Case Report An Intradermal Nevus of the - · PDF fileWe are reporting a case of an intradermal...
3
Central Annals of Otolaryngology and Rhinology Cite this article: Bakshi J, Yadav S, Kumar A (2017) An Intradermal Nevus of the External Auditory Canal - A Rare Occurrence. Ann Otolaryngol Rhinol 4(5): 1181. *Corresponding author Sanjeev Yadav, L-178, Department of ENT and head neck surgery, Post Graduate Institute of Medical Education and Research, Chandigarh, India, 160012; Tel-+91-8284896932, E-mail: Submitted: 21 June 2017 Accepted: 26 July 2017 Published: 27 July 2017 ISSN: 2379-948X Copyright © 2017 Yadav et al. OPEN ACCESS Keywords • Intradermal nevus • External auditory canal Case Report An Intradermal Nevus of the External Auditory Canal - A Rare Occurrence Jaimanti Bakshi, Sanjeev Yadav*, and Amit Kumar Department of ENT and head neck surgery, Post Graduate Institute of Medical Education and Research, India Abstract We are reporting a case of an intradermal nevus of the external auditory meatus. A 25-year-old young man presented with complaints of progressive hearing loss in the left ear, and otoscopic findings showed the presence of a papillomatous lesion that is dome shaped arising from the posterior wall of external auditory canal with impacted cerumen. Patient underwent detailed clinical and audiometry examination and after work up patient was planned for excision of mass. The postoperative histopathological examination showed the findings consistent with the diagnosis of intradermal nevus. We are reporting this case as the intradermal nevi of EAC has not been reported much in literature and the diagnostic possibility of intradermal nevi can be considered in external auditory masses. ABBREVIATIONS EAC: External Auditory Canal INTRODUCTION Intradermal nevi are benign cutaneous tumors more common in skin, and are from the group of common acquired nevomelanocytic nevi [1]. There are only a fewer than 50 cases described in English literature regarding nevus of external auditory canal [2-4]. They may be asymptomatic or can present with aural obstruction, aural fullness, recurrent attacks of acute otitis externa and sometimes with hearing loss [2]. CASE PRESENTATION A 25-year-old young man presented to our outpatient department of otolaryngology, with complaints of decreased hearing in left ear since 2 years. The clinical examination showed the presence of hard impacted wax in the right ear. The patient was put on cerumenolytics and was followed up. After removing the cerumen, otoscopic examination showed the presence of a large papillomatous lesion, which was dome shaped arising from the posterior wall of lateral external auditory canal almost completely occluding the canal and was compressible on palpation. The tympanic membrane behind the lesion was intact. Tuning fork tests showed the presence of conductive hearing loss in the left ear that was confirmed with pure tone audiometry examination. After detailed clinical and audiological examination, an incisional biopsy was taken in minor operation room under local anesthesia to rule out the possibility of malignant melanoma or any other external auditory canal malignancy. Pathological examination suggested intradermal nevus. Subsequently patient was planned for excision of the lesion under local anesthesia by transmeatal approach. The lesion was excised in toto with adequate margins, leaving a small area of exposed bone and perichondrium that was allowed to granulate and heal spontaneously. Merocel packing with mupirocin ointment was placed in the ear canal for 10 days to prevent stenosis. In surgical specimen epidermis showed hyperkeratosis and irregular acanthosis. The dermis showed presence of tumor arranged in nests and group of cells with round to oval hyperchromatic nuclei and scant to moderate cytoplasm. Several cells in upper dermis showed melanin pigments. No junctional activity or atypia noted. Sections from margins were free of tumor. On 6-month follow-up patient showed no evidence of recurrence or canal stenosis. DISCUSSION One of subtypes of melanocytic nevus is intradermal nevus, which is more common in skin, and occurrence within external auditory canal is rare. Intradermal nevi can slowly progress in size and can present with gradually progressive hearing loss, which is conductive in nature. Large intradermal nevi can also cause trapping of water medial to the mass and can lead to recurrent episodes of otitis externa [2]. Intradermal nevi can be incidental finding on routine otoscopic examination and can remain asymptomatic until the period when they grow in enough size to produce mechanical obstruction effects. Nevi can present as junctional, compound and intradermal
Transcript of Case Report An Intradermal Nevus of the - · PDF fileWe are reporting a case of an intradermal...

