Cardiac Emergencies
19
Cardiac emergencies Colin Powell Contents 4.1 Supraventricular tachycardia 4.2 Syncope 4.3 Kawasaki disease 4.4 Cyanotic episodes 4.5 Cardiac failure and congenital heart disease 4.6 Pericarditis and myocarditis 4. 1 Supraventricular tachycardia Supraventricular tachycardia will usually present with signs of congestive cardiac failure or shock, but will also depend on the age of the child. Sinus tachycardia can be up to about 200 beats per minute. Supraventricular tachycardia (SVT) is usually above 220 beats per minute. 4.1 .1 Assessme nt Symptoms Infants usually present with pallor, dyspnea and poor feeding. Older children have palpitations and chest discomfort. Sign s
-
Upload
rizqulloh-taufiqul-hakim-barsah -
Category
Documents
-
view
10 -
download
0
description
gghgh
Transcript of Cardiac Emergencies

Cardiac emergenciesColin Powell
Contents
4.1 Supraventricular tachycardia4.2 Syncope4.3 Kawasaki disease4.4 Cyanotic episodes4.5 Cardiac failure and congenital heart disease4.6 Pericarditis and myocarditis
4.1Supraventricular tachycardia
Supraventricular tachycardia will usually present with signs of congestive cardiac failure or shock, but will also depend on the age of the child. Sinus tachycardia can be up to about 200 beats per minute. Supraventricular tachycardia (SVT) is usually above 220 beats per minute.
4.1.1Assessment
Symptoms
Infants usually present with pallor, dyspnea and poor feeding. Older children have palpitations and chest discomfort.
Signs
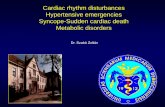
In SVT (Figure 4.1) there is a regular tachycardia with a heart rate usually 180–300 per minute. Hypotension might be present but is often compensated early on in presentation. Heart failure with hepatomegaly with gallop rhythm occurs, especially in infants.
Consult cardiology urgently if tachycardia is broad complex or irregular.

4.1.2Management
The child must be monitored with continuous ECG trace and frequent measurements of blood pressure. The options for treatment are listed below.
• If necessary apply oxygen 10 l min−1 by facemask• If child is shocked (i.e. hypotensive, poor peripheral perfusion, impaired mental state)
proceed to direct current cardioversion (see below)• If child is not shocked treat with intravenous adenosine
Figure 4.1 A 12-lead ECG showing regular narrow complex tachycardia.
Shocked child
If the child is shocked, then direct current cardioversion is needed. You must:
• Call ICU. Ensure experienced staff and full resuscitative measures are present• Ensure child is on oxygen, and has intravenous access• Administer diazepam intravenously if there is any chance of awareness• DC revert using a synchronised shock of 0.5 J kg−1. If this is unsuccessful, increase
dose to 1 J kg−1 and then to 2 J kg−1 if still unsuccessful• An unsynchronised shock is necessary for ventricular fibrillation or polymorphic
ventricular tachycardia
Stable child
If the child is stable, vasovagal maneuvers and adenosine should be tried:
• Vagal maneuvers—use the Valsalva maneuver if child old enough, the gag or icepack/iced water for infants (apply to face for a maximum of 30 seconds). Do not use eyeball pressure.
• Intravenous adenosine
• Insert cannula into a large proximal peripheral vein (the cubital fossa is ideal) with a

