
Cattedra di Medicina Interna ed U.O. Malattie ... · Università Magna Græcia di Catanzaro...
38
Università Magna Græcia di Catanzaro Dipartimento di Medicina Sperimentale e Clinica Cattedra di Medicina Interna ed U.O. Malattie Cardiovascolari Prof. Francesco Perticone Update Scompenso Cardiaco: Trattamento Chirurgico o Farmacologico?
Transcript of Cattedra di Medicina Interna ed U.O. Malattie ... · Università Magna Græcia di Catanzaro...

Università Magna Græcia di Catanzaro
Dipartimento di Medicina Sperimentale e Clinica
Cattedra di Medicina Interna ed U.O. Malattie Cardiovascolari
Prof. Francesco Perticone
Update Scompenso Cardiaco:
Trattamento Chirurgico o Farmacologico?
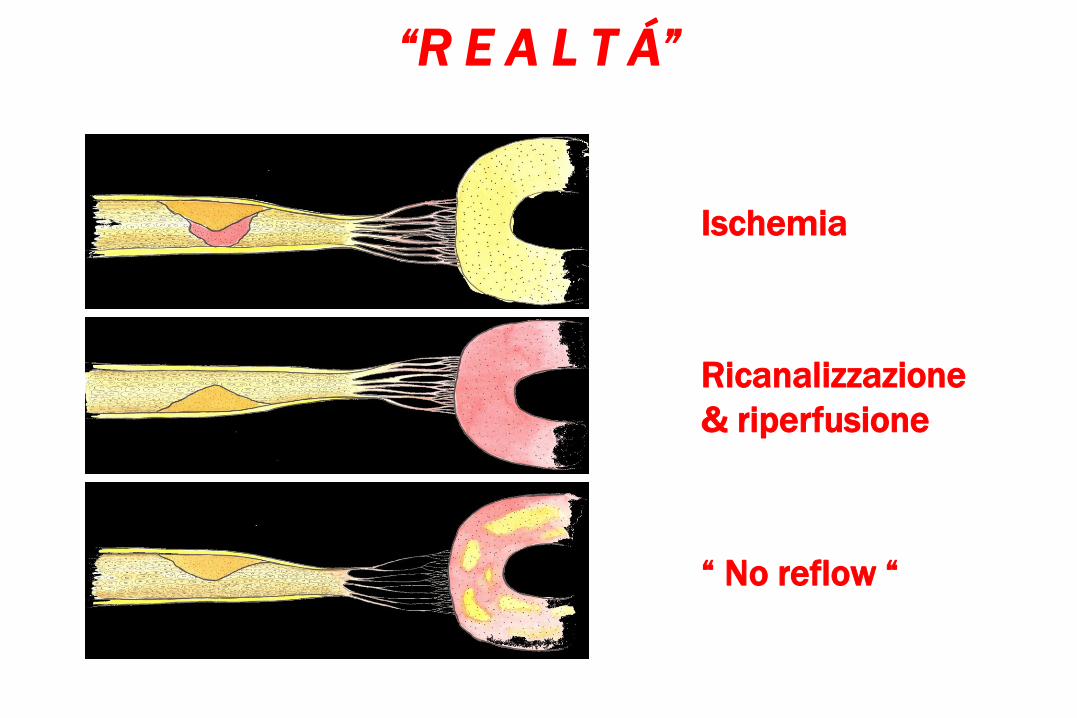
Ischemia
Ricanalizzazione
& riperfusione
“ No reflow “
“R E A L T Á”