Central Annals of Otolaryngology and Rhinology
Cite this article: Bakshi J, Yadav S, Kumar A (2017) An Intradermal Nevus of the External Auditory Canal - A Rare Occurrence. Ann Otolaryngol Rhinol 4(5): 1181.
*Corresponding author
Sanjeev Yadav, L-178, Department of ENT and head neck surgery, Post Graduate Institute of Medical Education and Research, Chandigarh, India, 160012; Tel-+91-8284896932, E-mail:
Submitted: 21 June 2017
Accepted: 26 July 2017
Published: 27 July 2017
ISSN: 2379-948X
Copyright© 2017 Yadav et al.
OPEN ACCESS
Keywords•Intradermal nevus•External auditory canal
Case Report
An Intradermal Nevus of the External Auditory Canal - A Rare OccurrenceJaimanti Bakshi, Sanjeev Yadav*, and Amit KumarDepartment of ENT and head neck surgery, Post Graduate Institute of Medical Education and Research, India
Abstract
We are reporting a case of an intradermal nevus of the external auditory meatus. A 25-year-old young man presented with complaints of progressive hearing loss in the left ear, and otoscopic findings showed the presence of a papillomatous lesion that is dome shaped arising from the posterior wall of external auditory canal with impacted cerumen. Patient underwent detailed clinical and audiometry examination and after work up patient was planned for excision of mass. The postoperative histopathological examination showed the findings consistent with the diagnosis of intradermal nevus. We are reporting this case as the intradermal nevi of EAC has not been reported much in literature and the diagnostic possibility of intradermal nevi can be considered in external auditory masses.
ABBREVIATIONSEAC: External Auditory Canal
INTRODUCTIONIntradermal nevi are benign cutaneous tumors more
common in skin, and are from the group of common acquired nevomelanocytic nevi [1]. There are only a fewer than 50 cases described in English literature regarding nevus of external auditory canal [2-4]. They may be asymptomatic or can present with aural obstruction, aural fullness, recurrent attacks of acute otitis externa and sometimes with hearing loss [2].
CASE PRESENTATIONA 25-year-old young man presented to our outpatient
department of otolaryngology, with complaints of decreased hearing in left ear since 2 years. The clinical examination showed the presence of hard impacted wax in the right ear. The patient was put on cerumenolytics and was followed up. After removing the cerumen, otoscopic examination showed the presence of a large papillomatous lesion, which was dome shaped arising from the posterior wall of lateral external auditory canal almost completely occluding the canal and was compressible on palpation. The tympanic membrane behind the lesion was intact. Tuning fork tests showed the presence of conductive hearing loss in the left ear that was confirmed with pure tone audiometry examination. After detailed clinical and audiological examination, an incisional biopsy was taken in minor operation room under local anesthesia to rule out the possibility of malignant melanoma or any other
external auditory canal malignancy. Pathological examination suggested intradermal nevus. Subsequently patient was planned for excision of the lesion under local anesthesia by transmeatal approach. The lesion was excised in toto with adequate margins, leaving a small area of exposed bone and perichondrium that was allowed to granulate and heal spontaneously. Merocel packing with mupirocin ointment was placed in the ear canal for 10 days to prevent stenosis. In surgical specimen epidermis showed hyperkeratosis and irregular acanthosis. The dermis showed presence of tumor arranged in nests and group of cells with round to oval hyperchromatic nuclei and scant to moderate cytoplasm. Several cells in upper dermis showed melanin pigments. No junctional activity or atypia noted. Sections from margins were free of tumor. On 6-month follow-up patient showed no evidence of recurrence or canal stenosis.
DISCUSSIONOne of subtypes of melanocytic nevus is intradermal nevus,
which is more common in skin, and occurrence within external auditory canal is rare. Intradermal nevi can slowly progress in size and can present with gradually progressive hearing loss, which is conductive in nature. Large intradermal nevi can also cause trapping of water medial to the mass and can lead to recurrent episodes of otitis externa [2]. Intradermal nevi can be incidental finding on routine otoscopic examination and can remain asymptomatic until the period when they grow in enough size to produce mechanical obstruction effects.
