Cardiac diseases in pregnancy - Wikispaces disease in... · Cardiac diseases in pregnancy •< 5 %...
38
Cardiac diseases in pregnancy Dr.Badi Albaqawi, MD Consultant Obs & Gyne MFM specialist KFMC-WSH, Riyadh
Transcript of Cardiac diseases in pregnancy - Wikispaces disease in... · Cardiac diseases in pregnancy •< 5 %...

Cardiac diseases in pregnancy
Dr.Badi Albaqawi, MD
Consultant Obs & Gyne
MFM specialist
KFMC-WSH, Riyadh

Objectives :
CONGENITAL HEART DISEASE
RHEUMATIC HEART DISEASE
CARDIAC ARRHYTHMIAS
ISCHEMIC HEART DISEASE
PERIPARTUM CARDIOMYOPATHY
MANAGEMENT OF CARDIAC DISEASE DURING PREGNANCY

Cardiac diseases in pregnancy
• < 5 % of pregnancies
• Important cause of maternal mortality.
• The CVS adaptations to pregnancy, delivery, and the early puerperium can trigger acute cardiovascular decom-pensation in women with high-risk lesions.
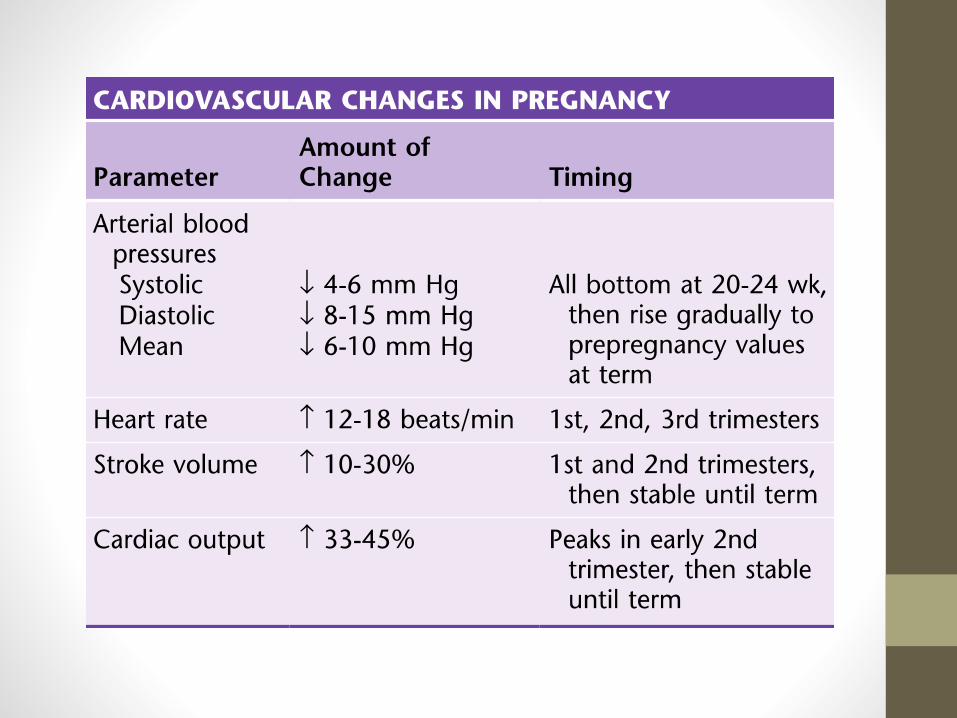

Physiological changes in pregnancy
parameterChanges at various times (weeks)
5 12 20 24 32 38
HR ↑ ↑↑↑ ↑↑↑ ↑↑↑ ↑↑↑↑ ↑↑↑↑
SBP ↔ ↓ ↓ ↔ ↑ ↑↑
DBP ↔ ↓ ↓↓ ↓ ↔ ↑↑
SV↑
↑↑↑↑↑ ↑↑↑↑↑↑ ↑↑↑↑↑↑ ↑↑↑↑↑↑↑↑↑↑
CO ↑↑ ↑↑↑↑↑↑ ↑↑↑↑↑↑↑ ↑↑↑↑↑↑↑ ↑↑↑↑↑↑↑ ↑↑↑↑↑↑↑
PR ↓↓ ↓↓↓↓↓ ↓↓↓↓↓↓ ↓↓↓↓↓↓ ↓↓↓↓↓↓ ↓↓↓↓↓
LV EF ↑ ↑↑ ↑↑ ↑↑ ↑ ↑
RHEUMATIC HEART DISEASE
• Most common lesion associated with rheumatic heart disease is mitral stenosismitral regurgitation.
• Mitral stenosis valve area less than 1.5 cm2, are at high risk of developing heart failure, subacute bacterial endocarditis, and thromboembolic disease & a higher rate of fetal wastage.