3-way tap attached• Draw up starting dose of adenosine 50 µg kg−1. If necessary dilute to 1 ml with
normal saline• Draw up 10 ml saline flush• Turn on the ECG trace recorder• Administer adenosine as a rapid i.v. push followed by the saline flush• Repeat procedure at 2-minute intervals, until tachycardia terminated, increasing the
dose of adenosine by 50 µg kg−1 to a total dose of 300 µg kg−1 for infants of less than1 month, and to a total dose of 500 µg kg−1 to children between 1 month and 12 years.
• Perform 12-lead ECG postreversion
The recorded strip at the time of conversion to sinus rhythm should be inspected and saved, for concealed pre-excitation may only be revealed during the first few beats after conversion to sinus rhythm. After a patient has been reverted, a 12-lead ECG should be performed to look for pre-excitation and other abnormalities. Rapid re-initiation of tachycardia is not uncommon, mostly because of premature atrial contractions stimulated by the adenosine. If this occurs consider trying adenosine again. Side effects including flushing and chest tightness or discomfort are not uncommon but they are usually brief and transient. Rarely atrial fibrillation or prolonged pauses may occur. Adenosine is contraindicated in adenosine—deaminase deficiency (rare immune deficiency) and patients taking dipyridamole (Persantin). Care is required in asthma, as it may cause bronchospasm. If these measures fail to revert the SVT, consult a cardiology specialist.
Disposition
A follow-up plan should be made in consultation with cardiology. Some children may be started on beta blockers. There may be an underlying conduction abnormality such as Wolff-Parkinson-White syndrome.
4.2Syncope
A syncopal attack is brief, usually with sudden loss of consciousness and muscle tone caused by cerebral ischemia or inadequate oxygen or glucose to the brain.
• It usually lasts only a few seconds• The child limp and unresponsive
4.2.1Features
• Tonic—clonic movements can occur with prolonged unconsciousness• The patient is back to normal on awakening

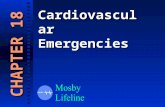
Figure 4.2 Diagnosis of syncope.
4.2.2Cause
There are several causes, including (Figure 4.2):
• Vasovagal (fainting)• Orthostatic or postural hypotension• Cardiac
• structural (e.g. critical aortic stenosis, tetralogy of Fallot, atrial myxoma etc.)• arrhythmia (e.g. prolonged QT, AV block, sick sinus syndrome)

• Respiratory (e.g. cough, hyperventilating, breath holding)• Metabolic (e.g. anemia, hypoglycemia, hysteria etc.)
4.2.3Management
A history of the surrounding events is important. Orthostatic hypotension usually occurs on standing suddenly. Vasovagal collapse is usually associated with environmental or emotional stresses. Structural cardiac lesion is more likely if the syncope is exertional. The patient should be examined for cardiac anomaly (e.g. murmur, heaves etc). Investigations should include an ECG to look for dysrythmias, short/abnormal PR interval (e.g. Wolff-Parkinson-White syndrome) or prolonged QT syndrome.If unconsciousness lasts more than a few seconds and the patient is not fully awake immediately after the event, then consider seizures as a cause (Table 4.1). The patient may need an EEG to clarify this issue. Hysterical syncope generally occurs in front of an audience, patients do not hurt themselves and there is associated moaning or non- rhythmical jerking.
4.2.4Follow up
All patients who have unexplained syncope should be reviewed in outpatients.
4.3Kawasaki disease
Kawasaki disease is a systemic vasculitis that predominantly affects children under 5 years old. Although the specific etiological agent remains unknown, it is believed that Kawasaki disease is a response to some form of infection (although it is not transmitted from person to person). Diagnosis is often delayed because the features are similar to those of many viral exanthems.
The diagnostic criteria for Kawasaki disease are fever for 5 days or more, plus four out of five of the following:
• polymorphous rash• bilateral (non-purulent) conjunctival infection• mucous membrane changes, e.g. reddened or dry cracked lips, strawberry tongue,
diffuse redness of oral or pharyngeal mucosa• peripheral changes, e.g. erythema of the palms or soles, edema of the hands or feet, and
in convalescence desquamation• cervical lymphadenopathy (>15 mm diameter, usually unilateral, single, non-purulent
and painful)
and exclusion of diseases with a similar presentation: staphylococcal infection (e.g. scalded skin syndrome, toxic shock syndrome), streptococcal infection (e.g. scarlet fever,