Nevi can present as junctional, compound and intradermal
Central
Yadav et al. (2017)Email:
Ann Otolaryngol Rhinol 4(5): 1181 (2017) 2/3
and this histological spectrum reflects the involution of nevi, with junctional type more common in the children [1,5].
Complete excision of the lesion is required because of possibility of melanoma and to rule out the possibility of seborrheic keratosis, benign pigmented keratosis, pigmented fibrous histiocytoma, squamous papilloma and malignancies such as squamous cell carcinoma [2,3]. Preoperatively biopsy is required to plan further management as treatment changes with the presence of melanoma or squamous cell carcinoma [6].
According to clinical manifestations, 5 types of melanocytic nevi can be flat, slightly elevated, papillomatous, dome-shaped and pedunculated lesion [7]. Literature shows that nearly all dome-shaped, pedunculated lesions and most of papillomatous lesions represent intradermal nevi [8].
The area of EAC after excision of nevi can be left bare or can be covered with skin graft. In our case, we had left the defect to be healed by secondary intention. But in cases of larger defects it is pragmatic to use skin graft because of possibility of granulation formation over the bare bone which can cause recurrent ear discharge. Complete excision is sometimes difficult as the medial margin is difficult to visualize and incomplete excision can lead to regrowth presenting as pseudomelanoma [1]. Angled endoscopes can be used sometime to delineate the full extent of lesion (Figures 1, 2).
Intradermal nevi seems to be more prevalent in Asian race and in middle age people, this may be attributed to the number of cases which are reported in the Asian race. Youngs et al. described the first case report of intradermal nevus of the EAC in the English literature in 1988 [2,3,9]. Review of literature showed a few case reports and only two larger case series in the English literature [3,4] (Figures3, 4).
In the two larger case series, Lee reported 10 of 11 patients with EAC nevi were intradermal and only one was compound nevus [3]. In another study, Lim et al. reported 18 of 23 patients with EAC nevi were intradermal and five were compound nevi [4]. Definitive treatment of intradermal nevi is surgical excision with or without skin canal reconstruction. In our case we have done primary closure and 6-month follow up show no
Figure 1 A nevus is identified in the dermis arranged in nests. No junctional activity is noted. (Haematoxylene and eosin, x 200)
