![Inflammation and cancer: How hot is the link? · carcinoma [30], colon carcinoma, lung carcinoma, squamous cell carcinoma, pancreatic cancer [31,32], ovarian carcinoma biochemical](https://static.fdocuments.net/doc/165x107/5fcdd6c81c76a34db570e7e6/iniammation-and-cancer-how-hot-is-the-link-carcinoma-30-colon-carcinoma.jpg)
Case Report Primary combined small cell carcinoma of ... · extension to left supraglottis, and had...
7
Introduction Small cell carcinoma neuroendocrine type (SCCNET) is an unusual neoplasm accounting for only 0.5% of all laryngeal carcinomas, and in western countries is often related to smoking and alcohol abuse [1,2]. When SCCNET is asso- ciated with a squamous or adenocarcinoma component, these tumors are referred to as combined or composite carcinomas [1,2]. The combined carcinomas are reportedly unusual, represent less than 10% of all the SCCNETs of larynx [2], and are summarized in Table 1. Most of these cases have been associated with a squamous cell carcinoma, either in-situ or inva- sive. The few reported cases have been mostly males in sixth and seventh decades of life, most commonly occurring in supraglottic region fol- lowed by glottis. However, the metastatic pat- tern of spread of combined carcinomas has not been described accurately with regards to its individual components. In this report, we de- scribe an unusual case of combined carcinoma of larynx, in which the small cell and squamous cell carcinoma components were lateralized to either side of larynx, a pattern which was also reproduced in its metastatic neck nodal spread. The diagnostic, management and histogenetic implications are discussed. Case presentation A 59-year-old white male presented with a 5- month history of worsening hoarseness, pro- Int J Clin Exp Pathol 2011;4(1): 111-117 www.ijcep.com /IJCEP1010001 Case Report Primary combined small cell carcinoma of larynx with lat- eralized histologic components and corresponding side- specific neck nodal metastasis: report of a unique case and review of literature Gitika Aggarwal 1 , Lana Jackson 2 , Suash Sharma 1 Departments of Pathology 1 and Otolaryngology 2 , Medical College of Georgia, Augusta, GA 30912. Received October 10, 2010; accepted November 25, 2010; Epub December 3, 2010; published January 1, 2011 Abstract: Combined small cell carcinoma (neuroendocrine) of the larynx has been rarely reported in the literature, and included in the current WHO classification. We hereby report an unusual case of combined carcinoma of the larynx; composed mainly of small cell neuroendocrine carcinoma nearly confined to the right side (mainly involving supraglottis extending to glottis) with synchronous minor in-situ and invasive squamous cell carcinoma component located on the left side of larynx (mainly glottis). Interestingly, this side-specific distribution of tumor was recapitu- lated in its metastatic nodal spread; so that right cervical lymph nodes showed only metastatic small cell carcinoma and left cervical lymph nodes only metastatic squamous cell carcinoma. To the best of our knowledge, the present case is the seventeenth reported case of a combined small cell carcinoma of larynx, second case in which individual tumor components were lateralized on either side of larynx, and the first case in which this side-specificity of tumor was reflected in its metastatic neck nodal spread. This report emphasizes the value of accurate pathologic diagnosis including diversity in differentiation and localization of laryngeal tumors, and underscores the need for thorough pathologic examination of bilateral laryngeal tumors. The pre-operative diagnostic yield of small cell carcinoma (pure or combined) can be enhanced by including deeper submucosal biopsies on laryngoscopy in all those cases in which the extent of disease on imaging is disproportionately larger than the apparent mucosal involvement on laryngo- scopy. This approach can facilitate selection of neoadjuvant or palliative chemo-radiotherapy in large or unresectable tumors. Keywords: larynx, combined small cell carcinoma, small cell carcinoma, squamous cell carcinoma, deeper biopsies, nodal metastatic carcinoma
Transcript of Case Report Primary combined small cell carcinoma of ... · extension to left supraglottis, and had...

