Case of Fatal Sickle Cell Intrahepatic Cholestasis Despite Use of ...
5
Case of Fatal Sickle Cell Intrahepatic Cholestasis Despite Use of Exchange Transfusion in an African-American Patient Daniel B. Costa, MD; Rebecca A. Miksad, MD; Michael S. Buff, MD; Yihong Wang, MD, PhD; and Bruce J. Dezube, MD Boston, Massachusetts Sickle cell intrahepatic cholestasis (SCIC) is a rare complica- tion of sickle cell anemia, characterized by marked hyper- bilirubinemia and acute hepatic failure with an often fatal course. However, the few reported adult cases that were treated with exchange transfusion had a favorable outcome. We herein descnbe a 48-year-old Afncan-Amencan man with hemoglobin S/13 thalassemia and previously treated hepatitis C with compensated cirrhosis, who presented with a total bilirubin of 59.7 mg/dL and direct bilirubin of 43.6 mg/dL in the absence of choledocholithiasis. Despite an exchange transfu- sion and aggressive packed red blood cell transfusions, which successfully decreased the hemoglobin S levels to <15%, he penshed from progressive hepatic and renal failure. Autopsy demonstrated extensive intrahepatocellular and intracanalic- ular cholestasis in a background of cirrhosis. Our case suggests that poor prognostic factors for adult SCIC patients treated with exchange transfusion may include older age and under- lying hepatic disease. Key words: sickle cell disease a sickle cell intrahepatic cholestasis a exchange transfusion a hepatitis C E cirrhosis © 2006. From the Departments of Medicine, Division of Hematology/Oncolo- gy (Costa, Miksad Buff, Dezube) and Pathology (Wang), Beth Israel Dea- coness Medical Center, Harvard Medical School, Boston, MA. Send corre- spondence and repnnt requests for J Natl Med Assoc. 2006;98:1183-1187 to: Dr. Bruce J. Dezube, Division of Hematology/Oncology, Beth Israel Deaconess Medical Center, 330 Brookline Ave., CC-913, Boston, MA 02215; phone: (617) 667-7082; fax: (617) 975-5665; e-mail: [email protected] INTRODUCTION H Tepatobiliary complications of sickle cell disease encompass many insults that range from benign liver function abnormalities to acute hepatic failure.' A rare entity named sickle cell intrahepatic cholestasis (SCIC) has been reported in <14 adults with sickle cell anemia.'-5 This clinical syndrome is charac- terized by marked hyperbilirubinemia with acute hepat- ic failure and is frequently accompanied by renal dys- function.`3,6 SCIC has been described in sickle cell patients who are homozygous for hemoglobin S (HbS), as well as in those who are heterozygous for HbS and B thalassemia. 1,3-6,10 Historically, SCIC proved fatal despite aggressive supportive care.2'7-9 However, since the advent of exchange transfusion, attempts have been made to lower the HbS fraction in patients with SCIC in order to mini- mize intrahepatic sickling. The four previously reported adults (ages 21-37) who had received exchange transfu- sions for SCIC survived.3-6 We present the case of a middle-aged man with HbS/B thalassemia and previously treated hepatitis C with compensated cirrhosis, who presented with SCIC. Despite an exchange transfusion and aggressive packed red blood cell (PRBC) transfusions, which decreased the HbS levels to <15%, he perished from progressive hepatic and renal failure. CASE REPORT The patient was a 48-year-old African-American man with HbS/B thalassemia. Hemoglobin elec- trophoresis at age 29 showed HbS 91.3%, HbF 2.6%, HbA2 6% and HbA 0%. The patient had a cholecystec- tomy at age 35 due to gallstone disease, and an abnor- mal liver was noted during the operation. Biopsy demonstrated cirrhosis, with mild chronic inflammation of fibrous septae and focal iron deposition within Kupf- fer cells and hepatocytes. Hepatitis C was diagnosed by serology; genotype and viral load assays were not com- mercially available. Apart from blood transfusions, he had no other kinown risk factor for hepatitis C. Interfer- on-a (3 million units three times a week) was started at age 36. After two years of therapy, hepatitis C viral load was undetectable. He had no evidence of portal hyper- tension or clinical manifestations of cirrhosis. Interfer- on was continued since the patient reported a decrease in the frequency of painful crises with this therapy. HIV antibody test was negative at age 44. His baseline total bilirubin was below 8 mg/dL for the previous 10 years. The patient presented to medical care with abdomi- nal discomfort, nausea, vomiting and jaundice for three JOURNAL OF THE NATIONAL MEDICAL ASSOCIATION VOL. 98, NO. 7, JULY 2006 1183
Transcript of Case of Fatal Sickle Cell Intrahepatic Cholestasis Despite Use of ...