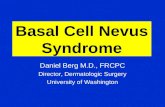
Figure 2 The nevus cells have uniform nucleus and many of them show cytoplasmic melanin pigment. (Haematoxylene and eosin, x 400).
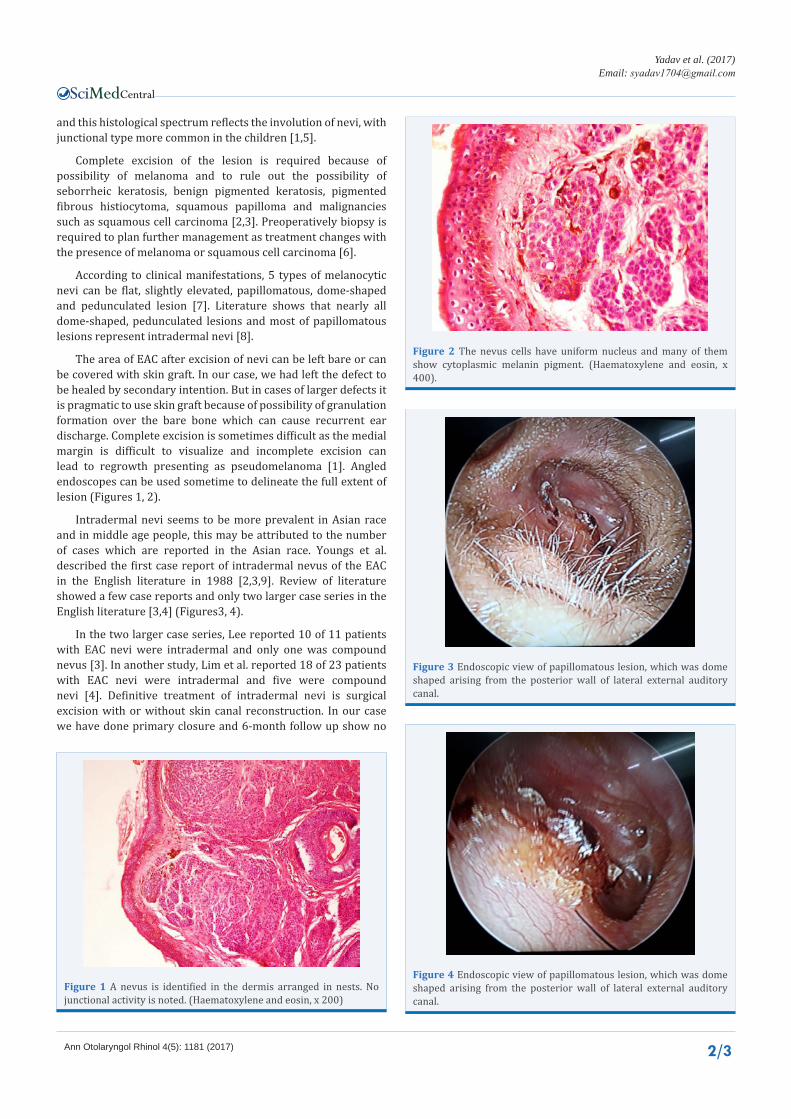
Figure 3 Endoscopic view of papillomatous lesion, which was dome shaped arising from the posterior wall of lateral external auditory canal.
Figure 4 Endoscopic view of papillomatous lesion, which was dome shaped arising from the posterior wall of lateral external auditory canal.

Central
Yadav et al. (2017)Email:
Ann Otolaryngol Rhinol 4(5): 1181 (2017) 3/3
Bakshi J, Yadav S, Kumar A (2017) An Intradermal Nevus of the External Auditory Canal - A Rare Occurrence. Ann Otolaryngol Rhinol 4(5): 1181.
Cite this article
recurrence or stenosis. However the use of skin graft is advisable for circumferential canal wall defects to reduce the possibility of granulation formation and stenosis.
REFERENCES1. Elder D, Elenitsas R, Jaworsky C, Johnson B. Levers histopathology of
the skin. 8th Ed. Lippincott- Raven, Philadelphia. 1997: 633-638.
2. Youngs R, Hawke M, Kwok P. Intradermal nevus of the ear canal. J Otolaryngol. 1988; 17: 241.
3. Fei-Peng L. Pigmented nevus of the external auditory canal. Otolaryngol Head Neck Surg2006; 135: 124-128.
4. Lim HJ, Kim YT, Choo OS, Park K, Park HY, Choung YH. Clinical and histological characteristics of melanocytic nevus in external auditory canals and auricles. Eur Arch Otorhinolaryngol. 2013; 270: 3035-3042.
5. Fitzpatrick TB. Wolf, Frredberg IN, Austen KF. Dermatology in general medicine. 4th. edition. New York: McGraw.
6. Cochran AJ, Bailly C, Paul E, Dolbeau D. Nevi, other than dysplastic and Spitz nevi. Semin Diagn Pathol. 1993; 10: 3-17.
7. Cağici CA, Yilmaz I, Ozlüoğlu L, Kayaselcuk F. Intradermal nevus of the external auditory canal: a case report. 2003; 12: 91-94.
8. Shaffer B. Pigmented nevi: a clinical appraisal in the light of present-day histopathologic concepts. AMA Arch Derm. 1955; 72: 120-132.
9. Fraser L, Smith WK. Excisional technique for intradermal nevi of the external auditory canal. J Otolaryngol Head Neck Surg. 2009; 38: 501-503.











![RESEARCH AND REVIEWS: JOURNAL OF MEDICAL AND … · Giant congenital nevus (Bathing trunk nevus / Garment nevus / Giant hairy nevus / Nevus pigmentosus et pilosus) – [6]have one](https://static.fdocuments.net/doc/165x107/5c8b90c109d3f21b168c6625/research-and-reviews-journal-of-medical-and-giant-congenital-nevus-bathing.jpg)