Introduction Small cell carcinoma neuroendocrine type (SCCNET) is an unusual neoplasm accounting for only 0.5% of all laryngeal carcinomas, and in western countries is often related to smoking and alcohol abuse [1,2]. When SCCNET is asso-ciated with a squamous or adenocarcinoma component, these tumors are referred to as combined or composite carcinomas [1,2]. The combined carcinomas are reportedly unusual, represent less than 10% of all the SCCNETs of larynx [2], and are summarized in Table 1. Most of these cases have been associated with a squamous cell carcinoma, either in-situ or inva-sive. The few reported cases have been mostly males in sixth and seventh decades of life, most
commonly occurring in supraglottic region fol-lowed by glottis. However, the metastatic pat-tern of spread of combined carcinomas has not been described accurately with regards to its individual components. In this report, we de-scribe an unusual case of combined carcinoma of larynx, in which the small cell and squamous cell carcinoma components were lateralized to either side of larynx, a pattern which was also reproduced in its metastatic neck nodal spread. The diagnostic, management and histogenetic implications are discussed. Case presentation A 59-year-old white male presented with a 5-month history of worsening hoarseness, pro-
Int J Clin Exp Pathol 2011;4(1): 111-117 www.ijcep.com /IJCEP1010001
Case Report Primary combined small cell carcinoma of larynx with lat-eralized histologic components and corresponding side-specific neck nodal metastasis: report of a unique case and review of literature Gitika Aggarwal1, Lana Jackson2, Suash Sharma1 Departments of Pathology1 and Otolaryngology2, Medical College of Georgia, Augusta, GA 30912. Received October 10, 2010; accepted November 25, 2010; Epub December 3, 2010; published January 1, 2011 Abstract: Combined small cell carcinoma (neuroendocrine) of the larynx has been rarely reported in the literature, and included in the current WHO classification. We hereby report an unusual case of combined carcinoma of the larynx; composed mainly of small cell neuroendocrine carcinoma nearly confined to the right side (mainly involving supraglottis extending to glottis) with synchronous minor in-situ and invasive squamous cell carcinoma component located on the left side of larynx (mainly glottis). Interestingly, this side-specific distribution of tumor was recapitu-lated in its metastatic nodal spread; so that right cervical lymph nodes showed only metastatic small cell carcinoma and left cervical lymph nodes only metastatic squamous cell carcinoma. To the best of our knowledge, the present case is the seventeenth reported case of a combined small cell carcinoma of larynx, second case in which individual tumor components were lateralized on either side of larynx, and the first case in which this side-specificity of tumor was reflected in its metastatic neck nodal spread. This report emphasizes the value of accurate pathologic diagnosis including diversity in differentiation and localization of laryngeal tumors, and underscores the need for thorough pathologic examination of bilateral laryngeal tumors. The pre-operative diagnostic yield of small cell carcinoma (pure or combined) can be enhanced by including deeper submucosal biopsies on laryngoscopy in all those cases in which the extent of disease on imaging is disproportionately larger than the apparent mucosal involvement on laryngo-scopy. This approach can facilitate selection of neoadjuvant or palliative chemo-radiotherapy in large or unresectable tumors. Keywords: larynx, combined small cell carcinoma, small cell carcinoma, squamous cell carcinoma, deeper biopsies, nodal metastatic carcinoma

Primary combined small cell carcinoma of larynx
112 Int J Clin Exp Pathol 2011;4(1):111-117
gressive otalgia and hemoptysis. He was also noted to have progressive dysphagia and aspi-ration with solids. There was no history of weight loss. His past medical history was signifi-cant for myocardial infarction and degenerative joint disease with back pain and arthritis. He quit alcohol consumption 20 years ago but had been smoking 3 packs per day of tobacco for 40 years. He had a positive family history of coro-nary artery disease and cerebrovascular dis-ease but no history of any malignancy in the family. He underwent cervical spine surgery twice in the past and had a chest tube place-ment for spontaneous pneumothorax. On laryngoscopic examination, a large fungating tumor mass was noted involving the right pyri-form sinus and aryepiglottic fold, obliterating the ventricle. There was impaired mobility of the right true vocal cord, and the airway was noted to be marginal. The CT scan demon-strated a right transglottic mass invading the pre-epiglottic space, as well as with subglottic extension, and crossing midline to the left side. There were multiple metastatic neck nodes at the right 2B, 3 and 4 levels. However, no distant metastases were noted on the chest roentgeno-gram, abdominal sonogram, and bone scan. He underwent a total laryngectomy with right hemithyroidectomy and bilateral modified neck dissection. The frozen sections on all the sub-mitted margins were reported as negative for tumor.