Case of Fatal Sickle Cell IntrahepaticCholestasis Despite Use of ExchangeTransfusion in an African-American PatientDaniel B. Costa, MD; Rebecca A. Miksad, MD; Michael S. Buff, MD; Yihong Wang, MD, PhD; andBruce J. Dezube, MDBoston, Massachusetts
Sickle cell intrahepatic cholestasis (SCIC) is a rare complica-tion of sickle cell anemia, characterized by marked hyper-bilirubinemia and acute hepatic failure with an often fatalcourse. However, the few reported adult cases that weretreated with exchange transfusion had a favorable outcome.We herein descnbe a 48-year-old Afncan-Amencan man withhemoglobin S/13 thalassemia and previously treated hepatitisC with compensated cirrhosis, who presented with a totalbilirubin of 59.7 mg/dL and direct bilirubin of 43.6 mg/dL in theabsence of choledocholithiasis. Despite an exchange transfu-sion and aggressive packed red blood cell transfusions, whichsuccessfully decreased the hemoglobin S levels to <15%, hepenshed from progressive hepatic and renal failure. Autopsydemonstrated extensive intrahepatocellular and intracanalic-ular cholestasis in a background of cirrhosis. Our case suggeststhat poor prognostic factors for adult SCIC patients treatedwith exchange transfusion may include older age and under-lying hepatic disease.
Key words: sickle cell disease a sickle cell intrahepaticcholestasis a exchange transfusion a hepatitis CE cirrhosis
© 2006. From the Departments of Medicine, Division of Hematology/Oncolo-gy (Costa, Miksad Buff, Dezube) and Pathology (Wang), Beth Israel Dea-coness Medical Center, Harvard Medical School, Boston, MA. Send corre-spondence and repnnt requests for J Natl Med Assoc. 2006;98:1183-1187 to:Dr. Bruce J. Dezube, Division of Hematology/Oncology, Beth Israel DeaconessMedical Center, 330 Brookline Ave., CC-913, Boston, MA 02215; phone: (617)667-7082; fax: (617) 975-5665; e-mail: [email protected]
INTRODUCTIONHTepatobiliary complications of sickle cell disease
encompass many insults that range from benignliver function abnormalities to acute hepatic
failure.' A rare entity named sickle cell intrahepaticcholestasis (SCIC) has been reported in <14 adults withsickle cell anemia.'-5 This clinical syndrome is charac-terized by marked hyperbilirubinemia with acute hepat-ic failure and is frequently accompanied by renal dys-function.`3,6 SCIC has been described in sickle cellpatients who are homozygous for hemoglobin S (HbS),
as well as in those who are heterozygous for HbS and Bthalassemia. 1,3-6,10
Historically, SCIC proved fatal despite aggressivesupportive care.2'7-9 However, since the advent ofexchange transfusion, attempts have been made to lowerthe HbS fraction in patients with SCIC in order to mini-mize intrahepatic sickling. The four previously reportedadults (ages 21-37) who had received exchange transfu-sions for SCIC survived.3-6
We present the case of a middle-aged man withHbS/B thalassemia and previously treated hepatitis Cwith compensated cirrhosis, who presented with SCIC.Despite an exchange transfusion and aggressive packedred blood cell (PRBC) transfusions, which decreasedthe HbS levels to <15%, he perished from progressivehepatic and renal failure.
CASE REPORTThe patient was a 48-year-old African-American
man with HbS/B thalassemia. Hemoglobin elec-trophoresis at age 29 showed HbS 91.3%, HbF 2.6%,HbA2 6% and HbA 0%. The patient had a cholecystec-tomy at age 35 due to gallstone disease, and an abnor-mal liver was noted during the operation. Biopsydemonstrated cirrhosis, with mild chronic inflammationof fibrous septae and focal iron deposition within Kupf-fer cells and hepatocytes. Hepatitis C was diagnosed byserology; genotype and viral load assays were not com-mercially available. Apart from blood transfusions, hehad no other kinown risk factor for hepatitis C. Interfer-on-a (3 million units three times a week) was started atage 36. After two years of therapy, hepatitis C viral loadwas undetectable. He had no evidence of portal hyper-tension or clinical manifestations of cirrhosis. Interfer-on was continued since the patient reported a decreasein the frequency of painful crises with this therapy. HIVantibody test was negative at age 44. His baseline totalbilirubin was below 8 mg/dL for the previous 10 years.
The patient presented to medical care with abdomi-nal discomfort, nausea, vomiting and jaundice for three
JOURNAL OF THE NATIONAL MEDICAL ASSOCIATION VOL. 98, NO. 7, JULY 2006 1183

FATAL SICKLE CELL INTRAHEPATIC CHOLESTASIS
weeks. On review of systems, he denied fevers, chills,chest pain, diarrhea and melena. Physical exam demon-strated jaundice as well as a distended abdomen withhepatomegaly and ascites but no asterixis. Laboratoryevaluation was notable for a markedly elevated totalbilirubin of 59.7 mg/dL (normal 0-1.5 mg/dL) with adirect bilirubin of 43.6 mg/dL. In addition, white bloodcell count was 18,000/tL, Hb 6.7 g/dL, hematocrit (Hct)20.7%, platelet count 225,000/L, mean corpuscularvolume 78 fL, alanine aminotransferase (ALT) 85 U/L,aspartate aminotransferase (AST) 190 U/L, alkalinephosphatase 513 U/L, prothrombin time (PT) 20.1 sec-onds (normal 11.6-13.6 seconds), INR 2.6, partialthromboplastin time (PTT) 100.2 seconds (normal22.0-35.0 seconds), and creatinine 3.3 mg/dL (normal0.5-1.2 mg/dL). Hepatitis A and B serologies were neg-ative. Hepatitis C viral load showed no detectable virus(<600 IU/ml ofHCV-RNA by RT-PCR).