RHEUMATIC HEART DISEASE (Mitral stenosis)• Mitral stenosismechanical obstruction
associated with mitral stenosis worsens as cardiac output increases.
• Asymptomatic patients symptoms of cardiac decompensation or pulmonary edema as pregnancy progresses.
• Severe mitral stenosis Atrial fibrillation

CONGENITAL HEART DISEASE • ASD
• VSD primary pulmonary hypertension (Eisenmenger syndrome)
• Cyanotic heart diseases such as tetralogy of Fallot and transposition of the great arteries.
CONGENITAL HEART DISEASE • If the anatomic defect has been corrected
during childhood with no residual damage, the patient is expected to go through pregnancy without complications.
CONGENITAL HEART DISEASE • Patients with primary pulmonary
hypertension or cyanotic heart disease with residual pulmonary hypertension are in danger of experiencing decompensation during pregnancy.

CONGENITAL HEART DISEASE • Pulmonary hypertension from any cause is
associated with an increased risk of maternal mortality during pregnancy or in the immediate postpartum period.
• Care should be taken to avoid overloading the circulation and precipitating pulmonary congestion, heart failure, or hypotension, all of which may lead to hypoxia and sudden death.

CONGENITAL HEART DISEASE • Significant pulmonary hypertension with
Eisenmenger syndrome is a contraindication to pregnancy due to the high maternal mortality that accom-panies this condition.

CARDIAC ARRHYTHMIAS
• Palpitations are common in pregnancy
• If an arrhythmia is detected, an echocardiogram underlying structural heart disease.
• Atrial premature beats are common, but usually benign and do not require therapy

CARDIAC ARRHYTHMIAS
• Quit caffeine and cigarettes.

CARDIAC ARRHYTHMIAS (SVT)• The management of supraventricular
tachyarrhythmias (SVTs) with carotid massage or the Valsalva maneuver, antiarrhythmic therapy, or direct current cardioversion is based on the patient’s hemodynamic status.

CARDIAC ARRHYTHMIAS (AFB) • Atrial fibrillation and atrial flutter, though
much less common than SVTs, are more serious and are usually associated with underlying maternal cardiac disease.

CARDIAC ARRHYTHMIAS
• Tests of thyroid function should also be done.
• Treatment is similar to that in nonpregnant adults, although antiarrhythmic agents cross the placenta and the fetal risks are largely unknown.
• Heparin (or low-molecular- weight heparin) should be used instead of warfarin when anticoagulation is indicated.
ISCHEMIC HEART DISEASE
• Comorbidities maternal age, DM,HTN
• Stress testing and angiography should be done before pregnancy.
• Use of lipid-lowering agents or angiotensin-converting enzyme (ACE) inhibitors should be avoided during pregnancy .

PERIPARTUM CARDIOMYOPATHY
• NO underlying cardiac disease, and symptoms of cardiac decompensation appear during the last weeks of pregnancy or within 6 months post- partum.

PERIPARTUM CARDIOMYOPATHY • Risk factors a history of preeclampsia or
hypertension and those who are poorly nourished.
• Hypertensive or drug-induced cardiomyopathy, ischemic heart disease, viral myocarditis, and valvular heart disease must be excluded .
• Decreased left ventricular ejection fraction (LVEF < 45%) .

PERIPARTUM CARDIOMYOPATHY • Rx including delivery if the disease
presents antepartum), maternal mortality rates have been declining but are still at least 10%.
• These women have a 30-50% risk of persistent cardiac dysfunction and a 20-50% recurrence rate in subsequent pregnancies.

MANAGEMENT OF CARDIAC DISEASE DURING PREGNANCY
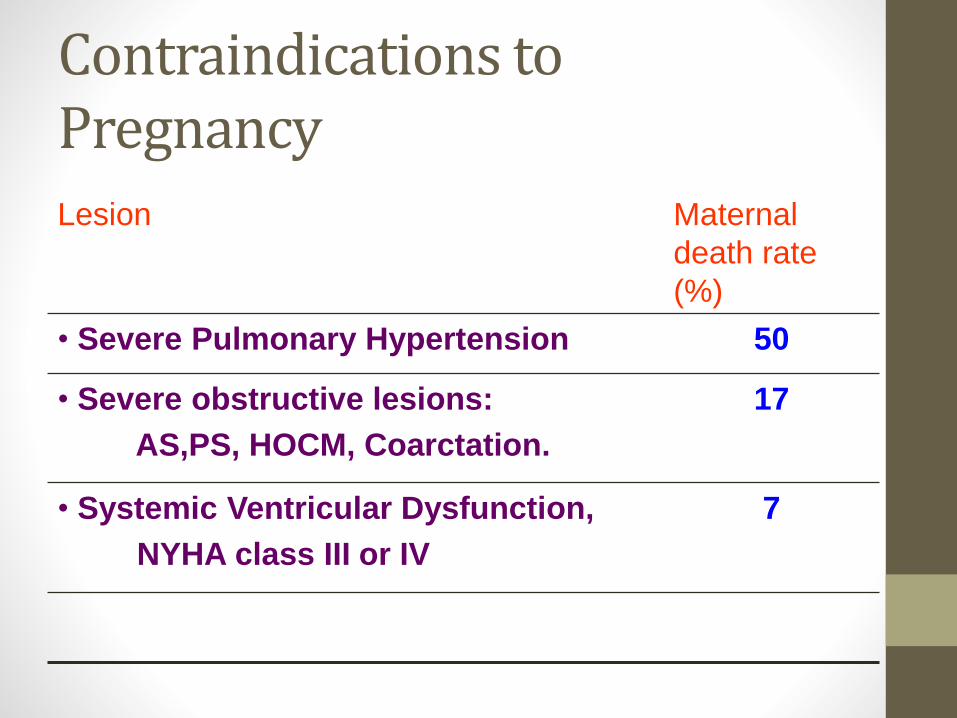
Contraindications to Pregnancy
Lesion Maternal
death rate
(%)
• Severe Pulmonary Hypertension 50
• Severe obstructive lesions:
AS,PS, HOCM, Coarctation.
17
• Systemic Ventricular Dysfunction,
NYHA class III or IV
7
MANAGEMENT OF CARDIAC DISEASE DURING PREGNANCY
• The maternal and fetal risks for patients with class I or II disease are small.
• Greatly increased in patients with class III or IV disease or if they have cyanosis.
• The type and severity of the defect is important as well.