Pathologic findings On gross examination of the laryngectomy speci-men, a 3.0 cm x 2.5 cm mass was palpable in-volving the right epiglottis and upper larynx. Se-rial sections revealed a large ill-defined 5.3 x 2.9 x 1.5 cm tumor mass located mainly in the right supraglottis and involving a portion of epi-glottis. The tumor extended inferiorly to involve right glottis and true vocal cord. The tumor also appeared to cross midline as a plaque like le-sion to involve left glottis and true vocal cord. The tumor had variable gross morphology rang-ing from ulcerated to nodular to plaque-like growth. The tumor infiltrated deeply to involve the thyroid cartilage. Cut surfaces of the submit-ted right hemithyroid were homogenous and tan-brown, without any gross involvement by the tumor. Microscopic sections from the larynx revealed a combined tumor, composed predominantly of small cell neuroendocrine carcinoma lateralized to the right side and squamous cell carcinoma to the left side. Majority of the tumor (>90%) involved right supraglottis with slight contiguous extension to left supraglottis, and had a his-tologic appearance of small cell carcinoma (Figure 1A). In contrast, the smaller plaque like tumor (<10%) involving left glottis showed mainly invasive squamous cell carcinoma with a small focus of in-situ squamous cell carcinoma (Figures 2A and 2B). Small cell carcinoma was deeply invasive reaching up to thyroid cartilage,
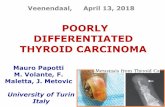
Figure 1. (A) Small cell carcinoma component showing infiltration by hyperchromatic, mitotically active small- sized tumor cells with frequent nuclear molding (H&Ex200). (B) Diffuse synaptophysin immunoreactivity in the small cell carcinoma component (synaptophysin x 200).

Primary combined small cell carcinoma of larynx
113 Int J Clin Exp Pathol 2011;4(1):111-117
whereas squamous cell carcinoma showed rela-tively superficial stromal invasion without thy-roid cartilage involvement. The two tumor com-ponents mostly showed a collision phase with distinct boundaries, but with a focus of gradual transition in one of the examined sections (Figure 3). All the surgical margins were free of tumor, however the tumor closely approached (~0.1 mm) the right anterior soft tissue margin. Neck lymph nodes showed metastatic carci-noma bilaterally. In right neck, the metastatic tumor involved 7 out of 14 right level II and 4 out of 6 right level III neck lymph nodes, and represented small cell neuroendocrine carci-noma morphology exclusively (Figure 4A). Right
level IIB (14) level IV (11) and superficial (3) lymph nodes were uninvolved. In left neck, only 1 out of 8 level IIB lymph nodes showed metas-tatic poorly differentiated squamous cell carci-noma (Figure 4B). Left level III (7), IV (4) and paratracheal (3) lymph nodes were all unin-volved. No metastatic small cell carcinoma was identified in the left neck nodes or soft tissue. Immunohistochemical profile of diffuse synapto-physin positivity in small cell neuroendocrine carcinoma component (Figure 1B) and CK5/6 and p63 positivity in squamous cell carcinoma component in the laryngectomy sections, sup-ported the histologic diagnosis. Immunostains for CK7, CK20 and chromogranin were nega-tive. The discohesive poorly differentiated neo-plastic cells in left neck level IIB lymph node showed immune-positivity for pankeratin, but were negative for pan-melanoma, CD45, CD30 and CD68, thereby confirming the histologic impression of metastatic squamous cell carci-noma. Discussion Primary laryngeal carcinomas constitute around 2% to 5% of all malignancies worldwide and approximately 12500 new cancer diagnoses in the United States every year [1]. Majority (95%) of the laryngeal carcinomas are primary squamous cell carcinomas. Neuroendocrine tumors of the larynx comprise only about 0.5% of all laryngeal tumors [2]. Pure small cell carci-noma of larynx was first described by Olofsson
Figure 2. (A) Invasive moderately differentiated squamous cell carcinoma component (H&Ex200).(B) In-situ and adjacent invasive squamous cell carcinoma component (H&Ex60).