Activation of RAS and SNS
Growth andfibrosis
Ischemia andEnergy depletion
Apoptosis
CAD progression
Necrosis
RemodelingRemodeling
Altered geneexpression
Myocardial DisfunctionMyocardial Disfunction Reinfarction
Cell DeathCell Death
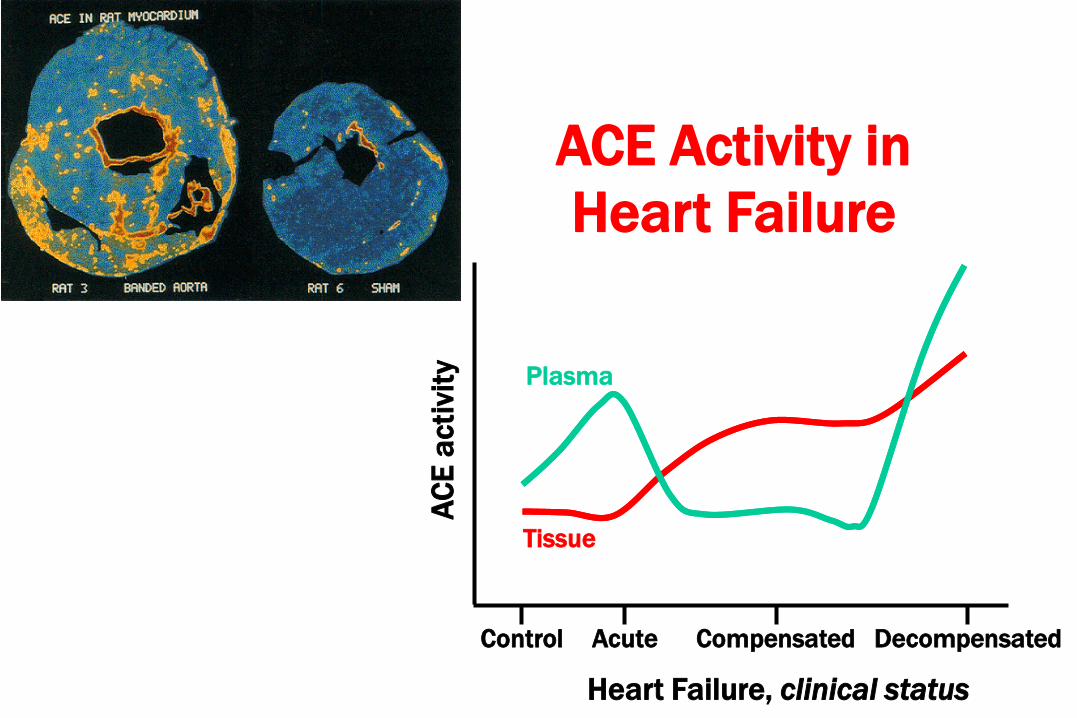
Control Acute Compensated Decompensated
Heart Failure, clinical status
AC
E a
cti
vity
Tissue
Plasma
ACE Activity in
Heart Failure
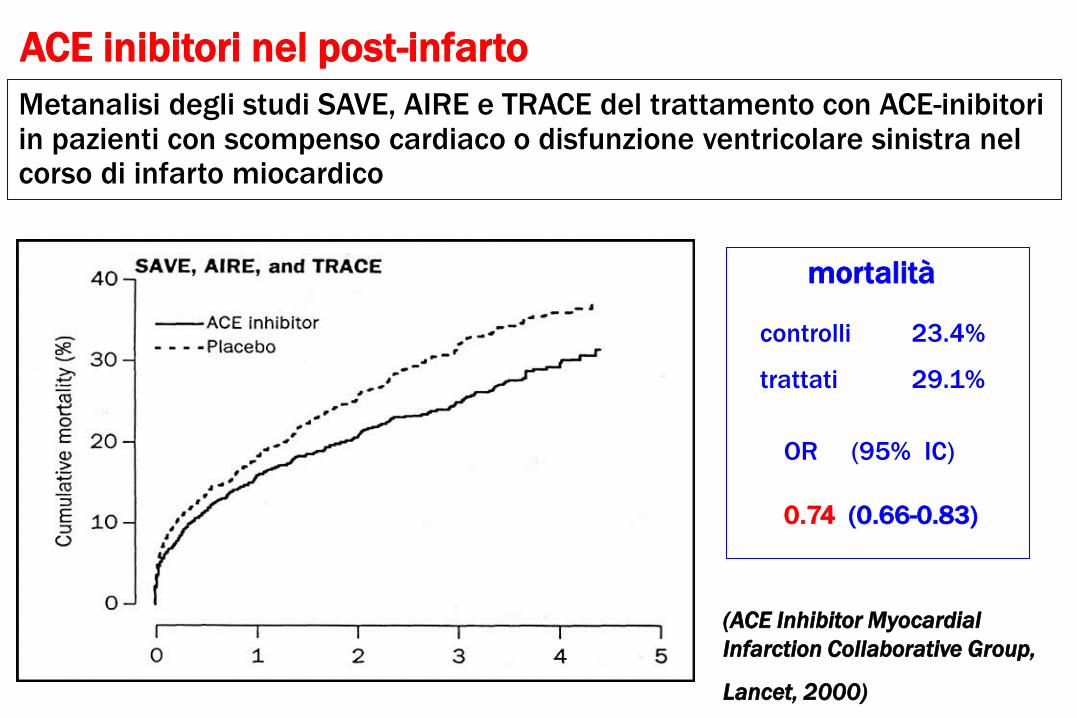
Metanalisi degli studi SAVE, AIRE e TRACE del trattamento con ACE-inibitori in pazienti con scompenso cardiaco o disfunzione ventricolare sinistra nel corso di infarto miocardico
(ACE Inhibitor Myocardial
Infarction Collaborative Group,
Lancet, 2000)
mortalità
controlli
trattati
23.4%
29.1%
OR (95% IC)
0.74 (0.66-0.83)
ACE inibitori nel post-infarto
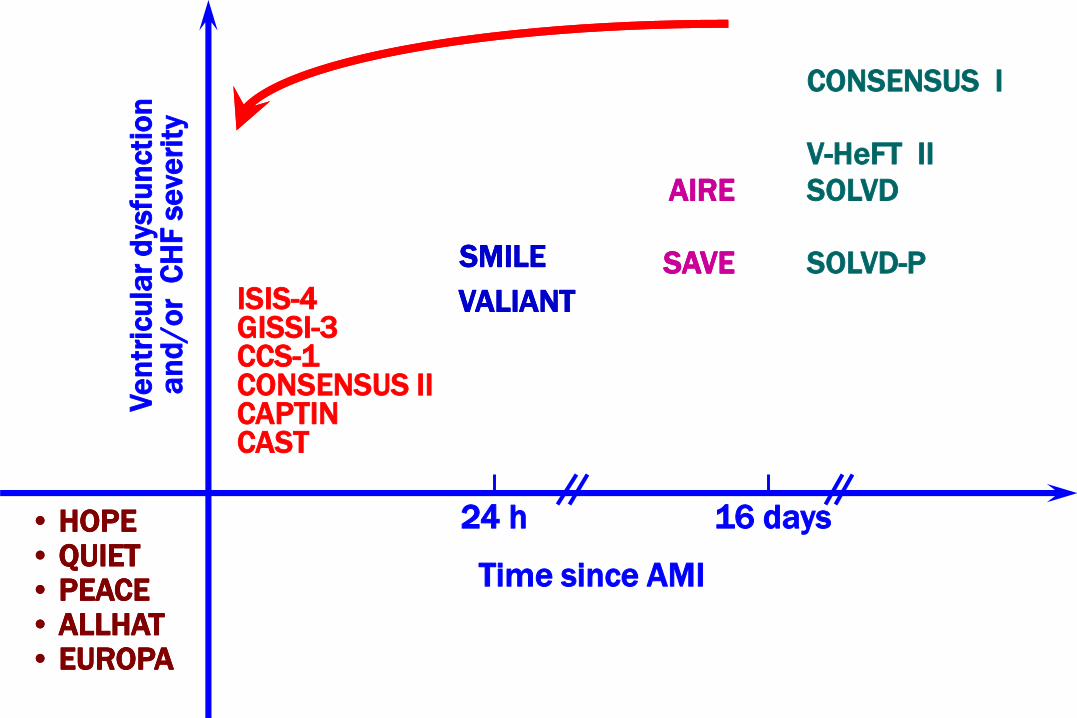
CONSENSUS I
V-HeFT II
SOLVD
SOLVD-P
Ve
ntr
icu
lar
dysfu
ncti
on
an
d/o
r C
HF
se
veri
ty
Time since AMI
24 h 16 days
ISIS-4GISSI-3CCS-1CONSENSUS IICAPTINCAST
• HOPE• QUIET• PEACE• ALLHAT• EUROPA
• HOPE• QUIET• PEACE• ALLHAT• EUROPA
SMILESMILE
AIRE
SAVE
AIRE
SAVE
VALIANTVALIANT
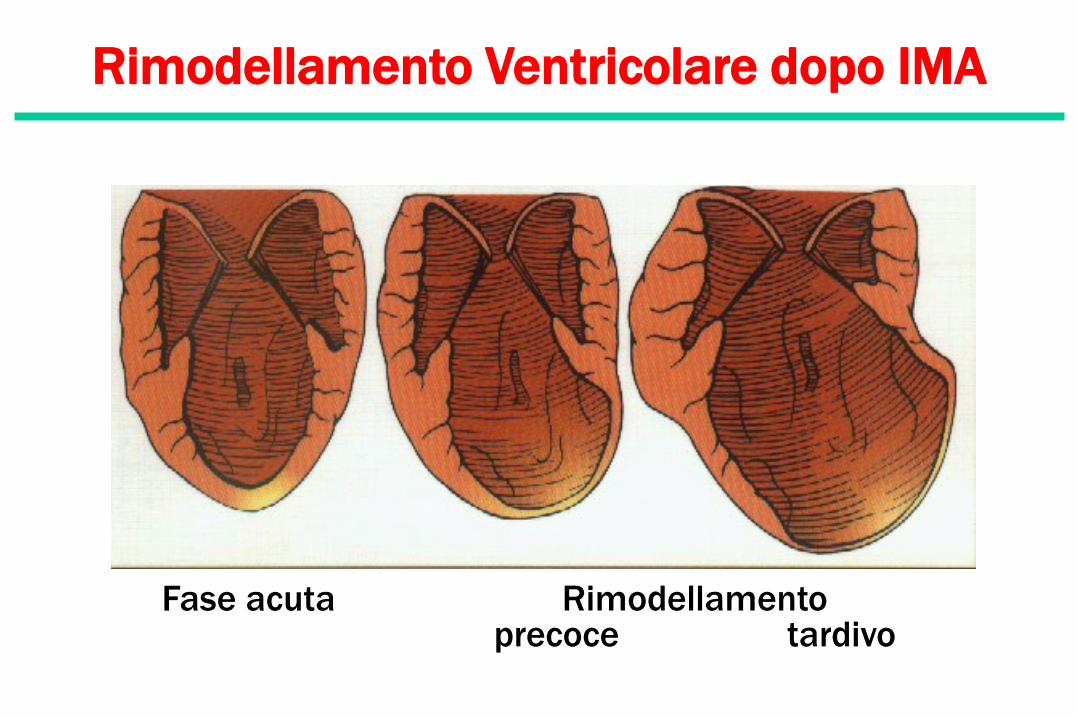
Rimodellamento Ventricolare dopo IMA
Fase acuta Rimodellamentoprecoce tardivo