MANAGEMENT OF CARDIAC DISEASE DURING PREGNANCY
• Mitral (valve area <2 cm2) and aortic stenosis (valve area <1.5 cm2) carry a much higher risk of decompensation than do mitral or aortic regurgitation.

High risk of morbidity and mortality • Significant pulmonary hypertension
• LVEF less than 40%
• Marfan syndrome
• a mechanical valve
• a previous history of a cardiac event or arrhythmia, or significant comorbidities.

Prenatal Management
• Cardiologist, a maternal-fetal medicine specialist, and an anesthesiologist .
• Careful history and physical examination should be performed, and an ECG and echocardiogram should be obtained.
• Frequent prenatal visits are indicated, and hospital admissions may be needed, especially for patients with class III or IV cardiac disease.

HistoryExercise capacity
Current or past evidence of HFAssociated arrhythmias
Physical exam
Cardiac HemodynamicsSeverity of heart disease, PA pressures
Echo, MRI.
Exercise testingUseful if the history is inadequate to allow assessment of functional capacity
During pregnancyEvaluate once each trimester and whenever there is change in symptoms Multidisciplinary
approach, Fetal Echo
Be
fore
co
nce
pti
on
During Labor & DeliveryMultidisciplinary approach (Obstetrician, Cardiologist, Anesthesiologist)
Tailor management to specific needs

Prenatal Management
AVOIDANCE OF EXCESSIVE WEIGHT GAIN AND EDEMA
• excessive salt intake should be avoided.
• Rest in the left lateral decubitus position
• Adequate sleep
• Aldosterone antagonists should be avoided because of their potential antiandrogenic effects on the fetus.

Prenatal Management
• AVOIDANCE OF STRENUOUS ACTIVITY.
• AVOIDANCE OF ANEMIA.
• AVOIDANCE OF INFECTION.
• Cesarean delivery should only be performed for clear obstetrical indications, in part because of the increased risk of endometritis and wound infections.

Prenatal Management
ANTICOAGULATION
• Mechanical valves and those with atrial fibrillation require full anti- coagulation with heparin or low-molecular-weight heparin in pregnancy.

Prenatal Management
FETAL ECHOCARDIOGRAPHY
• Increased risk of having children with heart disease.

Management of Delivery and the Immediate Postpartum Period
• Cardiac patients should be delivered vaginally unless obstetric indications for cesarean delivery are present
• frequent assessment of vital signs, urine output, and pulse oximetry.
• Adequate pain relief is important.
• Pushing should be avoided during the second stage of labor

Management of Delivery and the Immediate Postpartum Period
• To minimize the risks of volume overload or depletion, careful attention should be paid to fluid balance (avoiding overload)
• Prevention of uterine atony (avoiding depletion from blood loss) with oxytocin and uterine massage.
• Methergine should be avoided

Risk of endocarditis
• Antibiotic prophylaxis is recommended only for high-risk patients
• Prosthetic valves, unrepaired or incompletely repaired congenital heart disease, or a previous history of bacterial endocarditis.

Management of Delivery and the Immediate Postpartum Period
Acute cardiac decompensation
Medical management is directed at correcting the precipitating factors and may include administration of morphine sulfate, supplemental oxygen with ventilatory support if needed, and an intravenous loop diuretic (e.g., furosemide) to reduce fluid retention and preload.

Management of Delivery and the Immediate Postpartum Period
• β-Blockers should not be used in the setting of acute heart failure.
• Vasodilators such as hydralazine, nitroglycerin, and, rarely, nitroprusside are used to improve cardiac output by decreasing afterload.

Management of Delivery and the Immediate Postpartum Period
• Very frequent monitoring of vital signs, urine output, and pulse oximetry, along with continuous electrocardiographic monitoring, is advised.