Ultrasound demonstrated patent hepatic vessels andno evidence of choledocholithiasis. Abdominal comput-ed tomography confirmed hepatomegaly and ascites aswell as hepatic nodularity. Peripheral blood smear wasnotable for sickle cells, target cells, many nucleated redblood cells and Howell-Jolly bodies. Cultures fromblood, urine and peritoneal fluid were negative.
Initial management consisted of intravenous saline,vitamin K, PRBCs and fresh frozen plasma. He wastreated empirically with broad-spectrum antibiotics.Exchange transfusion was initiated within 12 hours of
admission due to his multiorgan failure, particularlyhepatic dysfunction. Five units of PRBCs wereexchanged in one session. Pre- and postexchange trans-fusion hemoglobin electrophoresis demonstrated adecline in hemoglobin S from 58% to <15% (Figure 1).Despite continued support with fresh frozen plasma andPRBCs, his total bilirubin remained constant around 50mg/dL. The presumptive clinical diagnosis of SCIC wasmade, and after initial exchange transfusion therapy, hisHbS level was maintained at <25%, and Hct was main-tained around 22% with subsequent PRBCs.
Despite an initial clinical improvement with the low-ered HbS level, his condition continued to deteriorate.He received aggressive supportive care in the intensivecare unit with mechanical ventilation. Both coagulopa-thy and renal dysfunction persisted, and 20 days afteradmission his PT was 18.5 seconds, PTT 150 secondsand creatinine 2.5 mg/dL. Due to unresponsivecholestasis, a trial of ursodeoxycholic acid was attempt-ed without benefit to the bilirubin levels. Twenty-sixdays after his initial admission, the patient succumbedto multiorgan failure. The day prior to his death, theHbS level was 12%.
Autopsy was notable for extensive intrahepatocellu-lar and intracanalicular cholestasis in a background ofcirrhosis, and also peripheral hemosiderin depositionconsistent with secondary hemochromatosis (Figure 2).There were no thrombi or prominent ischemic changeswithin the liver parenchyma. Brain dissection showed
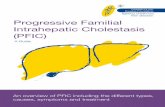
Figure 1. Graphic description of hemoglobin S (HbS) levels, total billrubin and hematocrit (Hct) duringinpatient course. Exchange transfusion (arrow corresponds to 5 units of PRBCs that were exchanged inone session), and PRBC transfusions are indicated.
'.:...-.:"".i "-... '' '.'4' ". 1-..--t.'' '' ",V...,.-'-..', ". "",,-..,.. '... .7-... ..-, ..--i---.'. Y'-. .;'if';- -.....---.',," ,,- -"';"-""-.;r-.. .4 ,- --,
....,i" '"' "'I.'q;.-,.-',, ,;----'. "-'"'.....i.1 -Ii':.-I--I--I':I-".:j-. -:!'.h'.'--..---.- --, "' "",.. -..-'. ,J. .'
""''; ". '- "' ,,, ." ';; ,," ,", ..."'!r, -.' ---"...'.-.-'-'"I "'.."7."', -, -'.-"--'-'..-.".-!---.-.. ---. :,,":.".,:-.'.'-.':-.;." " .", "-..--. i'.........' 'i "': .. :..' .',"'""" "-';".. .- ..- i. .--..--"-.'-.1'."'.-"-'..""'k...,... .,;-,.,.,.. .'.'S'1111..4,-'.j' .'.!"'.').,","" -." ?.-'-"-' "-.7 .", -'.'.,-- -"-'-:.'--.!"-.'.":--"i;-'-". "-.:' ...'.'.... -, "". ..... "' ."---." ...", "' -,,,,I-', ,-'?,', -,..'--.- .'--- .---,--.--- -.I- ..----.--"-'. ..-";..-' -'--'--"-' ..."_,.m..... -'..:' -.-'--..--'.'.-"'.-'-.. ..'....":..".-..".,....,.!...,...,.,.,.'.':'.',';,...,..,, -'.-.(-.i"--".---'.'.' "".,z",i.,."t,,...,,,..".,.,.....,,.-,.,.r'-..-.",.,., ."i"'.' ..'.; ...,i,...,.......-.,,....,.'..-.!..-','.-., '-'....i --'.-'.--".'-";'--'"...',...'.'.,.