0
5
10
15
20
25
30
35
0 1 2 3 6 9 12
An
gio
ten
sin
a I
I (p
g/m
l)
0
40
80
120
160
Ald
oste
ron
e (p
g/m
l)
Il Fenomeno dell’Escape del Sistema RAAin Corso di ACE-inibizione
mesi
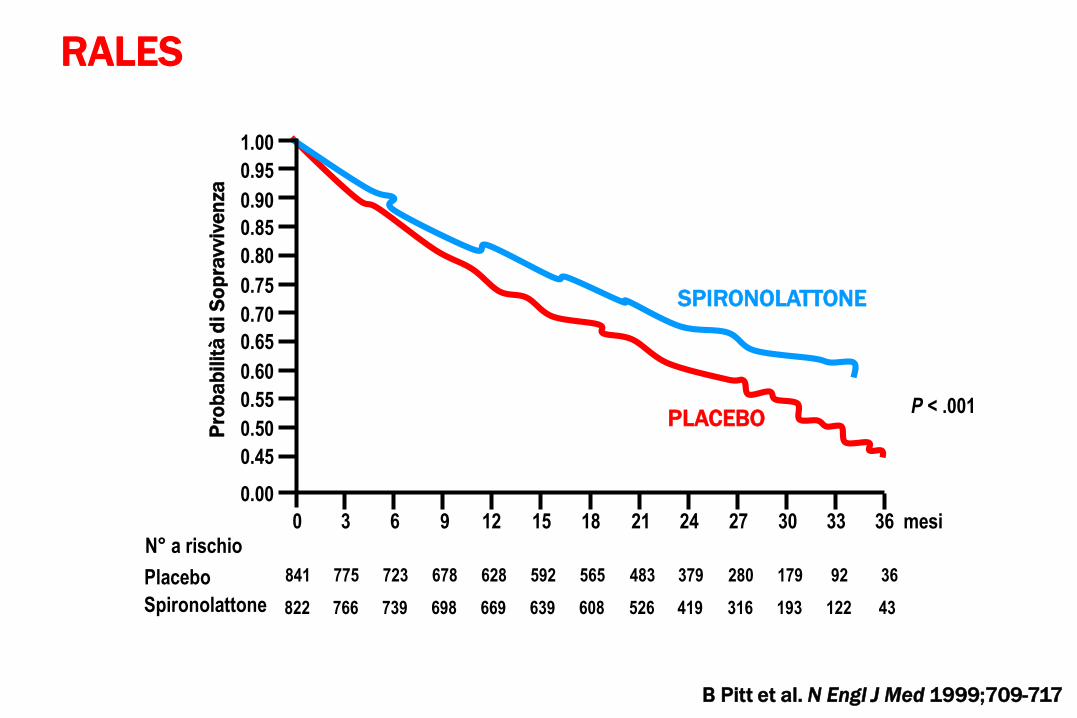
SPIRONOLATTONE
PLACEBO
Pro
ba
bilit
à d
i S
op
ravvi
ven
za
0 3 6 9 12 15 18 21 24 27 30 33 36 mesi
P < .001
0.00
0.45
0.50
0.55
0.60
0.65
0.70
0.75
0.80
0.85
0.90
0.95
1.00
Placebo
Spironolattone
N° a rischio
841 775 723 678 628 592 565 483 379 280 179 92 36
822 766 739 698 669 639 608 526 419 316 193 122 43
B Pitt et al. N Engl J Med 1999;709-717
RALES