Figure 3. Collision phase showing invasive squamous cell carcinoma in gradual transition with adjacent small cell carcinoma (H&E x 100).

Primary combined small cell carcinoma of larynx
114 Int J Clin Exp Pathol 2011;4(1):111-117
and van Nostrand in 1972 [3], and is a now a well recognized, uncommon entity. However, rarely small cell carcinomas have been reported as primary combined carcinomas of larynx with synchronous admixed squamous cell carcinoma [1,4]. Ferlito et al. [5] first used the term “Combined small cell carcinomas of larynx” to describe these morphologically distinct synchronous tu-mors showing divergent lineages of differentia-tion. Gnepp et al. [6] and Gianoli et al. [7] de-scribed the presence of mixed squamous cell and small cell anaplastic carcinoma in the lar-ynx as “Composite tumor of larynx”. Mills et al in 1981 [8] studied ultrastructural characteristics in 2 cases of small cell carcinoma of larynx which revealed the presence of both squamous features (intracytoplasmic tonofilaments and desmosomes) as well as dense core granules in the tumor cells. One of their cases also had a biphasic light microscopy consisting of both small cell and squamous cell components. Based on our review, a total of 16 cases of com-bined small cell carcinoma have been reported in the literature to date [1, 4-12]. Their main clinico-pathologic characteristics including the pattern of metastatic spread are summarized in Table 1. Majority of these patients were males, in sixth to seventh decade of life. Most common site of origin of the primary tumors appeared to be right hemilarynx involving suraglottic and glottic regions. Review of the metastatic pat-
terns of such combined tumors reveals that most reported cases have had mixed cellular patterns in varying proportions in metastases at different sites. To the best of our knowledge, the present case is the seventeenth reported case of a combined small cell carcinoma of larynx, second case in which individual tumor components were later-alized on either side of larynx [1,9], and the first case in which this side-specificity of tumor was reflected in its metastatic neck nodal spread (Table 1). Therefore, our case is unique in dem-onstrating a distinct pattern of metastatic in-volvement of regional lymph nodes that corre-sponded to the laterality of the histological com-ponents of primary tumor. Moreover, our case clearly showed that the tumor mass and extent of spread was recognized to be much greater on CT scan and on serial sectioning of laryngec-tomy specimen (transglottic, subglottic and crossing midline), than initially estimated on laryngoscopic examination or on external gross pathologic evaluation. This raises the point that pre-operative diagnostic yield of small cell carci-noma (pure or combined) can be enhanced by including deeper submucosal biopsies on laryn-goscopy in all those cases in which the extent of disease on imaging is disproportionately larger than the apparent mucosal involvement on laryngoscopy. The exact etio-pathogenesis of combined small cell carcinoma is uncertain. However, multiple
Figure 4. (A) Metastatic small cell carcinoma component involving lymph node (H&E x 200). (B) Metastatic squamous cell carcinoma component involving lymph node (H&E x 200).

Primary combined small cell carcinoma of larynx
115 Int J Clin Exp Pathol 2011;4(1):111-117
Table 1. Review of clinicopathologic features of the reported cases of combined carcinoma of the larynx Source Age/
sex Site Histologic pattern
of primary tumor Positive lymph nodes
Distant metastasis
Metastatic histologic phenotype
Therapy Follow-up
Eusebi et al, 1978
63/M
Rt.supraglottis and glottis
HL: SmCC and SCC
+ - SmCC (LN) HL +RND DOD at 24 mths. (reference: Ferlito et al;1985)
Mills et al, 1983
49/M
Rt. supraglottis and glottis
TLP: kSCC (60%) and
SmCC (40%)
+ - SmCC (1 LN, Rt. thy-roid)
SCC ( 2 LNs)
TLP+ RND+ Rt. thyroid lobectomy,
XRT
NED, at 6 mths.