toxic shock-like syndrome not just isolation from the throat), measles, other viral exanthems, StevensJohnson syndrome, drug reaction and juvenile rheumatoid arthritis. The diagnostic features of Kawasaki disease can occur sequentially and may not all be present at the same time. Moreover, it is recognised that some patients with Kawasaki disease do not develop sufficient features to fulfil the formal diagnostic criteria. Clinical vigilance and recognition of this possibility are necessary to recognise these ‘incomplete’ or ‘atypical’ cases. This is important because the atypical cases are probably at similar risk of coronary complications and require treatment. Other relatively common features include arthritis, diarrhea and vomiting, coryza and cough, uveitis, and gallbladder hydrops. Some patients get myocarditis.
Table 4.1 Differentiating syncope from seizures
Sign Syncope Seizures Hypoglycemia
Period of unconsciousness
Usually seconds Frequently 5 min or longer
Usually over a few minutes
Incontinence Absent May be present Absent
Confusion on waking
Absent Marked for 20–30 min
Usually, slow to improve
Tonic—clonic movements
Occasionally and brief, particularly if unconsciousness is prolonged
Frequently present Frequently absent
EEG Normal Frequently abnormal if done soon after event
Normal
4.3.1Investigations
All patients should have the following investigations:
• ASOT/anti-DNAase B• echocardiography (at least twice: at initial presentation and, if negative, again at 6–8
weeks)• platelet count (marked thrombocytosis is common in second week of illness).
Other tests are not diagnostic or particularly useful. The following may be seen:
• neutrophilia• raised ESR+CRP• mild normochromic, normocytic anemia• hypoalbuminemia• elevated liver enzymes.

Thrombocytosis and desquamation appear in the second week of the illness or later. Their absence earlier does not preclude the diagnosis.
4.3.2Management
Patients require admission to hospital if Kawasaki disease is diagnosed or strongly suspected. Intravenous immunoglobulin (2 g kg−1 over 10 hours) should be given, preferably within the first 10 days of the illness, but should also be given to patients diagnosed after 10 days of illness if there is evidence of ongoing inflammation, for instance with fever or raised ESR/CRP.
Aspirin (3–5 mg kg−1 once a day) should be given for at least 6–8 weeks. Some give a higher dose (10 mg kg−1 8 hourly for the first few days) but this probably adds nothing over immunoglobulin.
4.3.3Follow up
Pediatric follow up should be arranged on discharge. At least one further echocardiogram should be performed at 6–8 weeks. If this is normal, no further examinations are needed.
4.4Cyanotic episodes
Cyanotic episodes occur in children with cyanotic congenital heart disease, in particular tetralogy of Fallot and pulmonary atresia. There may be a previous history of squatting. The episodes usually occur early in the morning, or in the context of stress or dehydration with periods of increased oxygen demand or increased oxygen use. The pathophysiology is not fully understood, but relates to decreased pulmonary blood flow. Most episodes are self-limiting but cause hypoxic-ischemic brain injury or indeed may be fatal.
4.4.1Assessment
The assessment includes consideration of the severity of the cyanosis or pallor with either distress and hyperpnea (not tachypnea), or lethargy and a depressed conscious state. There may be evidence of structural heart disease occasionally with lessening or absence of a previously documented heart murmur.
4.4.2Management
This can be divided into initial measures for short periods of cyanosis and measures for more prolonged problems.