I.- .i);..'.-511-, -4, I... 0.-.g.,,, ...'i"--' -.--',.;-.t'. -'.-
-"''7,,m., ....-", "'" "'I"" -,I11 ",.....1.1, I.".I'l -1 :.-i.--'--''" '.". ,,, ",..,,- -... I. .--- ..-.'-.!-.".,."..-".,..,...;.-...,..;..,-----'.'--'-:..-.-"---r.,-'.'t.--"'..."-';-',4..-'.....,-.'-%--.--'",` '.. i. ."i,,. .. .: --. .'.. .'.. -....',....'........-',-,..'.'....";.......',- ". .."..."...........-..,.....:.,r,.....",....' .'.'...","'.......,....'."'....-..,.- -'.";.-'-.-.'-.'-;".'.:."7....,...,.'...-".,-,.-.,- .-i..'...-".'.'-;.-'-"'-- I'''1'..."...."-.'.."- . -.........-...,.-..,-,.-'---'-.'-.--"6-";'-.'----.t..' 1.'-'- .-".,.4-i-,...,.--.,..-,'...,.-..',.,;....,..-,,..,..r...i...,..:,.,.-..' .....'.'-.'j .'. ------..-'--.' -4 --. -, '.....'. -.-- ...... ".. --'.L;I- ...'- .1. -.1 -;--'.. 1...-'..---.' -.--- ..'.Ii-'-- .?"---- '.'-t "-`.. ,"...'..'"''.....
..:i'Y:--.- .---`. "i" ;'. ."', -'-'.-'..".'-, ,,r..-'-.,.".- ].-' -Zr_" "' --. '!"':--'......".',i.!. ..,.,,,'.
': -i.."" Y.-' ..- -,-. "'.".. .":, -'.1j!",!. ..' ':....i,..T":'--"%-I-';"- -.. ,.."f'I"'-I---."--"".II.'y'.---,I-'- ..'..", li.,.'.",...,..-I..,,.,.....-.- '-'.-':.. .-- .., .,..,: -.'.-... -.,-, ,'.I .-1..,..:,-'..-' -"'' ;. 'L''i,,"'. ", ." ".. ........' '----- . ...j. ---.---'---0'', --.--'"..'..'i .."..! f-'.'-- -'-'. --..' -;-'A ..---H--"---'-.'-F-,".. !--'.'z--'-f-1--'! ';.-'.-; .., -.,-t .s' ..1 .. -t.'v.....',, ...", 'i .'.N '.. .- .' -"".. ..' --'.'."'..7!7-.,-'- -,' ''. "'-
'.. .rw ----I I-:,-.". ,,i.:..'
.... .,.-. ;".'...... .'I,.t.-'-'-..,"'.. !..,.,.,...,.,*,.,...!.!....-.-...,..,,..,,....,!......."-,,,.'.--!... --"!--:-;I-----"-I.M.I.--". ,...,,.,.,, "'..'.`",.' ',,..I-, -'-.-- -.4"... .- --".'.--:,'-.-J.-.-"-..... ';-'.-'--.t -,. .".--.-- :-, - -.z . .-....--.' -'.'-'-'!..-.',t----' --.,---------'-- "'it' 7....,-- .-.,
..'"',.-.Z". .' --- ,,''-,;,...",`--'.--..!I; '---.----'.'. .." --!....4!'t .'!;;', .' ."'..' ,-,,,, 10t. 4-. .i... ;"... ---."-,- .',,....... -,?! e.'ti-; ,""-'..: ,-, ..----.--".:.-":111:..",...' ------. '.!.....--.'-. ... -!7" ""''-..-.?-,-*:'-;V-.7'7! '.?o..".'.-...--..-,; --..-. .'. ..' -'..'.....".:'.....;' .",.....-..."-,i.,...-".".,...,.,.,...,...."...'-.-.,.,...'.-I-", --1-. .,...,:".'.'i.'.'..-' .. ...".-r.. r. ..,,,'.",.. ... .' .'-..7-'.f.I...'.' "..". i.'-----j"-.' ". 1 4" -,.i...'.-''"...'..'. ...:.-------'Z.-"'-'---'.;.-. i.'.. .,-.-,,.. ..'. ..:."-,-,.."'
",
"' ... .'.--,-, - "r":,- --t' ""'....."',-'..."..'..:-,,..........' ...;----- -'--- wi-Y----'-"---'-!--','-'-----'-'7 --'-'.'ii',,....,.,,.;..-.i.;,;,,.i,7,...,...-.;....,!.,...!r.-,'.'..-.,
,'"-'. `7 bKft.-,-,--.. .".:..'' I-' .-" "--6-`-K'--.'--.. '-%-!.-,'
... ......';.z4fi.'--'r-i' -'P." ".'4i- .r"'. .." .'. .!. ..I" ..'?'.'-.'L--- .."...'-'.-!--'--' -i----P"V.4.-..-'r-I I-, .--"' ICI.-' .'-- ,..-., .'; -'.., ---'--;.I'---...'' '--f'-"'..--' "-.--- .-....,....-..-. .-..,--.--- .. .._, -,;. -...
-..'- -.vi': --"'...
.""'-'"..'."' '-"'.' ".::-".--' 2'-"..'-,,.':.'.1". -')';:..- .-- .'.-!',.-.-`.'-.4 .::.,'.-"'"--- .. ..-''!, -i. .,."',--..'--':' ..,._;'.4.