Pharmacologic Effects
vs
Biologic Effects

Le “sorprese” dei grandi trial
Ace-inibitori, sartani e ....
• prevenzione primaria della disfunzione
ventricolare e dello scompenso
•prevenzione degli eventi coronarici
• prevenzione degli eventi cerebrovascolari
• prevenzione della fibrillazione atriale
• prevenzione del diabete mellito
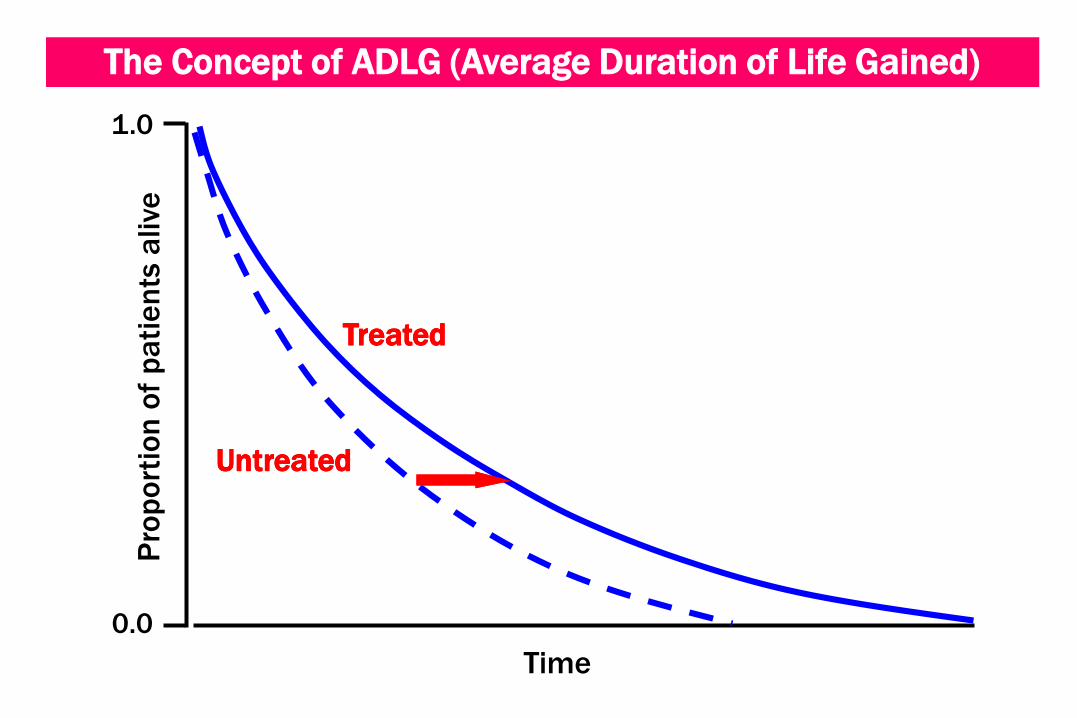
The Concept of ADLG (Average Duration of Life Gained)
Time
Pro
po
rtio
n o
f p
ati
en
ts a
live
TreatedTreated
UntreatedUntreated
1.0
0.0

Qual’ è la reale capacità degli ACE-I di prolungare la sopravvivenza ?
ADLG
9 mesi
3 mesi
1 mese
15 mesi
rischio relativo
27 %
16 %
7 %
18 %
Modello clinico
CONSENSUS I
SOLVD
GISSI / ISIS / CCS
TRACE

Randomised Clinical Trials in CHF
Trial
CONSENSUSRALESCOPERNICUSBESTCIBIS IIV-HeFT IISOLVD-TUS CARVEDILOLMERIT-HFSAVEELITE IIVal-HeFTELITE I
Annualized placebomortality rate
58.0 %24.0 % 18.5 %16.6 %13.2 %12.5 %11.8 %11.1 %11.0 %10.5 %10.4 %10.0 %8.7 %
HEART FAILURE
Pathophysiological Abnormalities
structural remodeling and dilation of LV
reduced myocytes shortening and wall motion
Na retention and circulatory congestion
vasoconstriction and vascular remodeling
neurohormonal activation

ATTIVAZIONE SIMPATICACONSEGUENZE SFAVOREVOLI
• Aumento del lavoro cardiaco
• Riduzione della perfusione coronarica
• Aumento del pre e post-carico
• Ritenzione idrica e congestione del circolo
• Ischemia e necrosi miocardica
• Ipokaliemia e aritmie
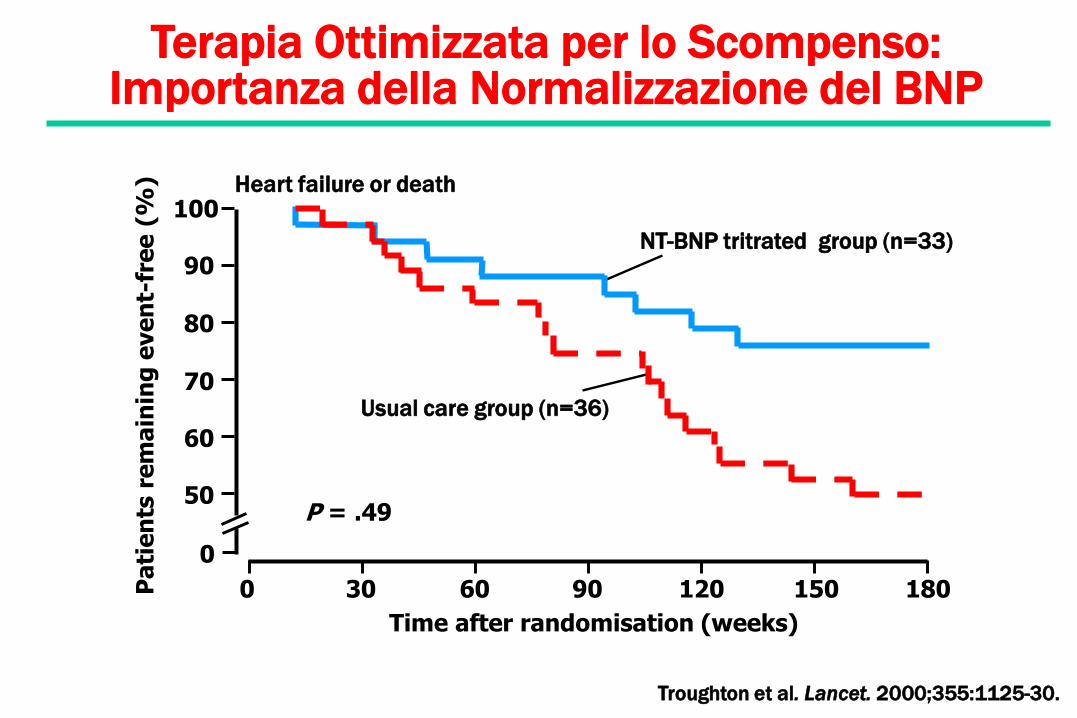
Terapia Ottimizzata per lo Scompenso: Importanza della Normalizzazione del BNP
Troughton et al. Lancet. 2000;355:1125-30.
NT-BNP tritrated group (n=33)
Usual care group (n=36)
Time after randomisation (weeks)
0 30 60 90 120 150 180
Heart failure or death
Pa
tie
nts
re
ma
inin
g e
ve
nt-
fre
e (
%)
0
50
60
70
80
90
100
P = .49