Ferlito et al, 1985
50/M
Lt. hemilarynx TLP: SCC and SmCC
+
NA SmCC TLP+LRND, XRT
DOD at 14 mths.
Ferlito et al, 1985
54/M
Glottis and sub-glottis
TL: SCC and SmCC - - TL+RND, XRT NED at 42 mths.
Ferlito et al, 1985
47/M
Rt.supraglottis and glottis
TL: SCC and SmCC +
+ Lung, bone, and brain
Chemo, XRT DOD at 48 mths.
Ferlito et al, 1985
45/M
Rt.supraglottis and glottis
TL: SCC and SmCC + - Chemo , XRT DOD at 21 mths. (of SCC of oral
cavity)
Ferlito et al, 1985
56/M
Epiglottis TL: SCC and SmCC - - Chemo , XRT NED at 77 mths.
Gnepp et al, 1983
57/M
Rt. glottis TLP: SCC and SmCC
+ + Bone
SmCC (>1 LNs) Combined SmCC and
SCC (2 LN)
TLP+ RRND, XRT
DOD at 3.5 mths.
Chen et al, 1986
56/M
Rt. supraglottis Bx: WD SCC
SL: Mixed SCC and SmCC
- - SL+ RRND, Chemo
AWD at 13 mths.
Chen et al, 1986
55/M
Rt.hemilarynx, Lt. supraglottis
Bx: PDSCC TL: Mixed MD SCC
and SmCC
+ + Bone, lung
SmCC (LN) TL+ RRND, XRT, Chemo
DOD at 9 mths.
Cosby and Babin, 1988
56/M
Lt. supraglottis Bx: PD SCC TL: Mainly SMUC
and SCC
+ - SmCC (LN) TL+ LRND, Chemo
Lost to follow up during Chemo
Gianoli et al, 1992
83/M
Rt. supraglottis Bx: WD k SCC TL: WD k SCC and
SmCC
- - TL+ MND NED at 8 mths
Yucel et al, 2000
32/M
Supraglottis + - SL+ MND, XRT, Chemo
AWD at 12 mths.
Jaiswal and Hoang, 2004
41/M
Lt glottis, Rt hemi-larynx
Bx Lt. vocal cord: SCC in situ
Bx Rt. hemilarynx: SmCC with SCC
NA - Chemo, XRT NED at 8 mths.
Barbeaux et al, 2006
61/M
Rt. glottis
Bx: Mixed SCC and SmCC
NA NA NA -Chemo, XRT; -TL+ RND - Chemo
AWRR at 44 mths.
Barbeaux et al, 2006
54/F
Lt. subglottis
Bx: Mixed SCC and predominant SmCC
- + bone, lung, peritoneum,
LN
SmCC (distant) XRT, Chemo AWD at 36 mths.
Our case 59/M
Rt.supraglottis, epiglottis and
glottis, Lt..glottis
+ TL+ BMND + Rt. thyroid lobectomy
Lost to follow up During XRT.
: Abbreviations: Rt.: Right; Lt.: Left; LN: lymph node; SMUC: Small cell carcinoma; SCC: Squamous cell carcinoma; WD: Well differentiated; MD: Moder-ately differentiated; PD: Poorly differentiated; k: keratinizing; Bx: Biopsy; SL: Supralaryngectomy; TL: Total Laryngectomy; HL: Hemilaryngectomy;TLP: Total laryngopharyngectomy; RND: Radical neck dissection; RRND: Right radical neck dissection; LRND: Left radical neck dissection; MND: modified neck dis-section; BMND: Bilateral modified neck dissection; XRT: radiotherapy; Chemo: Chemotherapy; NED: No evidence of disease; AWD: Alive with disease; AWRR: Alive with recurrent relapses; DOD: Died of disease; mths.: months; NA: not available; M:Male; F: Female.

