CASE REPORT Right coronary artery originating from the ...
2
CASE REPORT Right coronary artery originating from the distal left circumflex artery, evaluation using three imaging techniques Murat Turfan, I Cemalettin Aydın, II Mehmet Ali Elbey, III Ercan Erdog ˘ an, I Emin Asoglu, I Halil Basel, II O ¨ mer Go ¨ ktekin I I Bezmialem University, Faculty of Medicine, Department of Cardiology, Istanbul/Turkey. II Bezmialem University, Faculty of Medicine, Department of Cardiovascular Surgery, Istanbul/Turkey. III Dicle University, Faculty of Medicine, Department of Cardiology, Adnan Menderes Bulvarı Fatih, Istanbul/ Turkey. Email: [email protected] Tel.: 90 505 3197199 INTRODUCTION An isolated single coronary artery is extremely rare, with an incidence of 0.024% to 0.066% in the general population (1), and many patients with coronary artery anomalies are asymptomatic. However, some of these anomalies can lead to sudden death. In this report, we describe a rare case using three different imaging methods. CASE DESCRIPTION A 58-year-old man presented with exertional dyspnea and chest pain. His physical examination was normal, except for an apical, third-degree systolic murmur. The ECG showed normal sinus rhythm without any ischemic changes. Transthoracic echocardiography showed severe mitral valve insufficiency, and the left ventricular chamber size was in the normal range. The patient was then evaluated using 64-slice multidetector computed tomogra- phy of the coronary arteries, which revealed an anomalous single coronary artery arising from the left sinus of Valsalva and the absence of the right coronary artery (RCA). The left circumflex coronary artery (LCx) was the dominant vessel. It appeared to continue, without signifi- cant stenosis, beyond the atrioventricular groove up to the level normally occupied by the RCA (Figure 1). Mid-grade stenoses were observed in the middle segment of the left anterior descending coronary artery (LAD). The patient was symptomatic, and it was therefore decided that mitral valve surgery should be performed. Selective coronary angiogra- phy showed a normal left main coronary artery originating from the left sinus of Valsalva. Left coronary arteriography showed 90% stenosis in the mid portion of the LAD, and the left circumflex artery was a dominant vessel, with an aberrant branch from the distal left circumflex artery that crossed the crux and continued to the right atrioventricular groove. The vessel terminated near the right sinus of Valsalva (Figure 2). Right coronary arteriography could not be performed because the right coronary ostium was not present, which was also confirmed by aortography (Figure 3). The patient underwent mitral valve surgery, and during surgery, the right coronary artery ostium was not observed (Figure 4). DISCUSSION Lipton et al. classified single coronary arteries into nine patterns according to the site of origin and the anatomical distribution of the branch of the coronary artery (2). Our Copyright ß 2012 CLINICS – This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http:// creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non- commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. No potential conflict of interest was reported. Figure 1 - In the CT image, the LCx was the dominant vessel. It appeared to continue beyond the atrioventricular groove up to the level normally occupied by the RCA. CLINICS 2012;67(12):1517-1518 DOI:10.6061/clinics/2012(12)28 1517
Transcript of CASE REPORT Right coronary artery originating from the ...

CASE REPORT
Right coronary artery originating from the distal leftcircumflex artery, evaluation using three imagingtechniquesMurat Turfan,I Cemalettin Aydın,II Mehmet Ali Elbey,III Ercan Erdogan,I Emin Asoglu,I Halil Basel,II
Omer GoktekinI
I Bezmialem University, Faculty of Medicine, Department of Cardiology, Istanbul/Turkey. II Bezmialem University, Faculty of Medicine, Department of
Cardiovascular Surgery, Istanbul/Turkey. III Dicle University, Faculty of Medicine, Department of Cardiology, Adnan Menderes Bulvarı Fatih, Istanbul/
Turkey.