Tempo (mesi)
* BNP
Plasmatico
(pg/mL)
n = 844 PlaceboBasale = 177.6
ValsartanBasale = 183.5
n = 1890
n = 1710
n = 1850n = 1633
n = 823
P < 0.001 P < 0.001P < 0.001
0 4 12 24-40
-30
-20
-10
0
10
20
Latini R et al. J Card Fail. 2001;7(Suppl 2):Abstract 198.
Variazione dei Livelli Plasmatici di BNP
*Media ± SEM

Trial n Reduction in p value
relative risk
CIBIS-I 641 -20% ns
CIBIS-II 2647 -34% p<0.0001
ANZ 415 -23% ns
US Carvedilol 1094 -65% p<0.001
MERIT-HF 3991 -34% p=0.0062*
*Adjusted for two interim analyses
-Blockade in Mild-to-Moderate Heart FailureMortality Reduction
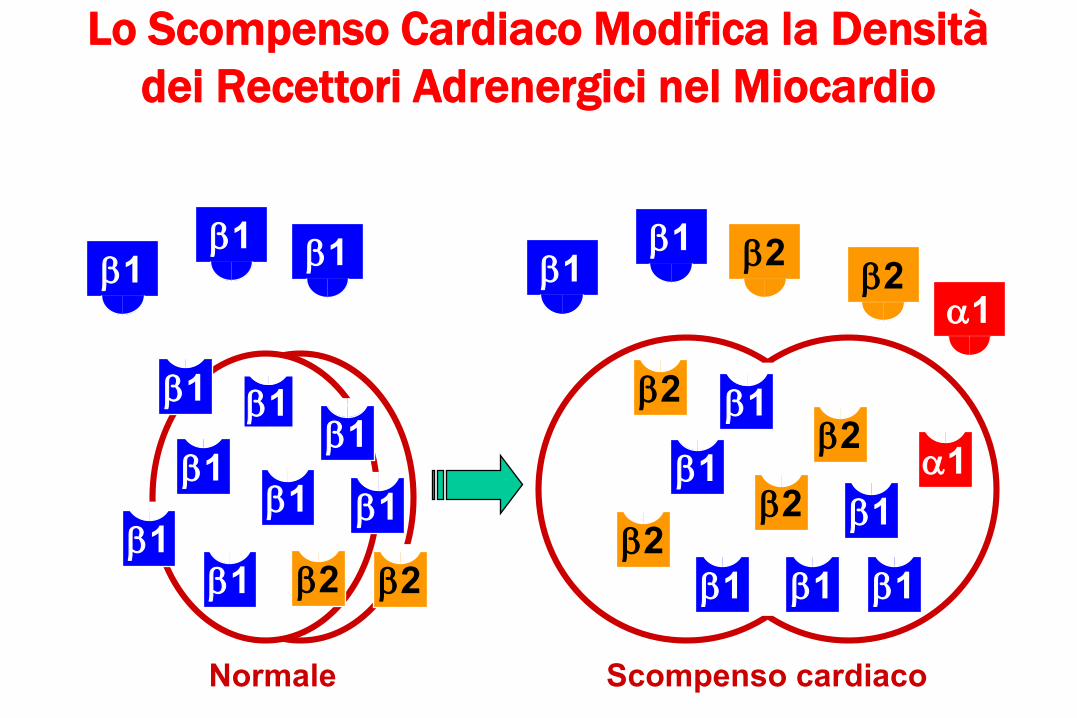
Normale
1 11
11
11
1
2 2
11 1
Scompenso cardiaco
1
2
2
2
2
1
1 1
1
1
11 2
2a1
a1
Lo Scompenso Cardiaco Modifica la Densità
dei Recettori Adrenergici nel Miocardio
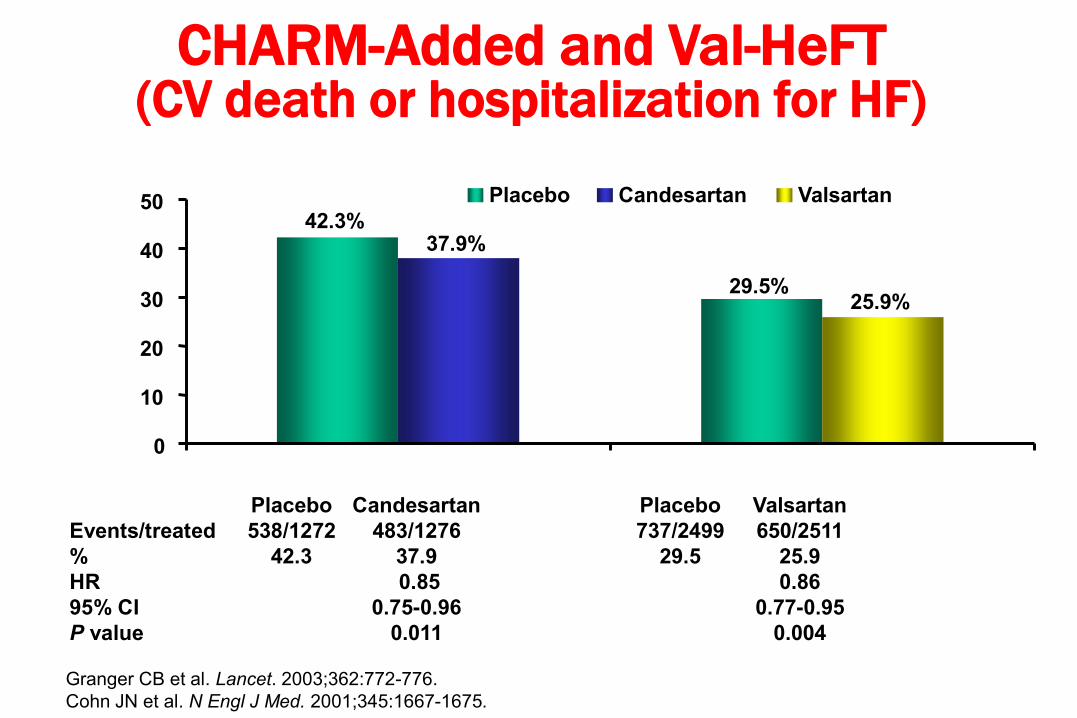
CHARM-Added and Val-HeFT (CV death or hospitalization for HF)
Placebo Candesartan Placebo Valsartan
Events/treated 538/1272 483/1276 737/2499 650/2511
% 42.3 37.9 29.5 25.9
HR 0.85 0.86
95% CI 0.75-0.96 0.77-0.95
P value 0.011 0.004
%
42.3%
29.5%
37.9%
25.9%
0
10
20
30
40
50
CHARM Val-HeFT
Placebo Candesartan Valsartan
Granger CB et al. Lancet. 2003;362:772-776.
Cohn JN et al. N Engl J Med. 2001;345:1667-1675.