.....11'..'.....,.'.,..;.,.'..'.", .. M. 1, .-I.'; .- "'. -, , -'.. .. -...'.'.. -.. "';', .. --;-'-.'2 --;--3----; .'.----...'.. .... ,-"".,,'.t---- --.? ..'....'.'.-...:..,.,..I -"-. ---'--'- M."., ... ...;.`.."."".-....., .. -, .-.. -----.---------- ..... .' .....4-'... ...-'-..'.---i. .-' ..!'.,-" .!.;----'-',.---- -.:...'.-,---,.. -'. -_. j4Ij..' ", -'.;.--- .";' -,..',.;...---`----'--`:. -.'-.--'--.'--.i'.....2) tii.......- .i!.. -,f'-'.-'.'-; --:--".-.".'-.; .-..-.-..-:.' -'. '. ..I*.4.0-
...,.-.T7./.,..,,. .,p-.---;: --'---!---'..-,-;:--:i,.' '. ." .'-.,--q
....-0-...-... ..,-7....'....''..,.-i... ., ,..' .-."'..";.'t.-- ---;-.-,-,-...,"-.......'.."..".."..-...:-.:."....- ...w-.--.'-';--..'--".-:;..--,.. .ir....",...,.,'..".,t.i,."..,.'-'-------7-----':---...-."..'....,.,.,.,..!,'..f,;,;.,.i......"...;,-.,...-...,.....",..,;'.: -.' -"!"'.!----. ,,...,Z -. .' ;,-....-,;,.. --'-----..i.r ,,, --n.. .....,.,.I` .. ..- ... -. I.. -...,.,., 1.1-..
... ...;. ..... T.-- i--"..:,,-.'--'-'.',;--.-I-,..-7 C.'r. .- "..i '' "..' -.. .'. .;
'.""' .. "'I .1.,.--.'-.-.;--.--. !..'. -:;---.-. --".-'-.. -, ..-- -,-.-.e;.!.-.......,..7.,...*-'.,',.i.'-....'.".".-,!.;,-"".,", ". ...!' -?.".-'. ..:.;" ---.` .'-Ii ..".-'
1.,, -,...,; ,.. ....' .f...- ..,i,-;i-'-'.'...,.,, ..:?,.".....'..'..--'-.-.!,, ".-, .; .-IN..'e ...".""..'.!:.,.";..-".6..,.,.,'.'......' .'............-;-,
""' --'.--.. '.-.".;'--.---. .. '. '-.,.".-''.".".,.,...."".'.'-.'-'.,.....--.,.,.'..1..f.,i.j'..4.' i.' "I .- -.--.'.14.--.i..1"- ,,,, -.;' "n ---.." -1, .. -'f.-'P-.-',,.-..-",...-.-...,..........;..-..?,.,....,...;".-,..." "..:;-'.,,f, ----i..:i' .' ";."' -'j.... .. ,' -, 't ,"..' ." .,.! -,-I.,.. ,.,,",I"...... -!, ..i,'...--.'-,')-'-----'.- ,.i'.::.... ....... -.' ."..-...''" '.':.' -0--"".',.!--'-.'-.! ".'' .I.. '.--'-'..IV:.....i.; ,,, ",t.,'...,...'. ...'-'...- .: -1-3--'.."'... I...". "..".,.1'-'.-J......."',V''''I.,... ......i,
-.. --;- `--.". '..?..-.,;,...".,...,..:,-.-.......,".-".'.'..I-..'.,.;.%".,...::-;i,.,..'.".,';,40....,:;"........'...-...-..7.; .';,;. .! ."'i....-..."......!,...'..,.-.....!...'.....l.'."-'.".,.ll.:;,,..,-.....'-.1.----t -,-- i,... .."' '' .. ... ." ..'-'......... ;.,... .....
.,:; I.-:..-.- .... -;',' ..'......'.""I", "..", ...-i,.'-..-.;. .,----k' -!.....I.,''-,;-'f-'.Vi. -'- ,,,..,,-,,..-
... --.-i'..!-'---,.;'.--" --.':'-..'-"':-'-i!. .: "-... ..'... ". :' ...'...`-.7;.-';'...'.- ..,-,. -"-"----- '-:"""',- ,,,--.7,.'..
--.:::,-I..-%:. .1,
:-I-.....'...... --- ,'-i ii..--.:.:"-, ....",----------.-:'-:' ,...-.-..--..-.-...;..,.,......,i':.'.-..,.',,.,.-,...:....,.-----:.,.'.'.,'t'.'-.-."-!.--- ---'--,;-" ."-'- -'.-.'.
-.4 -..""' -,,-... --'-- ------ ". '-..... ..",.t....'.- i.- --.'...- ----i .-?.-'- ..' ------------ T.-'------------."n,-.--I..;.. .". L-, -'-.'-..":..f-.----.-';':-- ..,.............-.-.......,.....-,..,,,....i. '." ..... .'.:..."' i..i-': ,- -.'........- '-... -::.i,..,. .-.:"'"..,..."...,.".,:,"...'."."..:....,.,,--.'-'--' .----7---. --..--.-'..--'-''.';', .-- ;...;, -..;..",,:.',. .. ""';'.-'V',:-.I,.q.." .- :.,.f"., ,,, "', .:' ..I,. %.. -::..,..;'.-- ol.- ...:..'. "-i....':. .1 .....z-,-- .-'-' ." .... :,'"..-;.:----',""--............. ...... .......'. -.--- -... -..--... .. .. - ,-'. .....
