2010 JohnWiley & Sons.
Practical Diabetes Int 2010; 27(1): 34–35
KEY WORDScerebral venous sinus thrombosis; diabetes; diabetic ketoacidosis
Akram A Hosseini, MD, MRCPMohammed El-Lahawi, MBBS, MRCPNeurology Department, New CrossHospital, Wolverhampton, UKRashmi S Manjunatha, MBBS, MRCPVaradarajan Baskar, MD, MRCPWolverhampton Diabetes Centre, New
Cross Hospital, Wolverhampton, UKAbraham Jacob, FRCP, FRCPath,Haematology Department, New CrossHospital, Wolverhampton, UK
*Correspondence to: Dr VaradarajanBaskar, Wolverhampton Diabetes Centre,
New Cross Hospital, Wolverhampton WV100QP, UK; e-mail: [email protected]
Received: 28 April 2009Accepted in revised form: 2 July 2009

CASE REPORT
Cerebral venous thrombosis in type 1 diabetes without ketoacidosis
Diabetes remains a controversialrisk factor for venous thrombo -embolism. While diabetes itself is associated with several defects of platelet function, coagulation and fibrinolytic systems resulting in a hypercoagulable state,1,5 theincreased rate of thrombotic compli-cations observed is often in the pres-ence of additional risk factors.6 It isevident that the rate of thromboticcomplications in diabetic patientswith frequent episodes of hyper -ketonaemia and hyperosmolarity isincreased.1,6,7 Published literatureon CVST and diabetes is limited tocase reports predominantly amongpatients with type 1 diabetes and isin the context of diabetic ketoacido-sis (DKA), dehydration or hyper -osmolarity.1,7,8 In association withtype 2 diabetes, two cases of CVSTare reported: one presenting withDKA while the other patient hadtransverse sinus aplasia.9,10 To ourknowledge, this is the first report ofa CVST in association with type 1diabetes but in the absence of con-comitant ketoacidosis or any knownprothrombotic conditions.
The optimum treatment forCVST and its duration haveremained uncertain, especiallywhere there is no identifiable aetiol-ogy.11 Based upon limited available
evidence, anticoagulation appears tobe safe and probably reduces therisk of death or dependency.12Treatment with systemic or localthrombolysis has been reported incases with a deteriorating clinicalcourse despite anticoagulation therapy. There are, however, no randomised controlled trial data tosupport efficacy or safety of throm-bolysis in CVST.12 In the presence ofa transient risk factor, anticoagula-tion is generally recommended forthree to six months. Patients withidiopathic CVST or those withhereditary thrombophilia are anti-coagulated for longer periods giventheir higher risk of recurrence.13 Inan international study that was performed in 624 patients withCVST, the cumulative risk for recur-rent CVST or other thromboticevents was 6.5%, with over half notundergoing anticoagulation at thetime of their recurrence.14
While our case might be consid-ered among the 20–35% of CVSTcases with no identifiable cause,4 wespeculate whether long-standinghyperglycaemia may have played arole in increasing our patient’sthrombotic risk, and highlight apotential direct association betweenCVST and hyperglycaemic state evenin the absence of dehydration or
ketoacidosis. If such a relationshipbetween diabetes and CVST were tobe found, new prognostic measuresmight become necessary and thismay also have an implication on therisk of recurrence and duration ofanti coagulation in this group ofpatients.
Our case highlights the need forclinicians to consider CVST amongpatients with diabetes even in theabsence of ketoacidosis or hyper -osmolarity.
Conflict of interest statementThere are no conflicts of interest.
ReferencesReferences are available at www.practicaldiabetesinternational.com.
Pract Diab Int January/February 2010 Vol. 27 No. 1 Copyright © 2010 John Wiley & Sons 35
Figure 1. (A) CT scan of the brain suggested the possibility of a dural sinus thrombosis. (B) Magnetic resonancevenogram confirmed the diagnosis of sagittal sinus and left transverse sinus thrombosis
Key points• The risk of thrombosis in thevenous tree in diabetes is lesswell studied
• Cerebral venous sinusthrombosis (CVST) is arecognised but rare complicationof diabetic ketoacidosis
• Our case illustrates the need toconsider CVST in patients withpoorly controlled diabetes evenin the absence of ketoacidosis orhyperosmolarity
a b

CASE REPORT
Cerebral venous thrombosis in type 1 diabetes without ketoacidosis
35i Pract Diab Int January/February 2010 Vol. 27 No. 1 Copyright © 2010 John Wiley & Sons
References1. Stam J. Thrombosis of the cerebral
veins and sinuses. N Engl J Med 2005;352: 1791–1798.
2. Bousser MG, Chiras J, Bories J, et al.Cerebral venous thrombosis – a reviewof 38 cases. Stroke 1985; 16: 199–213.
3. Allroggen H, Abbott RJ. Cerebralvenous sinus thrombosis. PostgradMed J 2000; 76: 12–15.
4. de Freitas GR, Bogousslavsky J. Riskfactors of cerebral vein and sinusthrombosis. Front Neurol Neurosci2008; 23: 23–54.
5. Jones EW, Mitchell JRA. Venousthrombosis in diabetes mellitus.Diabetologia 1983; 25: 502–505.
6. Keenan CR, Murin S, White RH.High risk for venous thromboem-bolism in diabetics with hyperosmo-lar state: comparison with other acute
medical illnesses. J Thromb Haemost2007; 5: 1185–1190.
7. Kalis NN, van der Merwe PL,Schoeman JF, et al. Cerebral oedemawith coning in diabetic ketoacidosis.Report of 2 survivors. S Afr Med J1991; 79: 727–731.
8. Keane S, Gallagher A, Ackroyd S, etal. Cerebral venous thrombosis dur-ing diabetic ketoacidosis. Arch DisChild 2002; 86: 204–205.
9. Usdan LS, Choong KWL, McDonnellME. Type 2 diabetes mellitus mani-festing with a cerebral vein thrombo-sis and ketoacidosis. Endocr Pract2007; 13: 687–690.
10.Nagai T. Diabetes mellitus with lefttransverse sinus thrombosis andright transverse sinus aplasia.Diabetes Res Clin Pract 2001; 51:39–43.
11.Ciccone A, Canhão P, Falcão F, et al.Thrombolysis for cerebral vein anddural sinus thrombosis. CochraneDatabase Syst Rev 2004; (1):CD003693.
12.de Bruijn SFTM, Stam J, for theCerebral Venous Thrombosis StudyGroup. Randomised, placebo-con-trolled trial of anticoagulation treat-ment with low-molecular-weightheparin for cerebral sinus thrombo-sis. Stroke 1999; 30: 484–488.
13. van Nuenen BFL, Munneke M,Bloem BR. Cerebral venous sinusthrombosis: prevention of recurrentthromboembolism. Stroke 2005; 36:1822.
14.Ferro JM, Canhão P, Stam J, et al, forthe ISCVT Investigators. Prognosis ofcerebral vein and dural sinus throm-bosis. Stroke 2004; 35: 664–670.
ONLINE ONLY