CHARM-Added: Prespecified subgroups, CV death or CHF hosp.
Beta- Yes 223/702 274/711
blocker No 260/574 264/561
Recom. Yes 232/643 275/648
dose of No 251/633 263/624
ACE inhib.
All patients 483/1276 538/1272
Candesartan Placebo
candesartan better
Hazard ratio
placebo better
0.6 0.8 1.0 1.2 1.4
p-value fortreatment interaction
0.14
0.26

Komajda M et al. Eur Heart J 2003
Utilisation of Blockade for CHFin Clinical Practice
32.721.2 20.5 17.2
61.8
36.9 35.7
86.9
0
50
100

Perceptions
Regarding Tolerability of Blockade in CHF
• Complexity in initiation and up-titration
• Risk of intolerance and / or worsening of CHF symptom status esp. with initiation
• Delay in beneficial effects on outcomes
• All of the above esp. true in patients with advanced disease
Cardiologo
Internista Geriatra
Medico di MG
Esistono differenze di trattamento
a seconda dei medici?

Cardiologi Internisti P
NYHA I-II <15% 50% 0.01
Età media 68±19 72±6 0.01
Ecocardiogramma 49% 34% 0.01
Uso diuretici 87% 76% 0.02
Inotropi ev 9% 1,3% 0.02
Reospedalizzazione 30% 44% 0.04
Reis SE et al. J Am Coll Cardiol 1997;30:733-8
CHF Hospitalization: Specialty Related
Disparities in Practice Patterns and Outcome

Cardiologi GP P
Maschi 78% 42% <0.001
Età Media 64,2 78,2 <0.001
Eco 97% 12% <0.001
Rx Torace 84% 51% <0.001
Coronarografia 26% 3% <0.001
C. Ischemica 56% 31% <0.001
ACE-I 76% 40% <0.001
Betabloccanti 30% 8,7% <0.001
Spironolattone 32% 11% <0.001
Dicumarolici 29% 6,8% <0.001
Rutten FH et al. Eur J Heart Failure 2003;5:337-44
Differences Between Practioners and Cardiologists in
Diagnosis and Management of Heart Failure: A Survey in
Every-day Practice
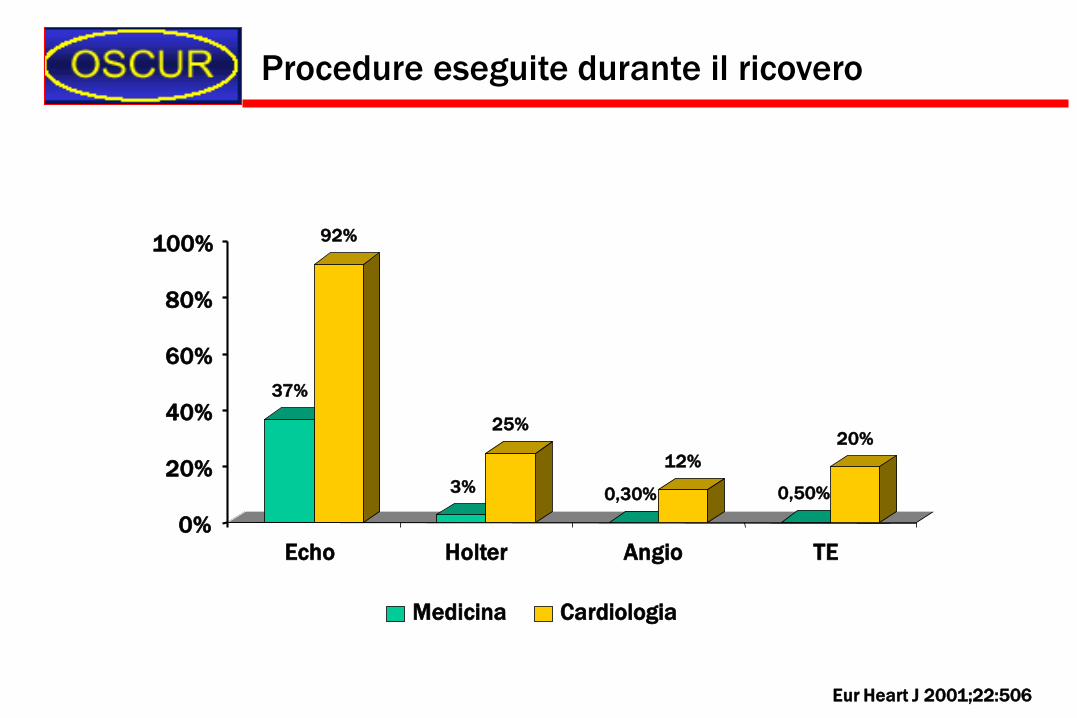
37%
92%
3%
25%
0,30%
12%
0,50%
20%
0%
20%
40%
60%
80%
100%
Echo Holter Angio TE
Medicina Cardiologia
Procedure eseguite durante il ricovero
Eur Heart J 2001;22:506