Primary combined small cell carcinoma of larynx
116 Int J Clin Exp Pathol 2011;4(1):111-117
hypotheses have been proposed to explain com-bined or mixed tumors. These include pluripo-tent precursor stem cell origin with subsequent divergent differentiation into Kulchitsky cells, squamous cells, and/or glandular cells [5]. Other theories include neoplastic stem cell dif-ferentiating into two or more morphologically and structurally different neoplastic cells. This concept has been proved experimentally [13]. Based on these theories, it appears that com-bined carcinomas likely arise from neoplastic transformation of a differentiated precursor or a neoplastic stem cell with divergent differentia-tion potential. Moreover, foci of transition be-tween the two morphotypes, and in-situ squamous component in this case suggest that combined tumors may represent examples of extreme tumor heterogeneity or dedifferentia-tion. In spite of the rarity of these tumors, the biologi-cal behavior of combined small cell carcinomas (neuroendocrine type) of the larynx appears to be comparable to that of the pure laryngeal small cell carcinoma, neuroendocrine type. The dominant prognostic impact of small cell carci-noma component in combined tumors is likely due to its rapid growth, increased bulk and ag-gressive metastatic potential. The apparent clinical course of all the 16 reported cases of laryngeal combined carcinomas was fatal with early lymph nodal and distant spread in 9 cases. Although occasional patients survived up to 3 years following pathologic diagnosis, major-ity of these patients died within 2 years [3,5,8]. The deeply invasive nature of small cell carci-noma in this case and in reported cases sug-gests that deep biopsies at the sites of domi-nant disease on imaging may be needed to es-tablish correct pre-operative diagnosis and al-low proper selection of neoadjuvant or palliative chemo-radiotherapy in large or unresectable tumors. Precise and detailed examination of laryngec-tomy specimens is very important for the appro-priate treatment as well as prognosis, and one of the most important component is reporting the pattern of metastatic spread. Squamous cell carcinomas of larynx may spread directly to con-tiguous structures, or via lymphatic and blood vessels to lymph nodes and more distant sites. On the other hand, small cell carcinoma is an aggressive tumor with early regional and distant metastases. Almost half of patients present with
positive cervical lymph nodes and about 60-90% develop distant metastases [2]. The tumor spread in vast majority of cases is by the direct extension, lymphatics and by blood stream in more advanced cases. Pressman et al. in 1981 [14] demonstrated that larynx must be considered a highly compart-mentalized organ in which right and the left halves except their mucosal surfaces, are physiologically and anatomically separated from each other. Lymphatic drainage from all levels, of larynx is mainly to ipsilateral cervical lymph nodes, except subglottic area which has a bilat-eral lymphatic distribution. Their basic study on anatomy of larynx concluded that direct, con-tiguous spread of laryngeal cancer from one side to the other is via interlacing superficial or mucosal lymphatics that spread over the entire mucosal surface without limitation. On the other hand, cancer spread to the ipsilateral lymph-nodes is limited by the fact that submucosal or deep lymphatics form an independent network on each side without any crossover beyond the midline. Based on this study, the side-specific pattern of metastatic neck nodal spread of the tumor in our case can be explained by the inde-pendent spread of deeply invasive tumor of both histologic types separately in either hemi-larynx along submucosal or deep lymphatics. This finding raises the consideration that pri-marily supraglottic or transglottic carcinomas such as our case should be substaged based on involvement of one or both sides similar to the current AJCC substaging of T1 glottic carcino-mas into T1a and T1b based on involvement of one or both vocal cords. Conclusion