.-' ""':,.....,...:.?.",...i---:.'..-......:..;::.,.,......-.,.k.:.---;.''-I-';'I..--'... :1.11, ''`--. -' '11-.''''..- -.41I ,------ii.---.---, -;." ", ....:-...---.;;-'-"- "...I.---,.,.-.'I-,I.:.-
._'..',....---,.5';"'. -.'.".".'.' --.- "',-...'.:' '..,-.- .-'-..-:---"--.'.I.-i--'-;-'-'.-'---"',."'.....--:,-t.f;F-.'.-.- "I'.....--;':.'-.'Z.'-'!'-)-.::i, ,..'-...., I- -'-'.--'..' -...;
--,'' -, -!:..-A-.::I':.:::r --. --. i, .... ")': ,.-.,-.-$;." .-" .'.-.'.'--' ."-"-'',",:. >4 .'.....,..:..'.'. -.
-i.'!-.",-".---! --ff ...... '.. -',-.
.'.- ."". ,.,-,-..fs:...-I ----'---i--..'--1,..'- i, .;'.--' --:;.;. --?.-'--..i.-.---.-........., 7.. J..'...'...'.. -iv. 1. ;1% ,.Zr''.'- " ". If,.. '.' 40,.. ........;..'.. .;'--.- -:.' ... .."..."...I.i.-71-l'-.1--'. .' -.;.'-.-- .I.i- ... ,'.-.'.,' -'.' ..',-.. S-..-17., -7- ...."..!-'.'...-...f'""..''..'-'-- .- I---.' P.Lt."'.A-i. '-I -, .1 1. ..... .,t, ';...'-.:.'--; .k;
'f'-.:.'.';":-.",",?..---.-""'..v."'.' ,.' . I;P..
..? k..-10'!--.----'-"' i.1-1----.--"--I- -';...' ... ."';'. ..' ,.,f.., ... ..:'---'-,--I'.',--'.'..'.::'.'.:.,.: -'?. ------'-..'-.....,-4.1..,-"'.."..'...".'.."'..." .."',. ..'.." 4, .-I'XI'-I---'--`.-'- ..'.",. -, '....'-Z'-. .-..... ...-.,.-....":."l".,.,...",.,:,.-.-",...,: ".:' '...----'.';-'f- -"". --..-'. -'.."?" .--'.' .".--'--'-.1.',..'r..;. ... -11 -.',, ,- ,-,r". ,"' --i"', --.' '.,.':1'. .1.I.............i..-.-...".:4...,.-1....'.......,-,...,..,."...-'.:i.,.,.......,..,.,,....'...;V.
-"""- ---'T-I"..'.-T.;'IWZ.- .."; -;:.-.': ..'.....t7.
'.1, --.'---'r .,.;" .".. ,.I.' ..'.:.'.-'7"' -, -'-r- '-,"O"..." :....' ".111 -f ...". I . .... ... .11 .." ".1-1' ...... .i--'.,.. .! 4.- ...". ". .... ..... .'..'.:.% .. j*....... -,-".: .-, .. .. .. ,'...",... ";--k- ....-f.."..-11 ,;_.. --';'' '-..:.. ..- i..--. --.';" '....'., .(....:...-, 3. ----;"-,.Ir -'--`.'--"IIII"------'-- :-"--- -,--i.-.,I F... .i. ... .,.. .,"---,--... '. -..''.. 1,.: I.- ..,-

FATAL SICKLE CELL INTRAHEPATIC CHOLESTASIS
type-2 astrocytes of Alzheimer's, consistent with hepat-ic encephalopathy.
DISCUSSIONThe first comprehensive review of abnormalities
within the hepatobiliary tract in patients with sickle celldisease was published in 1977. Eighty-eight cases werereviewed, and five specific syndromes identified.2These included viral hepatitis, hepatic crisis, cirrhosis,cholelithiasis with cholecystitis and intrahepaticcholestasis or SCIC.2 A more contemporary review ofsickle cell hepatopathy added new entities such as mul-titransfusion liver disease and chronic hepatitis B and Cinfections. I
SCIC is a rare but feared morbid complication ofsickle cell disease.",2'6 The etiology remains unknown,but widespread sickling within liver sinusoids has beenpostulated."2 The pathophysiology of SCIC is poorlyunderstood, but hepatic sinusoid sickling is thought to
cause vascular stasis with subsequent ballooning ofhepatocytes, which leads to intracanalicular cholesta-sis.'-3'6 Patients with SCIC experience right upper quad-rant pain, progressive hepatomegaly, coagulopathy withhemorrhage, and extreme hyperbilirubinemia with totalbilirubin levels that reach up to 200 mg/dL.1 2'4 In mostreported cases, the degree of transaminitis is modest(ALT and AST <3 times normal levels) in contrast to themarkedly elevated total and conjugated bilirubin.1 Renalimpairment commonly follows liver dysfunction.1'2
Liver biopsy and autopsy specimens from afflictedpatients generally show dilated intrahepatic canali-culus.2 Sickle cell thrombi, sinusoidal engorgement,scattered bile stained microinfarcts and Kupffer cellhypertrophy have also been reported.24'8 However, a liv-er biopsy is not without risks in the diagnostic work-upof acute sickle cell hepatopathy. A report from Englandshowed a 28% incidence of death complicating liverbiopsies in 14 patients with sickle cell disease and acute
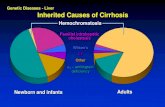
Figure 2. Autopsy and liver pathology. A: Hepatomegaly (liver weight: 2,200 g) with diffuse micronodularpaffern. B: Trichome stain (20x) showed bridging fibrosis (stage 4) and disruption of liver architectureconsistent with cirrhosis. C: Picture taken at the center of the nodules showing extensive intrahepatocellularand intracanalicular cholestasis (hematoxylin and eosin 40x). D: Iron stain (20x) showed intense peripheraland scaffered intrahepafic hemosiderin deposition, consistent with secondary hemochromatosis.