75%
16%
9%
0%
10%
20%
30%
40%
50%
60%
70%
80%
Medicina Cardiologia Altri Reparti
DRG 127 in Lombardia, Liguria e Toscana
1997
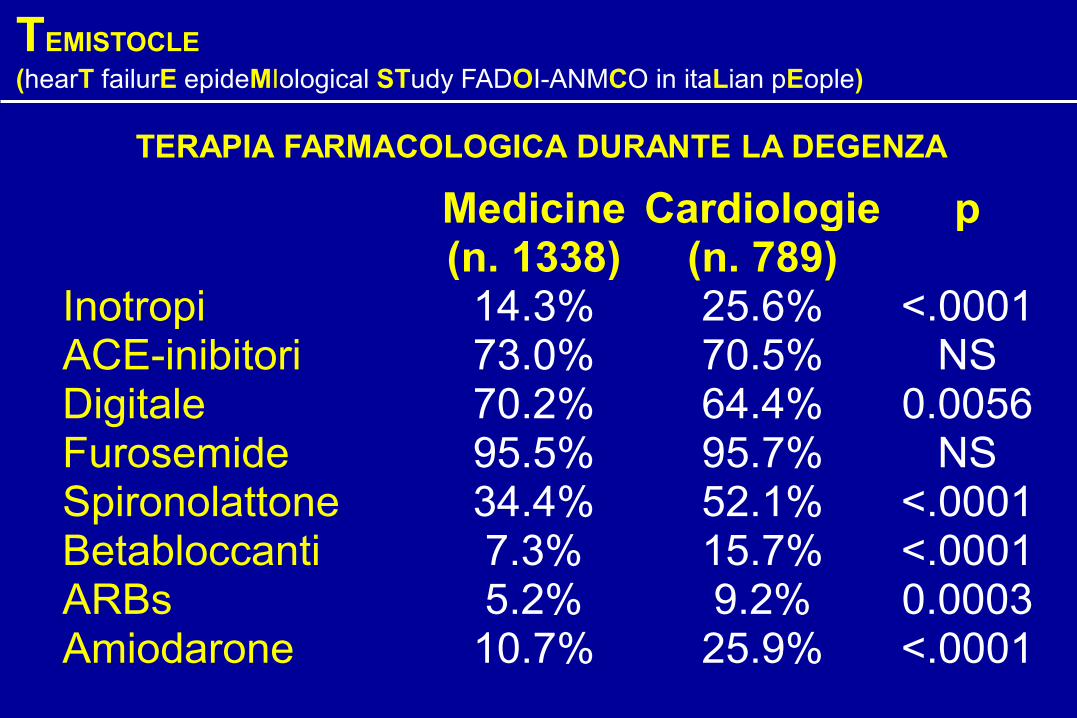
TERAPIA FARMACOLOGICA DURANTE LA DEGENZA
TEMISTOCLE
(hearT failurE epideMIological STudy FADOI-ANMCO in itaLian pEople)
Medicine(n. 1338)
Cardiologie(n. 789)
p
Inotropi 14.3% 25.6% <.0001ACE-inibitori 73.0% 70.5% NSDigitale 70.2% 64.4% 0.0056Furosemide 95.5% 95.7% NSSpironolattone 34.4% 52.1% <.0001Betabloccanti 7.3% 15.7% <.0001ARBs 5.2% 9.2% 0.0003Amiodarone 10.7% 25.9% <.0001

TERAPIA FARMACOLOGICA ALLA DIMISSIONE
TEMISTOCLE
(hearT failurE epideMIological STudy FADOI-ANMCO in itaLian pEople)
Medicine(n. 1259)
Cardiologie(n. 748)
p
Inotropi 5.9% 5.2% NSACE-inibitori 75.8% 71.0% 0.02Digitale 61.5% 59.9% NSFurosemide 85.5% 89.6% 0.0082Spironolattone 31.3% 49.1% <.0001Betabloccanti 8.7% 17.8% <.0001ARBs 6.2% 9.2% 0.012Amiodarone 8.1% 22.9% <.0001

Chi Deve Fare Che Cosa?