Email: [email protected]
Tel.: 90 505 3197199
INTRODUCTION
An isolated single coronary artery is extremely rare, withan incidence of 0.024% to 0.066% in the general population(1), and many patients with coronary artery anomalies areasymptomatic. However, some of these anomalies can leadto sudden death. In this report, we describe a rare case usingthree different imaging methods.
CASE DESCRIPTION
A 58-year-old man presented with exertional dyspneaand chest pain. His physical examination was normal,except for an apical, third-degree systolic murmur. The ECGshowed normal sinus rhythm without any ischemicchanges. Transthoracic echocardiography showed severemitral valve insufficiency, and the left ventricular chambersize was in the normal range. The patient was thenevaluated using 64-slice multidetector computed tomogra-phy of the coronary arteries, which revealed an anomaloussingle coronary artery arising from the left sinus of Valsalvaand the absence of the right coronary artery (RCA).
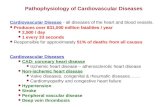
The left circumflex coronary artery (LCx) was thedominant vessel. It appeared to continue, without signifi-cant stenosis, beyond the atrioventricular groove up to thelevel normally occupied by the RCA (Figure 1). Mid-gradestenoses were observed in the middle segment of the leftanterior descending coronary artery (LAD). The patient wassymptomatic, and it was therefore decided that mitral valvesurgery should be performed. Selective coronary angiogra-phy showed a normal left main coronary artery originatingfrom the left sinus of Valsalva. Left coronary arteriographyshowed 90% stenosis in the mid portion of the LAD, and theleft circumflex artery was a dominant vessel, with anaberrant branch from the distal left circumflex artery thatcrossed the crux and continued to the right atrioventricular
groove. The vessel terminated near the right sinus ofValsalva (Figure 2). Right coronary arteriography couldnot be performed because the right coronary ostium was notpresent, which was also confirmed by aortography(Figure 3). The patient underwent mitral valve surgery,and during surgery, the right coronary artery ostium wasnot observed (Figure 4).
DISCUSSION
Lipton et al. classified single coronary arteries into ninepatterns according to the site of origin and the anatomicaldistribution of the branch of the coronary artery (2). Our
Copyright � 2012 CLINICS – This is an Open Access article distributed underthe terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided theoriginal work is properly cited.
No potential conflict of interest was reported.
Figure 1 - In the CT image, the LCx was the dominant vessel. Itappeared to continue beyond the atrioventricular groove up tothe level normally occupied by the RCA.
CLINICS 2012;67(12):1517-1518 DOI:10.6061/clinics/2012(12)28
1517

case had an anomalous coronary artery (L-1 subtype) thatoriginated from the left sinus of Valsalva, branched from theLCx in a normal fashion, and then continued in theatrioventricular groove up to the level of the RCA.
AUTHOR CONTRIBUTIONS
Turfan M was responsible for the manuscript writing and review. Aydin C,
Elbey MA and Basel H were responsible for the patient diagnosis. Erdogan
E was responsible for the data analysis. Asoglu E was responsible for the
literature search and Goktekin O was responsible for the manuscript
content and editing.
REFERENCES
1. Desmet W, Vanhaecke J, Vrolix M, Van de Werf F, Piessens J, Willems J,et al. Isolated single coronary artery: a review of 50,000 consecutivecoronary angiographies. Eur Heart J. 1992;13(12):1637-40.
2. Lipton MJ, Barry WH, Obrez I, Silverman JF, Wexler L. Isolated singlecoronary artery: diagnosis, angiographic classification, and clinicalsignificance. Radiology. 1979;130(1):39-47.
Figure 2 - The LCx was a dominant vessel, with an aberrantbranch from the distal left circumflex artery that crossed the cruxand continued to the right atrioventricular groove.
Figure 3 - No right coronary ostium was observed usingaortography.
Figure 4 - During surgery, the right coronary artery ostium wasnot observed.
RCA originating from the distal left cx arteryTurfan M et al.
CLINICS 2012;67(12):1517-1518
1518