V~~~~~~~~~ ~~~~~~7"~~~...
N4~~~~~~~~~~~~~~~~i
V~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~........
dv,~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~'~~~~~~~~~~~~~...4'...........A.........~l....
AB~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~....
4 *,~~~~~~~~~~~~~~~~~~~~~~~0~~~~~~~~ ~~ ~ ~ ~ ~ ~~~ ~ ~ ~ ~ ~ ~ ' 4 .~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.....
B~~~~~~~~~~~~(
Mlh. YV41'91*~~~~~~~~~~~~~~~~~~
JOURNALOFTHENATIONALMEDICALASSOCIATIONVOL98NO7JULY20061185~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.

FATAL SICKLE CELL INTRAHEPATIC CHOLESTASIS
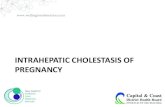
Table 1. Clinical-laboratorial characteristics and outcome of patients over 18 years of age with SCIC
Age (Years)/Type of Total Prothrombin Exchangeof Sickle Cell Bilirubin Time Transfusion
Year of Publication Syndrome (mg/dL) (Seconds) ofPRBCs Outcome19647 24/HbSS 100 - no died19658 23/HbSS 81 - no died19658 22/HbSS 89 - no died19658 20/HbSS 6 1 - no died19772 33/HbSS 112 53 no died19772 35/HbSS 64 - no died19772 23/HbSS 45 - no died19772 44/HbSS 98 47 no died19803 21 /HbSS 146 29 yes survived198613 35/HbSS 75 23 no survived19954 29/HbSS 106 35 yes survived199610 36/HbS-B thalassemia 47 32 no survived20026 37/HbSS 61 17 yes survived20025 22/HbS-B thalassemia 55 - yes survived2006 (current case) 48/HbS-B thalassemia 60 20 yes diedSCIC: sickle cell intrahepatic cholestasis; HbSS: homogyzous for hemoglobin S; HbS: B thalassemia: compound heterozygous forhemoglobin S and B thalassemia; PRBCs: packed red blood cells
hepatic disease. The authors concluded that within thatclinical setting percutaneous liver biopsy is contraindi-cated.'6 The diagnosis of SCIC is usually established bythe characteristic clinical and laboratory findings in theabsence of choledocholithiasis impacting within the bil-iary tract." 6
Fewer than 32 cases of SCIC have been reported."'The incidence seems to be greater in the pediatric thanadult population. Although the mortality in children canbe as much as 30%, their clinical course can also be mildand sometimes self-limiting." ''" The management andoutcomes of children have been reviewed elsewhere."16"14
We will focus our discussion on the adult population.Only 14 patients (Table 1) >18 years of age have beenreported with SCIC."-10",3 The first cases identified in the1960s and '70s proved to be almost invariably fatal,despite use of PRBCs and supportive measures.2,7-9 Ofthe four cases reported after 1980 of adult SCIC treatedwith exchange transfusion, all were successful.36 Thefirst successful use of exchange transfusion led to adecrease in the HbS level to 30% associated with adecrease in bilirubin from 146- to 16 mg/dL and withsurvival.3 Similar dramatic improvements have beendescribed in three additional adults treated withexchange transfusion, though in some the clinicalcourse was more protracted.46 Two other reported adultcases of SCIC were successfully treated with onlyPRBCs and fresh frozen plasma. 0,13
We were unable to find a report in an adult patientwhere exchange transfusion did not result in resolutionof the hyperbilirubinemia, hepatic dysfunction and mul-tiorgan failure. While reporting bias may limit the publi-cation of unsuccessful cases, our patient highlights thefact that SCIC continues to be a severe and potentially
fatal complication for adults with sickle cell disease.Two characteristics of our patient prior hepatic
injury from hepatitis C/cirrhosis and older age mayhave contributed to the observed poorer outcome whencompared to that expected from the SCIC literature.However, his undetectable hepatitis-C viral load, modesthyperbilirubinemia, and complete absence of signs andsymptoms of liver disease prior to his acute presentationgo against hepatitis-C-induced hepatic failure as thesole cause of his refractoriness. Another consideration isthat at age 48, our case is the oldest reported in the liter-ature. In the only other SCIC patient >30 years old treat-ed with exchange transfusion, it took almost a month tosee clinical improvement.6
In conclusion, SCIC is a rare hepatobiliary compli-cation of sickle cell disease that can be highly lethal.Despite the favorable outcomes of the adult cases inwhich prompt clinical diagnosis was made andexchange transfusions with a target HbS <20-30% wereperformed, our case illustrates that such positive resultsmay not always be achievable. Based on our case report,a worse response to exchange transfusion in SCIC maybe expected in older patients and in those with priorhepatic disease, such as hepatitis C and cirrhosis.