The explosion in HF devices, part 1: Culture,
economics, and unresolved issues
This represents a real ethical dilemma that in this country we tend not to be very good at facing directly
I think there is an ethical imperative to consider implanting these devices into all these patients
In Sweden there is not the money for this, so we don't screen
Some cardiologists are leaping onto devices as cure-alls when patients aren't even on maximal medical therapy
The trial experience is in a relatively select group
We may be changing their mode of death from a sudden arrhythmic death to drowning by heart failure
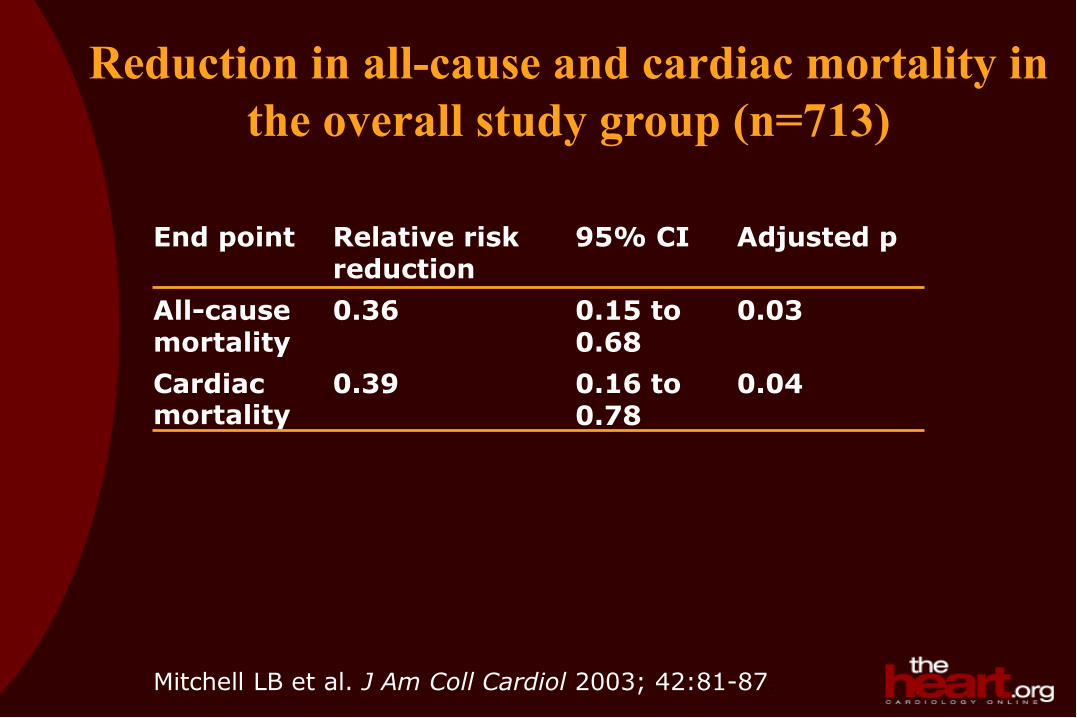
Reduction in all-cause and cardiac mortality in
the overall study group (n=713)
0.03 0.15 to 0.68
0.36 All-cause mortality
0.04 0.16 to 0.78
0.39 Cardiac mortality
Adjusted p 95% CI Relative risk reduction
End point
Mitchell LB et al. J Am Coll Cardiol 2003; 42:81-87.

Changes in Plasma Ang II Levels During Ang I Infusion
Ueda S et al. Hypertension 1998
0 5 10 15 20 0 5 10 15 20
0 5 10 15 20
0
50
100
150
200
250
300
0 5 10 15 20
Ch
an
ge
in
Pla
sm
a A
ng
II (p
mo
l/l)
Ang I (ng/Kg/ml)
II
II
DD
DD
enalaprilat
placebo1 hour
10 hours
0
50
100
150
200
250
300
0
50
100
150
200
250
300
0
50
100
150
200
250
300
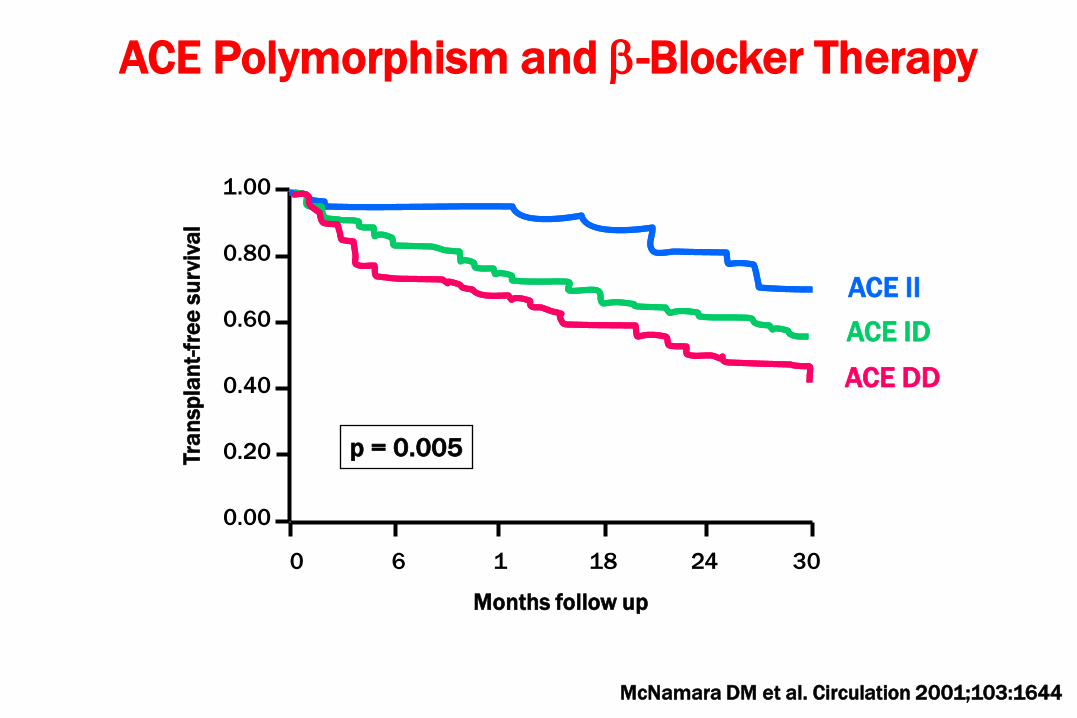
0 6 1 18 24 30
1.00
0.80
0.60
0.40
0.20
0.00
Months follow up
Tra
nsp
lan
t-fr
ee
su
rviv
al
ACE II
ACE ID
ACE DD
p = 0.005
ACE Polymorphism and -Blocker Therapy
McNamara DM et al. Circulation 2001;103:1644

0 6 1 18 24 30
1.00
0.80
0.60
0.40
0.20
0.00
Months follow up
Tra
nsp
lan
t-fr
ee
su
rviv
al
p = 0.007
No b-blocker
b-blocker
DD genotype
ACE Polymorphism and -Blocker Therapy
McNamara DM et al. Circulation 2001;103:1644



