Initial measures
• Put the child in knee to chest position• Give high flow oxygen via mask or headbox• Avoid exacerbating distress• Give morphine 0.2 mg kg−1 s.c.• Do continuous ECG and oxygen saturation monitoring and frequent blood pressure
measurements• Correct any underlying cause/secondary problems, which may exacerbate episode, e.g.
cardiac arrhythmia, hypothermia, hypoglycemia.
If the attack is prolonged
• Consult a pediatrician or a cardiologist• Give intravenous fluids—10 ml kg−1 bolus followed by maintenance fluids• Give sodium bicarbonate 2–3 mmol kg−1 i.v. (ensure adequate ventilation)• Consider admission
4.5Cardiac failure and congenital heart disease
4.5.1Presentation
Congenital heart disease may present as heart failure with or without shock or cyanosis. However, there are many causes of cardiac failure, including non-congenital reasons such as myocarditis. These may present with signs of heart failure, such as breathlessness, hepatomegaly, pallor and sweating, or may be severe enough to present as cardiogenic shock. Remember that heart failure in an infant can mimic bronchiolitis and the child may have contracted bronchiolitis. This in turn may be the precipitating cause of the heart failure. The likely causes are in Box 4.1.
In infancy heart failure is usually secondary to congenital structural heart disease. As pulmonary pressures reduce after birth over the first few hours to days of life, increased pulmonary flow from lesions such as VSD or PDA will become apparent. These infants are likely to have a cardiac murmur audible. Rarer duct-dependent lesions, such as pulmonary atresia or transposition of the great vessels, will also present after a few days to weeks as the duct closes. These infants may have a large liver but may not have a cardiac murmur audible. Coarctation and severe aortic stenosis will also present as the duct closes.

Box 4.1 Causes of cardiac failure
• Primary pump failure
• Myocarditis• Cardiomyopathy
• Left-sided outflow obstruction
• Aortic stenosis• Coarctation of the aorta• Hypoplastic left heart syndrome• Hypertrophic cardiomyopathy
• Left ventricular overload or excessive pulmonary blood flow
• Ventricular septal defect (VSD)• Atrioventricular septal defect• Patent ductus arteriosus (PDA)
• Rhythm disturbance
• Supraventricular tachycardia• Complete heart block
4.5.2Investigation
• CXR may be helpful to demonstrate cardiomegaly with pulmonary plethora or a characteristic cardiac shape and size
• 12-lead ECG• Cardiac echocardiography and cardiac consultation• Infection screen as above• 4-limb blood pressure
4.5.3Management
Shock
If there are signs of shock then treat as in the cardiogenic shock section.
Heart failure
If the ventilation is adequate, then oxygen by facemask will be sufficient. However, if

breathing is inadequate, intubation and artificial ventilation with PEEP will be required. If oxygenation improves with this maneuver, then the likely problem is that of pulmonary congestion secondary to increased flow from a VSD or PDA etc. A heart murmur may be heard and chest X-ray might be helpful in confirming the diagnosis (see below). Treatment needs to be discussed with the cardiologists. It will include oxygenation and reducing the preload with diuretics (with, for example, frusemide 1 mg kg−1 i.v., repeated if no response after 2 hours). Consideration will be given to improving cardiac contractility (using, for example, digoxin or inotropes, such as dopamine or dobutamine) or decreasing the afterload with vasodilatation (using, for example, captopril).
Cyanosis
Increasing breathlessness and cyanosis in the first few days of life is the presentation of the rarer duct-dependent disease, such as tricuspid or pulmonary atresia. In these conditions, oxygen may cause the duct to close further but, if it is considered necessary for ventilation, it should be carefully titrated. Intravenous prostaglandin El (0.01–0.1 µg kg−1 per min) should keep the duct open until cardiac opinion is available. Once a response occurs, the infusion rate should be titrated down. Prostaglandins may cause apnea and so the child should be ventilated during its administration.
All these children require careful monitoring by ECG, pulse oximetry and non-invasive blood pressure measurement. Remember to check blood pressure in lower limbs as well as upper limbs. It is essential to consider sepsis as a differential diagnosis of cardiac failure in infancy and most infants will require a full infection screen and possible antibiotic cover. These children need admission and assessment by the cardiology team.
4.6Pericarditis and myocarditis
Pericarditis and myocarditis can be bacterial, caused by Hemophilus influenzae or Staphylococcus aureus, or viral, caused by, for example, Coxsackie B. Children can present ill-looking, and should be considered in the differential diagnosis of sepsis in infancy.
Suggested reading
Penny, D.J. and Sherkerdemian, L.S. (2001) Management of the neonate with symptomatic congenital heart disease. Arch. Dis. Child. Fetal. Neonatal Ed. 84:F141–145.