REFERENCES1. Banerjee S, Owen C, Chopra S. Sickle cell hepatopathy. Hepatology.2001;33:1022-1028.2. Sheehy TW. Sickle cell hepatopathy. South Med J. 1977;70:533-538.3. Sheehy TW, Law DE, Wade BH. Exchange transfusion for sickle cell intra-hepatic cholestasis. Arch Intern Med. 1980;140:1364-1366.4. Shao SH, Orringer EP. Sickle cell intrahepatic cholestasis: approach to adifficult problem. Am J Gastroenterol. 1995;90:2048-2050.5. Gilli SC, Boin IF, Sergio Leonardi L, et al. Liver transplantation in a patientwith S(beta)0-thalassemia. Transplantation. 2002;74:896-898.
1186 JOURNAL OF THE NATIONAL MEDICAL ASSOCIATION VOL. 98, NO. 7, JULY 2006

FATAL SICKLE CELL INTRAHEPATIC CHOLESTASIS
6. Khurshid 1, Anderson L, Downie GH, et al. Sickle cell disease, extremehyperbilirubinemia, and pericardial tamponade: case report and reviewof literature. Crit Care Med. 2002;30:2363-2367.7. Klion FM, Weigner MJ, Schaffner F. Cholestasis in sickle cell anemia. Am JMed. 1964;37:829-832.8. Owen DM, Aldridge JE, Thompson RB. An unusual hepatic sequela ofsickle cell anemia: a report of five cases. Am J Med Sci. 1965;249:175-185.9. Bauer TW, Moore GW, Hutchins GM. The liver in sickle cell disease: a clini-copathologic study of 70 patients. Am J Med. 1980;69:833-837.10. Betrosian A, Balla M, Kafiri G, et al. Reversal of liver failure in sickle cellvaso-occlusive crisis. Am J Med Sci. 1996;311:292-295.1 1. Stephan JL, Merpit-Gonon E, Richard 0, et al. Fulminant liver failure in a12-year-old girl with sickle cell anemia: favorable outcome after exchangetransfusion. EurJ Pediatr. 1995;154:469-471.12. Svarch E, Gonzalez A, Villaescusa R, et al. Plasma exchange for acutecholestasis in homozygous sickle cell disease. Hoematologia. 1986;19:49-5 1.13. Morrow JD, McKenzie SW. Survival after intrahepatic cholestasis associ-ated with sickle cell disease. J Tenn Med Assoc. 1986:79:199-200.14. O'Callaghan A, O'Brien SG, Nikovic M, et al. Chronic intrahepaticcholestasis in sickle cell disease requiring exchange transfusion. Gut. 1995;37:144-147.15. Emre S, Schwartz ME, Schneider B, et al. Living related transplantationfor acute liver failure in children. Liver Transpl Surg. 1999;5:161-165.
16. Zakaria N, Knisely A, Portmann B, et al. Acute sickle cell hepatopathyrepresents a potential contraindication for percutaneous liver biopsy.Blood. 2003;10 :101-103. C
.0 REUSE THISCONTENT
To photocopy, e-mail, post on Internet ordistribute this or any part of JNMA, please
visit www.copyright.com.
We Welcome Your CommentsThe Journal of the National Medical Association
welcomes your Letters to the Editor aboutarticles that appear in the JNMA or issuesrelevant to minority healthcare. Addresscorrespondence to [email protected].
Journal of the Natinal Medical Association
. -7 Call for
.:..~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~. .. ..
Ixi_t;Papers
T I O N~DUATO OF;;-S IPHYSICINS
iS, ber2006*MJNMA will be publishira theme issue4 covering educatioarof physicians.{This is a "call for manuscripts."
Please refer to the education theme issue in yourcover letter. Submission guidelines are located onNMA's website at www.nmanet.org underpublications, JNMA. Please e-mail yoursubmissions to [email protected] Hoover, MD E JNMA Editor-in-Chief* Publication, not manuscript submission, dates. Mostsubmissions needed four months or more ahead ofpublication date.
NationalMedical .......|
~~jAssociatilone Association ................... ... ;Xks.^.>->-~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ ~ ~ .. . .... . ....Annual ConventionA
Scientific As;semblyaLU
AUGST 5-10, 200-4
m m~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Fo -to a_d Hou*_-_sininomto cotat
TJ SolO F urm t6 v
Org
JOURNAL OF THE NATIONAL MEDICAL ASSOCIATION VOL. 98, NO. 7, JULY 2006 1187