Herein we report the seventeenth case of a combined small cell carcinoma of larynx, sec-ond case in which individual tumor components were lateralized on either side of larynx [1,9], and the first case in which this side-specificity of tumor was reflected in its metastatic neck nodal spread. The predominance of the biologically aggressive component in the combined tumor may impact overall survival. Pathologists need to examine adequate sections from either side of laryngectomy specimens. This is particularly relevant to establishing the correct diagnosis of the uncommon combined carcinomas of larynx. The gradual transition between the two morpho-types, and in-situ squamous component in this

Primary combined small cell carcinoma of larynx
117 Int J Clin Exp Pathol 2011;4(1):111-117
case suggest that combined tumors may repre-sent examples of extreme tumor heterogeneity or dedifferentiation. Consideration may be given to substage supraglottic or transglottic carcino-mas based on tumor laterality akin to T1 glottic carcinomas in AJCC system. Finally, the pre-operative diagnostic yield of small cell carci-noma (pure or combined) can be enhanced by including deeper submucosal biopsies on laryn-goscopy in all those cases in which the extent of disease on imaging is disproportionately larger than the apparent mucosal involvement on laryngoscopy. This approach can facilitate selec-tion of neoadjuvant or palliative chemo-radiotherapy in large or unresectable tumors. Please address correspondence to: Suash Sharma, MD, Department of Pathology (Anatomic Pathology), Medical College of Georgia, Augusta, GA 30912. Tel: 706-721-9362, E mail: [email protected] References [1] Jaiswal VR, Hoang MP. Primary combined
squamous and small cell carcinoma of the lar-ynx. A case report and review of the literature. Arch Pathol Lab Med 2004; 128:1279-1282
[2] Barnes L. Neuroendocrine tumors. In: WHO clas-sification of tumors, Pathology and Genetics, Head and Neck Tumors (eds: Barnes L, Eveson JW, Reichart P, Sidransky D), 2004, pp.135-139
[3] Olofsson J, van Nostrand AWP. Anaplatic small cell carcinoma of larynx: case report. Ann Otol Rhinol Laryngol 1972; 81: 284-287.
[4] Barbeaux A, Duck L, Weynand B, Desuter G, Hamoir M, Gregoire V, Baurain JF, Machiels JP. Primary combined squamous and small cell car-cinoma of the larynx: report of two cases and discussion of treatment modalities. Eur Arch Otorhinolaryngol 2006; 263: 786-790
[5] Ferlito A, Recher G, Caruso G. Primary combined small cell carcinoma of the Larynx. Am J Oto-laryngol 1985; 6(4): 302-308
[6] Gnepp DR, Ferlito A, Hyams V. Primary anaplas-tic small cell (oat cell) carcinoma of the larynx: Review of the literature and report of 18 cases. Cancer 1983; 51(9): 1731-1745
[7] Gianoli GJ, Butcher RB, Martin EJ. Composite tumor of the larynx. Ear Nose Throat J 1992; 71(2): 81-82, 85- 87
[8] Mills SE, Cooper PH, Garland TA, Johns ME. Small cell undifferentiated carcinoma of the larynx: Report of two patients and review of 13 additional cases.Cancer 1983; 51(1): 116-120
[9] Chen DA, Mandell-Brown M, Moore SF, Johnson JT. ‘‘Composite’ Tumor: Mixed squamous cell and small-cell anaplastic carcinoma of the lar-ynx. Otolaryngol Head Neck Surg 1986; 95(1): 99-103
[10] Eusebi V, Betts CM, Giangaspero F. Primary oat-cell carcinoma of the larynx. Virchows Arch A Pathol Anat Histol 1978; 380(4): 349-354
[11] Cosby WN, Babin RW. Simultaneous oat cell and squamous cell carcinoma of the larynx. Military Med 1988; 153(4): 196-198
[12] Yucel OT, Sokmensuer C, Gedikoglu G, Ayas K. Combined small cell and squamous cell carci-noma of the larynx: short communication. Tu-mori 2000; 86(5): 434-436
[13] Kobori O, Oota K. Neuroendocrine cells in seri-ally passaged rat stomach cancers induced by MNNG. Int J Cancer 1979; 23:536-541
[14] Pressman J, Simon M. Anatomic studies related to the dissemination of the cancer of larynx. Cancer 1961; 14(5): 1131-1138.